
Abstract
Objectives
Integration of social media (SM) with mobile health (mHealth) platforms presents significant potential to address the persistent challenge of disengagement in digital health interventions among young people. However, empirical evidence supporting this combined approach remains limited, as SM and mHealth are often examined in isolation. This systematic review aimed to identify and synthesise the determinants influencing the participation in SM and mHealth interventions for behaviour change among young people aged 14 to 35 years.
Methods
A systematic search of Scopus, Web of Science, PubMed, and the ACM Digital Library was conducted to identify peer-reviewed empirical studies published between 2019 and 2024. The review followed the PRISMA framework. Eligible studies examined health behaviour interventions that employ mobile or web-based platforms accessible via smartphones or wearables. Thematic synthesis drew on constructs from the Unified Theory of Acceptance and Use of Technology (UTAUT) and the Expectation-Confirmation Model (ECM) to interpret determinants of engagement.
Results
Twenty studies met the inclusion criteria, representing diverse geographical contexts, with 35% from the USA and 15% each from South Africa and Australia, while other regions contributed 10% and 5% each. Sexual and reproductive health (55%) was the most common intervention focus above other health domains. Determinants of sustained engagement were identified at three levels: (i) user-level (ii) intervention-level and (iii) contextual-level factors. Engagement was highest when interventions aligned with behavioural readiness, provided peer-reinforced support, and offered user-centred adaptive design. Conversely, digital inequities, privacy concerns, and commercial algorithmic bias constrained participation in low-resource settings.
Conclusion
Sustained engagement depends on user motivation, health awareness, cultural and gender sensitivity, and equitable digital access. While integration improves behavioural adherence through social reinforcement and personalisation, risks linked to data privacy, misinformation, and commercial exploitation necessitate robust ethical governance. Context-responsive, rights-based, and gender-inclusive digital health strategies are essential to ensure equitable participation and sustained behavioural outcomes among young people.
1. Introduction
The rapid tide of advancements in digital technology has introduced a new era in healthcare delivery, profoundly transforming the way health services are provided.1,2 In this digital age, social media (SM) for health and mobile health technologies (mHealth) have emerged as effective tools for health promotion, awareness, and education, each demonstrating the ability to engage the public and promote changes in health behaviour.3,4 Digital health developments are designed primarily for use by health professionals, such as patient diagnostic and monitoring tools, electronic medical records, clinical decision support systems, among others. 5 However, mHealth and SM stand out as innovative platforms that engage and influence health behaviour in ways that are both accessible and appealing to young people, with opportunities to leverage emerging computing sciences such as big data, the Internet of Medical Things (IoMT), and artificial intelligence (AI).6,7
Despite the proliferation of digital health, maintaining user engagement remains a critical challenge. 8 Sustainable engagement—defined as consistent and meaningful interaction with health platforms over time—is essential for achieving significant behavioural health outcomes. 3 In the context of mHealth, engagement reflects not only the frequency of use but also subjective dimensions such as user experience, motivation, satisfaction, emotional involvement, and perceived social influence. 9 These experiential and social components align with theoretical constructs articulated in the Unified Theory of Acceptance and Use of Technology (UTAUT) and the Expectation-Confirmation Model (ECM).10,11 High user churn, typically manifesting as premature dropout or disengagement, significantly limits the long-term effectiveness of mHealth. 3 Standalone mHealth platforms report attrition rates of up to 49% in naturalistic settings, compared to 40% in controlled environments within the first few weeks. 3 Although clinical trials show retention rates above 70%, these results reflect short-term engagement under ideal conditions and do not translate into sustained use in real-world contexts. 12 Similarly, Sellak and Grobler 2 report dropout rates as high as 80%, with disengagement remaining the norm rather than an exception despite rising public awareness of health benefits. A review of digital health interventions found that fewer than 10% of users logged in daily after the first two weeks and engaged minimally, logging in fewer than twice before abandoning the platform. 3
Similarly, while young people are prolific and consistent users of social media, digital health strategies often do not take advantage of the persuasive and socially embedded nature of these platforms to support sustained behaviour change. However, despite the demonstrated value, the South African National Digital Health Strategy (2019–2024) omitted social media from its framework, unlike the earlier 2015-2023 National eHealth Strategy, which acknowledged its role.4,13 Young people routinely devote substantial amounts of time to social media and are particularly susceptible to social influence, peer norms, and trends. 4 These characteristics present a valuable opportunity to provide health content in ways that are interactive, peer-reinforced, and contextually relevant. 14 However, current interventions often rely on conventional approaches that lack resonance with a youth-centric digital culture. This shortfall is attributed to the absence of health strategies that are specifically tailored to the preferences and communication styles of young people. 15 The objective of this review is to systematically examine recent empirical evidence on the determinants of engagement in mHealth and SM interventions for behaviour change among young people, and to identify the key cognitive, behavioural, technological, and contextual factors influencing sustained participation. 16
1.1. The emergence of mHealth in digital ecosystems
Digital health, a broad term rooted in the concept of electronic health (eHealth), refers to the application of information and communication technologies (ICT) to improve the delivery of accessible, efficient, and high-quality healthcare services. 5 The World Health Organization defines digital health as a tool to address systemic healthcare challenges, including inaccessibility, fragmented health information, and poor continuity of care, with the potential to advance universal health coverage (UHC) and contribute to the achievement of the Sustainable Development Goals (SDGs). 17 In South Africa, although the government has set ambitious healthcare targets, the healthcare system continues to fall short of patient expectations. 18 The research found that while digital health tools, such as smart card technologies, showed some promise in Gauteng hospitals, including Steve Biko Academic Hospital, implementation was suspended by the South African Department of Health due to barriers to implementation.19,20
Mobile health (mHealth), a subset of digital health, encompasses the use of mobile devices and applications, wearable technologies, and wireless communication systems to support public health functions. 5 This evolution marks a paradigm shift in preventive health, and behavioural intervention. 1 Whereas earlier mHealth models were limited to basic short message service (SMS) reminders, contemporary platforms now integrate real-time health monitoring, personalised feedback, and interactive features enabled by smart devices and AI-powered chatbots.8,21 On the other hand, social media, defined as web-based platforms that facilitate interactive communication and exchange of user-generated content, offers a complementary pathway to enhance mHealth interventions by promoting peer-to-peer interaction, social reinforcement, and dynamic health messaging. 17 Popular platforms such as Facebook, TikTok, and WhatsApp are widely used among young people, providing a culturally relevant and engaging means of distributing health information. Young people who spend significant time on social media are highly responsive to peer norms and trends, representing a key demographic whose behavioural determinants can be positively influenced through socially driven interventions. Integrating the social influence and community-building capabilities of social media with the personalised data-driven features of mHealth creates a synergistic approach that addresses both individual and collective determinants of engagement. 4
