
Abstract
Healthcare systems in Europe are undergoing a transformation due to high costs of care. Remote measurement technologies (RMTs) such as wearable sensors, mobile apps and data analytics are expected to enable this transformation. To this effect, European funding bodies have announced calls for RMTs that make it possible to conduct data driven pre-emption of episodes of disease to avoid rehospitalisations. We follow the work of a group of investigators of a European research project funded by the European Commission and the Pharmaceutical industry seeking to develop RMTs and also explore ways in which these technologies could work in the clinic. For this reason, they engage in wide consultations with stakeholders such as patients, doctors, healthcare managers and regulators. Through their proposals, which we view as exercises in clinical world-making in action, we study how the hospital and clinical action may be transformed. These exercises raise questions about which actors are included in these proposals and what different roles they are given, which actors reject these technologies and what kind of counterproposals they produce. We show that the introduction of big data analytics and RMTs in the clinic have diverse consequences: they provoke changes to the core business of pharmaceutical industry and imply different understandings of what healthcare and therapy is or should be, requiring a different organisation of the hospital, its link to the home, and a modification of the patient–physician relationship. As we show, the direction of the transformation of the clinic is still highly uncertain.
Keywords
Introduction
Healthcare systems in Europe are currently undergoing a transformation. The challenge consists in the need to adjust them to keep them sustainable. As people live longer, this augments the prevalence of chronic conditions in the population, such as neurodegenerative diseases, cardiovascular diseases, cancer, diabetes and mental disorders, estimated to cost billions (European Commission, 2021). The cost of care has further risen due to new expensive treatments and new types of drugs during a time of austerity measures, cutting down public expenditures (European Commission, 2019) and a missing working force in the healthcare sector taking care of an aging population.
Transformation of healthcare systems can happen in diverse ways. Models for healthcare policies such as outcome-based healthcare and value-based medicine (EIT Health, 2020; European Commission, 2019; Porter and Teisberg, 2006), have been formulated to optimise the use of limited resources. These models propose the reorganisation of hospital routines to introduce protocols that cut down costs and improve clinical ‘health outcomes’ by bringing the patient to the clinic at the right time, adjust treatment based on their individual clinical profile and discharge them at the right time. Importantly, these policy models also embrace precision medicine and the promise of a fundamental change from reactive medicine that focuses on the treatment of existing diseases, towards ‘high-value interventions’ early in the patient's disease trajectory through measures of preventive medicine (Lewis, 2022). According to these models, predicting risk brings value both to the patient and the healthcare system: patients can manage symptoms early on (before they become difficult to manage) and healthcare systems can avoid unnecessary and costly rehospitalisations.
These models give a central role to digital technologies (Hurst et al., 2019). This especially pertains to the affordances of so-called remote monitoring technologies (RMTs), such as wearable sensors, mobile apps and data analytics platforms that would collect and analyse data from patients in real time. Such technologies are both mobilised to measure health outcomes based on real world evidence and are expected to effectuate the targeted predictions needed for this kind of anticipatory medicine. Therefore, RMTs bring together specific ideas about measurement, continuous data collection, early intervention, but also, as we will show in this article, ideas about the patient-doctor relationship, reimbursement of therapies and innovation of new medical devices and medicines.
This approach has also increasingly taken centre stage in funding programmes for research and innovation in Europe such as the Innovative Health Initiative (IHI), a public-private partnership (PPP) between the European Union and the European life science industries. As we discuss, these actors envision data driven technologies offering the possibility to pre-empt disease, by intervening at early stages of its development. Importantly, RMTs are credited with the capacity to revolutionise treatment of chronic disease by making possible the prediction of each relapse throughout the patient journey. For central nervous system (CNS) disorders, such as manic depression and epilepsy, this would be key: CNS disorders are detrimental to patients’ quality of life. Patients experience periods during which they can manage their conditions well, but these are followed by periods of relapse where things get out of control. Patients and clinicians consider prediction a valuable outcome (to stop relapse from happening altogether) and given the costs of relapse, healthcare managers and funders want to minimise it as much as possible (Basch, 2017).
The focus of the article is on ways in which the hospital and clinical action will be transformed by the introduction of digital remote monitoring technologies. For this purpose, we followed the work of a group of investigators of a major European consortium in a research project seeking to develop RMTs (mobile apps and a data analytics platform) for patients with serious conditions of the CNS. The project was funded by the IHI and the research team wanted to test the scientific feasibility of developing such tools, the acceptability of these tools for patients (Sideri and van Dijk, 2024), but also ways in which RMTs and big data analytics can be realistically inserted in the clinic to improve health outcomes and cut down costs. The project partners were from various university departments spread across Europe and included a large multidisciplinary team (computer scientists, data analysts, clinicians), a patient board, representatives from pharmaceutical companies and people who had experience with consulting national regulators about reimbursing digital therapies.
We explore how certain actors in the funded project, which we will call project entrepreneurs, propose to simulate the transformation of the clinic in advance. For this reason, they are engaged early on with stakeholders who would be transformed by the introduction of RMTs if these tools would be inserted in the clinic. These actors perform the entrepreneurial work of aligning technological innovation with the interests of potential allies to secure its stability (Callon et al., 2011; Latour, 1999). This work was performed firstly by project leaders, who were from medical schools with a scientific and clinical interest to develop digital medical tools to address CNS. They put the research consortium together and wrote the funding application. IHI project funding specifically requires that industry partners (pharmaceutical companies) provide ‘“in-kind” contributions (e.g. their researchers’ time, laboratories, data, compounds)’. 1 Secondly, the people who led a specific work package within the project on ‘clinical pathways’ are also considered project entrepreneurs. Their work was dedicated to collecting all possible information within and outside the research consortium to assess the kind of added value digital devices could bring to actors in the clinical ecology.
The project entrepreneurs collaborated in the research team with a patient board (with representatives of patient organisations) and pharmaceutical companies, but also conducted wide consultations with stakeholders such as clinicians, medical device regulators and health managers. As a result, project entrepreneurs produced specific propositions about where to insert these devices in the existing organisational routines of the clinic. We show that this practical (or co-productive) exercise is an attempt to increase their chances to interest society when the technology is ready for adoption and it essentially consists of world-making in action (Callon et al., 2011). The project entrepreneurs had specific propositions about effective integration of the digital tool in the network of existing actors, including the IHI, patients, clinicians, pharma companies, health managers and medical device regulators. We here studied which actors became enrolled or not, which actors reject the project entrepreneurs’ proposals and what kind of counterproposals they produce. We also inquire into the ways actors are transformed in these processes and into the mediating role of RMTs. As we show, the direction of transformation of the clinic is highly uncertain.
