
Abstract
Case summary
A 4-year-and-8-month-old, neutered male American Shorthair cat presented with acute hindlimb paralysis and was diagnosed with aortic thromboembolism (ATE) secondary to hypertrophic cardiomyopathy. Despite initial treatment, the cat developed anuric acute kidney injury (AKI), possibly due to ischaemia-reperfusion injury. As referral for haemodialysis was declined, peritoneal dialysis (PD) was initiated using a closed round drainage catheter and manually performed exchanges. Although serum creatinine levels continued to rise during PD, the cat remained clinically stable, and urination resumed on day 8 of PD (day 15 of hospitalisation). The cat was discharged on day 21 with marked improvement in renal parameters and remained stable without recurrence at follow-up.
Relevance and novel information
This case represents a rare report of a cat that developed anuric AKI after ATE and survived to discharge through PD with almost normalised renal values, despite an initial lack of improvement lasting for several days. A number of challenges were encountered, including the lack of standardised feline PD protocols, difficulty in evaluating dialysis efficacy and absence of guidelines for the optimal duration of PD in anuric patients. Despite these limitations, intensive supportive care and continued PD led to favourable clinical outcomes. This case highlights the potential role of PD as a life-saving renal replacement therapy in feline patients with thromboembolism-induced AKI when haemodialysis is unavailable.
Plain language summary
This report describes a cat that developed kidney failure after a blood clot blocked the main artery to its hindlimbs, a condition known as aortic thromboembolism. The cat was unable to produce urine for several days, indicating severe kidney damage. Because haemodialysis (using a machine to purify the patient’s blood outside of its body) was not available, peritoneal dialysis (PD) (infusing fluids into the patient’s abdomen to purify the blood) was performed using a simple drainage tube placed in the abdomen. Although kidney values initially worsened, the cat remained stable, and urine production resumed after 8 days of PD. The cat eventually recovered and was discharged in good condition. This case shows that PD can serve as a life-saving treatment option for cats with kidney failure caused by blood clots, especially when more advanced dialysis equipment is not available.
Keywords
Introduction
Hypertrophic cardiomyopathy (HCM) is a major predisposing factor for feline aortic thromboembolism (ATE), 1 which may cause severe peripheral ischaemia and reperfusion injury leading to multiorgan dysfunction. 2 Acute kidney injury (AKI) is a recognised complication of ATE,2,3 and progression to oliguria or anuria carries a grave prognosis; however, detailed descriptions of clinical course and management remain limited. Peritoneal dialysis (PD) is an established renal replacement therapy for feline AKI; 4 however, to the best of the authors’ knowledge, its use in anuric AKI associated with ATE has not been reported. Here, we report a cat with severe oliguric–anuric AKI after ATE that survived to discharge after PD.
Case description
A 4-year-and-8-month-old, neutered male American Shorthair cat presented to a veterinary emergency service (day 0) with acute hindlimb paresis, vocalisation and tachypnoea. Clinical signs developed acutely and the cat was presented 1 h after onset. The cat had no prior clinical abnormalities but had a history of ureterolithiasis. On physical examination, body weight was 4.2 kg and rectal temperature was 37.0°C. Both hindlimbs were non-ambulatory and cold to the touch, with femoral pulses weak and difficult to palpate bilaterally. Heart rate was 180 beats/min; no murmur or gallop rhythm was detected. Marked agitation limited handling, and respiration was characterised by panting. After sedation (midazolam 0.2 mg/kg IM and butorphanol 0.2 mg/kg IM), echocardiography and blood tests (via forelimb sampling) were performed by an experienced clinician. Echocardiography revealed interventricular septal thickening (IVSd 7.2 mm) just below the aortic valve and left atrial enlargement (left atrial diameter 16.3 mm; left atrium:aorta ratio 1.75), with no structural cardiac abnormalities identified. Creatine phosphokinase was elevated at 1174 IU/l (reference interval [RI] 87–309). Blood urea nitrogen (BUN), creatinine (Cre) and potassium concentrations were 31.3 mg/dl (RI 5.0–32.8), 1.83 mg/dl (RI 0.8–2.4) and 3.5 mEq/l (RI 3.4–4.6), respectively (Figure 1). Blood glucose levels differed between the forelimb and hindlimb (208 vs 113 mg/dl), suggesting hindlimb perfusion impairment. Abdominal ultrasonography identified an intraluminal structure within the abdominal aorta distal to the renal arteries, consistent with thrombus, with absence of blood flow at that site. Based on these findings, a diagnosis of ATE associated with suspected HCM was made. Thoracic ultrasonography revealed no pleural effusion or pulmonary oedema; however, furosemide (1 mg/kg IV) was administered prophylactically. Fentanyl (3 µg/kg/h constant rate infusion) was initiated for analgesia, and anticoagulant therapy with dalteparin (100 IU/kg SC q12h) was started. Fentanyl resulted in marked stabilisation of behaviour and respiratory status. On day 1, fentanyl was discontinued and replaced with buprenorphine (0.02 mg/kg IV q12h).

