
Abstract
Background
Ambient Artificial Intelligence (AI) medical scribes are emerging technologies designed to streamline clinical documentation. Although promising results have been reported in medical disciplines, limited research has examined their suitability for use in allied health services.
Objective
To evaluate clinician acceptance and patient acceptability of an AI scribe within allied health settings at an Australian public hospital and health service.
Methods
A mixed-methods design incorporating surveys and semi-structured interviews with allied health clinicians and patients.
Results
In total, 97 eligible clinician survey responses were analysed, and 27 clinicians participated in interviews. Most clinicians reported high perceived ease of use, citing the AI scribe’s intuitive design and adaptability. However, customisation challenges impacted their overall user experience. Perceived usefulness was also high, with reported improvements in documentation quality, workflow efficiency, patient care, and job satisfaction. Clinicians emphasised the importance of reviewing AI-generated documentation to ensure accuracy and patient safety. They also highlighted that, in certain contexts, the use of AI scribes requires careful consideration to ensure patient care and engagement are maintained and that use with some patients (i.e., those experiencing persecutory delusions involving surveillance) may be contraindicated. While patient sample size was limited (19 surveys, four interviews), data indicated overall comfort with the AI scribe, although concerns were raised regarding data privacy and accuracy.
Conclusion
AI scribes show promise for allied health practice, offering multiple benefits recognised by both clinicians and patients. Their effective use may depend on clinician review of generated notes, careful consideration of patient wellbeing, and addressing usability challenges related to customisation and integration. Responding to the concerns raised by both groups may be key to ensuring confident and sustainable adoption.
Keywords
Introduction
There are high expectations for artificial intelligence (AI) scribes to revolutionise healthcare documentation. 1 Ambient AI medical scribes, or ‘AI scribes,’ also referred to as digital scribes, are a recent technological advancement that uses machine learning to enable real-time recording and transcription of clinical encounters.1–4 As the patient and clinician interact, the information is automatically recorded and transcribed according to the clinician’s role, tone, and preferred output format, such as a medical note, letter, or referral form.3,4 This technology aims to streamline documentation, enabling clinicians to focus more on patient care and thereby increase efficiency while reducing clinician burnout.5–7
A 2025 evaluation of an AI scribe involving 7,260 physicians from various specialties, including mental health, primary care, and emergency medicine, across multiple locations in the United States found significant reductions in time spent on manual documentation, alongside improvements in physician–patient communication and increased work satisfaction. 4 Similar benefits have been reported in other evaluations of AI scribes among physicians.8–12 However, potential risks have also been identified, including concerns about data privacy and security, transcription inaccuracies, overreliance on technology, and integration challenges.1,13,14 Despite these risks, discourse to date suggests that the benefits of AI scribes outweigh potential drawbacks, and overall findings remain promising.2,4
Nonetheless, most AI scribes have been developed and tested primarily for use by medical doctors, with limited consideration of the workflows, documentation styles, and communication patterns of other healthcare professionals including nurses and those in allied health. 15 Specifically, allied health makes up the second largest health workforce in Australia, however few previous studies have explicitly focused on the experiences of allied health clinicians, highlighting the need for further investigation.15–17 One study examined the use of an AI scribe in simulated outpatient consultations involving five medical consultants and three allied health professionals in the United Kingdom. 16 The study compared the use of AI scribes to traditional documentation methods and found improvements in documentation quality and operational efficiency. Participants, including allied health professionals, recognised the AI scribe’s potential to enhance documentation, highlighting its promise for integration into allied health practices. 16
More recently, Evans et al. (2024) conducted a mixed-methods study examining the use of an AI scribe in Australian private practice settings for allied health. The study surveyed 119 allied health professionals, the majority of whom were physiotherapists (76%), followed by podiatrists (10%), occupational therapists (8%), and exercise physiologists (5%). 17 They also conducted follow-up interviews with 15 allied health professionals. Findings showed a significant reduction in time spent on notes and out-of-hours documentation, alongside an average 5.8% increase in productivity. Interviews revealed that the AI scribe had a positive impact on the therapeutic alliance and administrative workload. 17
While both these studies offer valuable insights into the role of AI scribes in allied health, particularly in improving documentation workflows, further research is needed to assess their acceptance and effectiveness in real-world clinical settings involving a broad range of allied health professionals. 15 Notably, the Evans et al. study was conducted in Australian private practice, which may limit the generalisability of its findings to public health settings. 17 Gaps in knowledge also remain regarding the long-term impact of AI scribes on clinical workflows, patient safety, and the potential for biased AI outputs.1,14,18,19
These gaps highlight the need for further research to evaluate the application of AI scribes in diverse clinical settings within allied health. To address this, the present study aimed to generate evidence to guide decision-making regarding their adoption within public health allied health services, emphasising both potential advantages and associated challenges and risks. By exploring staff and patient perceptions, this study sought to assess the suitability of AI scribes, identify areas requiring safeguards or additional support, and, where appropriate, enhance acceptability and inform broader implementation.
This paper focuses on the acceptance of the AI scribe through the lens of the Technology Acceptance Model.
20
A separate paper reports the COM-B analysis, which explores the behavioural determinants of adoption,
21
providing a complementary understanding of why and how clinicians engage with the technology beyond their perceptions of usefulness and ease of use. The research questions answered in this paper include: 1) What factors influence allied health clinicians’ acceptance of the AI scribe, particularly in relation to its perceived usefulness and ease of use within a public hospital and health service setting? 2) What factors influence patient acceptability of the AI scribe in an allied health public hospital and health service setting?
Methods
Methodology approach
This study adopted a pragmatic paradigm, which prioritises practical solutions and the use of multiple methods to address complex research questions. 22 This study used a convergent mixed-methods design, combining survey and interview data to explore the integration of the AI scribe into clinical practice. 23 While the interviews offered a deep, nuanced understanding of participant experiences, the surveys offered additional breadth, reinforcing and triangulating the key themes. 24 This combined approach enhanced the validity of the findings and enabled a comprehensive understanding of the factors shaping acceptance.
Setting
This study was conducted within an Australian public hospital and health service operating across a rapidly growing metropolitan area. The hospital and health service employs approximately 1,600 allied health professionals and serves a population of over 700,000, providing care through two hospitals (inpatient and outpatient services) and community centres. 25
Stakeholder and consumer involvement
This research was conducted by a multidisciplinary team comprising hospital consumers, researchers, allied health clinicians, clinical leaders, and a digital health team member, enhancing the legitimacy and relevance of the study. The consumer representatives were recruited through the health service’s Consumer Advisory Group. One had prior research experience, while the other was newer to the research process. Both were remunerated for their involvement. They participated in key team meetings and provided feedback on the study design, research materials, data interpretation, write-up and are listed as co-authors. One consumer conducted interviews with some patient participants. In addition, a reference group composed of consumers, health service, digital and research leaders, and clinicians was established to provide guidance at key stages of the project, further strengthening the study’s rigour.
