
Abstract
Objective
The Women's Health Initiative (WHI), a randomized controlled trial, found no overall health benefit of menopausal hormone therapy. Our objective was to evaluate the hypothesis that initiating hormonal therapy prior to age 60 or within a few years after the last menstrual period provides health benefits in menopausal women.
Design
A search was conducted in MEDLINE, Scopus, and ClinicalTrials.gov from inception until August 26, 2025. Randomized controlled trials in which at least one arm was a pharmaceutical oestrogen and one arm was a placebo were included. We required studies to present clinical health outcomes.
Setting
Systematic review
Participants
Menopausal women age 60 or younger or within a short time of the last menstrual period, as defined by individual study authors.
Main outcome measures
Studies were categorized based on primary endpoints, namely cardiovascular disease, cancer, depression, and cognition. Risk of bias was assessed using a standard tool. The reliability of conclusions was assessed using the core GRADE method.
Results
Thirty-one papers, reporting on seventeen randomized controlled trials, met eligibility criteria. Menopausal hormone therapy in young menopausal women was not shown to have beneficial effects on cardiovascular disease, cancer, depression, or cognition with the exception of some cardiovascular endpoints in women on oestrogen alone in the WHI, a finding not confirmed in other randomized controlled trials and not confirmed in women with vasomotor symptoms.
Conclusions
Menopausal hormone therapy in young menopausal women has not been shown in randomized controlled trials to have beneficial effects on cardiovascular disease, cancer, depression, or cognition.
Keywords
Introduction
Proponents of hormone therapy argue that while the therapy may be harmful for women distant from menopause, hormones will have long-term health benefits in younger women closer to the time of menopause. This critical period or timing hypothesis1,2 posits that beneficial health effects of menopausal hormone therapy require the initiation of therapy soon after the last menstrual period, for example, within 10 years.3,4 Our objective was to identify published randomised controlled trials (RCTs) that evaluated disease outcomes associated with menopausal hormone therapy in younger women closer to their last menstrual period.
Methods
The search strategy is described in Supplementary Appendix S1. Study quality was evaluated using the Cochrane Collaboration Risk of Bias system, 5 which assigns high, low or unknown risk of bias to six aspects of study design. Risk of Bias was assessed independently by two authors (PAB, ARS), and agreement was reached by consensus. No studies were excluded based on the Risk of Bias assessment, but a separate evaluation was conducted excluding papers with a high Risk of Bias. Papers were evaluated independently by two investigators.
After restricting papers to placebo-controlled RCTs on estrogen that included clinical endpoints in spontaneously menopausal women under the age of 60, we tabulated study interventions and results for four clinical endpoints: cardiovascular disease, cancer, depression and cognition. These endpoints were selected by the original study authors and were not selected by us as a basis for inclusion in the review. All studies excluded women with these disorders at baseline. Surrogate endpoints, including blood pressure and lipid concentrations, were not included. Synthesis of the results was based on consistency of findings among studies and comparisons to the Women's Health Initiative (WHI), the largest of the trials analysed. For all WHI analyses, we analysed the subgroups of women with a uterus randomised at age 50–59 and given daily conjugated equine estrogen (CEE) 0.625 + medroxyprogesterone acetate (MPA) 2.5 mg or placebo and hysterectomised women randomised at age 50–59 years to CEE only or placebo. A separate analysis included studies using 17β-estradiol. Data were presented as in the original papers without further manipulation or adjustment for missing data. The reliability of conclusions was assessed using the core GRADE method, which considers imprecision, inconsistency, risk of bias and indirectness.6–12 Ethics review and consent were not required for this study.
Results
Article searches retrieved 5388 items. Based on titles, abstracts for 2013 citations were reviewed, which yielded 621 papers for full-text review. The article review resulted in 592 papers being excluded and 29 papers being retained. ClinicalTrials.gov yielded 241 items. After review, 11 items were retained, four of which were duplicates and seven of which were retrieved and read. Two papers were retained. The search and review process is summarised in Figure 1. Papers excluded after full-text review are listed in Table S1. Risk of Bias for included studies is shown in Figure 2.
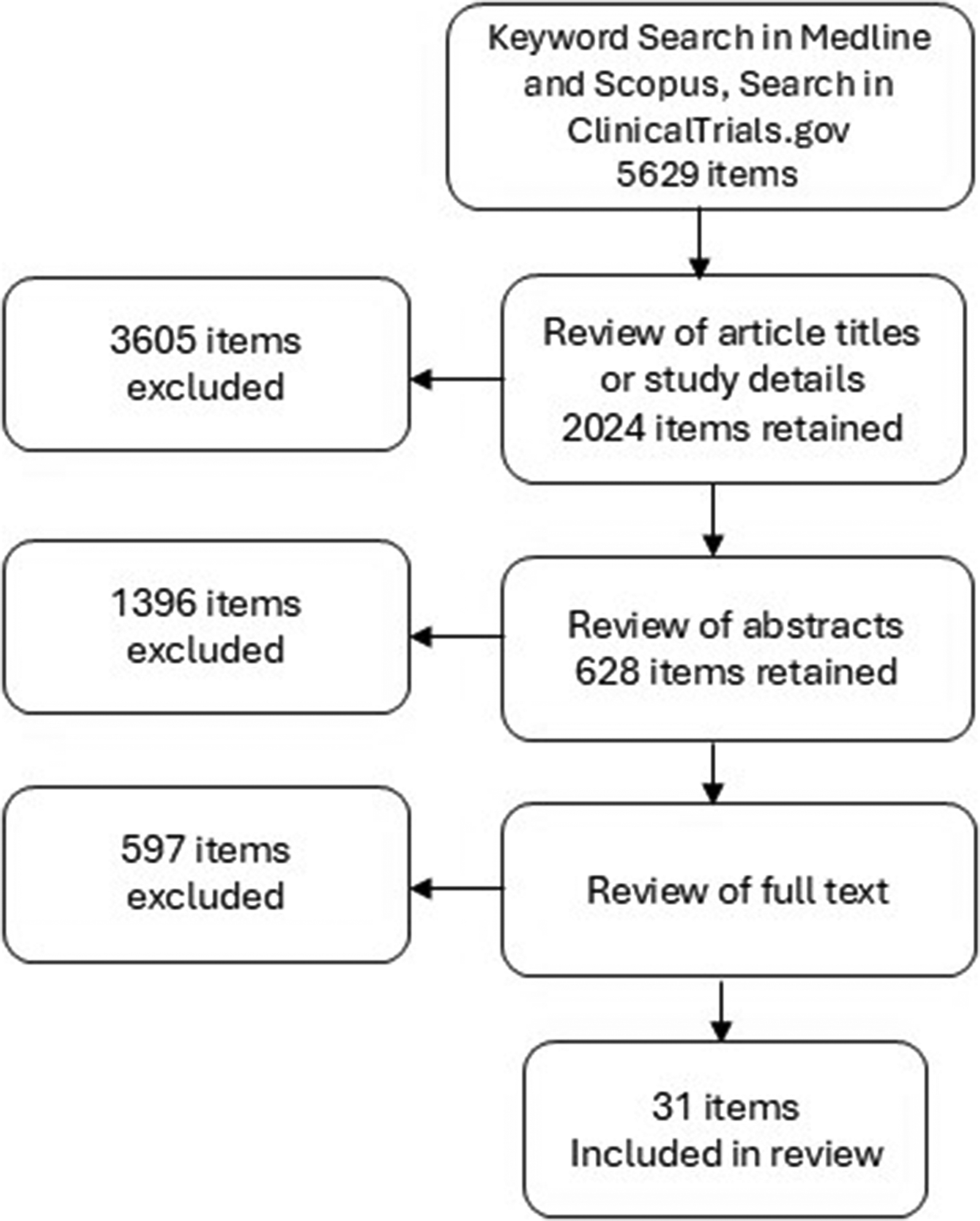
Results of the search and review of randomised controlled trials.
