
Abstract
Background
A prior study of living kidney donors demonstrated a substantially higher long-term risk of hydrocelectomy among male living kidney donors who underwent laparoscopic nephrectomy compared with nondonors. Given the potential shared anatomical pathways between hydrocele and indirect inguinal hernia formation, we aimed to evaluate the donation-attributable risk of inguinal hernia repair.
Objective
To evaluate long-term rates of inguinal hernia repair in male living kidney donors compared to nondonors.
Design and Setting
Population-based, retrospective matched cohort study using linked health administrative databases from Ontario, Canada.
Patients
848 male living kidney donors aged ≥18 years who underwent laparoscopic donor nephrectomy between April 1, 2002, and March 31, 2023, were matched (1:10) to 8480 healthy male nondonors based on age, cohort entry date, rurality, neighbourhood income, and prior vasectomy. Individuals with prior scrotal conditions or previous inguinal hernia repair were excluded.
Measurements
The primary outcome was inguinal hernia repair.
Methods
Risk was assessed using Cox proportional hazards models with robust variance. Cumulative incidence was estimated at key time points using Aalen–Johansen methods, treating death as a competing event. To contextualize the findings, incidence rates were also examined after other renal (e.g., nondonor nephrectomy, pyeloplasty) and abdominal surgeries.
Results
Over a median follow-up of 8.8 years, 4.7% of donors (40 of 848) and 3.4% of nondonors (287 of 8480) underwent inguinal hernia repair. Donors had a modestly higher risk of undergoing inguinal hernia repair than nondonors (4.9 vs. 3.5 events per 1000 person-years; hazard ratio (HR) 1.40; 95% CI, 1.01–1.93; P = 0.043). The cumulative incidence of inguinal hernia repair after laparoscopic donor nephrectomy was comparable to that observed after other renal and abdominal surgeries.
Limitations
This study relied on administrative data, which lacked information on hernia type (direct or indirect), laterality, pre-existing asymptomatic hernias, and key confounders such as body mass index and occupation. Donors may differ from nondonors in care-seeking behaviours and lifestyle factors, which could influence the observed risk.
Conclusions
In contrast to the markedly higher risk of hydrocele repair, the donation-attributable risk of inguinal hernia repair in the years following laparoscopic donor nephrectomy appears modest, and in some comparisons was not evident. These findings support current counselling and selection practices for prospective donors, for which this outcome does not warrant specific consideration.
Introduction
Living kidney donation offers the best outcomes for patients with kidney failure and accounts for approximately 25-30% of kidney transplants in Canada each year. 1 A clear understanding of long-term donation-attributable outcomes is crucial for informed consent, guiding post-donation follow-up care, and designing interventions to mitigate these risks.
In Canada, administrative healthcare databases allow for long-term follow-up of living kidney donors with minimal loss to follow-up due to the universal public healthcare system. 2 While these databases often do not capture patient-reported symptoms, the laterality of surgery, or the results of tests or procedures, they do reliably capture whether surgical procedures were performed. 3 Our team has previously used large health administrative databases in Ontario to evaluate the long-term outcomes of living kidney donors.4-12
In a recent study, we found that male living kidney donors who underwent laparoscopic nephrectomy had a substantially higher long-term risk of hospital admission for scrotal hydrocelectomy compared to matched male nondonors from the general population with similar baseline health indicators (hazard ratio, 38.8 [95% CI, 22.1 to 67.9]). 13 This unexpected finding prompted us to examine whether other post-donation complications might also occur more frequently, specifically inguinal hernias. Inguinal hernias are clinically meaningful as they can cause pain, limit physical activity, and may require surgical repair, which carries its own risks.14,15,16
Scrotal hydroceles and indirect inguinal hernias share overlapping anatomic pathways, as both can arise from a disrupted or patent processus vaginalis. When the patent processus vaginalis remains patent or incompletely closes, peritoneal fluid can track into the scrotum and accumulate as a hydrocele, or abdominal contents can protrude through the inguinal canal to form an indirect (lateral) inguinal hernia.15,17 Other mechanisms may also contribute; hydroceles can result from trauma, infection, or impaired fluid absorption within the tunica vaginalis, 15 whereas inguinal hernias may develop from acquired weakness of the abdominal wall, particularly within Hesselbach’s triangle (direct/medial hernia) or from chronically increased intra-abdominal pressure.15,17 Inguinal hernia repair is very common, with men having an estimated 27% risk of undergoing groin hernia repair in their lifetime.18,19 Population studies suggest that 56% of primary hernia repairs in adult men are for indirect hernias and 44% for direct hernias. 20
While an increased risk of inguinal hernia has been observed after lower pelvic surgeries such as prostatectomy,21-25 it has not been evaluated in the context of upper abdominal procedures such as living donor nephrectomy. We conducted this population-based cohort analysis to assess whether male living kidney donors who underwent laparoscopic nephrectomy had a higher long-term risk for undergoing inguinal hernia repair than male nondonors selected from the general population with baseline health indicators similar to those in donors. To contextualize our findings, we also examined incidence rates following other renal and abdominal surgical procedures.