Participants and recruitment
Eligible clinician participants included allied health clinicians from professions such as physiotherapy, occupational therapy, social work, dietetics, speech pathology, pharmacy, psychology, audiology, and podiatry. At the start of data collection, around 280 clinicians had been given access to the AI scribe. Patients were eligible if the AI scribe had been used during their allied health consultation and were able to complete an online survey. Their family members, carers, or support workers were also invited to respond to the survey. A convenience sample was used for both the clinician and patient surveys, while purposive sampling was employed for the interviews to ensure disciplinary diversity among clinicians implementing the AI scribe, and patients experiencing it.
Survey and interview invitations were distributed to clinicians via email, team meetings, and targeted outreach using AI scribe usage data. Patients were recruited through clinicians, who provided a handout with a QR code linking to the survey following an AI scribe-supported consultation. All survey respondents could opt into a follow-up interview. Participation was voluntary, with informed e-consent obtained. Patient survey participants could enter a draw for one of three $30 gift cards, and patient interview participants received a $25 gift card.
Data collection
Quantitative and qualitative data were collected concurrently between August and October 2025. Both clinician and patient surveys were administered via REDCap over six weeks. The clinician survey was guided by the Technology Acceptance Model and varied slightly depending on whether the participant was an adopter or non-adopter of the AI scribe. 20 This paper focuses on perceived ease of use and usefulness, drawing on insights from AI scribe adopters. Experiences of non-adopters are reported separately. Adopters completed Likert-scale questions across three broad areas (perceived ease of use, perceived usefulness, and overall usefulness), along with five free-text questions and five questions on usage and demographics (Supplemental Item 1). The patient survey included four demographic questions, seven Likert-scale questions, and one free-text question (Supplemental Item 2).
To further explore experiences and perspectives, semi-structured interviews were conducted via Microsoft Teams. Interested participants received an electronic consent form through REDCap, and demographic data were collected upon consent. Three tailored interview guides were developed and piloted: for clinician adopters, non-adopters, and patients (Supplemental Items 3-5). Guides explored experiences and factors influencing acceptance and acceptability, with the Technology Acceptance Model informing clinician questions and the Theoretical Framework of Acceptability guiding patient interviews.20,26
All interviews were conducted and recorded via Microsoft Teams at a time convenient for participants. Clinician interviews were conducted by a researcher (LR) with experience in interviewing and a social work background. Patient interviews were conducted by either LR or HS, a consumer representative, depending on availability. Recordings were transcribed using Microsoft Teams, and LR reviewed each transcript against the audio, removed identifiable information, and assigned a unique participant ID (C# for clinicians and P# for patients).
In line with current qualitative research guidance, data saturation was not considered a goal, as the purpose of qualitative inquiry is to explore depth and richness of experiences rather than to achieve statistical completeness; instead, the focus was on gathering sufficient data to enable meaningful insights into participant perspectives. 27
Data analysis
Survey responses were exported from REDCap into Microsoft Excel. Descriptive statistics (frequencies, percentages) summarised closed-ended items, while open-ended responses were thematically analysed in Excel. Clinician interview transcripts were analysed thematically using Braun and Clarke’s six-step framework. 28 Analysis began with familiarisation with the transcripts. Coding was conducted inductively, with codes generated directly from the data in response to the research questions. Coding was iterative, with codes refined and revised as analysis progressed. Codes were then examined for patterns and grouped into potential themes, which were reviewed and refined to ensure coherence and clarity. A final analytic report was produced, with themes illustrated using verbatim participant quotes. Themes were discussed within the research team to support analytic rigour. Given the small number of patient interviews, these data were not subjected to full thematic analysis. Instead, a pragmatic qualitative approach was adopted, whereby patient transcripts were reviewed to identify key insights relevant to the research questions, and illustrative quotes were selected to complement the clinician findings.29,30
Data were synthesised using a qualitatively driven mixed-methods approach, with qualitative data given interpretive priority due to their depth and richness relative to the survey data. Interviews provided detailed contextual insights into experiences and perceptions, while surveys offered complementary breadth and supported triangulation of key themes. Qualitative survey responses were reviewed alongside interview data to assess alignment; however, they did not contribute additional or distinct insights and are therefore not reported here. This approach aligns with qualitatively driven mixed-methods guidance, in which qualitative findings form the primary interpretive lens. 31
Ethical approval was obtained from Gold Coast Hospital and Health Service (GCHHS), Human Research Ethics Committee (HREC/2025/QGC/118766). Research governance approval was given by the Gold Coast Hospital and Health Service (SSA/2025/QGC/118766).
Results
Clinician demographics.

