
Abstract
Case summary
A 12-year-old male neutered domestic shorthair cat was referred with severe polyphagia, polydipsia, polyuria, weight gain and signs of neurologic disease, including blindness, head tilt, and ataxia. Magnetic resonance imaging (MRI) identified a suprasellar mass consistent with a pituitary macroadenoma. Hypersomatotropism (HST) was diagnosed based on phenotypic changes compatible with acromegaly and an abnormally high serum insulin-like growth factor 1 (IGF-1) concentration (1253 ng/ml). Medical treatment with cabergoline monotherapy (10 μg/kg PO q24h) was prescribed. Progressive improvement of clinical signs was observed, accompanied by a gradual decrease in serum IGF-1 concentrations. Based on clinical and hormonal response, the dosing interval was sequentially extended to q48h and subsequently to q72h. By week 16 of treatment, signs of neurologic disease had resolved and serum IGF-1 concentrations decreased to values within the reference interval (749 ng/ml), while visual deficits persisted. By week 30, signs of neurologic disease remained absent, serum IGF-1 concentration was maintained within the reference interval, and diabetes mellitus did not develop. Cabergoline was well tolerated, with mild gastrointestinal signs reported early in the course of treatment.
Relevance and novel information
This report describes a non-diabetic cat with HST secondary to a pituitary macroadenoma achieving sustained clinical and biochemical control with cabergoline monotherapy. This case demonstrates that a dopamine agonist might be an effective medical option in selected non-diabetic cats with HST, even in the presence of a large pituitary mass and signs of neurologic disease.
Plain language summary
This report describes a cat with a condition caused by a tumor in the pituitary gland, a small structure at the base of the brain. This tumor leads to the body producing too much growth hormone, which can cause increased appetite, excessive drinking and urination, weight gain, and neurologic problems such as balance issues or vision loss. This condition is usually treated with surgery or radiation therapy, but these options were not possible in this case due to limited availability and cost. Instead, the cat was treated with a medication called cabergoline, which is commonly used for other hormonal diseases and is increasingly being explored as a treatment option in cats with this condition. After starting treatment, the cat showed clear improvement. The excessive appetite, drinking and urination decreased, and the neurologic signs resolved over time. Blood tests also showed a marked decrease in the hormone levels associated with the disease. The medication was well tolerated, with only mild and temporary digestive side effects. Although follow-up imaging was not performed, so changes in tumor size could not be confirmed, the clinical and hormonal improvements were maintained over several months. The cat also did not develop diabetes, which is a common complication of this condition. These findings suggest that cabergoline may be a useful treatment option for some cats with this disease, especially when other therapies are not available. More research is needed to understand how this treatment works and which patients are most likely to benefit.
Case description
A 12-year-old neutered male domestic shorthair cat weighing 6.8 kg was referred to the Internal Medicine Service with severe polyphagia, polydipsia, weight gain and signs of neurologic disease, including blindness, head tilt and ataxia. The physical examination revealed a body condition score of 6/9, abdominal enlargement and prognathia inferior. Clinical findings during neurologic examination included ataxia likely due to vestibular involvement, bilaterally absent menace response and delayed proprioceptive placement in all four limbs. Abnormalities were not detected on biochemical analysis, urinalysis and ultrasonographic examination (Table 1). Systolic blood pressure was 136 mmHg (Doppler device). A suprasellar contrast-enhancing mass highly suggestive of a pituitary gland neoplasia, likely a macroadenoma, was identified on MRI, measuring 1.3 × 1.1 × 1.5 cm (length × width × height) (Figure 1). There was no clear evidence of compression of the optic chiasm or the cerebral ventricles. Supportive care during this period included fluid therapy (lactated Ringer’s solution administered subcutaneously) as part of initial stabilization. The cat remained clinically stable and was subsequently managed on an outpatient basis. Prednisolone was initiated at a dose of 0.25 mg/kg PO and administered for 7 days, following recommendation from the neurology service due to concern for peritumoral inflammation and/or cerebral edema associated with the pituitary macroadenoma, after which it was discontinued.
