
Abstract
Obstructive Sleep Apnea (OSA) is a prevalent respiratory disorder affecting millions worldwide, yet it remains underdiagnosed due to limitations in conventional diagnostic methods such as polysomnography. Recent advances in wearable technology and the integration of Internet of Things (IoT)-based systems have expanded options for OSA detection, offering real-time monitoring and improved accessibility. This paper presents a comprehensive survey of state-of-the-art diagnostic techniques, highlighting emerging wearable solutions, IoT-enabled data transmission, and machine learning algorithms for classification. While portable biomedical devices like HSAT and Morphea enhance patient comfort, challenges such as sensor displacement and measurement sensitivity persist. Furthermore, cloud-based analysis and smart patch antennas demonstrate feasibility in early studies but require rigorous validation and optimization to ensure accuracy and reliability. By synthesizing current advances, this study underscores the need for further research on sensor precision, algorithmic enhancements, and data integration to foster innovation toward effective and accessible OSA diagnostics.
Keywords
1. Introduction
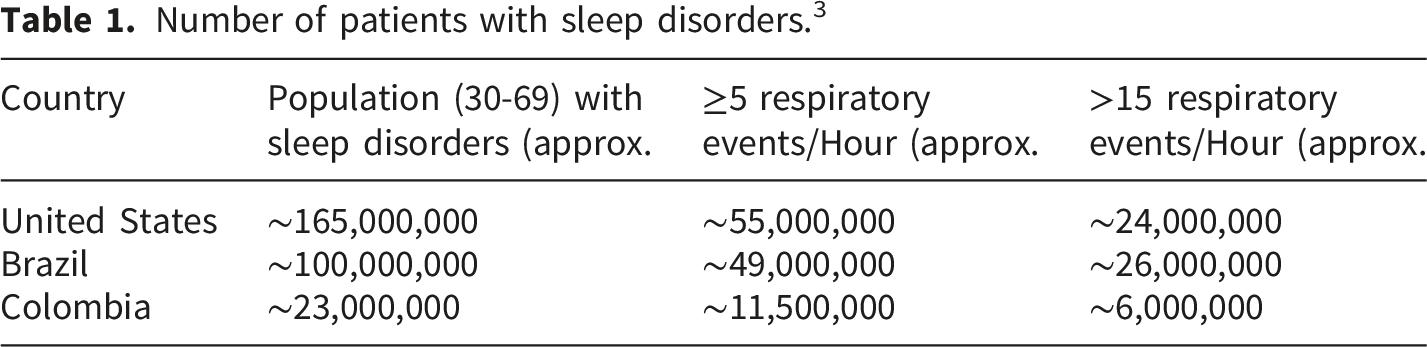
Number of patients with sleep disorders. 3
Recent advances in wearable technology allow individuals to monitor their vital signs and store real-time data. 5 Progress in these technologies plays a significant role in the development of smart devices, enabling effective data management. For instance, minimally invasive smartwatches use various sensors in contact with the body to facilitate data tracking and transmission to the cloud. 6 These devices can measure physiological parameters such as heart rate, sweat pH value, blood pressure, and more. Furthermore, the healthcare and fitness markets have driven advancements in wearable and portable technology. 7
From Table 1, it is evident that OSA is highly prevalent yet underrecognized. New mechanisms for efficiently diagnosing OSA have therefore been proposed. One of the most used techniques for assessing OSA is in-lab polysomnography (PSG); in clinical practice, home sleep apnea testing (HSAT, typically Type III cardiorespiratory polygraphy) is also employed, particularly in adults with a high pre-test probability and without relevant comorbidities. It is recommended alongside PSG within contemporary diagnostic pathways. 8 In parallel, the portfolio of FDA-cleared HSAT devices has expanded, with Type-3 devices dominating recent clearances, underscoring HSAT’s role in improving access while not fully replacing PSG given performance variability across products. 9
PSG and HSAT each have limitations related to robustness and patient comfort. Currently, integrating Internet of Things (IoT) technologies with respiratory recording systems offers a promising way to improve the accuracy and accessibility of OSA assessment. Using IoT devices such as portable systems that incorporate piezoelectric sensors, strain gauges, RFID tags, and optical fibers, real-time or near-real-time respiratory data can be collected, processed, and transmitted for analysis. 10 These advancements enable continuous data collection and facilitate integration with classification algorithms (e.g., support vector machines) for sleep apnea detection.11,12
Such integration supports personalized insights and timely interventions. Nonetheless, the use of IoT sensors in telehealth applications for OSA detection underscores the need for small, low-cost, and reliable devices to ensure accurate and safe diagnosis, posing ongoing challenges in portability, size, and performance. 13
Given the prevalence of OSA, several surveys have comprehensively reviewed diagnostic techniques. For instance, 14 studied various sensor technologies and found limitations in portability and cost-effectiveness. In this other work, the survey, in addition to examining diagnostic algorithms, highlighted issues of robustness and accuracy across diverse conditions. However, while additional reviews have addressed various aspects of OSA diagnostics, they fall short of providing a comprehensive overview that integrates emerging wearable technologies, real-time monitoring capabilities, and IoT. 15
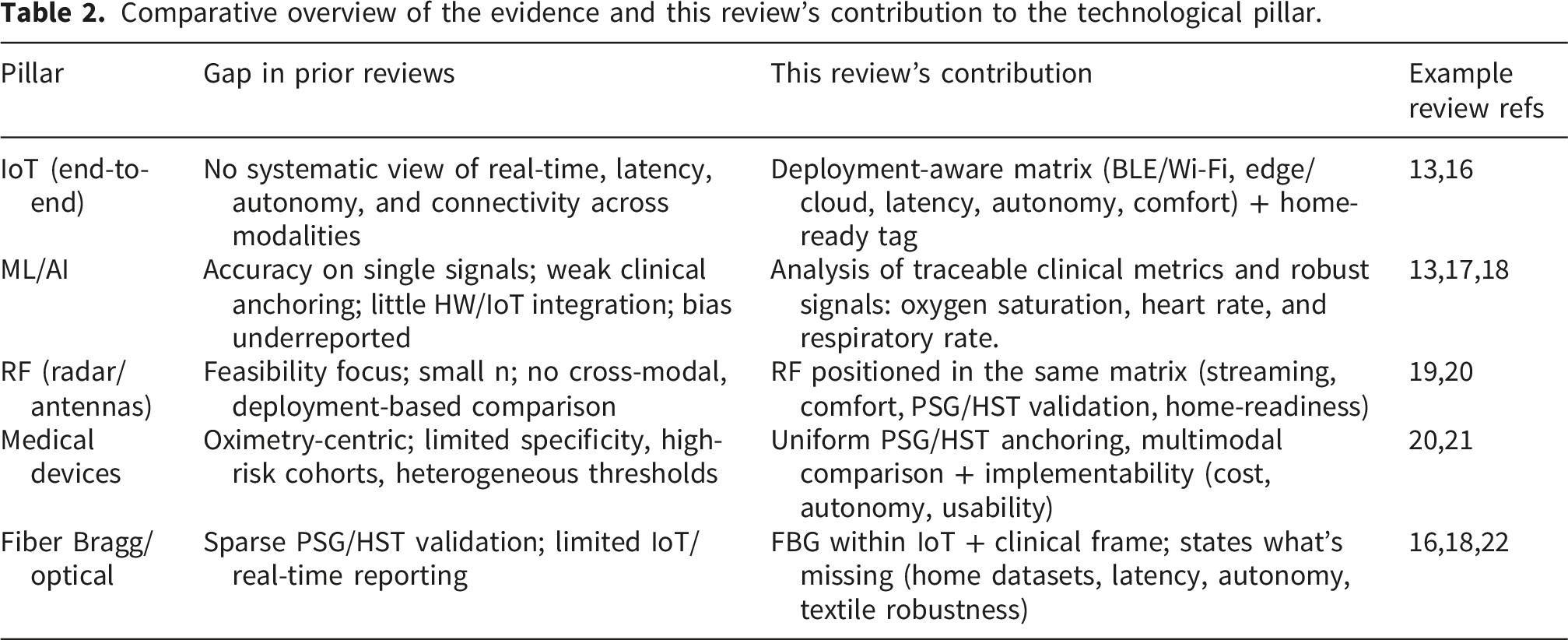
Comparative overview of the evidence and this review’s contribution to the technological pillar.
The structure of this paper is organized as follows. Section 2 presents the theoretical framework for conceptualizing Sleep Apnea Disorder and the nature of sleep, followed by a discussion of the techniques, methodologies, and algorithms used to diagnose and monitor sleep apnea. Section 3 analyzes each of these techniques, identifying the main advantages and disadvantages compared to other parts of the state of the art. Finally, Section 4 presents the main findings and provides key ideas for future research.
2. Background
The structures of the respiratory system are designed to perform their functions effectively. In this section, we will study the aspects of sleep physiology; then, we will review the characteristics of obstructive sleep apnea. The search methodology was designed to ensure the relevance and quality of the studies selected for this review. The search was conducted in the Web of Science and ScienceDirect databases, using the search equation: “sleep apnea” or “respiratory rate” and “sensors” or “wearable technologies” or “Bragg fiber” or “radiofrequency techniques.” Inclusion and exclusion criteria were defined to refine the results, including studies published from 2020 onwards, open-access articles, studies in English, and research articles only, while reviews were excluded. This process ensured the selection of current, accessible research of high scientific standards. Additionally, a bibliometric analysis of the number of articles published per year revealed a relatively steady publication trend in recent years, with a notable increase in 2023. This temporal analysis highlights the evolution and growing interest in research on sleep apnea and in technologies for its diagnosis and monitoring.