Methods
Study Design and Setting
We conducted a population-based, retrospective matched cohort study using multiple linked health administrative databases housed at ICES in Ontario, Canada. This study extends our prior work on scrotal surgery outcomes in living kidney donors. 13 We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) and REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines for reporting observational studies (see Supplemental Table 1).26,27
Data Sources
We used several linked health administrative databases held at ICES, including the Trillium Gift of Life Network (TGLN), the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD), Same Day Surgery (SDS), National Ambulatory Care Reporting System (NACRS), Ontario Health Insurance Plan (OHIP), and the Ontario Registered Persons Database (RPDB). CIHI-DAD provides detailed diagnostic and procedural information for all hospital admissions, while OHIP captures all physician billing claims for inpatient and outpatient services. RPDB contains demographic and vital status data for all residents of Ontario. These datasets were linked using unique encoded identifiers and analyzed at ICES.
The accrual period began on April 1, 2002, when the Canadian Classification of Health Interventions (CCI) was implemented. Living kidney donors were identified using TGLN, which captures all living donor procedures at the time of donation, supplemented by CIHI-DAD when TGLN data were unavailable (April 1, 2022 to March 31, 2023). 28
Participant Eligibility
We included male residents aged 18 years or older who underwent laparoscopic donor nephrectomy between April 1, 2002, and March 31, 2023. During this period, approximately 80% of male donor nephrectomies in Ontario were done with a laparoscopic procedure. The date of nephrectomy served as the cohort entry date. We excluded males with prior scrotal conditions (e.g., hydrocele, spermatocele, or haematocele), prior scrotal ultrasound, or prior scrotal procedures before donation (excluding vasectomy). To avoid confounding of recurrent hernias, we also excluded individuals with a history of inguinal hernia repair.
Only healthy persons are eligible to become donors. Using epidemiologic techniques of restriction and matching, a group of nondonors from the general population was selected to have baseline health indicators similar to those of donors. A simulated donation date (cohort entry date, also called the index date) was randomly assigned to each nondonor based on the distribution of donor nephrectomy dates. From the initial 5,106,777 men, we excluded anyone with medical conditions that would prevent donation. To ensure adequate access to health care, we included only men who had seen a primary care physician at least once in the previous two years. As with the donor group, men with a history of scrotal conditions or prior inguinal hernia repair before cohort entry were excluded. After applying these criteria, 1,322,291 men (26% of the original cohort) qualified as eligible nondonors (see Figure 1). Cohort creation. Abbreviations: HIV, human immunodeficiency virus; ICU, intensive care unit. a We included all male residents of Ontario who received a donor nephrectomy between April 1, 2002, and March 31, 