
Abstract
Case summary
A 9-year-old, male castrated domestic shorthair cat was presented for evaluation of progressive right pelvic limb lameness. Orthopedic examination revealed a weightbearing lameness of the right pelvic limb and a mass over the medial aspect of the right stifle, which elicited pain upon palpation. Preoperative complete blood count and serum biochemistry panel were unremarkable. Radiographs and CT identified a mass at the level of the distal femur, with focal mineralization and enlargement of the right semimembranosus muscle. Incisional biopsy suggested osteochondroma, osteochondromatosis and chondroma. The mass was marginally excised, with histopathology consistent with an intramuscular osteochondroma. The cat returned to normal activity and is currently healthy and alive 3 years postoperatively without evidence of recurrence.
Relevance and novel
information Soft tissue osteochondroma is a rare condition that can occur intramuscularly, and to the authors’ knowledge, this condition has not been previously reported at this location in a feline patient. Based on this report, although considered rare, clinical awareness of this tumor may aid practitioners in identifying intramuscular osteochondroma as a differential for firm intramuscular masses. Intramuscular osteochondroma carries a fair-to-good prognosis dependent on the location in an otherwise clinically healthy cat.
Plain language summary
A 9-year-old cat developed progressive lameness of one hindleg. No history of trauma was reported and the cat was otherwise healthy. During examination, a mass was palpated on the back of the right knee. Radiographs and CT scan showed a mass with mineralization in one of the hamstring muscles (semimembranosus). A biopsy was consistent with a benign tumor, and surgical removal was elected. The mass was removed along with a small portion of muscle. Analysis of the mass confirmed a benign tumor made of bone and cartilage (an osteochondroma). The cat recovered well and returned to normal activity. This case is important as it is the first to describe a rare tumor in cats that is not often considered in differential diagnosis. The long-term outcome can be good when identified and removed early in healthy patients.
Keywords
Case description
A 9-year-old, male castrated domestic shorthair cat was presented for evaluation of right pelvic limb lameness. The patient had no prior history of trauma or other orthopedic issues. Initial evaluation at the primary veterinarian revealed a firm mass at the level of the right distal femur. Lameness at the time of presentation was moderate.
Pelvic limb radiographs showed a soft tissue mass containing a 0.5 cm mineral density at the level of the right distal femur. Hematology and biochemistry revealed mild neutropenia; all other parameters were within normal limits. The patient tested negative for feline leukemia virus (FeLV) and feline immunodeficiency virus. An incisional biopsy of the mass was performed under sedation with an intramuscular injection of 29 μg/kg medetomidine, 0.5 mg/kg butorphanol and 2.9 mg/kg ketamine. Histopathology of the mass revealed a proliferative cartilaginous nodule; differential diagnosis included osteochondroma, osteochondromatosis and chondroma.
On presentation to the oncology service at the referral teaching hospital, the cat was bright, alert and responsive, with a body condition score of 7/9. All vital parameters were within normal limits. A CT scan of the cat’s right pelvic limb was performed for further characterization of the location and invasiveness of the mass. The CT showed focal mineralization and enlargement of the right semimembranosus muscle (caudal muscle belly, distally) (Figures 1 and 2). A small osseous fragment was identified within the right stifle joint, with no evidence of associated degenerative joint disease (Figure 3). Preoperative thoracic radiographs were recommended but declined by the owners. The cat was then transferred to the surgery service for excision of the mass.