2.1. Obstructive sleep apnea (OSA)
Obstructive sleep apnea (OSA) is a common sleep-related breathing disorder characterized by recurrent apnea and hypopnea due to upper-airway collapse.23,24 It is associated with non-restorative sleep, fatigue, increased accident risk, and metabolic comorbidities, reinforcing its public health importance.25–28 Global prevalence is estimated at ∼4–13% in men, and ∼2–5.6% in women, and AHI-based models suggest that ∼1 billion adults aged 30–69 have OSA worldwide, including ∼425 million with ≥15 events/h.24,25 In Colombia, reported) prevalence ranges ∼9–38% overall and rises with age (up to ∼84% in geriatric cohorts), with sex-specific estimates of ∼22% in men and ∼17% in women; by age group: 30–49 years ∼3% in women and ∼10% in men, and 50–70 years ∼9% in men and ∼17% in women.29,30 Clinically, France and the United States have advanced diagnosis and treatment through accredited sleep centers, home testing, and auto-titrating CPAP within multidisciplinary pathways. 31 At the same time, epidemiologic research and community programs continue to expand across Asia and Africa to improve awareness, early detection, and access.27,28
2.2. Monitoring and diagnosis of sleep apnea
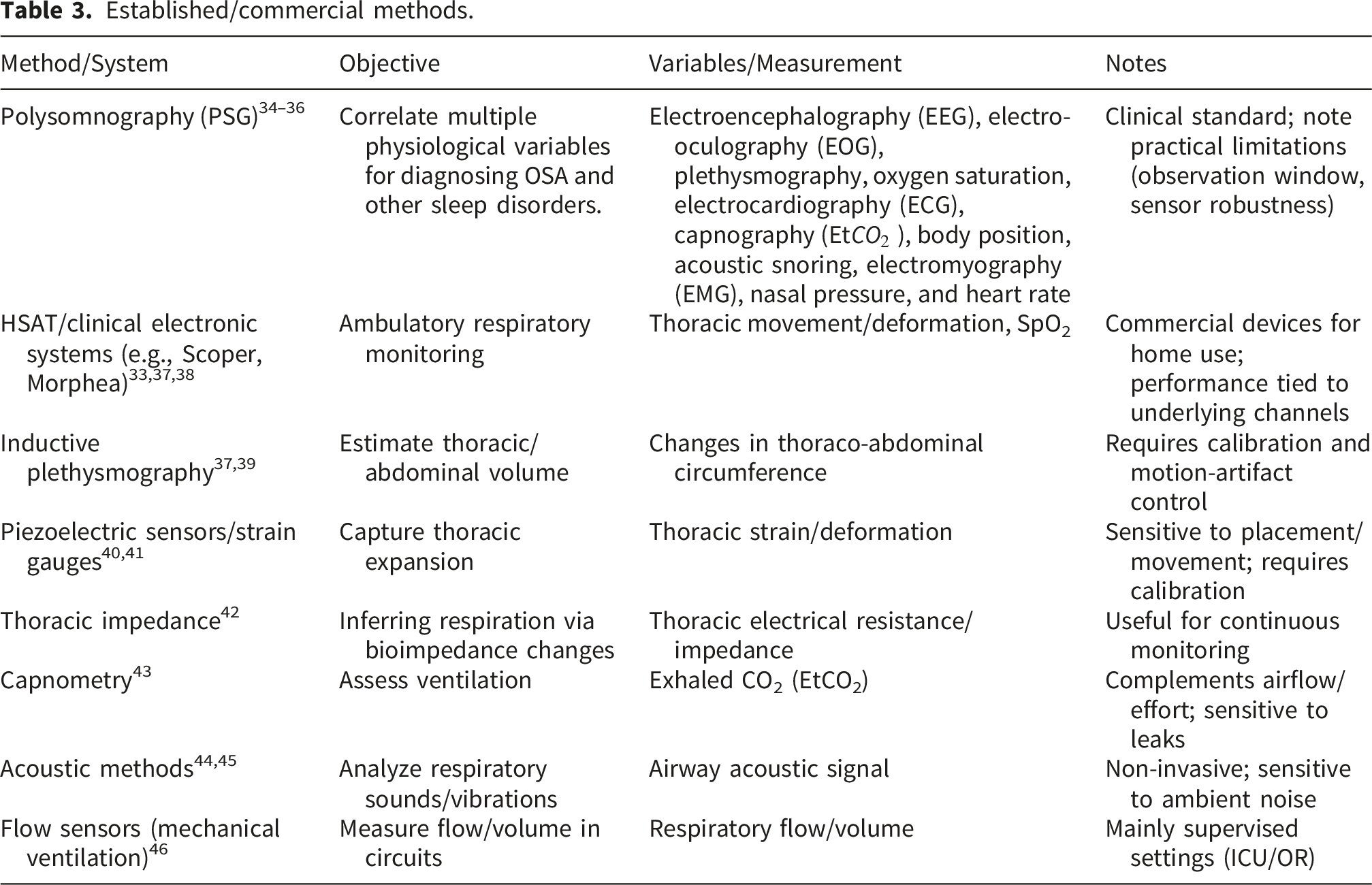
Established/commercial methods.
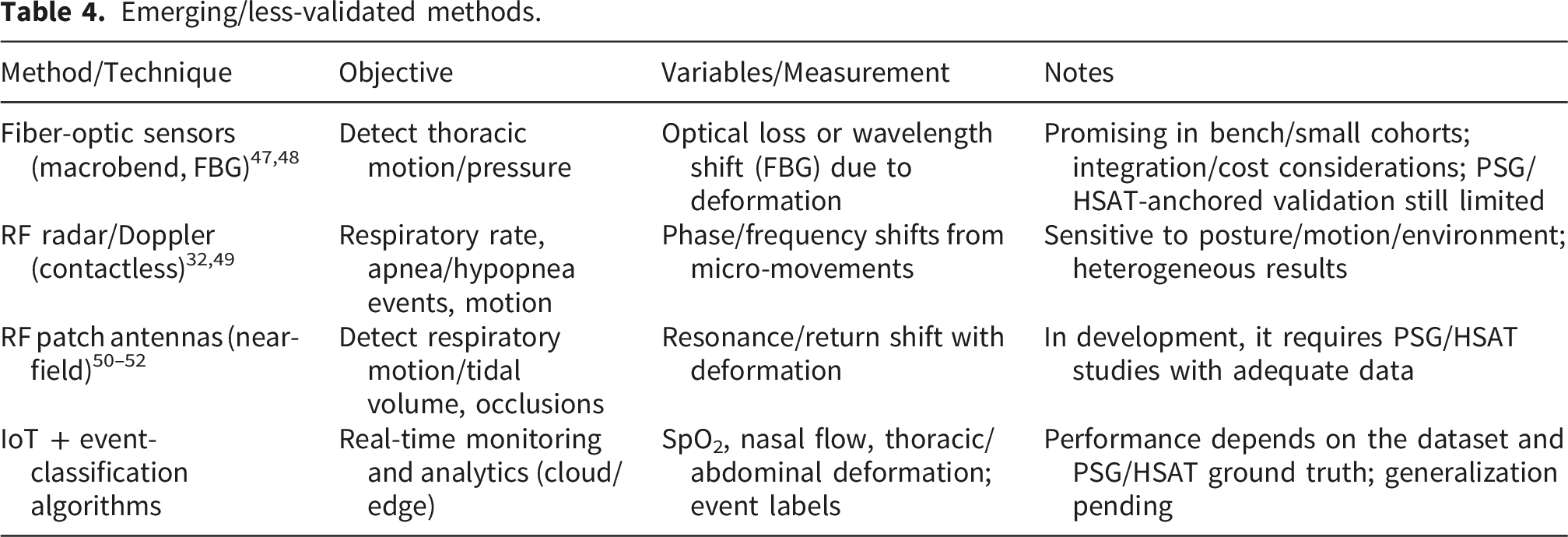
Emerging/less-validated methods.
2.2.1. Polysomnography (PSG)
In the context of sleep medicine, a variable refers to the specific physiological signals, or “channels,” acquired during a diagnostic recording, the exact configuration of which is governed by clinical indication and laboratory protocols. To ensure clinical validity, these channels must consistently align with the standards established by the American Academy of Sleep Medicine (AASM) and the American Association of Sleep Technologists (AAST), which provide the essential framework for the monitoring, recording, and clinical scoring of sleep architecture and respiratory events. 53
A standard diagnostic polysomnogram (PSG) integrates several core physiological variables to provide a multi-parametric assessment. These include electroencephalography (EEG) to identify sleep stages (N1, N2, N3, and REM) and detect micro-arousals, electro-oculography (EOG) to distinguish between NREM and REM phases through eye movement detection, and electromyography (EMG) to evaluate muscle tone for identifying REM atonia and periodic limb movements.53,54 Respiratory assessment is conducted via airflow monitoring using nasal pressure transducers or thermistors to detect apnea and hypopnea events, combined with the measurement of thoracic and abdominal expansion, typically through inductive plethysmography, to distinguish between obstructive and central events.
55
Furthermore, continuous pulse oximetry quantifies arterial oxygen saturation
Sleep medicine specialists interpret polysomnography (PSG) to diagnose conditions such as sleep apnea, insomnia, restless legs syndrome, and other sleep disorders.59,60 However, PSG presents several limitations: (1) limited event yield here, capacity refers to the restricted observation window (often a single night), and finite sampling resolution. For example, a technically adequate home sleep apnea test (HSAT) requires ≥4 hours of usable oximetry and flow data. If a single HSAT is negative, inconclusive, or technically inadequate, PSG should be performed.61,62 Moreover, night-to-night variability can lead to ∼17% misdiagnosis and ∼32% misclassification when relying on a single night, prompting algorithmic adjustments to increase effective sampling and event detectability 62 (2). PSG tends to capture static snapshots of sleep, whereas analyzing dynamic behavior may better correlate with comorbid conditions.10,34 (3) There remains a need to improve diagnostic performance and usability: in a type-III HSAT vs. PSG, accuracy metrics reached sensitivity 94.9% / specificity 62.5% for Apnea–Hypopnea Index (AHI) ≥ 5 and 80.0%/74.1% for AHI ≥ 15. 63 Peripheral arterial tonometry devices (e.g., WatchPAT) show high sensitivity but variable specificity (pooled 94.1%/43.5% at AHI ≥ 5; 92.2%/72.4% at AHI ≥ 15), underscoring heterogeneity across portable systems. 64 Usability/technical robustness also constrain yield: recent reviews of home-PSG report a pooled technical failure rate ∼7.8% (95% CI 5.5–10.1), and self-applied multi-night protocols still show ∼15% first-night failure. 34 (4) Precise, reproducible sensor placement for each physiological channel is required. 65 (5) Equipment robustness in routine use is variable.66,67 (6) Technical failures, such as electrode detachment, can invalidate a study and necessitate repeat testing. Taken together, addressing these limitations while leveraging newer technologies is key to bridging clinicians’ reliance on PSG with the expanding ecosystem of portable recordings. Although advances have improved availability, convenience, and cost-effectiveness, objective appraisal remains complicated by heterogeneous devices and clinical use-cases; recent syntheses conclude that more rigorous validation is still needed. 64
2.2.2. Medical devices used for sleep apnea monitoring
The growing demand for portable technologies for remote monitoring of physiological variables has driven the design of compact, cost-effective devices that enable accurate, secure diagnostics. For sleep disorders, which require monitoring 5 to 7 physiological variables, biomedical devices such as SCOPER, 68 Home Sleep Apnea Testing (HSAT), 9 and automated processing and machine learning analysis (APMLA) 69 have been developed. These devices allow simultaneous analysis of signals, such as thoracic movement or deformation and oxygen saturation, aiming to make physiological data monitoring and storage more efficient and patient-friendly. However, research on portable devices for polysomnography has identified several challenges that limit their effectiveness in assessing sleep patterns and related physiological events. Additionally, while effective at recording static sleep characteristics, such as stages and duration, these devices struggle to analyze dynamic behaviors across the sleep cycle, hindering the comprehensive correlation of sleep patterns with various health conditions.59,70–72 It is essential to improve these devices’ sensitivity, specificity, and usability (e.g., Type-III HSAT vs PSG: sensitivity 94.9%/specificity 62.5% at AHI ≥5 and 80.0% / 74.1% at AHI ≥15 63 ; peripheral arterial tonometry devices show high sensitivity but variable specificity pooled 94.1% / 43.5% at AHI ≥5 and 92.2%/72.4% at AHI ≥15. 64
Another significant challenge is the precise placement of sensors on the body, which is crucial for reliably collecting physiological data. Determining the optimal location for each sensor requires further research and development. In summary, these limitations underscore the inherent complexity of portable polysomnography devices and emphasize the need for continued innovation to improve the accuracy and utility of sleep monitoring technologies.11,59,73 Various techniques have been implemented to measure changes in thoracic volume during inhalation and exhalation, including inductive plethysmography, piezoelectric sensors, strain gauges, and thoracic impedance.74,75 Inductive plethysmography measures changes in thoracic or abdominal volume by detecting variations in inductance caused by respiratory movement. 76 This technique involves placing an elastic band around the patient’s chest or abdomen, which contains metal wires forming an inductive circuit. During breathing, the stretching and contracting of the band produce variations in inductance, which are translated into changes in the electrical signal. These data are processed through algorithms that calculate the respiratory rate and depth. Inductive plethysmography allows for continuous, non-invasive measurement of respiratory effort, although its accuracy can be affected by patient movement and positioning.76,77 On the other hand, piezoelectric sensors detect thoracic movement by generating an electrical signal in response to changes in pressure or deformation. Placed on the patient’s chest, these sensors generate a current proportional to the degree of chest deformation as it expands or contracts during breathing. The electrical signal is processed to calculate the respiratory rate and detect abnormal breathing patterns. This technique is sensitive to external movements, which can affect its accuracy in patients with sleep apnea, though it is effective for continuous and non-invasive monitoring.41,78