Theory: Technological world-making and delegation of action
Even if the digital tool would pass all the scientific tests and proves effective (in offering precise measurements), the next challenge pertains to its perilous introduction into the ‘big world’: will the knowledge and devices produced in the safe and confined space of the laboratory be able to survive when introduced into the world of the clinic?
Early studies in STS, especially Actor-Network Theory, have shown how entrepreneurial scientists and technologists do not only promote new knowledge or new technological devices but combine this with proposals of the kind of worlds in which these technologies would operate (Callonm, 1986; Latour, 1987). Such ‘cosmograms’ often include a sketch of a certain history we are moving away from, and which has given rise to a certain set of problems. The introduction of a new technology addresses such problems through envisioning a new future direction, a specification of the range of actors and entities involved, and a change in the roles, interrelations, or even identities assigned to them in this newly proposed future world. Whether this world eventually materialises will depend on the success of the proposal to translate the interests of the different actors mobilised. Does the proposal manage to render itself indispensable and oblige these actors to reach their goals by passing through this new checkpoint (the so-called obligatory passage point)? Or will they eventually reject the roles proposed for them? In certain cases, this will require catering to goals these actors explicitly entertain. In other cases, the newly introduced technologies might require transformations of their identities and of important relations between them.
This notion of transformation of actors and actions due to new technologies also gets us to the topic of delegation and redistribution of human agency to and through technological devices (Latour, 1999, 182). As Latour remarked, actions are not just performed by human beings, but comprise a range of ‘actorial roles’ some performed by humans others by objects. After the introduction of new technologies in society, some of these roles previously performed by humans might henceforth be delegated to technologies. We will explore these qualities of technological delegation of action, transformation of identities and world-making potential in the case of remote monitoring technologies. In this sense, these devices are like little monads that reflect an entire world inside themselves, like the intricate convex mirrors projected on canvas by diverse painters as Jan van Eyck and Maurice Escher. The world that these tiny devices have been burdened to transform is that of the broader healthcare ecology.
Different types of alliances are required for this that would satisfy the interests of a range of actors: doctors need to see how the device can improve therapy, industry must see opportunities in a market saturated with regulatory obligations, insurance companies want evidence before reimbursing, managers of public healthcare systems seek solutions to cut costs that weigh heavy on their budgets, regulators want to see general safety and performance requirements for medical devices satisfied, and patients demand better healthcare. In the language used by the project entrepreneurs, the device must be valuable or provide a specific ‘added value’ to each of the potential allies, given that ‘value’ is a multi-faceted concept within digital predictive medicine (Birk et al.., 2021). The concerns of all these allies need to be translated through the capture of data through digital means. The project entrepreneurs will thus try to make these digital devices the obligatory passage points for those whose support they seek, by trying to show their indispensability for fulfilling their needs (Callon et al., 2011).
A difference of our current case with older STS studies, is that this return to the real world is simulated in advance. The actors that are proposed to be transformed by the technologies have to be present from the start in the research project and partially agree to this transformation. Alliances are thus assembled early, and are already considered when drafting the project proposal. This early presence is of course not coincidental. Research projects funded by the European Union have increasingly incorporated requirements for the actors deemed relevant ('stakeholders’) to be involved early in research and innovation processes. In the medical field this can be seen in the IHI. One of its main tasks is fostering collaboration between the pharmaceutical industry, regulatory bodies, patient organisations, academia, clinical centres and enterprises (CEU, 2008). There are concrete requirements to ‘involve potential end-users and stakeholders in your proposal’, stressing this is not limited to consulting external actors, but to involve them ‘as partners in the project, or.. as members of an advisory board or user group tasked with testing the results and providing feedback’ (EC, H2020 Manual). This was indeed the case: since the project we followed was funded by IHI, representatives of pharmaceutical companies (who were also involved in drafting the IHI 2015 work plan) were included as partners and patient representatives formed a patient board as an integral part of the project.
The article is structured as follows: in section ‘A turn to digital pre-emption in medical innovation governance’ we analyse how ideas of using digital monitoring technologies to preempt instances of diseases develop in European medical innovation policies and funding structures. In sections ‘Uses for RMTs in the clinic’ and ‘Values and limits for clinical allies’, we look inside the world of clinical routines and show ways in which both policies pushing for adoption of digital tools and funding calls anticipating a world of digital innovation, threaten to change the position of established actors in healthcare (i.e. physicians and patients) (see also Lowe, 2001). In section ‘Extensions of the pharmakon’, we discuss the role of pharmaceutical companies as actors pushing for digital transformation and who may simultaneously themselves be profoundly transformed, given the push by regulators to make them meet higher safety, efficacy and quality standards. In the discussion section, we dig deeper into RMTs role in mediating the therapeutic relationship between physicians and patients, leading the way to transforming care in ways that may be (partially) rejected by the actors involved (see also Berg, 1996). There may be tensions concerning what RMTs imply for funders, pharmaceutical companies, managers and those working with RMTs in the clinic and of course patients (Bloomfield, 1991). RMTs may be rejected but if accepted, even partially, any transformation might be profound.
Method/Methodology
The article uses qualitative data comprising transcripts of institutional documents produced by regulators and funding bodies, such as regulations, strategic research agendas, annual work plans, call texts, and communication materials such as Q&As and webinars. Secondly, we studied documents by the research consortium such as reports on annual meetings, project deliverables (especially three stakeholder reports from the work package on clinical pathways in which the project entrepreneurs were active), and other project documents. Thirdly we engaged in interviews with members of the research consortium, regulators and software companies operating in the same space of innovation.