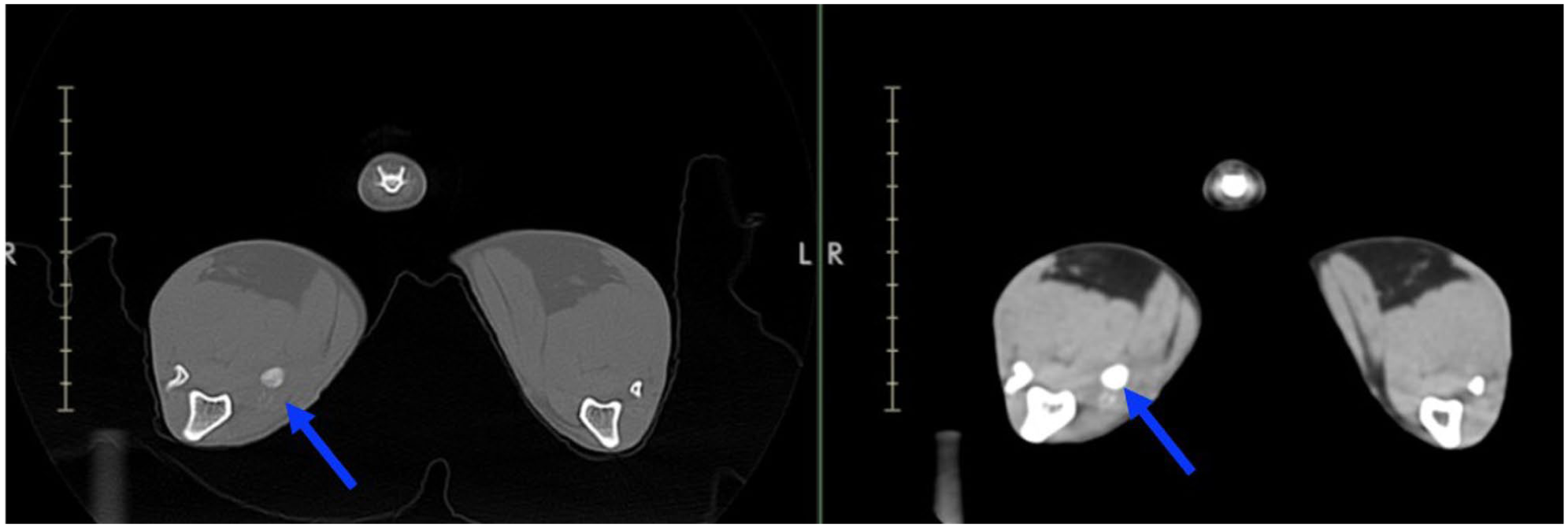
Right pelvic limb CT images in a transverse view. The blue arrow indicates a mass effect with focal hyperattenuation
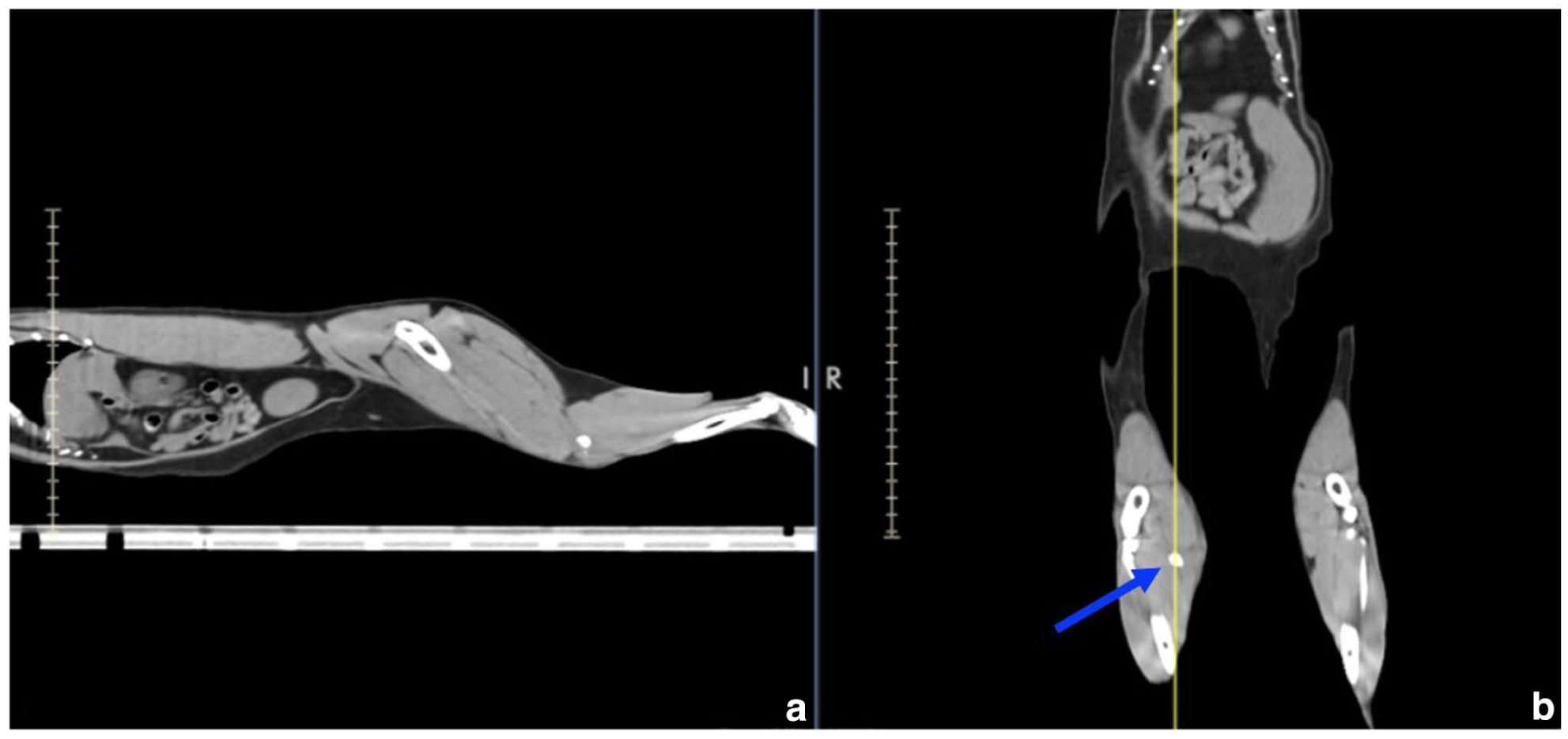
Right pelvic limb CT images in (a) sagittal and (b) dorsal views. The blue arrow indicates a mass effect with focal hyperattenuation

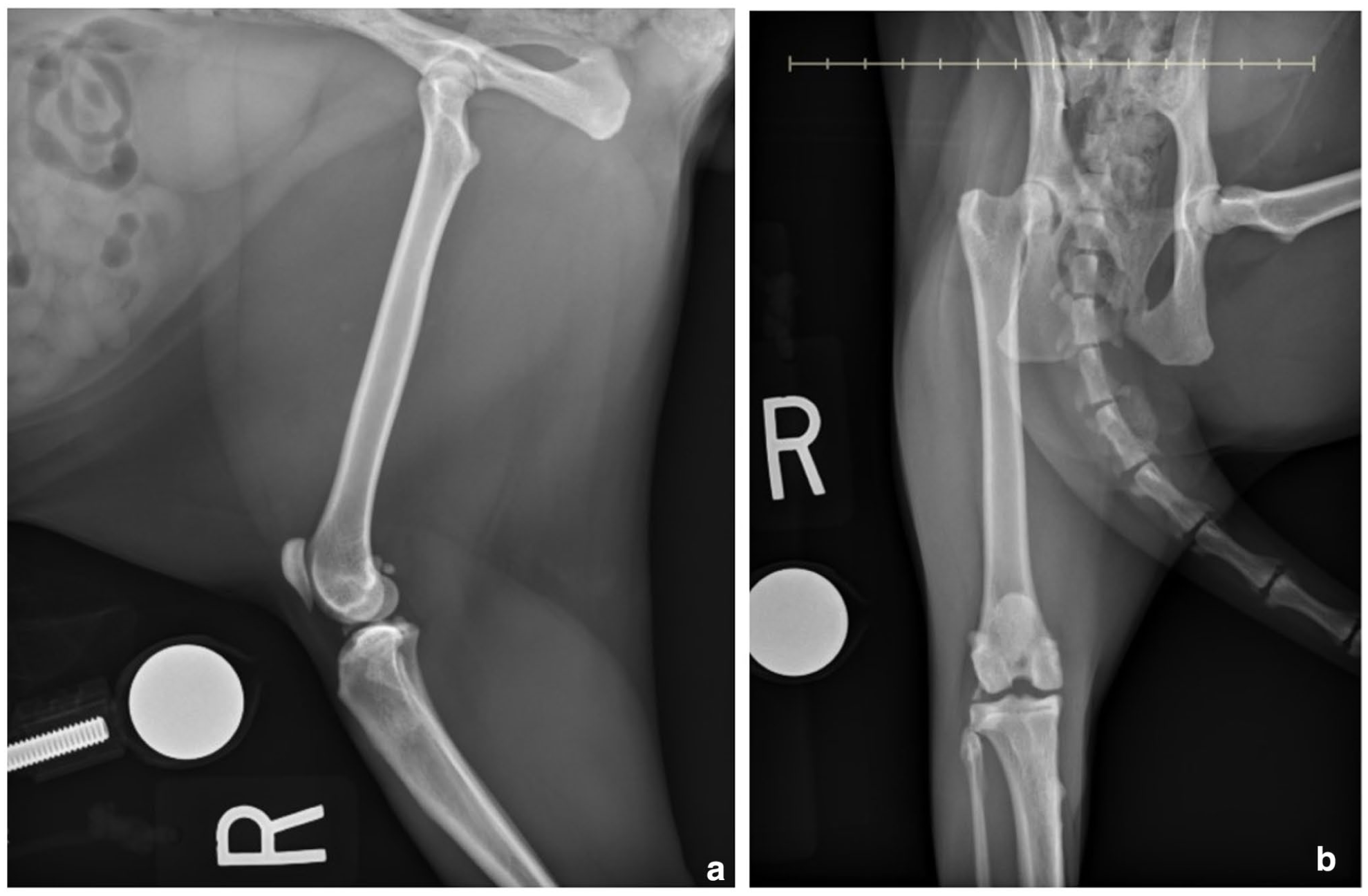
(a) Lateral and (b) ventrodorsal radiographs of the right pelvic limb. The focal radio-opaque lesion with mass effect associated is observed caudal and medial to the proximal tibia, respectively
A firm mass, approximately 4 cm in size, was palpable medial to the right stifle. The cat was uncomfortable on palpation of the mass. Orthopedic examination revealed a moderate weightbearing lameness of the right pelvic limb, with a shortened stride. During the swing phase of stride, internal rotation of the stifle and external rotation at the tarsus were observed. During the stance phase, there was a slight correction of limb rotation. There was decreased extension and flexion of the right stifle. The rest of the orthopedic and neurological examinations revealed no abnormalities.