2023. Of 1372 male donors, we excluded 64 for reasons of data cleaning (i.e., missing or invalid ICES key number, age, or sex; death before the index date; non-Ontario resident; Ontario Health Insurance Plan ineligibility; date of last contact in the Registered Persons Database <4 months after cohort entry date); or data errors (i.e., evidence of dialysis before donation or in the 4 months after donation; prior solid organ transplant; listed as a living kidney donor more than once; or no physician visits in the past year [donors have to see physicians multiple times in the year before donation]). Each donor’s nephrectomy date served as their cohort entry date. b We randomly assigned a cohort-entry date (a simulated nephrectomy date) to all male citizens of Ontario based on the distribution of cohort-entry dates among donors (April 1, 2002, to March 31, 2023). Of 11,311,796 males, we excluded 6,205,019 who were age <18 years at cohort entry or as part of data cleaning (i.e., missing or invalid ICES key number, age, or sex; death before cohort entry; non-Ontario resident; Ontario Health Insurance Plan ineligibility; or date of last contact in the Registered Persons Database < 4 months after cohort entry date). c Scrotal conditions excluded included hydrocele, spermatocele, or haematocele. d We matched each donor to 10 eligible nondonors on age at the time of cohort entry (±1 year), the cohort entry date (±3 years), urban or rural residence (population ≥10,000 or <10,000), income (categorized into fifths of average neighborhood income), and prior vasectomy. Each nondonor could only be selected once. All donors were successfully matched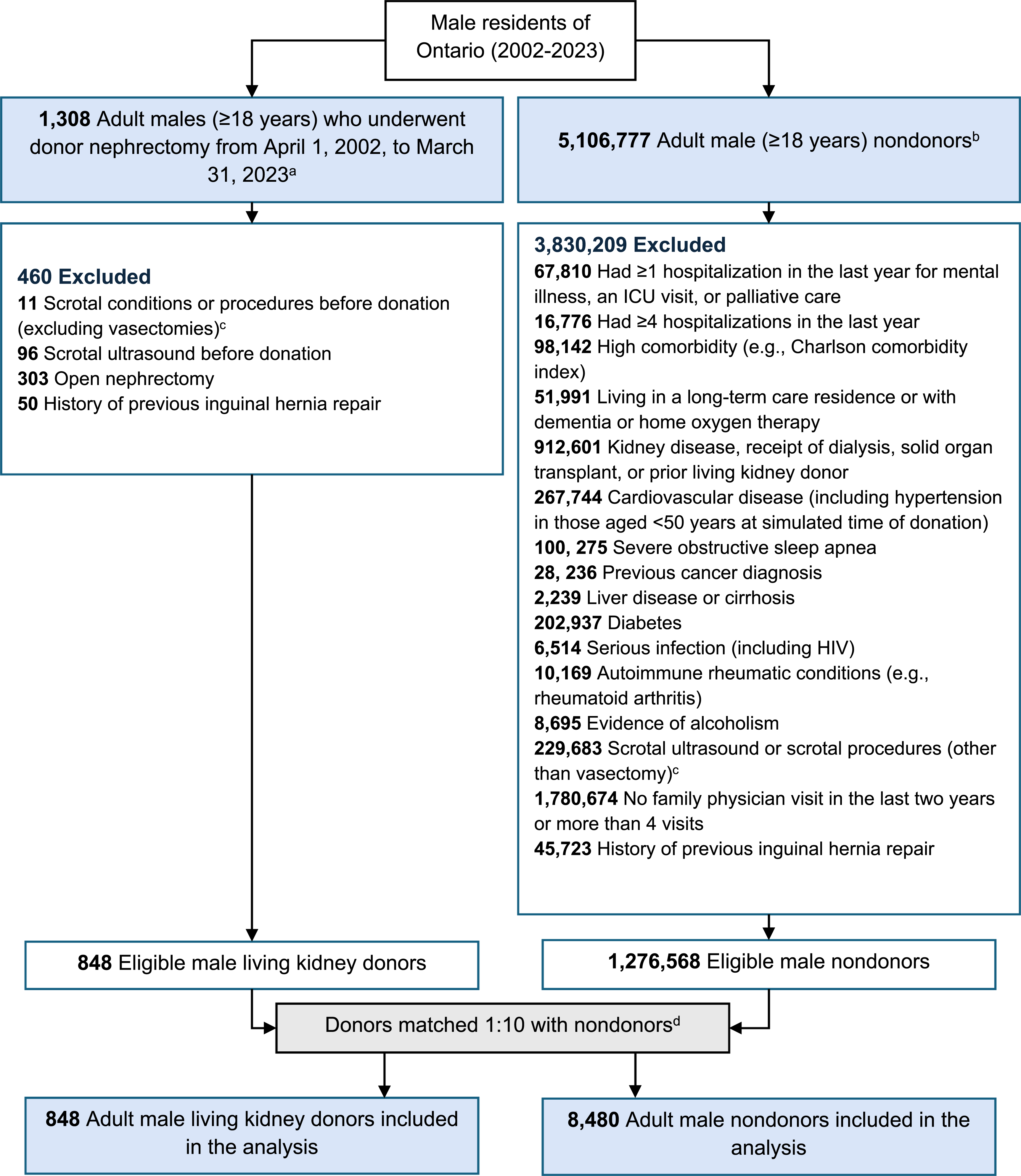
Matching
Each living kidney donor was matched to 10 eligible nondonors based on baseline characteristics associated with healthcare access and inguinal hernia risk. Matching variables were age at cohort entry (±1 years), cohort entry date (±3 years), urban vs. rural residence (population ≥10,000 vs. <10,000), neighbourhood income quintile, and prior vasectomy. Each nondonor could only be matched once.
Baseline Characteristics
Baseline characteristics were assessed at the index date, defined as the donation date for donors and the simulated donation date for nondonors. Demographic data, including age and sex, were obtained from RPDB. Medical comorbidities were identified using validated algorithms applied to hospital discharge records and physician claims.
Outcome
Participants were followed from cohort entry until death, emigration from the province (the only reason for loss to follow-up), or the end of the observation period (March 31, 2024). The primary outcome was an inguinal hernia repair. In Ontario, physicians are paid for fee-for-service procedures, such as surgeries or ultrasound readings, only after submitting the appropriate billing codes. Consequently, procedures are well coded.3,29 To further enhance confidence in primary outcome ascertainment, evidence of both a surgeon-fee-for-service code and a hospital procedural code was required, each recorded in separate health care databases by different personnel who were unaware that this study would occur in the future. Supplemental Table 2 provides further details on outcome codes.
