
Abstract
Background
Guidelines for anemia management in chronic kidney disease (CKD) adopted a conservative approach in response to landmark clinical trials demonstrating lack of benefit and potential harm associated with higher hemoglobin targets. Although the findings have been applied to all CKD populations, the concordance between trial populations and those being treated in clinical practice has not been well described.
Objective
We sought to evaluate trends in hemoglobin distribution and erythropoiesis stimulating agent (ESA) use among adult patients with CKD, and compare their characteristics to those of participants from landmark hemoglobin target trials.
Design
Retrospective observational cohort study.
Setting
A provincial clinical information system was used to identify patients with CKD under the care of a nephrologist in British Columbia between April 1, 2007 and March 31, 2018.
Patients
Adult patients (over 18 years) with estimated glomerular filtration rate (eGFR) less than 45 mL/min/1.73m2 and a minimum of three hemoglobin values during follow-up. Patients were censored if they left the province, died, or started kidney replacement therapy.
Measurements
Hemoglobin was measured in grams per litre (g/L) and treated as both a continuous and categorical variable. ESA use was defined as the proportion of patients who received at least one prescription for ESA therapy. The dose of ESA was quantified as an average monthly dose of epoetin alfa or darbepoetin alfa.
Methods
Descriptive statistics were used to compare characteristics of patients in the study population to those of trial participants including Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT), Correction of Hemoglobin and Outcomes in Renal Insufficiency (CHOIR), and Cardiovascular Risk Reduction by Early Anemia Treatment with Epoetin Beta trial (CREATE). Polytomous logistic regression was used to estimate odds ratios (OR) of different hemoglobin levels across cohort years. The model was adjusted for age, sex, race, comorbid conditions, eGFR, proteinuria, etiology of CKD and iron parameters.
Results
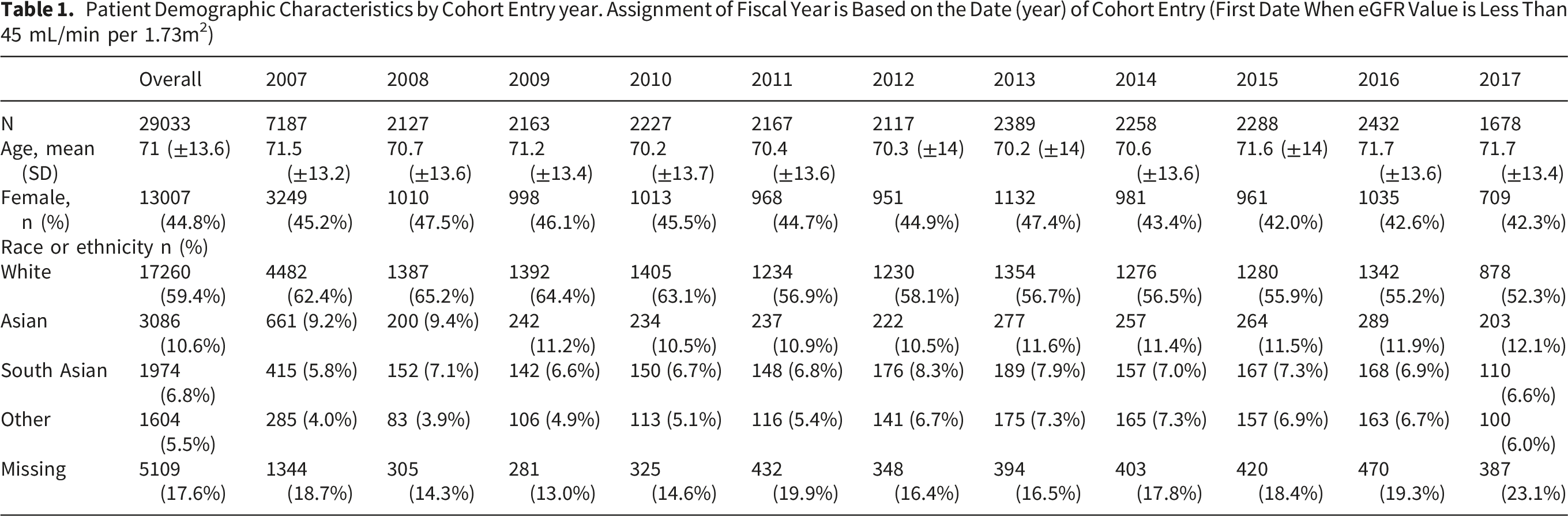
A total of 29,033 patients were included in the analysis (mean age 71 years, 45% female, median eGFR 29 mL/min/1.73m2). Average hemoglobin declined from 122 g/L in 2007 to 112.9 g/L in 2017 with a reduction in ESA use from 35% to 18%. The likelihood of patients having a hemoglobin below 90 g/L (versus 110-124 g/L) increased progressively over time (OR 5.3 in 2008; OR 16.2 in 2017). The proportion of patients meeting inclusion criteria for landmark trials ranged from 9% (TREAT) to 27% (CHOIR). Compared to trial participants, the study population had less comorbidities and received lower doses of ESA therapy.
Limitations
Measurement of hemoglobin may have been subject to confounding by indication, for example due to a bleeding episode. Physicians may have elected not to treat certain patients with ESA therapy, introducing selection bias. Data regarding blood transfusions were not available.
Conclusions
Despite a minority of patients meeting criteria for prior hemoglobin target trials, the universal adoption of guidelines favoring a conservative approach to anemia has culminated in a higher likelihood of patients experiencing severe anemia. The implications of this, particularly patient-reported outcomes, warrant further investigation.
Introduction
Anemia is a well-recognized complication of advanced chronic kidney disease (CKD) and is associated with fatigue and reduced quality of life. 1 Anemia is also associated with adverse clinical outcomes including heart failure, left ventricular hypertrophy, and increased requirement for blood transfusion.2,3 The optimal management of anemia, weighing risks versus benefits of treatment with erythropoiesis stimulating agents (ESA), in patients with CKD remains an area of controversy.
A series of randomized controlled trials conducted in the 1990s and 2000s, including Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT), Cardiovascular Risk Reduction by Early Anemia Treatment with Epoetin Beta trial (CREATE), and Correction of Hemoglobin and Outcomes in Renal Insufficiency (CHOIR), sought to identify an optimal hemoglobin target with the use of ESA therapy in patients with CKD.4-8 These trials were conducted predominantly in the United States, and trial participants had a high burden of comorbidities. Although these trials hypothesized that a higher hemoglobin target would benefit patients by reducing cardiovascular events, participants in the intervention arms experienced a higher rate of adverse outcomes including stroke, vascular access thrombosis, and cancer-specific and all-cause mortality. As a result of these safety concerns, the Kidney Disease Improving Global Outcomes (KDIGO) 2012 guidelines recommend against using ESA to intentionally increase hemoglobin above 130 g/L and suggest a more conservative hemoglobin target of between 90 g/L and 115 g/L in patients with CKD receiving ESA therapy. 9 The upper bound of this target range was informed by the aforementioned target hemoglobin trials; however, there is a paucity of evidence to guide the lower bound of this target range.