Strain gauges use extensometers placed on the chest or abdomen to measure changes in skin length or deformation during breathing. These gauges work by varying electrical resistance as the sensor stretches or compresses, and the data are processed to determine the amplitude and frequency of respiratory movements. Strain gauges help detect small movements, though their accuracy depends on careful placement, and they may be uncomfortable for long-term sleep monitoring. Thoracic impedance is another important technique that measures the variation in electrical impedance between two electrodes placed on the chest.79,80 Impedance changes with inhalation and exhalation due to alterations in tissue conductivity, allowing calculation of respiratory rate and depth. The impedance signal is processed and correlated with other data to detect sleep apnea and other respiratory disorders. This is a non-invasive technique, though its accuracy can be limited by patient movement and interference from other electronic devices.81,82
To accurately quantify thoracic volume change during sleep, mechanical-effort signals should be correlated with physiologic markers (e.g., oxygen desaturation), yet established methods show sensitivity/specificity trade-offs: esophageal manometry exhibits low sensitivity (64%) and moderate specificity (78%) for thoracic movement changes 83 ; a planar pressure sensor differentiated thoraco-abdominal motion in supine posture but performance depended on mattress firmness and position 84 ; capnometry provides real-time tidal volume/CO2 estimates but cannulas/masks can be uncomfortable and prone to displacement.58,85 Less obtrusive approaches, such as ultrasonic/Doppler propagation analyses and neck acoustics, offer contact-light monitoring but remain sensitive to medium complexity and cough/speech interference.86,87 Within a rapidly evolving HSAT regulatory context, U.S. FDA clearances have accelerated since 2022 and emphasize electrical/biocompatibility safety, performance testing, usability, cybersecurity, and clinical validation. 9 Consistent with this trend, a pediatric CSA prototype with miniaturized hardware and on-board analytics triggered reliable alarms during prolonged pauses and matched commercial monitors in adult tests. 88
Against this backdrop, photoplethysmography (PPG) has been explored for AI-enabled sleep analytics in pediatrics. In a multicenter study using the CHAT database, 366 children with suspected OSA (5–10 years) contributed PSG-derived PPG signals; these were resampled to 64 Hz and segmented into non-overlapping 30-s epochs labeled as W/NREM/REM by technicians. The cohort was split into training/validation/test sets with 219, 73, and 74 subjects, respectively. A convolutional neural network (CNN) operating on raw PPG (with temporal context) achieved 78.2% accuracy and Cohen’s κ = 0.57 for 3-class (W/NREM/REM) staging on the independent test set. Per-class performance (precision/recall/F1) was Wake 0.81/0.69/0.74, NREM 0.79/0.91/0.85, and REM 0.64/0.41/0.50. At the patient level, Wake% derived from the CNN showed an ICC of 0.59 vs. PSG (p = 0.002). These results indicate moderate agreement in pediatric staging with PPG-only CNNs, while highlighting lower REM performance and the need for external validation. 89
Over two decades, peripheral arterial tonometry (PAT), PPG, and Home Sleep Apnea Testing (HSAT) devices have moved from early wrist-worn WatchPAT systems that fused peripheral arterial tonometry with oximetry and actigraphy to estimate AHI at home, toward miniaturized fingertip probes with cloud-based analytics and more explicit handling of borderline categories (e.g., AHI 5–15) (historical overview and limitations of PAT without EEG for true TST/arousals in HSAT:
90
; meta-analysis detailing near-threshold discordance and the role of TST misestimation.
64
). NightOwl PATHSAT exemplifies this trajectory through a fingertip form factor that streams PPG-derived modalities, including oxygen saturation
In parallel, the next generation of peripheral arterial tonometry (PAT) devices, such as the Somfit system, integrates EEG-derived sleep/wake staging to mitigate common error sources that contribute to misestimation of Total Sleep Time (TST) and to misclassification of arousals. This multimodal architecture, combining forehead-based PAT with EEG signals, demonstrates balanced ROC performance across various AHI thresholds, with device-level failure and data-transfer characteristics comparable to those of established technologies such as WatchPAT. By incorporating cortical activity monitoring, this architecture reflects a maturing data path from edge devices to cloud processing, addressing traditional limitations in the accuracy of predicted apnea-hypopnea index (pAHI) and the agreement of oxygen desaturation index (ODI). Technical evaluations further highlight that this integrated approach reduces the comparative bias and meta-analytic discordance often observed in sensors that lack simultaneous EEG staging.
2.2.3. Fiber optic sensors used for sleep apnea monitoring
Fiber-optic sensors have gained popularity for measuring biophysical parameters due to their high sensitivity, immunity to electromagnetic interference (EMI), and long lifespan. These properties make them ideal for medical applications, such as sleep apnea monitoring, where it is crucial to measure respiratory behavior in the thoracic and abdominal regions precisely and continuously. Fiber optic sensors used in these applications, such as macrobend sensors, detect changes in light when the fiber bends in response to respiratory movements, enabling effective monitoring of chest expansion and contraction.92,93 These fiber-optic modalities are emerging: they show promising sensitivity and inherent EMI immunity in bench and small-cohort settings, but PSG/HSAT-anchored validation remains limited, integration is heterogeneous (textile/adhesive), and home-readiness is unclear; cost and durability under cyclic strain also remain open issues.
One of the most widely used technological advances in fiber optic sensors is the Fiber Bragg Grating (FBG). FBGs are characterized by a periodic structure in the fiber optic core that alters their refractive index. This periodic alteration causes the FBG to reflect a specific wavelength of light while allowing other wavelengths to pass through. Thanks to their small size and resistance to EMI, FBGs are highly sensitive to environmental factors such as mechanical strain, temperature, and humidity, making them an effective tool for monitoring physiological parameters.94,95 Overall, FBG-based solutions are emerging: while sensitivity and EMI immunity are attractive, comparative PSG/HSAT evidence is still sparse, integration pathways vary, and cost/durability under real-world cyclic loading require further study.
Figure 1 illustrates a Fiber Bragg Grating (FBG). The Bragg grating within the fiber acts as a wavelength filter that reflects only a specific wavelength, known as the Bragg wavelength ( Fiber Bragg Grating (FBG), source.
96

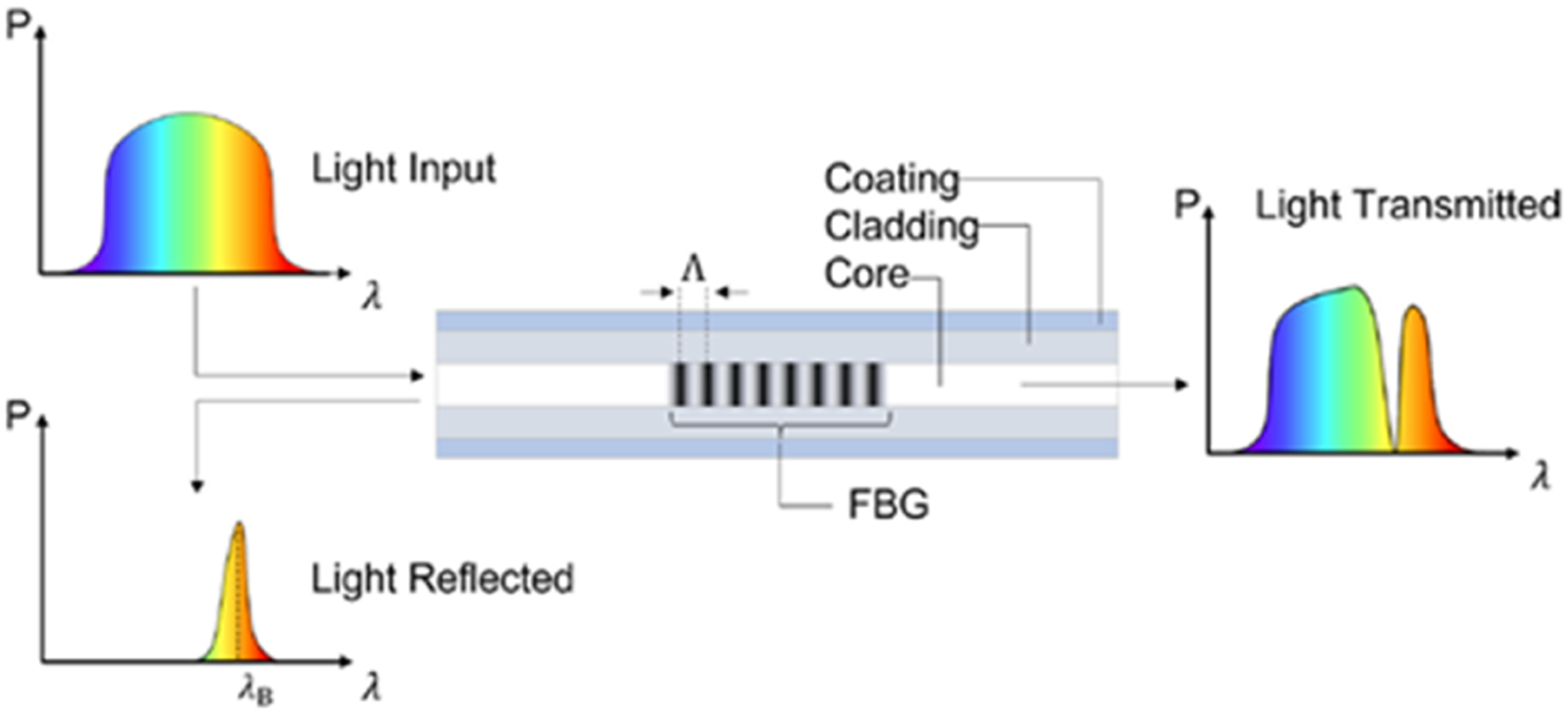
When the fiber is subjected to tension, as occurs during respiratory movements in the chest and abdomen, the grating period (Λ) and the effective refractive index (eta) change, shifting the Bragg wavelength. This shift is measured with high precision and allows the deformation in the fiber optic to be inferred, corresponding to respiratory movements. The high sensitivity of FBGs, with sensitivity values around 1.2 pm per micron of elongation (≈1.2 pm · με, allows for the detection of even small chest movements, essential for sleep apnea applications.47,97
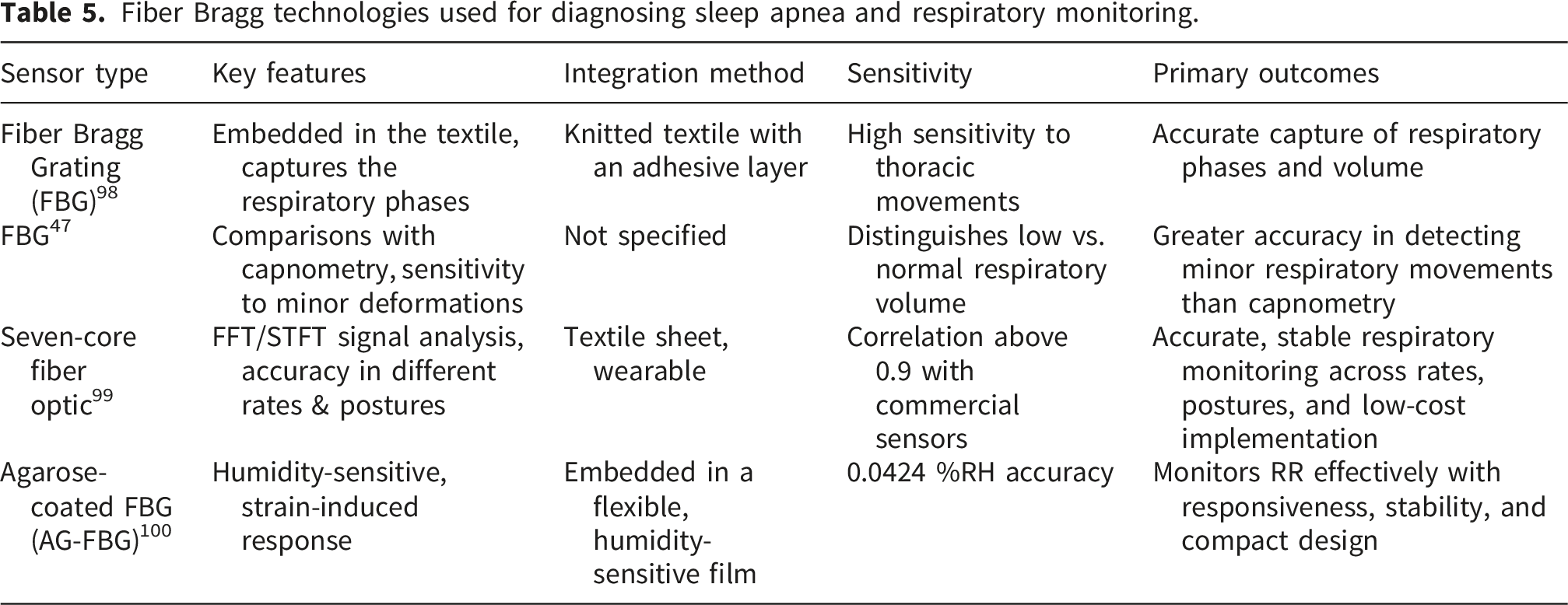
Recent studies show FBGs embedded in fabrics through sewing or knitting create garments that continuously monitor breathing patterns. This demonstrated that FBGs can effectively transduce thoracic movements using an adhesive rubber textile layer. This system precisely detects respiratory phases, including the respiratory period, inspiration and expiration durations, and tidal volumes for both lungs. 98
Additionally, in another study, the performance of fiber-optic sensors was compared with conventional capnometry devices, demonstrating that FBGs achieved greater accuracy in distinguishing between low and normal respiratory volumes. FBG technology is particularly effective at capturing minor respiratory movements due to its ability to discriminate against small deformations. Despite their multiple advantages, the use of FBG in textiles presents some challenges, such as the durability of the sensors under constant strain and the effect of body bioimpedance on measurements. Future research should focus on enhancing the robustness of FBG sensors on validating their accuracy in clinical settings, enabling broader implementation in medical applications. 47
