
Abstract
Background
Virtual reality (VR) is a promising tool to deliver medical treatments easily and safely. However, clear evidence on the effectiveness of these devices in cardiovascular rehabilitation is still lacking. The aim of this study was to test the efficacy of integrating the use of an immersive VR system based on driving simulation in cardiovascular rehabilitation.
Methods
A randomized controlled trial (ClinicalTrial.gov NCT07195279) was conducted with 60 subjects undergoing a cardiovascular rehabilitation program. The experimental virtual reality group (VRG) followed an experimental therapy through virtual car driving simulation sessions, while the control group attended a conventional program of calisthenics. In both groups, the above two interventions were formed by sessions of 20 min in addition to conventional therapy, so the two groups received the same amount of therapy time. Hospital Anxiety and Depression Scale, the Short Form 12 (SF-12) questionnaire for quality of life, and other clinical scales were administered to assess the efficacy of integrating VR into the rehabilitative intervention.
Results
Perceived quality of life SF-12 (p < 0.02) significantly improved only in the VR group, whereas other parameters such as pain, perceived exertion, and oxygen saturation improved in both groups.
Conclusion
VR resulted in improving some patients’ conditions, likely due to its high level of engagement. When assessing the effects of a VR system, it is important to consider the specific software with the exergame and the tasks administered: in this study, we selected a car driving simulation, which yielded positive effects.
Introduction
Cardiac rehabilitation is a multi-faceted intervention designed to support individuals with heart disease through exercise training, promotion of physical activity, health education, cardiovascular risk management, and psychological support, all tailored to the specific needs of each patient. Beyond its role in secondary prevention and improving cardiovascular outcomes, modern cardiac rehabilitation increasingly emphasizes enhancing patient well-being and health-related quality of life. 1
Since its introduction in the late 1950s, 2 cardiac rehabilitation has evolved significantly. Initially reserved for low-risk survivors of acute myocardial infarction, it is now widely recommended across a broad spectrum of cardiac conditions, including acute coronary syndrome, heart failure with reduced ejection fraction, and post-revascularization procedures. 1 Indeed, contemporary clinical guidelines 3 highlight the importance of structured, high-quality delivery of cardiac rehabilitation based on a multidisciplinary approach involving cardiologists, nurse specialists, physiotherapists, dietitians, and psychologists, all working together to provide exercise training, education in self-management, risk factor modification, and psychological support. While exercise training remains foundational, the modern model now addresses broader aspects of lifestyle, behavior change, and mental well-being, with the overarching goal of improving long-term quality of life.1,2
Building on this evolving framework, innovative approaches are emerging to further strengthen participation and outcomes. Virtual reality (VR) is a technology that allows users to experience and explore computer-generated environments as if they were real. By wearing a headset and using hand controllers, users can interact in real-time with a three-dimensional digital world through visual and auditory sensorial channels, perceiving to be present in that synthetic environment. 4 Over the past few decades, VR has been extensively used in psychological and neuroscientific research, as well as clinical applications, 5 yielding promising results for diverse clinical conditions.6,7 Furthermore, VR has also been employed in the cardiovascular field across various settings, including cardiovascular rehabilitation, interventional cardiology, and cardiovascular surgery, to assess both physiological and psychological outcomes.8,9 A recent meta-analysis 9 conducted on almost one thousand patients showed that VR-based cardiovascular rehabilitation significantly reduced symptoms such as anxiety and depression in patients with cardiovascular diseases compared to standard rehabilitation. However, the effects on cardiorespiratory functions were not significantly different between the two approaches. Another meta-analysis 10 confirmed that VR may reduce negative emotions in cardiovascular rehabilitation suggesting that VR can be effective in improving patients’ exercise capacity. VR does not seem to be less effective than conventional cardiovascular rehabilitation when tested in a longitudinal randomized controlled trial (RCT). 11
The benefits of using VR may stem from its ability to be customized, potentially enhancing the rehabilitation experience by offering cognitive, emotional, and physical advantages.12–14 It can improve patients’ motivation and engagement, 15 reduce anxiety. 16 At the same time, this type of approach is not without side effects, and some patients may experience discomfort 17 as well as dizziness, nausea, or eye strain, commonly referred to as cybersickness, can affect a subset of users, particularly those with vestibular sensitivities or neurological conditions. 18 However, recent advancement of technology minimizes discomfort and likelihood of fatigue. 19 These technological developments could make VR a more tolerable and accessible therapeutic tool for long-term rehabilitation programs as already proven by studies on motor treatment.13–15 Specific evidence for treatments regarding cardiovascular rehabilitation is still lacking.