These trials have had a profound impact on the management of anemia in patients with kidney disease. In the United States, the use of ESA therapy declined abruptly in 2011 following a black box warning regarding potential harm associated with ESA, and the introduction of a bundling funding policy for patients receiving dialysis which removed incentives for ESA prescribing.10,11 In European countries, where prescribing of ESA was not tied to the same market forces, it was evident that a decline in ESA use was occurring prior to the publication of TREAT in 2009.12,13 In Canada, the proportion of patients starting dialysis with severe anemia (a hemoglobin value below 80 g/L) increased from 8% in 2007 to 17% in 2015. 14 Outside of dialysis registries, there is comparatively little data regarding the downstream impact of target hemoglobin trials on the management of anemia among patients with varying severity of CKD. Furthermore, it is largely unknown how contemporary patients with CKD compare to participants from those trials, especially in terms of the burden of comorbidities which could limit the effectiveness of ESA therapy and/or contribute to adverse events in people receiving ESA therapy.
In a population-level cohort of patients with non-dialysis CKD in British Columbia, Canada, we sought to compare the characteristics of this contemporary population to those of patients recruited to prior target hemoglobin trials, and to evaluate trends in anemia management over time.
Methods
Study Design, Setting and Participants
This was a population-level, retrospective cohort study of adult patients (>18 years) with non dialysis CKD under the care of nephrologists in British Columbia (BC). Since 2000, all patients undergoing nephrology care in the province have been prospectively captured in a province-wide clinical information system (PROMIS). The present study included patients registered in PROMIS between April 1st, 2007 and March 31st, 2018 whose estimated glomerular filtration rate (eGFR) was less than 45 mL/min per 1.73m2. The time period was chosen because it spanned the practice-changing TREAT study (published in 2009), the release of KDIGO anemia guidelines in 20127,9 and the post-guideline period. The eGFR threshold of 45 mL/min per 1.73m2 was chosen because the development of anemia above this level of eGFR would more likely be due to causes other than CKD. Prevalent patients who were already registered in PROMIS at the beginning of the observation period entered the cohort on April 1st, 2007. Beyond this date, patients entered the cohort on the first date that their eGFR was below 45 mL/min per 1.73m2. Included patients required a minimum of three measurements of hemoglobin from the date of cohort entry until the end of follow up, which was defined as death, loss to follow up, renal replacement therapy (dialysis or transplant), or study end date (Mar 31, 2018) and were assigned a fiscal year based on the first date they met the inclusion criteria for the study. Patients with a history of prior dialysis or kidney transplant were excluded. Patients were censored if they died, left the province, or were initiated on kidney replacement therapy (dialysis or kidney transplantation). The study was approved by the Research Ethics Board of the University of British Columbia with waived patient consent (H19-00060).
Data Sources
The PROMIS database collects patient-level information from clinical encounters, pharmacy prescriptions, dialysis and transplantation events, and laboratory results for all registered patients. The database also captures medication data including the type, dose and frequency of ESA and iron supplementation. Data completeness for laboratory data and accuracy of ESA prescriptions in PROMIS are reported regularly as a data quality indicator. Blood transfusion is not consistently captured in PROMIS; therefore, this outcome was not assessed.
Exposure
The exposure variable in this study was year of anemia management between 2007 and 2017. Incident patients for each year comprised of those newly registered in the cohort (with eGFR < 45 mL/min/1.73m2) during that fiscal year (from April 1 to March 31). For example, if a patient joined the cohort between April 1, 2008, and March 31, 2009, they were considered an incident patient for 2008. Prevalent patients included all active patients in the cohort during a specific year, including both new and existing patients. For example, if a patient joined the cohort in a previous year (e.g., between April 1, 2007, and March 31, 2008) and was still an active patient in the current year, they were considered a prevalent patient for the current year.
Outcome
Hemoglobin was measured in grams per litre (g/L). If a patient had multiple hemoglobin values in the same fiscal year (their cohort entry year), their mean hemoglobin was used for that year. In descriptive analyses, hemoglobin was treated as both a continuous variable and categorized as follows: <80, 80-89, 90-99, 100-109, 110-119, 120-129 and ≥130 g/L. ESA use was defined as the proportion of patients who received at least one prescription for ESA therapy. The dose of ESA was quantified as an average monthly dose of either epoetin alfa or darbepoetin alfa.
Covariates
Demographic variables included age at cohort entry, sex and self-reported race/ethnicity. Clinical variables included the presence of diabetes, hypertension, ischemic heart disease, congestive heart failure, stroke or transient ischemic attack, peripheral vascular disease, dyslipidemia, smoking history, malignancy, and gastrointestinal disease. The etiology of CKD was also included. Clinical variables were captured in the same way across successive years of follow up. Laboratory parameters included eGFR, urine albumin to creatinine ratio (uACR, in mg/mmol), transferrin saturation (as a percentage) and ferritin (in µg/L).
Statistical Analysis
Continuous variables are presented as mean (standard deviation (SD)) or median (interquartile range [IQR]) as appropriate. Frequencies are reported as percentages. Patient baseline characteristics were determined at the time of cohort entry. We compared baseline demographic and clinical characteristics of patients overall and stratified by cohort entry year. Polytomous logistic regression was used to estimate the adjusted odds ratios of different hemoglobin levels across cohort years. 15 This model was fitted using 5 hemoglobin categories (<90, 90-99, 100-109, 110-124, >=125 g/L) and selecting 110-124 g/L as the reference category. The model was adjusted for age, sex, race, comorbid conditions, eGFR, uACR, etiology of CKD and iron parameters. The statistical analysis was conducted using SAS v9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Study Population
Patient Demographic Characteristics by Cohort Entry year. Assignment of Fiscal Year is Based on the Date (year) of Cohort Entry (First Date When eGFR Value is Less Than 45 mL/min per 1.73m2)
Patient Clinical Characteristic by Cohort Entry year. Assignment of Fiscal Year is Based on the Date (year) of Cohort Entry (First Date When eGFR Value is Less Than 45 mL/min)
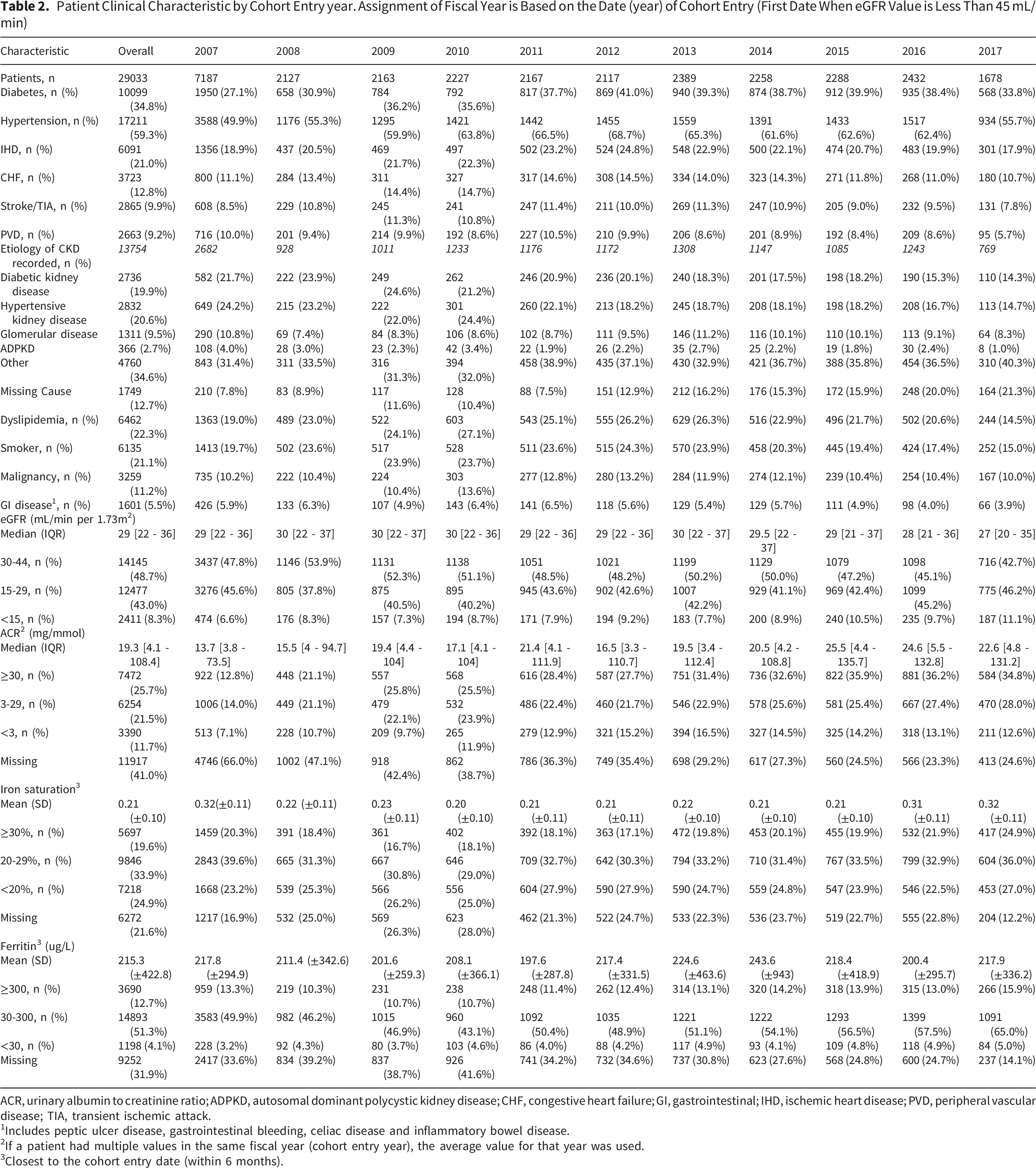
ACR, urinary albumin to creatinine ratio; ADPKD, autosomal dominant polycystic kidney disease; CHF, congestive heart failure; GI, gastrointestinal; IHD, ischemic heart disease; PVD, peripheral vascular disease; TIA, transient ischemic attack.