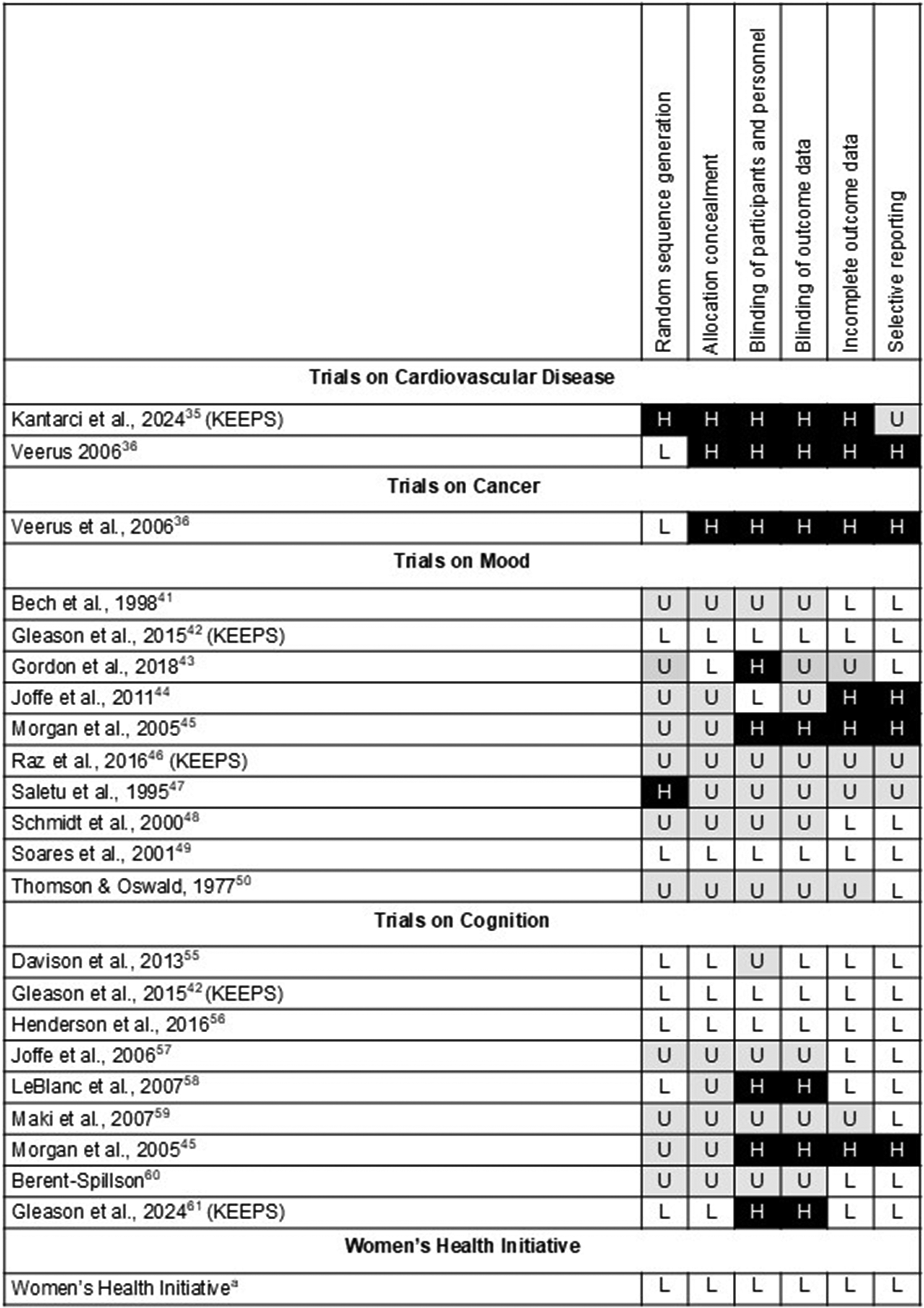
Risk of bias evaluations.
