
Abstract
Keywords
Introduction
Paediatric oncologists encounter considerable emotional challenges when delivering a diagnosis of childhood cancer and navigating complex treatment processes. In addition to the high medical responsibility they bear, these physicians are frequently exposed to repeated experiences of suffering, grief, and death. This repeated exposure to traumatic circumstances places them at substantial risk of psychological distress, including anxiety, depression, burnout, and compassion fatigue. Yet, beyond these adverse outcomes, recent psychological theories emphasize that physicians, like their patients, may also undergo posttraumatic growth (PTG)—positive psychological changes that arise following highly stressful experiences. These emotionally demanding clinical conditions make it important to understand not only distress-related outcomes but also adaptive psychological responses among paediatric oncologists (Gerhart et al., 2019).
Children and adolescents diagnosed with cancer, as well as their parents, experience profound psychological strain. Studies consistently report symptoms of posttraumatic stress disorder (PTSD), anxiety, and depression in both children and parents following a cancer diagnosis, independent of disease type or outcome (Kazak et al., 2004; Klašnja et al., 2023; Van Warmerdam et al., 2019). In summary, paediatric oncologists are operating in an environment in which traumatic stress is not solely a solitary occurrence but is also distributed across families. Given physicians’ ongoing awareness of and exposure to these emotional experiences, it is critical to understand their psychological responses.
Within this context, it is important to evaluate the relationship between psychological distress and posttraumatic growth among physicians working in paediatric oncology. Although burnout and other mental health outcomes in healthcare professionals have been widely studied, PTG has received comparatively less systematic empirical attention in this group (Gerhart et al., 2019). Understanding whether and how paediatric oncologists achieve positive psychological change in the face of recurrent occupational trauma is important, as PTG may enhance resilience, sustain professional motivation, and improve quality of care. Therefore, this study aimed to compare psychological distress and PTG between physicians working in paediatric and adult haematology-oncology settings (Tedeschi and Calhoun, 1996).
Tedeschi and Calhoun conceptualised the notion of PTG as positive psychological transformation resulting from wrestling with the inherently stressful aspects of life (Tedeschi and Calhoun, 2004). It involves domains such as improved self-perception, enhanced relationships, new possibilities, spiritual change, and appreciation of life. In clinical contexts, PTG has been studied mainly in patients and families facing cancer, trauma, or bereavement, but much less frequently among healthcare professionals. Given that paediatric oncologists often witness trauma vicariously through their patients and families, exploring PTG in this group can reveal whether positive transformation accompanies professional stress exposure. Such an approach is essential not only for supporting physician well-being but also for improving patient-centered care, as emotionally resilient physicians may provide more sustainable and empathetic medical support (Corn and Feldman, 2024; Dursun and Söylemez, 2020; İnci and Boztepe, 2013).
Methods
This cross-sectional study included 265 physicians working in General Paediatrics, Paediatric Haematology-Oncology, Adult Haematology-Oncology and Internal Medicine. Internal medicine physicians were included as a comparison group with relatively less frequent exposure to oncology-related stressors. Participants completed a questionnaire that captured their age, gender, specialty, years of employment, and institutional affiliation. The questionnaire also included questions on the difficulties physicians face, coping methods, hospital-related anxiety, and burnout levels. Participants completed the Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983), the Depression Anxiety Stress Scale–21 (DASS-21) (Lovibond, 1995), and the Turkish version of the Posttraumatic Growth Inventory (PTGI) (Kağan et al., 2012; Tedeschi and Calhoun, 1996).
Participants were recruited on a voluntary basis from physicians working in the predefined specialty groups at participating institutions in Turkey. Eligible participants were currently practising physicians in General Paediatrics, Paediatric Haematology-Oncology, Adult Haematology-Oncology, or Internal Medicine. Physicians not actively practising during the study period and incomplete questionnaires were excluded from the analysis. The survey was distributed through institutional communication channels. The response rate could not be calculated because the total number of physicians who received the survey invitation was not systematically recorded.
