
Abstract
Introduction
Antiretroviral therapy (ART) coverage has improved in the past few years in India. However, substantial non-adherence to ART has been reported among the people living with human immunodeficiency virus (PLHIV) in India. Digital health solutions can be potentially used as cost-effective interventions to address the problem of non-adherence. This study presents a systematic review followed with randomized clinical trial (RCT) only meta-analysis of existing literature conducted to assess the effectiveness of digital health interventions on ART adherence among the PLHIV in India.
Methodology
A comprehensive systematic review was done on articles examining digital health interventions on ART adherence among PLHIV in India, published till December 2024. Final search strategy was developed based on experiences from a preliminary search and was used to explore electronic databases- PubMed, EMBASE, ProQuest, Web of Science, SciELO, Grants, Google Scholar, and the grey literature. All the articles were reviewed independently by the authors. Bias and quality of the included studies were assessed by two independent authors using Cochrane collaboration tool. RCT only meta-analysis was done to synthesize results using fixed effect model due to low heterogeneity.
Results
In total, 441 articles were obtained using the final search strategy. A total of 415 articles were screened after removing duplicate articles. After abstract and full-text screening, only 04 studies met the inclusion criteria. Among the four included studies, three were conducted in southern India and one in eastern India. One of the four studies was quasi-experimental, and the rest were RCTs. Meta-analysis performed on three RCTs showed statistically significant positive effect on ART adherence with relative ratio of 1.18 (95% confidence interval (CI): 1.06 to 1.31, p = 0.002). As per Cochrane risk of bias assessment tool 2, three RCTs exhibited low risk of bias.
Conclusion
Meta-analysis result showed that digital health interventions led to improvement in ART adherence among the PLHIV in India. However, the generalizability of the findings is constrained by the limited number of studies included in the review.
Introduction
Human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) remains a public health challenge across the globe.1,2 Universal and effective coverage of antiretroviral therapy (ART) has resulted in decreased HIV-related morbidity, delayed progression to AIDS, enhanced survival, and reduced secondary transmissions.1,3,4 Risk of HIV transmission is associated with the levels of plasma viral load in an infected individual, 5 which can be greatly suppressed with the use of ART.6,7 The Joint United Nations Programme on HIV/AIDS (UNAIDS) has adopted the milestone of 95-95-95 for testing and treatment coverage by 2025 to fast track achieving the sustainable development goal (SDG) to end AIDS by 2030. 8 In 2023, there are 39.9 million people living with human immunodeficiency virus (PLHIV) globally, with 77% of them accessing ART and 72% virally suppressed.8,9 India has an estimated 2.5 million PLHIV in 2023 with the estimated incidence of 0.05 per 1000 uninfected population. 10 ART coverage has improved in the past few years in India. 11 India's AIDS response is steered by National AIDS Control Organization (NACO) through the comprehensive and expansive framework of the National AIDS Control Program (NACP) which was launched in the 1992. 10 Currently the NACP is in its fifth phase. As per March 2024, 775 ART centres were providing services to around 16.89 lakh PLHIV. 10 Out of total PLHIV in India, around 81% knew about their HIV status, 71% were on ART and 69% achieved viral suppression. 10
Use of ART as a strategy for preventing HIV infections has been widely discussed.4,5,12 Studies have showed association between reduced viral load and a decrease in new HIV infections.5,13 However, adherence to ART among the PLHIV is critical to the effectiveness of ART in achieving suppressed viremia.14–17 Though a benchmark for the optimal adherence to achieve viral suppression is yet to be defined, an adherence of ≥95% as provided by Paterson et al. (2000) has been suggested.18,19 Some studies have shown that high levels of viral suppression could be obtained with adherence levels below 95%.16,17,20–23
Adherence to ART among the PLHIV in India has been a challenge. A prospective observational study by Joshi et al. (2014) across 15 States of India found suboptimal (<95%) adherence at 24.5%. Bandopadhyay et al. (2019) found that 31.6% of patients missed at least one prescribed dose in last week. A cluster randomized controlled trial (RCT) for the efficacy of behavioural adherence intervention among PLHIV in southern India found that 27.9% of the participants took more than 80% of their prescribed doses in last month. 24 A meta-analysis by Mhaskar et al. (2013) estimated the pooled ART adherence in India at 70%. 25 While a meta-analysis by Chakraborty et al. (2020) reported that optimum ART adherence in India is not attained by 33% of PLHIV, 26 Basu et al. (2024) found the pooled adherence (of ≥95%) to be 54%. 27 Several factors related to demographic, socio-economic, psychological, and epidemiology pose serious roadblocks to engagement and retention in treatment. Various adherence barriers have been reported by the studies in India: forgetfulness, non-disclosure of HIV status, stigma fear, lack of support from family/friends, anxiety/depressive symptoms, drug stock-out, adverse reaction, and cost of drugs/financial reason.24,25,27–31
Several interventions have been executed to enhance adherence, for instance monetary incentives; direct administration of prescribed ART; health education, counselling and social support; and using information and communication technologies (ICTs). 32 ICTs such as electronic health (eHealth), mobile health (mHealth), and other digital innovations propose capable results that can enhance healthcare delivery. 33 In case of HIV treatment and care, digital health technologies can be exploited to improve ART access and delivery along with the monitoring of ART adherence and retention. Aside from SMS and mobiles apps that can deliver counselling sessions and personalized reminders about medications and ART visits, innovations like wireless electronic adherence monitors, smart pill bottles, and electronic pharmacy refills can aid in real-time monitoring of medication adherence. A study by Del Moral Trinidad et al. 2025 showed that SMS text messages as a reminder for upcoming medical visits and drug resupply were effective in improving adherence significantly along with lowered viral load. 34 In the RCT by Sabin et al. 2025, ART adherence improved significantly among the intervention participants who received real-time text reminders triggered by late dose taking (from wireless medication device ‘Wisepill’) combined with targeted counselling guided by device-generated adherence data. 35 Another study by Haberer et al. 2016 also found that adherence was significantly higher when study participants received scheduled SMS reminders along with the triggered SMS about late/missed doses by a real-time adherence monitor. 36 In an observational cohort study, mean adherence among the study participants increased significantly after they switched to real-time electronic adherence monitoring (EAM) from standard EAM. 37
Since technological developments are dynamic, it is crucial to keep abreast of the latest evidence of effectiveness to encourage their integration into healthcare system. To our knowledge, a systematic review focusing specifically on the effectiveness of digital health interventions to encourage ART adherence in the PLHIV in India is yet to be done. Hence, a systematic review followed with RCT only meta-analysis of the literature was conducted with the objective to assess the effectiveness of digital health interventions on ART adherence among the PLHIV in India. This study aims to enlist the types of digital health technologies employed in the Indian PLHIV population and their effectiveness in improving adherence to ART, and to assess the other treatment-related changes due to digital technology.
