
Abstract
Case summary
A 1-year-old, male neutered Persian cat presented to the emergency room with acute, severe wheezing and coughing after the introduction of a new kitten to the household. The patient progressed to hypoxemic respiratory failure consistent with acute respiratory distress syndrome (ARDS) and required mechanical ventilation. RT-PCR testing from a conjunctival and deep pharyngeal swab confirmed feline calicivirus infection. Because of refractory hypoxemia and declining lung compliance (2.4 ml/cmH2O), novel therapy with intratracheal porcine surfactant (Curosurf) was attempted. A dose of 1.5 ml/kg was administered over 60 s. After administration, pulmonary compliance improved to 3.1 ml/cmH2O. The patient was weaned from the ventilator on day 10; however, severe laryngeal swelling necessitated a temporary tracheostomy. The patient died on day 15 from tracheal stenosis and obstruction of the stoma site by granulation tissue.
Relevance and novel information
To the authors’ knowledge, this is the first report describing the development of ARDS from calicivirus pneumonia and the use of porcine surfactant in the treatment of ARDS in a cat. The administration of surfactant resulted in objective improvements in lung compliance.
Keywords
Introduction
Feline calicivirus (FCV) is a highly prevalent, non-enveloped RNA virus of the family Caliciviridae known for its significant genetic plasticity and high mutation rate.1,2 Although the majority of FCV infections result in self-limiting upper respiratory tract disease and oral ulceration, specific viral strains have been associated with distinct, severe clinical syndromes. 2 These include ‘limping syndrome’ associated with acute transient synovitis, virulent systemic FCV characterized by vasculitis and multi-organ failure,3,4 and severe viral pneumonia. 5 FCV pneumonia results from direct viral tropism of the lower respiratory tract. 5 The virus targets alveolar macrophages and type II pneumocytes, causing necrosis, alveolar collapse and a subsequent inflammatory cascade.5,6
Type II pneumocytes are responsible for the production of surfactant within alveoli. 7 Surfactant reduces the surface tension within alveoli, which prevents alveolar collapse at the end of expiration. The loss of surfactant that occurs with the destruction of type II pneumocytes leads to decreased lung compliance, atelectasis and ventilation-perfusion mismatching, which are all hallmark features of acute respiratory distress syndrome (ARDS). 7 In veterinary medicine, ARDS is defined by the acute onset of tachypnea, bilateral pulmonary infiltrates and severe hypoxemia not attributable to cardiac failure. 8 The prognosis for cats with ARDS is grave, with reported mortality rates in the range of 80–100% despite aggressive mechanical ventilation (MV).9,10
Surfactant therapy is a standard of care in human neonatal respiratory distress syndrome and has been investigated in adult human ARDS with variable success.11,12 Although the veterinary literature on surfactant replacement is limited, successful cross-species administration has been documented, including the use of equine surfactant in a premature alpaca cria. 13 To the authors’ knowledge, the use of porcine surfactant for the treatment of ARDS in a cat has not been reported. The purpose of this case report is to describe the administration of intratracheal porcine surfactant and clinical outcome in a cat with severe ARDS secondary to FCV pneumonia.
Case description
A 1-year-old, male neutered Persian cat presented to the emergency service with a 24-h history of hypersalivation, anorexia, dysphagia and lethargy. A kitten with serous ocular and nasal discharge and sneezing had recently been adopted from a shelter and introduced to the household.
On physical examination, the patient was quiet and alert, with mild serous ocular discharge and pyrexia (102.9°F [39.4°C]). Respiratory assessment revealed stertorous breathing consistent with a brachycephalic conformation and normal lung sounds. The patient received subcutaneous fluids (lactated Ringer’s, 25 ml/kg SC), robenacoxib (Onsior, 8 mg SC) and ondansetron (4 mg PO) and was discharged but re-presented 6 h later with progressive anorexia, vomiting and coughing. Physical examination revealed increased bronchovesicular sounds, a respiratory rate of 36 breaths/min, progressive pyrexia (103.9°F [39.9°C]) and a tense abdomen. Abdominal radiographs showed gastric dilation suspected secondary to aerophagia and no evidence of mechanical obstruction. The patient was discharged after receiving maropitant (1 mg/kg SC) and lactated Ringer’s (15 ml/kg SC).