1Includes peptic ulcer disease, gastrointestinal bleeding, celiac disease and inflammatory bowel disease.
2If a patient had multiple values in the same fiscal year (cohort entry year), the average value for that year was used.
3Closest to the cohort entry date (within 6 months).
Comparison of BC Cohort to Previous Clinical Trial Populations
Comparison of BC Cohort to Landmark Anemia Trials
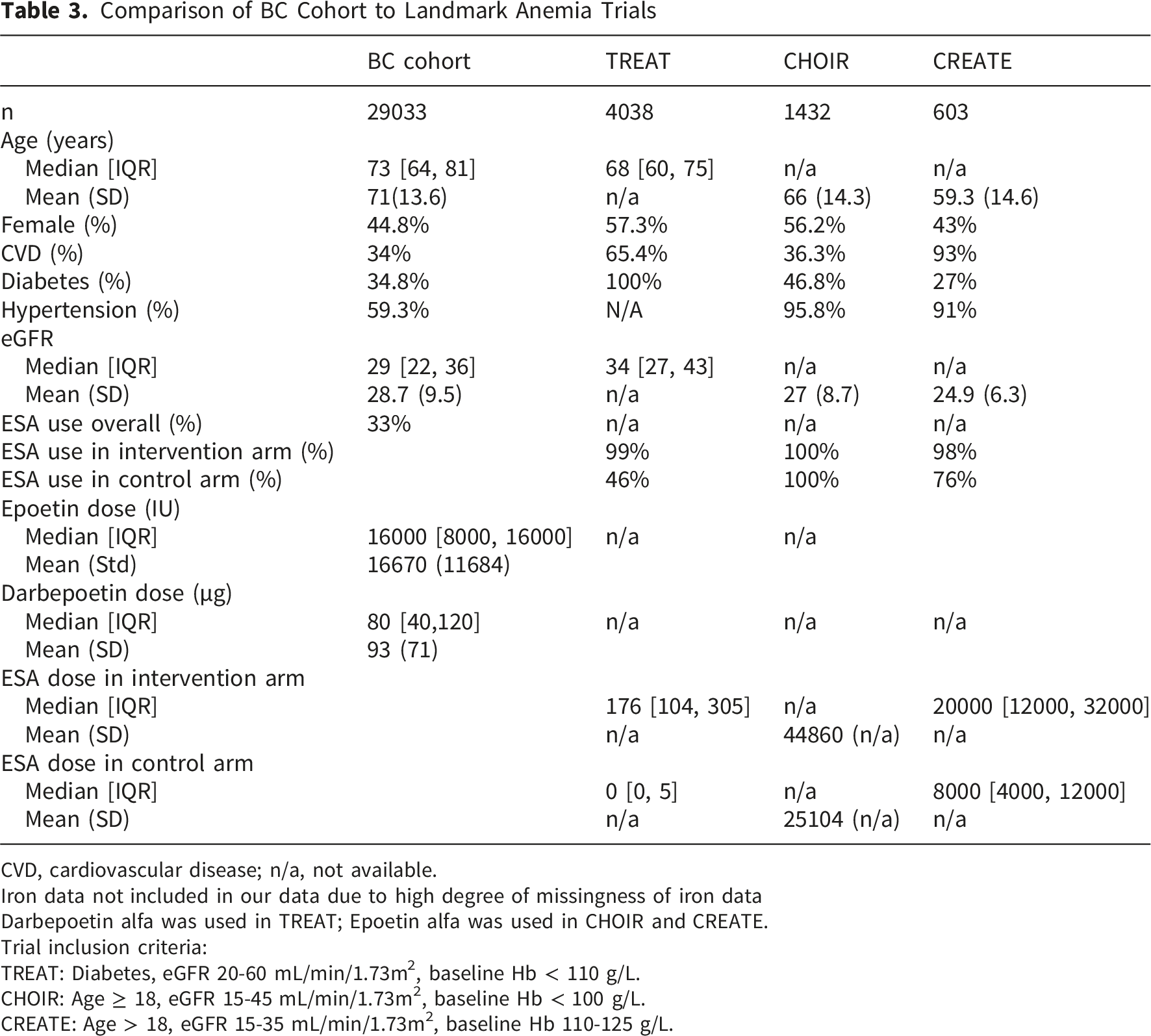
CVD, cardiovascular disease; n/a, not available.
Iron data not included in our data due to high degree of missingness of iron data
Darbepoetin alfa was used in TREAT; Epoetin alfa was used in CHOIR and CREATE.
Trial inclusion criteria:
TREAT: Diabetes, eGFR 20-60 mL/min/1.73m2, baseline Hb < 110 g/L.
CHOIR: Age ≥ 18, eGFR 15-45 mL/min/1.73m2, baseline Hb < 100 g/L.
CREATE: Age > 18, eGFR 15-35 mL/min/1.73m2, baseline Hb 110-125 g/L.
