
Abstract
Background
Chronic heart failure (CHF) necessitates ongoing self-management to reduce hospital admissions and enhance clinical outcomes. Mobile health (mHealth) applications are promising tools. However, most lack validated content and user-centered design. This study aimed to identify and validate core content for a CHF-focused mHealth application through expert consensus.
Methods
A two-round Delphi study was conducted with 24 experts, including physicians, nurses, and patients with CHF. In round one, 39 self-management items were evaluated. Based on quantitative scores and qualitative feedback, 5 items were excluded, and 13 new ones were added. In round two, 44 of 47 items (93.6%) achieved consensus (x̄ ≥ 7.5). Psychometric indicators included standard deviation, Content Validity Ratio (CVR), Content Validity Index (CVI), and Intraclass Correlation Coefficient (ICC).
Results
Validated content was categorized into two domains. Domain 1: Recording Functionalities included Signs and Symptoms (x̄ = 8.23 ± 0.88) and Medication Management (x̄ = 8.52 ± 0.94). Domain 2: Therapeutic Education included five classes: Basic Concepts (x̄ = 7.90), Self-care and Disease Management (x̄ = 8.27), Recognition of Signs and Symptoms (x̄ = 8.03), Psychosocial Support (x̄ = 8.15), and Lifestyle Management (x̄ = 8.06). Inter-rater reliability demonstrated variable but generally moderate to good agreement across items (ICC range 0.31–1.00), with statistical significance (p < 0.05). The overall CVI reached 0.82.
Conclusions
This study validated 44 items for CHF self-management via mHealth. The participatory, evidence-based approach ensures clinical relevance and usability. Implementation may improve adherence, decrease readmissions, and support quality of life.
Keywords
1. Introduction
Heart failure (HF) is recognized as one of the leading causes of morbidity and mortality worldwide. It primarily affects adults aged 65 and older. Its prevalence continues to increase due to aging populations and better survival rates for those with cardiovascular conditions.1,2 In developed countries, an estimated 1–2% of adults live with HF, with rates rising to 10% in those over 70. This burden strains healthcare systems. Nearly 50% of patients are readmitted within six months of hospital discharge.1,3
Self-care is now a key part of heart failure management. Conventional therapeutic education often falls short in sustaining adherence and effective follow-up. 4 In this context, mobile health (mHealth) technologies have emerged as promising tools. They provide continuous education, remote symptom monitoring, and personalized patient support. Evidence shows that digital health interventions can improve medication adherence and reduce hospitalizations for people with chronic diseases, including heart failure. 5
The World Health Organization (WHO) has emphasized the development of digital tools that foster equitable, accessible, and person-centered care. 6 This is reflected in its Global Strategy on Digital Health. Such digital transformation strengthens access to services. It also enhances functions like real-time clinical decision-making and continuity of care. 7 Despite their potential, most heart failure-specific mobile applications currently lack rigorous clinical validation. They are also not sufficiently tailored to individual patient needs. 5
A recent systematic review by Camino et al. (2025) critically analyzed mobile applications for chronic disease management and identified several methodological shortcomings. Among the most frequent were the lack of standardized development protocols, limited involvement of end users during design phases, scarce reporting of clinical validation, and insufficient integration with existing healthcare systems. These gaps were associated with poor usability, reduced patient engagement, and limited long-term adherence, ultimately hindering their integration into clinical practice. 8 When appropriately designed, however, these tools have been shown to reduce mortality, empower self-care, and improve clinical outcomes, particularly when they incorporate features such as symptom tracking, medication reminders, and therapeutic education through interactive or avatar-based approaches.9–14
A major limitation of many existing tools is the lack of patient involvement during development. This exclusion hampers the effectiveness and real-world applicability of these solutions.5,9,11,13,15,16 Addressing this gap requires participatory approaches that integrate both clinical expertise and patient perspectives. The Delphi method is widely recognized as a robust strategy for reaching consensus on the content of health interventions, bringing together diverse viewpoints to ensure clinical relevance, clarity, and usability.17,18
Therefore, the objective of this study was to identify and reach consensus on the essential content for developing a mobile application focused on therapeutic education and the monitoring of individuals with heart failure, using the Delphi method to ensure clinical appropriateness, clear communication, and practical applicability in real-world settings.