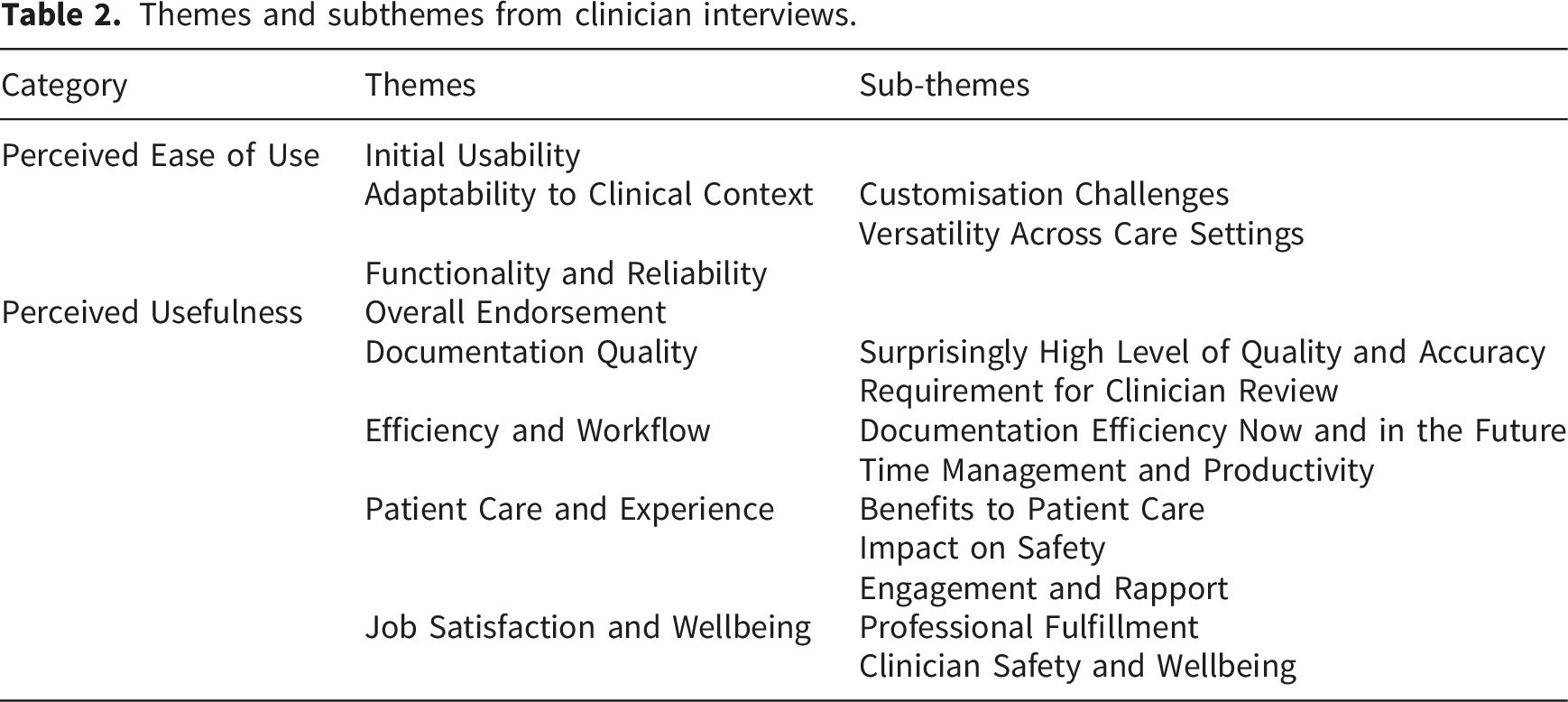
Themes and subthemes from clinician interviews.
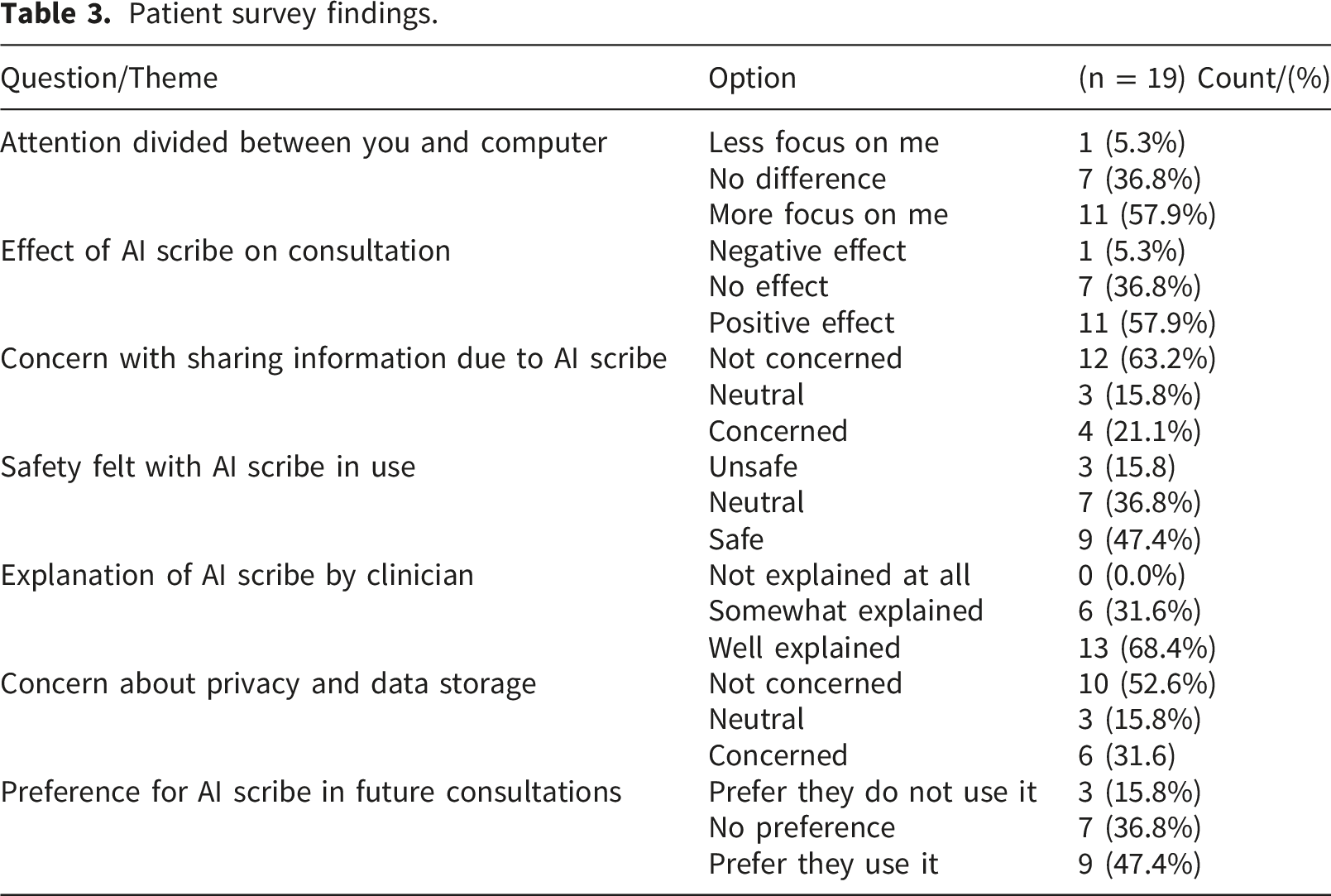
Patient survey findings.