This study presents a wearable optical fiber sensor designed for accurate respiratory monitoring, aiming to overcome manufacturing challenges, enhance precision, and improve comfort compared to traditional wearable sensors. The device uses a seven-core fiber embedded in a textile sheet, making it easy to wear on the upper body. Signal analysis is conducted with Fast Transform Fourier (FFT) and short-time Fourier (STFT) transforms. Experiments with six volunteers demonstrated the sensor’s high accuracy and versatility in detecting various respiratory rates (normal, slow, fast), body regions (abdomen, chest, back), postures (standing, sitting, lying), and irregular breathing. The sensor achieved a Pearson correlation coefficient above 0.9, comparable to commercial sensors, and maintained stable performance over six months with a minimal frequency error of 0.003 Hz. Combining high sensitivity, stability, and comfort, this affordable, compact optical fiber sensor shows great potential for healthcare, enabling precise, long-term respiratory monitoring. 99
Fiber Bragg technologies used for diagnosing sleep apnea and respiratory monitoring.
2.2.4. Radiofrequency techniques
In recent years, radiofrequency techniques have emerged as a promising tool in detecting and treating OSA. Radiofrequency techniques harness radiofrequency energy to provide a non-invasive and effective solution for diagnosing this condition. These techniques are based on the emission of high-frequency electromagnetic waves that penetrate the body’s tissues and generate controlled heat in specific areas. In the following, we will provide a detailed description of the use of radiofrequency techniques for diagnosing OSA.
2.2.4.1. Radars
In recent years, Doppler radar techniques have emerged as a promising tool in detecting and treating sleep apnea. A Doppler radar motion-sensing transceiver transmits a continuous wave signal, receives its reflection from a moving surface, and analyzes the phase of the signals to extract motion information. Although most physiological radar measurements employ fixed-beam antennas to narrow the radar field of view, the use of phased-array antennas, which can electronically steer the radar beam by adjusting the relative phase of the signal at each antenna element, has also been demonstrated to track and isolate specific subjects.32,101 When stationary surfaces are encountered in the radar signal path, the demodulated phase-difference signal remains constant. However, surfaces undergoing periodic motion generate a phase-demodulated output signal that varies in proportion to displacement over the motion cycle. The resolution of the received signal, however, is influenced by the standing wave pattern established by the nominal distance to the moving subject. Depending on the frequency of the transmitted wave, null points where destructive interference of transmitted and received signals occurs may compromise resolution, typically at even multiples of 

In 2018 a non-contact cardio-pulmonary monitoring system was developed with a Bioradar prototype using LabVIEW for real-time monitoring. Signals were captured by two antennas—a transmission and reception one. They designed a radio system for RF modulation and demodulation and developed two antennas: a 4×4 array and a patch antenna to improve signal quality. Three tests with a healthy volunteer’s normal breathing successfully captured respiratory signals without contact. The Bioradar was compared to a Biopac system, a standard device for recording respiration, heart rate, and vital signs. Synchronizing both systems and acquiring data simultaneously was the main challenge. While the Biopac showed clear signals, Bioradar signals were slightly distorted due to its operating principle and the patient’s irregular breathing. Despite distortions, both signals could be compared. The study concluded the Bioradar effectively monitored cardiovascular and pulmonary activity, confirming its potential as a safe, non-invasive alternative. 103
The basic principle of Doppler radar is to transmit a microwave signal toward a target, usually within ISM-licensed bands. In this work surveyed Doppler radar-based sleep apnea detection, detailing system architecture, noise elimination, and signal processing. They used a Support Vector Machine algorithm to detect apnea events with 69% accuracy and 88% reliability. Sleep stages cause body movement and respiratory changes that can affect classification. Results showed a correlation coefficient of 0.87 for Cheyne-Stokes respiration (%CSR > 5.0) and 0.8 for AHI >15. Cheyne-Stokes involves cyclic breathing changes and apnea, with >5% sleep time indicating potential health issues like heart failure. An AHI >15 indicates moderate sleep apnea and requires medical attention. Due to the small sample size, larger studies are needed to validate this radar system. 104
A contactless, non-invasive physiological monitoring radar system (K-MC1) was proposed for sleep studies. The system uses quadrature Doppler radar to detect motion, eliminating the need for body-mounted sensors. The physiological radar monitoring system (PRMS) employs a quadrature Doppler radar that outputs in-phase (I) and quadrature-phase (Q) signals to measure amplitude and direction of motion. This design aims to address signal “blind spots” in a single-channel RF system caused by interference or attenuation at specific frequencies. With only one channel, obstacles or interferences can weaken or block the signal. To detect sleep apnea in real time, a binary classification algorithm was developed. Results from the PRMS were compared to PSG data, showing substantial agreement in apnea and hypopnea event detection, with overall sensitivity of 86%, specificity of 91%, and accuracy of 92%. 105
In this work, we propose combining radar technology with pulse oximetry using a second-by-second sleep apnea event classifier. Fourteen patients referred for at-home sleep apnea testing were enrolled in the study: six controls and eight patients with sleep apnea (four mild, two moderate, and two severe). They were monitored using Somnofy, a radar-based sleep monitor that provides non-contact sleep tracking. Somnofy uses low-power radio waves to detect body movements and breathing patterns without the need for physical sensors, enhancing comfort during sleep studies. The monitoring with Somnofy was conducted concurrently with respiratory polygraphy. A neural network was trained using data from Somnofy and pulse oximetry and validated against polygraphy scores using cross-validation. 106
To evaluate the performance of their classifier, the authors used Cohen’s kappa coefficient, a statistical measure of inter-rater agreement for categorical items. Cohen’s kappa accounts for the agreement occurring by chance and provides a value between -1 and 1, where: Values ≤ 0 indicate no agreement
107
: • 0.21–0.40 represents fair agreement. • 0.41–0.60 represents moderate agreement. • 0.61–0.80 represents substantial agreement. • 0.81–1.00 represent almost perfect agreement.
In their results, Cohen’s kappa coefficient for classifying non-event/event seconds was 0.81, indicating almost perfect agreement between the classifier and the polygraphy scores. For classifying non-event/hypopnea/apnea, the kappa coefficient was 0.43, representing moderate agreement. When distinguishing between non-event/obstructive apnea/central apnea/mixed apnea, the kappa coefficient was 0.36, which is considered fair agreement. These values suggest that the classifier performs very well in detecting the occurrence of any event but is less accurate when distinguishing between specific types of respiratory events. Additionally, the authors employed the Bland-Altman method to assess the agreement between the respiratory event index (number of apnea events per recording hour) obtained from their classifier and the polygraphy scores. The 95% Bland-Altman agreement limits ranged from -8.25 to 7.47, indicating that 95% of the differences between the two measurement methods fall within this range. This range is acceptable in clinical settings and suggests good agreement between the methods. All participants were correctly classified by sleep apnea severity based on the Apnea-Hypopnea Index (AHI), which categorizes sleep apnea as mild (AHI 5–15), moderate (AHI 15–30), or severe (AHI >30). An AHI greater than 15, as observed in some participants, indicates moderate sleep apnea, a condition that is clinically significant and requires medical attention. Accurate classification across all severity levels indicates that the system is effective at identifying and categorizing sleep apnea. The results suggest that combining radar and pulse oximetry could be more accurate than either technology alone for detecting sleep apnea events. By achieving almost perfect agreement in event detection and acceptable agreement in event classification, the study demonstrates the potential of this combined approach for non-invasive, at-home sleep apnea monitoring.