In general, in the context of cardiovascular rehabilitation, the impact of VR was mainly assessed in terms of mental health, 20 particularly in relation to psychological aspects such as mood enhancement, stress reduction, and increased emotional well-being, whereas its role in improving other health indicators such as adherence, satisfaction, and overall quality of life has not been shown. 10 The reported benefits may be due to the immersive and engaging nature of VR, which can provide a sense of novelty, distraction from discomfort, and a greater feeling of control over the rehabilitation process. 12 However, current evidence related to cardiac parameters, exertion, pain, and other clinical and psychological parameters does not clearly demonstrate its superiority over conventional approaches. 20 This suggests that while VR may be an effective tool for supporting psychological recovery, its broader impact on the comprehensive spectrum of rehabilitation outcomes remains to be fully established.
The aim of this study was to test the efficacy of integrating the use of a VR system based on driving simulation in cardiovascular rehabilitation through a RCT. Cardiovascular disease has been linked to decreases in driving performance, and rehabilitation may also aim at the recovery of driving ability. 21 The use of driving simulators has already been tested in neurological 22 and orthopedic 23 patients. We tested this approach in a VR system for cardiovascular patients. The objective was to improve some psychological and physiological outcomes of cardiovascular rehabilitation.
Methods
Study design and participants
The study is a single blind RCT retrospectively registered on ClinicalTrials.gov (NCT07195279) and conducted following the current guidelines for the reporting (CONSORT). The Local Independent Ethical Committee of Santa Lucia Foundation approved this study (CE/PROG.795, date of approval 2 December 2019). Patients gave their written informative consent prior to participating in the study. Enrollment was performed at an Italian clinic that provides intensive inpatient cardiovascular rehabilitation, according to the following inclusion/exclusion criteria. The inclusion criteria were diagnosis of cardiovascular disease and need for intensive inpatient rehabilitation after cardiac surgery, age over 18 years, absence of comorbidities, ability to understand and follow instructions provided by physiotherapists. The exclusion criteria were presence of cognitive impairments (Mini Mental State Evaluation, MMSE, score < 24), presence of altered consciousness, psychotic symptoms, bipolar disorder, or other severe psychiatric conditions, conditions contraindicating physical training (e.g. bone fractures), conditions contraindicating the use of VR (e.g. blindness or deafness), refusal to participate in any phase of the research project, or failure to provide informed consent. Once the patient was declared eligible, a person not involved in the trial and not involved in patient treatment, indicated the group allocation following a sequentially numbered randomization list. All participants were inpatients in phase I of cardiac rehabilitation.
Rehabilitative interventions
Both groups performed 1.5-h per day, 6 days per week. For 100 min (with 10 min of break), patients performed calisthenics exercises and aerobic reconditioning exercises on a stationary bike or treadmill, depending on medical prescription and patient's health status, similarly to previous studies.24,25 Patients were randomly allocated to the experimental virtual reality group (VRG) or to the control group (CG). The latter performed additional 20 min every day of calisthenics exercises, whereas the former group underwent the immersive VR experience as part of their rehabilitation protocol for the same amount of time.