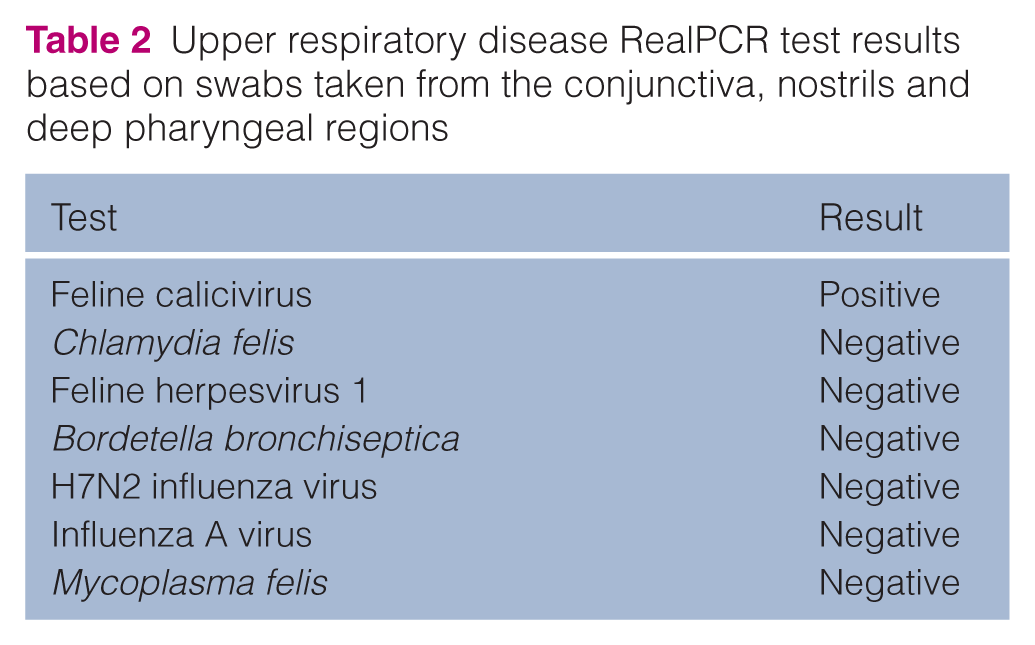
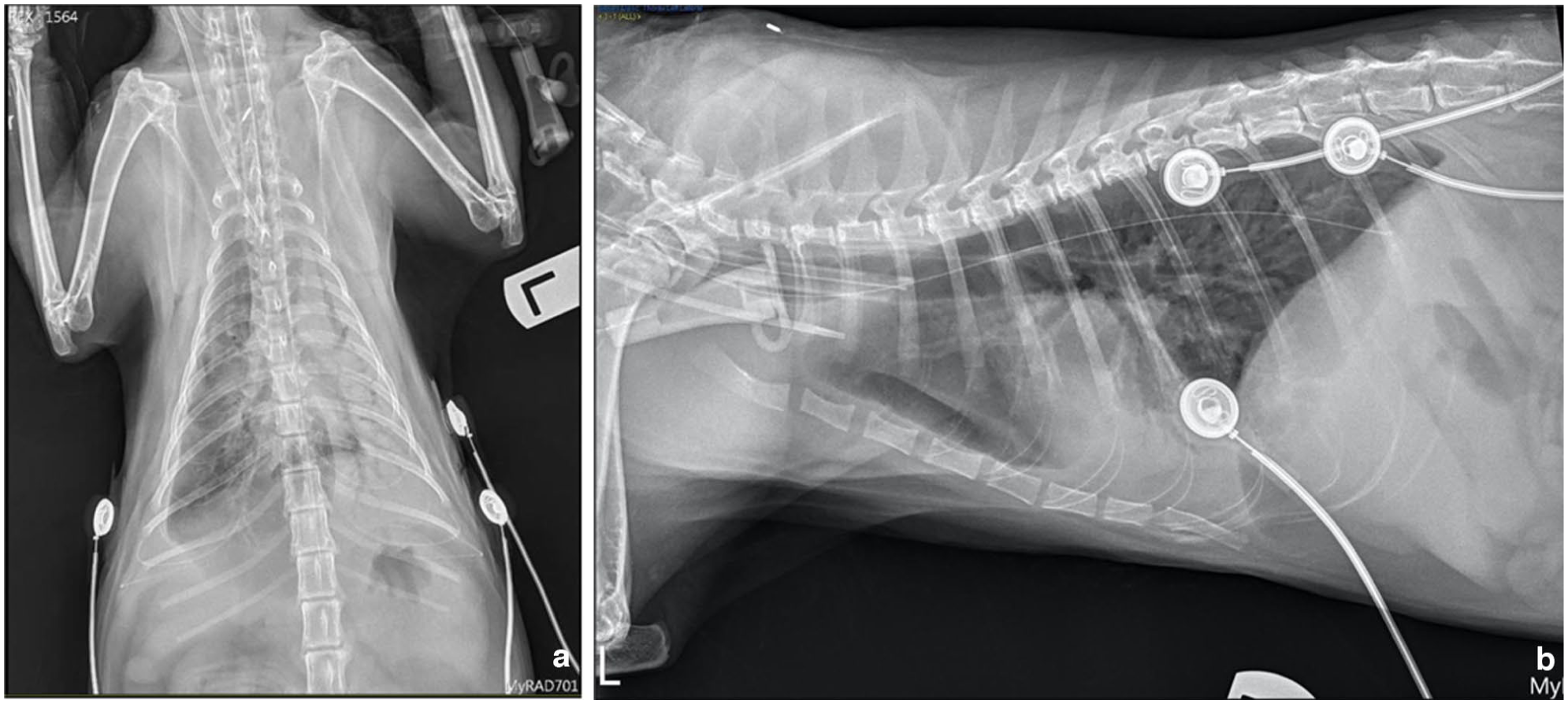
The patient re-presented to the emergency room the following day in respiratory distress, with worsening tachypnea (40 breaths/min), orthopnea, marked inspiratory effort and worsened pyrexia (105.0°F [40.6°C]). Point-of-care venous blood gas analysis revealed a mixed respiratory alkalosis and metabolic acidosis (Table 1). Thoracic radiographs demonstrated a diffuse, patchy interstitial-to-alveolar pattern (Figure 1), which is concerning for pneumonia. Swabs were obtained from the patient’s conjunctiva, nostrils and deep pharyngeal regions and submitted for a RT-PCR infectious respiratory disease panel (Upper Respiratory Disease RealPCR; IDEXX Laboratories). The patient tested positive for FCV (Table 2). The patient had received the trivalent feline viral rhinotracheitis, calcivirus and panleukopenia vaccine (TruFel HCP) 6 months before presentation. Retroviral testing (feline leukemia virus/feline immunodeficiency virus) was negative.