Given that donor nephrectomy involves an abdominal incision, there is a risk that some incisional hernias could be miscoded as inguinal hernias in administrative data, so we ensured there was no evidence of an incisional hernia code within the same hospitalization. In our health administrative data, we lack details on hernia type (indirect versus direct) and laterality (left versus right); we can only accurately determine that an inguinal hernia repair was performed.
Statistical Analysis
Baseline characteristics were compared between donors and nondonors before and after matching using standardized mean differences, with values >10% considered meaningful. 30 Descriptive statistics were reported as counts and percentages, medians and interquartile ranges (IQR), or means and standard deviations, as appropriate. All donor-to-nondonor comparisons had complete data, except for two baseline characteristics (rurality and income quintile) with less than 0.5% missing.
The association between laparoscopic donor nephrectomy and time to first event was assessed using Cox proportional hazards regression with robust variance estimation to account for correlation within matched sets. The proportional hazards assumption was evaluated and met using the Kolmogorov-type supremum test with 1,000 simulated patterns.
Outcomes were described using incidence rates per 1,000 person-years and cumulative incidence, estimated via the Aalen-Johansen estimator, treating death as a competing event. Incidence rate differences and 95% confidence intervals (CIs) were calculated using Poisson regression with a log-transformed offset for follow-up time.
To contextualize the risk observed among donors, we created additional male surgical cohorts using hospital procedural codes which were categorized by operation type and surgical approach. These cohorts included other renal surgeries (partial nephrectomy, total nephrectomy, and pyeloplasty), major intra-abdominal surgeries (adrenalectomy, splenectomy, and cholecystectomy), prostatectomy, and hip and knee surgeries. Individuals with a prior history of inguinal hernia repair were excluded from each cohort. We report incidence rates (events per 1,000 person-years) and cumulative incidence (at 1, 5, 10, 15, and 20 years) across surgical cohorts and between laparoscopic and open procedures. We expected incidence rates to be very high after radical prostatectomy, as this procedure is known to weaken the inguinal floor at the myopectineal orifice (transversalis fascia/posterior canal wall), unmasking occult defects and predisposing to both direct (Hesselbach’s triangle) and indirect (internal ring) hernias.22,24,25
In an additional analysis, the association between living kidney donation and inguinal hernia repair was examined separately among participants with and without a history of vasectomy before cohort entry. To assess whether prior vasectomy modified this association, an interaction term was included between donor status and prior vasectomy status in the Cox proportional hazards model. Results are presented in Supplemental Table 3.
All results are presented as point estimates with 95% CIs. Statistical analyses were performed using SAS software (version 9.4; SAS Institute, Inc, Cary, North Carolina).
Results
A total of 848 male living kidney donors and 8480 nondonors were followed for a median of 8.7 years and 8.8 years, with a maximum follow-up of 22.0 years and 22.0 years, respectively. During follow-up, patients were lost due to death (22 donors [2.6%], 287 nondonors [3.4%]), emigration (26 donors [3.1%], 301 nondonors [3.6%]), or reaching the end of follow-up (760 donors [89.6%], 7,605 nondonors [89.7%]).