Cardiovascular disease
Women's Health Initiative
Initiated in the early 1990s, the trial of CEE + MPA was halted in 2002 due to increased risks of breast cancer, heart disease, stroke and venous thrombosis (Table 1).13,14 Two years later, the estrogen-alone trial was stopped early due to an unfavourable risk-benefit profile, primarily affected by stroke risk. 14
Randomized clinical trials evaluating cardiovascular disease
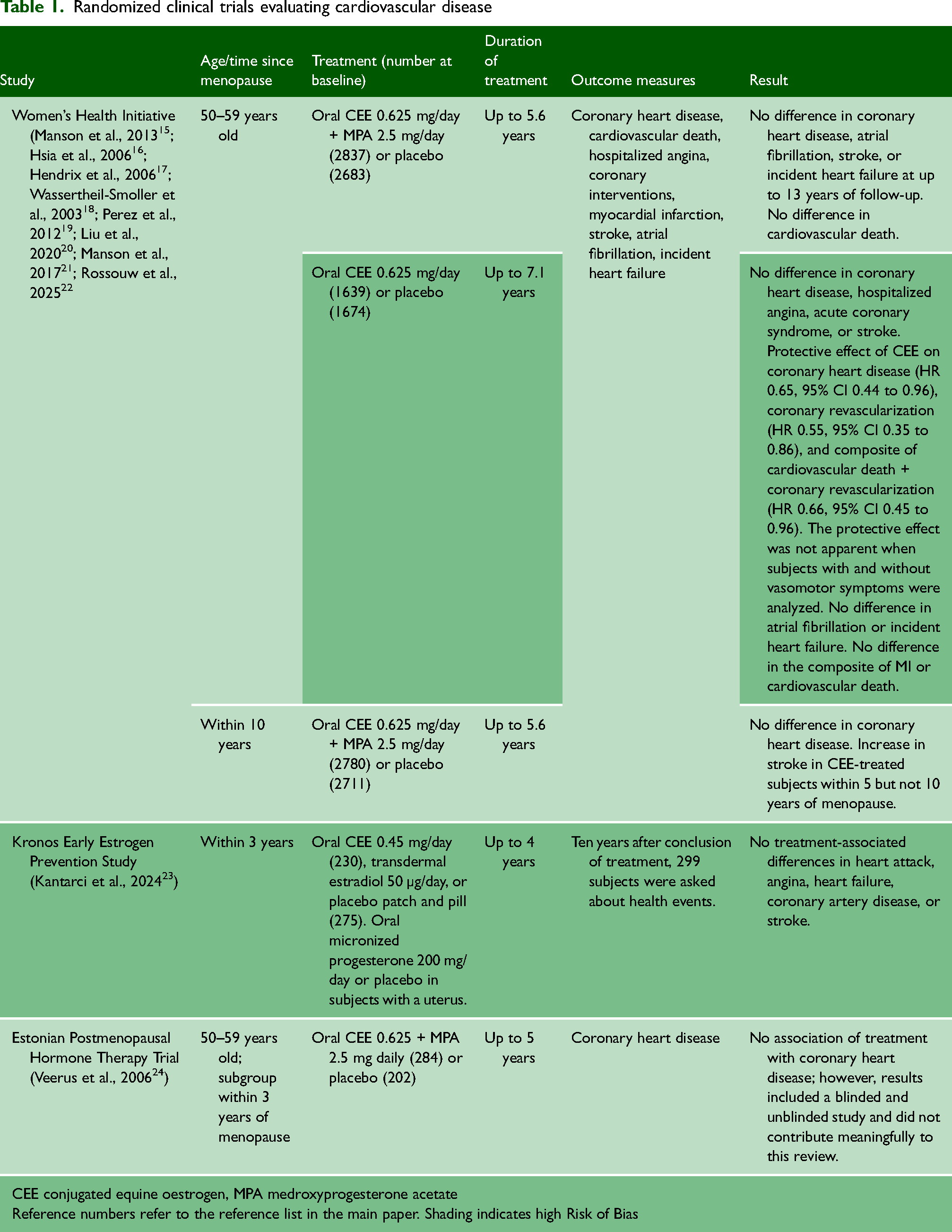
CEE conjugated equine oestrogen, MPA medroxyprogesterone acetate
Reference numbers refer to the reference list in the main paper. Shading indicates high Risk of Bias
With up to 13 years of follow-up, there was no significant effect of MPA + CEE on coronary heart disease or cardiovascular death in either the general WHI study population or younger women. Coronary heart disease was diagnosed in 38 subjects who received CEE + MPA, and 27 who received placebo (hazard ratio [HR] 1.34, 95% confidence interval [CI] 0.82 to 2.19). 15 In subjects randomised within 10 years of menopause, the HR was 0.90, 95% CI 0.56 to 1.45. 15
CEE alone had a protective effect on some cardiovascular outcomes, but increased stroke. Among the 1639 women taking CEE alone, a diagnosis of coronary heart disease, hospitalised angina, or acute coronary syndrome occurred in similar proportions among those given hormones or a placebo. 16 However, a protective effect was seen for CEE alone on coronary heart disease (HR 0.65, 95% CI 0.44 to 0.96), on coronary artery revascularisation (HR 0.55, 95% CI 0.35 to 0.86), and on the composite outcome of myocardial infarction, coronary heart disease, coronary revascularisation, and cardiovascular death (HR 0.66, 95% CI 0.45 to 0.96).
In subjects in the CEE-only arm, after an average follow-up of 7.1 years, there was no difference from placebo in stroke in women aged 50–59 at enrolment. However, stroke risk was increased in women randomised within 10 years of menopause, HR 2.62, 95% CI 1.01 to 6.81. 17 With up to 13 years of follow-up, there was no significant effect of either CEE + MPA or CEE alone on stroke. 15 There was no difference by hormone treatment in the occurrence of stroke among women enrolled at ages 50–59 and in women enrolled within five years of menopause.17,18
Neither CEE + MPA nor CEE alone affected the incidence of atrial fibrillation, 19 heart failure, or mortality from cardiovascular disease in women randomised at age 50–59.20,21 An evaluation of women with or without vasomotor symptoms randomised at age 50–59 or within 10 years of menopause found no effect of CEE + MPA or CEE alone on atherosclerotic cardiovascular disease (a composite of nonfatal myocardial infarction, hospitalisation for angina, coronary revascularisation, ischaemic stroke, peripheral arterial disease, carotid artery disease, and cardiovascular death). 22 There was no effect on total cardiovascular disease, all-cause death, coronary heart disease, stroke, or venous thromboembolism.
Other trials
The Kronos Early Estrogen Prevention Study (KEEPS) specifically enrolled younger women to test the effect of hormones on cardiovascular events, stroke and surrogate markers of atherosclerosis. KEEPS randomised menopausal women within three years of the last menses to oral CEE 0.45 mg/day (n = 230), transdermal estradiol 50 µg/day (n = 222), or placebo patch and pill (n = 275). Subjects with a uterus were given oral micronised progesterone 200 mg/day or placebo for 12 days/month. Treatment was continued for up to four years.
Ten years after the conclusion of the treatment period, 299 subjects, representing 41–43% of subjects assigned to each treatment arm, participated in a follow-up study in which they were asked about health events that had occurred after the original study ended. 23 This limited follow-up, representing less than half of the original cohort, identified no treatment-associated differences in heart attack or angina, congestive heart failure, coronary artery disease, or stroke. Although a sensitivity analysis of the 243 subjects who had not used menopausal hormone therapy after the end of the KEEPS study was described as showing no associations, the supplemental table showed only laboratory results and not diagnoses. At follow-up, subjects appear to have known their treatment assignment, giving rise to a high risk of bias.