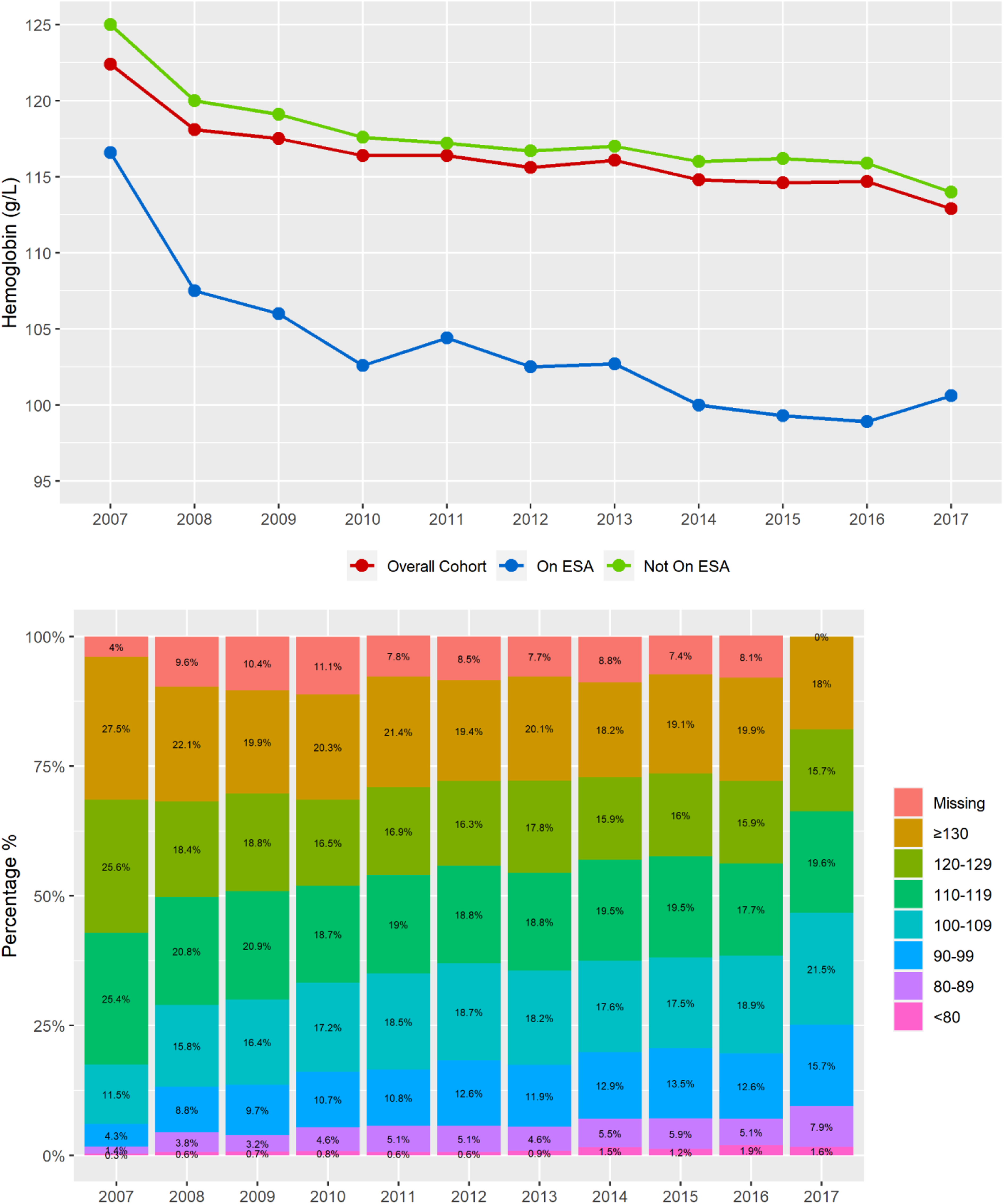
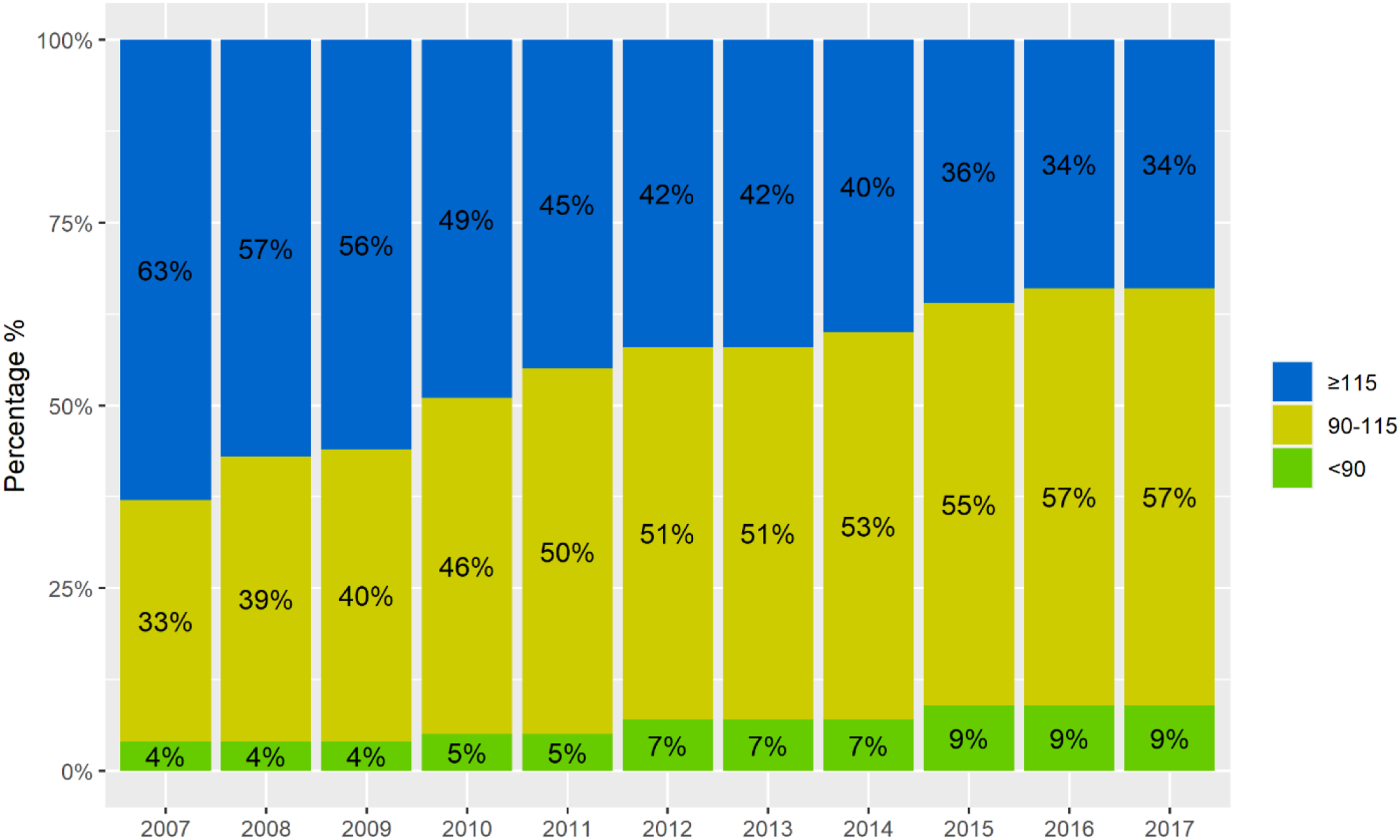
Mean hemoglobin of incident patients in each year overall and stratified by ESA use(top panel) and the proportion of patients in each hemoglobin category per year of the study period (bottom panel)
Hemoglobin Distribution Over Time
The mean hemoglobin among incident patients decreased from 122 g/L in 2007 to 112.9 g/L in 2017, with the most rapid decline occurring between 2007 and 2010 (Figure 1). The proportion of patients with mean hemoglobin below 100 g/L increased from 6% to 25% during the study period. Furthermore, the proportion of patients with mean hemoglobin below 90 g/L increased from 1.7% to 9.5%. Among patients receiving ESA therapy, the mean hemoglobin decreased from 117 g/L in 2007 to 100 g/L in 2014, then remained stable thereafter (Figure 1). In these patients, the proportion of patients with a hemoglobin value below 100 g/L increased from 8.2% in 2007 to 50% in 2017, and the proportion with a hemoglobin value below 90 g/L increased from 2.8% to 25.8% (Supplementary Table 1). The likelihood of having a hemoglobin below 90 g/L increased progressively over time (Figure 2). Relative to 2007, patients in 2008 had a higher adjusted odds of having a hemoglobin < 90 g/L rather than 110-124 g/L (OR, 5.3; 95% CI, 3.8-6.9), and patients in 2017 had a markedly higher adjusted odds of hemoglobin < 90 g/L rather than 110-124 g/L (OR, 16.2; 95% CI, 12.2-21.5). The likelihood of having a hemoglobin below 90 g/L per year of follow-up. Estimates are odds ratios (95% confidence intervals) from a polytomous regression model. The reference group is hemoglobin 100-124 g/L. The model was adjusted for age, sex, race, comorbid conditions, eGFR, uACR, etiology of CKD, and iron parameters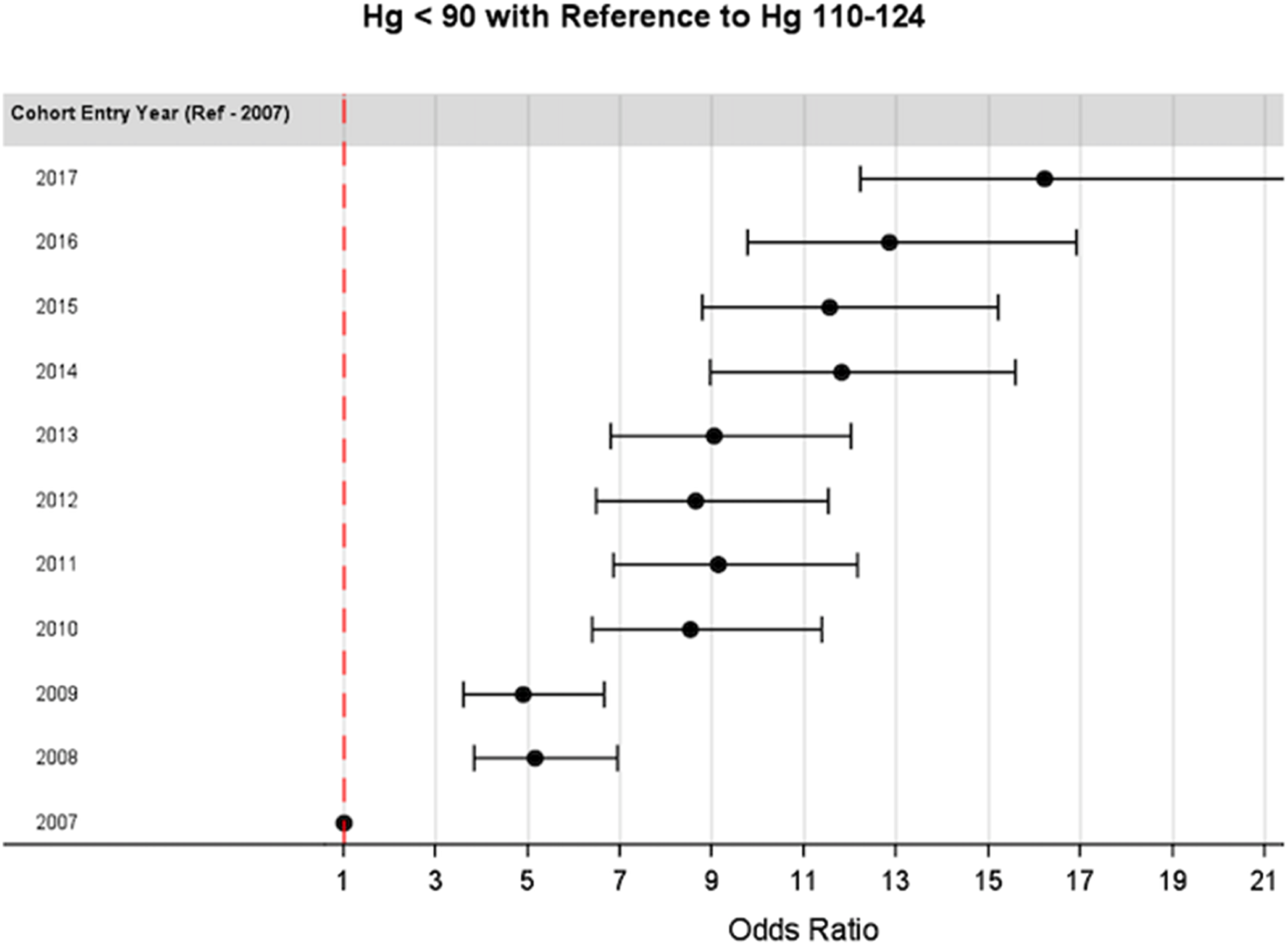