The CG of this study performed a conventional cardiovascular rehabilitation protocol that consisted of 1.5-h group calisthenics sessions with a 10-min break, held six times per week, The VRG completed an immersive VR intervention, which consisted of a simulated driving experience delivered over nine sessions, three times per week, each lasting 20 min, over a 3-week period. Participants observed the virtual scenario through Meta Quest 2 head-mounted display, offering an approximate 90–100° field of view and a resolution of 3840 × 1920 pixels per eye. The VR therapy employed a full immersion approach, delivering intense multisensory visual-auditory stimulation. Patients were exposed to diverse driving scenarios, specifically: urban streets (featuring intersections, traffic lights, and pedestrians to simulate complex urban environments), ring roads (designed for practicing smooth and confident high-speed driving in dense traffic), and tunnels (sections aimed at gradually desensitizing users to claustrophobic responses during driving) as shown in Figure 1.

Screenshots of the virtual reality driving environment as viewed by participants. The Figure represents first-person views of the immersive VR driving simulator used in the study. Driving in a tunnel with moderate traffic (upper left panel); City street scenario with ongoing traffic flow (lower left panel); Peri-urban roadway with traffic signs and surrounding buildings (upper right panel); Urban residential area with parked vehicles and cross traffic (lower right panel). The images illustrate the participant's perspective from inside the vehicle, including the steering wheel, dashboard instrumentation, and interactive interface elements. VR: virtual reality.
The virtual environment was designed by combining 3D objects and 360° VR videos using Unity 60000.0.33f1 game software environment (https://unity.com/). The 3D environment consisted of a realistic 3D model of a car's interior, simulating the driver's perspective (1:1 scale). The virtual cockpit incorporated an interactive steering wheel, controlled by participants from their perspective using Meta Controllers. This interaction, however, did not alter the vehicle's movement path. To optimize immersion, the Meta Controllers were rendered as hands, integrated with a 3D avatar model. Real-time arm movements of the avatar were achieved using inverse kinematics, precisely mirroring the participants’ physical actions. The 3D cabin was fully enveloped by 360° VR video showcasing the driving scenarios. The VR 360° videos were taken with a GoPro Max® 360° camera (GoPro Inc., San Mateo, CA, USA), with a spherical resolution of 5376 × 2688 at 30 fps and 3D spatial audio with an external Zoom H1 microphone. The spherical 360° videos were processed with Adobe Premier Pro® 2021 (Version 15) (Adobe, San Jose, CA, USA). The various scenarios the patient encountered corresponded to a progressively increasing level of difficulty as the rehabilitation sessions proceeded. Examples of challenging elements included narrow roads, urban traffic, tunnel driving, and high-speed roads. Each session lasted approximately 20 min, which was the time required to complete the driving route. However, the session might end earlier if the patient was unable to continue.
Randomization of patients in the two groups occurred using a random pre-generated concealed allocation list known only by researchers not involved in the enrollment and assessments for minimizing possible biases.
Assessment
All patients were assessed before the first session (baseline, Pre), and at the end of the 3-week rehabilitation protocol (endline, Post). Assessments were conducted by a clinician blinded to patient group allocation. At each time point, a comprehensive set of outcome measures was collected to evaluate the functional status, endurance capacity, mental state, quality of life, and patient engagement in daily activities. In particular, affective status was assessed using the Italian version of the Hospital Anxiety and Depression Scale (HADS, primary outcome): a 14-item scale used to assess anxiety (7 items) and depression (7 items) levels related to illness26,27; perception of quality of life was assessed with the Italian version of Short Form-12 questionnaire (SF-12), a 12-item health survey which generates physical and mental health summary scores. 28 Pain intensity was measured using the Visual Analog Scale, ranging from 0 (no pain) to 10 (worst possible pain), 29 while perceived exertion was assessed via the Borg Scale, ranging from 0 (“no exertion”) to 10 (“maximum exertion”). 30 Because the VR driving task was performed mainly using upper limbs, functional assessments included upper limb range of motion (ROM), evaluating shoulder flexion/extension and elbow flexion/extension, and Manual Muscle Testing (MMT), measuring strength of shoulder abduction, elbow flexion, and grip, with a total score ranging from 0 (no strength) to 15 (normal strength).31–33 In addition to these clinical measures, physiological measurements were recorded using the Oxy 4 pulsimeter (Gima, Oxy 4) before and after the first and the last sessions of rehabilitation. Heart rate (HR) was recorded in beats per minute (bpm), blood pressure (BP) was measured in millimeters of mercury (mmHg) for both systolic and diastolic values, and peripheral oxygen saturation (SpO₂) was expressed as a percentage (%). The Oxy 4 pulsimeter provides non-invasive, real-time monitoring of these parameters, ensuring standardized and reliable data collection across participants. Measurements were taken under resting conditions following the manufacturer's guidelines, with the device calibrated prior to each session to maintain accuracy.