Preoperative complete blood count revealed mild lymphopenia (0.882 × 103/μl, reference interval [RI] 1.5–6). The remaining parameters were within normal limits. Serum biochemistry was clinically unremarkable, with only a mild hypernatremia (157 mEq/l, RI 143–155). The patient was assessed to be American Society of Anesthesiologists (ASA) I for general anesthesia. The patient was anesthetized with a premedication of dexmedetomidine (5 μg/kg IM) and hydromorphone (0.1 mg/kg IM). The cat was induced with propofol (3.4 mg/kg IV) and anesthesia was maintained with isoflurane. A sacrococcygeal epidural block was performed. A first-generation cephalosporin, cefazolin sodium (22 mg/kg IV) with Gram-positive coverage for clean surgical procedures, was administered at the time of induction and repeated every 90 mins intraoperatively. Antibiotics were discontinued postoperatively in accordance with antimicrobial stewardship principles. The patient was surgically prepared in left lateral recumbency using a hanging limb technique. A medial approach was made to the distal femur and proximal tibia with a 10 cm skin incision extending just distal to the ischiatic tuberosity to the proximal tibia. Hemostasis was maintained with monopolar electrocautery. The mass was palpated within the semimembranosus muscle caudomedial to the tibia. The semimembranosus muscle was elevated off the medial aspect of the tibia. Stay sutures were placed in the distal margin of the mass to assist surgical manipulation and aid orientation for histopathology. The mass was localized to the semimembranosus muscle and dissected from surrounding tissues using a combination of blunt and sharp dissection. There was a small area of focal adherence of the gracilis muscle to the mass, which was suspected to represent the previous biopsy tract. The adhered overlying gracilis muscle was excised en bloc (approximately 5 × 2 × 1 cm) along with the primary mass. The surgical site was lavaged routinely. The remaining gracilis was sutured to the sartorius using 3-0 PDS (PDS II; Ethicon). The subcutaneous tissues were apposed using 4-0 Monocryl (Monocryl; Ethicon) with tacking bites to the deep muscle layer to eliminate dead space. A Nocita (Nocita; Aratana) incisional block was performed. The skin was closed with 4-0 Ethilon (Ethilon; Ethicon) in a Ford-interlocking pattern. The patient recovered from general anesthesia uneventfully. The mass was submitted for histopathology.
The cat was monitored in the intensive care unit for 1 day postoperatively. Supportive care included intravenous fluid therapy at a maintenance rate, analgesia with opioid therapy (methadone at 0.2 mg/kg IV q6h) and robenacoxib (1 mg/kg PO q24h). On the following day, the patient was assessed to be comfortable and was discharged home with robenacoxib (1 mg/kg PO q24h for 2 days) and buprenorphine (0.02 mg/kg sublingual q8–12h for 5 days).
The histopathology results were consistent with an osteochondroma within the right semimembranosus muscle with marginal excision of the mass. The distal margin was 3 cm and the proximal margin was 2.5 cm; however, the mass abutted the medial and lateral margins. The lateral and medial margins were considered to be incompletely resected; although no neoplastic cells were visible within those margins, the surgical margins were narrow (<1 mm). At 18 months postoperatively, the cat presented for a recheck. Physical examination revealed a mild right pelvic limb lameness. Radiographs of the limb did not show any evidence of local recurrence (Figure 4). Further imaging was not pursued owing to financial constraints.
Postoperative radiographs of the right pelvic limb after 18 months: (a) lateral and (b) ventrodorsal. No lesions are apparent
At the time of case writing, the cat was reported to be doing well at home, with static mild weightbearing lameness on the right pelvic limb that has not changed in the past 3 years. The cat has resumed near normal limb function without any activity limitations. There was no evidence of local recurrence based on clinical evaluation or radiographic assessment.