Perceived ease of use
Perceived ease of use captures participant views on the level of effort required to use the AI scribe, focusing on intrinsic factors. It encompasses three key themes: initial usability, adaptability to clinical context, and functionality and reliability. Figure 1 presents details on clinician survey responses related to perceived ease of use. Supplemental Item 7 provides a summary of survey findings, reported as n and %. Clinician ratings of AI scribe ease of use (survey data).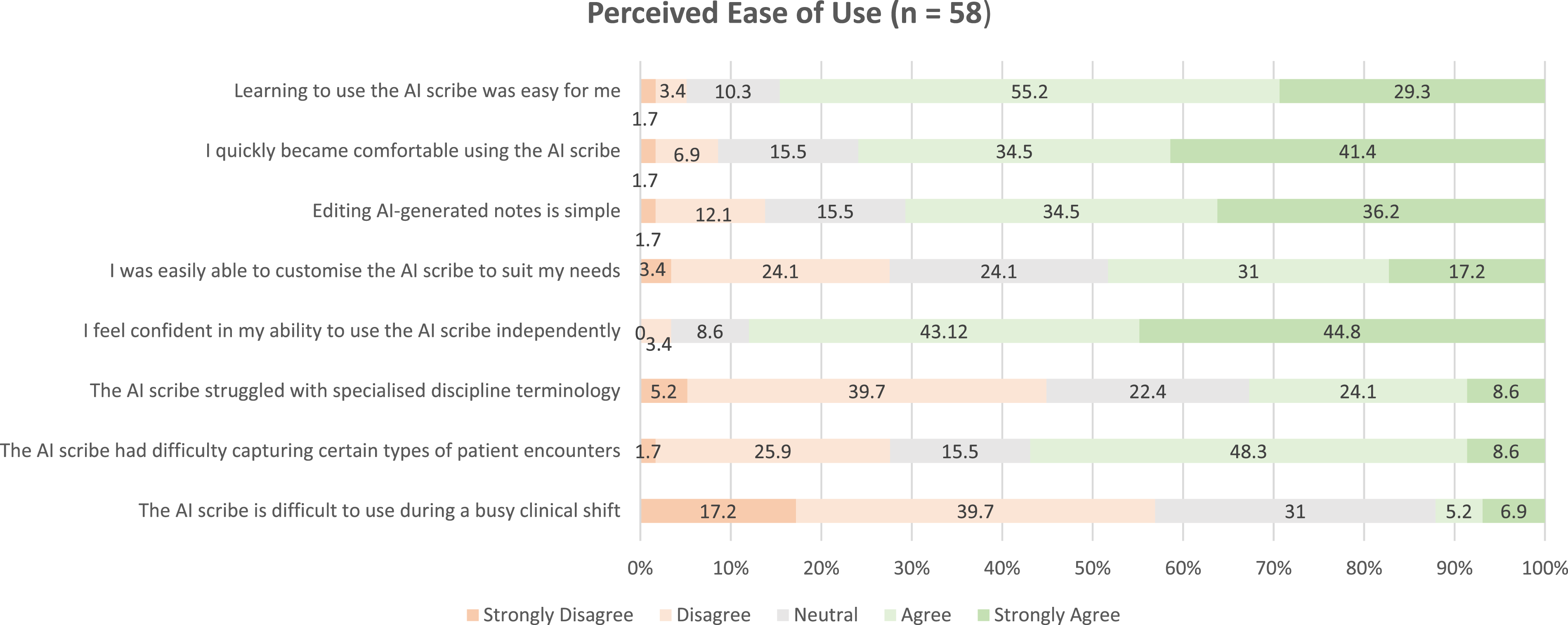
Initial usability
All interview participants who had adopted the AI scribe had completed the online training provided by the health service and had used it for at least one month before the interview. Most described the system as straightforward and intuitive, requiring minimal guidance to get started: “The functionality has been easy to use in terms of setting up, getting started” (C24). This perception was echoed in the survey data, where 84.5% (n = 49) of clinicians agreed or strongly agreed that learning to use the AI scribe was easy, and 87.9% (n = 51) felt confident using it independently. Several clinicians found it easier than expected: “I was a bit daunted at first, but once I started using it, it’s actually much easier to use than I anticipated” (C25). Survey responses supported this sentiment, with 75.9% (n = 44) of clinician respondents agreeing that they quickly became comfortable using the AI scribe. Apart from one isolated access issue, few initial barriers were reported.
Adaptability to clinical context
Customisation challenges
Customisation emerged as the main usability challenge, with clinicians describing the setup of templates for different clinical settings as time-consuming and tedious, though many reported it was worthwhile: “I think that might take a bit of time and effort, and that could be a barrier for others, but I can see the benefits” (C14). Those working across multiple settings found this particularly demanding: “I use about seven or eight templates … figuring out how best to set all those up for it to work the best took me, you know, took me a fair bit of time” (C12). Customisation was seen as an iterative process of refinement, balancing clinical accuracy with personal style preferences. This complexity was reflected in the survey responses: only 48.2% (n = 28) of clinician respondents agreed that it was easy to customise the AI scribe to suit their needs, suggesting that while the tool was usable, tailoring customisation required effort.
Versatility across care settings
Clinicians reported using the AI scribe across a wide range of settings, including the emergency department, inpatient wards, rehabilitation wards, outpatient clinics, community health services (including home visits), mental health and virtual care services. It was used in both adult and paediatric contexts, and across different modes of delivery, including in-person, telehealth, and telephone consultations. Clinicians reported the AI scribe was usable across diverse settings, whether accessed on a computer or mobile phone, and in both quiet and noisy environments, as well as during single encounters or when multiple speakers were involved. Survey data partly supported this perception of the AI scribe’s versatility: 56.9% (n = 33) of clinician respondents agreed that it was usable during a busy day. However, an equal proportion also reported that the tool struggled to capture certain types of encounters. Ease of use was also hindered when documentation required multiple small entries rather than a single free-text note: “I’ve got to divide all those sections up, it makes it a bit tedious” (C1).
Functionality and reliability
Helpful features included the notepad (for preparing background information) and speech-to-text functions, which supported use when ambient listening was unavailable. Some clinicians transitioned from dictation to ambient use over time: “I was using the smart dictate post-session for the other clinics, but now that we’re fine to use it in inpatient” (C14). Conversely, limited integration with the electronic medical record restricted formatting options, and occasional technical failures (e.g., timing out, loss of data) affected perceptions of ease and reliability. These issues led some to monitor the system during consultations or adopt contingency methods: “I don’t quite trust it enough not to take notes” (C9). Despite these frustrations, clinicians still considered the AI scribe easier and requiring less effort than manual note-taking, with 88.9% (n = 48) of clinician respondents agreeing that they enjoyed using it.