The Estonian Postmenopausal Hormone Therapy trial recruited women between 50 and 64 years of age, although some results were given for women 65–70 years of age. 24 Among 251 subjects recruited within three years of menopause, there was no association between therapy with CEE + MPA and coronary heart disease. The analysis combined data from women recruited to a blinded and an unblinded study of these hormones. This trial had been entered in a clinical trials registry (https://www.isrctn.com/ISRCTN35338757), but raw data had not been entered by 20 February 2026. Although mentioned here for completeness, we excluded this study from our analysis because we cannot separate the data from the blinded and the unblinded portions of the trial.
In summary, the WHI findings suggest a protective effect of CEE alone, but not CEE + MPA, against coronary artery disease in young menopausal women who had undergone hysterectomy. Two smaller randomised clinical trials and an analysis of the WHI CEE arm did not confirm a protective effect of menopausal hormone therapy on cardiovascular disease outcomes.
Excluding studies with a high risk of bias left only the WHI. None of the studies used 17β-estradiol. Our GRADE conclusion is that CEE alone in young menopausal women who have had a hysterectomy may decrease heart disease and total death. Our confidence in this conclusion is low due to inconsistency in the evaluation of WHI data, lack of confirmation in other studies, and the possibility that the apparent decrease in the first WHI analysis was due to estrogen mitigation of adverse cardiovascular effects of oophorectomy.
Cancer
Women's Health Initiative
In the WHI, there was no difference in invasive breast cancer among women ages 50–59 at two years, but there was a significant increase at 20-year follow-up (Table 2). At two years, invasive breast cancer was diagnosed in 52 of 2837 women randomised to CEE + MPA and 40 of 2683 women randomised to placebo (HR 1.20, 95% CI 0.80 to 1.82). At 20 years, 203 women in the CEE + MPA group had invasive breast cancer diagnoses, significantly higher than the 143 women in the placebo group (HR 1.36, 95% CI 1.09 to 1.69). 25 Invasive breast cancers associated with CEE + MPA compared to placebo were more frequent, more likely to be lymph-node positive, and more likely to be advanced compared to cancers in women on placebo across all age groups. However, these results were not shown by age at randomisation. 26 There was no difference in breast cancer mortality by treatment group.
Randomized clinical trials evaluating cancer
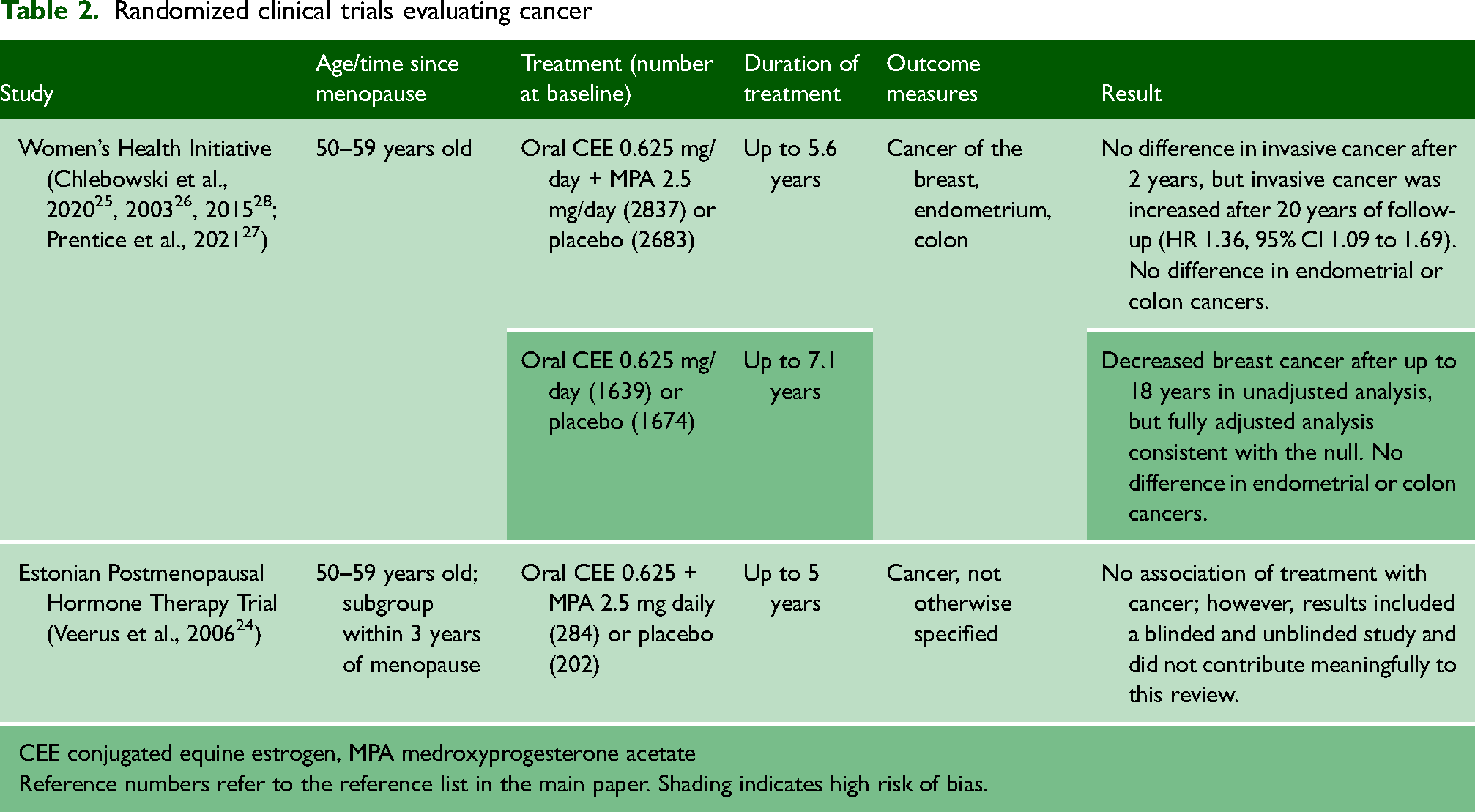
CEE conjugated equine estrogen, MPA medroxyprogesterone acetate
Reference numbers refer to the reference list in the main paper. Shading indicates high risk of bias.