Point-of-care blood results on the day of admission to the hospital
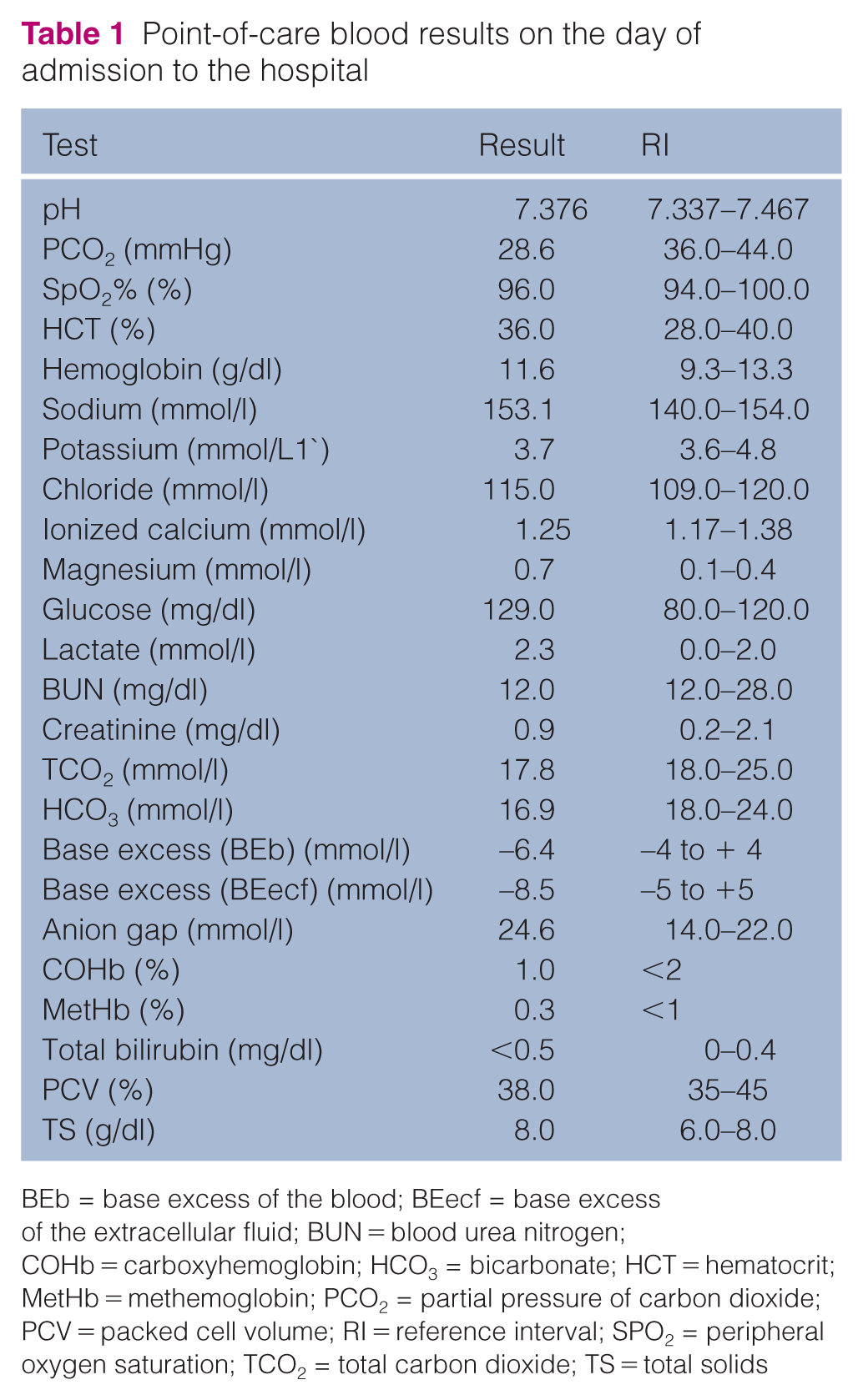
BEb = base excess of the blood; BEecf = base excess of the extracellular fluid; BUN = blood urea nitrogen; COHb = carboxyhemoglobin; HCO3 = bicarbonate; HCT = hematocrit; MetHb = methemoglobin; PCO2 = partial pressure of carbon dioxide; PCV = packed cell volume; RI = reference interval; SPO2 = peripheral oxygen saturation; TCO2 = total carbon dioxide; TS = total solids
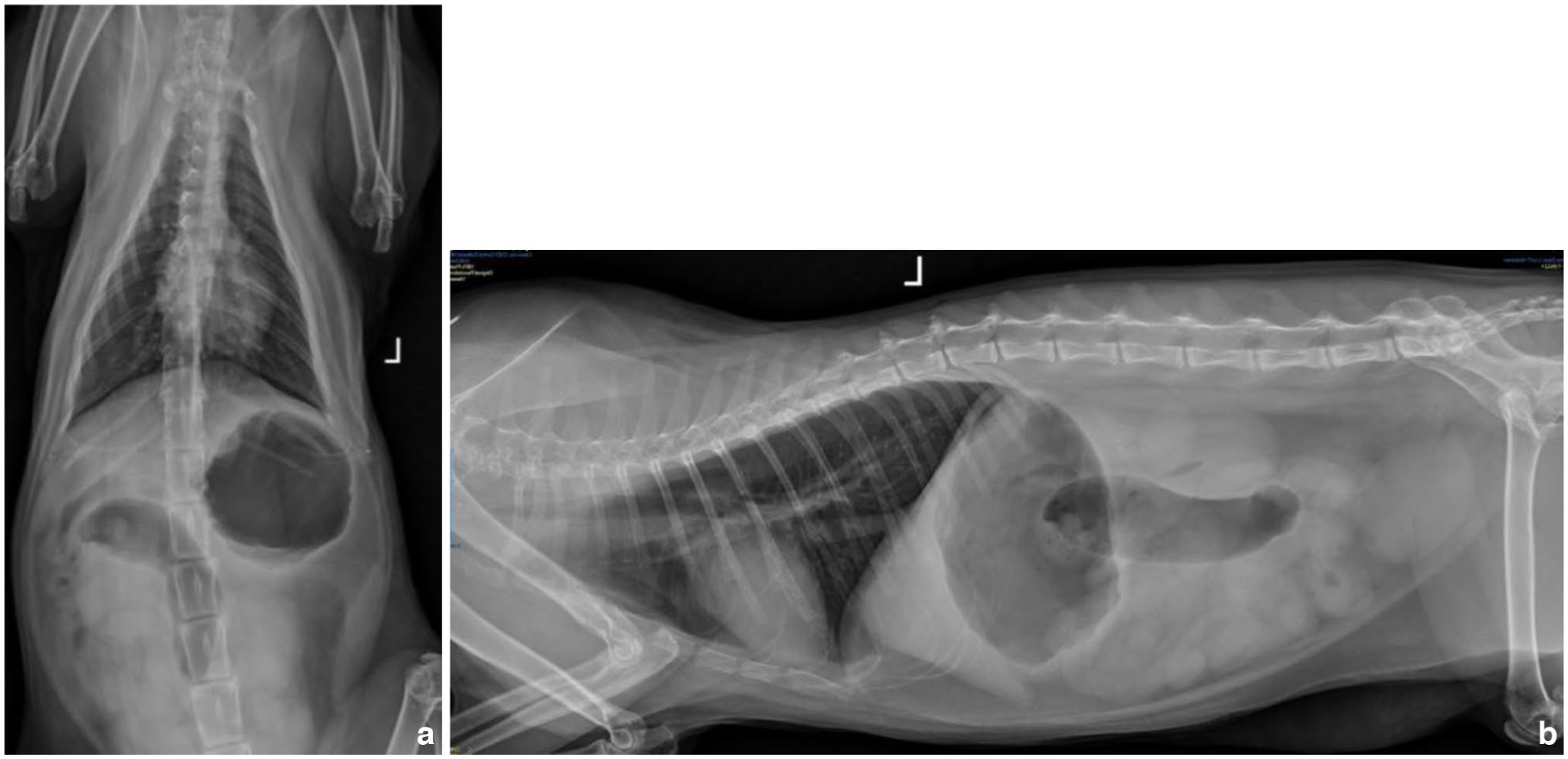
Day 1: (a) dorso-ventral and (b) left lateral thoracic radiographs at the time of admission to the hospital showing patchy interstitial pulmonary infiltrate
Upper respiratory disease RealPCR test results based on swabs taken from the conjunctiva, nostrils and deep pharyngeal regions
The patient was hospitalized with empirical ampicillin/sulbactam (120 mg IV q8h), maropitant (1 mg/kg IV q24h), enrofloxacin (5 mg/kg IV q24h) and metoclopramide (0.5 mg/kg SQ q8h). Enrofloxacin was added as a parenteral antibiotic choice for the treatment of Mycoplasma felis pending the results of the infectious respiratory disease PCR.