A contactless Impulse Radio Ultra-Wideband (IR-UWB) radar device (OrbSense) was evaluated against in-laboratory polysomnography (PSG) in 359 adults. It measures chest-wall motion at 7.29 GHz with 1.5 GHz bandwidth and 0.1 mW power. Recordings were analyzed automatically, and PSG was scored per guidelines. The OrbSense respiratory event index (REI) was slightly lower than the PSG apnea–hypopnea index (AHI) but highly correlated (r=0.92). Bland–Altman showed a mean difference of 1.5 events/h. For AHI > 5, an OrbSense cutoff of 8 events/h had 90.4% sensitivity and 77.6% specificity. For moderate to severe OSA (AHI > 15), a cutoff of 16.6 events/h achieved 87.1% sensitivity and 89.7% specificity. ROC curves had AUCs of 0.904, 0.942, and 0.966 for AHI thresholds ≥5, ≥15, and ≥30, respectively. Severity classification agreed in 69.6% of cases. These results support OrbSense as a reliable tool for sleep apnea screening, though further studies in community and home settings are needed. 108
Regarding the radar-based detection system, segment-level classification achieved AUC values of 0.796-0.859. While the system demonstrated robust ability to identify apnea-hypopnea events, performance metrics varied with OSA severity: sensitivities ranged from 49.0% to 67.6%, and false-positive rates per participant ranged from 23.4% to 52.8%. Despite this variability in sensitivity, the estimated Apnea-Hypopnea Index (AHI) showed high correlation with ground-truth PSG data (r = 0.805-0.949) and excellent reliability, as evidenced by intraclass correlation coefficients (ICC) between 0.776 and 0.929. Furthermore, the clinical severity classification showed substantial agreement (Kappa range: 0.648–0.736), underscoring the potential of contactless radar technology as a viable independent screening tool for OSA. 109
Finally, introduce a new biomedical radar-based IoT system with an automatic algorithm to precisely measure respiratory phases and amplitude during sleep, reducing the discomfort caused by traditional nasal cannulas. Tested on 10 adults, including those suspected of sleep apnea, and gathering around 3851 minutes of data, the system showed high accuracy: 97% for the respiration-to-respiration interval (RRI), 93% for inhale duration (ID), and 92% for exhale duration (ED). By reconstructing Doppler respiratory and airflow waveforms from radar signals, it can extract accurate respiratory variables. Importantly, it effectively distinguishes between REM and non-REM sleep by accurately detecting RRI, addressing the instability of respiratory activity during REM sleep. Although irregular breathing during REM increases detection errors, the results suggest this contactless monitoring method has great potential for future medical IoT applications, improving long-term respiratory monitoring and sleep analysis without patient discomfort. 110
2.2.4.2. Internet of Things (IoT) and respiratory event classification algorithms
Internet of Things (IoT) techniques have been widely used in sensor applications and detection systems.
111
Integrating IoT, machine learning, and cloud computing enables real-time detection and diagnosis of sleep apnea (See Figure 2). This framework consists of three layers such as the sensing layer, where wearable sensors collect physiological data such as thoracic deformation, heart rate, and oxygen saturation; the fog layer, which processes and filters data locally to reduce latency and enhance real-time analysis; and the cloud layer, which stores, analyzes, and interprets data using machine learning, allowing remote monitoring and early diagnosis.112–114 Architecture of the IoT healthcare system. Source: Author.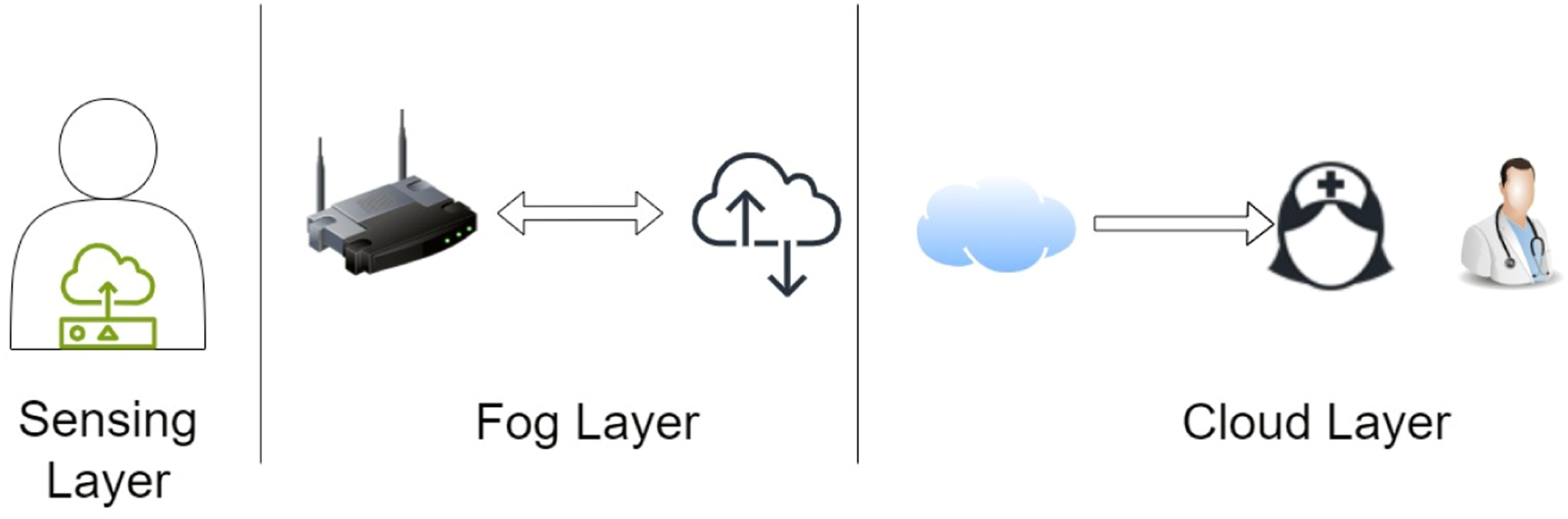
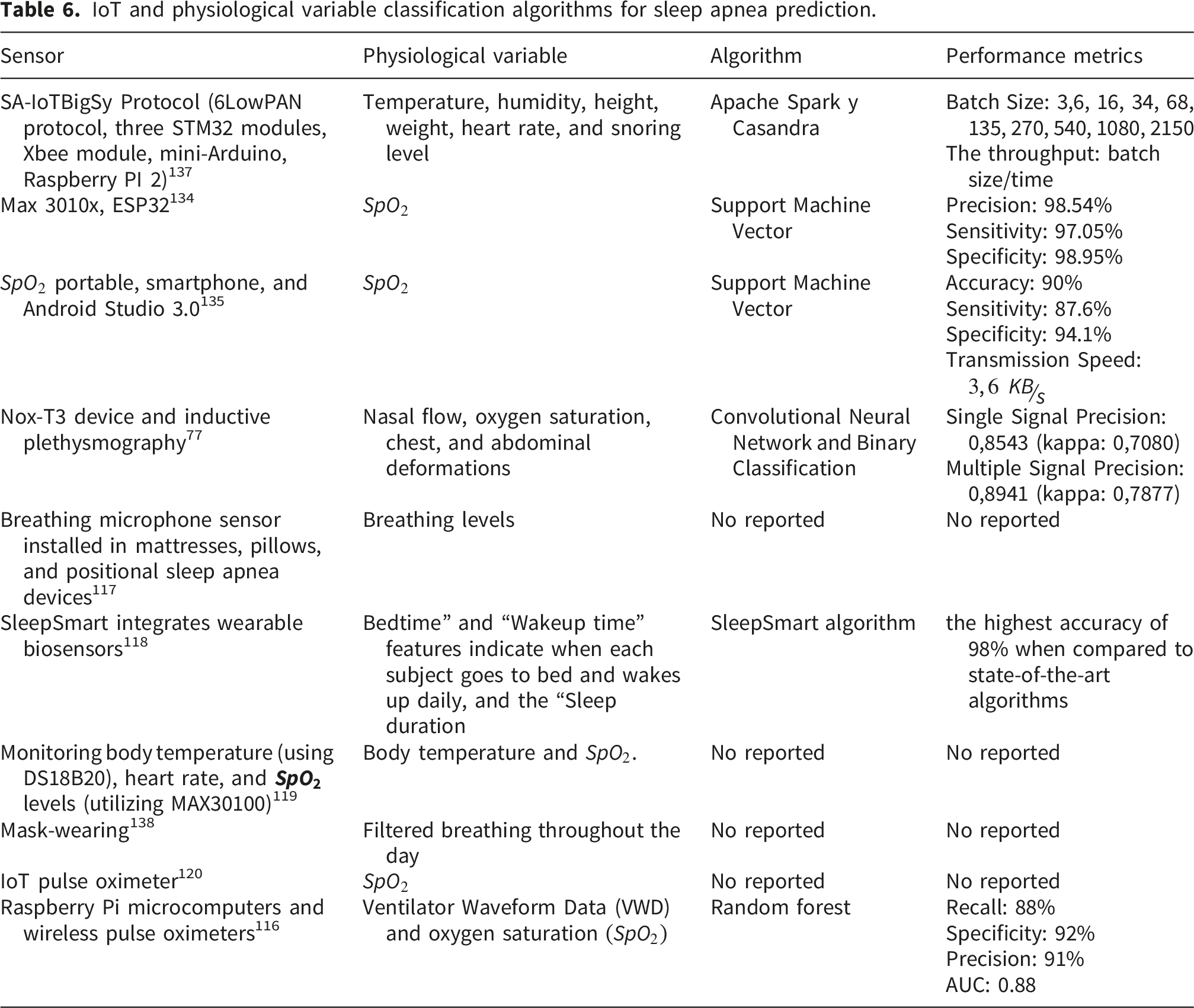
For example, multiple datasets of oxygen saturation data were collected and used to train a Support Vector Machine (SVM) for binary classification of sleep apnea events. The study proposed an apnea detection system based on the Internet of Things (IoT), consisting of three main components: a portable device for data acquisition, a smartphone-based monitoring system, and a cloud-based monitoring center for storage, analysis, and visualization. Oxygen saturation data were sent to a mobile phone and processed using an SVM algorithm, enabling real-time event classification. The system achieved 90% accuracy, 87.6% sensitivity, and 94.1% specificity, demonstrating its effectiveness in detecting significant, potentially severe apnea events. 115
Additionally, a Clinical Decision Support System (CDSS) was developed specifically for managing ICU patients. It utilizes IoT devices that collect real-time physiological data from ventilators and other medical equipment. The prototype architecture employs Raspberry Pi microcomputers to gather and stream Ventilator Waveform Data (VWD) and blood oxygenation (SpO2) data from wireless pulse oximeters. Machine learning models, particularly Random Forest classifiers, analyze this collected data to assess whether the ventilator is administering potentially harmful therapy and to detect acute respiratory distress syndrome (ARDS), a serious respiratory condition. The Random Forest classifier achieved a recall of 88%, specificity of 92%, precision of 91%, and an AUC of 0.88, demonstrating strong performance in classifying respiratory issues relevant to sleep apnea diagnosis. 116
Another study focused on detecting sleep posture and respiratory disorders during sleep by measuring the sensory response of pressure sensors and a breathing microphone sensor installed in mattresses, pillows, and positional sleep apnea devices. Three pressure-sensor positions were used for the analysis, and the breathing microphone measured breathing levels during sleep. An advanced sleep monitoring system based on a non-intrusive approach was developed, using an ESP8266 microcontroller to transmit sensor data and display it in web applications. This system provides real-time monitoring of sleep posture and respiratory patterns, aiding in the detection of sleep apnea events. 117
On the other hand, the study demonstrated the feasibility of automated detection of sleep apnea-hypopnea events for obstructive sleep apnea (OSA) diagnosis using a 60 GHz continuous-wave frequency-modulated radar combined with convolutional and recurrent neural networks. The dataset included 44 participants recruited between July 2021 and April 2022 who underwent overnight polysomnography (PSG) with a radar sensor. All PSG recordings, including sleep and wakefulness, were included in the dataset. The performance of the automated detection system was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC) for 1-minute segment classification, which ranged from 0.796 to 0.859. The AUC measures the classifier’s ability to distinguish between classes, in this case, segments with and without apnea-hypopnea events. An AUC of 1.0 indicates perfect classification, while an AUC of 0.5 suggests no better accuracy than random chance. Therefore, an AUC of 0.796-0.859 indicates good to excellent classification performance, suggesting that the radar-based system can accurately detect apnea-hypopnea events 0.929. 109
Then, in another study, SleepSmart, a smart sleeping enhancement system leveraging IoT and continuous learning from biometrics, was proposed. SleepSmart integrates wearable biosensors to collect physiological data during sleep, which is then analyzed by an IoT platform to generate personalized recommendations to optimize sleep. Through continual learning, the system refines its recommendations, enhancing accuracy over time. A pilot study involving human participants was conducted to assess the system’s efficacy, revealing significant improvements in sleep quality and reductions in sleep disturbances. The proposed SleepSmart algorithm achieved 98% accuracy, surpassing state-of-the-art algorithms such as SleepGuard, SleepSense, SleepGAN, and SleepEEGNet, reinforcing its ability to predict sleep quality and detect sleep-related disorders accurately. 118
In 2023, an IoT-based monitoring system was used to track essential health parameters and transmit data over a network. The study focused on remotely monitoring body temperature, heart rate, and SpO2 levels using sensors such as the DS18B20 and MAX30100. The patient’s position could also be retrieved on demand using the SIM7600E GSM and GNSS HAT Module. The Raspberry Pi 4B served as the microcontroller for gathering data from health parameter sensors. The collected sensor data were sent to cloud storage via a network, and a cross-platform mobile application with a graphical user interface (GUI) was developed to deliver real-time data to both medical professionals and patients. This system enables synchronous monitoring of a patient’s health status, empowering doctors to make timely medical decisions, including detecting sleep apnea events based on SpO2 levels. 119
Edge computing enables critical functions such as data collection and analysis to operate independently of a centralized server. In 2024, an IoT pulse oximeter was developed for medical institutions using edge computing, along with architecture for delivering real-time monitoring services. The system processes raw biosignals, such as pulse, and data from IoT pulse oximeters. Edge nodes are installed in each hospital ward to wirelessly gather, analyze, and monitor patient biosignal data. This data is then sent to the cloud for centralized management of all patients’ information. By enabling real-time collection and analysis of raw biosignals, the system supports an integrated management network connecting various IoT medical devices. This improves the efficiency of biosignal data collection and analysis for sleep apnea diagnosis by reducing delays associated with cloud computing and allowing real-time detection of sleep apnea events. 120