2. Materials and methods
2.1. Study design
A structured consensus study used the e-Delphi method, an iterative technique in which a group of experts participates in multiple rounds of online surveys to reach agreement. This method, widely used in health research, helps develop and validate content, especially when little empirical evidence is available. Experts complete secure, anonymous digital questionnaires in each round. This allows participants to reflect on their views, avoids undue influence from stronger voices in the group, and supports objective decision-making.17,19–21
2.2. Process coordination and implementation
The study was coordinated by a team of six professionals with expertise in chronic heart failure (CHF), clinical research, and academic teaching. This group designed the methodological protocol, selected participants, developed and reviewed the questionnaire, analyzed the data, and oversaw the consensus process.22,23
Questionnaires were distributed and collected via a secure online platform (Google Forms), ensuring anonymity and data traceability.
2.3. Phases of the e-Delphi Process
The Delphi process was conducted in two rounds. In the first round, participants rated 39 items on a 9-point Likert scale (1 = not relevant, 9 = highly relevant). Items were considered accepted if their mean score was≥7.5. Those scoring between 7.0 and 7.4 were revised based on participant feedback and reassessed in the second round. Items with a mean <7.0 were excluded. This decision framework was based on measures of central tendency (average values) derived from participant ratings.
2.4. Questionnaire development
The coordinating group developed the initial version of the questionnaire and validated its content through a nominal group composed of professionals from the disciplines included in the Delphi panel: family medicine, family nursing, advanced practice nursing in heart failure, internal medicine, cardiology, and patient representatives. This preliminary step ensured the internal consistency, clarity, and relevance of the items.
The questionnaire was structured into two domains: the first focused on functionalities for recording symptoms, signs, and medication use, while the second addressed therapeutic education, including basic knowledge of heart failure, self-care, identification of warning signs, lifestyle adjustments, psychosocial support, and navigation of the healthcare system.
The final version was distributed and collected using a secure online platform (Google Forms), guaranteeing participant anonymity and data traceability throughout the Delphi process.
2.5. Expert panel selection
Experts were selected using purposive snowball sampling and invited via email and professional networks. Professional background and experience in heart failure management were prioritized. The final panel had 24 experts, evenly distributed among six categories: family medicine, family nursing, advanced practice nursing, internal medicine, cardiology, and expert patients. Selection criteria included professional credentials, clinical experience, and involvement in education or research. Researchers did not participate in the panel.
The study included only highly qualified professionals. Expert competence was assessed using the K coefficient. This was calculated as the average of two parts: the knowledge coefficient (Kc), based on self-assessed knowledge (scaled 0–10 and multiplied by 0.1), and the justification coefficient (Ka), based on theoretical understanding, practical experience, familiarity with scientific literature, and reasoning. Only professionals with K >0.8 were included in the final panel.
For expert patients, a structured six-item self-assessment was used. It evaluated: time since diagnosis, participation in education, treatment adherence, peer support involvement, understanding of medical information, and prior research experience. Each item was rated on a scale of 0 to 5. A minimum score of 21 out of 30 was required for inclusion as an expert participant.
2.6. Statistical analysis
Descriptive statistics were used to summarize the characteristics of the expert panel, including means and standard deviations for continuous variables, and absolute frequencies for categorical variables.
For each item evaluated in the Delphi process, measures of central tendency (mean) and dispersion (standard deviation) were calculated. Additionally, psychometric validation included the computation of the Content Validity Ratio (CVR) and the Content Validity Index (CVI), with CVI ≥ 0.78 considered acceptable.
Inter-rater reliability was evaluated using the Intraclass Correlation Coefficient (ICC), which measures the degree of agreement among raters. ICC values range from 0 to 1, with higher values indicating stronger reliability. Interpretation followed established criteria: values <0.4 were considered poor, 0.4-0.75 moderate, and ≥0.75 indicative of good agreement. Additionally, Kendall’s W coefficient was calculated to assess concordance among expert ratings, with values interpreted as <0.4 poor agreement, 0.4–0.7 moderate agreement, and >0.7 strong agreement. Statistical significance was set at p < 0.05.
All analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA).