Progression to ARDS and mechanical ventilation
On day 2, the patient’s pyrexia had improved (102.4°F [39.1°C]) but his respiratory status continued to deteriorate. The patient developed open-mouth breathing and was anesthetized and intubated because of the concern for respiratory fatigue. Synchronized intermittent MV was initiated. The patient was hypoxemic (SpO2 91%) on the ventilator with a fraction of inspired oxygen of 100%. An endotracheal wash was consistent with septic suppurative inflammation with intracellular Gram-positive diplococci. Aerobic and anaerobic bacterial cultures of the endotracheal wash were submitted. All cultures yielded no growth. The patient was started on empiric antibiotics several hours before cultures were obtained, which may or may not have affected the culture results.
Hospitalization and surfactant administration
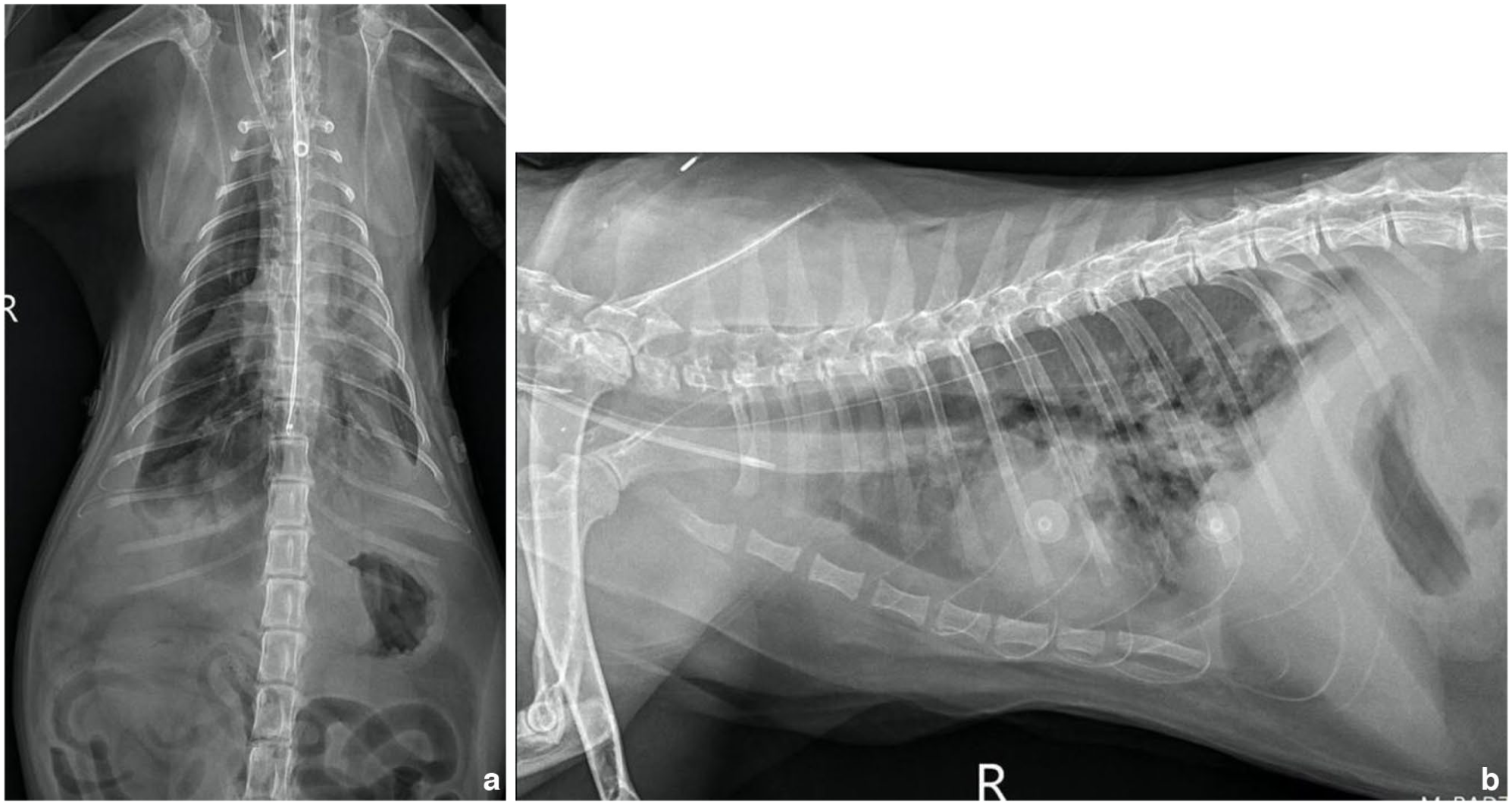
Management of the patient’s respiratory disease is summarized in Figure 2. On day 3, the patient met the criteria for severe ARDSVet II, with bilateral pulmonary infiltrates (Figure 3) and profound hypoxemia (SpO2:FiO2 ratio <200).