Clinicopathologic findings and hormone analysis at hypersomatotropism (HST) diagnosis and during cabergoline treatment

ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; IGF-1 = insulin-like growth factor 1; RI = reference interval; TT4 = total thyroxine; UCCR = urinary cortisol:creatinine ratio
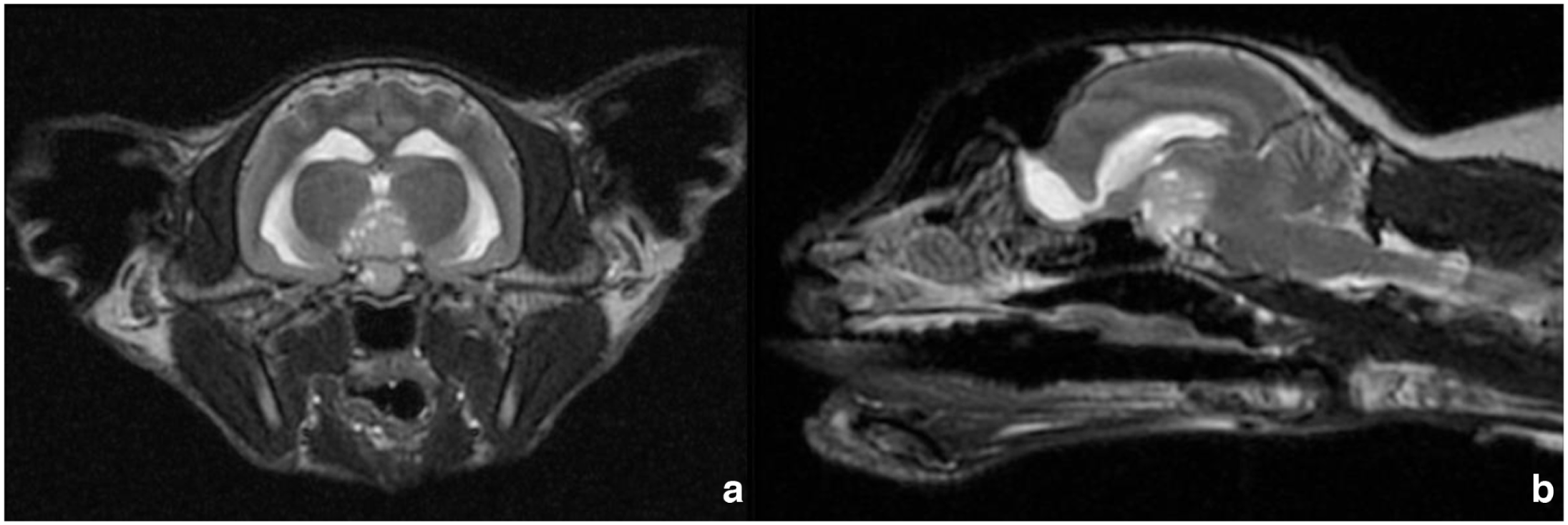
Suprasellar mass, highly suggestive of a pituitary gland neoplasia, likely a macroadenoma, on MRI (cross section, 1.3 × 1.1 × 1.5 cm): (a) transverse and (b) sagittal view. Hyperintense regions within the mass most likely represent intratumoral degenerative or necrotic changes, although hemorrhagic components cannot be excluded
Hypersomatotropism (HST) was suspected based on clinical signs compatible with growth hormone (GH) excess, as well as the space-occupying neurologic effects of the pituitary tumor. Serum insulin-like growth factor 1 (IGF-1) concentration was measured using a commercially available chemiluminescence assay (IDEXX Laboratories; referral test performed at Michigan State University). The assay had been recently updated with a change in units (from nmol/l to ng/ml), resulting in revised reference intervals (RIs); therefore, all values were interpreted according to the updated RI provided by the laboratory. Given the presence of the pituitary mass, the serum IGF-1 concentration above the RI and the phenotypic changes compatible with acromegaly, HST was diagnosed. Fasting blood glucose concentration was normal (6 mmol/l) and serum fructosamine concentration was within the RI (253 μmol/l, RI 200–380).