Perceived usefulness
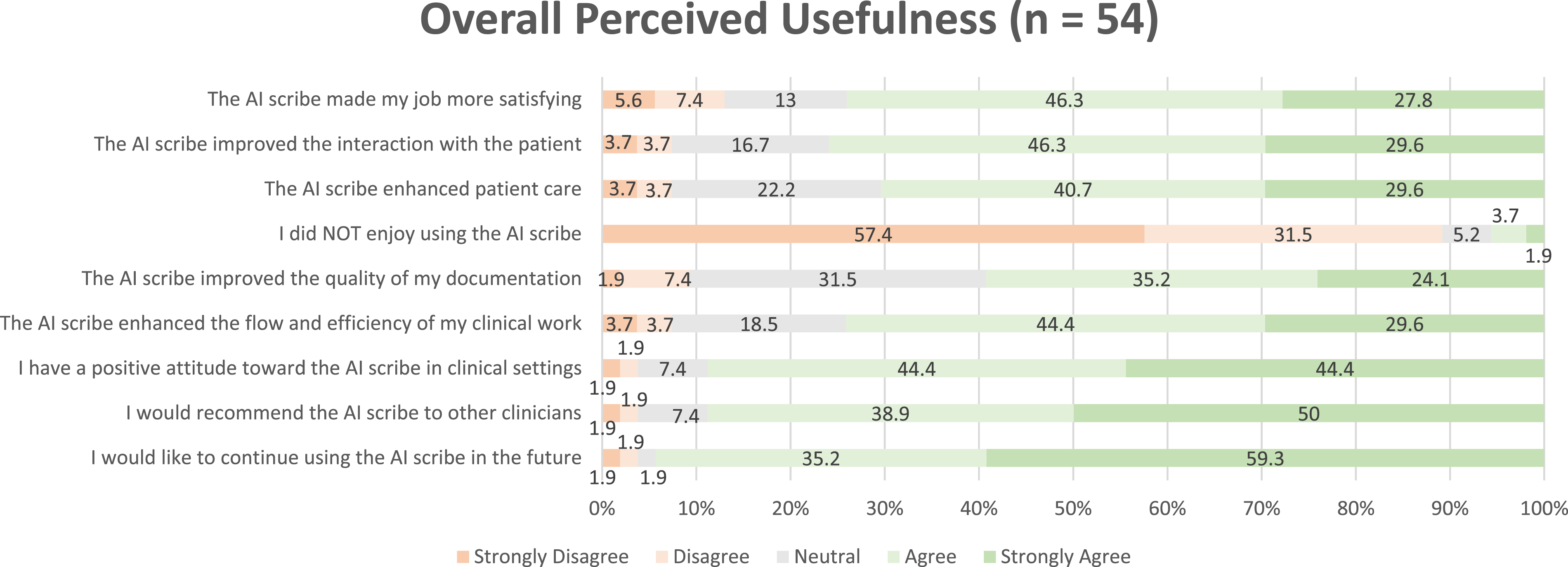
Perceived usefulness reflects the extent to which the AI scribe was viewed as providing value across several key themes, including overall endorsement, documentation quality, efficiency and workflow, patient care and experience, and clinician job satisfaction and wellbeing. Figures 2 and 3 present additional details on survey responses relating to perceived usefulness. Supplemental Items 8-9 provide a summary of survey findings, reported as n and %. Clinician ratings of AI scribe usefulness (survey data). Clinician ratings of overall AI scribe usefulness (survey data).
Overall endorsement
Clinicians generally perceived the AI scribe as highly useful across multiple areas, with several describing it as indispensable: “I’d struggle not using it from now on. I dread the day that I ever have to not use it, to be honest” (C19). Survey data supported this strong endorsement. 88.8% (n = 48) of clinician respondents agreed having a positive attitude toward the AI scribe in clinical settings and 88.9% (n = 48) agreed they would recommend it to other clinicians. The survey data also suggested a positive view of future use, with 94.5% (n = 51) of clinician respondents indicating they would like to continue using the AI scribe.
This sentiment was echoed in the patient survey data, where nearly half (47.4%, n = 9) of patient respondents expressed a preference for clinicians to use the AI scribe in the future. This strong endorsement was also reflected in the patient interview data. One patient, in particular, conveyed a high level of confidence and trust in the clinician’s use of the AI scribe. However, he acknowledged that this trust was partly informed by limited understanding: “I do, because I don’t know any different” (P1).
Documentation quality
Surprisingly high level of quality and accuracy
Clinicians were often surprised by the accuracy and quality of the AI scribe’s documentation after it was customised to their clinical context. Overall, the AI scribe effectively captured multiple speakers, improved language expression, and proved useful in handling discipline-specific terminology and documentation requirements: And I think we’ve all been very surprised by how well it can pick up on observations. We as a team go, ‘Oh wow! That’s an amazing tone of voice!’ We have a template for a mental state examination, and it writes it beautifully and generally quite accurately. (C14)
Several described improved clarity, detail, and capture of information compared to manually writing notes: “I think in that way it’s just like a lot more accurate, not relying on me trying to remember stuff from earlier in the day” (C26). Again, this was reflected in the survey, with more than half (59.3%, n = 32) of clinician respondents commenting that it enhanced the overall quality of their documentation. Notably, respondents highlighted improvements in the accuracy (44.5%, n = 24), organisation (46.3%, n = 25), and language and/or expression (61.1%, n = 33) of their clinical notes.
Several clinicians also noted its capacity to transcribe voices that clinicians might otherwise struggle to capture, including those of patients with non-English speaking backgrounds, speech disorders such as dysarthria, or softer voices: “It picks up very quiet voices and quite significant dysarthria. It’s picked up quite well” (C25). Non-native English speakers highlighted the tool’s ability to improve written expression: English is not my first language, and I also have difficulty building sentences and speaking in a very formal way. That’s always been my gap, I guess. So for me, that’s another highlight of the program that I can say something in a very simple way, but the scribe tool will actually put it into a very beautiful sentence. (C20)
The potential for AI scribes to enhance the quality of documentation was also reflected in the patient interview data: “I understand the ethics of it, but I think that the benefits far outweigh the disadvantages in terms of having accurate information recorded about my health” (P4).
Requirement for clinician review
Despite perceiving the AI scribe as delivering a high level of accuracy and quality, clinicians emphasised the importance of reviewing outputs before inclusion in the patient notes. Accuracy concerns included content allocation to the wrong speaker, hallucinations (plausible-sounding but false outputs), spelling mistakes, omissions, and terminology errors, including difficulties with discipline-specific language (such as occupational therapy language related to play skills or psychological language describing mood) and Aboriginal and Torres Strait Islander place names.