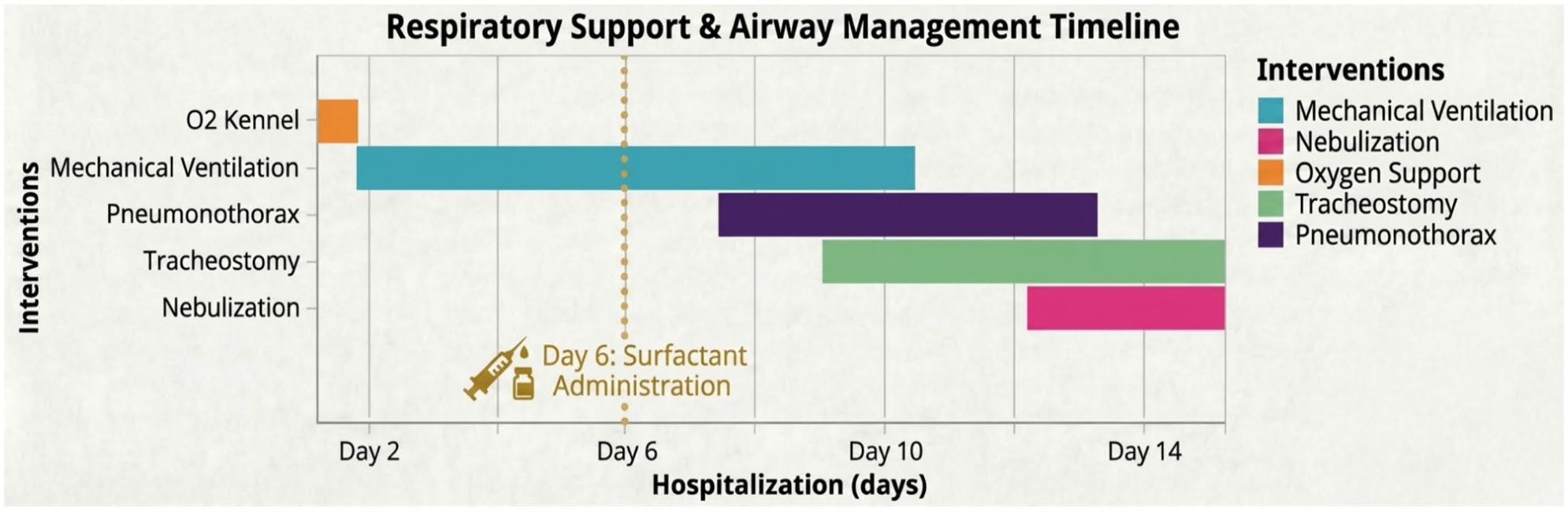
Gantt diagram showing the evolution of respiratory support and interventions from the day of hospital admission (day 1) to the time of patient arrest (day 16)
Day 3: (a) dorso-ventral and (b) right lateral thoracic radiographs showing complete consolidation of the left lung, patchy interstitial to alveolar infiltrates in the right lung and scant pleural effusion
On day 6, the patient had refractory hypoxemia and declining pulmonary compliance. The extra-label use of porcine surfactant (poractant alfa, Curosurf; Chiesi USA), a human licensed product for the treatment of respiratory distress syndrome in premature infants, was discussed as a therapy to help recover lung function and reduce the viscosity of airway secretions. Surfactant was prescribed in accordance with the US Food and Drug Administration regulations 14 and prepared and administered the next day in line with manufacturer recommendations.
The patient was pre-oxygenated with 100% FiO2 and additional sedation provided with propofol titrated to effect to minimize coughing. A dose of 1.5 ml/kg (6 ml total) was administered via a sterile 8 Fr catheter passed through the endotracheal tube. The surfactant was instilled as a single bolus over 60 s followed by manual ventilation. After administration, a transient decrease in tidal volume (from 36 ml to 24 ml) and systemic hypotension (86/42 mmHg) were observed. No bradycardia or desaturation were observed. Transpleural pressure was measured via an esophageal catheter. Pressure readings before and immediately after administration were 10 mmHg and 8 mmHg, respectively.
The airway was suctioned after a 70-min dwell time to restore airway patency. Ventilation parameters before and after surfactant administration are summarized in Table 3. Blood gas values are also summarized in Table 4. Thoracic radiographs obtained 48 h after surfactant (day 8) revealed mild aeration of the previously consolidated left cranial lung lobe (Figure 4).