Methodology
This systematic review and meta-analysis is registered on PROSPERO, with registration number CRD42025641256.
Search strategy of the study.
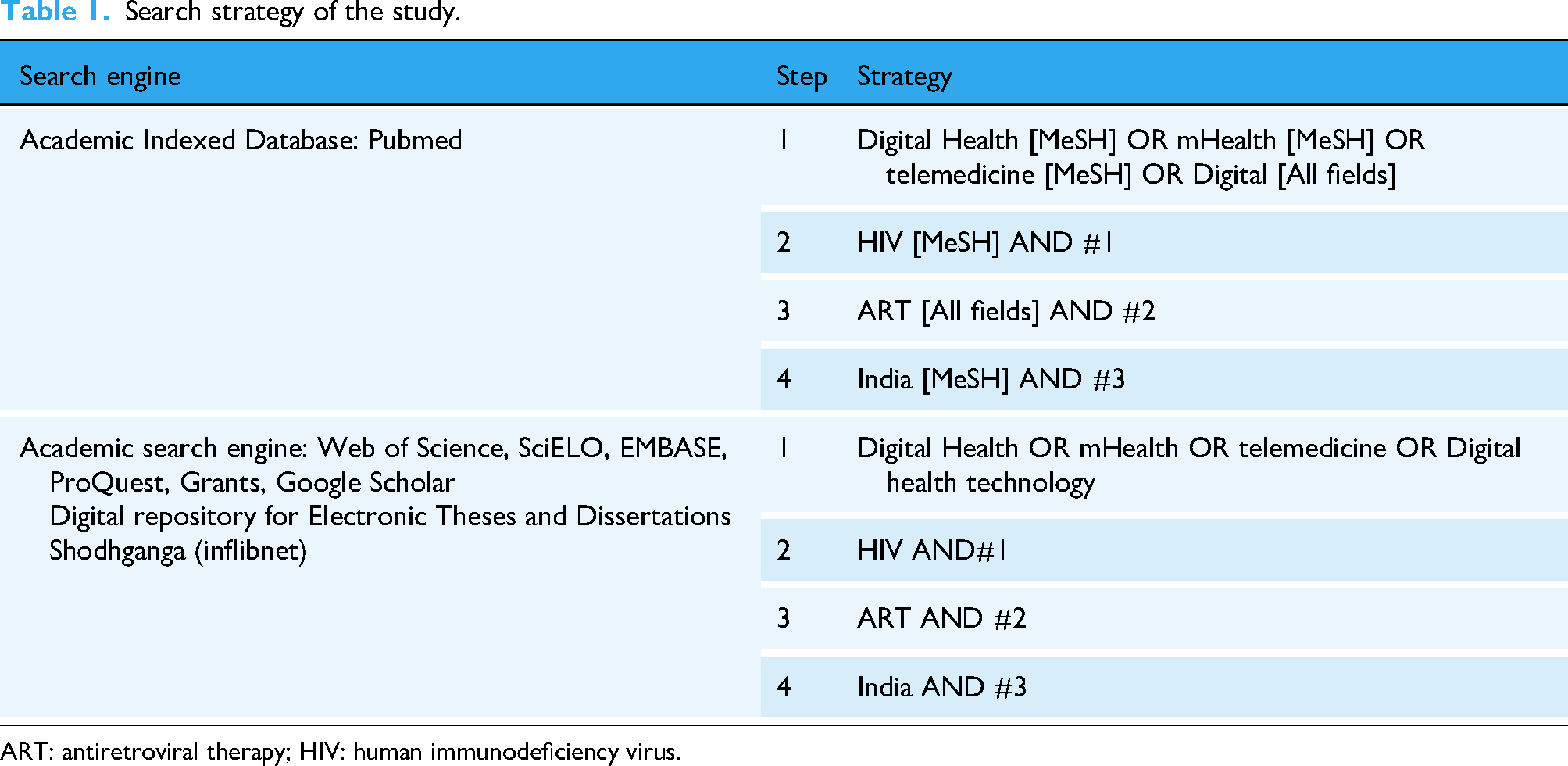
ART: antiretroviral therapy; HIV: human immunodeficiency virus.
Eligibility criteria
Studies were included if they met the listed conditions:
have enrolled Indian population as participants with HIV infection; all peer-reviewed interventional studies (experimental or quasi-experimental); employed digital health intervention, defined as health facilities imparted via evaluated digital tools such as SMS reminders, interactive voice response (IVR), mobile phones
38
; encompassed as a minimum one quantitative outcome criteria for ART adherence, like pill count, self-reported adherence measures, CD4 cell counts, viral suppression, or medication refill rates;
The studies were excluded if they were
using intervention other than digital health; animal studies; did not report adherence-related outcomes; observational studies, systematic reviews, and meta-analyses; qualitative study design.