1.2. Health challenges and behavioural risks in the youth population
According to the South African National Youth Policy 2020–2030, young people aged 14 to 35 years experience a developmental period marked by cognitive and psychological changes, increasing susceptibility to high-risk behaviours. 22 Therefore, young people face a complex set of health challenges, including communicable and non-communicable diseases. Michie et al. contend that global health problems are fundamentally behavioural in nature and therefore require interventions that address the underlying determinants of human behaviour. 23 Risk behaviours prevalent among young people, such as unprotected sexual activity, substance use, physical inactivity, and unhealthy dietary patterns, contribute significantly to rising rates of HIV/AIDS, obesity, and chronic diseases, which together account for nearly 70% of global mortality annually.23,24 Inconsistent condom use and poor adherence to HIV prevention methods elevate vulnerability to sexually transmitted infections.25,26 Concurrently, high intake of processed, calorie-dense foods 27 and sedentary lifestyles exacerbate the risk of type 2 diabetes and cardiovascular conditions. 28 Substance use, including tobacco and alcohol consumption, further compounds these risks by contributing to long-term morbidity. 23 Health-seeking behaviours, such as early diagnosis and sustained adherence to treatment, are essential for disease control and improved outcomes. However, stigma, low health literacy, and delayed access to care remain barriers to timely intervention. For instance, a national South African survey reported that 38% of new HIV infections among young people occurred in individuals unaware of their positive status. 24 Addressing these interrelated health behaviours requires comprehensive technology-supported strategies that promote behavioural change across multiple domains. 12 By consolidating information delivery, behavioural tracking, and social reinforcement, this approach reduces the burden of self-management and improves both adherence and participation, particularly among hard-to-reach youth populations. 2
2. Methods
This systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework, 29 ensuring a structured, transparent, rigorous, and replicable research process. Although theoretical models were not used to determine inclusion or exclusion criteria, post hoc behavioural constructs were employed to support the interpretation of the findings. The analysis is grounded in behavioural theory, particularly Social Cognitive Theory, which asserts that human behaviour is shaped by outcome expectations and that perceived value influences both attitude and intention toward the adoption of innovation.9,16 Building on this foundation, themes emerging from the reviewed literature were synthesised and interpreted using constructs drawn from the UTAUT and ECM models.10,11 These theoretical lenses provide explanatory value to understand how expectations, facilitating conditions, perceived usefulness, satisfaction, and social influences shape user engagement and continued participation in SM and mHealth interventions.
2.1. Search strategy
A systematic search was conducted on 3 November 2024 across multiple electronic academic databases selected for their relevance to the digital health, technology, and behavioural sciences. These included subject-specific databases such as Digital Health, PubMed, Web of Science, and the ACM Digital Library, as well as multidisciplinary sources such as Scopus and EBSCOhost, ensuring broad coverage of literature on mHealth, social media, and behaviour change. The search strategy employed Boolean operators and keyword combinations to increase precision and relevance, targeting studies conducted in diverse geographical contexts, including developed, developing, and sub-Saharan African settings, with a specific emphasis on South Africa.
The search terms were structured to capture core concepts related to digital health engagement and behavioural interventions among young people. The key terms included combinations of “social media” OR “social networks” OR “mHealth” OR “mobile health” OR “digital health” AND “health behaviour” AND “youth” OR “young adults” OR “adolescents.” To broaden the scope, additional terms such as “health promotion” and “health education” were integrated. Queries were adapted for each database to optimise sensitivity and specificity. Limiters were applied to restrict the results to peer-reviewed studies published in English, ensuring the relevance and quality of inclusion.
2.2. Inclusion criteria
The review covered publications from 2019 to 2024 to capture recent advances in SM and mHealth aligned with the evolving landscape of digital health. Publications were restricted to English to ensure accessibility, consistency in interpretation, and comparability of findings. Eligible studies included empirical, peer-reviewed interventions that employ mobile applications or web-based platforms accessible through smartphones, tablets, or wearable technologies. Selected sources of grey literature and global reports (e.g., World Health Organization and the South African National Digital Health Strategy) were reviewed to inform the background discussion and strengthen the contextual and intersectional framing of digital health engagement. Empirical studies were required to focus on health behaviours among individuals aged 14 to 35 years, consistent with the South African National Youth Policy. Both high-income and low- and middle-income countries were included to generate a global perspective, with emphasis on South African studies to examine regional relevance and sociocultural appropriateness.
2.3. Exclusion criteria
Studies published in languages other than English were excluded. Research published before 2019 was also excluded to focus the review on contemporary interventions that reflect current trends in technology and digital health. Studies focussing on populations outside the 14 to 35 age range were excluded, as behavioural patterns in other age groups can differ, thus requiring a specific age lens. Non-empirical articles—including commentaries, editorials, and opinion pieces, unless they present original data, such as post-intervention feedback—were excluded due to the absence of primary data essential for evidence-based synthesis. Finally, SMS-only interventions were excluded on the grounds that they lack key features of interest, such as interactivity, multimedia content, and social engagement mechanisms.
2.4. Study selection process
Selection process stages.
2.5. Data extraction
Data extraction was systematically conducted using a structured template to ensure consistency. All extracted data was compiled into a central spreadsheet to facilitate thematic analysis. Sources were appropriately cited to ensure proper acknowledgement of original authorship. To minimise bias, the selection, extraction, and analysis processes were rigorously documented. The following key information was extracted. • Study details (author, year, geographical context) • Demographic data of the participants (age, sex, region) • Intervention characteristics (platform type, content, duration) • Outcome measures (behaviour change, health indicators, user engagement) • Barriers and facilitators to engagement (technological access, usability, social support) • Key findings (health and behavioural outcomes) • Study limitations
3. Results
3.1. Overview of selected and included studies
The initial search retrieved 521 records, with filters applied for the English language, a publication year between 2019 and 2024, and peer-reviewed research articles. Records were managed using Mendeley, a cloud-based reference management software used to organise citations, import and export research documents in PDF, BibTeX, and RIS formats, and deduplicate entries.