Regarding interviews, we conducted 24 in total, from which 17 with researchers from the consortium with diverse backgrounds (four psychiatrists, two clinical psychologists and seven computer scientists), including 2 interviews with patient representatives, and 3 interviews with representatives of pharmaceutical companies. Our interviewees participated in different work packages of the project (i.e. building a platform, engaging patients, clinical pathways), and came from various levels in the hierarchy (leaders and team members). The remaining 7 interviews were with people from the European Commission (2) and software companies (5) operating in the medical device market and promoting privacy friendly solutions. These interviews gave us insights into broader regulatory, policy and ethical problems. Interviews were conducted between 2019 and 2020 on condition of anonymity and an informed consent document approved by the university ethics committee was signed by participants after discussing with them its contents. Interviews were semi-structured allowing our interviewees to choose topics of concern to them and express their views freely. We sought to mainly analyse interviewees’ understandings and reports on how they envision the clinical space and how clinical action will be transformed due to introducing RMTs, what they expect from using such tools, where the limits of any transformation lie, the challenges they see in introducing big data analytics tools into the clinic, how they construct strategies for addressing them, and how different views suggest alternatives. We also used situational analysis to understand the ‘big picture’ of the broader political, economic, regulatory and innovation context. Materials were synthesised into relational maps during an iterative process with findings (Clarke et al., 2018). Three types of maps were produced: situational maps, social world/arena maps, and positional maps, which formed the basis for the analysis. In the following sections, we refer to reports and interviews in a way that preserves anonymity of interviewees, and we conceal the identity of the research project.
A Turn to Digital Pre-emption in Medical Innovation Governance
In this section, we want to dig deeper in the larger set of research policy frameworks behind and leading up to the call in which the project we followed was funded. We argue that within this set of policies we can detect a certain ‘innovation frame’ (compare Jasanoff, 2016). Such an innovation frame includes important problematisations of the field in question, such as framing of societal problems; the future direction that research and innovation will need to take to address these problems; and the specific assembly and reconfiguration of actors required for this task (see Rommetveit et al., 2020). The innovation frame in question was explicitly called ‘digital pre-emption’ by the IHI (WP, 2015), the funders of the research project we followed. It assigned a crucial role to digital technologies such as remote measurement technologies (RMTs) and specifically tied them to prevention and cutting down costs. This innovation frame was anticipated by crucial policy documents establishing the European Commission's Horizon 2020 Program (CEU, 2013), and the documents that operationalise it into strategic research agendas (IHI SRA, 2014), annual work plans (IHI WP, 2015b), research programs and concrete calls for research project proposals (IHI CfP, 2015a).
Indeed, prevention and early detection were already identified as societal problems in early discussion fora in which scientists put forward their visions for the H2020 program (Copenhagen Research Forum, 2012). They discussed the importance of a ‘shift toward personalised medicine’ (p. 8) aligning with literature that describes it as part of a fundamental change away from reactive medicine (focusing on therapy for preexisting diseases) and towards anticipatory medicine that predicts risk of developing a certain disease (Galas and Hood, 2009). Yet, the emphasis in personalised medicine has been on biological data regarding people's genes (Flores et al., 2013). Digital technologies were originally only mentioned to the extent they facilitated computation of large amounts of bio-genetic data of individual patients thus enabling genetic personalisation (Galas and Hood, 2009). Over time, there has been an increased appraisal of the affordances of digital technologies, such as the possibility for patients to search and exchange relevant information about their health conditions online, self-management of patients of their personal lifestyle data about activity levels, sleep and nutrition (Flores et al., 2013), and obtaining real world data needed for clinical trial validation of drugs through IT monitoring devices (IMI SRA, 2014: 28). But as we show, data analytics for prevention and personalised medicine have now taken centre stage in funding programmes such as ones by the IHI.
Of particular importance is the IHI's annual working plan setting research priorities for 2015 (IHI2 WP, 2015b), as it prepared the ground for the funding call to which the research consortium that we studied applied. It specifically mentioned problems associated with chronic disease pointing both to inadequacies of clinical care and the problem of cost-effectiveness. The IHI WP (2015b) report explains: ‘This change in focus …will drive a paradigm shift towards disease interception, i.e., move from a ‘diagnose and treat’ to a ‘predict and pre-empt’ approach. In this model, pre-emption, i.e., intervening early enough in the disease process to prevent serious effects of the disease associated with progression, becomes a critical component of managing chronic disease. Additionally, as the trajectory of chronic diseases is often cyclical, this offers multiple interception opportunities to prevent serious decline, for example, predicting and pre-empting recurrence/suicidality in severe depression. Measuring physiological and activity-based parameters remotely and continuously via unobtrusive on-body sensors or smartphones has the potential to revolutionize our ability to predict and pre-empt harmful changes in disease trajectory (IHI WP, 2015b, our italics)’.
In short, we see that with the accompanying digital turn, a distinct socio-technical model of healthcare innovation is at stake that is different from that of bio-personalisation (Baumgartner, 2021). The distinctive traits are: the collection of digital data about behaviour of patient with a manifest diagnosed chronic disease (not just a risk of developing a disease), and the continuous measurement and analysis of data to pre-empt concrete predicted episodes of this disease through specific measures of interception (in a determined window of time). As an interviewee (Interview 2, psychiatrist) remarks: One can imagine, .. given the fairly catastrophic consequences of developing a manic episode, [the usefulness] for the patients [of] having some early warning sign .. specific to an individual. You are talking about some use already…. So, it's very much .. about ongoing care and prevention of worsening ..[of people that] were already in the system.
But first, we will ask: How will these digital devices be adapted to the local conditions of the clinic and how will the clinical ecology need to be transformed to accommodate these devices?
Uses for RMTs in the clinic
How would pre-emption of episodes of disease through RMTs work in practice? To answer this, we study the work of the project entrepreneurs in a project work package dedicated to ‘translating [RMTs] efficiently and effectively into real-world clinical applications and services’ (Stakeholder report 1). We follow how the project entrepreneurs engage in mapping the world of the clinic, inserting these devices at places where they could be of interest and exploring their potential uses.
We will refer to the clinic as the institutional hub that links the main sites of healthcare such as the general practitioner, clinics, hospitals; healthcare actors such as doctors, nurses, patients, administrative staff, managers; and a range of normal and specialised instruments, professional routines, regulations, organisational procedures and schedules, protocols and social relations. As such it is a complex heterogeneous space with many local organisational and cultural differences from hospital to hospital, region to region and country to country.