Estrogen alone appeared to be protective against breast cancer in initial reports, but this effect disappeared in adjusted analyses. Women randomised at ages 50–59 to estrogen alone (n = 1629) had decreased invasive breast cancer diagnoses compared to placebo (n = 1674) in unadjusted analysis with up to 18 years of follow-up. However, the difference was no longer significant in the fully adjusted analysis. 27 The authors suggested that women with a longer time between oophorectomy and estrogen therapy had protection from invasive breast cancer.
Women with a uterus who are prescribed estrogen receive a progestogen to mitigate the risk of estrogen-induced endometrial cancer. There was no significant difference in endometrial cancer among women randomised to hormones or placebo at age 50–54 after a median cumulative follow-up of 13 years; seven women developed endometrial cancer in the CEE + MPA group compared to 11 women in the placebo group (HR 0.57, 95% CI 0.22 to 1.48). 28
After up to 18 years of follow-up, there was no difference in colorectal cancer risk among women taking CEE, CEE + MPA, or placebo at age 50–59 in the fully adjusted analysis. 27
Other trials
In the Estonian Postmenopausal Hormone Therapy Trial, risk of cancer, not otherwise specified, was similar among 251 women randomised to hormones or placebo within three years of menopause during the blinded portion of the trial (HR 3.26, 95% CI 0.35 to 9.95). 24 This study had a high Risk of Bias. There were no trials of 17β-estradiol.
In summary, CEE + MPA, but not CEE alone, increased breast cancer at 20-year follow-up. CEE-alone did not increase or decrease breast cancer risk. We had moderate certainty in the conclusion that CEE + MPA increases breast cancer at 20-year follow-up due to a lack of confirmation by another trial. In women under 60 years of age at randomisation, CEE with or without MPA had no effect on the risk of endometrial or colorectal cancer.
Depression and mood
The WHI RCTs on hormone therapy did not measure depression or mood (Table 3). Nine smaller RCTs with a combined total of 1280 women between the ages of 40–60 evaluated mood using oral CEE, oral 17β-estradiol, or transdermal 17β-estradiol, with different scales or inventories assessing depression and other mood states.29–38 Some women met criteria for major depressive disorder at baseline, and some did not. Four of the nine trials had a high Risk of Bias.31–33,35
Randomized clinical trials evaluating depression
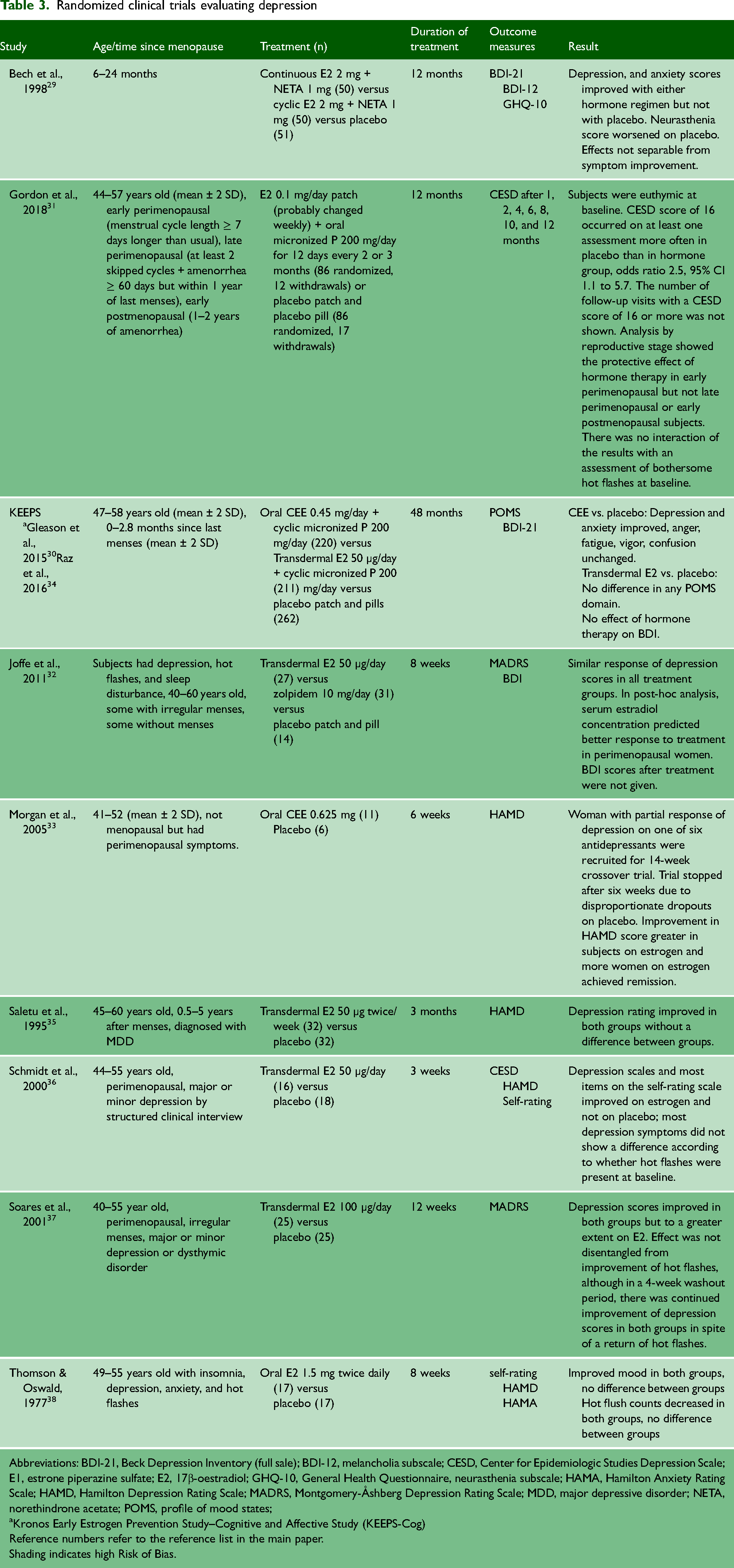
Abbreviations: BDI-21, Beck Depression Inventory (full sale); BDI-12, melancholia subscale; CESD, Center for Epidemiologic Studies Depression Scale; E1, estrone piperazine sulfate; E2, 17β-oestradiol; GHQ-10, General Health Questionnaire, neurasthenia subscale; HAMA, Hamilton Anxiety Rating Scale; HAMD, Hamilton Depression Rating Scale; MADRS, Montgomery-Åshberg Depression Rating Scale; MDD, major depressive disorder; NETA, norethindrone acetate; POMS, profile of mood states;
Kronos Early Estrogen Prevention Study–Cognitive and Affective Study (KEEPS-Cog)
Reference numbers refer to the reference list in the main paper.