In addition, clinicians highlighted the risk of increased inaccuracies if the AI scribe failed during a consultation, particularly where clinicians had been relying on it to capture information. These concerns about accuracy were also reflected in the patient data, with one participant expressing doubts about the technology’s reliability and citing this as a reason she did not want it used in her care: “I could imagine that it would be time saving, but I'm still a little bit worried that they’re not accurate enough… we haven't quite got there in the technicalities of doing those things” (P3)
Clinicians also described some quality issues, including the use of tone, expression and problematic language in its output: “With my impression, we want to be using neurodiversity affirming and strengths-based language. So sometimes some of it is quite pathologising or quite clinical” (C27). Structure and formatting challenges included inconsistency, provision of excessive or insufficient detail, and outputs not aligning with participants’ required format, which was a particular source of frustration. Meaning-related issues involved misinterpretation of language and contextual cues, both of which were perceived as having the potential to compromise patient care and safety: So, if the patient says, ‘Oh, look, you know, sometimes I just wish the earth would swallow me up’. It'll miss that altogether, you know. And it just won't even comment that, it won’t have got that she’s feeling suicidal. It won't have interpreted that. (C9)
Clinicians regarded reviewing the AI scribe outputs as an integral part of safe practice: “I don’t think that the AI is really doing the work for us. It's just helping us to do it quicker or better” (C8). Patients also expressed confidence in the review process, suggesting it was sufficient to prevent inaccuracies in their medical record: “It’s no different from them manually recording what was said anyway… if anything, it just lets something else do it, and they check it” (P2).
Efficiency and workflow
Documentation efficiency now and in the future
Clinicians consistently reported that the AI scribe improved efficiency in completing documentation, referrals, and letters: “So, I think before [the AI scribe], I would have probably had to finalise my documentation the following week, but because I use [the AI scribe], I got all my documentation done in that one day” (C27). The clinician survey findings supported this view, with 74.0% (n = 40) of respondents agreeing that the AI scribe enhanced the flow and efficiency of their clinical work. Some clinicians suggested that with further training, experience, and technological advancement, the potential for even greater documentation efficiency in the future could be realised: “So, I’m pretty optimistic that like once I get a bit more confident, particularly around that prompting the template structure, that the outcome will be such that the benefits will outweigh the costs within the immediate future” (C16).
Time management and productivity
During interviews, clinicians described improved time efficiency when using the AI scribe, and 77.7% (n = 42) of clinician respondents agreed that it helped them save time. This additional time was used for non-clinical activities such as professional development, quality improvement, or research, and in some cases allowed participants to see more patients. However, a few clinicians noted that the AI scribe had a limited impact on time savings during the initial learning phase, as they familiarised themselves with it. One clinician also expressed concern that increased efficiency might lead to unrealistic expectations: But it has occurred to me that if I get more efficient, people might start saying I can see more patients in my day, and I would hate to think that would take me back to the situation of being even more unable, potentially, to get my work done. (C11)
Patient care and experience
Benefits to patient care
The AI scribe was seen to improve patient care by enabling more time with patients and better preparation for consultations: It’s basically just given me more time to then focus on my next task. So instead of having, you know, another hour and a half after the clinic’s finished writing letters, I can then start prepping for my next clinic (C5). We’re sometimes in community, we’re running around with a lot of different competing priorities, and sometimes the GP letter is that last point of contact. It might get left to the wayside… the AI scribe gives you that access, it's already generated, and you can flick that off straight away. (C22)
Impacts on patient safety
Despite the acknowledged potential benefits to patient care, clinicians raised concerns about risks associated with using the AI scribe. These included potentially serious impacts if documentation was not appropriately reviewed and errors or harmful language remained in the patient record, as well as the risk of over-documentation that exposed unnecessary details of a patient’s life. Additionally, clinicians raised specific safety risks for patients experiencing acute mental illness, particularly those experiencing persecutory delusions related to surveillance. Clinicians emphasised the need for caution and sensitivity when using the AI scribe in this context to protect the safety and wellbeing of patients: “So you can’t use it for anybody who’s thinking that the TV’s bugged or you know my neighbours have hacked my house, you can’t!” (C9). Despite these concerns, clinicians did not tend to perceive data security issues to pose a significant risk to patient safety, reporting confidence in the technology to protect patient data and minimal concern about potential adverse impacts. The majority of patients surveyed felt neutral or safe with the AI scribe’s use, 15.8% (n = 3) reported feeling unsafe and 31.6% (n=6) reported concerns regarding privacy and confidentiality.
Engagement and rapport
Most clinicians reported that the AI scribe enhanced patient engagement and rapport as it allowed greater patient attention, active listening, eye contact, and better interpretation of facial expressions, without the distraction of typing or the cognitive demands of remembering information for later documentation: Knowing that the AI scribe is recording that rather than me furiously taking notes… it’s allowed me to then, you know, focus on the client more… it has a really nice flow on effect for the start of that kind of therapeutic relationship. (C24)
One patient also noted that they were able to focus more on the conversation when it was not interrupted by the clinician looking at their computer: “It keeps my thoughts more front and centre” (P2). The survey supported these findings, as 83.3% (n = 45) of clinician and 57.9% (n = 11) of patient respondents agreed that the AI scribe allowed the clinician to focus on the patient. However, a few clinicians who regularly conducted psychologically focused consultations felt the AI scribe had little impact on engagement or rapport, as they already maintained strong connections with their patients.
Clinicians noted that the requirement to verbalise their assessments for the AI scribe held potential value for patients, as it enabled the patient to hear more detail about what was occurring and to gain greater insight into their clinician’s perspectives during the consultation: “It’s making me really be mindful of talking through what I'm doing… And so that's probably another benefit to the patient of using it” (C24). However, some clinicians described reverting to manual documentation for sensitive contexts: “So, for instance, a patient with an eating disorder… we never explicitly discuss what their calorie intake or what their actual weight is in the consult” (C1).
Another concern raised by clinicians was that the presence of the AI scribe might discourage patients from engaging or disclosing sensitive or personal information: “You know that’s starting their healing journey, I guess. And I think the opportunity for that will be lost. So, we'll have people that are holding on to their trauma because we've implemented [the AI scribe]” (C4). In some situations, this made them hesitant to use the AI scribe with patients who were difficult to engage, fearing it could further contribute to disengagement.
This concern was not strongly reflected in survey data, with 94.5% (n = 51) of clinicians reporting that patients appeared comfortable with the use of the AI scribe, and 79.0% (n = 15) of patients indicating that they were either neutral or unconcerned about sharing information when it was in use. Furthermore, several clinicians expressed surprise at how openly patients, particularly those with complex medical or psychosocial circumstances (such as severe mental health issues, domestic violence, or sexual assault), shared personal information despite its use.