Results
After thorough screening, reports retrieval and eligibility assessment, four articles fulfilled the inclusion criteria. Figure 1 illustrates the flowchart for the present systematic review according to PRISMA 2020 guidelines. The articles included in the study analysed effectiveness of different types of digital technologies on ART adherence among the PLHIV in India.
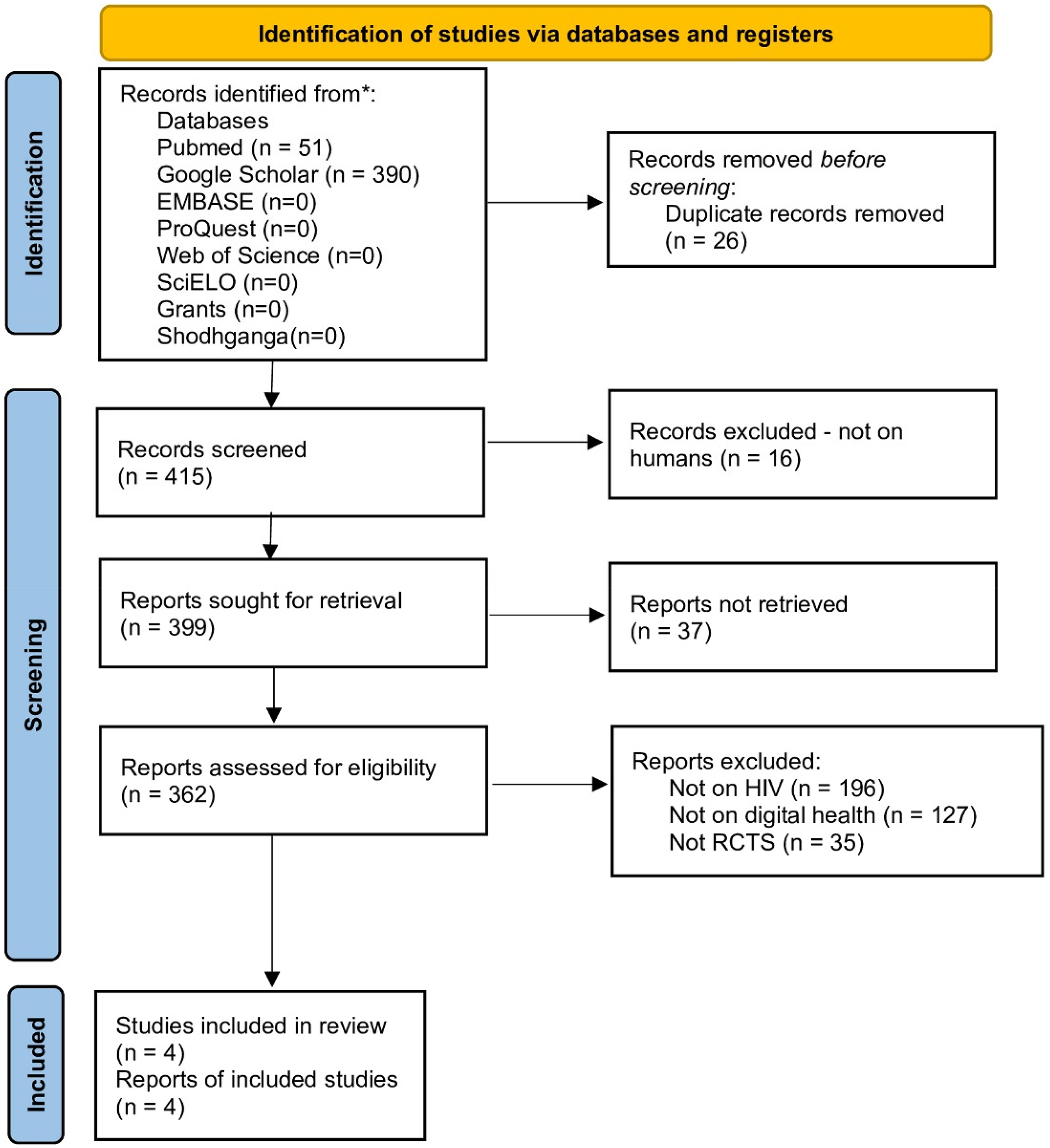
PRISMA 2020 flow diagram showing identification of studies for systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics: Characteristics of the included articles are presented in Table 2. Together, the four included articles enrolled 1263 participants in total. All the included articles were published between 2012 and 2024 (Table 2). One of the included studies was conducted in eastern India (Kolkata, West Bengal). 43 The remaining three studies were conducted in Southern India (two were conducted in Karnataka32,44 and one was conducted in Karnataka and Tamil Nadu). 45
Characteristics of the studies included in the review.