2.2.4.3. Antennas used as thoraco-abdominal movement sensors
Antennas can monitor thoracic motion by transmitting RF signals toward the chest and analyzing the reflected waves, which vary subtly as the lungs expand and contract; by tracking changes in resonant and scattering behavior, systems estimate breathing rate and detect irregularities such as apneas or hypopneas in real time. Advanced designs employ phased arrays to electronically steer the beam and isolate a target even amid other moving subjects, enabling non-contact, continuous respiratory assessment useful for sleep apnea monitoring.
Designed a vector patch antenna to detect respiratory movement without direct contact with the patient’s body. The vector antenna configuration comprises four patch antennas combined with a splitter (used here as a combiner), yielding improved gain and bandwidth. This vector antenna must improve its experimental sensitivity to better align with theoretical calculations. 121 Subsequently, implemented a radio frequency identification (RFID) sensor based on a slotted patch antenna, which changed its resonance frequency when subjected to specific deformation. This sensor was used to measure cracks smaller than 1 mm in civil structures by conducting mechanical traction experiments to demonstrate the correlation between deformation and changes in resonance frequency. Further, more exhaustive testing is required to improve the sensor’s performance in detecting cracks of varying sizes, necessitating increased sensor sensitivity. 122
During breathing, the human chest and abdomen undergo mechanical deformation and changes in RF properties. Inhalation primarily involves contraction of the diaphragm, which reduces intrathoracic pressure. This induces lung expansion during inspiration. Exhalation sees the relaxation of the diaphragm and intercostal muscles, restoring the chest and abdomen to a resting position. The tidal volume during normal breathing is generally estimated at 7 ml/kg of body mass, equivalent to a 7.37 cm chest circumference expansion in a 25-34-year-old male. 123 A possible way to detect breathing is by using a highly sensitive sensor capable of detecting both physical deformation and changes in dielectric properties. The study conducted a numerical analysis of human breathing to support experimental detection, and both results agree. Different breathing types: low, fast, regular, irregular, and shallow were successfully recorded within a frequency range of 0.16 to 1.2 Hz, resulting in a breathing frequency varying from 10 to 72 breaths per minute. 124
In 2019, an electromagnetic simulation of a system to detect upper-airway occlusion using a neck-conformal RF patch antenna and anatomical phantoms with realistic dielectric properties was presented, the model incorporated EM physics, cervical geometry, and RF safety verification via SAR. Specific Absorption Rate (SAR) is the rate at which RF power is absorbed by biological tissue per unit mass (expressed in W/kg), and it is used to ensure exposure remains within safety limits. The authors evaluated eight scenarios varying antenna orientation and standoff distance, comparing open versus occluded airway states; in all cases, distal-neck energy levels differed significantly (p ≤ 0.001), supporting the approach’s discriminative capability and its potential to identify the characteristic open-collapsed-open sequence of OSA events. However, the evidence is simulation-only (no bench or clinical validation), and diagnostic metrics vs. PSG/HSAT (e.g., sensitivity, specificity, AUC) are not reported; progression to bench and human studies is needed to set operating thresholds, obtain patient-level diagnostic metrics, and assess robustness/usability (posture, motion, anatomical variability) while maintaining SAR compliance. 125
While the previous system focused on detecting upper-airway occlusion through RF energy distribution and simulation-based discrimination of airway states, alternative wearable solutions have also been explored for unobtrusive respiratory monitoring. One such approach is based on tracking the movement of the chest or abdominal wall during inhalation and exhalation, which modulates the distance between a wireless reader and a planar spiral resonator (SR). In this device, the SR is placed on a thin, flexible textile substrate, allowing it to conform to non-planar surfaces, such as the human torso, and facilitating integration into clothing. The operating principle is based on tracking the movement of the chest or abdominal wall during inhalation and exhalation, which modulates the distance between the reader and the SR. The proposed device can measure breathing frequency by analyzing the modulated signal collected by the probe. The wearable respiratory rate sensor based on a planar spiral resonator (SR). The SR is placed on a thin, flexible textile substrate that enables the sensor to conform to non-planar surfaces, such as the human torso, making it suitable for integration into clothing. Respiratory frequency is obtained using the SR and a nearby wireless reader probe. The detection concept was verified through preliminary experimental measurements using a breathing simulator. The actual impedance at the probe terminals was measured at 294.5 MHz over the entire test duration (20 seconds). The impedance remained stable during the observation window, showing no significant variation throughout the measurement period. From this time-domain signal, it can be observed that the amplitude-modulated signal due to the movement of the water bottle (emulating breathing) was accurately recovered, clearly showing the measured impedance values relative to the extreme positions, around 145 when the normal distance between the SR and the probe, d, is minimal, and 70 at maximum d. Furthermore, the measured period equaled the input period (2.5 seconds). 126
Wearable medical devices have demonstrated that Silbione adhesive offers reliable adhesion and reusability, maintaining its adhesion strength after 7 days of use and multiple washing cycles. With a thickness of 250 μm, the adhesive maintained its adhesive properties with minimal degradation and exhibited low skin-electrode impedance, comparable to that of standard gel electrodes. Additionally, the signal-to-noise ratio (SNR) indicated sufficient signal quality for sleep monitoring, with successful clinical results at the Emory Sleep Center and in home-based tests, yielding measurements similar to those of traditional polysomnography. A neural network model was used to analyze sleep stages, showing high agreement with manual scoring and PSG measurements, further confirming the accuracy of the wearable system. These findings confirm that Silbione is a viable, reusable, and effective material for physiological monitoring medical devices.
In this study, 32 a contact-free Wi-Fi CSI system was built on ESP32 hardware to estimate respiratory rate (RR). They compared it against a respiratory belt (NUL-236) as ground truth. Agreement was evaluated using Bland–Altman analysis, showing validity within [1.06, 1.29] breaths/min across typical adult RRs; repeatability was assessed at 14 bpm by evaluating measurement spread and random error. The authors released paired CSI–belt datasets for validity/repeatability analyses. This supports the feasibility of RR monitoring, but it does not report PSG/HSAT-anchored OSA metrics (e.g., sensitivity/specificity/AUC), so its role in OSA screening remains under investigation.
In this work, 50 a wearable patch antenna sensor made of cotton/polyester (polycot) fabric was designed, and a flexible copper layer was modeled in CST Studio Suite to operate at 2.4 GHz in the ISM band for measuring respiratory rate via thoracic excursion. A thoracic anamnesis was conducted to validate the measurements manually. Results showed a linear, decreasing trend in the resonant frequency between 2.15 and 2.6 GHz (450 MHz bandwidth), with a sensitivity of −2.56 MHz/µϕ, inversely proportional to the applied effort. Placing the sensor on the lateral thorax enabled accurate detection of thoracic expansion, particularly in patients with obesity and respiratory conditions. These findings validate the wearable antenna as an innovative instrumental technique for measuring thoracic deformation, representing a step toward automating respiratory monitoring in smart biomedical devices. 50
3. Discussion
Based on the literature review, various techniques commonly used to detect thoracic deformation for sleep apnea monitoring were identified. Numerous published examples exist concerning contactless assessment of respiratory and cardiac frequencies. Contactless approaches show feasibility in small to moderate cohorts with variable agreement against PSG; however, evidence remains heterogeneous (sample sizes, severity mix, artifact handling), and home-readiness depends on validation under multi-subject, posture-changing scenarios. It is important to emphasize that new IoT and Machine Learning trends will enable the creation of portable, accurate, and more versatile technologies that link comprehensive datasets and connect them from anywhere in the world. One of the primary challenges is dealing with patient analog signals, where recognizing their behavioral patterns is essential. This allows the assessment of heart rate variability and chest expansion in “non-stationary” subjects, posing a more significant challenge in processing signals or noncontact Doppler radar systems.32,105,127 Alongside continuous advancements in non-contact physiological vital sign estimation, two key areas can be considered for contactless sleep monitoring: the Internet of Things (IoT) and Machine Learning.
