
Abstract
Background
Wearable devices present unique opportunities to gather behavioural and physiological data to augment digital health interventions for adolescents. However, the acceptability of these tools for mental wellbeing remains underexplored.
Objective
This systematic review synthesises existing research on the factors that influence the acceptability of wearable devices for adolescent mental wellbeing support.
Methods
Studies were included if they focused on participants aged 10-24, examined wearable devices for mental wellbeing, and presented acceptability-related outcomes. A search strategy was applied to five academic databases (Web of Science, PubMed, Scopus, Embase, and PsycINFO) up to April 11th, 2025. Study quality was appraised using the Mixed Method Appraisal Tool (MMAT). Results were synthesised narratively, with qualitative findings analysed using thematic analysis and quantitative findings summarised descriptively. This review was registered in PROSPERO (CRD420251118226) and funded by the Royal College of Surgeons in Ireland.
Results
Screening identified 19 studies with 1,055 total participants. Most studies were mixed methods (n=12), used wrist-worn devices (n=14), and measured heart activity (n=9). The main factors influencing acceptability included perceived effectiveness, device comfort, technical reliability, social acceptability, privacy and safety concerns, and contextual adaptation to different settings and participant needs.
Conclusion
The findings highlight that the acceptability of wearables is largely context dependent. Additionally, while wearables were noted to increase awareness and motivation, they could also amplify negative emotions which underscored a tension between the potential benefits and harms of wearables for adolescents. Limitations included heterogeneity in study design, variable reporting quality, and limited methodological consistency across studies.
Keywords
Introduction
Mental health challenges in adolescents have escalated throughout the 21st century.1–3 In particular, female adolescents have experienced increasing rates of internalising conditions, lower life satisfaction, and psychological distress compared to their male counterparts.3,4 The COVID-19 pandemic exacerbated these trends, which saw rises in depression and anxiety for youth globally 5 and in mental health-related emergency room visits in the United States. 6 These trends highlight the urgency of providing tools to promote adolescent mental wellbeing.
As adolescents increasingly use digital technologies, these tools present scalable approaches to support their wellbeing needs, such as online therapies or wearable devices for anxiety and depression treatment and monitoring.7,8 Wearable devices are digital tools that enable continuous, non-invasive physiological data collection. These devices show promise for several health applications, 9 including tracking and detecting mental health disorders.8,10 Biofeedback offers interventions focused on increasing self-awareness or altering real-time physiological data captured with wearables. 11
While wearables offer novel ways to promote adolescent wellbeing, these tools are rapidly evolving, and researchers must keep up with these advances to understand the potential impacts of these technologies. A critical gap exists in our current understanding of the factors that make wearables acceptable for adolescent cohorts. Adolescents face several barriers to benefit from existing digital technologies, including competition for screentime, privacy and safety concerns, and the rapid pace of technology development.12,13 This underscores the importance of evaluating the acceptability of the design and implementation of emerging wearable devices that target adolescent mental wellbeing to ensure that they are relevant, effective, and safe for young people. 13
Acceptability studies offer a method for assessing the perceptions and experiences of participants around the suitability of an intervention to their needs. 14 There are several models of acceptability such as the Technology Acceptance Model (TAM) that outlines factors related to perceived usefulness and ease of use 15 and the Theoretical Framework of Acceptability (TFA) which separates acceptability temporally into prospective, concurrent, and retrospective components. 16
Previous research has reviewed the acceptability of mobile mental health apps for adolescents based on usage and participant feedback, finding generally positive acceptance. 17 Another review summarised research on the application of wearables in educational settings, for both students and educators, highlighting the lack of user-experience feedback in the studies. 18 Although there are several reviews on the applications of wearable devices for adolescent preventative healthcare, such as physical activity 19 and sleep monitoring, 20 there are limited reviews of wearables as mental health interventions. For example, a review found that the majority of existing research on wearable device applications for adolescent health is focused on preventative healthcare and disease state monitoring. 21 Additionally, the reviews of wearable interventions mainly include outcomes for feasibility and effectiveness, rather than the acceptability of the underlying design or implementation of these systems.13,21 Despite the ubiquity of both adolescent mental wellbeing challenges and digital technologies, there remains a gap in existing reviews focused on the factors that influence the acceptability of wearable devices that offer support for adolescent mental wellbeing.
Therefore, this review aims to identify and synthesise existing research on the factors that influence the acceptability of wearables in supporting mental wellbeing in adolescents. In this review, we investigate the question: “What factors influence the acceptability of wearable devices for adolescent mental wellbeing?” This review contributes an overview of existing literature in the expanding area of wearable devices for adolescent mental health promotion.
Methods
We used the PRISMA 2020 checklist 22 when writing this report, which is provided in Appendix A. The study protocol was registered with PROSPERO (CRD420251118226).
Search strategy
A search strategy was developed in consultation with an RCSI librarian experienced with conducting systematic reviews. Five academic databases were searched: Web of Science, PubMed, Scopus, Embase, and PsycINFO. These databases were selected to capture a range of research across health and medicine, engineering, behaviour and social sciences, and humanities. The final search was completed on April 11th, 2025, with no restriction on publication date or language.
The search was constructed using the SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) framework 23 to capture quantitative and qualitative research designs. The search was conducted with terms from four categories: (1) adolescent populations, (2) wearable devices, (3) mental wellbeing, and (4) acceptability evaluations and assessments. Search terms were expanded using synonyms and MeSH terms when applicable, and reference lists from systematic reviews and included studies were hand-searched for study eligibility. The complete search strategy and results count for each database are included in Appendix B.
Eligibility criteria
Studies were eligible for inclusion if they: (1) focused on adolescents as the target population, aged 10-24 as defined by Sawyer et al., 24 (2) examined wearable devices used for mental wellbeing support, and (3) included either qualitative or quantitative acceptability-related outcomes such as participant interviews and intervention satisfaction questionnaires. Wearable devices were defined as technologies worn on the body to measure physiological or behavioural data such as heart activity, movement, and sleep. Mental wellbeing support included interventions for mental health conditions or psychological wellbeing such as stress management, anxiety, and depression. Studies were excluded if they only included measures of intervention effectiveness without acceptability measures which were defined as evaluations of user perceptions, experiences, or satisfaction towards wearable devices. Additionally, studies were excluded if they were review papers, conference abstracts, editorials, commentaries, opinion pieces, case reports, or study protocols.
