
Abstract
Background
Many living kidney donors (LKDs) describe their evaluation process as the most difficult part of donating a kidney. The process is often lengthy, complex and inefficient, frequently requiring several months to complete. A more efficient and donor-centered evaluation may improve LKD experiences, reduce attrition, and encourage more individuals to donate.
Methods
We employed a Delphi approach to define and select metrics of a high-quality LKD evaluation. Four multidisciplinary working groups were created in which LKDs (n=8), healthcare professionals (n=11), and administrators (n=3) collaborated to develop evidence and experience informed recommendations.
Results
This work culminated in a national consensus conference held virtually in September 2024, which brought together over 100 LKDs, nurses, nephrologists, surgeons, researchers, and representatives from transplant organizations. Of the 42 recommendations evaluated through the e-Delphi process, 35 achieved consensus (≥75% agreement) across four domains. Ninety-two percent were supported by moderate-quality evidence, while 8% had no supporting evidence, reflecting the limited empirical data available for several aspects of donor evaluation processes. The recommendations clustered into four overarching themes included: (1) increasing donor numbers and evaluation efficiency (e.g., eligibility for donation determined within three to six months), (2) enhancing program resources and donor reimbursement (e.g., metrics on donor financial neutrality), (3) ensuring a donor-centered evaluation process (e.g., donor-centered metrics such as donor satisfaction), and (4) promoting consistency and evidence-based practice across programs (e.g., consistent evaluation nationally).
Conclusion
Collectively, these recommendations provide a framework to guide quality improvement, benchmarking, and policy development, with implications for strengthening the LKD evaluation process worldwide.
1. Introduction
The best treatment option for many patients with kidney failure is a kidney transplant, as it offers patients a longer and better quality of life, at a fraction of the cost of dialysis.1,2 A patient can receive a kidney transplant from a living or deceased donor; however, a transplant from a living donor offers improved patient and graft survival rates.3,4 Unfortunately, there are many barriers to accessing a living donor transplant, including a long and inefficient donor evaluation process.5-9 Donor candidates make several trips to labs or hospitals to complete tests and consultations, and often spend months waiting to hear if they are eligible to donate. 5 The median evaluation time in Canada is 10 months, 10 which can negatively impact work and family life, and reduce the opportunity for pre-emptive kidney transplants. Ultimately, a prolonged evaluation can lead to fewer donors coming forward to donate and fewer living kidney donor transplants. 8 It is important to note that this estimate reflects previously published national data and may represent historical practice, as some transplant programs have recently implemented initiatives aimed at streamlining donor evaluation processes.11,12
In Canada and other countries, living kidney donor (LKD) programs are working to improve the donor evaluation process11-14; however, they have limited guidance on the elements of a high-quality evaluation or on how to measure evaluation performance. A high-quality living donor evaluation may be defined as a comprehensive assessment that ensures donor safety and readiness to donate, while also being timely, efficient, and respectful of the candidate’s preferences.
On September 26, 2024, a virtual consensus conference was held in collaboration with Canadian Blood Services (Canadian organization responsible for coordinating organ donation and transplantation) 15 to define a high-quality LKD evaluation, including metrics.
1.1. Conference Objectives
1) To define a high-quality LKD evaluation that considers the perspectives of living kidney donors, clinicians, and administrators, and aligns with the Institute of Medicine’s (IOM’s) six domains of healthcare quality (Supplementary Table 1).
16
2) To select and define metrics of a high-quality LKD evaluation for program benchmarking and quality improvement initiatives.
2. Methods
This report follows the ACCurate COnsensus Reporting Document (ACCORD) guideline for reporting consensus-based methods in clinical practice (Supplementary Table 2). 17 The focus of the conference was the evaluation of candidates for living kidney donation. The evaluation period was defined to start when a donor candidate first contacts the transplant center about becoming a donor and end when the candidate’s eligibility is determined by the transplant center or the candidate withdraws from the evaluation process. The following two elements were considered out of scope: The preoperative period (starting once donor eligibility is determined, up to the postoperative period) and recipient factors (e.g., a delayed recipient evaluation, which is outside the control of the donor program but may impact the timing of a donor’s evaluation). This study was not prospectively registered, and ethics approval was not required.