Figure 3 demonstrates the mean yearly hemoglobin in prevalent patients in the cohort within subgroups by sex, age category, eGFR category, etiology of CKD, and comorbid conditions. Females had lower mean hemoglobin compared to males, and hemoglobin decreased progressively over time in both sexes. Older patients had lower hemoglobin values but patients in all age categories experienced a decline in hemoglobin during the study period. Patients with eGFR of 30-44 mL/min per 1.73m2 and eGFR of 15-29 mL/min per1.73m2 experienced a decline in hemoglobin over time, while patients with eGFR < 15 mL/min per 1.73m2 had stable hemoglobin throughout the study period. Patients with autosomal dominant polycystic kidney disease tended to have the highest hemoglobin values, and patients with diabetic kidney disease tended to have the lowest values. Although mean hemoglobin levels differed by etiology of CKD, all groups showed a decline in hemoglobin values over time. This pattern was also consistent across comorbidity subgroups including diabetes, ischemic heart disease, and congestive heart failure. Mean yearly hemoglobin in prevalent patient subgroups by years, including sex (top left panel), age (top right panel), eGFR (middle left panel) and etiology of CKD (middle right panel). The bottom panel shows mean hemoglobin at 3 points of the study: 2007 (beginning), 2012 (mid-point), and 2017 (end) in subgroups of comorbidity including diabetes, ischemic heart disease (IHD), and congestive heart failure (CHF)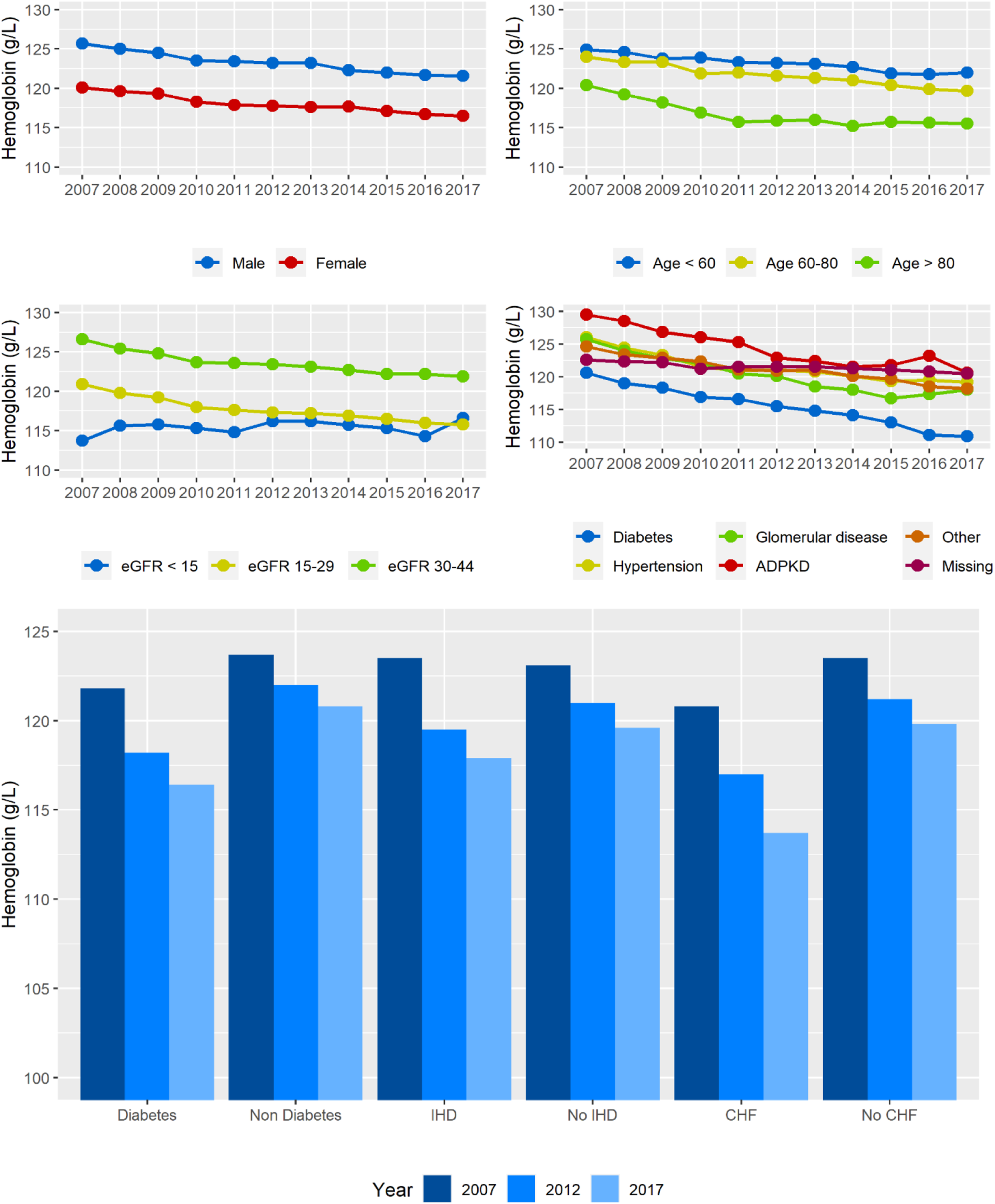