2.7. Ethical considerations
The study received approval from the Research Ethics Committee of Hospital Universitario de La Princesa (CEIm Act 14/24). All participants (healthcare professionals and expert patients) were informed about the study objectives, procedures, voluntary nature of participation, and data confidentiality, and provided informed consent electronically prior to participation. Given the non-interventional study design and the absence of patient-level data collection, the Ethics Committee formally waived the requirement for written informed consent. The study complies with current data protection regulations, including the General Data Protection Regulation (GDPR) and Spanish Organic Law 3/2018. All data were anonymized and handled confidentially, ensuring participants’ privacy and security. No personally identifiable information was stored in the application, and only the research team had access to the data managed on secure servers.
3. Results
Sociodemographic characteristics of Delphi panel participants by specialty.
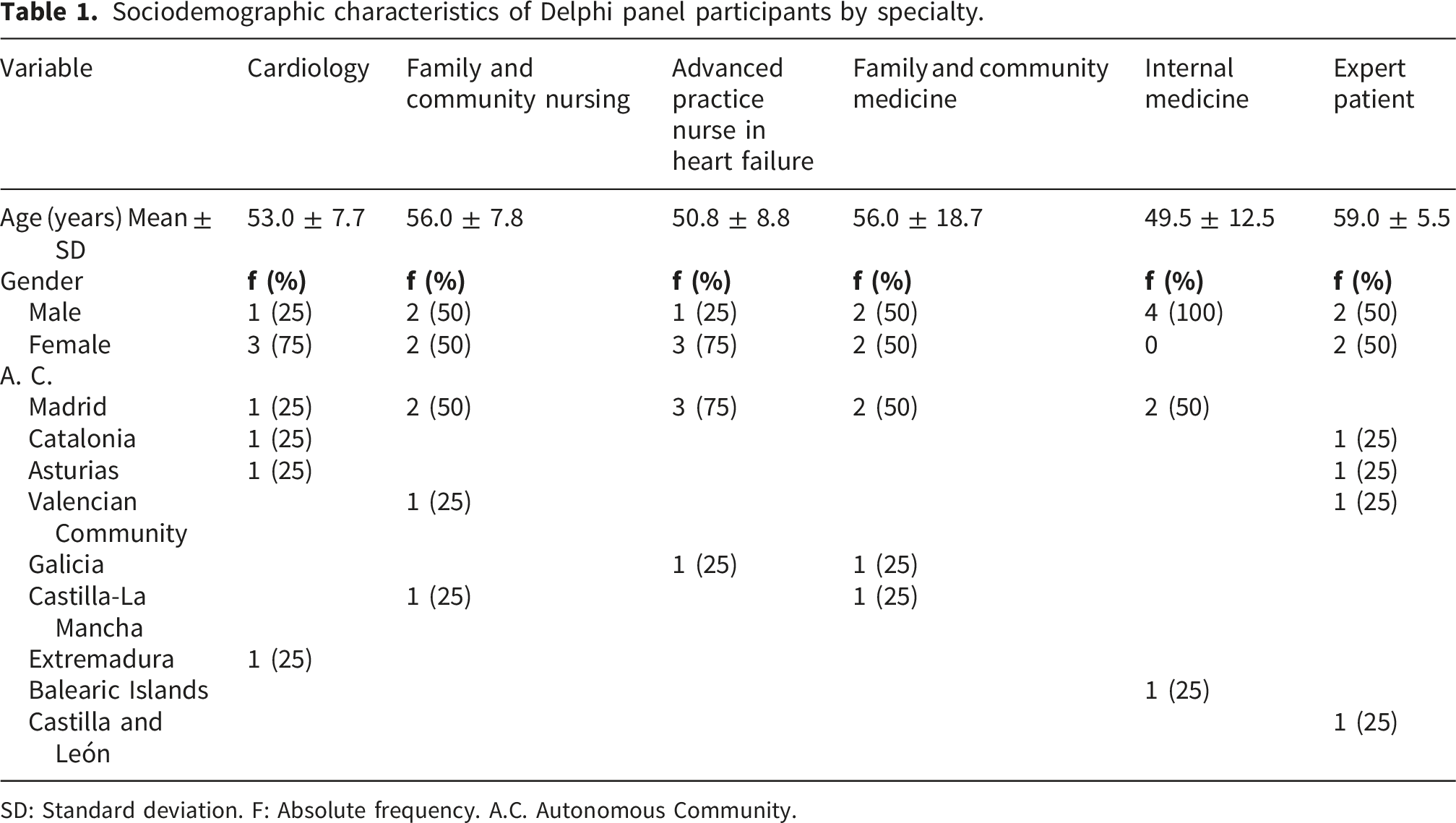
SD: Standard deviation. F: Absolute frequency. A.C. Autonomous Community.