30
Mendeley also facilitated the management of in-text citations and the automatic generation of the reference list according to the Vancouver citation style. After the removal of duplicates, 261 (50.1%) records remained for title and abstract screening. Following the eligibility assessment, 76 full-text articles (29.2%) were reviewed in detail. Of these, 20 studies (26.4%) met the inclusion criteria and were retained for final data synthesis. The study selection process, including the number of records excluded at each stage and reasons for exclusion, is summarised in Figure 1. PRISMA flow diagram.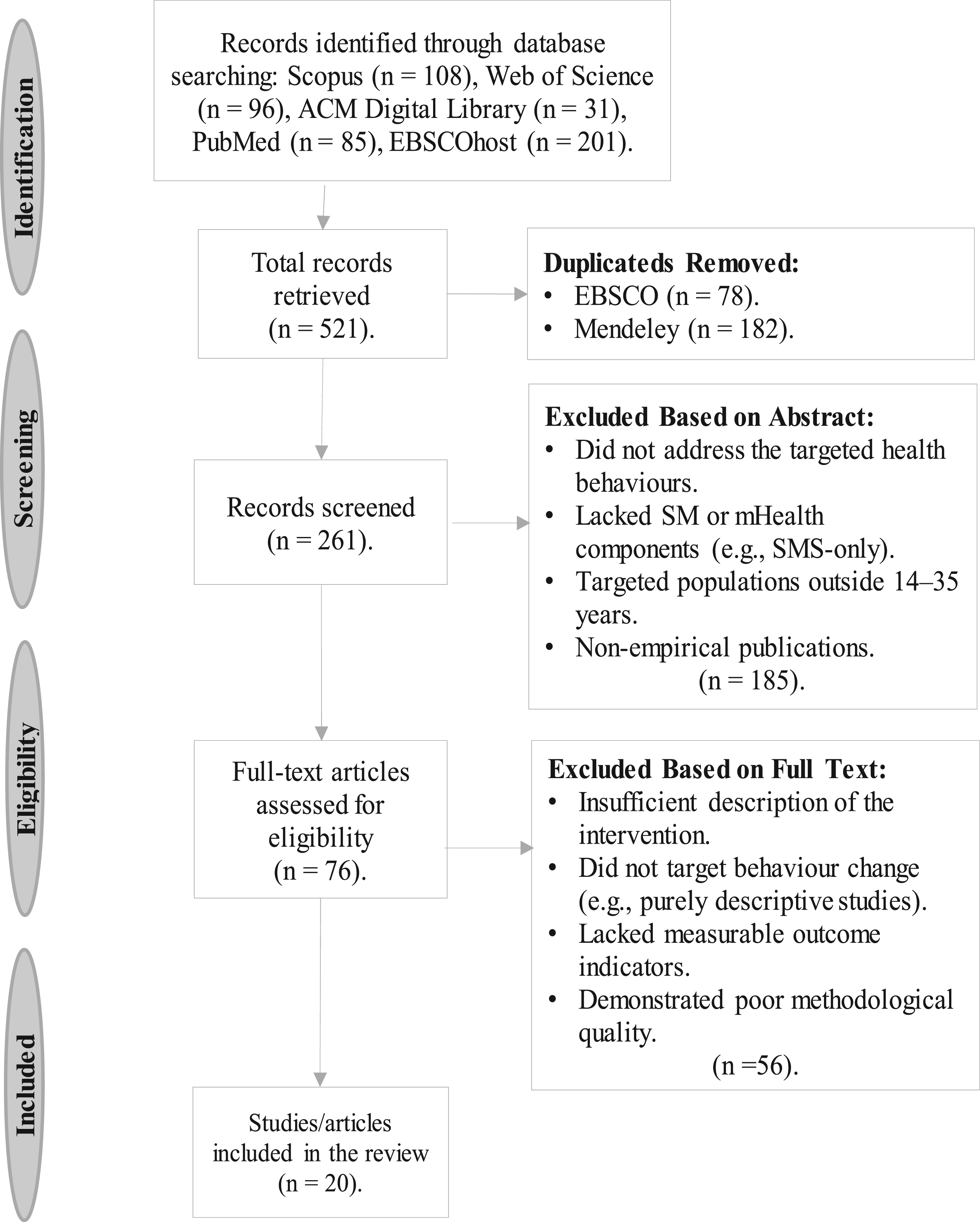
3.2. Characteristics of the included studies
A total of 20 studies met the inclusion criteria and were synthesised in this review. Pilot randomised controlled trials (pilot RCTs) were the most commonly employed study design, accounting for 35% of the included studies. These were followed by full-scale randomised controlled trials (RCTs) and mixed-method evaluations, each comprising 20%. Pilot RCTs typically assess feasibility, implementation, and acceptability, whereas full RCTs provide more rigorous evidence on intervention efficacy through random assignment. Other study designs, including qualitative and quasi-experimental approaches, appeared less frequently, each representing 5% of the total.