Job satisfaction and wellbeing
Professional fulfillment
Clinicians described experiencing greater professional fulfilment through using the AI scribe, as it allowed them to focus on the most meaningful aspects of their role, particularly patient interaction, rather than documentation. This fulfilment was linked to a perceived improvement in patient care, efficiency, and documentation quality: “Being in a caring profession, I think being as engaged as I possibly can be within the means and confines of my work environment is of high value to me” (C1). This was reflected in the clinician survey as 74.1% (n = 40) agreed that the AI scribe made their job more satisfying.
However, some clinicians expressed concerns that reliance on the AI scribe could erode professional skills, create self-doubt, or reduce confidence in their own clinical reasoning and documentation: “We don’t want them [the allied health clinician] necessarily to be relying on the impression section [created by the AI scribe]… part of our practice is we review that, and the clinician generates the conceptualisation” (C6). Some clinicians expressed concern about losing their voice and sense of ownership in their documentation, which could affect how their work is interpreted in referrals and related processes. However, many felt that as long as the information was captured accurately, that was the most important factor.
Clinician safety and wellbeing
Clinicians reported that the AI scribe significantly improved their sense of safety and wellbeing, primarily by reducing the burden of documentation and associated stress: Because we have that pressure for documentation to be completed, that’s hanging over you, I guess, that can be a stressor. Obviously, you learn to let it go, but just knowing that… I’m going to have [the AI scribe] running… makes me feel confident that I will be able to achieve everything. (C27)
The clinician survey supported this finding, with 66.7% (n = 36) agreeing that AI scribe reduced stress related to documentation. It was also reported to help limit after-hours work and enabled participants to take breaks during the day, supporting both wellbeing and quality of care. One clinician even noted they might have left their role had the AI scribe not been introduced: Liberated, maybe relieved, I was starting to wonder how much longer I had in this role because of the tiredness and the mental load it was having on me. Because they are very complex patients, basically. So, I feel invigorated to stay on longer. I’m not feeling like I have to get to the point of going; I can't keep doing this any longer. (C# not included for confidentiality)
Physical wellbeing was also positively impacted, with a reported reduced risk of repetitive strain injuries (RSI) associated with manual documentation. However, one clinician flagged a safety concern when using the scribe during phone calls without a headset, which was ergonomically problematic.
Discussion
This study explored clinician acceptance and patient acceptability of an ambient AI medical scribe within allied health clinical practice in a large Australian public hospital and health service. Findings demonstrated high levels of perceived usefulness and ease of use among allied health clinicians, with many describing the AI scribe as indispensable to their workflow. The technology was associated with improvements in documentation quality, clinical efficiency, patient care, and clinician wellbeing. Patient responses were generally positive or neutral, with a few concerns raised regarding privacy or comfort. These findings contribute to the growing body of evidence supporting the integration of AI scribe in healthcare and extend prior research by including a broad range of allied health disciplines in real-world settings.
Most clinician participants found the AI scribe intuitive and easy to learn. This aligns with findings from a recent systematic review involving predominantly doctors and medical students, 32 as well as a study of allied health clinicians. 17 In our study, however, perceived ease of use was affected by challenges with customisation. Tailoring the AI scribe to produce the required outputs was often described as time-consuming and demanding. This was compounded by the limited capacity of allied health clinicians, a phenomenon well-documented in the literature.33,34 While customisation challenges have been noted in other studies, they were not reported as a significant concern,2,13 suggesting that this may be a more prominent consideration in allied health contexts.
The potential for heightened customisation challenges among allied health clinicians may stem from the fact that many AI scribes are designed, or at least initially developed, around medical workflows and documentation styles. 1 The greater need for discipline-specific templates and the additional effort required to adapt the tool to allied health practice styles may therefore represent more of a barrier to adoption or optimisation compared to medical colleagues. These findings highlight the importance of designing AI scribes that are flexible and aligned with the diverse documentation needs of allied health professionals, or providing support to assist with customisation.
Clinician participants consistently reported that the AI scribe added value across multiple areas, including documentation quality, workflow efficiency, patient care, and professional fulfilment, which mirrors the broader literature on this topic.4,7–9,11,16,17,35–37 These perceived benefits, together with the reported ease of use, explain the strong acceptance of the AI scribe among clinicians, 20 with the majority of participants in our study expressing a strong desire to continue using the tool.
While the present study did not quantify the workflow efficiencies following use of AI scribes, findings support previous studies in allied health.16,17 Considering the global shortage of allied health professionals, 38 any potential improvements to documentation efficiency which may optimise existing staffing resources are promising and warrant further investigation. A novel finding from the present study however was the perception that these efficiency gains could inadvertently lead to an increased workload - a perception managers may need to consider when communicating the benefits of AI scribes to clinicians.
Documentation burden associated with electronic health records may not only lead to negative impacts on time but also contribute to burnout of health professionals and decreased job satisfaction.39,40 In the present study, clinician participants reported reduced stress and improved job satisfaction, resulting in part from less documentation burden and better time management. In a healthcare environment where clinicians face increasing pressure and burnout is becoming more prevalent, this study adds to the growing evidence that AI scribes have the potential to help alleviate these challenges.4,12,41,42 Specifically, this may in turn support the retention of allied health staff, reducing the high turnover often seen in this workforce. 38
Encouragingly, allied health clinicians were surprised by the level of quality and accuracy the AI scribe delivered following customisation. However, they emphasised the importance of clinician review to ensure that critical patient information is accurately captured and reported. While clinicians perceived the AI scribe’s output to be of high quality, our study did not include an objective measure of quality or accuracy. Moreover, there is currently no validated instrument for assessing the quality of allied health documentation, such as the Physician Documentation Quality Instrument (PDI-9) or the Sheffield Assessment Instrument for Letters (SAIL), used in medical documentation studies to enable consistent evaluation.43,44 This highlights a key gap for future research: the need for a validated measure to assess AI scribes’ impact on documentation quality, as emphasised in existing literature.9,45 Evaluating quality in allied health documentation may be particularly challenging, however, due to wide variation in documentation styles and professional expectations of what constitutes quality.46–48
While clinicians generally reported confidence in the accuracy and safety of the AI scribe and high acceptance, it should be noted that broader governance considerations remain critical to its responsible implementation. Key issues include accountability for errors, auditability of AI scribe outputs, and clarity around data processing arrangements. 45 Although clinician review can mitigate some risks, it has inherent limitations. Ensuring robust governance requires clear assignment of responsibility for decision-making, routine audit processes, transparent data handling practices, and adherence to relevant regulations and organisational policies. 45 Addressing these governance and accountability mechanisms is essential to maintain patient safety, build trust, and inform policy for the ethical and sustainable use of AI-scribes in practice. 49 Indeed, other research with health professionals, specifically nurses, has reiterated the importance of considering potential risks that AI presents to ensure ethical principles and values of professionals are upheld. 49
The AI scribe was perceived to enhance patient care by giving clinicians more time with patients, improving consultations and enabling stronger engagement and rapport during consultations. These findings align with previous studies involving both allied health professionals and physicians,4,17,32 adding to the evidence base that AI scribes can help strengthen the therapeutic alliance - that is, the bond between the patient and therapist. This is an important potential benefit, as a strong therapeutic alliance can facilitate patient engagement and has been reported to improve clinical outcomes in allied health literature.50,51 In contrast, some participants expressed concern about the AI scribe’s impact on patient care and safety in specific contexts, particularly with patients experiencing acute mental illness. Clinician participants reported exercising caution and self-monitoring its use, for example, in cases involving persecutory delusions involving surveillance. However, if such considerations are overlooked, there may be risks to patient safety.