All expert patients had lived with chronic heart failure for over five years, participated in educational programs, adhered to medical treatment, and engaged in peer support groups. All had prior research experience. Competence analysis confirmed high expertise among professionals (K > 0.8), while expert patients reached a mean competence score of 24.25 out of 30.
The Delphi process consisted of two rounds (Figure 1). In the first, 39 items were assessed; 29 were accepted, 5 revised, and 13 new items incorporated. In the second round, 44 items (93.6%) reached consensus, and 3 (6.4%) were excluded. A third round was unnecessary due to high agreement levels. Flowchart of the Delphi process for item selection and validation.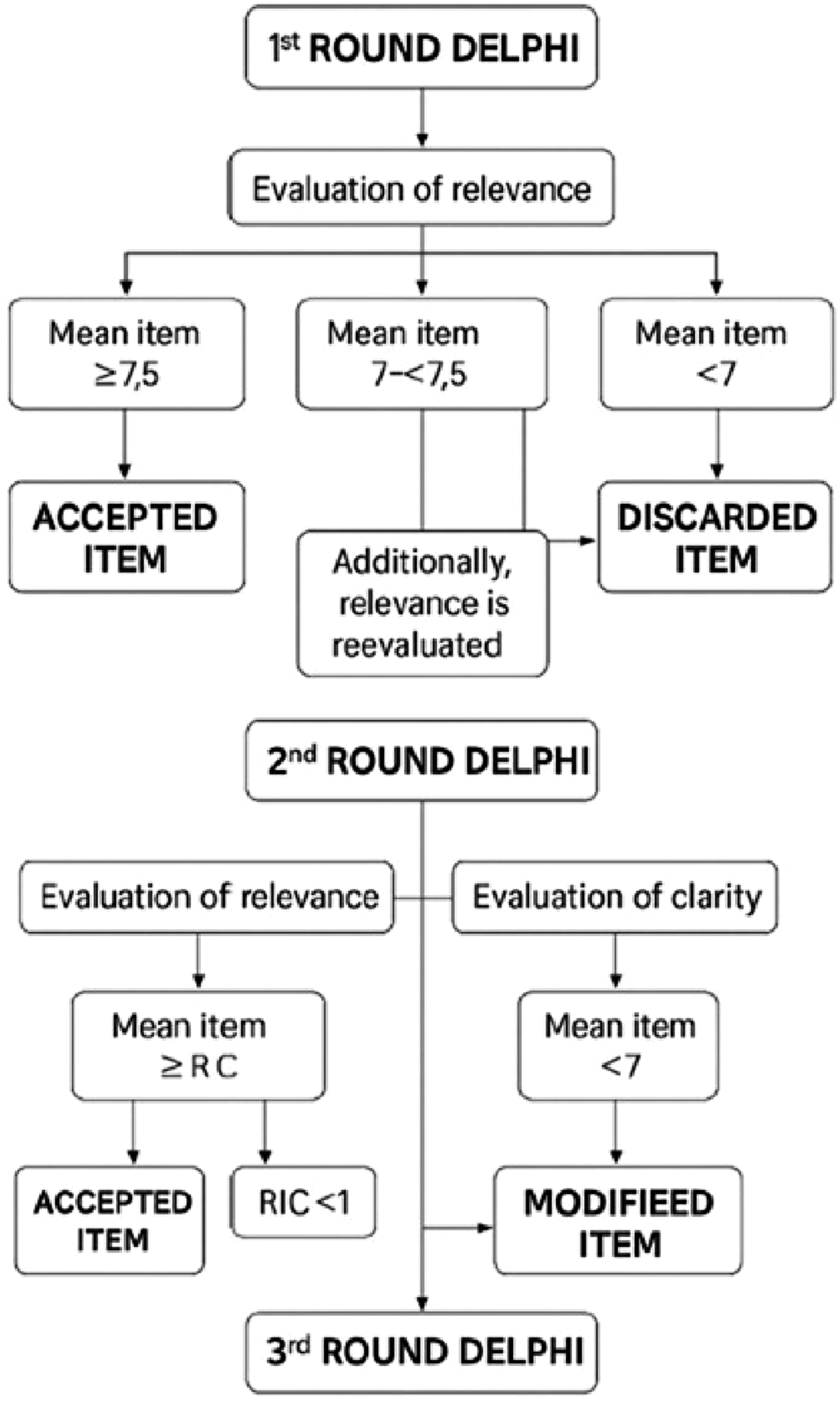
Expert validation metrics of educational content for patients with heart failure.