A steering committee was established in the summer of 2023, comprising 15 individuals with expertise in LKD evaluation from 9 out of 10 provinces in Canada; members included nephrologists, a clinical nurse leader, living kidney donors, researchers, and healthcare administrators (Supplementary Appendix 1). The committee met twice to plan conference proceedings (Supplementary Appendix 2). All members also participated in the working groups (described below), attended the virtual conference, and participated in the eDelphi consensus panel. An eDelphi exercise was employed to achieve consensus on the recommendations, as its use of anonymity can mitigate the inclination to conform to group dynamics. 18
2.1. Preparatory Research: Overview
Working Groups and Objectives
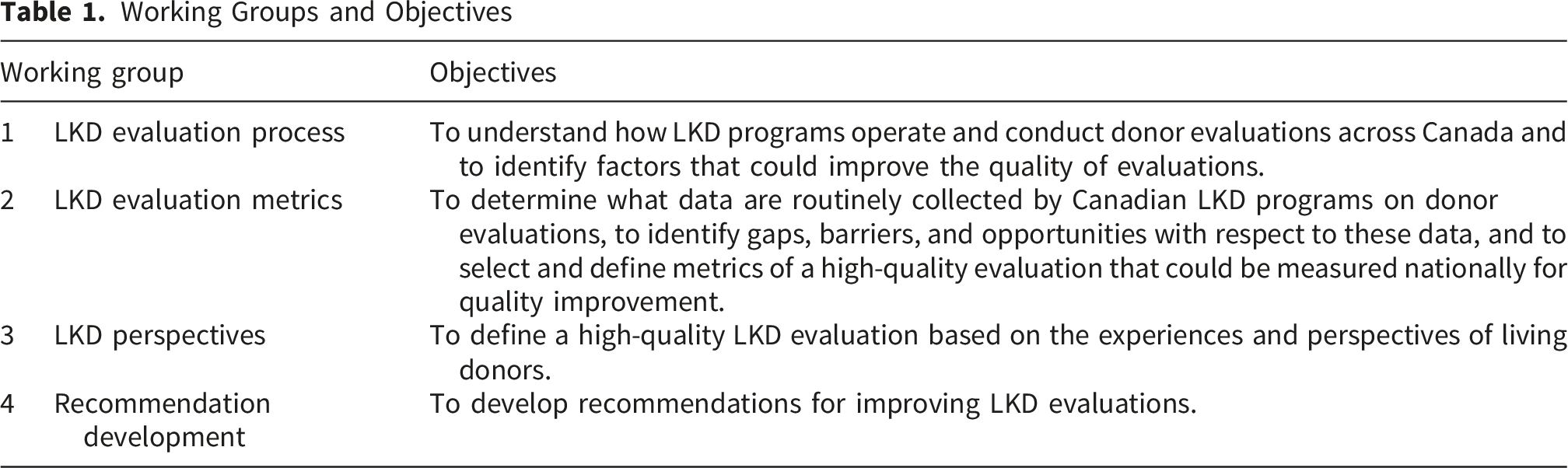
2.1.1. Working Group 1: LKD Evaluation Process
Working group 1 comprised a clinical nurse leader, three nephrologists, and a living kidney donor (Supplementary Appendix 1). Objectives were to understand how Canadian LKD programs operate and conduct donor evaluations, and to identify factors that could enhance the quality of LKD evaluations. To support these objectives, Canadian Blood Services conducted an environmental scan, which included reviewing LKD protocols from 10 out of 26 LKD programs across Canada and collecting information on the evaluation process, including the tests performed, the order of compatibility testing and the allowable number of donors evaluated per recipient (Supplementary Appendix 6). The review of LKD evaluation protocols from 10 LKD programs across Canada revealed considerable variability in how LKD evaluations are conducted among programs (Supplementary Appendix 7). While some tests were universally performed, the order, type, and timing of the tests varied, as did the timing of decisions. For example, some centers begin by testing the candidate’s blood type and HLA, while others do not. Some limit the number of candidates assessed per recipient, and others offer expedited testing and virtual consultations. A lack of evidence supporting certain tests, including cardiac and respiratory testing, was identified. The group noted that the testing burden was substantial, with many candidates required to undergo additional tests even after completing the initial evaluation. The group drafted 25 recommendations (Supplementary Appendix 8).