Hospital Anxiety and Depression Scale (HADS): A 14-item self-report scale originally developed by Zigmond and Snaith in 1983 (Zigmond and Snaith, 1983) and validated in Turkish populations by Aydemir et al. (Aydemir et al., 1997), who identified cut-off scores of 10/11 for HADS-A and 7/8 for HADS-D; scores at or above these thresholds indicate risk. It consists of two subscales: the anxiety (HADS-A) and depression subscales (HADS-D), each containing seven items. It is scored 0–3, and each subscale can range from 0 to 21. Subjects are requested to select the response that is most relevant to them regarding their feelings over the previous week.
The Depression Anxiety Stress Scale was developed by Lovibond and Lovibond (Lovibond, 1995) and validated in Turkish populations (Yıldırım et al., 2018). It is a theoretically relevant assessment of negative emotions that includes depression, anxiety, and stress symptoms subscales. Each subscale comprises seven items, rated on a 4-point Likert-type scale, ranging from 0 (never) to 3 (always). Higher scores indicate greater emotional distress. DASS-21 subscale scores were analysed as raw scores without applying the standard multiplication factor. This approach was preferred to preserve the original distribution of responses and to facilitate direct comparisons across subscales within the study. However, it is acknowledged that this method limits direct comparability with studies using standard severity cut-offs.
Posttraumatic Growth Inventory (PTGI): Tedeschi and Calhoun developed the Posttraumatic Growth Inventory (PTGI) to assess posttraumatic growth and self-improvement a person undergoes. A 21-item inventory based on Tedeschi’s five-factor model, widely validated for assessing personal growth following stressful events. Items are rated on a 6-point Likert scale, yielding a total score ranging from 0 to 105. The five factors are New Possibilities, Relating to Others, Personal Strength, Spiritual Change, and Appreciation of Life (Tedeschi and Calhoun, 1996). The Turkish adaptation of the scale, which was examined for validity and reliability in a Turkish sample, has a three-factor structure comprising Changes in Self-Perception, Changes in Philosophy of Life, and Changes in Relationships. Subscale scores range from 0 to 50 for Self-Perception, 0 to 30 for Philosophy of Life, and 0 to 25 for Relationships, with higher scores indicating greater change within each domain (Kağan et al., 2012). In our study, PTGI was evaluated on a 3-factor structure. Given evidence supporting a stable three-factor structure in Turkish samples, analyses were conducted using the validated Turkish three-factor model rather than the original five-factor structure.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the data. Continuous variables (e.g., HADS-A and DASS-21 scores) were reported as mean ± standard deviation, while categorical variables (e.g., gender, age group, hospital type) were presented as frequency and percentage.
Group comparisons for categorical variables such as gender, age group, years of experience, and hospital type were conducted using the Chi-square test.
The age variable was categorized into two groups: “under 40 years” and “40 years or older.” Years of experience were grouped into two categories: “less than 10 years” and “10 years or more.” These cut-offs were selected to reflect early-career versus more experienced physicians, consistent with previous research examining occupational stress and professional development stages in healthcare settings.
Hospital type was initially recorded in three categories (state hospital, university hospital, and other). Due to the small number of participants in the “other” category (n = 6, 2.3%), these cases were excluded from hospital-type comparisons and analyses were conducted using two categories (state and university hospital).
Differences in continuous outcomes across department groups (e.g., HADS, DASS-21, and PTGI scores) were evaluated using one-way analysis of variance (ANOVA). When a significant difference was detected, post-hoc comparisons were performed using Tukey’s honestly significant difference (HSD) test to control for multiple comparisons. Adjusted comparisons were performed using analysis of covariance (ANCOVA) within the general linear model framework, controlling for age group, years of experience, and hospital type. ANCOVA was applied as an adjusted analytical approach to control for potential confounding by age group, years of experience, and hospital type, in line with recommendations for appropriate covariate adjustment in observational studies (Miller and Chapman, 2001). These models were considered complementary to the unadjusted ANOVA results and were included to evaluate whether observed group differences remained after adjustment for prespecified covariates.