Shading indicates high Risk of Bias.
Six RCTs showed an improvement in some aspect of mood on hormone therapy,29–31,33,36,37 while three studies showed no effect of hormones on any mood endpoint.32,35,38
Among studies that specifically evaluated depression, hormone therapy improved depression scores compared to placebo in two studies,29,30 and three studies found no difference in depression scores between hormone and placebo groups (both groups improved).32,35,38
Mood may be affected by the presence of menopausal symptoms and by sleep, which may be disrupted by vasomotor symptoms. Some studies were able to disentangle improvements in mood from reduced hot flashes and improved sleep, while other studies were unable to do so. A study that randomised women with depression, hot flushes and sleep disturbances to estrogen therapy, zolpidem (a sedative-hypnotic), or placebo found similar responses of depression in all groups. Improvement in depressive symptoms was predicted by improved sleep quality in peri- and postmenopausal women. 32 In an RCT that tested an estrogen patch against a placebo, estrogen improved sleep only in women with severe nocturnal hot flashes. 39
In two short-term studies (8–12 weeks) that tested transdermal hormone therapy in perimenopausal women (women who were menstruating and had blood hormone concentrations suggestive of approaching menopause), depressive symptoms improved to a greater extent on estrogen compared to placebo.36,37 Another study of euthymic women concluded that estrogen plus progestogen prevented the onset of depression in early perimenopausal women but not in late perimenopausal women or early postmenopausal women. 31 The depression outcome was determined by a score of 16 or more on the Center for Epidemiologic Studies Depression Scale in any of seven follow-up periods. In a six-week study in perimenopausal women, estrogen augmented the effect of antidepressant medications. 33
Transdermal estrogen had no clear advantage on mood. The KEEPS study found that depression and anxiety, in the Profile of Mood States Domain, improved among women taking oral CEE but not transdermal 17β-estradiol when compared to placebo.30,34 Three of four studies investigating the effects of transdermal 17β-estradiol therapy found no difference between hormone and placebo groups.30,32,35 The one study of transdermal estrogen that found an improvement in mood included data from participants on placebo who dropped out before completion of the trial. 36
In summary, inconsistent findings and measurements of hormone therapy effects on mood from RCTs do not support the hypothesis that hormones, independent of effects on hot flashes and sleep disturbance, are beneficial for depression. There was no clear advantage of 17β-estradiol over CEE. More detailed information on hormones used and outcome measures can be found in Table 3. Based on the GRADE evaluation, we have very low certainty that menopausal hormones decrease depression scores. Certainty was decreased by risk of bias, inconsistency and possible publication bias.
Cognition
Nine RCTs evaluated cognition in 2452 women. Two studies had a high Risk of Bias (Table 4).
Randomized clinical trials evaluating cognition
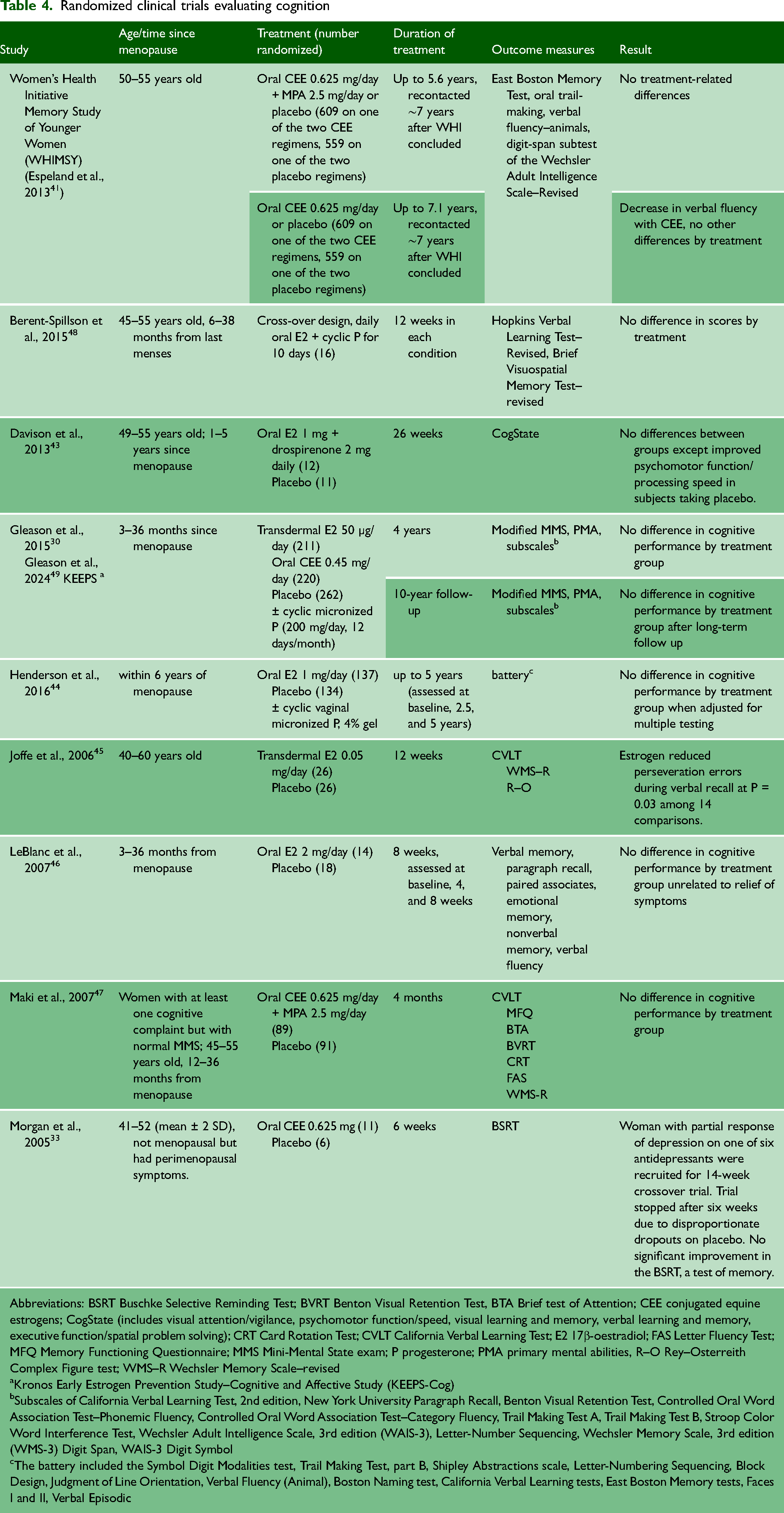
Abbreviations: BSRT Buschke Selective Reminding Test; BVRT Benton Visual Retention Test, BTA Brief test of Attention; CEE conjugated equine estrogens; CogState (includes visual attention/vigilance, psychomotor function/speed, visual learning and memory, verbal learning and memory, executive function/spatial problem solving); CRT Card Rotation Test; CVLT California Verbal Learning Test; E2 17β-oestradiol; FAS Letter Fluency Test; MFQ Memory Functioning Questionnaire; MMS Mini-Mental State exam; P progesterone; PMA primary mental abilities, R–O Rey–Osterreith Complex Figure test; WMS–R Wechsler Memory Scale–revised
Kronos Early Estrogen Prevention Study--Cognitive and Affective Study (KEEPS-Cog)
Subscales of California Verbal Learning Test, 2nd edition, New York University Paragraph Recall, Benton Visual Retention Test, Controlled Oral Word Association Test–Phonemic Fluency, Controlled Oral Word Association Test–Category Fluency, Trail Making Test A, Trail Making Test B, Stroop Color Word Interference Test, Wechsler Adult Intelligence Scale, 3rd edition (WAIS-3), Letter-Number Sequencing, Wechsler Memory Scale, 3rd edition (WMS-3) Digit Span, WAIS-3 Digit Symbol
The battery included the Symbol Digit Modalities test, Trail Making Test, part B, Shipley Abstractions scale, Letter-Numbering Sequencing, Block Design, Judgment of Line Orientation, Verbal Fluency (Animal), Boston Naming test, California Verbal Learning tests, East Boston Memory tests, Faces I and II, Verbal Episodic
Women's Health Initiative
The Women's Health Initiative Memory Study (WHIMS) reported that global and domain-specific cognitive function were impaired in women randomised to receive hormone therapy at age 65 or older.40,41 The Women's Health Initiative Study of Younger Women (WHIMSY), a sub-study of the WHI, included women starting treatment at age 50–55. Telephone assessments of cognition in these subjects 7.2 years after the WHI ended included the East Boston Memory Test, the Oral Trail Making Test, Verbal Fluency–Animals, and the Digit Span subtest of the Wechsler Adult Intelligence Scale–Revised. Except for a decrease in verbal fluency among women who received CEE only, there were no differences among placebo, CEE-treated, or CEE + MPA-treated women in global or domain-specific cognitive function. 42