Statistical analysis
Data are reported in terms of mean ± standard deviation for continuous physiological measures and in terms of median and interquartile range for ordinal clinical scores. Clarity, but given the ordinal scales used, non-parametric tests were used within subjects (Wilcoxon test) and between subjects (Mann–Whitney u-test). Sample size was computed based on previous data related to the use of VR in cardiovascular rehabilitation, 33 setting an alpha level at 5%, power of the test (1-beta) at 80% and with an effect size of 0.9 (that can be considered beyond large effect, being >0.8), obtaining a minimum number of participants of 58 for the whole sample. The alpha level of statistical significance for all the analyses was set at 0.05.
Results
Sixty patients were enrolled in this study. Their mean age was 70 ± 9 years old, with 77% men and 23% women. All of them needed cardiovascular rehabilitation. Ninety-seven percent of them had surgical intervention: 40% for the replacement of mitral and/or aortic valve, 33% after bypass surgery, 24% after other kinds of cardiovascular surgeries. The mean time between surgery and beginning of rehabilitation was 16 ± 11 days. Only 3% of patients had heart failure without any surgical intervention. These patients were randomly allocated in the two groups, each consisting of 30 patients. Figure 2 shows the consort flowchart of the study.
Table 1 shows the clinical variables assessed pre- and post-rehabilitation, revealing significant improvements in terms of pain and Borg score in both groups, physical and mental health only in VRG.
Affective evaluation and perceived quality of life assessment.

VR: virtual reality; CG: control group; HADS: Hospital Anxiety and Depression Scale; SF-12: Short Form 12; VAS: Visual Analog Scale. Scores are reported as medians (interquartile ranges) of the clinical variables assessed in VRG and CG, at the first and last time point (before the first session, last session). The p-values refer to the within-group comparison performed with Wilcoxon test, marked in bold for significant values.