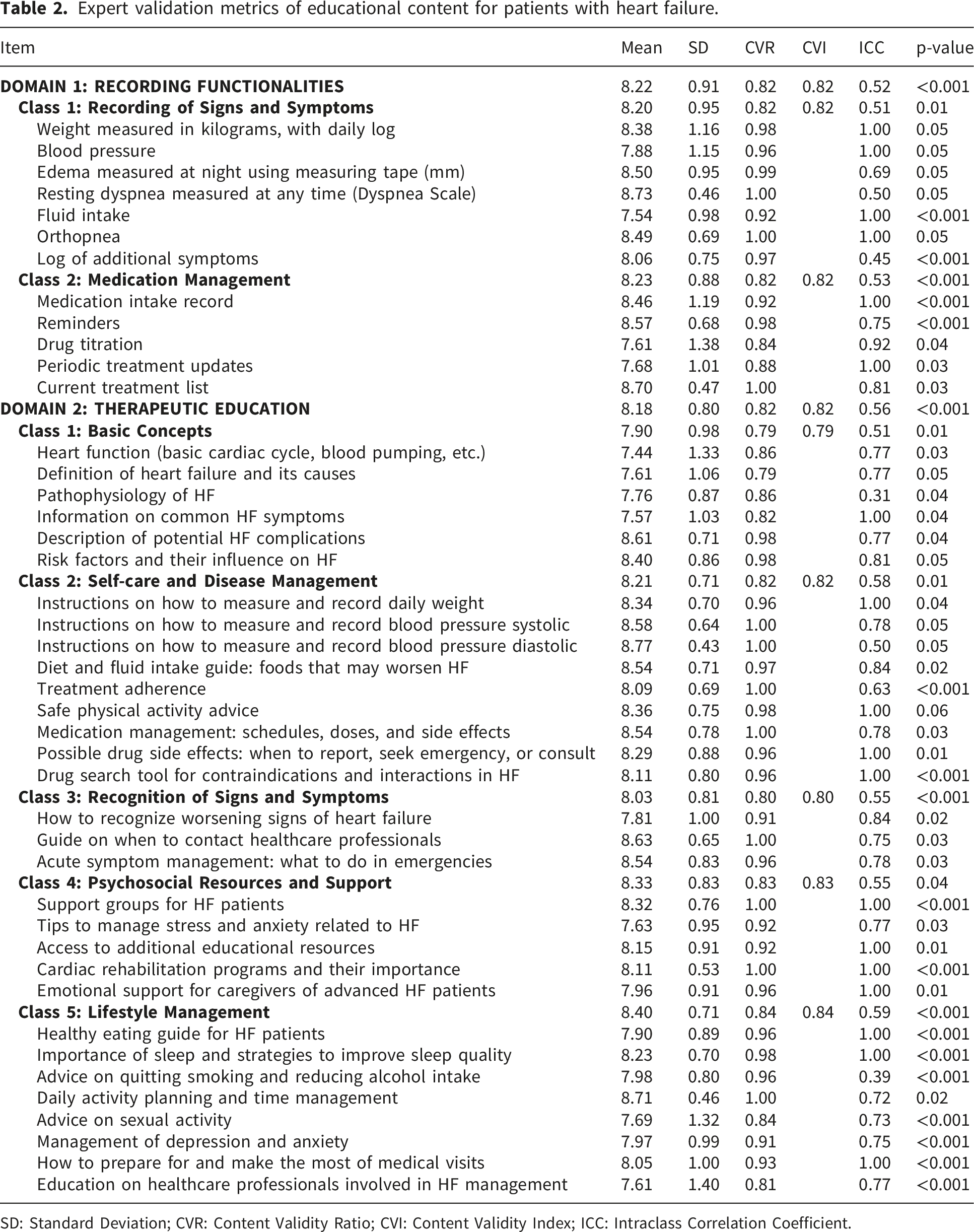
SD: Standard Deviation; CVR: Content Validity Ratio; CVI: Content Validity Index; ICC: Intraclass Correlation Coefficient.