Other trials
Eight other RCTs are summarised in Table 4.30,33,43–49 With one exception, no trial showed an improvement in any cognitive measure in menopausal women randomised to hormone therapy. The exception, the paper by Joffe et al., reporting a 12-week trial supported by industry, 45 was one of two in the cognitive group with a high risk of bias. Among 14 comparisons in this study, not necessarily independent, only one comparison favoured 17β-estradiol therapy; perseveration errors on verbal recall in the California Verbal Learning Test decreased by a mean of 2.2, 95% CI −4.0 to −0.3. None of the other studies confirmed memory errors, and the association may have arisen by chance. The KEEPS study did not find a difference in cognitive performance during the four-year trial, 30 neither was there any difference between treatment group and placebo in the 10-year follow-up. 49
In summary, no benefit of hormones on cognition was shown in eight RCTs; the ninth showed a benefit in only one of 14 comparisons and is not reliable. There was no apparent advantage of 17β-estradiol, used in six of the studies, over CEE, used in three of the studies. Our conclusion, using GRADE criteria, is that available RCTs do not show a cognitive benefit of menopausal hormone therapy.
Discussion
Main findings
Although critics have stated that women in the WHI were too old to provide informative data about hormone therapy in women close to menopause, the WHI remains the largest RCT of menopausal hormone therapy in young menopausal women. In the CEE + MPA trial, the WHI randomised 5522 women who were 50–59 years old, 4092 of whom were fewer than 10 years from the onset of menopause. 50 The CEE-only trial included 3310 women 50–59 years old, 1237 of whom were within 10 years of menopause onset. Some results given for women 50–55 years of age or within five years of menopause did not show benefits. Whether these women might have benefited from starting menopausal hormones at a younger age or sooner after menopause is unknown.
In this systematic review, we examined randomised clinical trials of women aged 50–60 years or women who were within a short period of time after their last menses, as defined by the individual study authors. Despite casting a wide net (we did not restrict pharmaceutical estrogen, dose or route of exposure except vaginal administration), we found no preparation or route of administration that offered superior health benefits to those found in the WHI. Oral CEE was used in five trials, oral 17β-estradiol therapy was used in six trials, and transdermal 17β-estradiol therapy was used in six trials. Our findings are consistent with a Cochrane meta-analysis of randomised, placebo-controlled trials that lasted more than a year.54 The analysis did not identify a beneficial effect of hormone therapy on the prevention of chronic disease.
Our results differ from three previous analyses. A systematic review and meta-analysis included open-label studies and surrogate endpoints, deficiencies that might account for its claim of a benefit of hormone therapy on cardiovascular mortality. 51 Another meta-analysis of menopausal hormone therapy and coronary heart disease reported a reduction in disease in women enrolled before age 60, but the four-page report was too brief and lacked detail about its methods. 52 A meta-analysis from the same group, reported in greater detail, noted a decrease in overall mortality in women starting hormone therapy before age 60, but found no advantage for hormones in cardiovascular or cancer mortality. 53 Some trials in that meta-analysis did not have a placebo arm or used calcium pills as a placebo. The authors of a Cochrane systematic review criticised the Salpeter et al. meta-analysis for including trials without a placebo arm and studies of less than one year duration, inappropriate for drawing conclusions about chronic diseases. 54
Among women in the WHI randomised to CEE at age 50–59, 1129 women had bilateral salpingo-oophorectomy, and 2008 women had hysterectomy with retention of at least part of one ovary. 51 There was a decrease in all-cause mortality in oophorectomised women randomised to CEE (HR 0.68, 95% CI 0.48 to 0.96), but no effect of CEE treatment on coronary heart disease or invasive breast cancer. This possible protective effect on mortality was seen primarily in women randomised to estrogen within 10 years of surgery; it was not seen in women randomised 20 or more years after surgery. It is possible that oophorectomy increased the risk that was mitigated by estrogen treatment. No other randomised trial evaluated this possibility. Because the use of CEE alone in the WHI was a proxy for hysterectomy, which often included oophorectomy, we could not determine whether the protective effect in the CEE-alone group was due to attenuation of oophorectomy-associated risk or to hormone treatment independent of oophorectomy.