Future research should expand to include noncontact assessment of heart rate and oxygen saturation, as well as sleep monitoring for “non-stationary” objectives and measurements of “not directly oriented” subjects. Additionally, pulse pressure, intrapulmonary pressure, tidal volume, minute ventilation, airflow, oxygen saturation, and Cheyne-Stokes patterns should be widely explored.68,128 It is recommended for future research to consider the complexity of the sleep environment, including noises associated with unpredictable body movements, body orientations, changes in sleep posture, multiple subjects, unwanted harmonics, and intermodulation. Advances in these areas will significantly contribute to the practical realization and commercialization of noncontact sleep monitoring and diagnostic technology.120,129
The integration of IoT technology into sleep apnea management requires a clear distinction between data-acquisition modalities to ensure clinical and technical accuracy. In this analysis, “recording” is defined as the acquisition of physiological data intended for post-hoc evaluation, whereas “monitoring” is reserved for systems that provide real-time analysis and feedback. This classification framework guides the subsequent evaluation of the evolving technological landscape and its impact on diagnostic pathways.
3.1. IoT in sleep apnea diagnosis: Real-time monitoring and analysis
Following the aforementioned distinction, real-time monitoring systems leverage IoT architectures to provide immediate physiological feedback, which is a critical requirement for detecting transient apnea and hypopnea events. However, deploying these systems in clinical environments faces significant technical challenges, particularly the heterogeneity of network protocols and the current lack of standardized architectures for medical data exchange.57,130,131 Furthermore, the continuous acquisition of high-resolution multi-parametric signals generates substantial data volumes; without robust analytical frameworks, this can result in processing delays or data loss, potentially compromising diagnostic accuracy. Consequently, the integration of scalable cloud infrastructures and edge-computing nodes is essential to manage computational loads and ensure the reliable dissemination of real-time alerts to healthcare providers.132,133
The detection of sleep apnea increasingly relies on integrating multiple sensing modalities, including SpO2, ECG, EOG, and EEG. In these frameworks, physiological data is acquired via specialized sensors and transmitted to cloud-based infrastructures, where advanced processing and classification algorithms facilitate the delivery of diagnostic reports to both clinicians and patients. This remote monitoring paradigm addresses critical accessibility gaps for populations in rural or underserved areas where traditional medical consultations are hindered by geographical distance and inconsistent internet infrastructure. While IoT-based systems offer portable, minimally invasive alternatives to conventional diagnostics, implementation costs currently limit widespread adoption. Within this architecture, machine learning algorithms serve as a high-precision analytical layer, enabling the identification of respiratory anomalies and the real-time dissemination of clinical data. By utilizing body-worn IoT sensors, these systems automate continuous monitoring and generate data-driven reports for medical oversight and familial awareness, offering a scalable solution for long-term sleep apnea management in remote settings.59,77,134–136
IoT and physiological variable classification algorithms for sleep apnea prediction.
The implementation of IoT systems for sleep apnea monitoring is fundamentally constrained by network heterogeneity and the absence of standardized architectures, which complicates seamless communication across diverse medical applications. Current deployments frequently rely on cloud-based centers that are susceptible to computational overload, increased latency, and potential signal degradation during the diagnostic workflow. To address these infrastructure vulnerabilities, research emphasizes an “ethical by design” approach that prioritizes user-configurable consent and direct visibility into algorithmic decision-making to enhance the security of the user-IoT relationship. From a deployment perspective, the feasibility of these integrated systems depends on the balance between initial capital expenditure and clinical scalability. While acquiring specialized hardware and establishing cloud infrastructure require significant upfront investment, these architectures facilitate a transition from hospital-centric diagnostics to scalable remote resource management. Beyond financial metrics, the technical efficacy of real-time monitoring is determined by the synchronization between sensor-level processing capacity and network stability, where the high-integrity transmission of biometric signals such as peripheral oxygenation
Furthermore, the efficacy of sleep apnea classification depends on data integrity, precise feature selection, and optimized detection thresholds. Variability in sensor quality and data interpretation can lead to inconsistent diagnostic outcomes, compromising treatment effectiveness and fostering mistrust among patients and healthcare professionals, potentially hindering the widespread adoption of IoT technology. This lack of reliability is compounded by the privacy and security risks associated with the collection of sensitive health information, necessitating robust cybersecurity measures to prevent unauthorized access or disclosure. Finally, the diversity of devices and platforms available on the market restricts interoperability and complicates the integration of data between different systems. This lack of standardization limits healthcare professionals’ access to comprehensive patient records, ultimately affecting the quality of clinical care coordination and decision-making for patients with sleep apnea.
3.2. Antennas for wireless sleep apnea monitoring
Radiofrequency techniques.
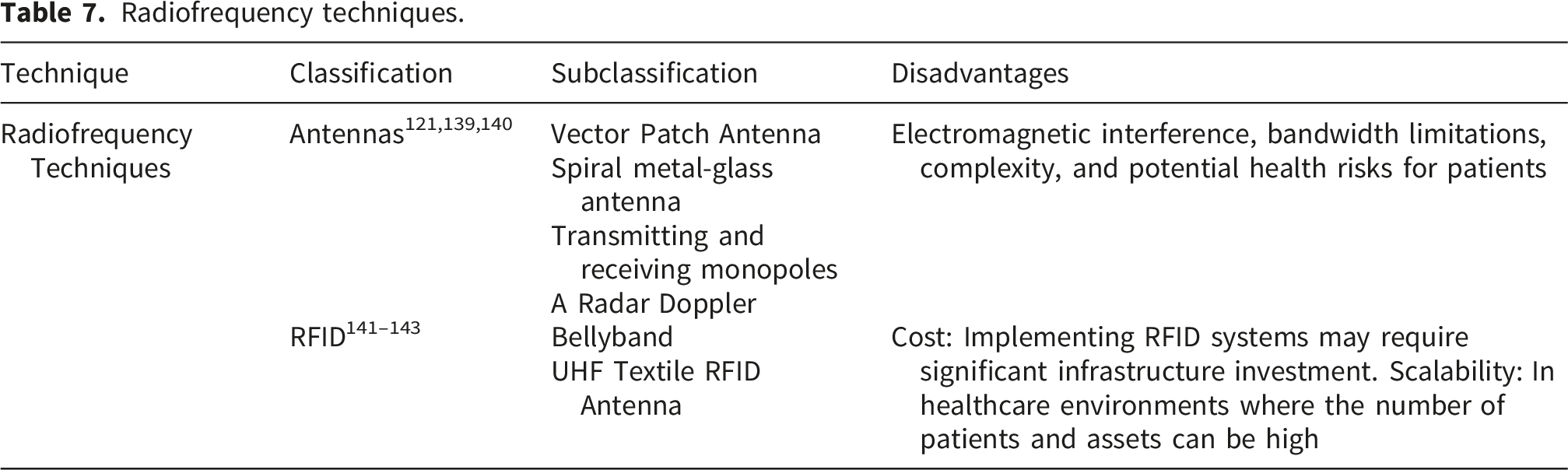
Sensors based on the Doppler effect (see Table 7) have been used in monitoring and diagnosing sleep apnea due to their ability to detect and measure body movements during sleep. The main advantages are shown to follow: ⁃ ⁃ ⁃
In terms of cost, Doppler radar sensors are more cost-effective than other techniques. This makes them more accessible for implementation in portable monitoring devices and large-scale diagnostic systems. However, Doppler effect sensors that detect body movements during sleep may be affected by various factors, potentially reducing their accuracy. For instance, they might struggle to distinguish between movements caused by sleep apnea and those that are normal. The accuracy of Doppler effect sensors can vary depending on their placement. The sensor’s position and orientation can influence measurement quality, necessitating careful positioning and proper calibration. These sensors focus on detecting and measuring body movements, which might limit their ability to provide detailed information about other physiological aspects relevant to sleep apnea diagnosis, such as breathing patterns or blood oxygen saturation.106,110,144
The use of Doppler techniques for monitoring sleep apnea has faced several significant challenges. One of the main issues is the limitation in detecting apnea events in real-time. Although Doppler techniques can provide valuable information about blood flow and respiration, accurately detecting apnea episodes can be challenging, especially during sleep when respiratory patterns can be irregular and variable. This limitation can affect the ability of Doppler-based monitoring systems to accurately identify and record apnea events, compromising the reliability of the obtained results.102,103 Another significant problem is external interference and noise that can affect the quality of measurements made with Doppler techniques. Doppler signals can be susceptible to interference from external sources, such as body movement or muscle activity, which can distort the collected data and hinder the accurate interpretation of results. This interference can generate artifacts in measurements, making it difficult to distinguish real apnea events from spurious signals and leading to incorrect or imprecise diagnoses. Additionally, the comfort and practicality of using Doppler techniques for continuous sleep apnea monitoring can be challenging. Doppler-based devices often require the placement of sensors or transducers on the patient’s body, which can be uncomfortable and restrictive, especially during sleep. This lack of comfort can affect the patient’s sleep quality and adherence to long-term monitoring, limiting the clinical utility of these techniques in managing sleep apnea.105,110 The antennas exhibited the following characteristics: they produced a strong, measurable response with resonant behavior sharp enough to detect deformation changes. When the antennas were in contact with the skin, they lost effectiveness and sensitivity. Moreover, the antennas used to sense thoracic deformation allowed for measuring fluctuations generated by respiratory movements and shallow and deep breathing.11,125,126
In the works121,126,143 studies with patch antennas made from flexible laminar dielectric substrates are referenced. These antennas were used as sensors to detect thoracic deformation induced by respiratory movements via dielectric substrate deformation. While these antennas are small and portable, they fail to adapt anatomically to the human body, adversely affecting the acquisition of physiological variables due to their high bioimpedance, leading to increased attenuation, reduced sensitivity, and significant loss of data, thus negatively impacting reliability.49,143,145
Therefore, it becomes crucial to delve into the design of patch antennas based on textile fiber substrates (wearables) that, by being able to anatomically adhere to various areas of the human body, even on the patient’s clothing, achieve the sensitivity required to obtain the maximum amount of information possible in the sensor’s deformation range.32,50 This guarantees optimal performance in sensing. Additionally, various technologies, such as patch antennas and IoT, are required to detect minute changes in chest box deformation caused by inhalation and exhalation. These technologies must be integrated to minimize the antenna’s coupling impedance. The data will be sent to a broker and then to the cloud, where it will be stored and interconnected with various mobile devices, aiming to create a portable device that can be used for multiple cycles and washes while ensuring result reliability.50,126,143
The use of wearable antennas and RFID tags for sleep apnea monitoring poses significant challenges, particularly regarding user comfort and usability. Although these devices promise non-intrusive monitoring, the need to wear them throughout the night can cause discomfort, especially if the design is not ergonomic enough or if the device interferes with natural sleep movements. This discomfort can negatively affect the quality of the patient’s sleep, alter the monitored sleep patterns, and skew the results. Long-term patient adherence to these devices is crucial for effective monitoring, and discomfort can lead to lower adherence.
Another significant issue is the accuracy and reliability of the data collected by wearable antennas and RFID tags. Since monitoring sleep apnea requires high precision to detect breathing interruptions, any limitations in the sensitivity and specificity of these devices can lead to incorrect diagnoses or missed apnea episodes. Environmental factors, such as electromagnetic interference from other electronic devices in the home, can also affect measurement accuracy. Moreover, body position and movements during sleep can influence the ability of antennas and RFID tags to collect consistent data, posing challenges in data analysis and interpretation.