An oral dose of cabergoline (10 μg/kg q24h, Dostinex; Pfizer) was prescribed.1,2 Follow-up was initially weekly and then monthly. Assessment included physical examination, serum IGF-1 measurements, routine blood tests and urinalysis.
During week 4 of cabergoline treatment, polyphagia, polydipsia and polydipsia were reduced and serum IGF-1 concentrations had decreased (950 ng/ml). Since the signs of neurologic disease gradually improved and serum IGF-1 concentrations progressively decreased, the dosing interval of cabergoline administration was progressively extended. The frequency was modified from q24h to q48h at week 5 (Table 1). During week 8 of cabergoline treatment, the cat’s head tilt was reduced and serum IGF-1 concentrations showed a progressive decrease (829 ng/ml), although it remained above the RI. The frequency of cabergoline administration was changed from q48h to q72h at week 13. The clinical signs of neurologic disease, particularly the head tilt and ataxia, showed a clinical resolution by week 16, when serum IGF-1 concentrations were within the RI (749 ng/ml). The cat remained blind and did not recover its menace response. On week 30 of cabergoline treatment, systemic clinical signs (polyphagia, polydipsia, polyuria and weight gain) and vestibular deficits remained absent, while serum IGF-1 concentration was maintained within the RI (703 ng/ml).
A potential adverse effect of cabergoline was observed in week 4, when the cat developed a short episode of gastrointestinal signs, characterized by mild vomiting and decreased appetite for approximately 48h. These signs resolved rapidly with symptomatic therapy and did not require a discontinuation or dose reduction of cabergoline.
The cat did not develop diabetes mellitus (DM) at any time during the 30-week follow-up period, as documented by the absence of hyperglycemia or glucosuria, and serum fructosamine concentrations were within the RI, according to the Agreeing Language in Veterinary Endocrinology (ALIVE) criteria for the diagnosis of DM. 3
Discussion
This case report describes a non-diabetic cat with HST presenting signs of neurologic disease associated with a pituitary macroadenoma. Cabergoline treatment was associated with clinical improvement, including resolution of neurologic signs, together with a decrease in serum IGF-1 concentrations to values within the RI under a progressively extended dosing interval.
HST, or acromegaly, is a neuroendocrine disease caused by hypersecretion of GH. In the domestic cat (Felis catus), HST is caused either by a functioning adenoma or hyperplasia of the somatotropic cells of the pituitary gland. 4 HST is commonly described in cats with concurrent DM, with prevalence rates in the range of 12–25%.5 –8 HST can also develop in cats without DM; a few case reports have been published to date.9 –11 A recent case series of 28 non-diabetic cats with HST reported that 93% of cases were males and 68% of cases presented with phenotypic changes consistent with acromegaly, similar to the cat in this report. 12 Likewise, non-diabetic cats with HST have been described by performing serum IGF-1 screening in cats with chronic kidney disease as well as in overweight or obese cats, suggesting that HST is likely underdiagnosed when DM is not present.13,14
Cabergoline is a dopamine agonist with a high affinity for dopamine receptor 2 (D2R). In humans with acromegaly, cabergoline monotherapy is mainly indicated in patients with mildly to moderately high serum IGF-1 concentrations, either as a first- or second-line treatment. Cabergoline achieves biochemical control in approximately 35% of these cases.15,16 In diabetic cats with HST, one study from Argentina (n = 23) reported that cabergoline improved diabetic control and is associated with normalization of serum IGF-1 concentration and diabetic remission in 26% and 35% of cats, respectively.1,2 In a pilot study from the UK (n = 9), cabergoline did not normalize serum IGF-1 concentrations or improve diabetic control. 17 Differences in therapeutic responses could be due to pituitary tumor size, the existence of various somatotropinoma subpopulations, regional variants of HST, different dosing regimens, sample size and commercial preparations of cabergoline used.1,17 In non-diabetic cats with HST, studies are lacking; in a pilot study, cabergoline monotherapy reduced serum IGF-1 concentrations in 44% and 33% of non-diabetic cats with HST at 3 and 6 months, respectively. 18 In the cat in this case report, a progressive decrease in serum IGF-1 concentrations was observed, with values within the RI by week 16 and maintained within the RI by 30 weeks.