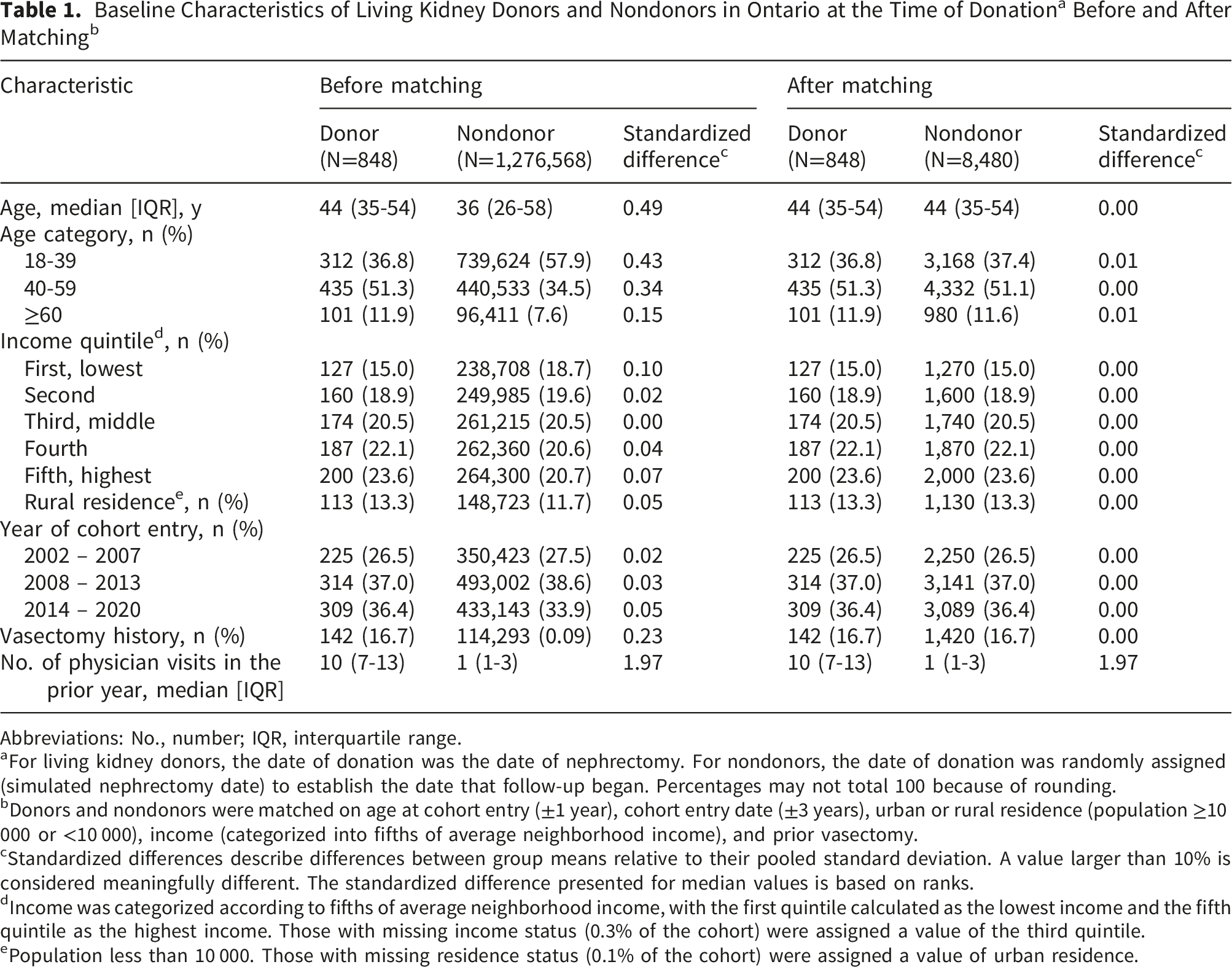
Abbreviations: No., number; IQR, interquartile range.
aFor living kidney donors, the date of donation was the date of nephrectomy. For nondonors, the date of donation was randomly assigned (simulated nephrectomy date) to establish the date that follow-up began. Percentages may not total 100 because of rounding.
bDonors and nondonors were matched on age at cohort entry (±1 year), cohort entry date (±3 years), urban or rural residence (population ≥10 000 or <10 000), income (categorized into fifths of average neighborhood income), and prior vasectomy.
cStandardized differences describe differences between group means relative to their pooled standard deviation. A value larger than 10% is considered meaningfully different. The standardized difference presented for median values is based on ranks.
dIncome was categorized according to fifths of average neighborhood income, with the first quintile calculated as the lowest income and the fifth quintile as the highest income. Those with missing income status (0.3% of the cohort) were assigned a value of the third quintile.
ePopulation less than 10 000. Those with missing residence status (0.1% of the cohort) were assigned a value of urban residence.