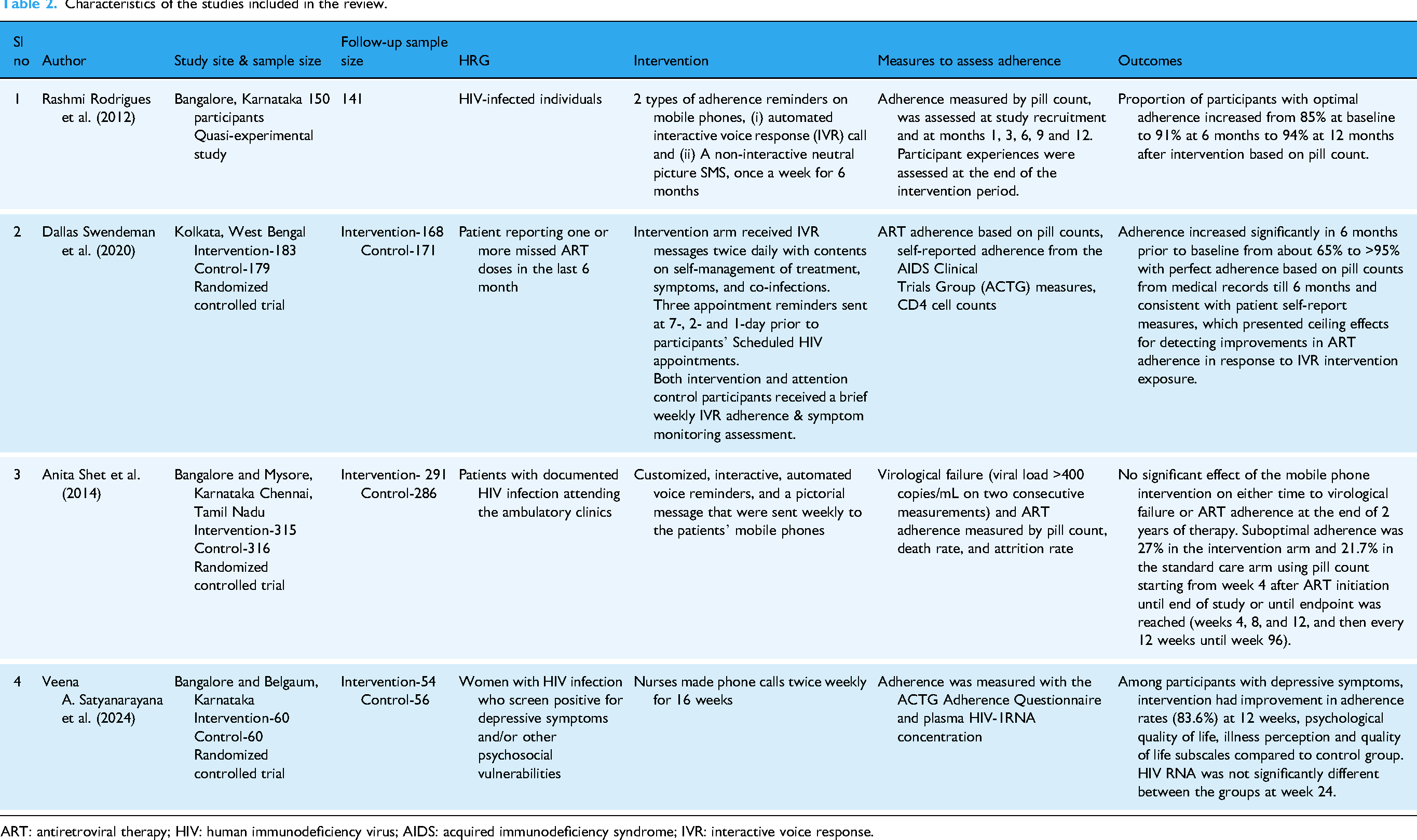
ART: antiretroviral therapy; HIV: human immunodeficiency virus; AIDS: acquired immunodeficiency syndrome; IVR: interactive voice response.
Study quality assessment: As per Cochrane RoB 2,39,40 overall, the three RCTs exhibited low risk of bias (Figure 2). Figure 3 illustrates the risk of bias and evidence quality using JBI Critical Appraisal Tools for RCTs. 41 And all the four articles were rated good for the strength and internal validity using Study Quality Assessment Tool developed by the National Heart, Lung and Blood Institute. 46
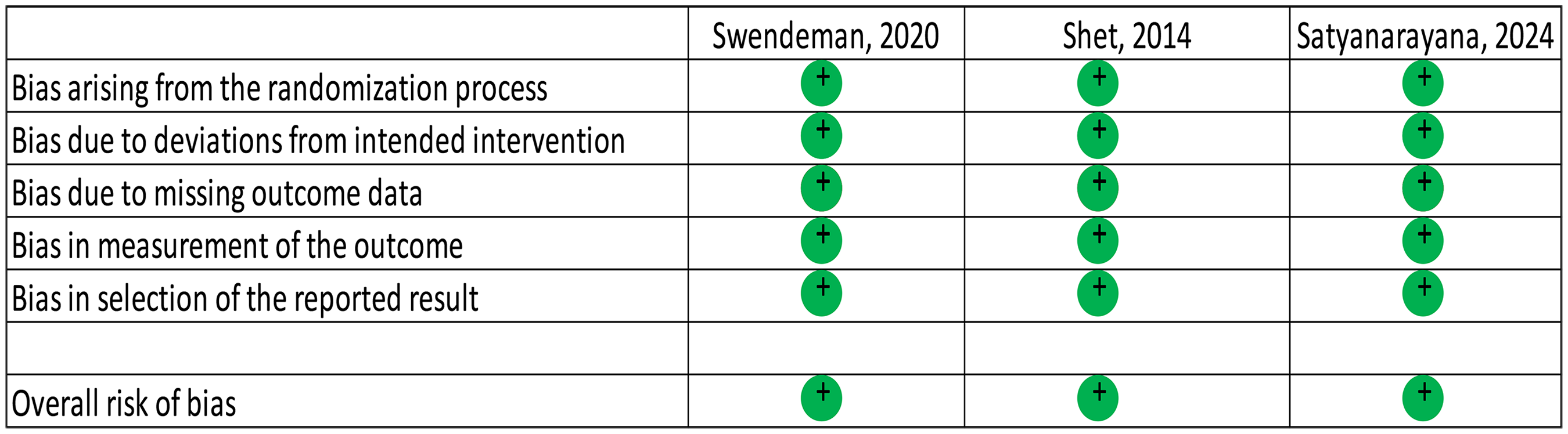
Risk of bias rating according to Cochrane tool. 40
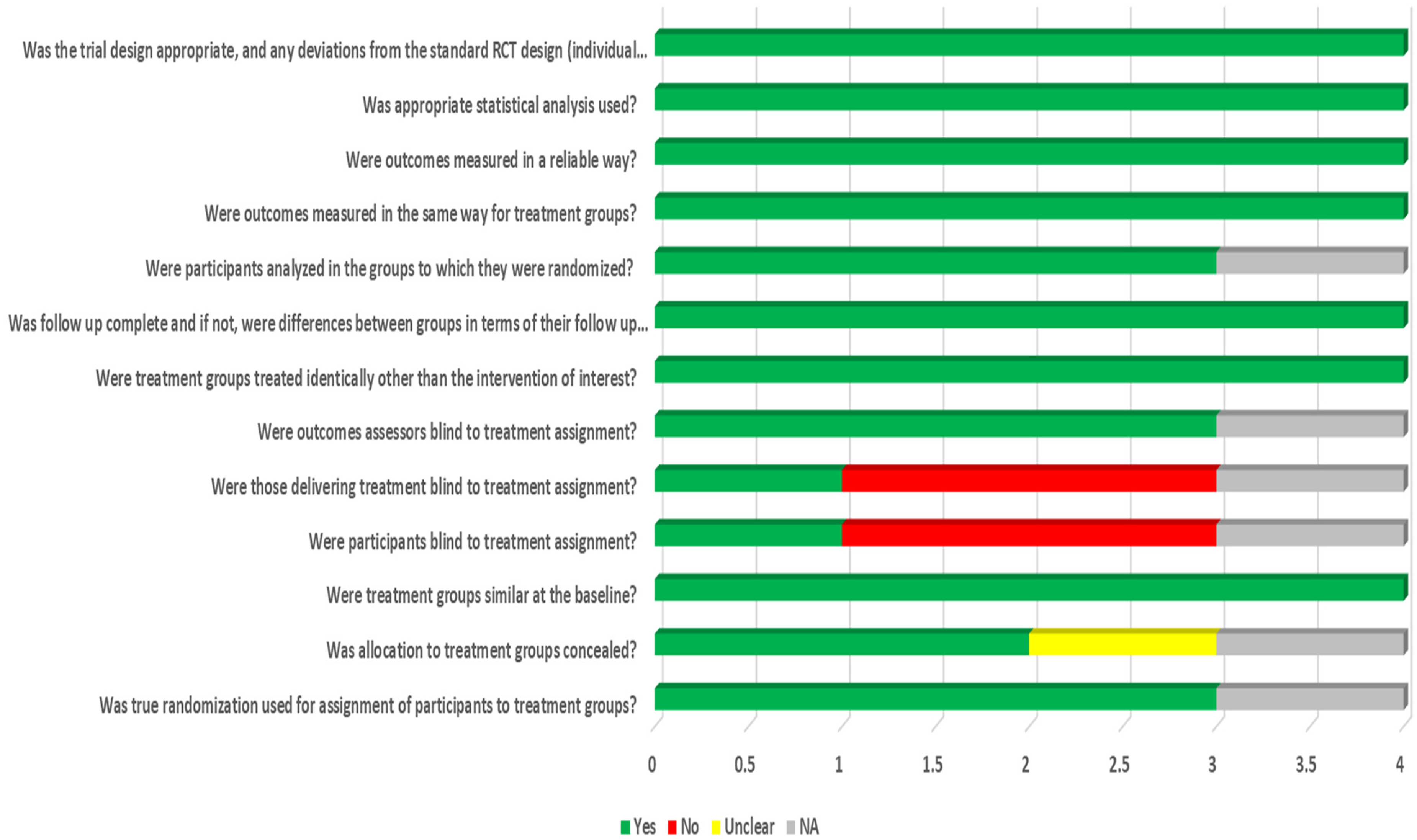
Depicts methodological quality and bias of included studies using JBI critical appraisal tool. 41
Study Interventions: All the studies delivered ART adherence care to study participants mainly via phone calls. In the study by Rodrigues et al. (2012), the intervention arm received two forms of adherence reminders, (a) automated IVR call and (b) a non-interactive neutral picture SMS, once a week for 6 months. 32 ART adherence was assessed using pill count, which was measured at the time of recruitment, and at months 1, 3, 6, 9 and twelve. Swendeman et al. (2020) included individuals who had reportedly missed ART doses during past 6 months. 43 The intervention group received IVR messages twice daily with contents on self-management of treatment, symptoms, and co-infections. They also received three appointment reminders. Adherence was assessed using pill counts, CD4 cell counts, and self-reported adherence using AIDS Clinical Trials Group (ACTG) measures. In the study by Shet et al. (2014), the digital health intervention involved delivery of customized, interactive, automated voice reminders, and a pictorial message to the participants on a weekly basis. 45 Assessment of ART adherence outcome was based on pill count, and attrition rate. Death rate and virological failure were also reported as outcomes. 44 Satyanarayana et al. (2024) enrolled HIV-positive women exhibiting depressive symptoms and/or other psychosocial vulnerabilities, who received a nurse-delivered intervention via biweekly telephone calls over a 16-week period. 44 ART adherence was measured by ACTG Adherence Questionnaire on missed doses and plasma HIV-1RNA concentration.