Associations between HADS, DASS-21, and PTGI subscale scores were assessed using Pearson correlation analysis. A p-value of <0.05 was considered statistically significant. An a priori power analysis was conducted using G*Power 3.1 software. Based on a one-way ANOVA design with four groups, a medium effect size (Cohen’s f = 0.25), a significance level of α = 0.05, and a desired statistical power of 0.80, the minimum required sample size was calculated as 180 participants. The final sample size of 265 exceeded this requirement, indicating that the study was adequately powered to detect group differences. Given the observed effect sizes in the current study (η2 ranging from 0.033 to 0.085), the achieved statistical power is likely to be higher than the initially estimated value.
Prior to analysis, data were screened for missing values. Cases with incomplete responses for key variables were excluded from the relevant analyses. The assumptions of normality and homogeneity of variances were evaluated using visual inspection of histograms and Levene’s test, respectively. These assumptions were considered adequately met for the applied parametric tests.
Human ethics and consent to participate
All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the Declaration of Helsinki. Participation was voluntary, and informed consent was obtained from all participants prior to survey completion. This study was approved by the Dr Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital Clinical Research Ethics Committee (Approval No: 2019-05/300; Date: 15/05/2019).
Results
Demographic characteristics.

Comparison of demographic characteristics by department groups.

Participants in the “other” hospital category (n = 6) were excluded from comparative analyses due to small sample size. Italic font is used to indicate statistically significant p–values (p < 0.05).
Hospital Anxiety and Depression Scale (HADS) scores and group-wise distribution.

Unadjusted analyses showed no statistically significant differences in HADS-A or HADS-D across department groups. In adjusted models controlling for age group, years of experience, and hospital type, department was associated with HADS-D (p = 0.047; partial η2 = 0.030).
Depression Anxiety Stress Scale (DASS-21) scores and group-wise distribution.
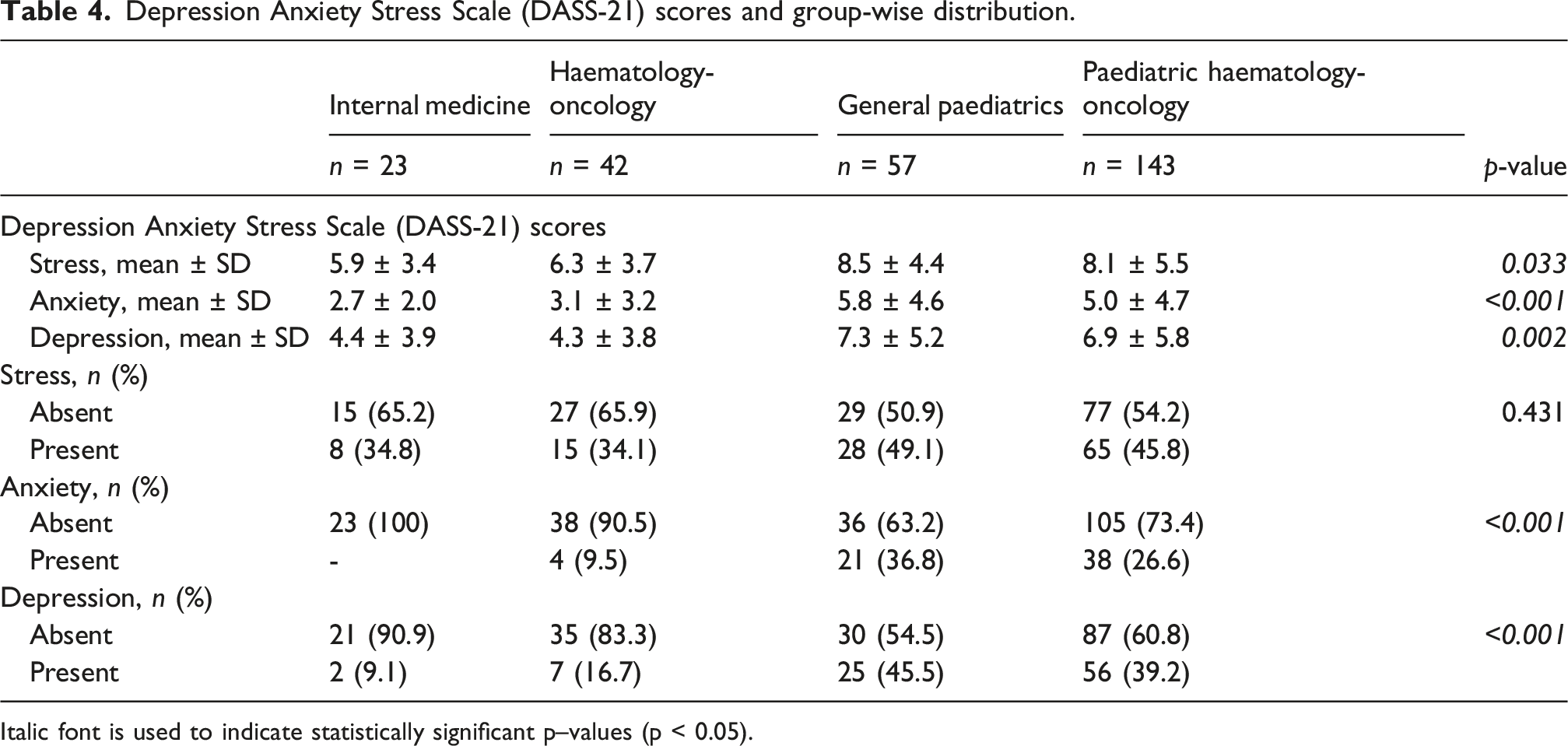
Italic font is used to indicate statistically significant p–values (p < 0.05).
Age group and years of professional experience were significantly associated with distress outcomes and were therefore retained as covariates in adjusted models.
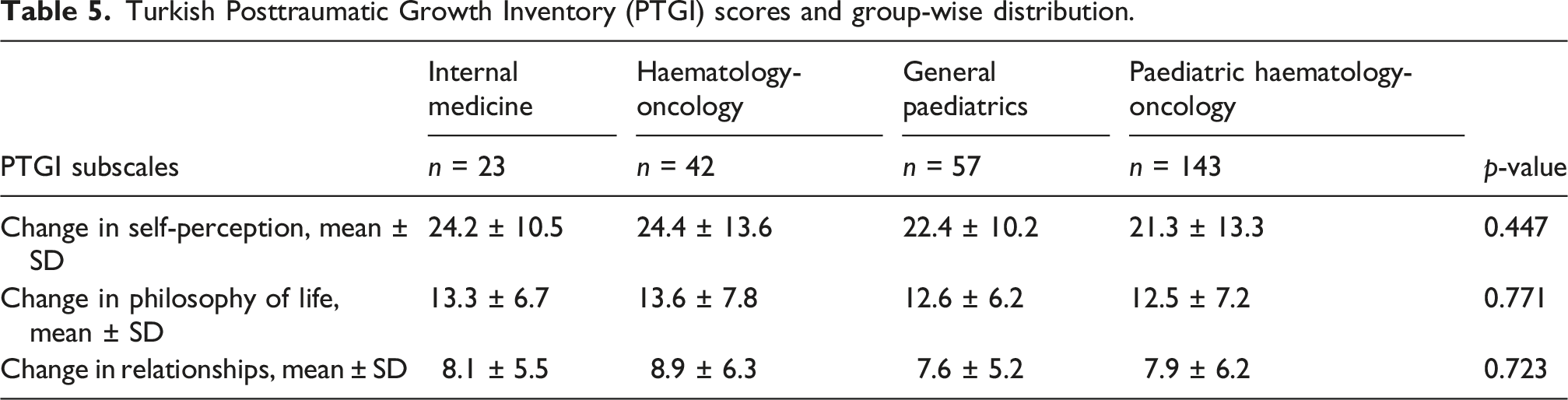
Turkish Posttraumatic Growth Inventory (PTGI) scores and group-wise distribution.
Pearson correlation matrix between HADS, DASS-21, and Turkish PTGI subscales.

Pearson correlation coefficients (r) are reported. (1) p < 0.05, (2) p < 0.01, (nˢ) not significant (p ≥ 0.05). Values are shown in the upper triangle.
Discussion
This study investigated the psychological well-being and posttraumatic growth (PTG) of physicians working in paediatric and adult oncology and haematology using validated psychological instruments (DASS-21, HADS, and PTGI). The results shed light on the emotional toll on physicians in high-stress medical environments, offering comparative insights into the experiences of paediatric- and adult-focused professionals.