Outcome Events Among Living Kidney Donors and Matched Nondonors
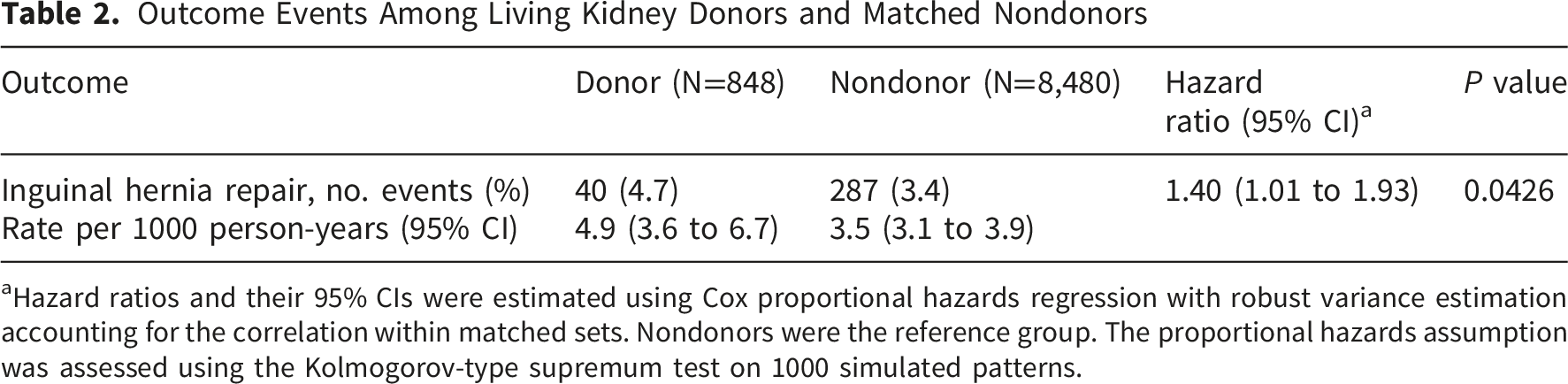
aHazard ratios and their 95% CIs were estimated using Cox proportional hazards regression with robust variance estimation accounting for the correlation within matched sets. Nondonors were the reference group. The proportional hazards assumption was assessed using the Kolmogorov-type supremum test on 1000 simulated patterns.
Hospital Admission for Inguinal Hernia Repair in Male Living Kidney Donors, Male Nondonors From the General Population in Ontario, and Males Who had Different Types of Surgery During the Study Period
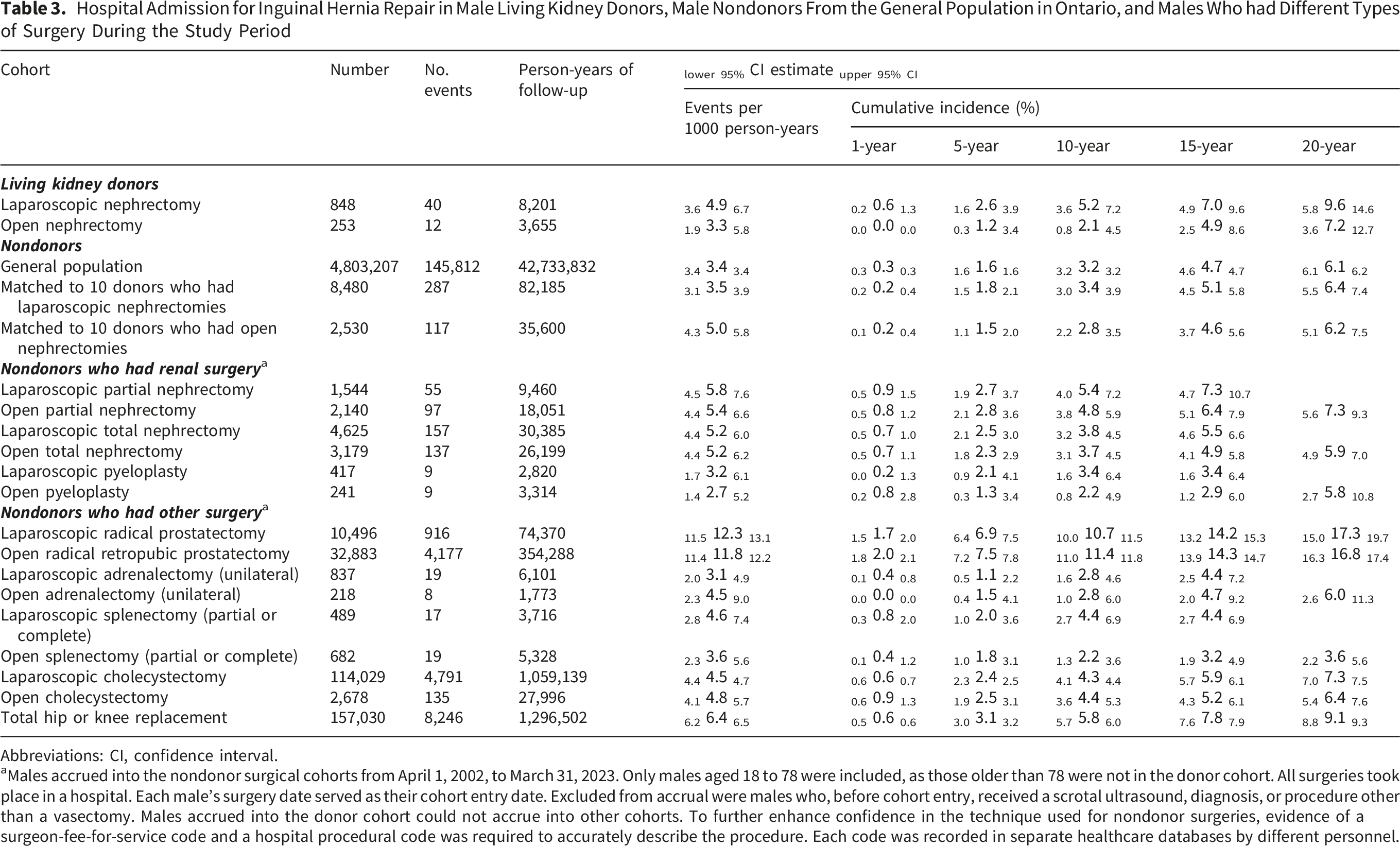
Abbreviations: CI, confidence interval.