Affective assessment with HADS is shown in Figure 3.

CONSORT flowchart of the research trial.
Quality of life assessed with the SF-12 is graphically shown in Figure 4.
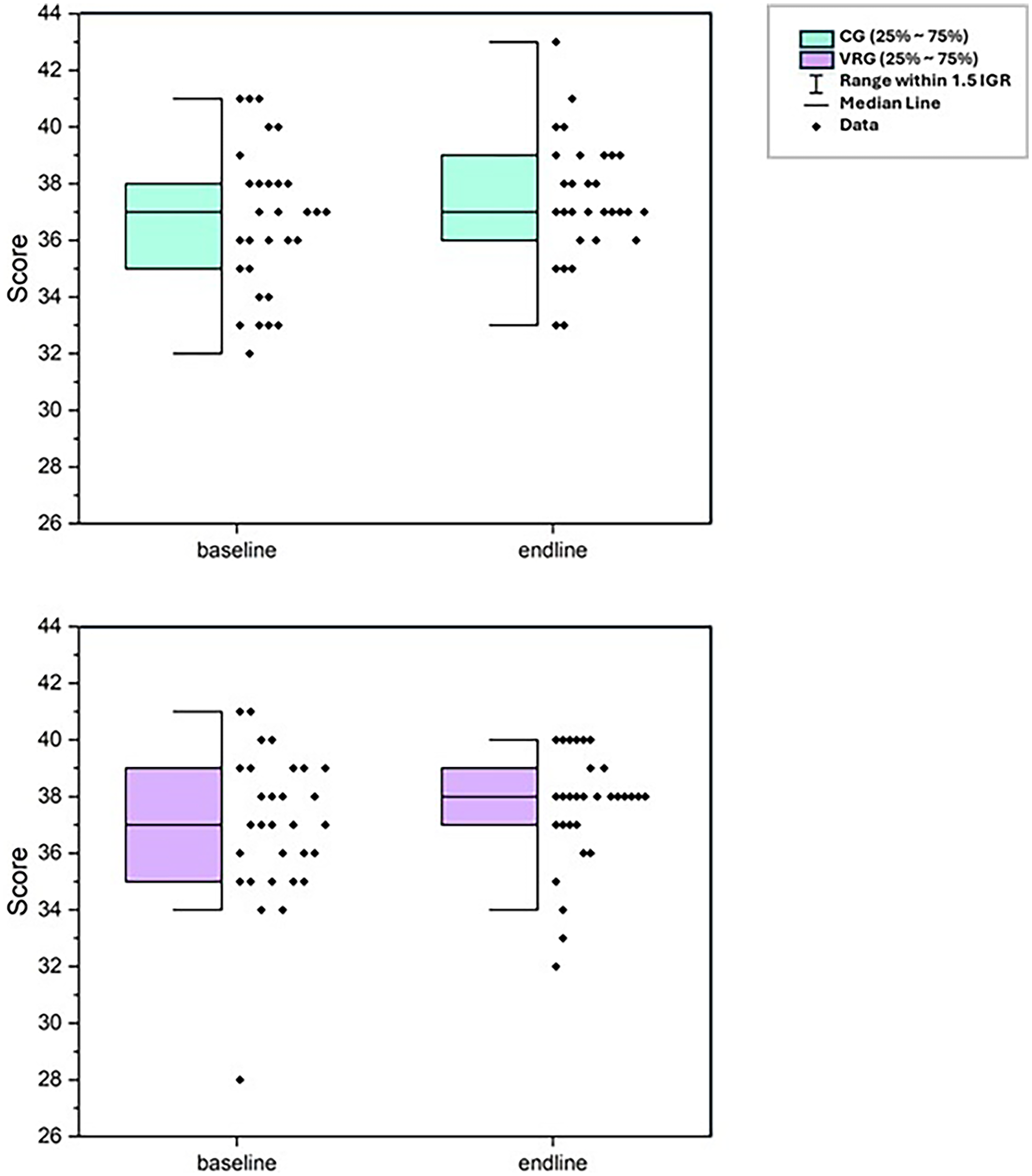
Half boxplots of affective assessment of control group (CG, top panel) and virtual reality group (VRG, bottom panel) through HADS scale. Figure shows total scores obtained by all groups at baseline and at the completion of the treatment (endline). Black dots represent individual data points, boxes represent the interquartile range (25%–75%), whiskers indicate 1.5×IQR, and horizontal lines inside boxes mark the medians. VRG: virtual reality group; CG: control group; HADS: Hospital Anxiety and Depression Scale; IQR: interquartile range.

Quality of life assessment. Violin plots show the distribution of range values for the conventional therapy group (left) and the virtual reality group (right). Within each panel, purple violins correspond to physical health and green violins to medical health scores. The dashed line indicates the median, while the dotted lines represent the interquartile range (25th–75th percentiles).
The purple violins (physical health scores) show a more pronounced improvement from baseline to endline for VRG. By endline, participants reported substantial improvements in their physical functioning after the intervention shown by the shifted upward distribution of the violins, with the median clearly higher and more participants clustered at better physical health scores. In contrast, the CG shows only a modest upward shift in the purple violins, with less change in both the median and the spread of scores, suggesting smaller perceived gains in physical health. The green violins (mental health scores) in both groups show upward trends as well, but the change is less pronounced than for physical health in the VRG.