Study selection and data extraction
Abstract screening, full-text screening, and data extraction were conducted in the Covidence review software. At abstract and full text screening each paper was independently screened by two reviewers, including a PhD researcher (J.L.) and one of two medical students (M.M. or R.R.). When conflicts were identified, the reviewers met to discuss these and to reach a consensus. Data extraction was conducted by two independent extractors for each paper (J.L. and M.M. or R.R.) followed by a consensus stage where data was consolidated for the final data extraction. The data were extracted using an extraction template that included study characteristics (author, year, country, design, duration, sample size, demographics), intervention details (intervention description, setting, wearable device, metrics measured), acceptability outcomes (qualitative themes and survey summary statistics), and recommendations from the authors in relation to acceptability.
Quality assessment
The 2018 version of the Mixed Methods Appraisal Tool (MMAT) 25 was used to assess the quality of the included papers in this review. Two reviewers independently assessed quality (J.L. and M.M. or R.R.), with disagreements resolved through discussion. The MMAT was used to provide a standardised appraisal tool for the diverse study designs anticipated in this review. It includes two screening questions and five criteria to assess study methodology which are tailored based on the study design (qualitative research, randomised control trials, non-randomised studies, quantitative descriptive studies, and mixed methods studies). The MMAT does not provide an overall score, so quality assessment summaries are presented in a summary figure and described narratively. The confidence in the results was determined by the quality of the included studies. Findings drawn from lower-quality studies were treated with appropriate caution, and their methodological limitations are noted in the results synthesis where relevant.
Data synthesis
Based on the heterogeneity of acceptability measures and studies, data were synthesised narratively in this review. Study characteristics and intervention details were summarised in tables. Quantitative acceptability outcomes were summarised descriptively. Meta-analysis was not possible due to the variability of data types. Qualitative findings were synthesised using thematic analysis. 