2.1.2. Working Group 2: LKD Evaluation Metrics
Working group 2 comprised two epidemiologists, a healthcare administrator, and five nephrologists (Supplementary Appendix 1). Objectives were to determine what data were routinely collected by Canadian LKD programs on donor evaluations, to identify gaps, barriers, and opportunities regarding these data, and to select and define metrics of a high-quality evaluation that could be collected nationally for program benchmarking and to support and evaluate quality improvement initiatives. The group reviewed the literature on quality indicators for LKD, 19 including indicators of an efficient evaluation, 20 and considered relevant metrics proposed for national reporting by the Canadian Institute for Health Information. 21 To support these objectives, Canadian Blood Services emailed a survey to 26 living donor coordinators and program managers at LKD programs across Canada. The survey included questions on data routinely collected on donor evaluations, including equity measures (e.g., race), as well as barriers to data collection (Supplementary Appendix 6). Discussions considered factors such as the intended users of the indicators and the feasibility of collecting and reporting data without burdening LKD programs. 22 Recommendations were drafted and anonymously evaluated using an eDelphi process within the group, considering the criteria listed in Supplementary Table 3. The analysis of survey responses from 20 LKD coordinators and program managers across Canada revealed considerable variability in the definitions and collection of measures for LKD evaluations across programs. Definition variability was recognized as a barrier for comparisons between programs. Limited resources for data collection and a lack of information systems to easily collect this information could also impede national data reporting. The group drafted 20 recommendations (Supplementary Appendix 9).
2.1.3. Working Group 3: LKD Perspectives
Working group 3 comprised seven living kidney donors, one nephrologist, and the Kidney Foundation of Canada’s National Director of Programs & Public Policy. The donors were from three provinces, and some had experience donating outside of their home province. Objectives were to define a high-quality LKD evaluation based on the experiences and perspectives of living donors. The group discussed key issues that could improve the quality of LKD evaluations, as well as measures that could be collected nationally, such as donor reimbursement policies and support received during the evaluation process. Seven key areas to enhance the quality of LKD evaluations were identified: (1) providing more guidance throughout the evaluation process; (2) increasing transparency about out-of-pocket expenses and improving reimbursement of out-of-pocket expenses; (3) facilitating more effective communication between donor and recipient teams; (4) offering greater emotional support for the mental well-being of donors, including those deemed ineligible to donate; (5) providing more support for donors in rural and remote areas who often travel much greater distances to complete each evaluation step; (6) reducing the overall burden of the evaluation process, including the duration, number of tests, and visits; and (7) increasing consistency across transplant centers, such as allowing multiple donor candidates versus one. The group drafted 13 recommendations (Supplementary Appendix 10).
2.1.4. Working Group 4: Recommendation Development
Working group 4 comprised the leads and co-leads of working groups 1, 2, and 3. The objectives were to review the recommendations of working groups 1-3 to ensure they fell within the project’s scope. Recommendations that did not reach consensus within the working groups were either revised or removed. In a few instances where similar recommendations were generated by different groups, the recommendations were merged. Working group 4 reviewed 58 recommendations (42 that reached consensus within individual working groups and 16 that did not). Out of the 42 recommendations that reached consensus, 20 were refined for clarity, four were combined with existing recommendations due to redundancy, two were removed (one for being out of scope and one for having a low quality of evidence) and five that initially did not reach consensus were discussed and subsequently included, and one new recommendation was added, resulting in 42 recommendations for evaluation at the consensus conference (Supplementary Appendix 11).
2.2. Delphi Panel Recruitment and Composition
Potential participants for the eDelphi panel were identified based on their expertise and experience with LKD evaluations. The steering committee and Canadian Blood Services created a comprehensive list of invitees to ensure national representation from various professions, including nephrologists, researchers, living kidney donors, nurse coordinators, and health administrators. Canadian Blood Services emailed invitations to invitees, with reminders sent to non-responders. Participation in the conference was deemed informed consent. No compensation was provided for participation.