Discussion
The primary clinical finding in this case was progressive weightbearing lameness and pain on palpation of an intramuscular mass in an otherwise healthy cat. Osteochondromas are benign growths; however, in cats, they can show progressive enlargement and, depending on the location, can lead to pain, dyspnea, stridor, lameness, decreased range of motion or even neurological deficits.1–3 Lameness in adult cats is less commonly documented when compared with dogs. 4 Common differentials for lameness in cats include trauma, neurological disease, degenerative joint disease and systemic illness. 4 To the best of the authors’ knowledge, intramuscular osteochondroma of the semimembranosus muscle in cats has not been reported, and nor has it been identified as the sole cause of lameness in cats. In humans, osteochondromas are the second most common benign tumor and arise from the metaphysis of long bones, with the majority arising from growth plate cartilage.5,6 Soft tissue osteochondromas are defined as benign tumors containing bone and cartilage that exist in mesenchymal tissues with no connection to adjacent bone, cartilage or periosteum. 7 Soft tissue osteochondromas are rare but have been reported in humans. Current reports on soft tissue osteochondromas include tumors of the submandibular, metatarsal, elbow and heel pad regions.5–8
There is no consistently effective treatment for feline osteochondroma, although surgical excision has been reported to result in good outcomes even with marginal excision.9,10 Recurrence has also been described even after complete mass removal. 11 There are also rare reports of osteochondroma transformation into malignant tumors such as osteosarcoma or chondrosarcoma.12–14 Overall, the prognosis of feline osteochondroma is guarded to grave, with a life expectancy of less than 1 year after the onset of clinical signs because of the risks of malignant progression, recurrence or multifocal lesions.15,16
Based on the cat’s rapidly progressive clinical signs and no previously reported case in such a location in the species, the patient was considered to have an unknown prognosis by the primary clinician. Given the absence of local metastasis or other systemic disease, and the cat’s mass was largely contained within one muscle body, specifically within the semimembranosus muscle, surgical resection was still a feasible option. If the mass had been more invasive or expansile in nature, surgical excision would not have been an option.
Amputation had also been discussed with the owners; however, a marginal excision had been elected. Given the rapid growth rate of the mass – from 1 × 3 cm to 2 × 5 cm within 41 days – excision may not have been feasible if treatment had been delayed. Marginal excision appears to have been sufficient for this cat; however, without advanced diagnostic imaging, recurrence cannot be confirmed definitively.
The histological finding of the mass within the right pelvic limb musculature was consistent with an osteochondroma. Although most osteochondromas are reported to be painless,1,2 the palpated pain in this case was likely from mechanical impingement that could have compressed adjacent structures. It remains unknown where the cartilaginous mass originated, as no parent bone was identified; there was no appreciable attachment grossly or microscopically to the bone, cartilage or periosteum. Rarely, proliferation of cartilage can occur in soft tissues associated with joints such as synovial osteochondromatosis, which is not believed to be the case in this study as the mass was not close to a joint. 2 The cause of osteochondroma remains unknown; however, it has been reported that feline osteochondroma has been associated with FeLV and feline sarcoma virus infection.17,18 The significance of these viruses in the development of osteochondromas has not yet been determined.16,19 In this case, the patient was FeLV negative. Further studies to identify potential causes and predispositions of the disease will be beneficial.
The mass was successfully excised without major impairment of gait, although the lameness did not fully resolve, likely because of the extensive muscle resection. The persistent lameness is likely caused by the absence of part of the hamstring muscles. In our case, excision of the muscle was unavoidable because of the location of the mass and adhesions noted intraoperatively. In a human case report, the absence of the semimembranosus muscle was compensated for by unconventional recruitment of the semitendinosus and biceps femoris muscles during gait, which mimic the function of the semimembranosus muscle. This gait adaptation could potentially be expected over time, especially if physical therapy had been pursued postoperatively. 20 Overall, the client was pleased with the outcome and the patient’s recovery. Based on communication with the owner, the cat resumed his normal life once recovered from surgery, and no other concerning signs were reported.
Conclusions
This case report discusses intramuscular osteochondroma as a differential cause of lameness in an adult cat. Soft tissue osteochondromas are benign tumors that can cause clinically significant lameness. Intramuscular osteochondromas can have a fair to good prognosis when diagnosed and excised in a timely manner, even when only marginal excision is performed. Although considered rare, increased clinical awareness about this tumor is warranted.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.