The analysis of upper limb ROM and MMT-score did not show any significant differences between groups before rehabilitation, except for left elbow flexion (CG: 143 ± 15°, VRG: 137 ± 8°, p = 0.006). After rehabilitation, significant differences in ROM were observed for left (CG: 123 ± 9°, EG: 129 ± 14°, p = 0.020) and right (CG: 121 ± 13°, VRG: 129 ± 15°, p = 0.042) shoulder flexion, without differences at left elbow flexion (CG: 147 ± 12°, EG: 146 ± 8°, p = 0.187). In terms of MMT-scores, after rehabilitation significant differences were observed for right shoulder flexion (CG: 4.8 ± 0.5; VRG: 5.0 ± 0, p = 0.042) and right elbow flexion (CG: 4.9 ± 0.4, VRG: 5.0 ± 0, p = 0.042).
Physiological parameters were also assessed before the 1st session of therapy, immediately after it, and before the last session. Data are reported in Table 2. Both groups showed an increase in SpO2 after rehabilitation. The maximum BP resulted slightly but significantly increased in patients in the CG.
Physiological evaluation of heart rate (beat per minute, bpm) variability, arterial oxygen saturation (SpO2), and the maximum and minimum blood pressure (SBP = min, DBP = max).
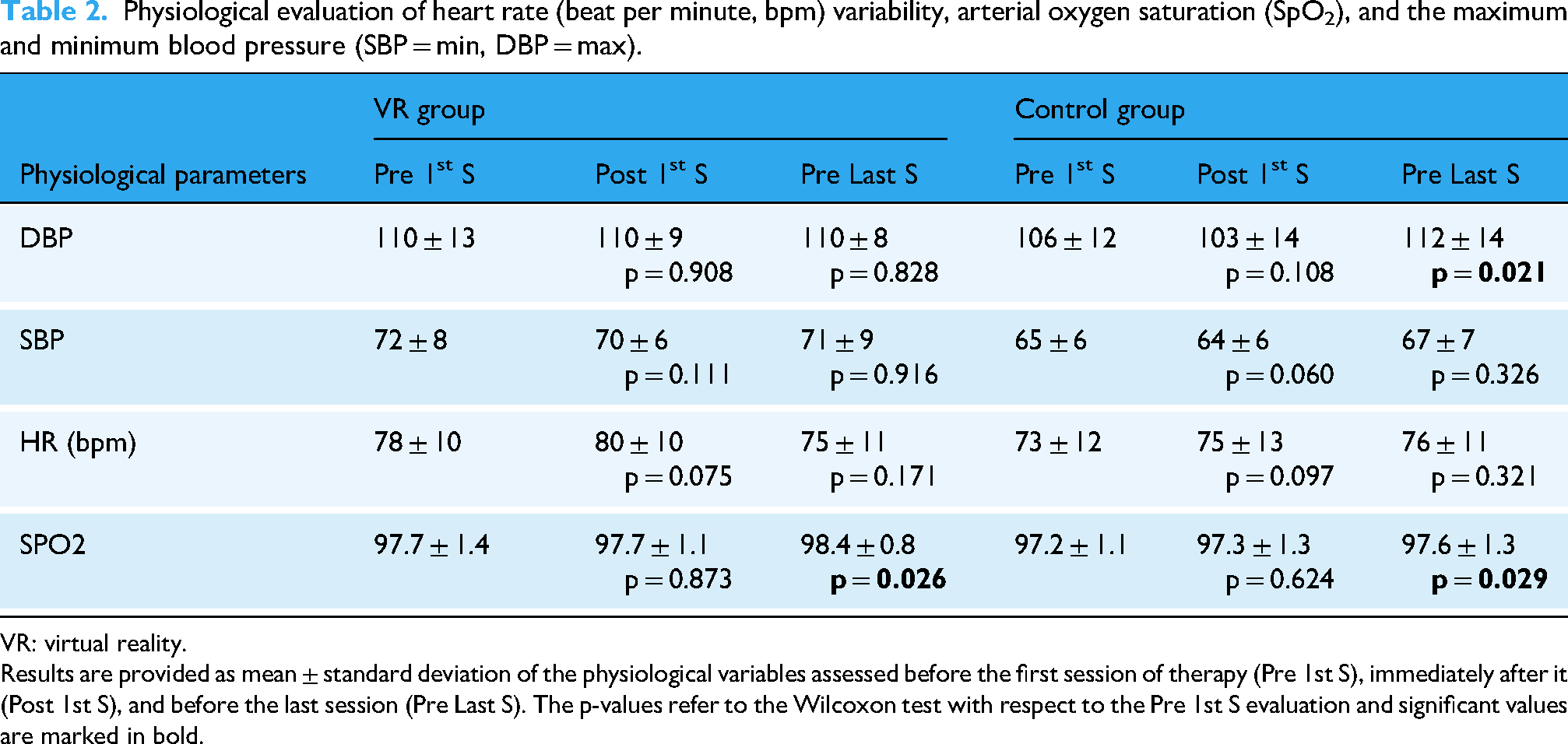
VR: virtual reality. Results are provided as mean ± standard deviation of the physiological variables assessed before the first session of therapy (Pre 1st S), immediately after it (Post 1st S), and before the last session (Pre Last S). The p-values refer to the Wilcoxon test with respect to the Pre 1st S evaluation and significant values are marked in bold.
Discussion
This study aimed to assess the efficacy of integrating an immersive VR treatment into a cardiovascular rehabilitation program, in which patients simulated driving in a different stressful context. Thirty patients received conventional cardiovascular rehabilitation, and the other 30 patients underwent the VR-based treatment combined with conventional therapy. At baseline, the VRG had a slightly lower Borg score for perceived exertion, higher physical health, but also slightly higher BP and HR, and reduced mobility in the left elbow.
After rehabilitation, we found that in both groups pain and exertion were reduced, and oxygen saturation increased. For the VRG (and not for CG), physical and mental health and upper limb mobility improved. Conversely, for the CG (and not for the VRG), the maximum BP after rehabilitation slightly but significantly increased. Overall, Figure 2 highlights a modest decline in scores from the first to the last assessment, while individual differences are still evident, and the presence of outliers suggests some participants deviated significantly from the central trend.