ART adherence outcomes
Adherence outcomes of the included studies are briefed in Table 2. Rodrigues et al. (2012) reported adherence at baseline, month 1, 3, 6, 9 and 12 as 85%, 94%, 93%, 91%, 95%, and 94%, respectively, and this change in proportions was significant over time (p = 0.016). According to 17% of the participants, forgetfulness for non-adherence reduced significantly after intervention (p < 0.001). Though participants considered that IVR was more helpful and easy to use in comparison to SMS (p < 0.001), in terms of confidentiality and intrusion, both SMS and IVR were analogous. Study conducted by Swendeman et al. (2020) in Kolkata, West Bengal reported a significant increase in adherence after IVR intervention. Adherence based on pill counts from medical records and subject self-report measures increased from 65% at baseline to >95% after 6 months of intervention. 43 The study MAHILA (Mobile phone-based Approach for Health Improvement, Literacy, and Adherence) by Satyanarayana et al. (2024) concluded counselling by mobile phone-based intervention demonstrated promising results among HIV-positive women with psychosocial vulnerabilities due to its feasibility and acceptability. ART adherence at baseline between both Treatment as Usual (TAU) Plus mHealth, and TAU only was similar. At week 4, adherence increased from 83.3% to 89.5% in TAU Plus mHealth but decreased to 83.6% at 12 weeks and further decreased to 79.2% by week 24. Whereas in TAU only group adherence slightly increased from 80% to 81% at week 4, but drastically reduced to 69.6% at week 12, further at week 24 it slightly increased to 70.2%. Intervention also improved their psychological quality-of-life (p < 0.05) and illness perception (p < 0.05). Shet et al. found comparable ART adherence between the intervention (27%) and the control group (21.7%). 45
Viral load suppression
Shet et al. assessed the rate of virological failure as an additional outcome and observed statistically insignificant difference to virological failure between intervention (15.6%) and control group (15.5%). 45 Satyanarayana et al. assessed plasma HIV RNA concentration to detect HIV viral load and found insignificant difference between the TAU and TAU plus mHealth groups at week 24. 44
Meta-analysis
Initially meta-analysis was performed on the three RCTs with outcome as ART adherence using both random and fixed effect models. Zero value of the I2 statistic suggests a lack of significant heterogeneity between the studies. After heterogeneity assessment, it was decided to use fixed effect model due to low heterogeneity. Results showed statistically significant positive effect on ART adherence with pooled fixed-effects estimate of RR as 1.18(95% CI: 1.061 to 1.31, p = 0.002). That is, ART adherence in the PLHIV group receiving digital intervention was significantly (18%) higher compared to the control group. Moreover, all the studies distinctly showed directionally positive effect to the digital interventions (Figures 4).
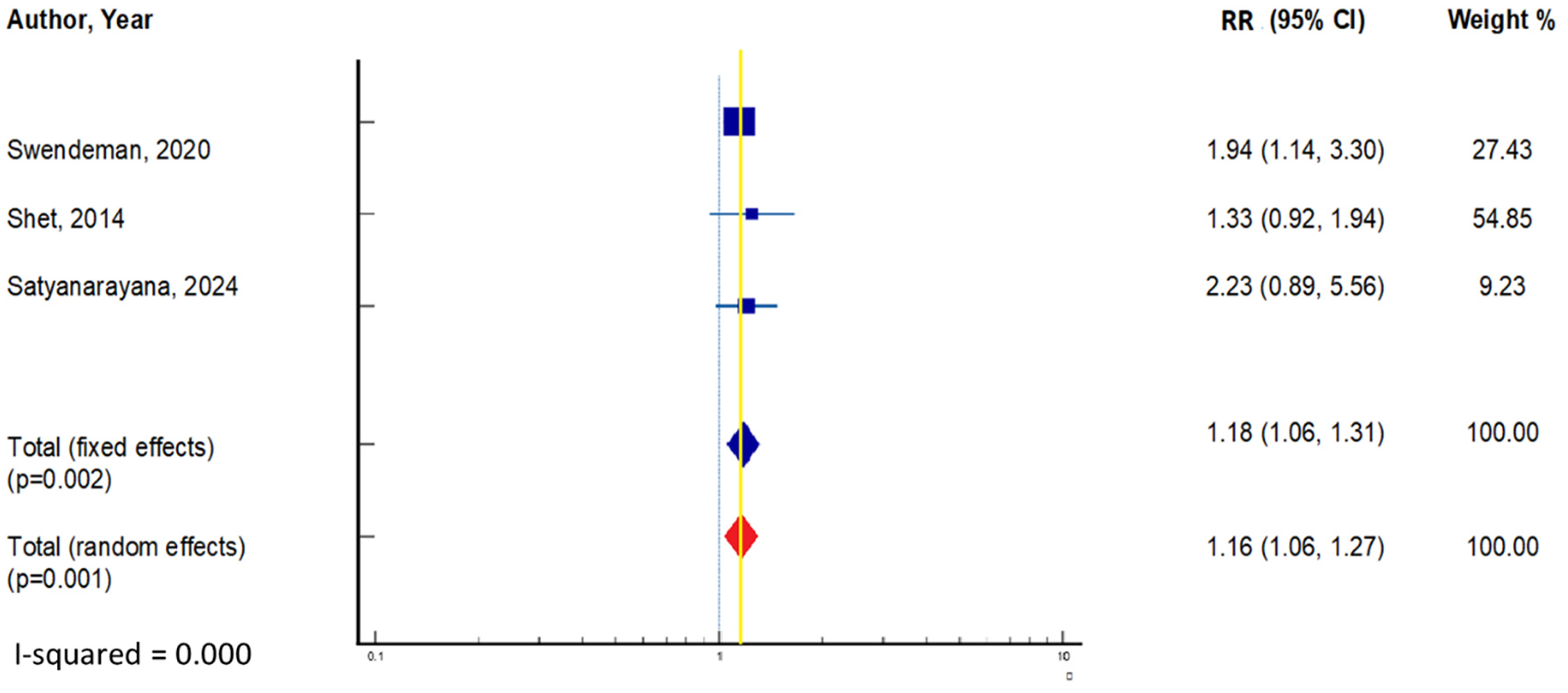
Effect of digital technology intervention on ART adherence among patients with HIV, using fixed effect model. ART: antiretroviral therapy; HIV: human immunodeficiency virus.