Evidence on the efficacy and safety of AI scribes in acute mental health or more psychosocially complex settings remains limited. A recent scoping review identified no studies conducted specifically within mental health contexts. 3 While some studies have included mental health settings as part of broader evaluations of AI scribes across healthcare services,4,8 we identified only one study that focused specifically on mental health, examining neuropsychiatric symptom documentation in outpatient primary care. 52 This highlights the need for further research to inform hospital policies and clinical guidelines that ensure the safe use of AI scribes in these contexts, including the possible contraindication of AI scribe use with some patients or areas, for example, when patients experience persecutory delusions involving surveillance.
Patient interviews and survey responses indicated general openness to the AI scribe, with most reporting positive or neutral experiences. Patient acceptability may be influenced by perceptions of data security, with mixed views expressed: some patients felt confident that their data were handled securely, while others reported uncertainty or concern, although the limited number of patient interviews precluded strong conclusions. Although privacy and data security did not emerge as key themes in this analysis, these issues remain central to the ethical implementation of AI scribes, and future research should explore patient and clinician perspectives on data governance, transparency, and security safeguards in greater depth.
Strengths and Limitations
A key limitation of this study was the difficulty in recruiting patients, which constrained the depth of analysis from this group. Despite deploying several recruitment strategies, including the use of incentives, uptake remained low, and the reasons for this are unclear. Given clinicians’ observations in this study, alongside findings from other research, that patients are generally accepting or indifferent toward the use of AI scribes, some may question the value of further investigation into patient perspectives.4,17 While a priori sample size calculation was not undertaken, the small sample size and participants’ potentially limited exposure to the AI scribe may have influenced their responses. The risk of power dynamics when patients are asked to consent, combined with the fact that some patients expressed some strong objections underscores the importance of further understanding patient perspectives. 53 Developing insight into patient acceptability and addressing their concerns will be particularly important if AI scribes become a routine part of clinical practice.
As a qualitatively dominant mixed-methods study, the interviews provided the primary depth and insight into clinicians’ and patients’ experiences with the AI scribe, while the survey data complemented these findings by offering broader contextual understanding and confirming the wider relevance of emerging themes. A further strength of the study was the diversity of allied health clinician who participated, which contributed to a wide range of perspectives and enhanced the richness and applicability of the findings. Additionally, the relatively large qualitative dataset strengthened the credibility and robustness of the thematic analysis, supporting greater confidence in the transferability of the results.
While the Technology Acceptance Model 20 was the primary framework to examine perceived usefulness and ease of use of the AI scribe, key determinants of technology adoption, it does not fully capture broader considerations such as appropriateness, safety, or ethical implications that emerged from the clinician data. The Theoretical Framework for Acceptability for example may be useful in conceptualising the issues of ethicality, while an ecological validation framework intended for use of AI in clinical settings which covers safety, trust and accountability may also assist conceptualising future research. 26
Conclusion
This study provides valuable insight into the use of an AI scribe in allied health practice, demonstrating strong clinician acceptance and clear perceived benefits. The technology was associated with improvements in documentation quality, workflow efficiency, and patient care, while helping to alleviate one of the most persistent sources of burnout - the documentation burden. Although challenges with customisation and integration were reported, the findings highlight the transformative potential of AI scribes to positively reshape allied health clinical practice. As these tools become more widely adopted, ensuring they are adaptable, safe, and responsive to the complexity of real-world practice, while keeping clinician and patient wellbeing at the centre, will be essential to realising their full potential.
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Supplemental material
Supplemental material - Acceptance of AI scribes within hospital allied health settings: A mixed methods study
Supplemental material for Treatment Strategies for Acceptance of AI scribes within hospital allied health settings: A mixed methods study by Laura Ryan, Laetitia Hattingh, Dominic Wall, Hayley Stanich, Nicole Ross, Juan Da Cal, EJ Milne, Rachel Wenke in DIGITAL HEALTH
Footnotes
Author note
Microsoft Copilot and Grammarly were used to support language clarity, grammar, and readability during manuscript preparation. These tools were used solely to enhance expression and presentation; all substantive content, analysis, and interpretation remained the responsibility of the authors.
Acknowledgements
We acknowledge and pay respect to the people of the Yugambeh language region of the Gold Coast where this project took place, and all their descendants, both past and present. We want to thank the consumers and staff who participated in this study. We acknowledge the reference group members who provided advice during key stages of this project. Finally, we wish to recognise Gold Coast Health’s Allied Health Research Department for its in-kind support of the project.
Ethical considerations
Ethical approval was obtained from Gold Coast Hospital and Health Service (GCHHS), Human Research Ethics Committee (HREC/2025/QGC/118766). Research governance approval was given by the Gold Coast Hospital and Health Service (SSA/2025/QGC/118766).
Consent to participate
All participants provided informed e-consent prior to taking part in the study. For both the survey and interview components, consent was obtained electronically via REDCap. Participants were first presented with a detailed information sheet outlining the purpose of the study, what participation involved, potential risks, and data management procedures. They were also given the option to contact the research team to discuss any matters relating to the information provided before deciding whether to participate. The requirement for consent was not waived by the Human Research Ethics Committee, and written (electronic) informed consent was therefore obtained from all participants.
Author contributions
All the named authors (LR, RW, LH, DW, HS, NR, JDC, EJM) were involved in conceptualising and designing the project. LR and HS collected the data. LR analysed the data with input from RW. All the named authors contributed to the interpretation of the data. LR drafted the manuscript with input from RW. All authors reviewed the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available on request due to privacy/ethical restrictions.
Guarantor
Dr Laura Ryan accepts full responsibility for the integrity of the work as a whole, including the study design, data collection, analysis, interpretation, and the decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.