26 The main acceptability themes identified in each paper were extracted by two separate reviewers during data extraction (J.L. and M.M. or R.R.). These themes were then deductively mapped independently by two reviewers (J.L. and R.R.) to the seven components of the TFA: affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness, and self-efficacy. 16 The TFA was chosen to guide our synthesis and organise findings across studies because it provides a robust framework to capture prospective and retrospective elements of acceptability for health and wellbeing interventions. Inter-rater agreement was calculated based on the percent agreement between labels and themes. The themes within each TFA component were described narratively to highlight patterns across studies.
Results
Study selection
The study selection process is outlined in the PRISMA flow diagram in Figure 1. There were 4,096 studies imported from the databases searched and one relevant reference found during citation searching. After duplicate removal, reviewers screened the remaining 2,650 studies. During title and abstract screening, 2,557 studies were removed based on not meeting one or more of the study inclusion criteria, requiring adolescent study populations, the use of wearable interventions, and acceptability-related outcomes. Additionally, results were removed at this stage if they were one of the predefined excluded study types. If there was insufficient detail to determine eligibility of studies based on the title and abstract, studies were retained for full-text screening. In this phase, 93 studies were reviewed and exclusion reasons were recorded. Of these studies, two were not retrieved despite contacting the corresponding authors.27,28 The most common reason (n=31) for paper exclusion was the age of the study participants falling outside of the age range set for inclusion of 10-24.
24
Two papers were included that had an age range of 15-25 and 18-25 because the studies focused on adolescents and included a majority of participants aged 10-24.29,30 Other papers were excluded based on missing acceptability outcomes, lack of reported data, being a design outlined in the exclusion criteria, and not including a focus on wearable devices or mental wellbeing. The study selection process resulted in 19 studies for inclusion in the review, amounting to 1,055 total participants.29–47 PRISMA study selection flow diagram.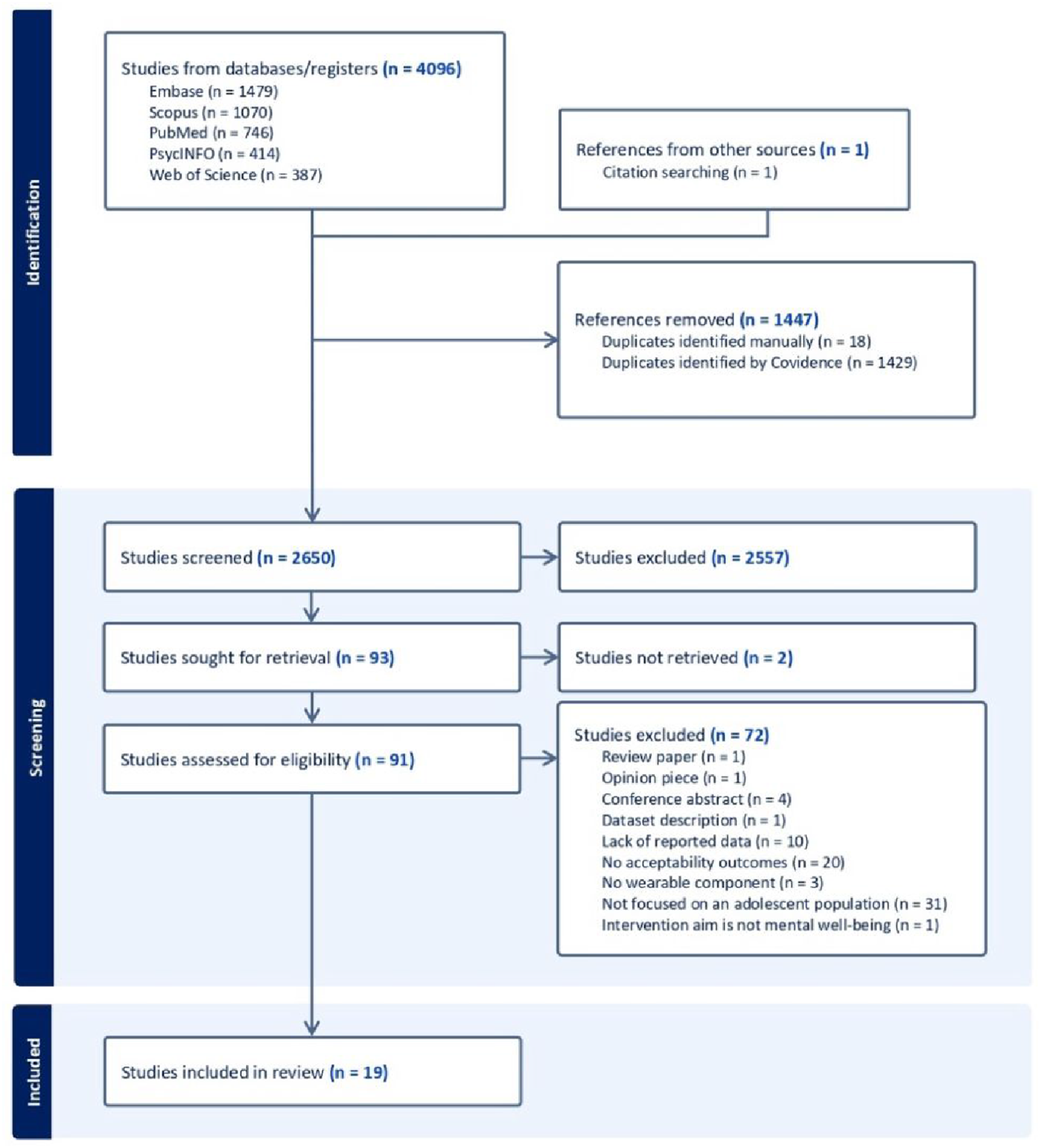
Study characteristics
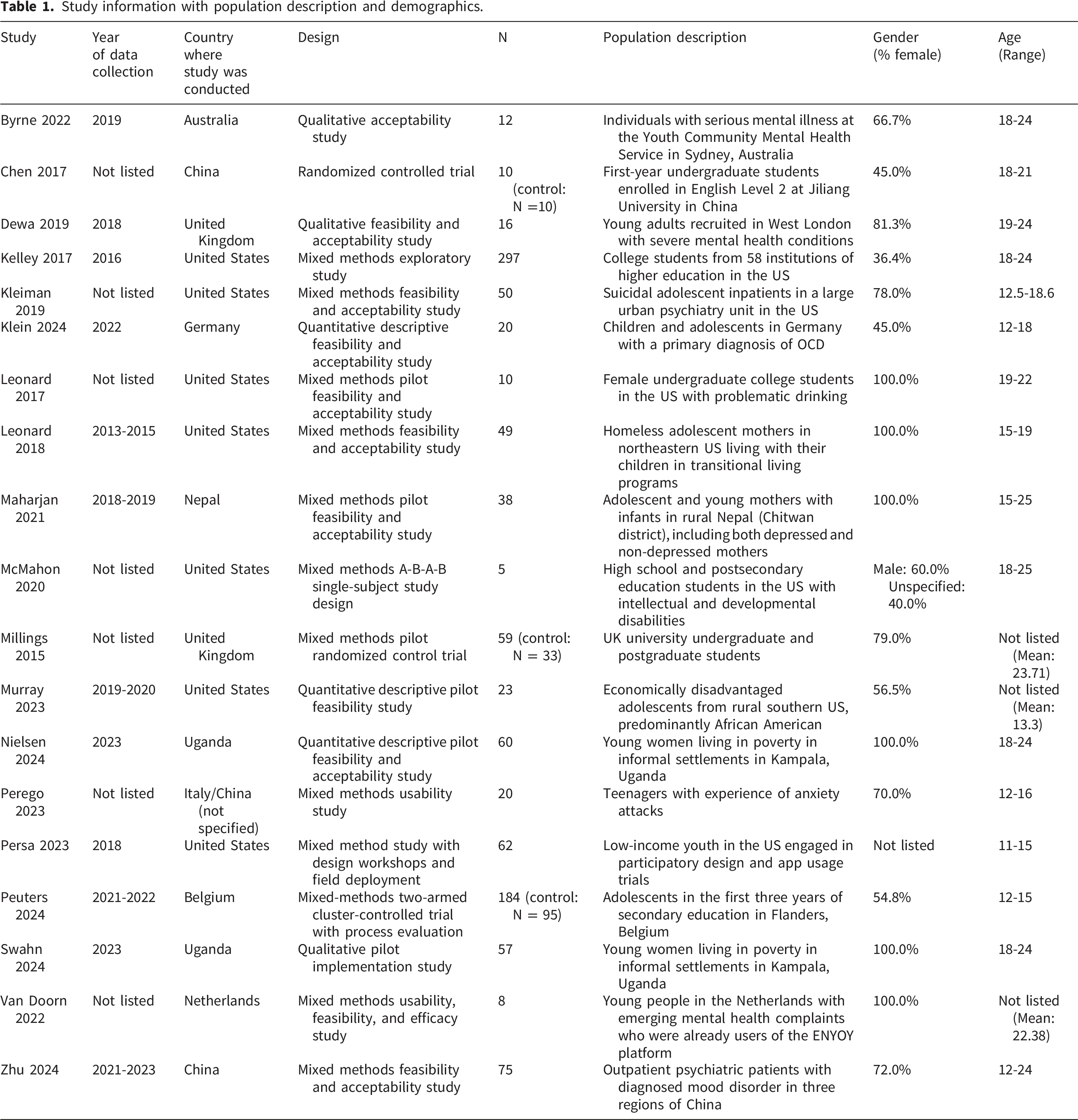
Study information with population description and demographics.
Intervention details, including the study duration, setting, wearable used, signal measured, use of incentives, and adherence metrics.