HADS results indicated that elevated anxiety and depressive symptoms were familiar but not universal, with 38.9% of participants above the cut-off for anxiety risk and 47.2% above the cut-off for depression risk. These proportions should be interpreted as screening-level risk rather than clinical diagnoses. They may reflect, in part, self-selection into a voluntary survey and measurement characteristics of brief self-report tools. Consistent with expectations, HADS and DASS-21 subscales showed strong positive correlations, supporting convergent validity. By contrast, associations between distress and PTG were statistically significant in some comparisons but small in magnitude, suggesting that distress and growth may coexist and are not simple opposites.
From a health psychology perspective, psychological distress and posttraumatic growth should not be viewed as opposite ends of a single continuum. Rather, they represent partially independent processes that may coexist under conditions of sustained occupational stress. In the present study, strong intercorrelations were observed among distress measures, whereas associations between distress and PTG were weak and predominantly negative. This pattern suggests that elevated emotional burden may hinder meaning-making processes when supportive contextual factors are insufficient. This finding reinforces the health psychology view that adaptive psychological outcomes depend not only on individual exposure to stress but also on the availability of meaning-making resources.
The DASS-21 results further clarified these findings, showing that physicians working in paediatric departments—especially in Paediatric Haematology-Oncology—have significantly higher scores for depression, anxiety, and stress compared to their counterparts in internal medicine or Adult Haematology-Oncology. This aligns with previous literature indicating that paediatric oncologists face unique challenges due to their frequent exposure to child mortality, deep emotional involvement with families, and the psychological complexity of communicating complex diagnoses (Gerhart et al., 2019; Kaye et al., 2017).
Physicians working in paediatric oncology may be particularly vulnerable due to the moral and emotional complexity of caring for children with life-threatening illnesses. Unlike adult oncology, paediatric settings often involve prolonged relationships with families, heightened identification with patients, and repeated exposure to perceived injustice, loss, and moral distress. Health psychology models emphasise that such chronic exposure, when not accompanied by opportunities for reflection and cognitive processing, may amplify distress without facilitating growth.
Our findings indicate a consistent trend: physicians working in paediatric settings experience significantly greater emotional strain than their adult oncology counterparts. The elevated DASS-21 scores for stress and anxiety among paediatricians support the hypothesis that early-career physicians—most of whom are under 40 years old and have less than 10 years of experience—are especially exposed to emotional distress in high-intensity paediatric care environments. This is consistent with prior findings, which indicate that younger and less experienced physicians may be at an elevated risk of burnout and emotional distress as they have not yet developed coping strategies (Shanafelt and Dyrbye, 2012).
Interestingly, although paediatric physicians reported higher levels of emotional distress, their scores on the Posttraumatic Growth Inventory (PTGI) were not significantly higher than those of adult oncology physicians. This finding suggests that posttraumatic growth may not necessarily increase in proportion to psychological burden. Instead, it might depend on certain moderating factors, such as social support, resilience training, supervision, or individual coping styles (Kağan et al., 2012; Tedeschi and Calhoun, 1996, 2004).
The subscales of Posttraumatic Growth Inventory (PTGI) in our study—Self-Perception, Philosophy of Life, and Relationships—did not show significant differences among the various specialty groups. However, paediatric oncologists tended to score slightly lower. Correlation analysis indicated that higher scores of depression, measured by HADS and DASS-21, were negatively associated with PTG scores, particularly in the Relationship and Self-Perception subdomains. This inverse relationship suggests that ongoing psychological distress may impede growth processes, especially if it is not adequately addressed through reflection or support systems. Within the framework of posttraumatic growth, personal empowerment denotes positive change in self-perception—often described as a shift towards greater perceived personal strength and agency. By contrast, depression is characterized by pervasive negative cognitions about the self, the environment, and the future (Beck, 2008). Accordingly, in our study, it is theoretically consistent that participants with higher depression scores exhibited lower scores on the Self-Perception domain.