Quantitative ratings were consistent across expert subgroups. Qualitative analysis revealed distinct emphases: physicians prioritized clinical precision, nurses focused on educational clarity, and patients favored practical, user-friendly content.
4. Discussion
The findings of this study emphasize the relevance of incorporating self-monitoring functionalities and therapeutic education into mHealth tools for chronic heart failure (CHF). The strong consensus reached around key parameters such as daily weight tracking, blood pressure and dyspnea monitoring, and medication adherence underscores both their clinical value and their practical applicability in everyday patient self-care. These priorities align with earlier research demonstrating that routine monitoring of these variables can significantly reduce hospital readmissions and improve quality of life.1,4,24 Furthermore, their inclusion directly reflects the recommendations of international guidelines from the European Society of Cardiology and the American Heart Association, which advocate for structured home-based monitoring and patient-centered follow-up.1,24
The standardization of these recording practices is particularly relevant, as it promotes consistency in patient-generated data and fosters a more transparent and trustworthy therapeutic relationship with healthcare providers. This is consistent with previous findings that suggest mobile health technologies can enhance structured self-management and support the continuity of care.9,10 Moreover, the capacity of these platforms to identify early signs of decompensation offers an opportunity for timely interventions and potential reductions in avoidable hospitalizations.10,14
The proposed mobile application follows a modular architecture built on HL7 FHIR interoperability standards, enabling seamless integration with electronic health records (EHRs) and existing hospital information systems. This structure supports continuity of care and aligns with the World Health Organization’s Global Strategy on Digital Health (2020–2025). Furthermore, the client–server model ensures scalability and robust data security through encrypted storage and controlled access. Such architecture facilitates longitudinal monitoring, supports multi-institutional implementation, and provides a framework adaptable to other chronic diseases beyond heart failure.
The expert panel also emphasized the inclusion of functional components such as medication reminders, personalized education modules, and dynamic feedback loops. These features were considered critical for tailoring content to individual patient needs and for ensuring effective communication, both of which are central to treatment adherence and self-efficacy.5,24 Evidence from previous programs such as HOM-HEMP 11 and multiple systematic reviews 5 has consistently shown that digital empowerment strategies not only increase patient engagement but also foster autonomy in disease management. Targeted alerts and self-care support mechanisms have demonstrated reductions of up to 30% in hospital readmissions among CHF populations.11,15,16
In parallel, previous work in health informatics and computational sciences has highlighted the importance of robust computational validation approaches to ensure reliability and clinical relevance in digital health tools, reinforcing the need for methodologically sound foundations when designing mHealth solutions.25,26
These outcomes suggest that a well-designed mobile application, grounded in expert consensus and enriched by patient perspectives, could represent a valuable tool to support integrated care pathways in CHF. Its implementation, however, will require addressing challenges such as digital literacy disparities, long-term adherence to digital tools, and interoperability with electronic health records.
While the quantitative results revealed a shared understanding among experts, the qualitative feedback offered richer nuance. Physicians emphasized clinical accuracy, while nurses focused more on educational aspects. These different perspectives reflect the complexity of patient care and support the idea that educational interventions work better when tailored to each patient’s needs.12,24
Unlike many Delphi-based studies on chronic conditions such as type 2 diabetes or COPD that often focus solely on the healthcare professionals’ perspective, this work intentionally included expert patients in the process. Although this is still relatively uncommon, their contribution is increasingly recognized as vital.27,28 Interestingly, the challenges identified here differ from those described by Tchero et al. (2020), who highlighted technological barriers as a primary cause of app abandonment. Our participants were more focused on how professionals can coordinate effectively and ensure that digital content remains useful over time.
The application’s development follows a user-centered design approach based on ISO 9241-210 standards for human–computer interaction in healthcare. This approach prioritizes usability, accessibility, and personalization. Iterative feedback from clinicians and patients will guide interface refinement, ensuring that the design supports diverse literacy levels, including older adults with limited digital familiarity. Planned accessibility features include voice-assisted navigation, high-contrast visualization, and intuitive icons to reduce cognitive load.
Importantly, the expert panel positively evaluated the inclusion of emotional support, stress management, and caregiver-oriented content. This holistic perspective aligns with recent research advocating for broader psychosocial support in CHF self-management strategies. 28 In this sense, the developed app is not merely a clinical instrument; it is envisioned as a bridge between patients and care teams, helping coordinate care and human communication. This role becomes especially crucial in value-based healthcare models, where patient engagement and education are cornerstones of quality and sustainability.