We observed slight and not significant effects on HADS total score (and to a lesser extent on HADS-anxiety), despite they have already been reported in many previous studies on the use of VR in cardiovascular rehabilitation.33–36
Some other studies reported contrasting results. One study showed a positive effect of VR in cardiovascular rehabilitation on selective attention, conflict resolution ability, and executive functions, but not on quality of life, depression, anxiety and stress. 37 This latter study included smaller patient groups compared to our study and the previously cited ones, which could have limited the statistical power of the performed analyses. Indeed, the study was designed as a Kinect based rehabilitation system via tablet in which the degree of immersivity is reduced. Another study tested exergaming, performed with a commercial videogame console, in cardiovascular rehabilitation, without finding clinically or statistically significant improvements compared to those obtained with conventional rehabilitation. 38 However, the use of videogame-based trainings is different from the use of an immersive VR systems, which facilitate the sense of presence, the sense of agency, and thus the participation, in the digital environment. 5
The impact of VR on quality of life is also controversial. We found positive improvements in terms of physical and mental health only in the VRG, and not in the CG. Specifically, both groups demonstrate an increase in range from baseline to endline, with the VRG showing a more pronounced improvement, particularly in the SF-12 physical health scores.
Our findings were in accordance with a previous study reporting the positive effects of a VR-based videogame program in ergometry, resistance to fatigue, and health-related quality of life, with excellent adherence and patient-perceived satisfaction in individuals with ischemic heart disease. 39 However, another study reported no statistically significant impact of VR on health-related quality of life in patients undergoing cardiovascular rehabilitation. 9 At the same time, this study confirmed the positive impact of VR on quality of life.