Publication bias
A funnel plot was prepared for ART adherence outcome reported by the included studies (Figure 5). Due to small number of the studies in the plot, it is challenging to decide whether the asymmetry in funnel plot is attributable to chance, heterogeneity in the studies, publication bias or methodological quality. Though, the Egger's test presented an indication of publication bias (p-value = 0.0194) but the limited number of studies may render the test result unreliable due to violation of underlying assumptions such as normality of the residuals of the regression between effect size and precision, or due to large CI. 47
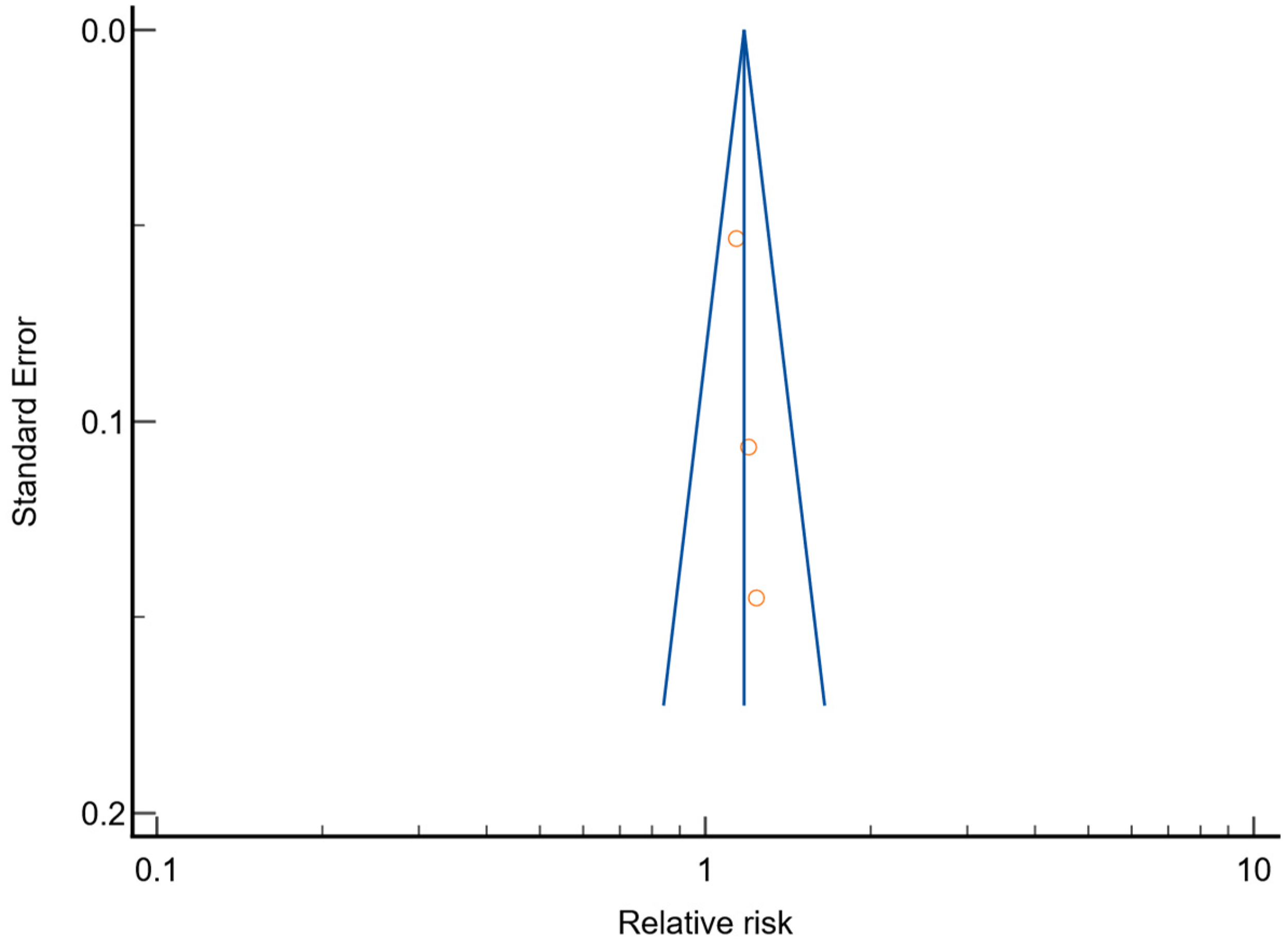
Funnel plot depicting the effect of digital technology intervention on ART adherence. ART: antiretroviral therapy.
Discussion
In recent years, major progress has been made in the fight against HIV, and adherence to ART has been a key part of managing the disease. 48 In 2014, UNAIDS launched the Fast-Track strategy, setting the 95-95-95 goals to be reached by 2025. 8 These goals aim for: 95% of PLHIV to know their status, 95% of those who know their status to be on ART, and 95% of those on ART to achieve viral suppression. 49 According to the Sankalak 2023 report, 82% to 86% of PLHIV in India were taking ART during 2022–23. 50 To further improve ART adherence, potential of scalable digital health interventions may be explored. This systematic review and meta-analysis aimed to summarize existing research on effectiveness of digital health interventions in improving ART adherence among HIV-positive individuals in India. Our findings showed that phone-based digital interventions, significantly improved ART adherence in all the included studies. However, most of these studies were published recently, and the overall conclusions are limited by the small number of available studies. Relative risk was evaluated in three of the included studies, all of which demonstrated a positive effect from the digital technology intervention. Meta-analysis showed statistically significant improvement in ART adherence with RR of 1.18 (95% CI: 1.06 to 1.31, p = 0.002). This is consistent with the findings of another meta-analysis by Esmaeili et al. (2023) who showed increased ART adherence with pooled RR of 1.18 (95% CI: 1.03 to 1.35, p < 0.05). 51 Whereas, systematic review by Masosa et al. (2024) showed statistically insignificant slight positive change in ART adherence with SMD=0.19 (95% CI: −0.03 to 0.41, p = 0.09) and heterogeneity of 44%. 52
Previously, Griffee et al. (2022), using a similar methodology among HIV-positive youth in sub-Saharan Africa, concluded that while evidence on digital interventions is varied, these approaches demonstrate potential in enhancing ART adherence. 53 Similarly, Esmaeili et al. (2023) emphasized that telehealth can serve as a supportive tool to improve adherence to ART. 51 According to their findings, telehealth offers an alternative to in-person visits, potentially reducing stigma, social isolation, and financial burdens associated with accessing HIV treatment. There were other systematic reviews and meta-analysis, conducted on global setting that included articles ranging from 8 to 12, has also inferred that digital intervention can be a valued approach to improve ART adherence and to reinforce the capacity of HIV management.54–56
Our findings suggest that integrating digital health technologies into prevailing healthcare delivery structure at ART centres could serve as a strategic approach to enhance ART adherence, reduce the frequency and cost of in-person clinic visits, and potentially mitigate HIV-related stigma. Moreover, the broader implementation of such technologies could support more efficient use of healthcare resources and facilitate patient-centred care models, especially in resource-limited settings. Future research and pilot programs should consider these alternative technologies to determine their feasibility, acceptability, and effectiveness across diverse healthcare contexts in India.