Changes in blood urea nitrogen (BUN), creatinine (Cre) and serum potassium (K+) levels during hospitalisation. BUN values exceeded the upper detection limit of the analyser (⩾140 mg/dl) from day 5 to day 16. Peritoneal dialysis (PD) was initiated on day 7 and continued for 10 days. Although BUN remained above measurable limits during PD, potassium values fluctuated and occasionally reached critical levels. Glucose–insulin therapy was administered at the time points indicated by red markers. Renal parameters began to improve after urination resumed on day 15. Reference intervals used by the laboratory (FUJIFILM DRI-CHEM NX500V IC) were as follows: BUN 5.0–32.8 mg/dl, creatinine 0.8–2.4 mg/dl, potassium 3.4–4.6 mEq/l.
From day 2 onwards, BUN, Cre and potassium concentrations showed a progressive increase, and by day 6, the absence of urine within the bladder was confirmed, leading to a diagnosis of severe oliguric–anuric AKI (Figure 1). Ureteral obstruction, renal infarction and myoglobinuric renal injury were considered unlikely based on ultrasonographic findings and urine colour. Management during this period consisted solely of intravenous fluid therapy aimed at maintaining renal perfusion, with lactated Ringer’s solution administered at 2.3 ml/kg/h. Given the underlying cardiac disease, left atrial size and the presence of pleural effusion and pulmonary oedema were assessed using ultrasonography; however, adequate evaluation was not possible on some days owing to the patient’s temperament.
As the owner declined referral for haemodialysis, a peritoneal catheter was placed on day 7. A closed round drain (Kirikanyoko silicone round drain; Kaneko Chemical; 10 Fr catheter, 1.5 mm × 3.3 mm trocar) was selected. Anaesthesia was induced with alfaxalone to effect and lidocaine (2 mg/kg) was locally injected at the planned incision site. To reduce the risk of hyperkalaemia-associated intraoperative arrhythmias, calcium gluconate (Calchicol 8.5% 1 ml/kg IV, diluted two- to three-fold) was administered. Ampicillin (20 mg/kg IV) was administered as an antimicrobial agent. A midline laparotomy was performed. The catheter was introduced into the peritoneal cavity and advanced along the abdominal wall, with the catheter tip positioned on the diaphragmatic surface of the liver. A trocar was passed through the abdominal wall 2–3 cm to the right of the incision site and a subcutaneous tunnel 4–5 cm cranially was created from this exit point; the catheter was then secured to the skin using a Chinese finger-trap suture. A brief episode of ventricular tachycardia occurred intraoperatively without hypotension and required no intervention. Postoperative analgesia consisted of buprenorphine (0.02 mg/kg IV q12h) for 3 days. Ampicillin (20 mg/kg IV q12h) was continued until completion of PD.
PD was initiated after postoperative stabilisation. A commercially available dialysate (Mid-Peric; Terumo) was used with dextrose concentrations of 1.35%, 2.5% and 4.0%. The initial dialysate concentration was selected as 2.5% to balance solute clearance and ultrafiltration while minimising adverse effects. When body weight increased, 4.0% dialysate was used intermittently. The 1.35% solution was used only after the onset of urination and was not administered during the anuric phase. The intraperitoneal instilled volume was 20–30 ml/kg per exchange and dwell time was typically 1 h, extended up to 5 h overnight when staffing was limited. Exchanges were performed 4–10 times/day depending on clinical status. The system was not a fully closed circuit, and drainage was performed manually using a 50 ml disposable syringe (Terumo) while wearing disposable gloves. As a result of incomplete medical record documentation, quantitative assessment of recovery efficiency was not possible retrospectively.