Geographically, the United States of America (USA) accounted for the largest proportion of studies (35%), followed by South Africa (SA) and Australia (15% each). The United Kingdom (UK) contributed 10%, while Nigeria, Zambia, India, Japan, and New Zealand each represented 5% of the included literature. Figure 2 presents the distribution of studies by geographic region, highlighting the concentration of research in high-income settings but also including valuable representation from sub-Saharan Africa. Table 2 outlines key characteristics of the included studies. Regional distribution of publications. Characteristics of the included studies on digital and social media interventions.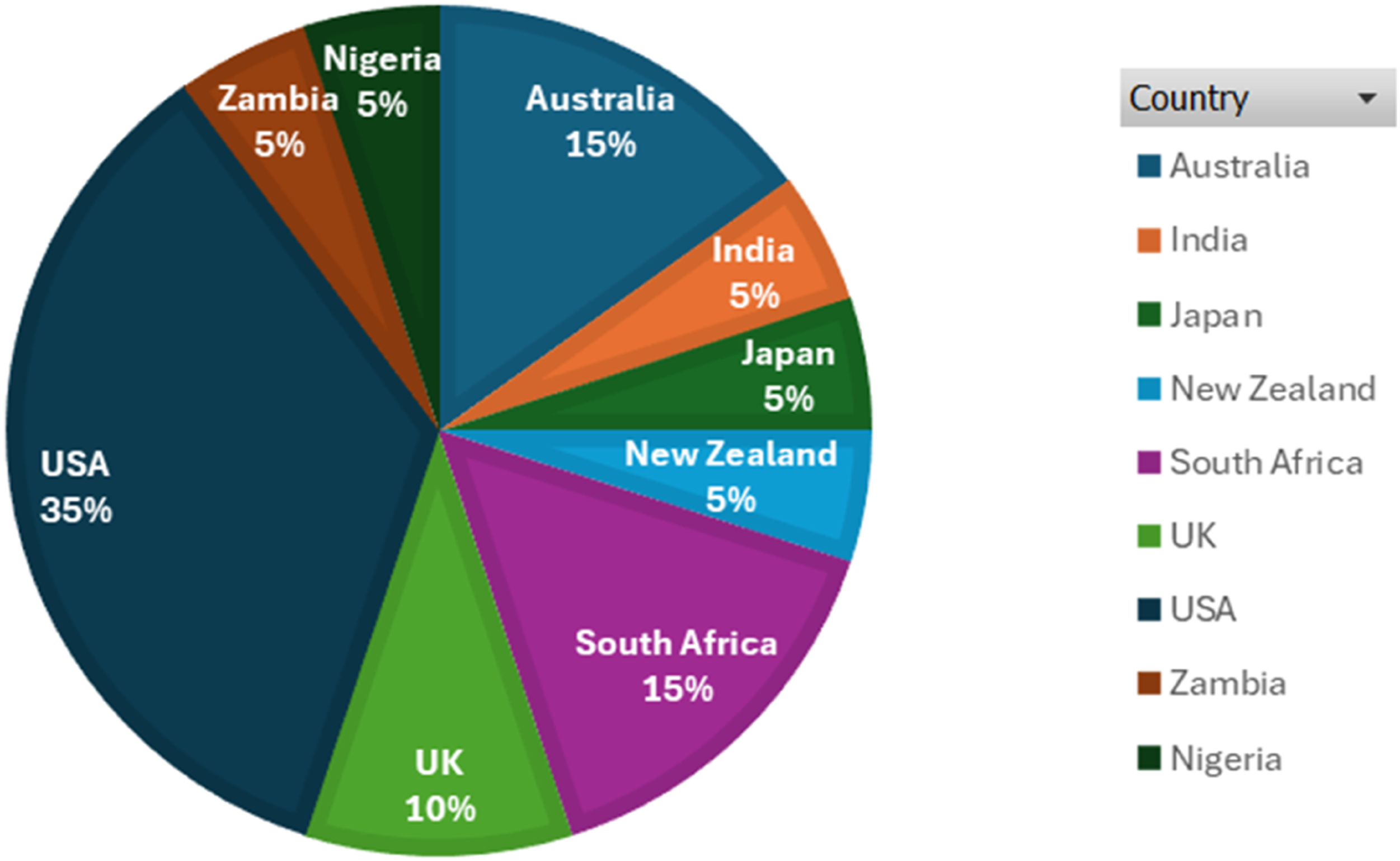

Eighteen of the 20 (90%) included studies were published within the five-year period (2020–2024). Specifically, 2 studies (10%) were published in 2024, 3 (15%) in 2023, 4 (20%) in 2022, 3 (15%) in 2021, and 6 (30%) in 2020. Only two studies (10%) were published in 2019, thereby falling outside the five-year window but retained due to their methodological and thematic relevance. The year 2020 yielded the highest number of publications (n = 6; 30%). Of these, three (50%) originated from the United States, while one study (16.7%) each was conducted in Australia, Japan, and Nigeria. This temporal distribution of publications is illustrated in Figure 3, reflecting both the emerging interest in digital health interventions and geographical research patterns during the post-Covid acceleration of SM and mHealth technologies. Frequency of publications by year.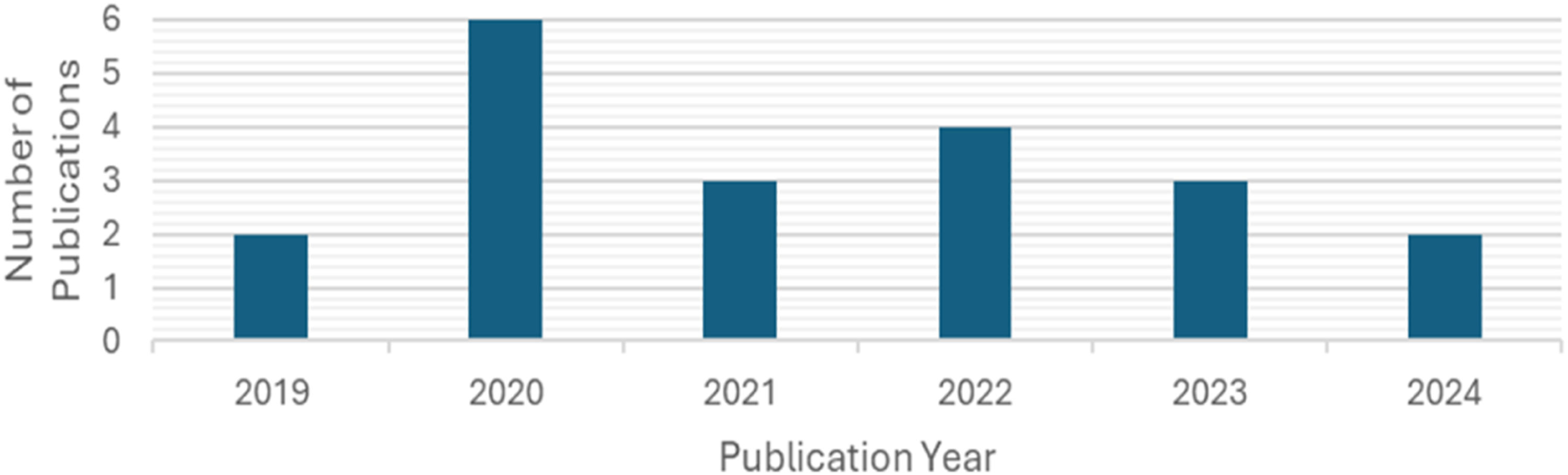
3.3. Characteristics of mHealth interventions
Figure 4 illustrates the distribution of digital platforms employed in the included studies. Facebook was the platform used most frequently, appearing in 35% of the studies, underscoring its prominence in digital health communication strategies. This was followed by stand-alone mHealth-specific applications, which featured in 30% of the reviewed interventions and were primarily designed for behaviour change support, symptom tracking, and health education. Integrated SM and mHealth platforms, which combine traditional mHealth functions with social media features (such as AI-powered chatbots or cross-platform integration with Facebook), accounted for 20% of the studies. These hybrid systems reflect a growing trend towards personalised, interactive, and socially embedded digital health interventions. WhatsApp was the least frequently used platform, identified in 15% of the interventions. Its lower representation may reflect either its more limited programmability compared to other platforms or underutilisation of its potential for targeted health promotion. This distribution highlights an ongoing preference for mainstream SM platforms and stand-alone mHealth technologies while also signalling an emerging shift toward more integrated, intelligent digital health solutions that aim to enhance user engagement and facilitate sustained behavioural outcomes. Distribution of the intervention platforms used in the included studies.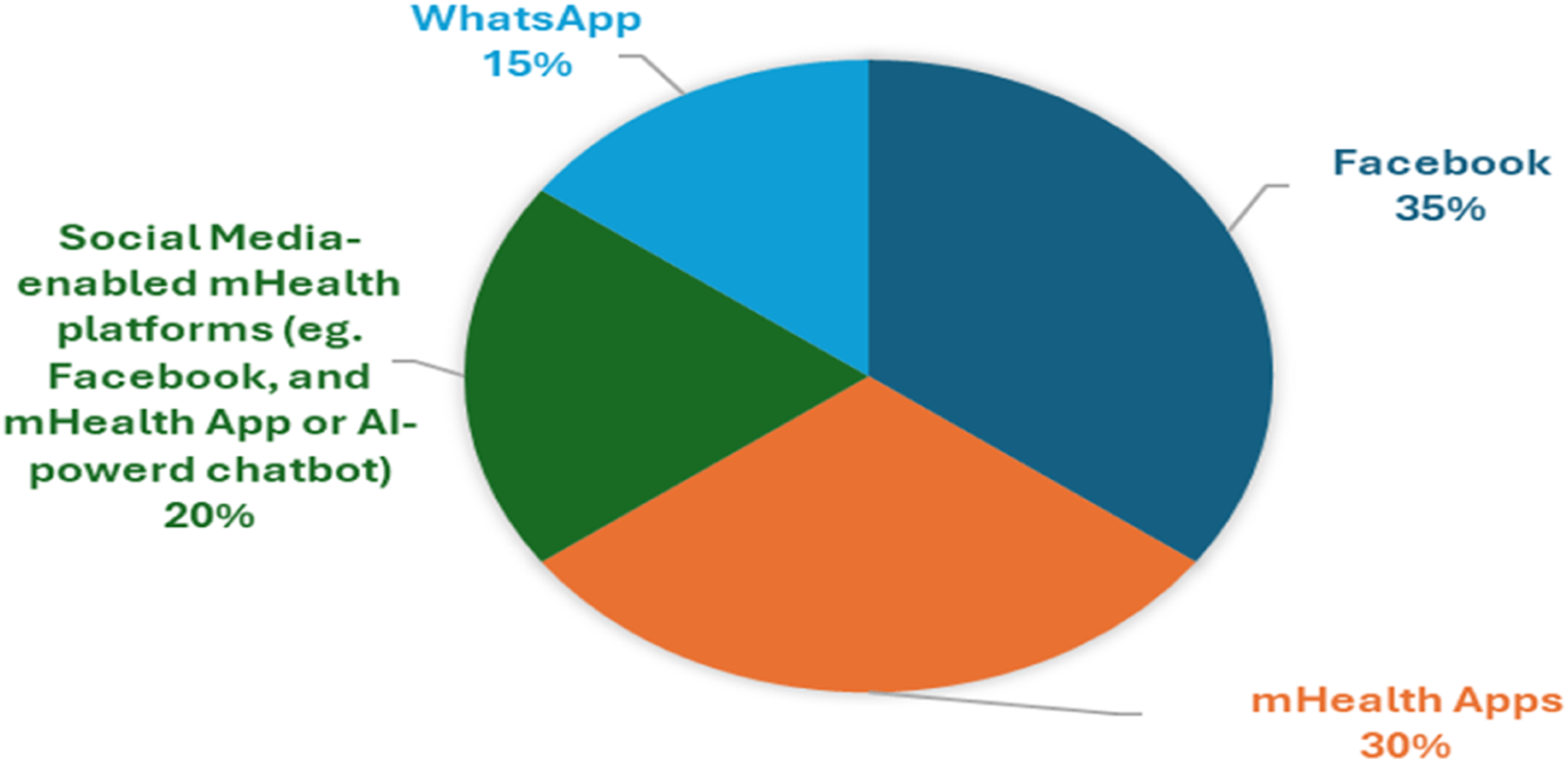