Beyond regulatory compliance, broader ethical and practical considerations are essential for responsible digital health implementation. Issues such as algorithmic transparency, potential bias in decision-support rules, and equity in access must be addressed, particularly in populations with limited digital literacy or restricted connectivity. From a practical perspective, long-term user engagement, potential digital fatigue, and sustainability within routine clinical workflows represent key challenges. These aspects should be systematically evaluated during future implementation phases to ensure that the proposed framework remains inclusive, transparent, and scalable across diverse healthcare settings.
4.1. Equity and social implications
The implementation of digital health tools must also address social and equity dimensions. Older adults and patients with limited technological literacy remain at risk of digital exclusion. By integrating accessibility standards and patient feedback on heart failure, this project contributes to digital equity and inclusion in chronic disease management. This commitment aligns with the United Nations Sustainable Development Goals (SDG 3 and SDG 10), promoting reduced inequalities and improved access to healthcare innovations across populations.
Age-related differences and heart failure severity are expected to influence digital engagement, with older patients or those with more advanced disease potentially requiring simplified interfaces, additional support, or caregiver involvement to ensure effective use. Barriers related to device availability, affordability, and access to digital infrastructure may further exacerbate digital exclusion in these populations. Ethical aspects related to patient-generated health data, including informed consent, data governance, and transparency in decision-support logic, are central to ensuring trust and accountability in the deployment of such digital health solutions.
4.1.1. Clinical implications and functional development of the mobile application
This study provides a robust foundation for the functional design of a mobile application focused on self-management for patients with chronic heart failure. The results of this consensus study provide a robust foundation for the computational modeling and structured development of a mobile application for chronic heart failure (CHF). The validated items will be integrated into a modular architecture using a client-server model, supporting both offline and online functionalities. The design will adhere to HL7 FHIR standards for interoperability and data exchange, facilitating potential integration with electronic health records (EHR).
Planned functionalities include symptom and medication tracking modules, decision rules based on threshold algorithms, and automated alerts. The application will employ a hybrid development framework (e.g., React Native or Flutter) and a secure backend infrastructure using encrypted databases (e.g., Firebase or PostgreSQL with AES256).
Later, machine learning techniques will be applied to longitudinal patient data to develop predictive models of decompensation episodes. This computational method aims to improve resource allocation and assist in timely clinical decision-making.
The utilization of expert consensus to guide the development of the initial functional architecture guarantees the application’s usability, modularity, and compatibility with clinical workflows. This design approach anticipates future scalability, implementation, and potential integration with hospital information systems. Overall, this methodology fosters a validated, collaborative, and patient-centered digital solution for the management of heart failure.
4.1.2. Study limitations
As with any Delphi-based research, this study has inherent limitations. Although the panel was composed of highly qualified participants (K > 0.8), the findings may not be fully generalizable, partly because participants were geographically concentrated within specific Spanish regions and the proportion of expert patients was smaller than that of healthcare professionals. This phase focused on content validation rather than clinical outcomes, and external validation through usability testing or real-world implementation was beyond its scope. Consequently, future studies with broader and more diverse samples and longitudinal evaluation will be necessary to assess real-world applicability, adherence, and patient autonomy.
5. Conclusion
This study achieved multidisciplinary consensus on the clinical, educational, and technological components required for a patient-centered mobile application in chronic heart failure. The validated content was integrated into an interoperable and secure digital framework that supports scalability, accessibility, and equitable implementation. By merging evidence-based practice with inclusive digital design, this initiative contributes to the global digital transformation of chronic disease management and strengthens the alignment between patient empowerment and sustainable healthcare innovation.
Footnotes
ORCID iDs
Ethical considerations
This study was approved by the Research Ethics Committee of Hospital Universitario de La Princesa (CEIm Act 14/24). The study complied with the ethical principles of the Declaration of Helsinki and current data protection regulations, including the European Union’s General Data Protection Regulation (GDPR) and Spanish Organic Law 3/2018 on the Protection of Personal Data and Guarantee of Digital Rights.
Consent to participate
All participants provided informed consent before participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has been funded through the Fundación para la Investigación e Innovación Biosanitaria de Atención Primaria (FIIBAP).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.