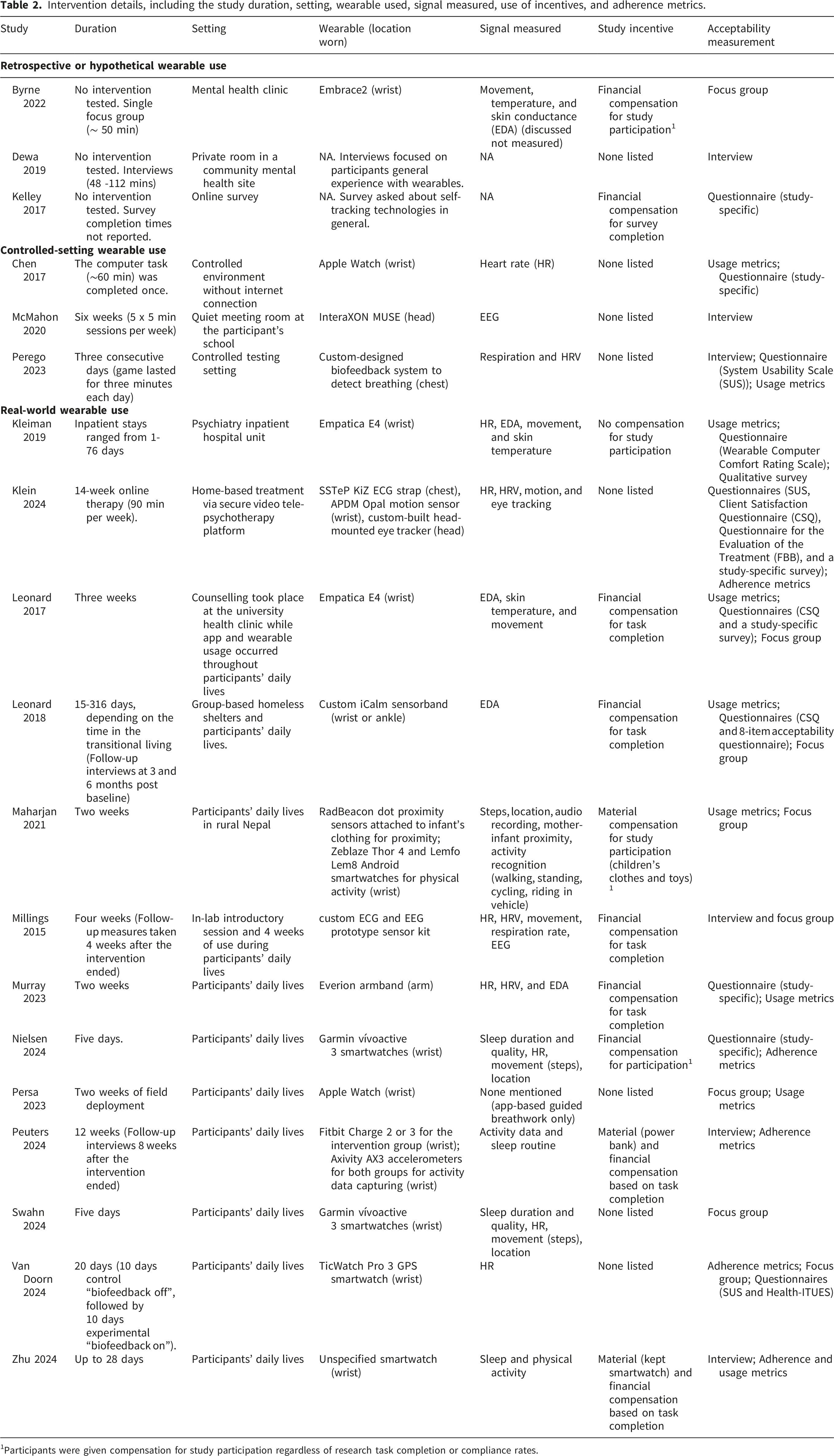
1Participants were given compensation for study participation regardless of research task completion or compliance rates.
These studies were published between 2015 and 2024 with data collection reported between one and five years prior to paper publishing (Table 1). The studies took place in the United States (n=7), China (n=2), Uganda (n=2), the United Kingdom (n=2), Australia (n=1), Belgium (n=1), Germany (n=1), Nepal (n=1), and the Netherlands (n=1). One study was conducted by Italian and Chinese researchers, but the location where the study took place is unclear. 43 The majority of study designs were mixed methods (n=12), followed by qualitative research (n=3), quantitative descriptive studies (n=3), and a randomised control trial (n=1).
Two studies reported independent outcomes related to adult cohorts alongside adolescent participants.31,34 Kelley et al. 34 gathered feedback from healthcare professionals in the first phase of the study and experiences of college students in the second phase. Byrne et al. 31 gathered acceptability feedback from clinicians and adolescent patients. The outcomes related to the adult cohorts in these studies were excluded from the population characteristics and results reported in this review.
Nielsen et al. 41 and Swahn et al. 42 report on the same study, outlining the quantitative and qualitative outcomes separately. Leonard et al. 2017 37 and 2018 38 are two distinct studies included in this review.
Regarding the participant populations, the number of intervention participants ranged from 5-297 with a median of 38. Three studies32,39,45 included control groups with 10, 33, and 94 control participants. The age ranged from 12-25 years. Six studies29,37,38,41,42,46 included all female participants, while two studies30,44 did not specify the gender of all participants. In the eleven studies with both male and female percentages reported, the percent of female participants ranged from 36.4-81.3% with a mean of 62.2%. The studies focused on adolescents who were students (n=6), diagnosed with a specific mental health condition (n=6), economically disadvantaged (n=5), patients in clinic or hospital (n=2), or adolescent mothers (n=2). The populations that were selected based on mental health conditions included adolescents with suicidal ideation, 35 anxiety, 43 mood disorders, 47 depression, 29 and general serious mental illness diagnoses.31,33 Additionally, two studies included neurodivergent populations of adolescents with obsessive compulsive disorder 36 and students with autism spectrum disorder and down syndrome. 30 Economic disadvantage was based on various conditions including household income levels, 40 school socioeconomic classifications, 44 and physical locations within low-income countries.29,41,42 Other information reported about participants in several studies included ethnicity, technology access, and education level.
The studies included a range of intervention types (Table 2), grouped into retrospective or hypothetical wearable use, controlled-setting wearable use, and real-world wearable use. Two studies33,34 gathered feedback about participants’ previous experiences with wearables and self-tracking technologies for mental wellbeing. Byrne et al. 31 presented participants with an overview of the Empatica E4 wearable and asked about hypothetical perceived benefits, barriers, and facilitators to using the device for stress management. Three studies30,32,43 included wearable interventions that were facilitated by researchers in a controlled setting for 3 to 60 minutes. The remaining thirteen studies included wearables that were used throughout participants’ daily lives, lasting from 1-316 days. Wearable devices were most often worn on the wrist (n=14), followed by the chest (n=2), head (n=2), and arm (n=2), with one wristband also able to be worn on the ankle. Four of the devices used were custom developed devices, one device was unspecified, and the remaining were commercial wearables such as the Apple Watch, Garmin Vivoactive 3, and the Interaxon Muse. The three most common physiological metrics collected were calculated based on heart activity (n=9), physical activity (n=8), and skin conductance (n=5). Financial and material compensation for participants were detailed in ten papers, three of which were given for study participation, regardless of intervention usage, while the rest depended on participant compliance to study tasks. Eight other studies did not mention participant incentives and one specified that there was no compensation for participants. Intervention acceptability was evaluated qualitatively, using focus groups (n=7), interviews (n=7), and open-ended surveys (n=2), and quantitatively through questionnaires (n=10).
Quality assessment
Quality assessment using the Mixed Methods Appraisal Tool (MMAT).