Erythropoiesis Stimulating Agent Use
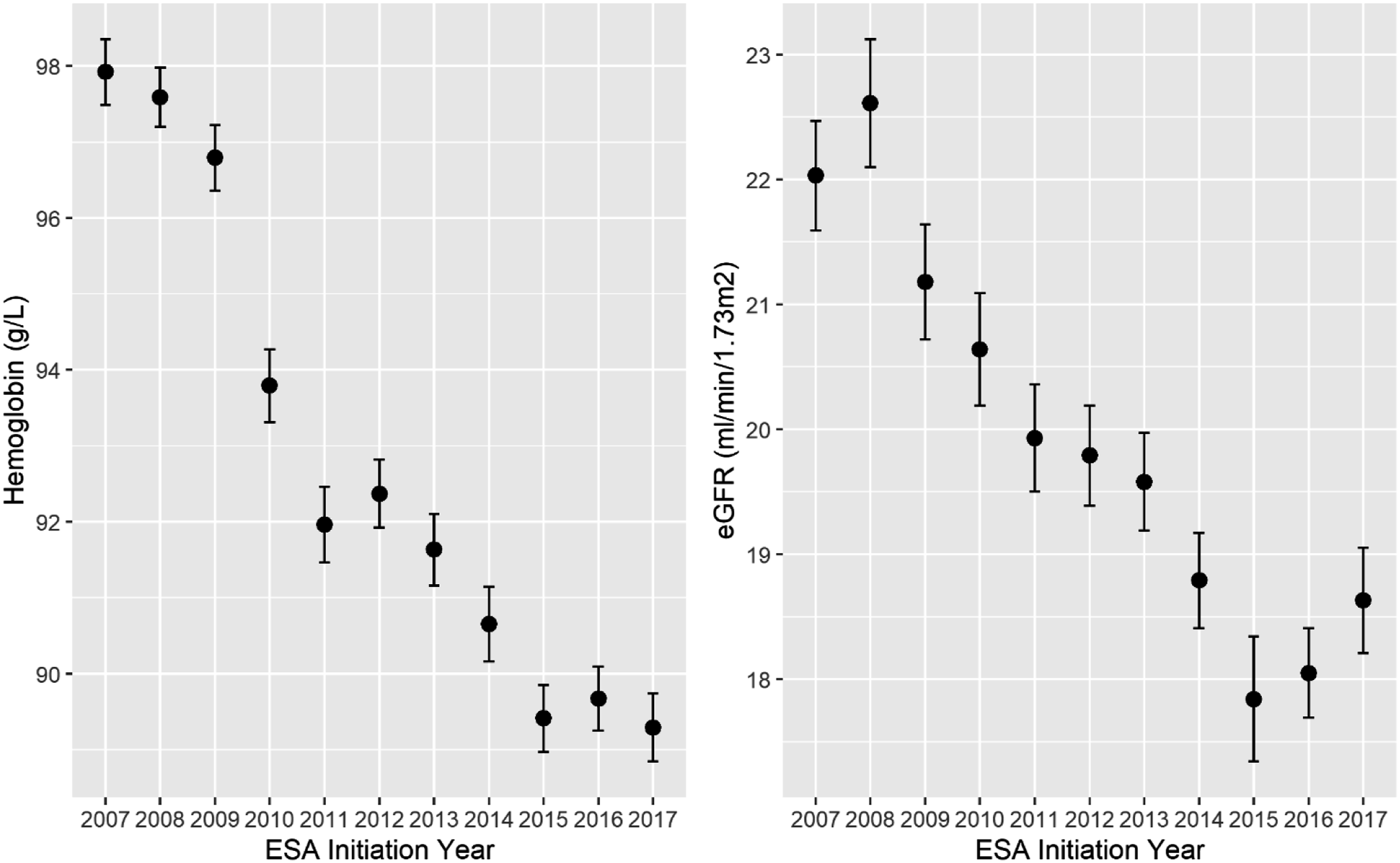
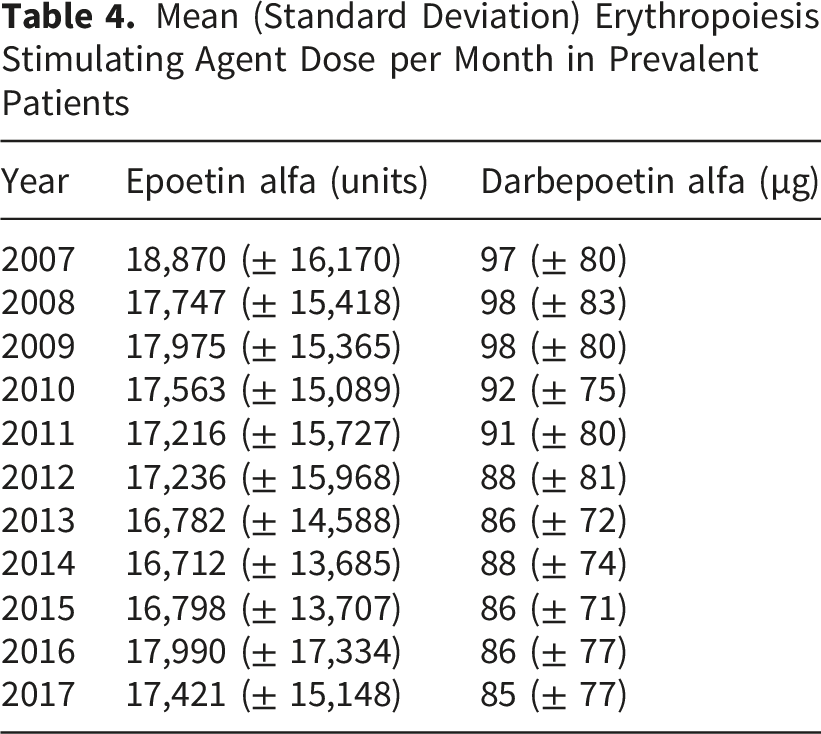
The proportion of patients receiving ESA therapy decreased from 34.8% in 2007 to 17.1% in 2014, with a similar pattern in both prevalent and incident patients (Figure 4). Mean hemoglobin at the time of ESA initiation declined from 98 g/L to 89 g/L over the study period, and mean eGFR at ESA initiation also decreased from 22 to 19 mL/min/1.73m2 between 2007 and 2014 before plateauing (Figure 5). The proportion of patients receiving ESA who achieved the recommended hemoglobin range of 90-115 g/L increased from 33% to 57% between 2007 and 2017 (Figure 6). This was driven by progressively fewer patients having a hemoglobin above 115 g/L. Of those with hemoglobin values below 90 g/L, 50.8% were on ESA therapy in 2007 and this declined to 22% in 2017 (Supplementary Table 2). There was a modest reduction in average monthly dose of ESA therapy over time (Table 4). In each year, the mean dose of ESA therapy was lower among incident patients compared to prevalent patients (Supplementary Table 3). Proportion of patients each year receiving ESA therapy. Green indicates incident patients and blue indicates prevalent patients Mean (95% confidence interval) hemoglobin (left panel) and eGFR (right panel) at time of ESA initiation by year in prevalent patients Proportion (%) within the guideline recommended hemoglobin range (90-115 g/L) by year in patients receiving ESA therapy Mean (Standard Deviation) Erythropoiesis Stimulating Agent Dose per Month in Prevalent Patients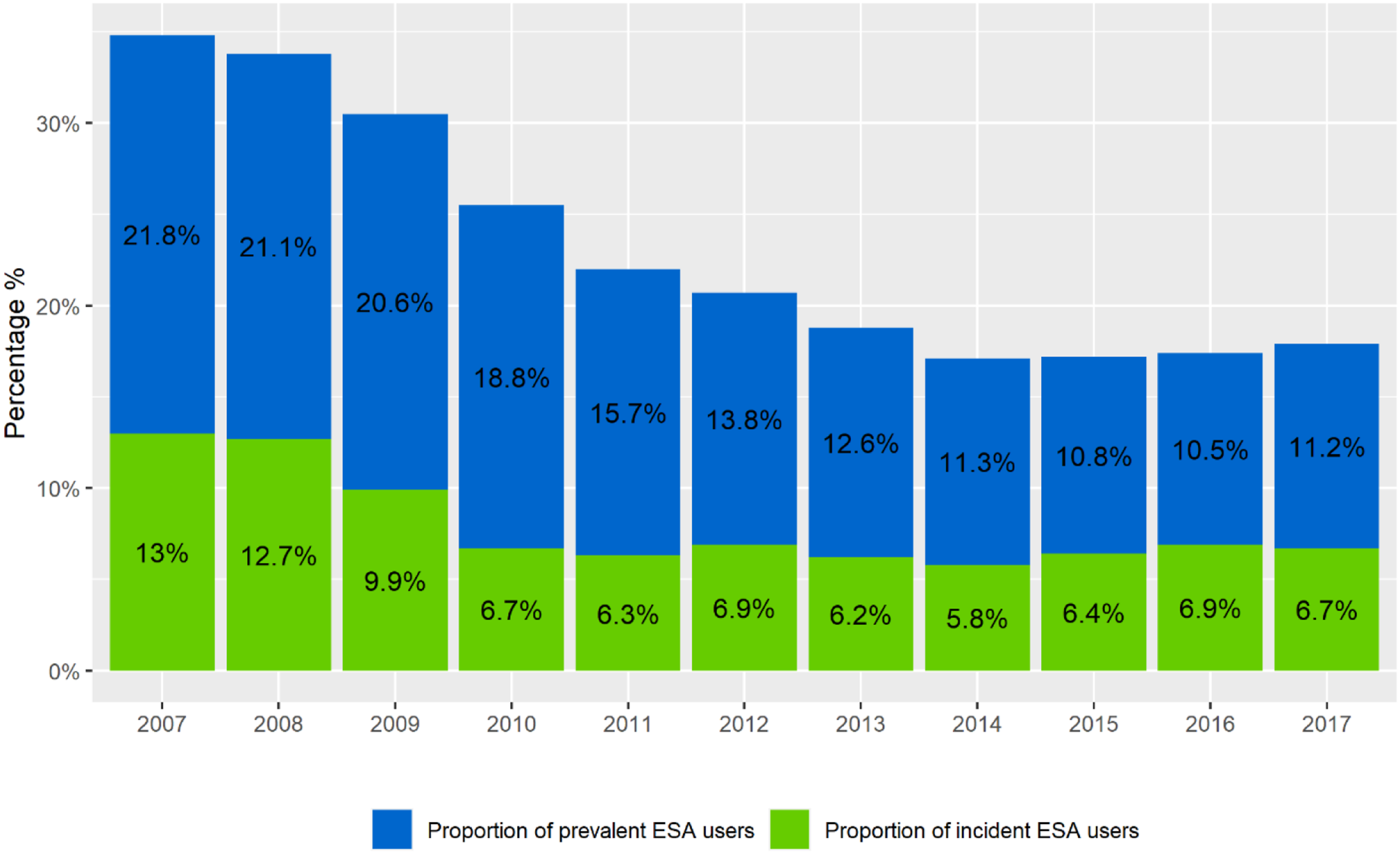
Discussion
We examined ESA and hemoglobin trends in a large cohort of CKD patients managed by nephrologists in a universal healthcare system in BC, Canada, between 2007 and 2017, a period encompassing practice-changing anemia trials and changes to clinical practice guidelines. We found that hemoglobin values steady declined over this timeframe across all demographic and clinical subgroups of patients with CKD, with the most pronounced decline occurring between 2007 and 2010. Individuals in 2017 were 16 times as likely to experience a hemoglobin value below 90 g/L compared to the reference category of 110-124 g/L. Among patients receiving ESA therapy, the proportion of patients who experienced a hemoglobin value below 90 g/L increased almost 10-fold from 2.8% in 2008 to 25.8% in 2017. Although clinical guidelines were largely informed by pivotal trials published between 2006 and 2009, only a minority of patients in BC would have met inclusion criteria for those clinical trials, and the doses of ESA used in BC were comparatively much lower. Taken together, these findings suggest that the adoption of a conservative approach to anemia therapy has contributed to an increasing prevalence of severe anemia despite the fact that the clinical trials that drove this change were not necessarily generalizable to the broad population of patients living with CKD.