From day 13 onwards, Cre showed a decreasing trend; however, renal parameters overall continued to increase during PD (Figure 1). Potassium concentrations were unstable, and glucose–insulin therapy (regular insulin 0.2 U/kg IV with 20% glucose diluted 2:1 and administered slowly intravenously; blood glucose monitored hourly) was implemented when potassium concentrations were deemed clinically significant; however, no predefined threshold was established, and treatment decisions were based on overall clinical assessment. Urination was confirmed on day 15 (day 8 of PD). Because of the patient’s temperament, urinary catheterisation was not feasible, and urine output could not be quantified; urine production was therefore assessed subjectively and was initially considered polyuric. On day 16, oral administration became possible, and clopidogrel was added. Five days after the resumption of urination, urination frequency decreased. PD was discontinued on day 17 (day 10 of PD), and the cat was discharged on day 21.
At discharge, hindlimb motor function and femoral pulse quality appeared improved; however, owing to the patient’s temperament and limitations of the observation environment, the degree of recovery could not be adequately evaluated. Discharge medications included clopidogrel (25 mg/cat), rivaroxaban (2.5 mg/cat) and beraprost sodium (55 µg/cat). By day 63, BUN and Cre were 28.7 mg/dl and 1.87 mg/dl, respectively, and inorganic phosphate remained 4.2 mg/dl. No recurrence of thrombus formation was detected, and the cat maintained good hindlimb mobility and overall clinical condition.
Discussion
This report describes a cat that developed severe oliguric–anuric AKI temporally associated with ATE. In this case, the patient was managed with prolonged supportive care including PD and ultimately survived to discharge despite the absence of initial biochemical improvement. One of the major challenges was the lack of a standardised protocol for feline PD. Although previously published methods4–6 were used as a reference when performing PD, the circuit configuration, exchange frequency and dialysate concentration were determined based on practical constraints and the patient’s clinical condition.
The major issues during PD were dialysate leakage outside the body and reduced drainage efficiency, with a marked decline in recovery efficiency observed particularly during the later phase of PD. Catheter repositioning by traction was attempted, resulting in temporary improvement; however, drainage efficiency subsequently declined again, and this manoeuvre had to be repeated twice. Previous reports have suggested that omentectomy and the addition of heparin to the dialysate may be effective in preventing catheter obstruction.4,7 However, in the present case, these interventions were not performed because of concerns regarding prolonged anaesthesia time and an increased risk of bleeding associated with concurrent anticoagulant therapy.
The initial dialysate volume was set at 50 ml/kg (during the first two exchanges of PD) but was subsequently reduced to 20–30 ml/kg in response to leakage. This reduced leakage; however, it worsened when drainage efficiency decreased. When residual intraperitoneal volume was anticipated to be high, the instilled volume was adjusted accordingly. In this case, a conventional drainage system was used, which may have contributed to dialysate leakage. Although a conventional drainage system may be used as an alternative in emergency situations, in cases requiring prolonged PD, the consideration of adding heparin to the dialysate and omentectomy may be desirable to maintain drainage efficiency (Figure 2). Complete aseptic technique was not ensured during PD in this case. Septic peritonitis was clinically excluded based on the patient’s general condition, body temperature and macroscopic appearance of the dialysate; however, from a safety perspective, microscopic evaluation of the dialysate may have been desirable. Fluid balance was assessed based on body weight (Figure 3) and ultrasonographic findings (left atrial size and the presence or absence of pleural effusion and pulmonary oedema), and congestive heart failure was clinically excluded throughout hospitalisation. Subcutaneous oedema and hyperglycaemia were observed but did not interfere with continuation of PD.