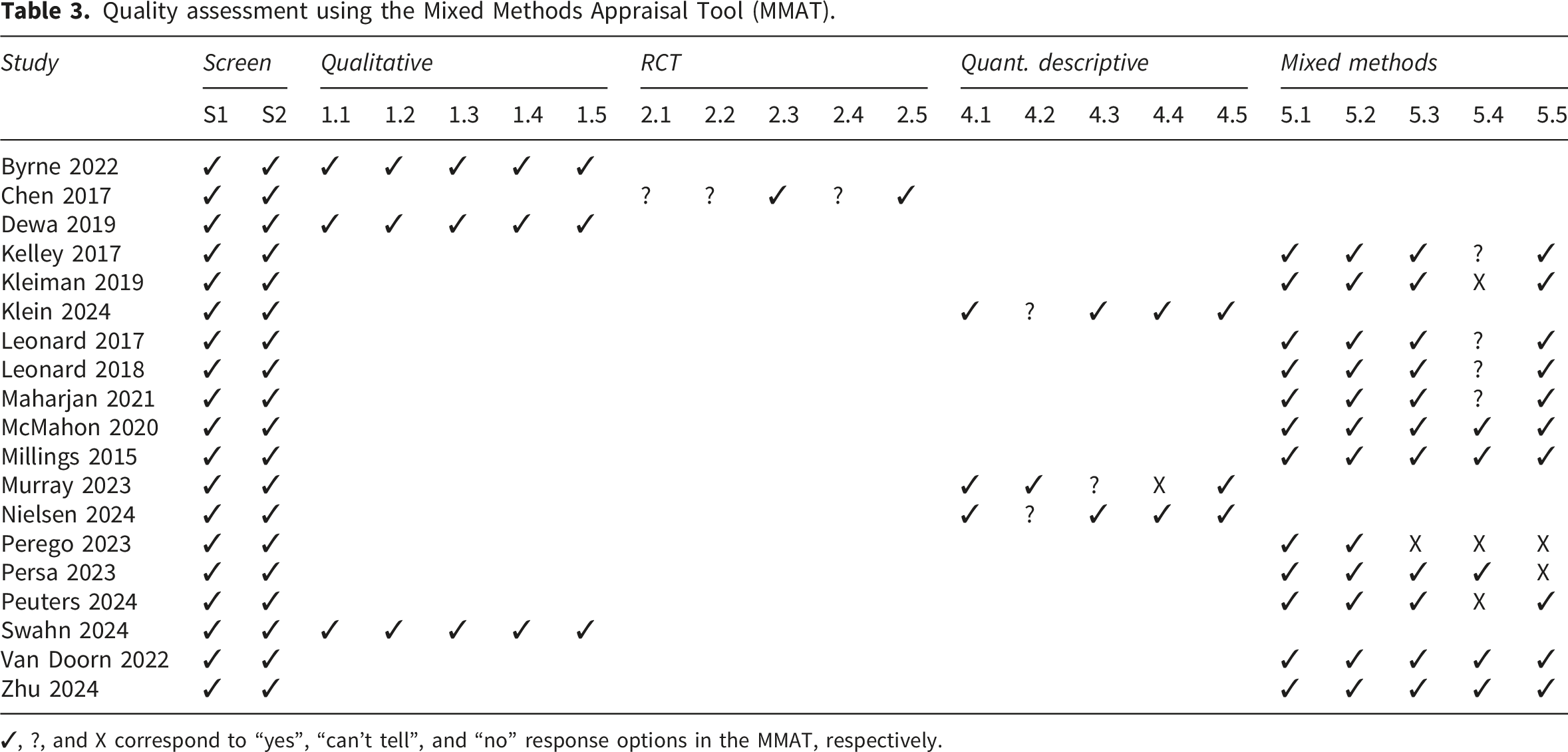
✓, ?, and X correspond to “yes”, “can’t tell”, and “no” response options in the MMAT, respectively.
Study results
Acceptability outcomes reported in each included paper.
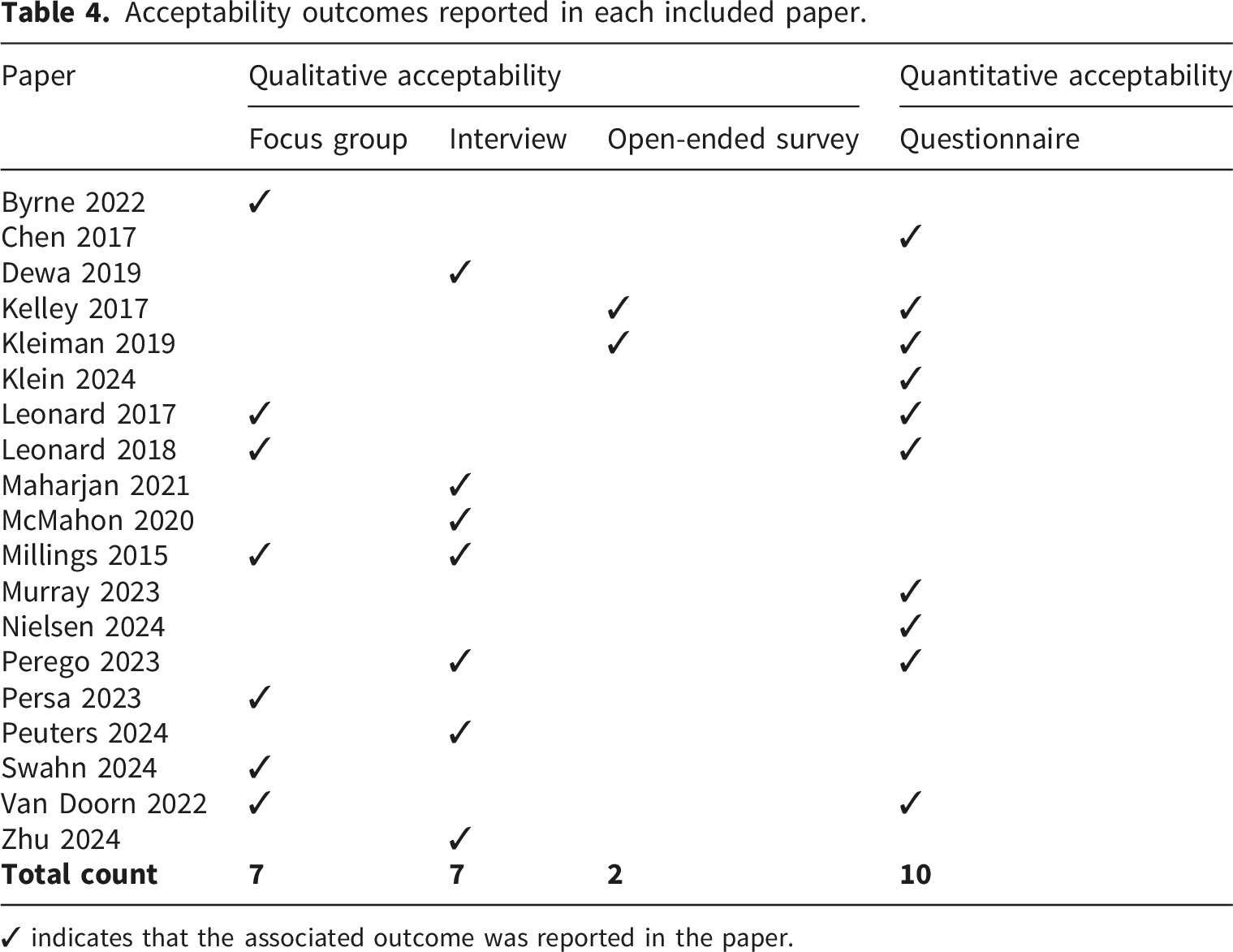
✓ indicates that the associated outcome was reported in the paper.