This makes the clinic not immediately accessible as the entry point for exploring the question of added value of RMTs. Some sort of map is needed to navigate this obstinate medical territory. The project entrepreneurs find the solution in the mediating ontology of clinical pathways. These are ‘care maps’ or an ‘overview’ that provides an ‘outline [of] the optimal sequence and timing of interventions’ (De Bleser et al., 2006: 561). As the project entrepreneurs state, clinical pathways represent ‘healthcare provision processes and clinical decision points’ and as such they provide a schematic ‘representation of the organizational and decision-making context in which RMTs will be implemented in clinical care settings’ (Stakeholder Report 1). In this sense, clinical pathways already carry their managerial orientation on their sleeves (Martin et al., 2017), and such managerial organisation varies from one healthcare system to the other (although good practice benchmarks are provided). For example, to identify and organise pathways around a disease in a specific healthcare system, the system needs to first assemble the fact base. Taking the example of depression, it is crucial to establish prevention results in better care and cutting down costs. Then, the system needs to determine when, where, and how the prioritised services can best be delivered (in the case of major depression, a general practitioner or a psychiatrist? How often and why? What types of treatment should be prioritised?). Once pathways are established, they become rigid: they constrain ways in which new interventions can be introduced into the clinic.
Digital devices barely figured in the literature on clinical pathways and there were no clear mechanisms to introduce them. The project entrepreneurs had to address this problem by linking clinical pathways to ‘new concepts of value’ (they specifically refer to value-based healthcare frameworks discussed in the introduction) to capture the benefit of these changes for the different actors involved (Stakeholder Reports 1 and 2). Medical thinking about clinical pathways has been very centred on healthcare professionals, whereas a broader range of relevant stakeholders needs to be identified, such as patients, pharma, insurers, and researchers. Thus, they make proposals about where to integrate RMTs in clinical practice and how they can bring value to diverse stakeholders.
After reviewing the relevant literature and consulting partners internally, the project entrepreneurs produced a figure that visualises the major decision points in the clinical pathways (Figure 1). They used the colour red to indicate no potential role for RMTs (i.e. they explicitly saw no role for RMTs in initial diagnosis). Yellow indicated a potential role (i.e. they saw potential in initial management after a diagnosis). Green on the other hand, indicated a definitive role for RMTs. Taking the example of depression, the project entrepreneurs saw a definitive role in cases of persistent symptoms especially where there is inadequate response to existing treatments. They also saw a role in cases of complex and severe depression. In these instances, they proposed that objective monitoring and prediction of relapse can bring value to patients, clinicians, and hospital managers. They suggested (Stakeholder Report 2) various use cases for RMTs such as collecting data in great detail and frequency so as to provide a fine-grained image of the condition of the patient; measure patient response to certain regimes of treatment; measure their adherence to medication; and crucially, predict relapse based on a patient's individual data (so called ‘red flags’, warnings a mobile app sends to the patient).
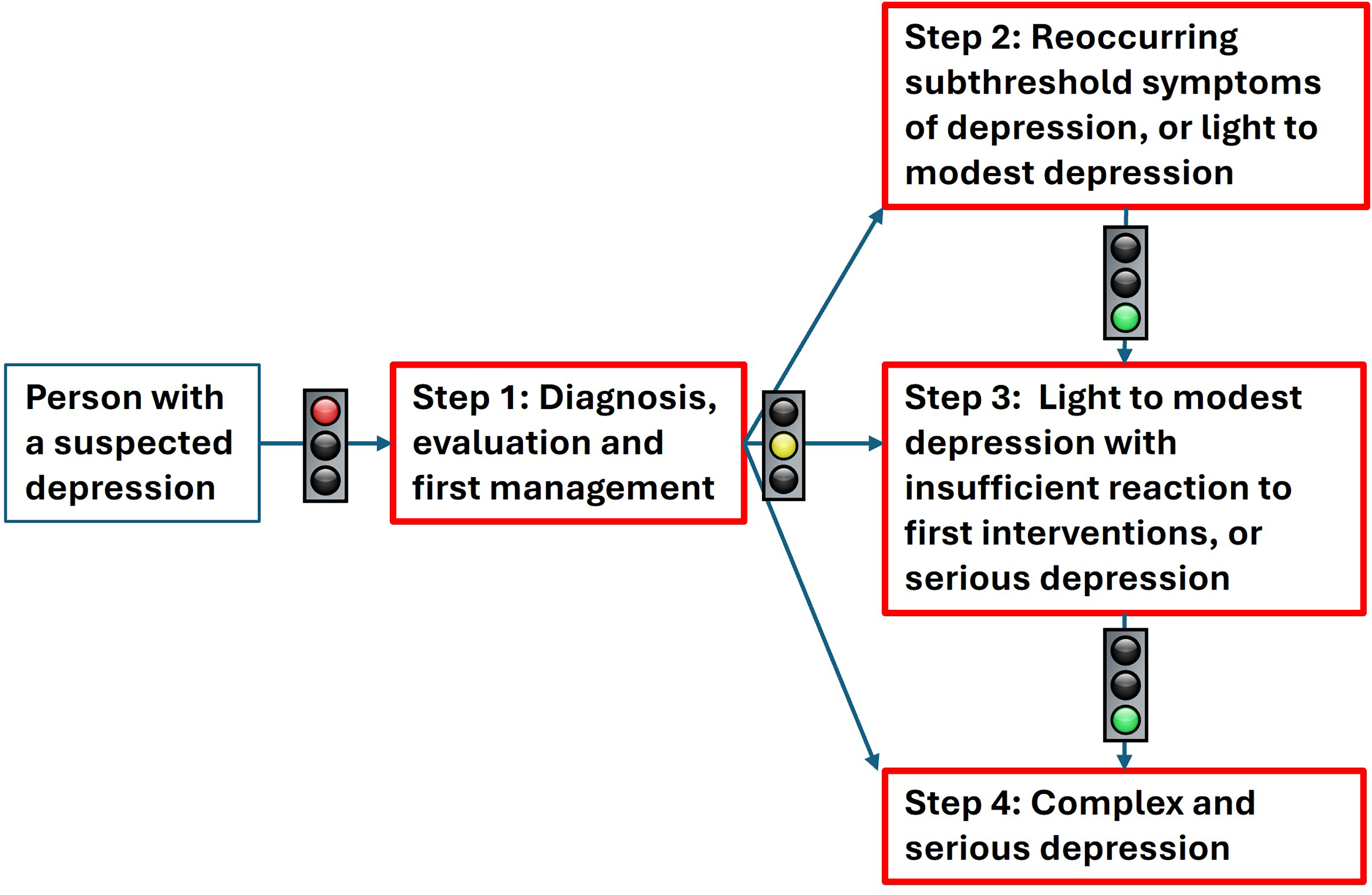
Colour ‘coding for potential role of RMT in depression clinical pathway’. Image inspired by Stakeholder Report 1. Traffic lights attributed to maix, derived from: Ampel.svg: CC-BY-SA 2.5.