3.4. Characteristics of the targeted health behaviour
As illustrated in Figure 5, the included studies were classified into four primary health behaviour domains, based on the main focus of each intervention: sexual and reproductive health (SRH) (n=11; 55%), nutrition-related behaviours (n=4; 20%), substance abuse (n=3; 15%), and physical activity promotion (n=2; 10%). All interventions conducted in South Africa (n = 3; 15%) were exclusively focused on SRH, reflecting national public health priorities, particularly in relation to HIV prevention and sexual health education. In contrast, studies conducted in high-income countries, such as the US and the UK, demonstrated broader thematic diversity, targeting a wider range of health behaviours. It should be noted that none of the included studies explicitly addressed alcohol cessation, representing a critical gap in the current literature, particularly given the high prevalence of alcohol-related harm among young people in both high- and low-income settings. Proportional distribution of studies by health domain.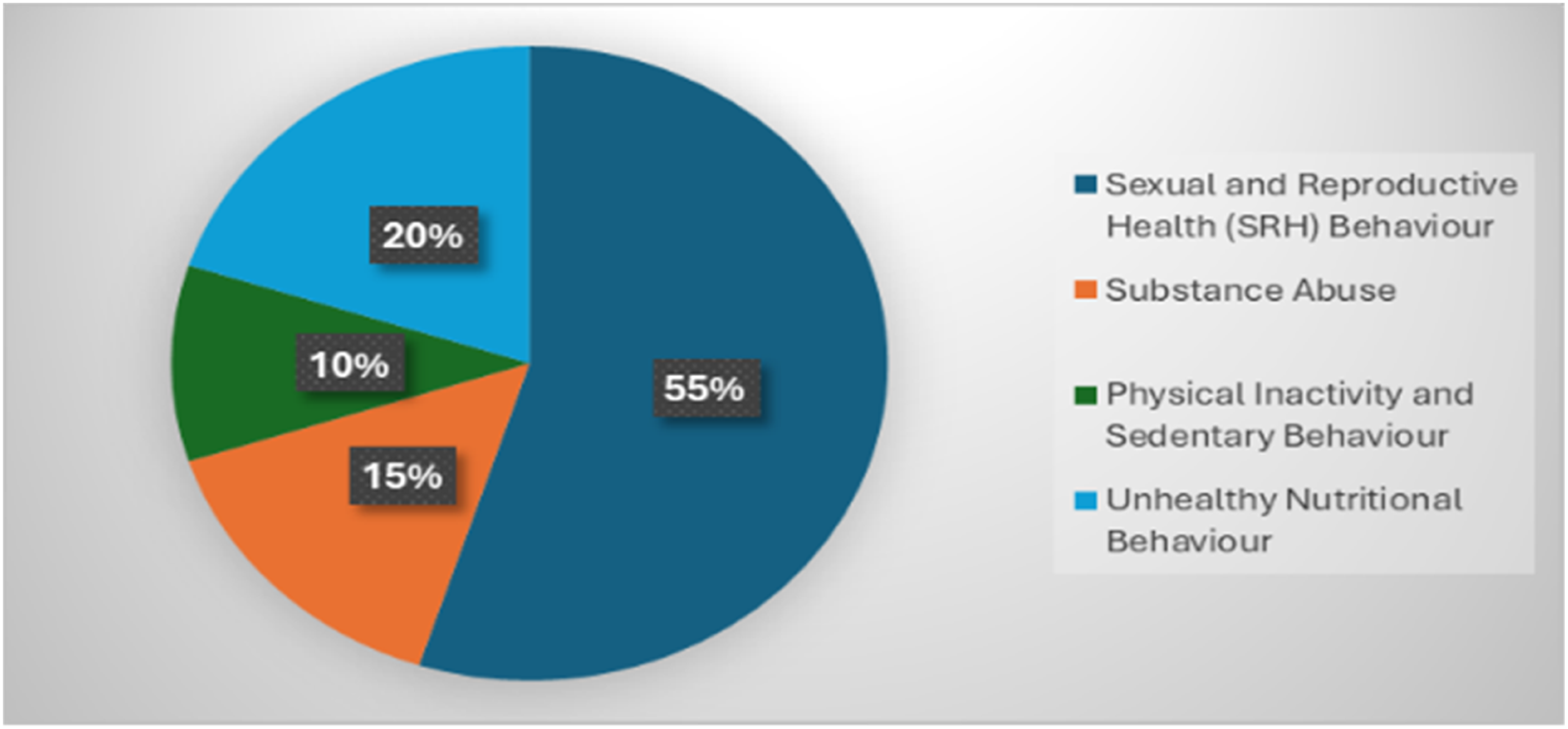
4. Discussions
This section critically interprets the findings of the review by examining the determinants that influence engagement and participation in mHealth interventions. These determinants are analysed on three levels—user, intervention, and contextual—framed within the main thematic domains: (i) barriers and facilitators of participation, (ii) strategies and mechanisms that influence sustainable engagement and behaviour change, and (iii) measurable effects on health and behavioural outcomes. Although the included studies did not explicitly apply constructs from the UTAUT or ECM models, they reported empirical findings conceptually aligned with these models. 16 Constructs from UTAUT, 10 such as performance expectancy, effort expectancy, social influence, and facilitating conditions help elucidate initial adoption and engagement with digital interventions. In parallel, ECM 11 constructs, such as perceived usefulness, confirmation, and satisfaction, explain the intentions of users to continue engaging with platforms after initial exposure. These theoretical lenses are particularly useful for interpreting why certain digital interventions sustain user participation while others experience high attrition rates. 16
4.1. Defining engagement in mHealth