Qualitative
The data extracted from the qualitative study articles included 181 sub-themes which were grouped into 24 themes and independently mapped to the categories of the TFA by two authors (J.L. and R.R.). The TFA categories with the most studies were affective attitude (n=14) and perceived effectiveness (n=14), while intervention coherence (n=6) and opportunity cost (n=7) had the lowest number of studies. Seven sub-themes were marked as not applicable to acceptability, and all themes were captured by a TFA category. The complete list of extracted themes with associated TFA component labels is included in Appendix D. The percent agreement between the two authors (J.L. and R.R.) on at least one TFA category assigned to the extracted themes was 72.8%. Figure 2 demonstrates the categories of themes in each group across the studies, with certain themes connecting to multiple categories. Qualitative data themes grouped by category of the TFA with lines connecting TFA components to the acceptability themes. Each category label includes the number of studies that included related subthemes (ns) and the total number of subthemes grouped in each category (nth).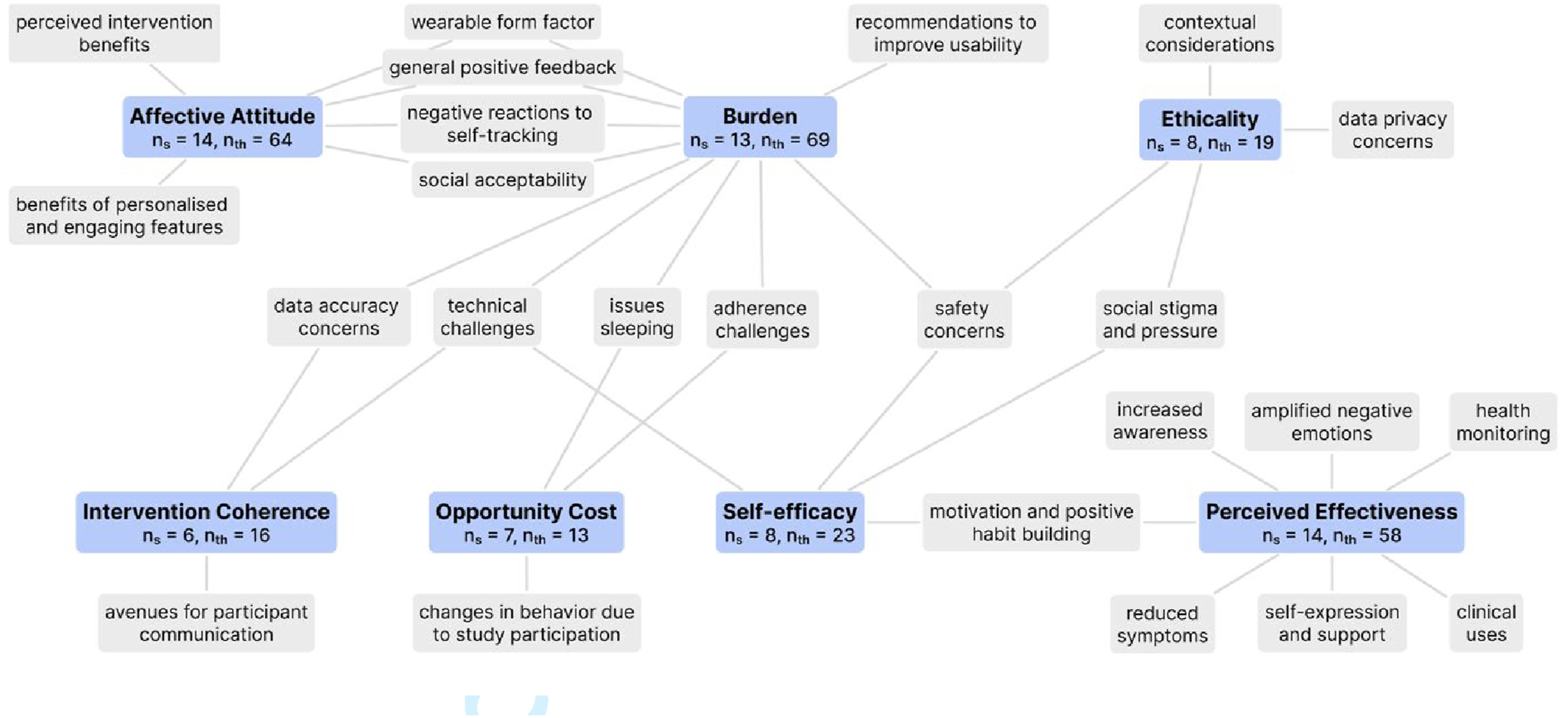
Affective attitude
Affective attitude refers to feelings that someone has about an intervention, oftentimes before engaging with it. 16 Fourteen studies included sub-themes which were categorised under this TFA component, with a total of 64 sub-themes. These were grouped into six themes: (1) perceived intervention benefits, (2) benefits of personalised and engaging features, (3) wearable form factor, (4) wearable social acceptability, (5) negative reactions to self-tracking, and (6) general positive feedback. The latter four categories overlapped with themes identified in the Burden category which is discussed separately with the general positive feedback theme.
Perceived intervention benefits: Participants across studies noted prospective optimism about how wearable devices could support them. For example, a participant in Byrne et al. 31 highlighted the potential benefits of self-tracking to “identify a trigger or something you might not have known before” (Participant 7, Byrne et al. 2022) to help them gain insights into their mental health. Several other participants described specific perceived impacts after using wearables which are discussed further in the perceived effectiveness category.