Our interviewees confirmed that adjusting treatment and red flags are of major importance: ‘this could be helpful in allowing …withdrawal of patients from medication earlier’ (Interview 2, psychiatrist). Furthermore: ‘one of the aspirations is .. to identify signatures, of early clinical change in which case [the patient] would be prepared to act on that’. As the interview emphasises, the goal is not only prediction, but also to make patients act on that information so that events of relapse are intercepted. This includes contacting their doctor and effectively bringing the patient to the clinic to intervene at the right window of time (Interviews 6, 13 with clinical psychologists; interviews 2, 4, 15, with psychiatrists), which is specified according to a person's individual data signature (Interviews 1, 3, 8, 12, 14, 21 with computer scientists).
Values and Limits for Clinical Allies
The use cases articulate certain problems and ways in which RMTs can be a solution. There is of course no guarantee that the initial value assessments of RMTs and the use cases proposed by the project entrepreneurs will correspond with the valuations of the relevant actors working on the terrain. A further task in this project is therefore to elicit the opinions of these actors on these proposals. Therefore, later in the project, interviews and a large-scale survey were conducted with stakeholders, especially clinicians such as doctors, nurses, clinical psychologists, physiotherapists, and dietitians. The project entrepreneurs stressed the importance of early engagement and co-design with healthcare practitioners before the RMT become applied in practice. For them, this is the way to establish new ways to think about ‘value’ challenging established concepts premised solely on the drive to cut down costs. The second report thus discusses the use case in terms of the benefits (or interests) of RMTs for the different actors (or ‘beneficiaries’). In this scenario, a specification is produced about how this benefit will be operationalised, and the challenges (or ‘obstacles’) that need to be overcome for their implementation in clinical practice.
Clinicians
The use cases would provide various kinds of benefits for clinicians. First, clinicians said that they would lead to better scientific and diagnostic understanding of depression. ‘depression is .. the most imprecise diagnosis. We have this huge kind of amorphous blob of different sorts of symptoms and presentations. These behavioral .. markers are potentially a very nice way ..to tease apart different subtypes.. in .. precision psychiatry’. (Interview 4, psychiatrist).
Second, clinicians agreed that the use of RMTs could lead to better validation of treatment and to more effective health outcomes. The ongoing monitoring of patients enables determining effectiveness of various kinds of treatments in real world settings with a high validity. Thirdly, RMTs could provide ease of use and relieve burden for healthcare professionals.
Nevertheless, during engagement with clinicians several doubts and issues were also raised, which could provide limits to the role of RMT. One limitation pertained to concerns by doctors regarding loss of their autonomy due to delegation of clinical action to these devices. Care ‘should not be replaced by an RMT-enabled approach’ (Stakeholder Report 2). Members of the research team were of the same opinion. An interviewee (Interview 13, clinical psychology and behavioural science) stressed the importance of ‘having a dialogue and using [RMT data] as a source of information but not fully relying on it’, but to then ‘always talk it through with the patient.. to ask for more information’. Another interviewee added (Interview 6, clinical psychologist) ‘we need to understand that these are complementary technologies to our healthcare system…It's the responsibility of governments, of health services of the community to support the health of every individual’ otherwise we put the blame on patients to do something about their health.
An interviewee who was a patient representative for patients with depression (Interview 24) added:
Mental health is quite complex … it's not just physical causes, there are lots of different reasons .. which cause people to relapse. [unemployed, loss] This system, whilst it does look at quite a lot of these, obviously cannot capture .. everything like that. So that's why ..it's important to continue to have that conversation between the clinician and the patient. And that's why we can't replace it. But this definitely.. can complement it.
Patients
The project had a patient board that consisted of representatives of different patient organisations consulted throughout the project on research matters pertaining to patients. Patients hereby obtained a voice early in the development of these RMTs and actively participated in design. For example, epilepsy patients said they do not want a wearable device that gives away their condition and found visualisations very useful. Generally, patient representatives saw in RMTs a way to transform prevention and improve care of chronic disease. ‘As a patient you need to figure out when relapse is coming-before it happens … you could, after a relapse, sit down with your doctor and look at the dates … [There] the wearable devices .. says, okay we can see that when you are starting to feel low in your mood, actually .., your sleep was a bit disturbed, you stop .. walking as much, the activity level gone down’. (Interview 24, Depression Patient Representative)
Yet, there are indications of a series of challenges for patients regarding the use of these technologies. Some of these are personal issues. Making patients more health conscious can also have downsides, such as causing health anxiety, stigmatisation and disengagement (Sideri and Van Dijk, 2024). Data security and privacy are also often-heard concerns, which link to trust. The project entrepreneurs conducted surveys with patients, from which various questions emerged as to who has access to confidential data and what happens if, for example, a wearable digital device is lost.
There was also a different set of issues. As an interviewee (Interview 5, software developer for privacy friendly medical apps) explained, digital tools exclude people who are old, poor or marginalised. ‘It just excludes all the people that you need’. Another interviewee (Interview 4, psychiatrist) explained that psychiatric drugs do not work very well and this negatively affects the relationship between patients and clinicians: ‘There[are] reasons why people feel that way and very justifiable cause we give drugs
Healthcare managers
Mental healthcare managers were also consulted as a category of stakeholders. They saw clear benefits in the use of RMTs, since they could address the more financial and managerial aspects of mental healthcare clinics. A major problem for these managers is the issue of (lack of) funding and they were concerned with cutting costs wherever reasonably possible. In many countries, it's [the] split between the health care system and the social care system.. If [we] throw people out of the hospital before they're ready, it gets picked up by the social care system .. you overburden ..[the] health system. … [as] They will also pick up the cost when that person is readmitted …. (Interview 5, software developer for privacy friendly medical apps).