In our study, also kinematic (ranges of motion) and kinetic (muscle strength) aspects of upper limb were assessed, finding significant positive effects in the group of patients who experienced the VR system, especially at shoulder level. This result is in accordance with the positive effect of VR rehabilitation on upper limb strength already observed in neurological patients.40,41
There are two main pitfalls in using VR in rehabilitation: the definition of VR systems, and the poor importance given to content. The former problem is related to the fact that in some studies commercial consoles and computer-based systems were used, but authors referred to them as VR systems, even if they are not immersive.37,42 The last problem is that most of the studies discussed the effects of VR regardless of the type of stimuli or games used. 43 In our study, we used a car driving simulator featuring realistic 360° VR videos that depicted real-life city driving. This setup provided a highly controlled and safe environment for practice within the hospital, offering a realistic simulation of an important daily activity patients aim to recover and may sometimes fear resuming. Our application also allowed for progressive increases in task difficulty during rehabilitation by adjusting speed, the number of cars, and street width.
Our study has some limitations that should be considered when generalizing its results to the population of cardiovascular patients needing rehabilitation. First, the wide variability in the subjects limited the significance of between-group differences, and statistically significant results were mainly found for within-group analyses. Then, despite enrolling 60 patients, the sample is quite small when that variability is considered. The collected physiological measures were limited to HR, BP, and SPO2; the recording of other outcomes, such as HR variability, could allow us to gain more information. Finally, we tested only one driving simulator, and hence, to replicate our results, similar software would be required.
In the future, it will be important to understand, through specifically designed studies, the influence of immersive VR rehabilitation systems on autonomic aspects, which are important for motor learning aspects but even clinically significant in individuals suffering from a cardiovascular disability.
Conclusion
Cardiovascular rehabilitation aims to help individuals recover from heart events or procedures by improving their cardiovascular health and overall well-being. It encompasses a multi-faceted approach including exercise training, lifestyle modification, education, and psychological support for returning to a complete independence and functioning during the activities of daily living. The use of VR in cardiovascular rehabilitation has shown some positive findings in scientific literature, but also some controversial results.8,9,44 These controversies could be due to the developed tasks. We tested an immersive VR system with a car driving simulator that combined realistic 360° video and computer graphics. The task of driving in a realistic environment with streets of different width and other moving cars imply the involvement of cognitive functions such as attention, vigilance, visuo-spatial cognition, and upper limb motor functions, and it could also be an exerting and anxious task. This approach led to significant improvements in physical and mental health, psychological well-being, and upper limb ranges of motion, which were not observed in patients undergoing a conventional therapy program. Other parameters, such as oxygen saturation, showed improvements in both groups. In conclusion, immersive VR seems to be a promising technology that could be easily and positively integrated into cardiovascular rehabilitation, but it is fundamental to consider the type of digital task proposed to the patients according to a personalization of therapy within the framework of evidence-based rehabilitation. We selected a car driving simulated task because it allowed a progressive increment of difficulty, involving a mix of psychological and physiological factors, and ensured a high level of engagement among patients.
Footnotes
Ethical approval
All study procedures and protocols were in accordance with the Declaration of Helsinki and were approved by the Local Independent Ethical Committee of Santa Lucia Foundation (approval code: CE/PROG.795, date of approval 2 December 2019).
Consent to participate
The participants provided written informed consent to this study.
Author contributions
RDG, MI, and GT designed and developed the training content and led the project. RDG, supervised clinical trial. RC, AP, FG, SC, and CR contribute to data acquisition. DDB, CS, and GM monitored the data collection and were responsible for the qualitative data analysis and drafted the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received financial support for the research, authorship, and/or publication of this article: This article was financed by Sapienza University of Rome in the framework of the Project HeART (RM123188B4C92FF4).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Note
Clinical trial registration: the clinical trial is registered to ClinicalTrial.gov (ClinicalTrial.gov NCT07195279).