Though phone-based digital health interventions proved to be effective but, in India, there are many constraints which need to be addressed before its implementation. Barriers like digital literacy gaps, the lack of awareness regarding app function, difficulty in understanding language while using application, unequal access to mobile devices, gender-related barriers, stigma related to technology and to diseases worsening due to technology use, the lack of human touch, privacy concerns, and infrastructural limitations should be critically considered. 57 Methodical efforts are needed to anticipate and address these constraints to make digital health intervention feasible to uptake.
Strengths and limitations
This meta-analysis has several notable strengths and limitations. The inclusion of only RCTs enhanced the methodological rigour and strengthened the internal validity of the conclusions. A comprehensive and systematic search strategy was employed to identify studies evaluating the effectiveness of digital technology in promoting ART adherence, conducted under the guidance of a subject-matter expert. This approach further reinforced the internal validity of the review. Moreover, the analysis did not reveal any evidence of publication bias.
However, the generalizability of the findings is constrained by the limited number of studies included in the review. Additionally, while the review focused on the Indian population, the studies represented only three states, limiting applicability to the broader Indian population living with HIV. Despite the methodological rigour and a low risk of bias in the included studies, the lack of blinding among treatment providers introduces a potential for performance bias.
Assessment of the overall effectiveness of phone-based digital interventions was further complicated by heterogeneity in follow-up durations, sample sizes, and methods used to measure ART adherence. Nonetheless, the findings of this meta-analysis offer valuable insights and can inform the design of future large-scale, high-quality trials across diverse regions of India, exploring the potential of digital health interventions to enhance ART adherence and treatment fidelity.
Conclusion
This systematic review and meta-analysis synthesized evidence from studies evaluating the effectiveness of digital technologies in enhancing adherence to ART among the PLHIV in India. Due to the limited number of studies available that also conducted in few states, we strongly emphasize the need for multi-state, large-scale randomized controlled trials with longer follow-up and broader outcomes (e.g. ART adherence, viral load suppression, retention in care and plasma HIV-1RNA concentration).
The pooled estimates from the meta-analysis indicate that phone-based digital interventions are associated with improved ART adherence in the Indian PLHIV. These findings suggest that integrating digital health technologies into existing healthcare delivery systems at ART centres could serve as a strategic approach to enhance treatment adherence, reduce the frequency and cost of in-person clinic visits, and potentially mitigate HIV-related stigma.
NACP in India is considered as one of the largest HIV/AIDS control programs in the world. NACO has formulated and implemented Integrated and Enhanced Surveillance and Epidemiology framework as a strategy under the NACP-V to achieve the goal of eliminating AIDS as a public health threat by 2030 in line with the United Nation's SDG 3.
At this juncture, it is most pertinent that we develop cost-effective and individual-centric digital health solutions and integrate it within the NACP to address the issue of non-adherence to ART. This systematic review and meta-analysis is an effort towards identifying the types and modes of digital interventions which have been tested among the PLHIV in India, and to synthesize the evidence on their effectiveness in Indian context.
Improved adherence through digital interventions may contribute to better clinical outcomes and overall quality of life for PLHIV. Furthermore, the broader implementation of such technologies could support more efficient use of healthcare resources and facilitate patient-centred care models, especially in resource-limited settings.
It is also important to highlight that most interventions assessed in the included studies utilized mHealth platforms, such as SMS reminders, IVR calls, and mobile applications. This indicates a significant opportunity to explore and expand the use of other digital health modalities, including telemedicine, electronic health records, artificial intelligence-driven adherence tools, and wearable technologies. Future research and pilot programs should consider these alternative technologies to determine their feasibility, acceptability, and effectiveness across diverse healthcare contexts in India.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261423270 - Supplemental material for Effectiveness of digital health interventions on antiretroviral therapy adherence among people living with HIV in India: A systematic review with an RCT-only meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076261423270 for Effectiveness of digital health interventions on antiretroviral therapy adherence among people living with HIV in India: A systematic review with an RCT-only meta-analysis by Vaibhav Gupta, Vishal Deo, Barnali Deka, Garima Jain, Sunny Yadav and Sanghamitra Pati in DIGITAL HEALTH
Footnotes
Ethical approval
Ethical approval is not applicable as all data are derived from publicly available resources.
Authors contributions
Conceptualization was done by SP and VD; overall coordination was done by VD; study design by VD, VG, and GJ; literature search was done by VG, GJ, and SY; abstract and full-text screening was done by VG, VD, BD, and GJ; data extraction was done by VG and SY; analysis and appraisal for quality of evidence by VG and VD; writing by VG, VD, and BD; reviewing and editing were done by SP.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
VD takes full responsibility for the article, including the accuracy and appropriateness of the reference list.
PROSPERO registration number
CRD42025641256.
Data sharing
The datasets generated from this review are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.