Whereas the remote digital devices are supposed to help cut the cost of healthcare systems there are also several factors that might actually increase overall costs (Stakeholder report 2). RMTs would require significant staff with clinical, technical, and administrative qualifications (such as data managers). They also require extra costs for training staff and patients in working with these devices and building new professional routines. Another point is the cost of the underlying technical infrastructure that needs to be put in place to enable the use of these technologies. These pose significant extra costs that must be weighed against the benefits, whereas some of these benefits might only accrue very slowly over time. Furthermore, some benefits of clinical usage are premised on achieving interoperability between the RMTs and other systems (e.g. the electronic patient file). If such integration does not materialise, clinicians will have to use these systems on top of all the others already used and it might become a burden rather than a relief. Lastly, there is the expectation that clinicians would have to spend more time on reviewing the data of patients and thus being able to see less patients All in all: ‘the question whether it gets into healthcare systems, [.. which] will depend on whether it's actually getting … something useful clinically. … So in the future, you will have to think in the design how many messages, how many red flags, how much more work you are creating for the healthcare system (interview 4, psychiatrist). These cost issues are important potential obstacles. Healthcare managers will need overcome them to make the introduction of these RMTs in the clinic a reality.
Extensions of the pharmakon
The concept of pharmakon (φάρμακον), with its ancient Greek roots, denotes an ambivalence: it can both heal and poison. The problem of control of a potential toxic substance was addressed in early 20th century by state regulation that required drugs to pass tests of safety and efficacy before they were marketed. The rise of the modern pharmaceutical industry is closely tied to these processes (Gabriel, 2019). Today, plagued by the problem of costs and scandals (Geiger and Bourgeron, 2025), the industry is looking for novel ways to address this problem of controlling toxic substances. One avenue is by exploring the opportunities of digital technologies, through early-stage collaborations with research institutions and universities. Indeed, pharmaceutical companies participated in the project from the start. They jointly led with universities and other research partners. ‘Our involvement [is about] trying to understand our patients and their interaction with digital tools’. ….’ We have to be more patient centric and less molecular centric. Not just test a molecule and market it. Everything is going to be about value for the patient’. (Interview 11, Computer scientist/biologist for a pharmaceutical company).
Indeed, stakeholder report 2 says that value is created by continuously collecting real world evidence through software attached to a drug, so that pharmaceutical companies can convince regulators regarding the value impact of their drugs. The project entrepreneurs here also show more possible extensions of pharmaceutical products through RMTs and indicate where they can offer value beyond the generic prescription of drugs during therapy. First, pharmaceutical companies could move to the follow-up of therapeutical visits, by monitoring patient adherence to drugs and by obtaining evidence of their effectiveness (especially if tied to specific populations). Moreover, pharmaceutical companies could also expand into areas of diagnosis. Here they could improve decisions about early detection and patient's individual disposition to specific drug treatments. The creation by the project of a ‘reliable and trusted infrastructure to measure outcomes’ and the inclusion of AI and analytics would improve such early ‘detection, diagnosis, decision-making, treatment and research’ (Stakeholder report, Nr. 2).
This is all very ambitious. Our interviewees help us better understand some of pharma's specific interests. In the context of Parkinson’s disease they said: We need a better understanding of the progression of aging, so that we engage in preventive treatments and not symptomatic treatment. There is investigation onto early signs and symptoms of Parkinsons … ….to understand the disease even before it is diagnosed. We need drug targets not only for symptomatic but also for stopping the progression… And then, pharma researchers can target disease earlier—and you can see how medical devices and pharma companies.. [it] can be a happy marriage. (Interview 9, chemical engineer/pharmaco-geneticist for a pharmaceutical company).
Altogether, there are thus several interests of the pharmaceutical industry in RMTs: discovery of new drug targets, repurposing old drugs for new indications, measuring effectiveness of their drugs to satisfy regulatory thresholds. Stakeholder report 2 concludes that digital technologies are reshaping the pharmaceutical industry itself as ‘digital services beyond the drug itself’. As another of our interviewees explained (Interview 9): ‘Drugs and software, this has become a reality, we have connected products for personalized treatment. A complementary device that tracks your health, how the drug is treating you. Software can and is working with drugs’. The traditional product of the pharmaceutical industry – the pharmakon – can thus no longer be limited to drugs. It has to be extended and become a kind of drug + (software & services) and pharma itself also has to be transformed as an entity in the process.
Discussion: RMTs and clinical worldmaking
Pre-emption and the politics of health
In his writings on the genesis of the institution of the hospital in the 18th century, Foucault (2014: 118) says that the politics of health was organised around the idea that good health is a state to be restored to normal functioning and this requires putting in place a system for ‘the perpetual observation, measuring, and improvement of a “state of health” of the population’. This wider definition of health and medicine made prevention a central political objective. The hospital was a central component in this system from the start. Since the 18th century, a system of observations and recordkeeping was kept on the progression of disease and success or failure of treatments over long periods of time. This longitudinal approach made data aggregation possible for the whole population and the hospital thus functioned as a (therapeutic) ‘instrument’ for collecting data to advance medical knowledge. Such information fed into decisions about how long to hospitalise a patient, transfer them to other departments or to home care and back to hospital if necessary (Foucault, 2014, Foucault, 1994) and remain of central importance today.
Public health policies are currently reimagining the function of public health systems in the light of a new explicit set of problematised challenges of an aging population with chronic disease, skyrocketing health expenses and costly treatments. Digital devices such as remote monitoring technologies and big data analytics have increasingly become positioned as a crucial promising mediating node in bringing about this transformation. We have seen how regulators and funders think they can provide continuous real-time clinically relevant information about everyday behavior of individuals. For them, this would allow more detailed preventive action no longer merely based on the perpetual observation and measurement of the state of health of the population through general statistics, as in Foucault's quote, but that of the individual patient through concrete digital techniques of personalisation. They envision a future where such digital devices would further advance insights into the clinical picture of certain diseases such as depression and epilepsy, and they will be used for clinical decision-making (when to administer drugs, when to start treatment, when to hospitalise a patient).