Mood and cognition may be influenced by vasomotor symptoms that interfere with sleep. Neither the WHI nor the other RCTs definitively addressed this possibility, with the exception of one study that showed similar benefits on depression of a sleep aid, hormone therapy, and placebo.
Strengths and limitations
This systematic review included all RCTs of menopausal hormone therapy in women under 60 or within a short period of time after the last menses. A strength is our acceptance of authors’ definitions of a short period of time after the last menses and our consideration of all pharmaceutical estrogens by any route except exclusively vaginal administration.
It could be considered a weakness that our review did not consider surrogate endpoints, including mechanistic endpoints, blood pressure, lipid concentrations, or other cardiovascular disease risk factors. Surrogate endpoints do not represent disease and may be misleading. For example, serum lipid concentrations in the WHI were favourably altered by menopausal hormone therapy, but cardiovascular disease was increased. 55 In the GRADE system, use of surrogate endpoints results in downgrading of certainty due to lack of direct evidence for the clinical outcome. To the extent that surrogate endpoints predict clinical disease, our review has not considered these endpoints.
Our findings offer little support for the timing hypothesis, although there is a reduction in some measures of cardiovascular disease and all-cause mortality in women treated with estrogen within 10 years after oophorectomy, particularly oophorectomy prior to age 45. 56 This protective effect was not confirmed in other studies or in a subsequent analysis of the WHI data. One study cited by proponents of the timing hypothesis is Schierbeck et al., 57 which was not included in our analysis because of the lack of a placebo arm. In the Schierbeck et al. study, 1006 women aged 45–58 years and 3–24 months since their last episode of bleeding were randomised to menopausal hormone therapy (a cyclic estrogen- progestogen regimen in women with a uterus, estrogen-only in women who had a hysterectomy), or no therapy. After 10.1 years, when the findings of the WHI came out, subjects were advised to stop hormones, but continued to be followed up via national registries for an additional 5.7 years. At the end of the 10.1-year study period, a composite endpoint of death, myocardial infarction, and heart failure was reduced in the women taking hormones. At the end of the full 15.8 years of follow-up, the composite endpoint was described as reduced in women who were randomised to hormones. However, the result was not significant, because the 95% CI included the null value of 1.0. None of the secondary endpoints, including stroke, venous thromboembolism, pulmonary embolism, breast cancer, any cancer, or the individual components of the composite endpoint (death, myocardial infarction, heart failure) showed any difference between groups. This trial does not provide convincing evidence in favour of the timing hypothesis.
The Cochrane meta-analysis 54 found substantial heterogeneity among trials in hormone preparations and duration of treatment, and only meta-analysed subgroups of studies with the same active hormone treatment and similar lengths of treatment. As those authors found, the WHI was a prominent driver of findings due to its larger size compared to the other trials. We separately evaluated studies without a high Risk of Bias and studies of 17β-estradiol therapy and did not find evidence to support the timing hypothesis.
We did not consider the beneficial effects of hormones on vasomotor symptoms or bone health, which have been amply demonstrated. We do not suggest that it is inappropriate to prescribe menopausal hormones. However, in the risk-benefit calculus, the prevention of chronic disease should not be identified as a benefit unless and until randomised clinical trials demonstrate a benefit.
Conclusion
We did not identify consistent evidence to support the timing hypothesis for menopausal hormone therapy in the prevention of chronic disease. The WHI found no health benefits for early menopausal women using menopausal hormone therapy on cardiovascular disease, cancer or cognition, except a possible decrease in cardiovascular disease or all-cause mortality in women given estrogen within 10 years of oophorectomy, which may have been due to protection from oophorectomy-associated risks. The null findings of the WHI with respect to prevention of chronic disease have not been contradicted by other RCTs, including trials that tested different preparations and routes. We did not identify data supporting the concept that women starting hormone therapy in their 50s and stopping therapy after a given number of years have a rebalancing of risks and benefits. This systematic review supports the recommendations of professional groups not to use menopausal hormone therapy for the prevention of chronic disease.58–61
Supplemental Material
sj-docx-1-shr-10.1177_20542704261455970 - Supplemental material for The effects of menopausal hormone therapy on cardiovascular disease, cancer, cognition and depression in younger women: A systematic review
Supplemental material, sj-docx-1-shr-10.1177_20542704261455970 for The effects of menopausal hormone therapy on cardiovascular disease, cancer, cognition and depression in younger women: A systematic review by Patricia A Bencivenga, Natalie Fort, Adriane Fugh-Berman and Anthony R Scialli in JRSM Open
Footnotes
Acknowledgements
The authors thank Caroline Renko for expert manuscript preparation.
Contributorship
Patricia A. Bencivenga: conceptualisation, data curation and validation, manuscript review and editing. Natalie Fort: data curation and validation, manuscript review and editing. Adriane Fugh-Berman: methodology, data validation, manuscript review and editing. Anthony R. Scialli: conceptualisation, supervision, investigation, original draft. All authors read and approved the final version.
Declaration of conflicting interests
Anthony R. Scialli has been a consultant for pharmaceutical companies, including AbbVie, Altimmune, Alvylam Pharmaceuticals, Amgen, Biohaven Pharmaceuticals, Bayer, Bristol Myers Squibb, Celgene, Eisai, Harmony Biosciences, Jazz Pharmaceuticals, Merck, Mitsubishi Tanabe, Myovant Science, Moderna, Novartis, Roche, Sanofi, Satsuma Pharmaceuticals, Seqirus, and Vertex Pharmaceuticals. Adriane Fugh-Berman is a paid expert witness at the request of plaintiffs in litigation regarding pharmaceutical marketing practices. Patricia A. Bencivenga and Natalie Fort have no conflicts of interest.
Ethical approval
Ethical approval was not required because no patients were involved in this systemtic review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Anthony R. Scialli, M.D.
Provenance
Not commissioned, peer reviewed by Julie Morris and Roxanna Pirhadi.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.