2.2.1. Conference Proceedings and Assessment of Consensus
At the start of the conference, two living kidney donors shared their experiences with the donor evaluation process, including challenges such as a lengthy evaluation that required extensive travel. The working groups provided an overview of the environmental scan, the survey results, an evidence summary,19-21 and factors and criteria to consider to ensure quality indicators are useful and purposeful (Supplementary Table 3).22,23 Two questions were asked for each recommendation: one regarding consensus and the other on the quality of evidence. Consensus was measured on a 5-point Likert scale (strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree). The consensus threshold was defined a priori as 75% or more of the respondents voting “agree” or “strongly agree” with a recommendation. The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework, in which the quality of evidence is categorized as high, moderate, low, or very low/absent (Supplementary Table 4).24,25 Conference participants rated the evidence quality based on their knowledge of the available scientific evidence rather than a formal systematic review of the literature and their personal and clinical experience. Many of the recommendations related to pragmatic aspects of program organization and quality measurement for which limited empirical evidence currently exists. If participants felt they lacked the necessary knowledge or experience, participants were reminded that it was appropriate to abstain from voting.
The online Delphi process (eDelphi) was administered using the Zoom voting platform, ensuring participant anonymity. Participants could ask questions about the recommendations before voting and suggest rewording to improve clarity. During the voting round, participants indicated that some recommendations were unclear; therefore, these recommendations were rephrased, and about one month after the conference, a link to an online Delphi was sent to participants to complete voting on the revised recommendations. Responses were collected electronically.
3. Results
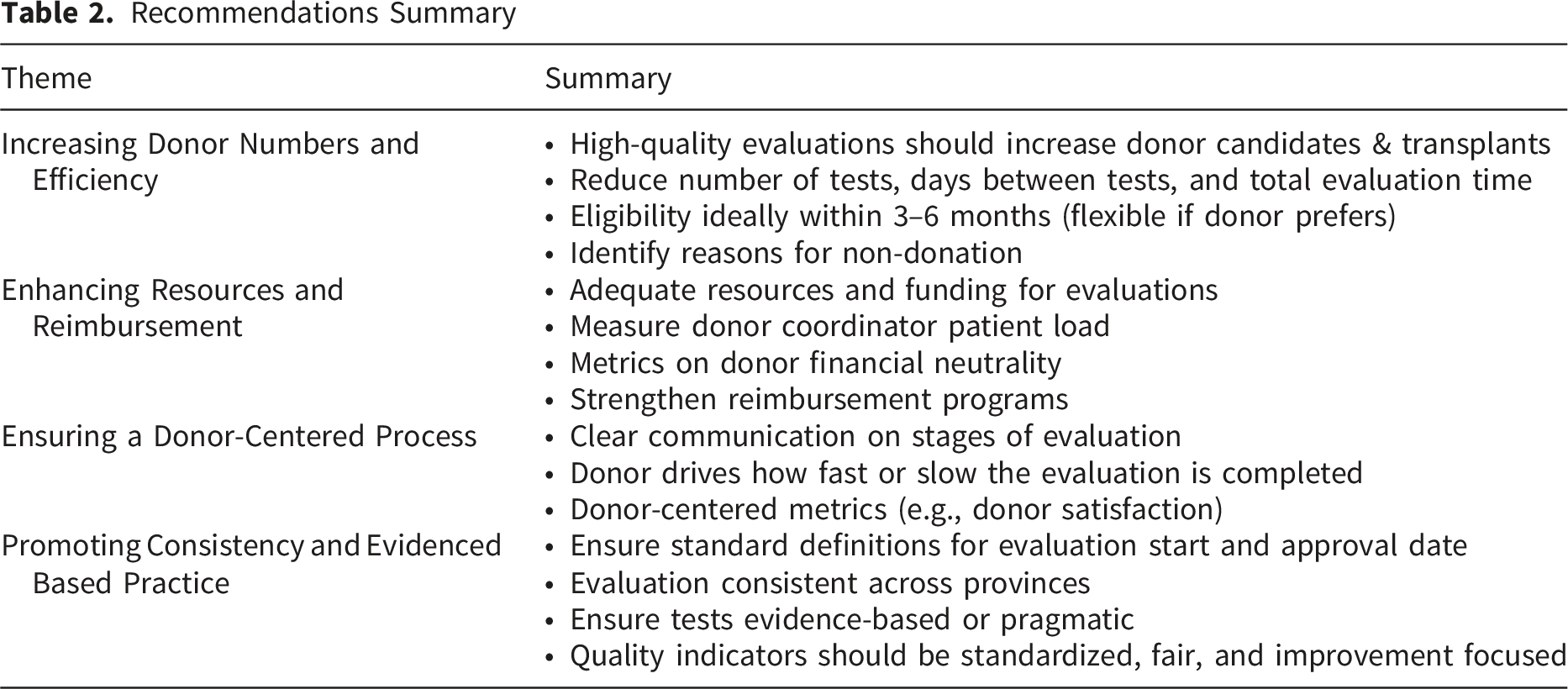
Recommendations Summary
Recommendations That Reached Consensus Through the Delphi Process
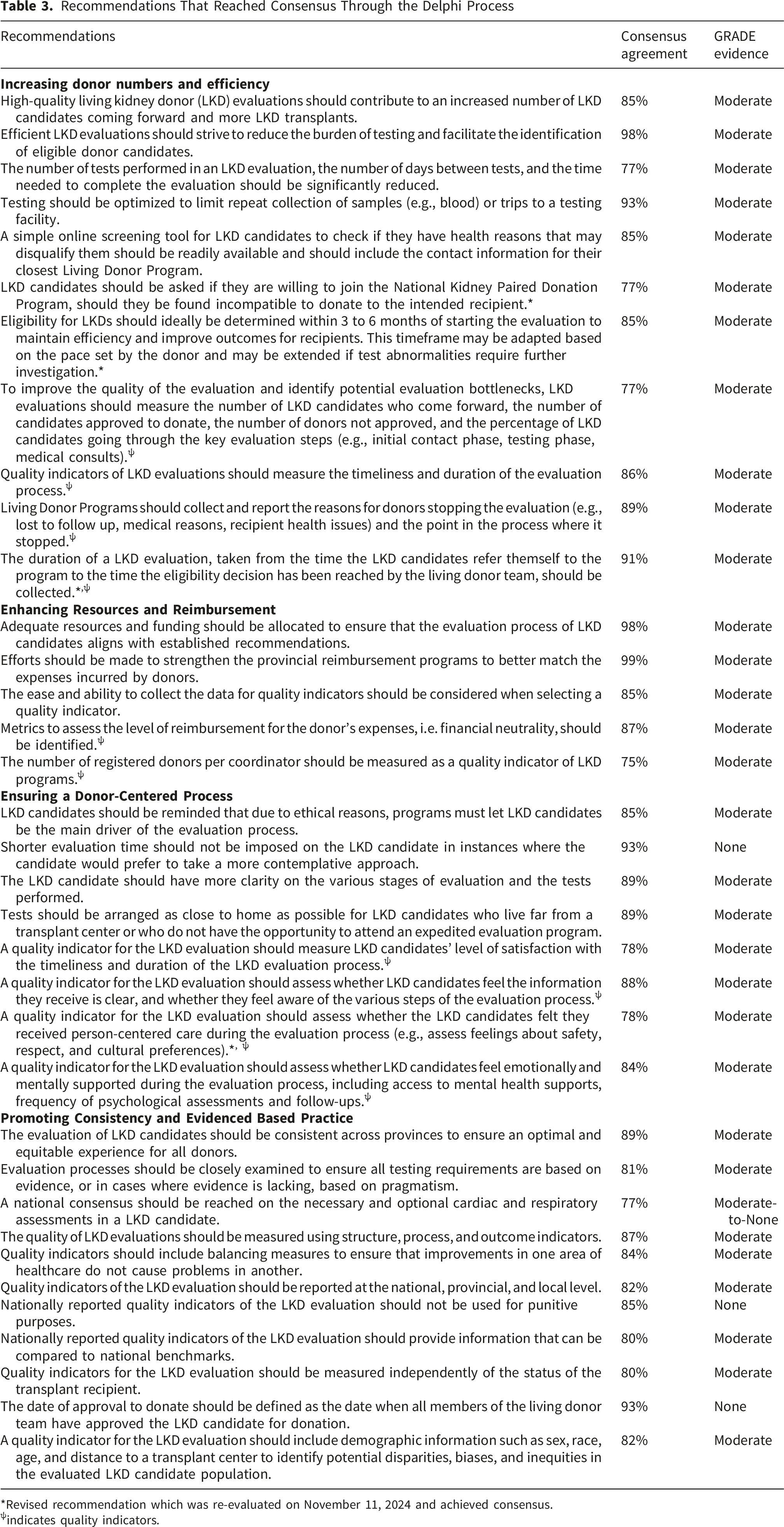
*Revised recommendation which was re-evaluated on November 11, 2024 and achieved consensus.