Benefits of personalised and engaging features: Participants valued interventions that could adapt to their individual needs and preferences. In Van Doorn et al., 46 participants had individual preferences for an appropriate amount of biofeedback interventions and felt that the intervention exercises should be short, practical, and adapted to their needs. Participants in Byrne et al. 31 shared the influence that engaging features and wearable form factors would have on the intervention acceptability. One participant stated that “if it’s comfortable using it and easy to use it, [they] would use it” (Participant 10, Byrne et al. 2022).
Wearable form factor: General discomfort from wearable devices was noted in seven studies.29,35,37,38,42,44,46 In Van Doorn et al., 46 participants noted discomfort with the device’s appearance and the feeling when worn. One participant noted that for them, “the watch was quite big, as [they] have small wrists” (Participant 5, Van Doorn et al. 2022). Mixed reactions to the wearable appearance were noted in four studies.35,38,44,46 For example, Kleiman et al. 35 described how some participants liked the wearable appearance while others felt it was too big.
Wearable social acceptability: The device appearance could impact social acceptability, or how the wearable was perceived by peers or community members and how it affected social interactions. Appearance of devices was noted as positive in some cases, such as in Persa et al. 44 where student participants saw the Apple Watch as a fashion statement and marker of status. However, this study had notable quality concerns around minimal methodological detail. 44 In Swahn et al., 42 participants also noted that the Garmin smartwatches were a status indicator, although they elicited unpredictable, and often negative, reactions from community members.
Negative reactions to self-tracking: Participants in five studies34,37,44,46,47 described negative reactions to biofeedback, such as amplified negative emotions and inopportune timing or unhelpfulness of alerts. In Kelley et al., 34 over one third of participants indicated feeling that self-tracking data reflected something negative about them. They found that participants often experienced a disconnect between how they felt and what the data presented. One participant who had difficulties losing weight noted that they “started questioning [their] physical health and wondering if there was anything wrong with [their] body” (Participant 228, Kelley et al. 2017) because of their self-tracking data.
Burden
Burden refers to the factors that increase or decrease the challenges related to engaging with an intervention. 16 Thirteen studies included sub-themes which were grouped under this category, with a total of 69 sub-themes. These were grouped into ten themes: three have been discussed above (wearable form factor, negative reactions to self-tracking, and social acceptability), four will be discussed in other sections (issues sleeping, adherence challenges, data accuracy, and safety concerns), and three are discussed below: (1) general positive feedback, (2) recommendations to improve usability, and (3) technical challenges.
General positive feedback: One theme that emerged was general positive feedback from participants about the minimal challenges engaging with interventions. In McMahon et al.,
30
for example, students shared that the MUSE was easy to use, they would recommend it to other students, and they found it helpful in facilitating mindfulness sessions. Similarly, participants in Millings et al.
39
evaluated the “Optimise Me” programme and noted enjoying biofeedback exercises with one participant sharing: “Yeah, they were a lot of fun. I really liked the EEG thing, it was so cool. I actually did it in front a couple of my friends and they thought it was cool as well.” (Participant 55, Millings et al. 2015)
Recommendations to improve usability: Another theme was participant suggestions aimed at increasing the ease of use and usefulness of interventions. In Van Doorn et al., 46 participants offered several recommendations to improve the usability of the intervention such as having reminder notifications for engagement and centralising the intervention in one app. Participants in Kleiman et al. 35 noted that the wearable should have a clock. Additionally, several sub-themes overlapped with those previously discussed in the “benefits of personalised and engaging features” theme.
Technical challenges: A substantial burden frequently noted in the studies was difficulty with the intervention technologies. Four studies29,37,38,46 had qualitative themes related to issues with charging or battery life. Van Doorn et al.
46
included one participant who shared that the complicated login process kept them from engaging with the ENYOY platform. Other participants of this platform described challenges with the app interface and wearable battery life running out. In Leonard et al. (2018),
38
participants had difficulty integrating the device into their daily routine and knowing when the device was charging. Several participants in Millings et al.
39
also noted how technical challenges interfered with the ease of use: “When you can’t get the signal and you can’t do it in the first place that’s really annoying, and it can end up being very time consuming.” (Participant 39, Millings et al. 2015)
Ethicality
Ethicality refers to the alignment of the intervention with the values of the participants. 16 There were 8 studies and 19 sub-themes grouped under this component, which were further grouped into four themes: (1) contextual considerations, (2) data privacy concerns, (3) safety concerns, and (4) social stigma and pressure.
Contextual considerations: Participants across studies emphasised the importance of considering local contexts when designing and implementing wearable interventions. In Maharjan et al.,
29
this was underscored by the participants’ appreciation of frequent communication with researchers. The researchers in Maharjan et al.
29
also collaborated with local health clinics to adapt their protocol. Dewa et al.
33
discussed participants’ general concerns and values related to technology, outlining potential benefits such as anonymity and accessibility. These participants also highlighted pragmatic concerns around placing more responsibility on patients and relying on WiFi or battery: “If you can get technology which will say something is going wrong with them, then yes I mean I think technology is the ideal way to monitor . . . [but] You see, the thing about having a mental health disorder is that you are already not mentally healthy. Expecting a person who is not mentally healthy to then also monitor themselves and their disorders is a bad idea” (Participant 13, Dewa et al. 2019) “If that person was in a crisis and then your battery dies or something, then they’re by themselves again” (Participant 19, Dewa et al. 2019)
Data privacy concerns: Privacy emerged as an ethical concern across four studies29,31,42,47 with relation to surveillance and data misuse concerns. Notably, the settings and purpose of the wearables vary widely across these studies (Table 1) including, adolescent mothers in rural Nepal monitored for proximity to their children, mood tracking in psychiatric outpatients in urban China, wearable use among women in informal urban settlements in Uganda, and young adults with serious mental illness discussing physiological stress monitoring in Australia. While privacy concerns are shared across these contexts, they manifest differently depending on the application and setting. For example, in Maharjan et al.,
29
several participants worried about the potential use of audio recordings from the devices in private spaces, with one mother stating: “I like using the devices but I feel worried because you might know all our family matters and our conversations.” (Maharjan et al. 2021)
Similar concerns about surveillance were marked by participants in Byrne et al.,
31
Swahn et al.,
42
and Zhu et al.
47
One participant in Byrne et al.