Data integration and interoperability among different systems and devices represent a third challenge. Sleep apnea monitoring systems often need to work in conjunction with other medical devices to provide a comprehensive view of the patient’s health. The lack of uniform standards for communication and data exchange among wearable devices, RFID tags, and electronic health systems can limit the usefulness of collected data, complicating tracking, and analysis for healthcare professionals. This interoperability issue can hinder the widespread adoption of these technologies for sleep apnea monitoring, limiting their potential to improve diagnosis and treatment of the condition.
3.3. Optical fiber sensors for sleep apnea monitoring
Research on fiber optic sensors for respiratory monitoring.
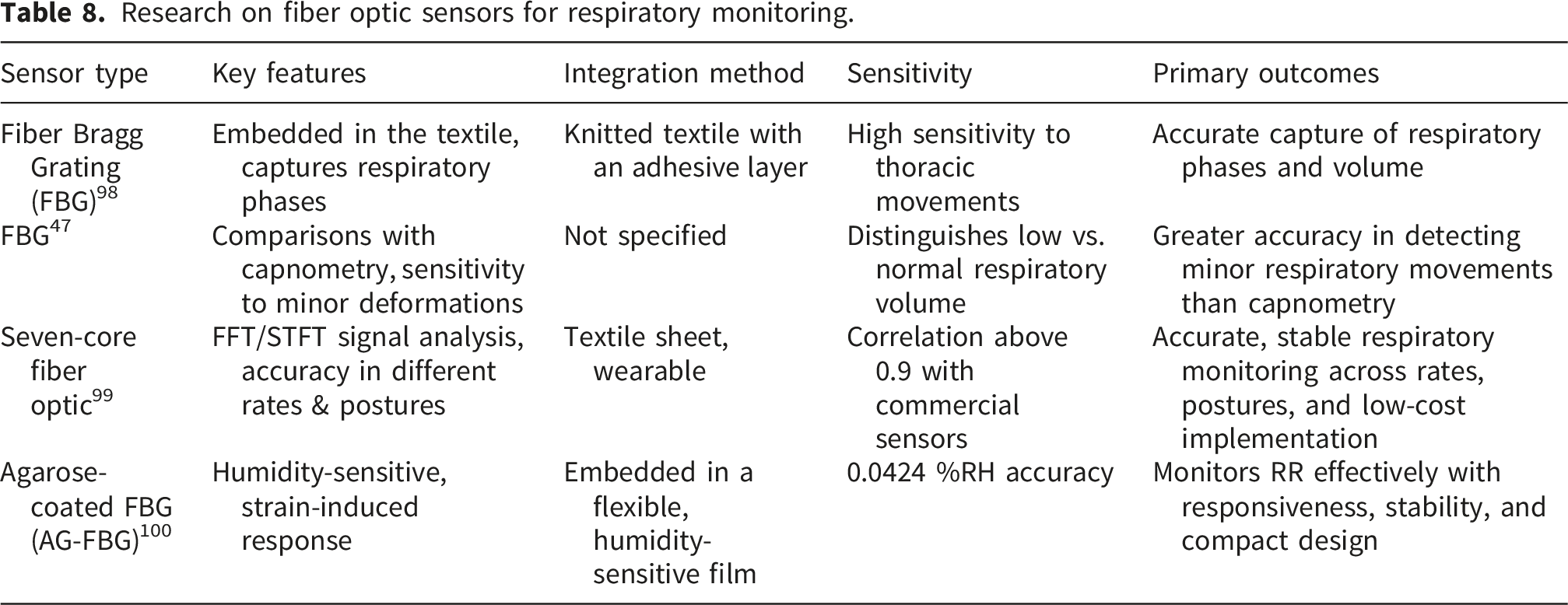
Optical fiber sensors have proven to be highly effective for monitoring biological parameters due to their high sensitivity, immunity to electromagnetic interference, and long lifespan. In the context of sleep apnea monitoring, these characteristics are essential as they allow for accurate and continuous measurement of respiratory movements in the thoracic and abdominal regions. Among these technologies, fiber Bragg gratings (FBG) have been extensively studied due to their ability to detect changes in the reflected wavelength in response to mechanical deformations, making them ideal for medical applications.94,95
Various studies have evaluated the integration of FBGs into smart textiles for non-invasive respiratory monitoring. For example, demonstrated the effectiveness of FBGs in transducing thoracic movements by incorporating them into an adhesive rubber textile layer, enabling precise capture of respiratory phases such as the respiratory period and inspiration/expiration duration. 98 Similarly, compared the performance of optical fiber sensors with conventional capnometry devices, concluding that FBGs can more accurately distinguish between low and normal respiratory volumes, reinforcing their potential in sleep apnea detection. 47
On the other hand, a seven-core optical fiber sensor was introduced, integrated into a wearable textile sheet. Their analysis of signals using the Fourier Transform (FFT) and the Short-Time Fourier Transform (STFT) enabled accurate detection of different respiratory frequencies and body postures. The study results indicated a high correlation (above 0.9) with commercial sensors and six-month stability with a frequency error of only 0.003 Hz, demonstrating the reliability and feasibility of these sensors for long-term monitoring applications. 99 Additionally, in other work, a humidity-sensitive sensor based on a Bragg grating coated with agarose (AG-FBG) was proposed, capable of recording respiratory rates with an accuracy of 0.0424 %RH. During experimental tests, response, and recovery times of 778 ms and 762 ms, respectively, were observed, confirming its ability to monitor breathing across different patterns and human postures with excellent stability and reproducibility.
Despite these advantages, integrating optical fiber sensors into smart textiles presents certain challenges. Their high sensitivity enables the detection of subtle deformations, enabling precise identification of abnormal respiratory patterns. Furthermore, their resistance to electromagnetic interference makes them ideal for clinical and home environments without compromising data quality. However, one of the main drawbacks is sensor durability when integrated into textile materials subjected to constant deformations. Factors such as body bioimpedance can also influence measurement accuracy, requiring fine-tuning of calibration parameters. Another aspect to consider is the manufacturing cost and complexity of the integration process, especially compared to conventional respiratory monitoring methods. Therefore, optical fiber sensors, particularly FBGs and their multicore or coated variants, represent a promising alternative for monitoring respiration in patients with sleep apnea. Their integration into smart textiles enables continuous and non-invasive monitoring with high precision and long-term stability. However, future developments should focus on improving sensor durability for prolonged use and validating their performance in clinical settings to ensure their applicability in diagnosing and treating respiratory disorders.
4. Open issues and conceptual roadmap
Despite significant advancements in IoT and non-contact sensing, a critical gap remains between experimental prototypes and clinically validated tools. To fully realize the potential of these emerging technologies as viable alternatives or complements to standard polysomnography (PSG), the research community must address several overlapping challenges. The following open issues outline the conceptual roadmap for transitioning these systems from bench studies to standard-of-care clinical practice.
4.1. Algorithmic robustness and clinical validation
• Handling Non-Stationary Signals in Real Environments: The most significant hurdle in processing signals from non-contact devices (such as Doppler radar) is recognizing physiological patterns in “non-stationary” subjects. Unpredictable body movements, changes in sleep posture, and environmental noises severely compromise data interpretation. Advancements in digital signal processing, specifically techniques to filter out unwanted harmonics, intermodulation, and movement artifacts, are mandatory to ensure diagnostic reliability. • Multi-site ML/DL Validation: Current machine learning algorithms often struggle with the complexity of sleep patterns and variations in respiratory signals when evaluated outside their training environments. Future work must transition from small, homogenous datasets to multi-site, diverse clinical validation. The incorporation of adaptive deep learning models capable of continuous feedback is essential to achieve the sensitivity and specificity required to rival Type-III HSAT devices, particularly in distinguishing central from obstructive events.
4.2. Hardware translation and real-time architectures
• Ergonomics and Signal Integrity: Wearable devices must balance patient comfort with strict signal acquisition requirements. Many existing systems remain intrusive, which artificially alter sleep architecture. The development of patch antennas based on textile fiber substrates presents a promising milestone; these allow devices to anatomically adhere to the body or clothing, reducing bioimpedance and minimizing signal attenuation without compromising the user’s natural sleep state. • Edge Computing Integration: The continuous monitoring of high-resolution variables generates massive volumes of data. While cloud computing offers robust storage, its inherent latency is incompatible with the need for real-time apnea event detection and immediate intervention. Transitioning towards efficient Edge computing architectures is a critical open issue. Processing data near the source not only eliminates cloud latency but also enables the creation of standalone devices that can operate in regions with limited internet infrastructure, significantly improving accessibility.
4.3. Data governance and system integration
• Interoperability: The lack of standardized communication protocols currently prevents the seamless integration of IoT sleep monitors into existing hospital electronic health records (EHR). Establishing universal data formats is a non-negotiable step to ensure that healthcare professionals can access and coordinate comprehensive patient care without being hindered by proprietary data silos. • Privacy and “Ethical by Design” Frameworks: The continuous transmission of sensitive physiological data introduces severe cybersecurity vulnerabilities. Transitioning prototypes to clinical use requires implementing secure, privacy-preserving data management frameworks that comply with strict healthcare regulations (e.g., HIPAA, GDPR). Furthermore, an “ethical by design” approach must be adopted, ensuring transparent data practices, patient autonomy, and configurable consent settings to mitigate the risks of unauthorized medical disclosure.
5. Conclusion
The evolution of sleep apnea diagnostics marks a shift from resource-intensive polysomnography toward portable biomedical systems, such as HSAT and SCOPER. While these modalities enhance patient accessibility, their clinical implementation remains limited by measurement sensitivity and signal stability during longitudinal monitoring. Emerging technologies, including fiber-optic sensors and radar-based radiofrequency techniques, offer non-contact alternatives, but their diagnostic reliability remains constrained by sensor displacement and motion artifacts. The integration of IoT frameworks with deep learning models, specifically convolutional neural networks (CNNs) and support vector machines (SVMs), has demonstrated potential to optimize event classification and improve cost-efficiency in remote settings. Textile-based patch antennas represent a viable sensing modality for tracking thoracic deformation, provided the signal loss that occurs when the sensor makes direct contact with the skin can be overcome through advanced materials and ergonomic design. Ultimately, transitioning these experimental prototypes into standard clinical practice requires a collective focus on refining sensor precision and optimizing algorithms for a wider range of patients. Addressing systemic constraints related to data governance, mitigating processing latencies through edge computing, and reducing environmental interference are critical steps to ensure the reliability and autonomy of modern sleep apnea management.
Footnotes
Acknowledgements
The author gratefully acknowledges Dr. Jorge Alonso Monsalve Jaramillo, Academic Vice Rector of the Institución Universitaria Salazar y Herrera, for the valuable support provided throughout the research process and for granting the time required to develop this article.
Ethical considerations
Ethical approval was not required for this study as it did not involve human participants, animals, or any procedures requiring ethical oversight.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed during the current study. Therefore, data sharing is not applicable to this article.
Use of generative AI declaration
The authors confirm that they used ChatGPT to correct typos, improve grammar, translate excerpts from Spanish, and enhance the readability of the manuscript. However, they state that the manuscript is original and that the improved texts generated by the language models have been carefully reviewed.