aMales accrued into the nondonor surgical cohorts from April 1, 2002, to March 31, 2023. Only males aged 18 to 78 were included, as those older than 78 were not in the donor cohort. All surgeries took place in a hospital. Each male’s surgery date served as their cohort entry date. Excluded from accrual were males who, before cohort entry, received a scrotal ultrasound, diagnosis, or procedure other than a vasectomy. Males accrued into the donor cohort could not accrue into other cohorts. To further enhance confidence in the technique used for nondonor surgeries, evidence of a surgeon-fee-for-service code and a hospital procedural code was required to accurately describe the procedure. Each code was recorded in separate healthcare databases by different personnel.
The incidence rate of inguinal hernia repair after laparoscopic living donation was similar to rates seen in the general population and after several other non-laparoscopic donor surgeries (Table 3). In the general population, the rate was 3.4 events per 1000 person-years (95% CI, 3.4–3.4). Comparable rates were observed after open donor nephrectomy (3.3; 95% CI, 1.9–5.8). Rates were slightly higher following total laparoscopic nondonor nephrectomy (5.2; 95% CI, 4.4–6.0) and total open nondonor nephrectomy (5.2; 95% CI, 4.4–6.2) and ranged from 3.1 to 6.4 after other surgeries such as adrenalectomy, splenectomy, cholecystectomy, and hip or knee replacement. As expected, incidence rates were substantially higher after procedures involving the prostate: 12.3 (95% CI, 11.5–13.1) after laparoscopic radical prostatectomy and 11.8 (95% CI, 11.4–12.2) after open radical retropubic prostatectomy.
When stratified by prior vasectomy status, the association between living kidney donation and inguinal hernia repair was similar among participants with and without a history of vasectomy before cohort entry, with no evidence of effect modification by vasectomy status (interaction p=0.54; Supplemental Table 3).
Discussion
In this population-based study, adult males who underwent laparoscopic donor nephrectomy experienced modestly higher rates of inguinal hernia repair over the subsequent decade compared with matched healthy non-donors. However, when interpreted in the context of incidence rates after other renal and intra-abdominal operations (ranging from 2.8 to 5.8 per 1,000 person-years), rates among donors appeared to fall within this range. Overall, the findings suggest there is no clinically important excess risk of inguinal hernia repair.
Our results substantially differ from the markedly higher risk of hydrocele repair after laparoscopic donor nephrectomy observed in our prior study. 13 Hydrocele formation and indirect inguinal hernias share related anatomical pathways involving the processus vaginalis and the inguinal canal, which prompted investigation of whether a similar association might exist for inguinal hernia repair after kidney donation.
Indirect (lateral) inguinal hernias arise through a patent processus vaginalis at the internal ring, whereas direct (medial) hernias protrude through weakened transversalis fascia in Hesselbach’s triangle.15,17 Known risk factors for inguinal hernia repair include male sex, lower body mass index, older age, connective tissue disorders, and occupations involving heavy physical activity.14,15,17,31-36 Additional factors that increase intra-abdominal pressure, such as chronic liver disease, chronic cough, constipation, obesity, and benign prostatic hyperplasia, have also been associated with hernia formation. 18 Because living kidney donors undergo extensive screening before donation, they are selected for excellent baseline health and are unlikely to have these additional risk factors. In our study, the nondonor comparator cohort was restricted using stringent eligibility criteria designed to approximate the health status required for kidney donation and minimize baseline differences in these risk factors between groups.
As our outcome was inguinal hernia repair rather than hernia diagnosis, greater clinical contact among donors during routine follow-up could contribute to earlier detection and referral for surgical repair. It is therefore possible that differences in health care contact or timing of repair, rather than true differences in hernia incidence, may partly explain the modestly higher repair rates observed in donors.
Comparisons with other surgical cohorts help contextualize our findings, acknowledging these are crude rates unadjusted for differences in baseline health characteristics. Procedures that involve extensive preperitoneal dissection near the internal inguinal ring, such as radical prostatectomy, are associated with substantially higher subsequent inguinal hernia rates, whereas operations performed higher in the abdomen generally carry a lower risk. 25 In laparoscopic donor nephrectomy trocar placement and retroperitoneal/upper abdominal dissection are generally remote from the inguinal canal, making a direct procedure-related weakening of the inguinal floor less biologically plausible. In our study, differences between laparoscopic and open nephrectomy were modest.