ψindicates quality indicators.
Theme one, Increasing Donor Numbers and Efficiency, emphasized that enhancing the quality and structure of donor evaluations is anticipated to expand both the number of eligible donor candidates and the total number of transplants performed. Programs should therefore prioritize redesigning evaluation pathways to minimize unnecessary testing, reduce total evaluation duration, and facilitate eligibility determinations within three to six months. Theme two, Enhancing Resources and Reimbursement, highlighted that the successful redesign of donor evaluations is contingent upon adequate program funding. In many jurisdictions, evaluation costs for donor candidates who do not ultimately proceed to donation are not reimbursed, a policy that is inconsistent with the objective of increasing living donor numbers through broader evaluation. This theme further reinforced that the evaluation process should be financially neutral for donor candidates, and that formal mechanisms should be established to ensure cost neutrality. Theme three, Ensuring a Donor-Centered Process, underscored the importance of reducing the logistical and emotional burden of the evaluation process to ensure equitable access to living donation. Donor candidates should be empowered to determine the pace of their evaluation, and testing should be conducted as close to their home location as feasible to promote convenience and accessibility. Theme four, Promoting Consistency and Evidence-Based Evaluation, emphasized the need for standardization across programs in alignment with the best available evidence. The adoption of uniform definitions for evaluation start and end dates would enable robust data collection, inter-program benchmarking, and continuous quality improvement efforts.
4. Discussion
Recommendations for a high-quality LKD evaluation were developed using a robust and systematic approach, with input from living kidney donors, nurses, nephrologists, surgeons, researchers, and representatives from provincial transplant bodies who participated in several virtual working groups and a virtual consensus conference. A total of 35 recommendations reached consensus. The recommendations included four themes: increasing donor numbers and efficiency, providing resources and reimbursement, ensuring a donor-centered process and consistent and evidenced based evaluations.
Currently, little guidance is available on how to provide a high-quality LKD evaluation from the perspectives of key stakeholders in the kidney transplantation and living kidney donation journey. In 2017, a Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors was developed by KDIGO (Kidney Disease: Improving Global Outcomes). 26 These guidelines inform the medical, surgical and social aspects of caring for donor candidates before, during, and after donation, but do not help living donor programs design their evaluation processes in ways that consider all dimensions of healthcare quality, and importantly, meeting the needs of the donor candidates. Our recommendations complement and extend these guidelines by providing recommendations that focus specifically on a high-quality LKD evaluation from the perspective of living kidney donors. A previously conducted environmental scan of quality indicators across Canadian transplant centers identified only 4 indicators related to LKD evaluation, with few person-centered or equitable care indicators. 23 A key strength of this work is the integration of living donor perspectives throughout the consensus process, ensuring that the proposed quality indicators reflect not only clinical priorities but also the experiences and values of donors themselves.