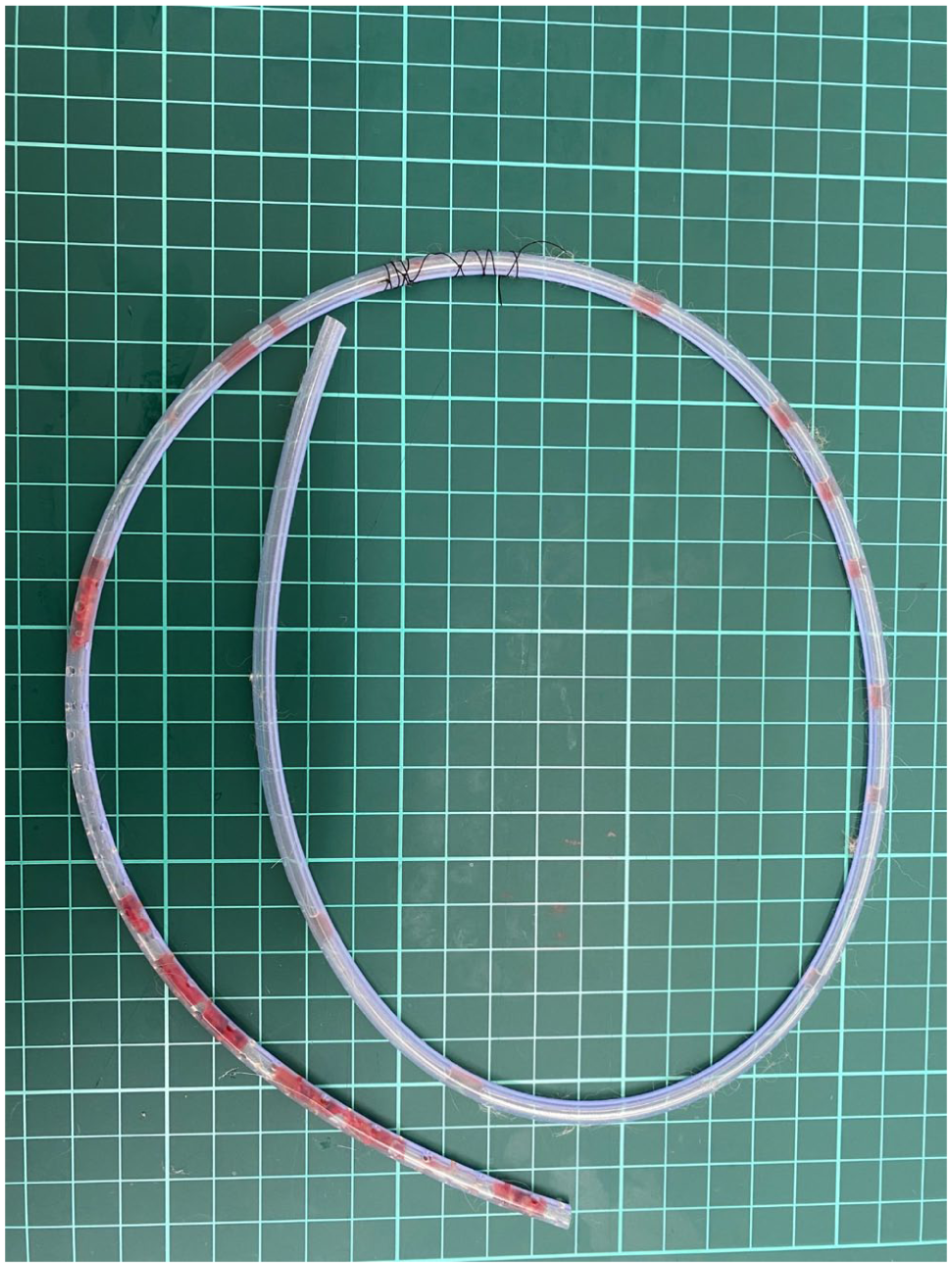
Removed peritoneal dialysis (PD) catheter after 10 days of treatment. After removal, fibrinous material was found within the catheter lumen, which may have contributed to the decreased drainage efficiency observed during the later phase of PD.
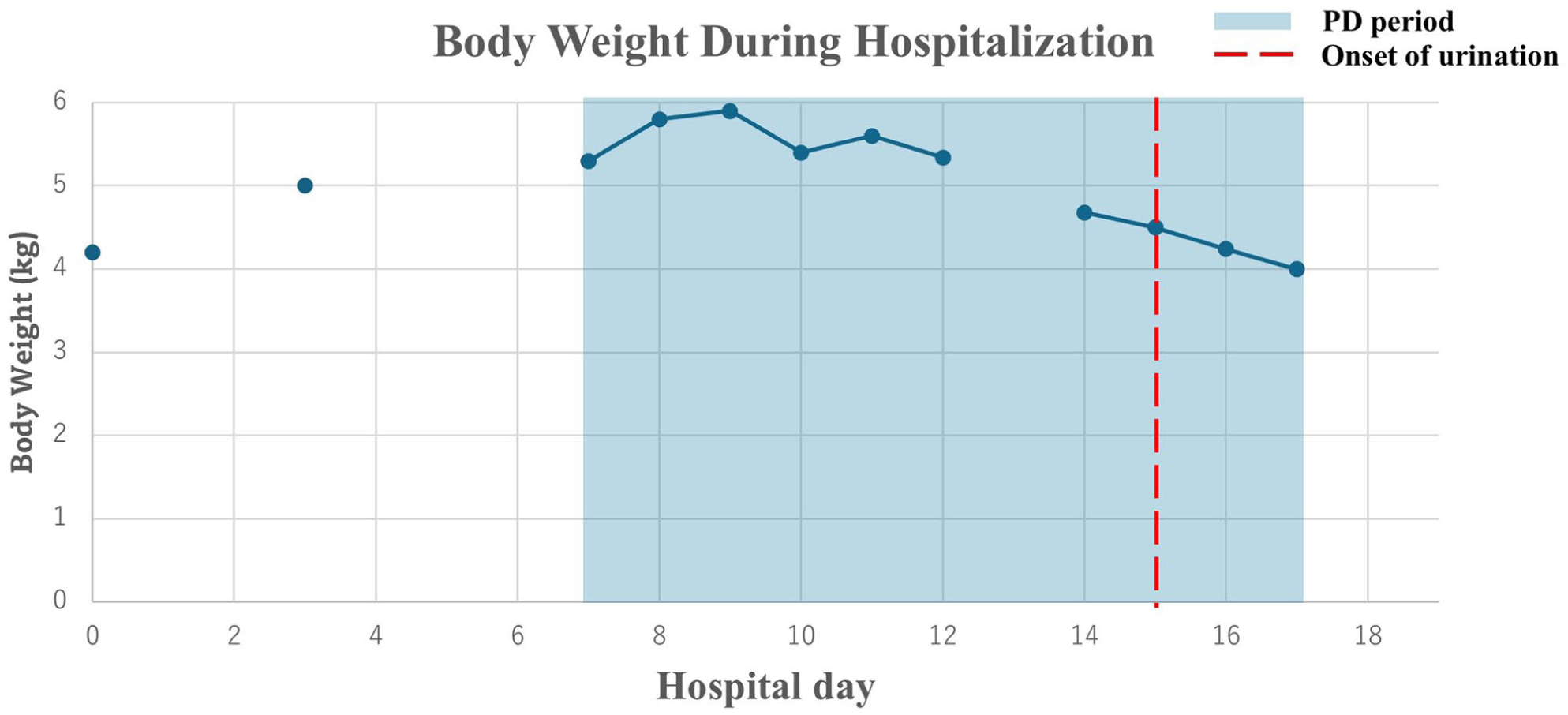
Changes in body weight during hospitalisation. Intravenous fluid therapy (lactated Ringer’s solution at 2.0–2.3 ml/kg/h IV) was continuously administered throughout hospitalisation, including during the oliguric–anuric phase and peritoneal dialysis (PD). Although transient increases in body weight were observed when drainage efficiency decreased, no clinical evidence of fluid overload was noted. Overall, body weight remained relatively stable, suggesting that PD contributed to maintenance of fluid balance. Body weight was not measured daily owing to the patient’s temperament; consequently, data for some days are unavailable
Assessing PD efficacy was challenging. BUN and Cre showed poor response, and potassium concentrations lacked stability. Although a higher exchange frequency might have improved dialysis efficiency, further increases were not feasible because of practical limitations. Survival for more than 1 week in an anuric state is generally unlikely without intervention, and we interpreted the prolonged survival observed in this case as indirect evidence suggesting a beneficial supportive effect of PD. However, urine output was not quantified and was instead assessed based on ultrasonographic detection of urine accumulation in the bladder. Therefore, the possibility that extremely small amounts of urine production were present cannot be excluded.
PD was continued for 8 days before spontaneous urination was observed. The decision to continue PD was based on the relatively stable systemic condition of the patient, the inability to definitively conclude irreversible renal failure during the early course of treatment and the owner’s preference for continued aggressive therapy. No clear criteria exist to determine the optimal duration of PD in severe oliguric–anuric AKI potentially associated with ischaemia–reperfusion injury, and treatment decisions must therefore be individualised.
Finally, long-term outcome data for cats surviving to discharge after PD for anuric AKI potentially associated with ATE remain scarce. Continued follow-up is needed to evaluate the durability of renal recovery and longer term clinical impact in similar patients.
Conclusions
This report describes a cat with ATE-related severe anuric AKI that survived after prolonged PD. Our findings suggest that meaningful recovery is achievable with sustained supportive care, even without early biochemical improvement. This case encourages clinicians to consider PD as a viable option when haemodialysis is unavailable, provided they recognise the challenges in quantifying dialysis efficacy and the necessity for diligent monitoring of potential complications to optimise outcomes.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.