D2R expression is demonstrated in the pituitary gland of diabetic cats with HST. A moderate negative correlation between pituitary size and D2R expression is described. 4 Diabetic cats with a relatively small pituitary tumor and serum IGF-1 concentrations below 1500 ng/ml appear to potentially have the best response to cabergoline. 1 Likewise, cats that achieved diabetic remission have relatively smaller pituitary sizes than those that did not achieve remission.¹ In the present case, on MRI the pituitary lesion was likely a macroadenoma, yet the IGF-1 concentration at diagnosis (1253 ng/ml) was below 1500 ng/ml, which might have contributed to the good hormonal response despite the large tumor size and advanced signs of neurologic disease.
MRI showed a large, strongly contrast-enhancing mass centered over the pituitary fossa. The rostral aspect of the mass approached, but did not definitively involve the optic chiasm, while the dorsal aspect was immediately ventral to the lateral ventricles without obvious compression. This anatomic relationship provides a plausible explanation for the visual deficits observed, as functional compromise of the optic pathways can occur even in the absence of overt evidence of severe compression. However, the visual deficits may not have been solely attributable to direct compression, and alternative mechanisms such as vascular or ischemic events affecting the optic pathways cannot be excluded. Intratumoral degenerative, necrotic or hemorrhagic changes may also have contributed to the neurologic presentation. No definitive evidence of cavernous sinus involvement was identified on the available imaging. Central diabetes insipidus was considered a possible differential diagnosis for the polyuria and polydipsia in the context of a pituitary macroadenoma and neurologic involvement; however, this was not further investigated. Although there is evidence that cabergoline may reduce serum IGF-1 concentrations and improve metabolic control in a subset of cats with HST,1,2 there is limited evidence to support a direct effect of cabergoline on neurologic or vestibular signs. Improvement in these signs may therefore reflect overall clinical stabilization or the self-limiting nature of vestibular disorders, rather than a reduction in pituitary mass size or a direct structural effect on the optic pathways. In this cat, head tilt and ataxia resolved during cabergoline treatment, and the owner reported improved navigation at home with fewer collisions, although menace response remained absent on neurologic examination, suggesting partial functional adaptation rather than complete restoration of vision.
The relatively high initial cabergoline dosage used in this case (10 μg/kg PO q24h) and the subsequent extension of the dosing interval (to q48h and then q72h) suggest that individualized titration based on clinical and hormonal response might be a useful strategy in some cats with HST and macroadenomas.1,2,17 In this cat, clinical and biochemical control were maintained despite lengthening the dosing interval, which could be clinically relevant in terms of treatment cost, owner compliance and potential long-term adverse effects.1,2 Apart from a short, self-limiting episode of mild gastrointestinal disease early in the course of therapy, cabergoline was well tolerated.
This case report has several limitations. Histopathologic confirmation of the pituitary lesion was not obtained, and no follow-up MRI was performed due to owner decision; therefore, the effect of cabergoline on tumor size could not be assessed. In addition, continuous glucose monitoring was not performed, which would have allowed a more exhaustive assessment of glycemic variability and detection of potential transient dysglycemic episodes. More specific tests to characterize a potential prediabetic state, such as an oral or intravenous glucose tolerance test, were also not undertaken. Finally, as a single case report, the observations described should be interpreted within the inherent constraints of an individual case.
Conclusions
This case describes a non-diabetic cat with HST secondary to a pituitary macroadenoma who showed a favorable clinical and hormonal response to cabergoline. Treatment was associated with resolution of neurologic signs and serum IGF-1 concentrations within the RI under a progressively extended dosing interval. Cabergoline appears to be a safe and potentially effective medical option for selected non-diabetic cats with HST and pituitary macroadenoma when other therapies are unavailable or declined. Further research is warranted to establish optimal dosing regimens, define predictors of response, evaluate long-term outcomes and explore whether combination protocols might enhance the effectiveness of cabergoline in cats with HST.
Footnotes
Conflict of interest
The authors declared no conflicts of interest with respect to the authorship, research and publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.