Ventilation characteristics before and after surfactant administration
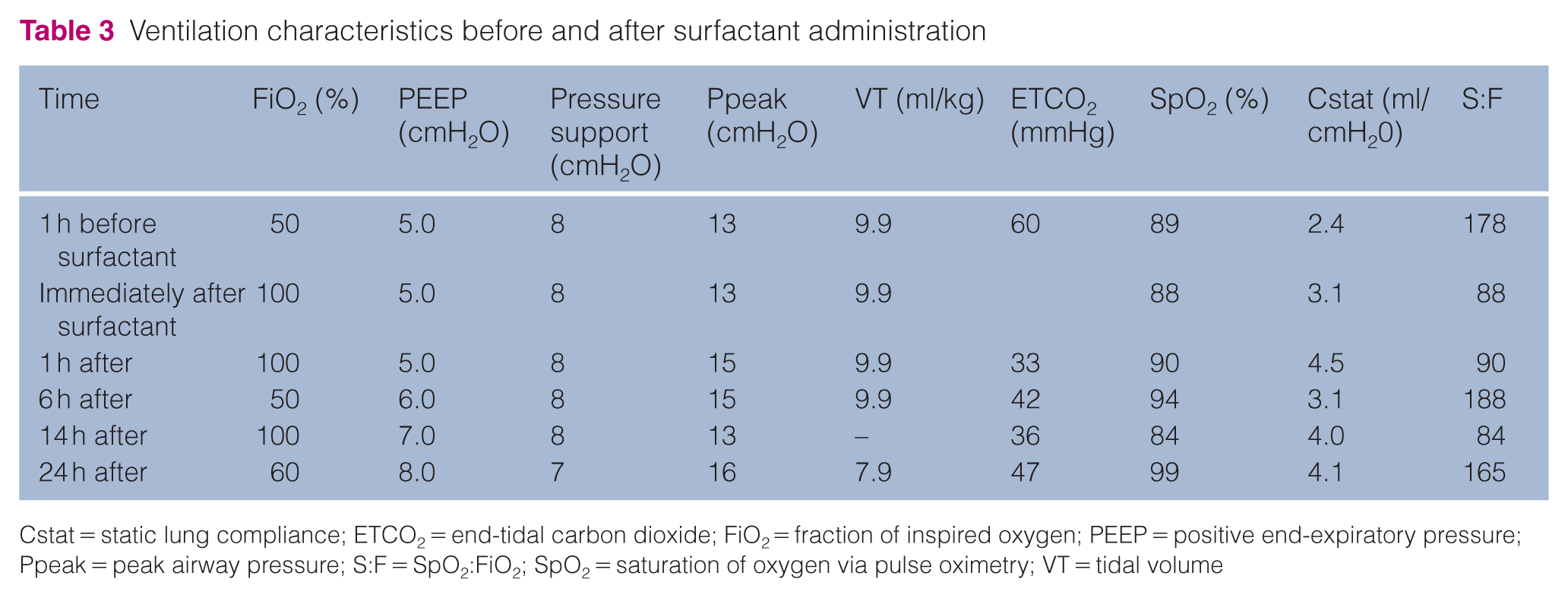
Cstat = static lung compliance; ETCO2 = end-tidal carbon dioxide; FiO2 = fraction of inspired oxygen; PEEP = positive end-expiratory pressure; Ppeak = peak airway pressure; S:F = SpO2:FiO2; SpO2 = saturation of oxygen via pulse oximetry; VT = tidal volume
Blood gas results before and after surfactant administration

ARDS = acute respiratory distress syndrome; HCO3 = bicarbonate; MV = mechanical ventilation; PCO2 = partial pressure of carbon dioxide
Day 8: (a) dorso-ventral and (b) right lateral thoracic radiographs showing mild improvement in aeration of the left lung field 48 h after surfactant administration
Complications and outcome
The patient’s MV was complicated by a pneumothorax on day 7, which was medically managed with bilateral thoracostomy tubes.
A tracheostomy was performed on day 9 as a weaning mechanism to lower sedatives and increase chest wall strength. Successful ventilator weaning was accomplished on day 10. The patient was dependent on the tracheostomy tube because of laryngeal edema and marked inspiratory respiratory effort.
The patient experienced recurrent obstructions of the tracheostomy tube secondary to fibrin and mucus. On day 15, the patient developed acute airway occlusion leading to cardiopulmonary arrest. Resuscitation efforts were unsuccessful owing to stenosis of the tracheal stoma by granulation tissue and fibrin.
Necropsy and histopathological examination of the lungs revealed marked diffuse interstitial pneumonia with type II pneumocyte hyperplasia, alveolar edema and rare fibrin thrombi. There was also marked laryngitis and segmental, ulcerative and fibrinous tracheitis and peritracheitis, with abundant granulation tissue extending to the regional skeletal muscle. A thick firm white plaque of fibrin surrounded the stoma site and extended to the serosa of the esophagus (Figure 5).