Engagement has emerged as a central construct in digital health research, yet its definition remains contested. 47 In the context of mHealth, engagement refers to the extent and manner in which individuals interact with a health intervention over time. 48 It arises from the dynamic interaction between micro-level user mechanisms and macro-level contextual conditions. At the micro-level, engagement is driven by cognitive, affective, and behavioural determinants that explain how users think, feel, and act when interacting with digital systems. 49 Cognitive determinants include perceptions of usefulness, confirmation, and performance expectancy, while affective determinants capture satisfaction, trust, and enjoyment. Behavioural determinants reflect observable actions such as frequency and duration of use, which translate cognition and emotion into sustained participation.47,50 At the macro-level, engagement is shaped by contextual determinants—technological, cultural, and institutional—that influence access, affordability, and social inclusion. 51
Therefore, this study defines engagement as the dynamic interaction between users and digital health systems, driven by cognitive, affective, and behavioural determinants at the micro level, and conditioned by technological, sociocultural, and institutional factors at the macro level. This definition acknowledges that, while adoption is necessary, sustained behavioural interaction ultimately determines whether mHealth interventions realise their intended health impact. Building on this conceptualisation, the subsequent sections synthesise the key findings derived from the reviewed studies, organised across three analytical levels—user, intervention, and contextual—to illustrate how individual, technological, and environmental determinants collectively influence engagement in mHealth interventions.
4.2. User-level determinants of engagement
User-level determinants encompass individual and psychosocial characteristics influencing adoption and sustained participation in mHealth. Factors such as digital literacy, motivation, perceived privacy, and awareness of personal health status consistently shaped user engagement. 4 Limited digital literacy and perceived unaffordability were notable constraints, especially in low-resource contexts.46,52 For instance, in the South African InTSHA intervention, which employed WhatsApp for SRH education among youth with perinatally acquired HIV, engagement was strengthened by peer support, confidentiality, and digital literacy. 33 However, low smartphone access and high data costs constrained sustained use. Similarly, Zanoni et al. demonstrated that WhatsApp-based mHealth support for adolescents living with HIV in South Africa improved care retention and viral suppression, but participation was limited by privacy concerns and scheduling conflicts. 46 These findings illustrate how motivational and contextual factors intersect, with confidentiality and trust driving engagement, while digital inequities constrain it.