Our findings of declining ESA use and hemoglobin values among patients with CKD are consistent with previous studies in the USA and Europe that have shown a decline in ESA use, particularly since the publication of the TREAT study.11-13 In the US, patients with CKD KDIGO stages 3 and 4 were found to have a 38% and 22% decline in ESA use between 2007 and 2011. 11 A Swedish retrospective cohort study of CKD non-dialysis patients showed that ESA use declined from 25.9% to 18.6% between 2008 and 2013. 12 Our analysis adds to these prior studies by extending the timeline to facilitate a more comprehensive examination of trends in practice pattern over time. Patients in BC during the timeframe of the study were managed by nephrologists within a universal healthcare system, such that all patients had an equal opportunity to receive the drug which was not influenced by billing incentives as may have been the case in US patient populations. Furthermore, we assessed anemia management trends within clinically relevant subgroups. Hemoglobin was typically lower in females, in those with lower values of eGFR, and varied by etiology of CKD. This is in keeping with a previous study of 58,613 CKD patients across 21 cohorts that demonstrated substantial variation in hemoglobin distribution by region, sex, eGFR and etiology of CKD. 16 These findings underscore the importance of considering an individualized approach to anemia management and the potential limitations of using a single threshold to guide clinical care.
Like in other CKD populations, anemia practice in BC changed to prevent potential harm through the targeting of higher hemoglobin values based on landmark trials.5-7 By comparing the BC population to the trial populations from target hemoglobin trials, we were able to demonstrate that the majority of patients with CKD would not have met eligibility criteria for those trials, and that ESA doses prescribed by nephrologists in BC were considerably lower than the doses used in both the higher and lower hemoglobin target groups from the trials. The lower doses used are important because post hoc analyses of TREAT and CHOIR suggested that ESA dose and responsiveness, as opposed to the achieved hemoglobin itself, were associated with the observed higher risk of cardiovascular disease and stroke in those studies.17,18 Patients in the BC cohort also had a lower burden of comorbidities such as hypertension and cardiovascular disease. Therefore, by using considerably lower doses of ESA therapy in a less comorbid population, it is reasonable to question whether a causal association between ESA and adverse clinical outcomes such as stroke would necessarily have been observed in this population. In support of this hypothesis, a previous study of patients starting dialysis in Canada did not show a reduction in stroke incidence between 2007 and 2015 despite progressively lower hemoglobin levels and ESA use over time. 14 A recent multinational longitudinal study of anemia management in patients with CKD not requiring dialysis between 2013 and 2018 also reported low treatment rates of anemia among patients with hemoglobin values below 100 g/L, with only 28% of these patients being on ESA. 19 The clinical significance of prolonged exposure to lower hemoglobin levels warrants further study in this patient population.
It is highly unlikely that the outstanding questions about ESA therapy will be answered in a future clinical trial. The discovery of a novel alternative treatment in the form of hypoxia-inducible factor-prolyl hydroxylase inhibitors (HIF-PHI) has not sufficiently addressed the concerns about ESA therapy because these trials have not demonstrated a superior safety profile compared to ESA therapy.20,21 Patients will continue to be faced with treatment decisions based on a trade-off of potential benefit (transfusion avoidance, symptom improvement) and harm (access thrombosis, stroke and cancer-associated risks). There is, therefore, a critical unmet need to evaluate patient-centred outcomes and patient experience outcomes so that patients have a full understanding of this trade-off. A recent example of such an approach was the use of plasma exchange in the treatment of anti-neutrophil cytoplasmic antibody (ANCA) associated vasculitis in which recommendations for treatment were underpinned by considering whether a patient would place a higher value on avoiding kidney failure (the potential benefit of plasma exchange) or avoiding serious infections (the potential risk of plasma exchange) based on their risk of both outcomes. 22 Importantly, the guideline panel incorporated the perspectives of patients and caregivers, a strategy endorsed by the Standardized Outcomes in Nephrology initiative for the evaluation of treatments in people living with kidney disease. A similar approach could be employed in decision-making about anemia therapy in CKD. 23
Strengths of this study include its large sample size and the use of a detailed provincial registry containing data on all patients with CKD managed by nephrologists who had access to standardized anemia protocols. The database captures all patients with kidney disease receiving ESA prescriptions, as funding for these medications in BC is tied to being enrolled in the renal program. Our study has a number of limitations. ESA utilization was limited to prescription data and it is possible that dose or frequency changes were made outside of those prescriptions. Similarly, physicians may have elected not to prescribe ESA to specific patients based on anticipated risk of an adverse outcome such those with prior history of malignancy. It is possible that hemoglobin values were measured for reasons other than CKD monitoring and may thus have been subject to confounding by indication, for example in the context of a bleeding episode. Mean hemoglobin was used if a patient had multiple hemoglobin values in the same year to limit misclassification from using only one value and to provide a more accurate reflection of an individual’s anemia status; however, this does come with the limitation of losing granularity including short term temporal hemoglobin changes. Given the rising incidence of diabetes in Canada it was unexpected to observe a decreasing proportion of diabetic kidney disease over the later years of the cohort and we suspect this was related to a reporting issue leading to misclassification of etiology. This study is limited to British Columbia in Canada and may not be generalizable to other regions, especially those without a universal healthcare system or without standardized anemia management in CKD. This study describes hemoglobin management trends in but does not address potential impact of these trends on clinical outcomes. Finally, there were missing data for iron parameters over time and blood transfusion events were not included due to inconsistent capture of this outcome in the database.
Conclusion
Despite a minority of contemporary patients with CKD meeting inclusion criteria for prior hemoglobin target trials, the widespread adoption of a conservative approach following the publication of those trials has culminated in a progressively higher likelihood of patients experiencing severe anemia. The implications of this, both in terms of patient-reported outcomes and clinical outcomes such as the frequency of blood transfusions warrant further investigation.
Supplemental Material
Supplemental Material - Evaluation of Anemia Management in a Contemporary Population of Patients With Chronic Kidney Disease in Canada Since the Publication of Target Hemoglobin Trials: A Retrospective Observational Cohort Study
Supplemental Material for Evaluation of Anemia Management in a Contemporary Population of Patients With Chronic Kidney Disease in Canada Since the Publication of Target Hemoglobin Trials: A Retrospective Observational Cohort Study by Peter Birks, Mark Canney, Ognjenka Djurdjev, Dilshani Induruwage, Mohammad Atiquzzaman, Adeera Levin in Canadian Journal of Kidney Health and Disease
Supplemental Material
Supplemental Material - Evaluation of Anemia Management in a Contemporary Population of Patients With Chronic Kidney Disease in Canada Since the Publication of Target Hemoglobin Trials: A Retrospective Observational Cohort Study
Supplemental Material for Evaluation of Anemia Management in a Contemporary Population of Patients With Chronic Kidney Disease in Canada Since the Publication of Target Hemoglobin Trials: A Retrospective Observational Cohort Study by Peter Birks, Mark Canney, Ognjenka Djurdjev, Dilshani Induruwage, Mohammad Atiquzzaman, Adeera Levin in Canadian Journal of Kidney Health and Disease
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.