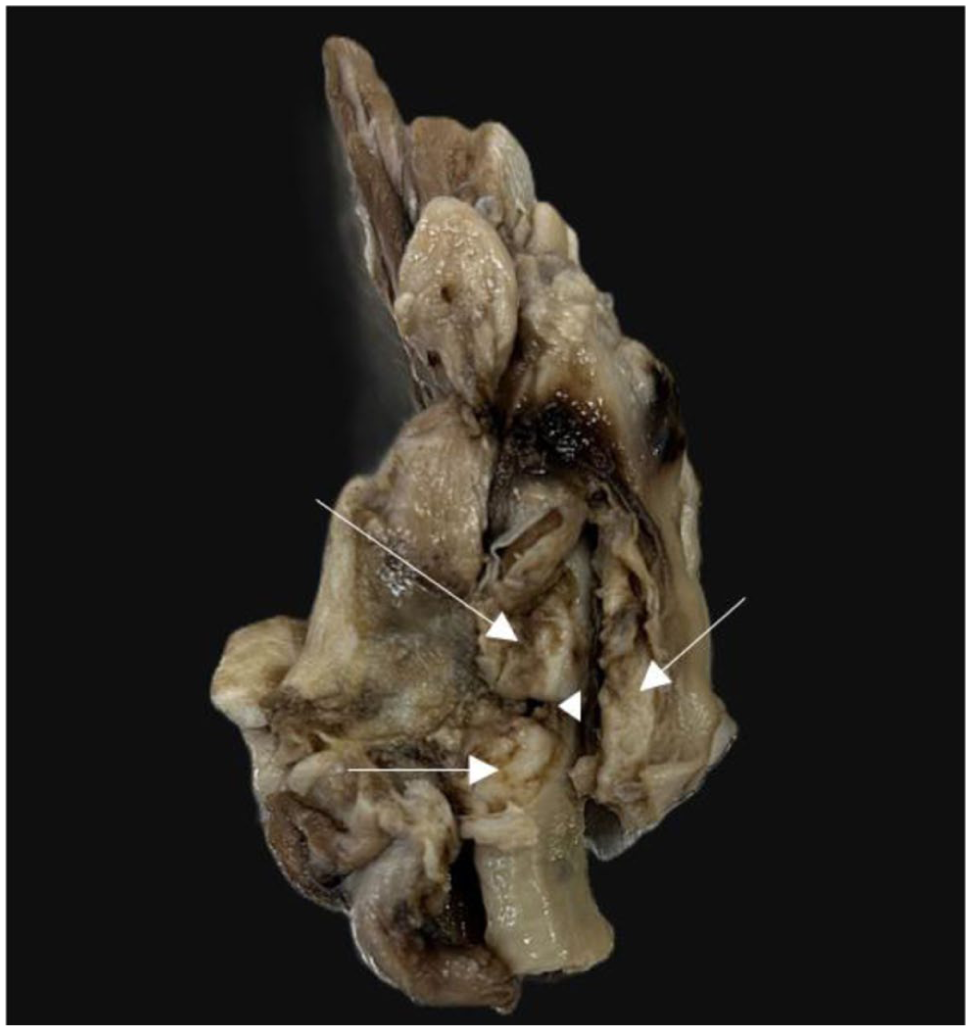
Post-mortem image of the trachea and surrounding structures. The tracheal stoma (arrowhead) was stenotic and surrounded by an extensive fibrinous plaque (arrows)
Discussion
FCV is a common upper respiratory pathogen in cats, which, in rare cases, can develop into viral pneumonia. The diagnosis of calicivirus in this case was based on consistent clinical signs in both the patient and the young housemate and a positive FCV RT-PCR. Thoracic radiographs also showed a diffuse interstitial infiltrate consistent with viral pneumonia.
The cat in this report met the clinical criteria for ARDS based on the acute onset of respiratory failure, bilateral pulmonary infiltrates, severe hypoxemia and absence of cardiogenic causes.8,10 MV is the mainstay of treatment to improve oxygenation and support the work of breathing. Histopathology of the lungs showed type II pneumocyte hyperplasia and fibrin deposits, consistent with interstitial viral pneumonia and the proliferative stage of ARDS.5,7,11,12,15 Previous studies on ARDS report mortality rates in the range of 80–100% for cats. 16
Surfactant was chosen in this case to target the type II pneumocyte destruction reported in FCV.5,12 The rapid increase in compliance seen after surfactant administration was considered a direct effect of the surfactant in lowering surface tension and recruiting alveoli, particularly as the ventilator settings were the same before and after surfactant was given. In human medicine, standard protocols typically leave surfactant in situ. In this case, we employed a suctioning maneuver after a 70-min dwell time due to the hypotension experienced by the patient. This suction modification effectively converted the procedure into a ‘surfactant lavage’. Surfactant lavage has been proven to improve oxygenation in babies by removing inflammatory debris while retaining a therapeutic phospholipid film on the alveolar surface. 17 The sustained improvement in our patient’s pulmonary compliance, despite suctioning, suggests that adsorption of the surfactant occurred during the dwell period.
In this case, the cause of death was the development of fibrinous tracheitis and tracheal occlusion. This was likely caused by a combination of FCV infection and prolonged intubation. FCV has documented tropism for respiratory epithelium 18 and can cause severe fibrinonecrotic tracheitis, 6 characterized by deep mucosal necrosis and fibrin deposition in up to 50% of fatal cases. 19 This is consistent with the large fibrin plaques seen in our patient (Figure 5). Given our experience with this case, we recommend avoiding tracheostomies in FCV cases, if possible, and considering early stoma revision in cats experiencing similar occlusion issues.
Conclusions
Surfactant therapy is not without risk and should be considered an adjunct therapy to improve pulmonary function in feline ARDS. Tracheostomies should be avoided in cases of FCV because of the concern for tracheal necrosis and occlusive fibrin deposits.
Footnotes
Acknowledgements
The authors would like to thank Mary Milewski and Danielle Garrison from Tufts Pharmacy for their help in procuring and advising on the administration of porcine surfactant.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.