Our report has some limitations. As the conference progressed, fewer individuals participated in the eDelphi voting exercise. Potential cultural factors (e.g. Indigenous identity) related to the living kidney donor evaluation were not assessed, and this should be examined in future work. While many steering committee members also participated in the eDelphi consensus voting, undue influence is unlikely, given that an average of 79 participants voted per recommendation. Many recommendations were not supported by high quality evidence as they related to pragmatic aspects of living donor program structure, organization and quality measurement, for which limited empirical evidence exists. The recommendations represent expert consensus intended to guide quality improvement efforts and should be evaluated prospectively to determine their impact on donor evaluation processes and outcomes. During the consensus process, several potential definitions for the start of donor evaluation were considered, but consensus on a single operational definition was not achieved. Subsequent discussions within the Ontario Living Kidney Donor Working Group identified the date of completion of the medical–social health questionnaire as consistently documented and is being adopted as a practical reference point for the start of the evaluation in Ontario. Broader engagement with transplant programs across Canada will be needed to harmonize the definition of the evaluation start date and support consistent measurement of evaluation timelines. The recommendation to measure donor satisfaction reflects the importance placed by patient participants on donor experience during the evaluation process. However, satisfaction can be challenging to measure reliably and may be influenced by the outcome of the donation process. Future work will be required to develop or adapt standardized patient-reported experience measures that can capture the perspectives of donor candidates across transplant programs. Last, our conference focused on the donor evaluation process, future work should extend to the preoperative period (i.e., time from when donor eligibility is determined to the postoperative period).
Following the consensus conference, our goal will be to move from agreement to implementation, through a structured process that ensures our conference outcomes lead to measurable change. These steps include engaging with key partners and policy makers (e.g. provincial health authorities) to share recommendations and gain endorsement and using an implementation framework to plan short, medium and long-term goals with key parties, timelines and measurable outcomes.
5. Summary
A consensus conference was held in September 2024 to define a high-quality living kidney donor evaluation based on multiple perspectives resulting in 35 recommendations. The recommendations aim to ensure a consistent, supportive, and transparent evaluation process for all LKD candidates. Next steps include creating working groups to implement these recommendations. Future research should establish national benchmarks for a high-quality LKD evaluation.
Supplemental Material
Supplemental Material - Defining a High-Quality Living Kidney Donor Evaluation: A Delphi Survey and Consensus Conference Summary Report
Supplemental Material for Defining a High-Quality Living Kidney Donor Evaluation: A Delphi Survey and Consensus Conference Summary Report by Seychelle Yohanna, Kyla L. Naylor, Linnea Holtby, Jessica M. Sontrop, Ahsan Alam, Brent Cheal, Christine Dipchand, Amit X. Garg, Jagbir Gill, Steven Habbous, Jay Hingwala, Peggy John, Jessica King, Michael Koch, Ngan N. Lam, Scott Morrison, Christine Pisapia, Marian Reich, Shaifali Sandal, Craig Settee, Terry Smith, Carrie Thibodeau, Lynn van der Linde, Carol Wang in Canadian Journal of Kidney Health and Disease
Supplemental Material
Supplemental Material - Defining a High-Quality Living Kidney Donor Evaluation: A Delphi Survey and Consensus Conference Summary Report
Supplemental Material for Defining a High-Quality Living Kidney Donor Evaluation: A Delphi Survey and Consensus Conference Summary Report by Seychelle Yohanna, Kyla L. Naylor, Linnea Holtby, Jessica M. Sontrop, Ahsan Alam, Brent Cheal, Christine Dipchand, Amit X. Garg, Jagbir Gill, Steven Habbous, Jay Hingwala, Peggy John, Jessica King, Michael Koch, Ngan N. Lam, Scott Morrison, Christine Pisapia, Marian Reich, Shaifali Sandal, Craig Settee, Terry Smith, Carrie Thibodeau, Lynn van der Linde, Carol Wang in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors wish to acknowledge the patient partners who contributed to this work. The authors thank STA HealthCare Communications with developing and organizing the consensus conference. The authors also wish to thank the Canadian Blood Services for their support in organizing the consensus conference. SS is supported by the Chercheur boursier clinicien - Junior 1 award from the Fonds de recherche du Québec – Santé; an educational scholarship to support protected time for researchers in Quebec, Canada. KLN was supported by a Health System Impact Embedded Early Career Researcher Award from the Canadian Institutes of Health Research. AXG was supported by the Kay Family Chair in Transformational Kidney Care.
ORCID iDs
Consent for Publication
All co-authors consent to manuscript publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Executive Committee of Can-SOLVE CKD (Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease), a patient-orientated research network to transform the care of people affected by kidney disease (![]() ).
).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No data were utilized in the preparation of this conference report.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.