Comparatively, in Nigeria, the SMART Connections study using Facebook secret groups for young people with HIV also found that peer support and confidentiality facilitated active participation, whereas stigma and gender disparities hindered consistent involvement. 35 These African studies collectively show that in contexts marked by social stigma and infrastructural barriers, trust, and social connection are decisive motivators for engagement. In contrast, in high-income contexts such as the USA and Australia, motivation and self-efficacy, rather than access constraints, were stronger predictors of continued use. For example, Pope et al. 28 reported that American college students using the MapMyFitness app and Facebook maintained engagement through feedback, gamification, and social reinforcement, while attrition was linked mainly to competing content priorities rather than resource constraints. Likewise, Ashton et al. found that over 42,000 Australian users of a healthy-eating website integrated with social media platforms (Facebook, Instagram, Twitter) sustained participation due to usability, goal setting, and self-monitoring features that enhanced perceived control and enjoyment. 32 These cross-context findings indicate that user-level engagement drivers differ by socioeconomic setting: in high-income countries, engagement is reinforced by self-determination and perceived usefulness, whereas in low- and middle-income settings, it is heavily mediated by affordability, social stigma, and access to digital infrastructure. Similarly, in physical activity and smoking cessation interventions, intrinsic motivation and readiness to change were key. For example, Thrul et al. 43 in the USA demonstrated that Facebook-based smoking cessation groups achieved higher quit success when participants reported strong motivational intent and perceived social support. In contrast, attrition occurred mainly among those in the early stages of readiness. This pattern mirrors the findings of Peiris et al. in Australia, where a smoking cessation app designed for Aboriginal users achieved increased quit attempts through social reinforcement and cultural adaptation, despite the persistence of social norms that normalised smoking. 39 Collectively, these findings underscore that sustained engagement requires not only accessible platforms, but also behavioural, cognitive, and affective reinforcement that strengthens users’ belief in efficacy and satisfaction. Consistent with UTAUT 10 and ECM, 11 engagement emerges when users perceive interventions as useful, relevant, and emotionally rewarding. 53
4.3. Intervention-level determinants of engagement
At the intervention level, usability, interactivity, personalisation, and adaptive feedback mechanisms were critical to sustaining engagement. Evidence across health domains showed that user-centred design enhances participation and mitigates attrition. For example, in the Indian SnehAI chatbot study, a Facebook-integrated artificial intelligence platform SRH education, engagement was driven by personalised, interactive dialogue and trust-based feedback that created a safe space for young people to discuss sensitive topics. 44 Similarly, in the United States, the Crush SRH mHealth app employed gamification and adaptive learning modules to sustain adolescents’ motivation and enhance contraceptive awareness and health-seeking behaviours, although novelty decay and limited offline usability presented minor challenges. 14 These examples demonstrate how personalised and gamified interventions translate abstract health messages into engaging, relatable experiences that strengthen both perceived usefulness and satisfaction.
In nutrition and physical-activity interventions, adaptive goal-setting, interactive dashboards, and gamified challenges increased motivation by translating abstract goals into tangible achievements. For instance, Worthington et al. 27 in New Zealand reported that combining Facebook with the Easy Diet Diary mHealth app enhanced dietary adherence and healthy food choices through personalisation and adaptive feedback, while the “No Money No Time” healthy-eating website 32 demonstrated how social marketing principles and self-monitoring tools attracted over 42,000 young Australian users by promoting usability and aesthetic appeal. Similarly, the MapMyFitness App integrated with Facebook improved goal adherence and activity levels among college students by using gamification and real-time feedback to reinforce behavioural consistency. 28
Smoking cessation studies also highlighted the importance of tailored content and stage-matched communication. Thrul et al. 43 found that Facebook interventions that incorporate live and automated counselling improved the success of quit, particularly among users whose readiness to quit was high, confirming the need to align digital content with the behavioural stage. Similarly, Peiris et al. 39 showed that the culturally adapted “Can’t Even Quit” app for Aboriginal Australians enhanced motivation through social reinforcement and trust-based interaction, although long-term adherence remained challenged by community-level social norms that normalised smoking from young ages. These mechanisms align with the UTAUT constructs of effort expectancy and social influence, 10 as well as the ECM constructs 11 of satisfaction and confirmation. For example, interventions such as Hanass-Hancock et al. in South Africa—combining WhatsApp workshops and live sessions—illustrated that when trust, cultural resonance, and peer interaction were integrated into the design, young adults showed improved HIV literacy and empowerment. 27 However, the same study reported that gender taboos and data costs undermined participation, underscoring the need for contextual adaptability.
In general, interventions that included personalisation, feedback, and interactivity within culturally and linguistically appropriate frameworks achieved higher levels of sustained participation, particularly among youth populations accustomed to social-media dynamics. This pattern was evident across contexts: from SnehAI in India, 44 where conversational AI increased SRH engagement, to Crush in the USA, 14 where gamification fostered contraceptive confidence, to Worthington’s dietary app in New Zealand, 27 which improved healthy-eating behaviours. These comparative examples affirm that while the technological sophistication of interventions enhances usability, cultural and social relevance ultimately determines their effectiveness in sustaining engagement.
4.4. Contextual-level determinants of engagement
Contextual determinants, which comprise of sociocultural, economic, gender, commercial, and political conditions—play a decisive role in shaping the sustainability of engagement. Studies across sub-Saharan Africa highlighted that affordability, infrastructure, and digital inequities were persistent barriers to inclusion.1,4,54 Limited connectivity, high data costs, and low device ownership continue to constrain participation, particularly among rural youth.33,46 For example, in South Africa, both the InTSHA 33 and Masibambane–Ladies Chat 26 interventions underscored that although WhatsApp-based mHealth programmes improved peer interaction, privacy, and cultural resonance, gender access barriers and stigma restricted full participation. Similarly, Zanoni et al. 46 found that HIV-positive young people have benefited from encrypted WhatsApp support through improved retention in care, yet unequal access to devices and scheduling conflicts persisted. These examples illustrate that even when usability and trust are high, structural inequalities in connectivity and gender norms remain decisive. In Nigeria, the SMART Connections intervention 35 confirmed this pattern: while Facebook secret groups offered confidentiality and peer solidarity for young people with HIV, connectivity limitations, data costs, and gender disparities curtailed engagement. Similarly, in Zambia, Sharma et al. showed that the BITKZ mHealth app, designed to promote SRH knowledge and condom use, improved self-efficacy and decision-making, but faced retention challenges and user fatigue caused by inconsistent internet access. 25 Collectively, these African cases demonstrate that the promise of digital health cannot be disentangled from the infrastructure and socioeconomic realities that frame daily digital experiences of users.