Our study’s strengths include its population-based cohort of male living kidney donors, careful selection of male nondonors with baseline characteristics similar to those of donors, unbiased outcome ascertainment, and a median follow-up of 8.8 years (maximum of 22.0 years) with less than 6.8% lost to follow-up (provincial emigration) or death. Donors and nondonors had access to a universal health care system in which physician billings and hospital procedures are routinely captured in administrative health databases.
This study has some limitations. Administrative data does not capture pre-existing asymptomatic hernias that later worsened, hernia laterality or type (direct vs. indirect), hernia size, or symptom severity. As a result, some post-nephrectomy hernia diagnoses may reflect the progression or detection of pre-existing disease rather than incident hernias attributable to nephrectomy. Laterality is of particular interest because right-sided inguinal hernias are more common, 17 while donor nephrectomies are typically performed on the left. 37 Without information on the side of the hernia, it is not possible to assess whether hernias occur ipsilateral to the nephrectomy. Distinguishing between direct and indirect inguinal hernias would provide additional insight into the underlying mechanisms of hernia development, as these hernia types arise through different anatomical pathways and may reflect distinct contributions of surgical disruption versus underlying tissue weakness.
Future studies should incorporate operative details, including side of nephrectomy, intra-abdominal pressure from the pneumoperitoneum, and duration of surgery. Future work could also extend these analyses to women; however, effect estimates would likely be imprecise given their substantially lower lifetime risk of inguinal hernia repair, approximately 3% compared with 27% in men. 19
Conclusions
In contrast to the markedly higher risk of hydrocele repair, higher donation-attributable risk of inguinal hernia repair in the years following laparoscopic donor nephrectomy appears modest or non-existent. Overall, these findings support current counselling and selection practices for prospective donors, for which this outcome does not appear to warrant specific consideration.
Supplemental Material
Supplemental Material - Risk of Inguinal Hernia Repair Following Laparoscopic Living Donor Nephrectomy: A Population-Based Cohort Study
Supplemental Material for Risk of Inguinal Hernia Repair Following Laparoscopic Living Donor Nephrectomy: A Population-Based Cohort Study by Rhiannon Lyons, Eric McArthur, Liane S. Feldman, Ngan Lam, Kyla L. Naylor, Chris Nguan, Doug Quan, Alp Sener, Jessica M. Sontrop, Amit X. Garg in Canadian Journal of Kidney Health and Disease.
Supplemental Material
Supplemental Material - Risk of Inguinal Hernia Repair Following Laparoscopic Living Donor Nephrectomy: A Population-Based Cohort Study
Supplemental Material for Risk of Inguinal Hernia Repair Following Laparoscopic Living Donor Nephrectomy: A Population-Based Cohort Study by Rhiannon Lyons, Eric McArthur, Liane S. Feldman, Ngan Lam, Kyla L. Naylor, Chris Nguan, Doug Quan, Alp Sener, Jessica M. Sontrop, Amit X. Garg in Canadian Journal of Kidney Health and Disease.
Footnotes
Acknowledgments
The authors acknowledge that the data used in this study were provided by the Trillium Gift of Life Network (Ontario Health), 2023; Toronto, Ontario. The researchers’ interpretations and statements in this publication are those of the researcher only and not those of Trillium Gift of Life Network (Ontario Health). We thank IQVIA Solutions Canada Inc. for use of their Drug Information File.
Ethical Considerations
ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from REB review. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Consent for Publication
All authors consent to the publication of this study.
Author Contributions
All authors participated in the research design, data analysis, and performance of the research. RL drafted the manuscript and all authors contributed to the completion of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a foundation grant awarded to Dr. Garg from the Canadian Institutes of Health Research (funding reference number 148377). Dr. Garg is supported by the Kay Family Chair in Transformational Kidney Care. Dr. Naylor is supported by a Health System Impact Embedded Early Career Researcher Award from the Canadian Institutes of Health Research. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from the Canadian Institutes of Health Research. The research was conducted by members of the ICES Kidney, Dialysis, and Transplantation team, at the ICES Western facility. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by: Canadian Institute for Health Information and the Ontario Ministry of Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Parts of this material are based on data and information provided by Ontario Health (OH). The opinions, results, view, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of OH. No endorsement by OH is intended or should be inferred.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data set from this study is held securely in coded form at ICES. Although legal data sharing agreements between ICES and data providers (for example, health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() (e-mail,
(e-mail,
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.