Funding calls in the EU advance innovation alongside this direction. The IHI's funding call under which the project we studied was funded, proposed a move from ‘diagnose and treat’ towards ‘prevent and pre-empt’-ing diseases. This idea required the generation of information and the reorganisation of internal routines via big data analytics. The imperative to cut costs inscribed in the research agendas and funding call also loomed large over the project evidenced in the statement that any future decision ‘will be informed to a large extent by its cost effectiveness (Stakeholder Report 3). Moreover, the affordances of big data analytics would enable precise measurements to make such assessments about costs. Funders also envisaged extending the clinical space to include the patient's home as patients are expected to self-manage symptoms and enable continuous flows of data from their bodies to the clinic (which we can call the clinic without walls). This last point needs to be stressed: without this patient centric element, the whole scheme cannot work, as it is entirely based on continuous data collection. Importantly, pharmaceutical companies (involved in IHI) also see opportunities in an ever-changing environment by higher thresholds imposed by regulators.
To further understand funders’ strategic interests, we need to zoom in on pharmaceutical companies’ interests in ‘disease preemption’ and interception (see Narchi and Winkler, 2021, Wagers, 2023). 3 Pharma supports RMTs as they provide data for measuring the effects and effectiveness of their drugs. Secondly and more related to the notion of pre-emption is the opportunity pharma sees in digital devices for identifying more ‘drug targets’ upstream in the clinical pathway trajectory of illness. Thus, as concluded in the final stakeholder report (Nr. 3) of the project, ‘harnessing digital technology, pharmaceutical companies can not only limit the threat represented by value-based healthcare but can also turn it into an opportunity’. This new high-tech approach fits their old pattern of creating markets for medicines by expanding disease categories (Dumit, 2020).
Pharma as an entity seems to become something else in this process, no longer merely focused on the production of drugs (pharmakon). In the project they are subsequently designated as ‘life science companies’ that occupy themselves, in the words of our interviewee (Interview 9, chemical engineer/pharmaco-geneticist for a pharmaceutical company) ‘with the life-cycle management of the whole journey of mental illness’. Their business is not only about inventing new drugs to target disease earlier but also about adjusting dosage and repurposing old drugs (for new indications). Continuous data collection is key in the process. This indeed implies a transformation of pharmaceutical industry as a potential ally via RMTs, which becomes an entity focused on continuously following the patient, watching over life, or engaging in bio-epaγrípnisi, 4 so that disease or episodes of disease are pre-empted before there is clinical manifestation.
Yet, the tool can imply different things for different actors and various issues remain unresolved, including the degree of automation, the remediation of the relationship between patients and physicians, and the question of patient participation. To put it differently, for funders RMTs are valuable because data can be used to fuel innovation and data collection, measure quality, encourage efficiency, ensure safety, and standardise clinical care
Which transformations of the clinic?
The scientific project entrepreneurs whose project received funding from the call, never used the term pre-emption or embraced the linguistic move from diagnose and treat to intercept and pre-empt. Their own descriptions of the project and its objectives rather breath a mixed air of scientific and technology innovation excitement in building new technological devices and a clinical emphasis on improving the quality of care for patients. These positions indeed partially align with the pre-emptive frame, but they do not coincide. Funding frames always leave a certain room for manoeuvring the research along lines of scientific interest and entrepreneurship. This becomes especially clear in the work of interessement and clinical world-making, where the project entrepreneurs simulated and explored the transformations of the clinic and clinical action due to the introduction of RMTs. Hereafter we will discuss three transformations: delegation of clinical action to technological devices, redistribution of clinical roles between patients and clinicians, and action-at-a-distance by clinicians. The project entrepreneurs solicited the views of clinicians, patients, healthcare managers and pharma companies regarding the ‘value’ their devices could bring, and thereby tried to make them the ‘obligatory passage point’ for innovation in healthcare. Nevertheless, throughout the consultations with several actors, certain limits of these proposals also became gradually apparent, and other possible avenues were opened. In this way, these exercises also offer glimpses of other ways of ‘world-making,’ where every ‘world’ presupposes specific options (Callon et al., 2011). These counterproposals go hand in hand with diverse understandings of what healthcare is or should be about, what therapy is, and they would require a different organisation of the clinic and the patient-doctor relationship.
Doubts were raised about whether RMTs will organise care routines more efficiently. Our interviewees stressed that the question of how many red flags a patient should receive so that they do not give up using the tool is not settled (Interview 4, psychiatrist) But there are more issues not settled yet, such as who is brought to the clinic and who is left to self-manage their symptoms and the degree to which automation is desirable. The project entrepreneurs designated with the colours green and red, the points in clinical pathways where RMTs can be inserted or not. RMTs are not to be used for making an initial diagnosis (colour red), a patient seeking help for the first time will need to talk to a doctor. But there is also the colour yellow for RMTs that could potentially inform decisions about continuing or stopping treatment with drugs for epilepsy. Patient self-monitoring (as a proactive strategy) may here be important even for decisions that concern changing medication regimes so that seizures are reduced or remitted. Although the report mentions that clinical examination should also be conducted, elsewhere in the report we see references to the inability of cash-strapped systems in developing countries to cope with supervision of medication intake. The question is whether colour yellow will become de facto green in times of crisis or in cases of cash strapped healthcare systems, even in the developed world? In other words, will RMTs become a cheaper substitute for clinicians if no human resources are available? These issues are widely discussed in the medical literature, where some argue the problem lies in today's push for efficiency and productivity (Sparrow and Hatherly, 2020). Although doctors consider AI as the means to spend more time with their patients, big data analytics may in fact have the opposite effect, as savings made possible by a reduction in the administrative burdens on physicians will be used to move more patients through the system. The result might be to spend even less time talking to and caring for patients.
With this notion of substitutes for clinicians we also get to the different ways in which RMTs would remediate or transform clinical action, due to redistributions of ‘actorial roles’ among doctors, patients, and these technological devices. In their stakeholder consultations (Stakeholder Reports 1 and 2) the project entrepreneurs found that clinicians pointed to several limits of the technological delegation of clinical action (Latour, 1999) to these digital systems. This can be summarised in the statement that care by doctors ‘should not be replaced by an RMT-enabled approach’. An example is the case of adjusting dosage regimes: clinicians indicated they would want to first see the patient and talk to them. For them big data analytics involves bringing people to the clinic at the right time. Although for pharmaceutical companies or regulators automation of dosage adjustment could be desirable if RMTs are precise and accurate in their measurements, for physicians this would not be enough. To understand their reasons, we need to understand the nature of therapy and the work that goes into diagnosis and choices among treatments, and especially empathy and skills in communication (Lantos, 2024). As Sparrow and Hatherly (2020) state ‘Sometimes physicians gather information by examining or asking questions of the patient, and this process is an opportunity for the conversation to roam more widely and is thus also an opportunity for “care.”’