Building on this perspective, the posttraumatic growth framework posits that growth is not an automatic consequence of distress exposure but emerges through deliberate cognitive and emotional processing supported by internal and external resources (Corn and Feldman, 2024; Dursun and Söylemez, 2020; Tedeschi and Calhoun, 2004; İnci and Boztepe, 2013). In the absence of such meaning-making opportunities, elevated distress may remain unresolved and may even inhibit growth-related processes, as observed in highly distressed paediatric physicians in the present study.
Accordingly, the present findings highlight the role of organisational and contextual factors—such as supervision, peer support, and reflective practice—in shaping adaptive psychological responses to occupational stress.
The high prevalence of anxiety and depression across all groups, particularly among Paediatric Haematology-Oncologists, indicates the importance of interventions that promote physician mental health. Although burnout and distress in healthcare workers are well studied, the concept of posttraumatic growth is understudied, especially in paediatric oncology. Mental health support, supervision models, and resilience programs should be integrated into day-to-day professional development. The goal of this approach is not just to prevent detriment, but to support thriving in high-intensity oncology settings (Kamau-Mitchell, 2019; Shanafelt and Dyrbye, 2012).
Differences in psychological profiles between adult and paediatric oncologists highlight the importance of targeted rather than blanket interventions. Paediatric specialists may find it more beneficial to support feelings and peer relationships. Adult oncology physicians may benefit from interventions addressing meaning-making, professional identity, and work–life balance.
Importantly, the absence of higher PTG levels despite elevated distress highlights the role of environmental and organisational determinants of psychological adaptation. Health psychology frameworks emphasise that posttraumatic growth is facilitated not merely by exposure to adversity but by access to resources that support meaning-making, such as peer support, supervision, and institutional acknowledgement of emotional labour. Without these structures, distress may remain unresolved and maladaptive.
Limitations
While this study has provided several significant findings, some limitations need to be acknowledged. First, a cross-sectional design does not allow for finding a causal direction between distress and PTG. Longitudinal studies are necessary to chart the trajectory of distress and growth over time. In addition, reporting biases probably had a significant effect on the validity of the data obtained, given the stigma in clinical settings towards mental health. The stigma can lead participants to underreport symptoms or adjust their experiences in a way that aligns with societal expectations, thereby compromising the integrity of research findings. Finally, changes in cultural and institutional context between different types of hospitals were not adjusted for, which may have influenced our results. Additionally, DASS-21 scores were analysed without applying the standard multiplication factor, which limits direct comparison with studies using established severity classifications. Therefore, the results should be interpreted in terms of relative group differences rather than clinical severity thresholds. However, as the multiplication factor represents a linear transformation, it does not affect between-group comparisons or statistical significance.
Future research should adopt longitudinal designs to better elucidate the temporal relationship between psychological distress and posttraumatic growth among physicians. In addition, qualitative approaches may provide deeper insight into the contextual and individual factors that facilitate or hinder PTG in clinical settings. Finally, intervention-based studies targeting organisational support, resilience training, and coping strategies are warranted to determine whether PTG can be actively promoted in high-stress medical environments.
Conclusion
This study demonstrates that physicians working in haematology-oncology report substantial psychological distress, with higher DASS-21 depression and anxiety scores observed in paediatric groups compared with adult haematology/oncology. However, posttraumatic growth levels (PTGI) were broadly similar across specialties. Given the cross-sectional design and potential self-selection, findings should be interpreted as associations. Institutional strategies—such as accessible mental health services, structured supervision/peer support, workload and recovery-time protections, and targeted training—are warranted to support physician well-being in high-intensity oncology care. These findings underscore that physician mental health should be addressed as a health system responsibility rather than an individual coping issue.
Footnotes
Ethical considerations
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Ethical approval was obtained from an institutional clinical research ethics committee (Approval No: 2019-05/300, Date: 15/05/2019).
Consent to participate
Informed consent was obtained electronically from all participants prior to participation in the study.
Consent for publication
Not applicable. This manuscript does not contain any identifiable individual data.
Author contributions
S.S. contributed to study conception and design. Data collection and statistical analysis were performed by S.S. and M.K. All authors contributed to data interpretation, manuscript drafting, and critical revision, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Trial pre-registration
Not applicable, as this was an observational cross-sectional study and was not prospectively registered.