Persistent gender disparities and sociopolitical structures further complicate digital inclusion. For example, in India’s SnehAI chatbot, 44 females reported low self-confidence and discomfort discussing SRH topics, reflecting the cultural stigma surrounding sexuality. In contrast, male users interacted more frequently and openly, highlighting gender asymmetries in the digital agency. Similar patterns were reported by Hanass-Hancock et al. 27 in South Africa, where taboos around teenage pregnancy and HIV disclosure reduced young women’s willingness to participate. These findings affirm that digital participation is both a technological and a sociocultural act mediated by gendered power relations. In several African contexts, including South Africa,26,33,46 Nigeria, 35 and Zambia, 25 restrictive cultural and legal environments around sexual health amplify the risk of online surveillance, stigma, and discrimination, particularly for young women and sexual minorities. Such risks discourage open participation and reinforce digital exclusion. Addressing these systemic barriers requires rights-based and gender-sensitive frameworks that embed privacy-by-design, contextual adaptability, and cultural resonance. Interventions such as Masibambane–Ladies Chat and InTSHA exemplify how the integration of local languages, peer mentorship, and ethical data governance can mitigate contextual constraints and foster sustained participation.26,33,46
While social media platforms were used repeatedly for health promotion, their algorithmic bias towards advertising and attention retention introduces ethical complexities. In social media interventions, engagement was strong due to familiarity and social reinforcement, yet the potential for data commodification and misinformation remained a concern.32,37,43,46,52 Young women often experience online abuse and harassment, including doxxing and non-consensual data sharing, whereas young men are more likely to encounter restrictive social expectations and exposure to harmful online masculinities. These patterns reflect the gendered nature of digital interaction and its implications for psychological wellbeing. 55 These findings echo Zenone et al., who argue that the social media industry operates as a commercial determinant of health, prioritising user retention and profit maximisation over public health objectives. This dynamic not only reinforces digital inequalities but also contributes to emerging concerns about digital fatigue, compulsive use, and adverse mental health outcomes. 56 When situated within an ethical and social context, engagement emerges not merely as a function of individual motivation or user-interface usability but as an outcome shaped by structural access, regulatory capacity, and commercial power. Consistent with the UTAUT construct, facilitating conditions, and the confirmation principle of the ECM, engagement depends on trust, digital equity, and governance mechanisms that balance technological innovation with public accountability.10,11
4.5. Limitations
This systematic review presents several methodological and contextual limitations that should inform the interpretation of its findings. The restriction to studies published in English may have excluded relevant evidence from non-English speaking regions, particularly in sub-Saharan Africa and parts of Asia, thus narrowing geographical and cultural representation. The review period (2019–2024), although aligned with the rapid evolution of digital health, may have omitted earlier interventions that could reveal longitudinal patterns of engagement or foundational behavioural mechanisms.
Most of the included studies were short-term pilot trials or feasibility studies, which limits the ability to draw conclusions about sustained engagement or long-term behavioural outcomes. Furthermore, the predominance of evidence from high-income countries raises concerns about generalisability to low-resource settings, where infrastructural, sociocultural, and economic determinants differ substantially. Heterogeneity in intervention design, outcome metrics, and theoretical grounding restricted the scope for direct comparison and meta-analytic synthesis. The reliance on self-reported engagement measures in several studies introduces potential reporting bias, particularly where social desirability may influence disclosures about sexual and reproductive health behaviours. Finally, the rapid pace of technological change means that the digital platforms assessed in the included studies may evolve or become obsolete, challenging the transferability of the findings to emerging mHealth and social media ecosystems.
4.6. Implications for practice, policy, and future research
The findings indicate that effective mHealth and social media interventions for young people require user-centred design, cultural relevance, and features such as personalisation, adaptive feedback, and peer reinforcement to sustain engagement. In practice, interventions should prioritise usability, confidentiality, and support for digital literacy, particularly in low-resource settings where affordability, access constraints, and sociocultural stigma limit participation.
From a policy perspective, digital health strategies must address persistent structural barriers, including high data costs, poor connectivity, and gendered digital inequalities. Stronger regulatory frameworks are needed to ensure privacy, mitigate misinformation, and recognise social media as an essential health-promotion tool within national digital health strategies.
Future research should adopt longitudinal designs, employ theory-based frameworks, and expand the scope of youth-focused digital health interventions. In South Africa, current efforts are concentrated almost exclusively on sexual and reproductive health, despite the high prevalence of other behavioural risks such as alcohol misuse, inactivity, and poor diet. Broader research agendas are therefore essential. In contrast, studies in high-income countries cover multiple behavioural domains, offering a comparative foundation for designing more diverse and context-responsive interventions in low- and middle-income settings.
5. Conclusions
Engagement in integrated mHealth and social media interventions is a multidimensional construct shaped by cognitive, behavioural, technological, and sociocultural determinants. User-level factors—such as motivation, digital literacy, health awareness, and perceived usefulness—were the strongest predictors of sustained participation. Interventions that incorporated interactivity, personalisation, and adaptive feedback achieved higher engagement and lower attrition, underscoring the importance of usability and real-time responsiveness. Contextual disparities remain a major constraint, particularly in low-resource settings such as South Africa and Zambia, where limited connectivity, affordability challenges, and gendered digital inequalities continue to restrict participation. Although technology design can improve usability, engagement ultimately depends on addressing broader socio-technical and cultural barriers. The predominance SRH interventions in African contexts reflects national health priorities, while studies from high-income countries demonstrated greater thematic diversity across domains such as nutrition, physical activity, and smoking cessation. The absence of alcohol and mental health–specific interventions indicate a neglected yet critical area of youth health behaviour research. Platform trends show a sustained reliance on mainstream social media, especially Facebook, alongside emerging integration with intelligent mHealth systems. This progression reflects the growing global interest in hybrid digital health models accelerated by the post-COVID-19 digital transformation. However, meaningful engagement requires equitable digital access, ethical governance, and cultural inclusivity. In general, integrated digital health interventions show considerable promise for youth health promotion, but their effectiveness depends on context-sensitive design and the mitigation of socio-technical disparities.
Footnotes
Acknowledgements
The author expresses sincere gratitude to the supervisor Prof B. Chimbo for her exceptional academic guidance, methodological insight, and sustained mentorship throughout the course of this research. Deep appreciation is also extended to Dr L. Malungana, the co-supervisor, for her invaluable theoretical contributions, constructive critique, and continuous encouragement, which strengthened both the analytical depth and overall coherence of this work. The author further acknowledges the University of South Africa (UNISA) for providing the digital infrastructure, library resources, and institutional support necessary for the successful completion of this study.
Ethical considerations
Ethical approval for this research was granted by the College of Agriculture and Environmental Sciences – Health Research Ethics Committee (CAES_HREC) of the University of South Africa (UNISA). Registration Number; REC-170616-051; and Reference Number: 2025/CAES_HREC/6657.
Authors contribution
The conceptualisation, design, data collection, analysis, and drafting of this manuscript were undertaken by Mr Moses Mbetse as part of the fulfilment of the requirements for the Master of Science in Computing degree within the Department of Information Systems under the College of Science, Engineering, and Technology (CSET) at UNISA. Prof B. Chimbo served as the supervisor, providing academic direction, guidance, and critical oversight throughout all stages of the research. Dr L. Malungana acted as the co-supervisor, contributing theoretical insight, analytical feedback, and support in refining the structure of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data extracted from the included studies is available and is provided.
Registration
The review was not registered.