In some of these statements we can observe the seeds of a counterproposal for different clinical world-making. RMTs are also inscribed here, but in a way that implies a different configuration of the actors in the clinical ecology. RMTs could play a significant role in clinical action since they can help to signal early on when patients get worse. Yet, this signal would constitute a new and early activation point for engaging with the doctor. RMTs would thus not ‘replace’ the therapeutic relation between doctors and patients, but rather function as a ‘complement’ (Sideri and van Dijk, 2024). These devices would thus need to be resituated into existing clinical practices, where they would be assigned a more limited role, rather than radically transform them. The difference between the two ways of clinical world-making enabled by RMTs is best expressed by contrasting the position of the clinicians with the innovation formula of pharmaceutical interception. Pharma wants to effect a ‘move away from diagnose and treat, towards predict (through RMTs) and pre-empt’ through new medicines. Clinicians would want to however use RMTs to predict and then move towards treatment through consulting with their patients, rather than away from it.
On this second view, RMTs would be enrolled in a different composition of clinical action. We could call this a kind of technologically mediated action-at-a-distance by the clinicians. The etymology of the term ‘clinicians’ harbours the meaning of the old Greek klinike referring to the physicians visiting patients at home in their beds. Eventually due to the rise of professional clinical institutions these practices were gradually substituted with visits by the patients to the clinic. Interestingly, here we see a proposal for reinstating a limited form of clinical visitation at the patient's bedside. The RMTs are supposed to allow the doctor to engage in clinical action at a distance, by monitoring, predicting, and intervening in the patient's condition when at home.
A last technologically mediated redistribution of clinical action is to the patient who is expected to self-manage important aspects of their condition. An important proposal of the project consists in an exchange of passive and active properties between patient and clinician. RMTs are supposed to empower patients to take a ‘leading role’ in managing their own condition. They would simultaneously ‘change the role of the clinician’ who hereby more becomes a ‘passive recipient of the data’ and has to collaborate with the patient in their interpretation (Stakeholder Report 2). These statements echo Latour's (1999) remarks about how technologies can lead to changes in actorial roles.
Interestingly, the patients consulted were more ambivalent about automation. Representatives of patient organisations did see in these tools opportunities for self-monitoring, since they do not get to see their physicians as often as they would like to. The use of RMTs outside the hospital could however also increasingly burden individuals with controlling their own bodies (Ma et al., 2023), in the context of a governance framework that shifts responsibility for health from collective systems to individual patients (Prainsack, 2017) under the banner of empowerment. This is also likely to most affect vulnerable groups (McCradden et al., 2023).
The affordances of RMTs and big data analytics make possible not only continuous monitoring but also connected homes and virtual care teams (Pita-Barros et al., 2019). The clinic is extended and becomes decentralised, as networks inhabited by private spaces link to it. This proposed transformation implies fundamental changes in the way health systems are organised and financed, the role of clinicians and patients, the way in which health services are provided and the degree of automation (Pita-Barros et al., 2019). Clinicians might be justified in worries about their future role in this system.
These remarks point to limits when RMTs go out in the real world of healthcare systems, rather than in the simulated research collective that the funding call put together (Callon et al., 2011). Here, the patient population at large enters the scene, and the question is whether the digital transformation of the clinic will still be successful: will they accept the project entrepreneurs’ propositions, or will they resist and reject them? This is crucial to consider since the scheme will not work without collaborative patient populations. One important issue here concerns representativity: to what extent are the patients participating in the project representative of the general population of CNS patients? Members of patient organisations have unique characteristics such as intellectual curiosity and novelty (Callon et al., 2011). They are eager to participate in research projects such as the one we followed. Yet, most patients are not members of patient organisations. For some, the reasons lurk in the shadowy corners of stigma, fear, and disempowerment. People do not want others to know that they or their families have a disease. They do not even want their names in a list of members of a patient organisation. Data driven technologies could in fact further aggregate these already existing concerns (Sideri and Van Dijk, 2024).
Conclusions
Callon et al., (2011, 68) ask ‘How else, other than as politics, could we describe the …exploration of possible worlds, and the choice between them?’ What is at stake here are our common ways of living, and the reorganisation of health services is certainly a core aspect of it. Will the public healthcare system be reorganised without losing its solidaristic character? What is expected from patients who refuse to act on data and take control of their conditions? Is care going to lose its empathetic character? Will this drive to develop more technical tools deepen existing inequalities?
The scheme proposed by the research alliance is fragile. Various questions loom large: will such digital technologies be able to reduce overall costs of healthcare systems, provide reliable evidence of clinical effects, pass stringent quality and safety tests for medical devices (as opposed to consumer devices), and technically work sufficiently accurately?
There are also limits inherent in the efforts to discipline the new kind of patient into the kinds of behavior that would be required for the overall system to work well. At the core there is a reorganisation of the patient-doctor relation. Although we have seen a refusal on the part of the doctors for their clinical actions to become overly delegated to this digital systems, the techno solutionism push and the drive to establish standardised outcomes to measure effectiveness point to a system biased towards technology adoption (even if outcome benefit are modest), rather than investing in social care or patient support by allowing doctors to spend more time with their patients.
The direction of advancement of the field is at present still open-ended as well as the specific configurations of humans and technology needed for clinical action. By laying bare the different ways of clinical world-making all condensed in these small RMT monads, we have tried to unearth the kinds of political choices between worlds that can and have to be made in society and to open them up for broader discussion.
Footnotes
Ethical approval and informed consent statements
Qualitative Research (interviews) has been approved by the ethics committee of Panteion University, Athens Greece. The informed consent document we used has also been reviewed and approved.
Author contributions
The authors contributed in equal degree to the present publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HFRI - Hellenic Foundation for Research & Innovation Grant Number 14781 ‘Smart Pharma: Re-imagining therapy and the softwarization of drugs (2023-5).
European Commission Marie Sklodowska-Curie Individual Fellowship, grant number 794604-Biased AI-H2020-MSCA-IF-2017 (2018–2020).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Interview transcripts are not available due to confidentiality.
Any other identifying information related to the authors and/or their institutions,funders,approval committees,etc,that might compromise anonymity
None.