31
sharing: “Personally, I get really paranoid about a lot of things. I don’t like people watching me… my concern would just be: are they doing more than what they told? Are they tracking your heartbeat going up and then you feel paranoid?” (Participant 10, Byrne et al. 2022)
Safety concerns and social stigma and pressure: The visibility of wearables created complex social dynamics, sometimes leading to participant concerns about their safety. Physical safety concerns were mainly reported in studies conducted in low-resource communities. In Swahn et al., 42 the women reported experiencing several reaction and unexpected questions about the device from community members. These interactions caused some participants to worry about losing the device or getting it stolen. Participants also noted the social status that the watch gave them describing how they would get “showered with praises for looking smart while walking around with [the device]” or get nicknames at home: “they have been calling me ‘rich woman’.” The community reactions led to increased speculation from participants about the safety and privacy concerns such as potential diseases or audio recording from the device. To reduce questions and community reactions, participants in the first pilot noted covering their devices with fabric. Because of this, all participants in the second pilot were given a fabric bracelet to cover the device.
Intervention coherence
The ability of participants to understand the intervention is referred to as intervention coherence. 16 In this review, there were 16 themes from 6 studies grouped under this component of the TFA. The three categories of themes included (1) data accuracy concerns, (2) avenues for participant communication, and (3) technical challenges. Technical challenges that hindered participants’ understanding were discussed previously in the Burden category.
Data accuracy concerns: Concerns about the accuracy of wearable data emerged as a barrier to engagement across three studies,42,46,47 often leading to mistrust or confusion during interventions. For example, participants in Zhu et al.
47
shared concerns around the accuracy of wearable sleep and activity measurements, with 32.2% of participants stating that assessments were not accurate representations of how they felt. In Van Doorn et al.,
46
most participants (5/8) also expressed doubts in the accuracy of stress detection metrics, with one participant sharing: “Sometimes I got a notification while I was sitting still, it said that my heartbeat was too high and I thought ‘That’s weird’, because I wasn’t doing anything stressful. There was also a situation in which I was stressed but I didn’t see that on the watch” (Participant 6, Van Doorn et al. 2022)
Avenues for participant communication: Another important component of intervention coherence was the establishment of an avenue for questions from the study participants. As discussed previously, the participants in Maharjan et al. 29 noted appreciating the availability of the research team to answer questions and assist throughout the study. Peuters et al. 45 offered a chatbot which participants highlighted as an engaging feature that they mainly used to ask questions about the functionality of the app.
Opportunity cost
The opportunity cost encompasses themes related to how suitable the intervention was for integration into participants’ daily lives. 16 There were 13 sub-themes across 7 studies that were included in this TFA category. The three themes were (1) issues of sleeping or sleeping difficulties, (2) adherence challenges, and (3) changes in behaviour due to study participation.
Issues of sleeping or sleeping difficulties: While wearable discomfort was noted across multiple studies, participants in Kleiman et al.
35
and Swahn et al.
42
specifically noted issues sleeping while wearing a smartwatch. One participant in Kleiman et al.
35
shared that the device “was uncomfortable during sleep” which was expressed by 11% of participants in qualitative feedback. In addition to device discomfort, participants in Swahn et al.
42
indicated that the light emitted by the PPG sensor on smartwatches interfered with sleep for both them and others in the room. “I sleep with my younger sister, now at night she would wake up and call me to remove my watch, because it was lighting” (Swahn et al. 2024)
Adherence challenges: Additionally, there was feedback across three studies about challenges integrating the intervention into participants’ daily lives.38,46,47 Leonard et al. (2018)
38
described how participants found that night-time reports fit in well to their daily lives, while general smartwatch use during the day was challenging due to the numerous responsibilities of adolescent mothers. “I don’t have any time. I’m always like, doing something and then when I get home I’m always doing something, for my son or like my boyfriend or something...” (Participant 228, Leonard et al. 2018)
Both Van Doorn et al. 46 and Maharjan et al. 29 described that participants found it difficult having to carry both their personal phone and a research-specific phone.
Changes in behaviour due to study participation: Maharjan et al. 29 and Swahn et al. 42 also reported feedback from participants that they changed their behaviour because of their awareness that they were part of a research study. This is distinct from habits and behaviours that may have been encouraged because of the intervention which will be discussed later. For example, participants in Swahn et al. 42 shared that they reduced their daily activity during the intervention due to concerns related to privacy, losing the device, or social judgement. On the other hand, 60% of participants in Kleiman et al. 35 described that being part of a research study was a motivator for engaging with the intervention because they “felt [they] were helping.” This may also have influenced participants to change their behaviour because they were part of a research study.
Self-efficacy
Self-efficacy refers to the confidence of participants in their ability to complete the tasks associated with the intervention on their own. 16 There was a total of 23 sub-themes grouped in this TFA category, representing 8 studies. The four themes were (1) technical challenges, (2) safety concerns, (3) social stigma and pressure, and (4) motivation and positive habit building.
All four themes overlap with other TFA categories, and the first three themes were discussed above. As noted previously, social pressures, safety concerns, and technical challenges were commonly shared barriers to engaging with the intervention that either added burdens for participants, conflicted with their ethical values, or made the technology difficult to use or understand. These barriers also contribute to the ability of participants to confidently engage with an intervention. Swahn et al.
42
detailed how participants received many questions about their smartwatch from the members of their community, and they feared robbery. Similar fears of breaking the device, losing it, or getting it stolen were mentioned in Persa et al.
44
and Maharjan et al.
29
Participants in these studies also described challenges charging and working their devices. The student participants in Leonard et al. (2018)
38
emphasised social reactions to the device by their peers such as questioning whether it was a legal monitor or probation bracelet while other reactions were more positive: “Um, they thought it was interesting and kind of...a few people wanted to participate in it...and others were like...oh, that’s pretty cool...” (Participant 231, Leonard et al. 2018)
Motivation and positive habit building: The included studies demonstrated that using wearables for behaviour tracking can act as a motivator to engage with the intervention and build positive habits. Zhu et al. 47 noted that participants felt “a flame of hope” and clearer goals because of biofeedback and all of them tried to change their behaviour because of it. Similarly, Peuters et al. 45 stated that self-tracking acted as a motivator and triggered participants to change their behaviour. Swahn et al. 42 detailed that, in addition to acting as a motivator, the wearable device gave participants a positive sense of responsibility. Kelley et al. 34 shared participant feedback on self-tracking data which acted as a motivator for participants to set goals and maintain healthy habits to help mitigate anxiety and stress. In Kelley et al., 34 one participant explained that “tracking strength growth encourages [them] to continue working out, which in turn mitigates the anxiety/stress,” (Participant 238, Kelley et al. 2017) while another tracks “exercise, sleep, and caffeine intake to minimise triggers [of anxiety]” (Participant 127, Kelley et al. 2017).
Perceived effectiveness
The final component of the TFA is perceived effectiveness, or the participants’ subjective experience of the impacts of the intervention. 16 There were 58 sub-themes from 14 studies that were grouped under this category. Motivation and positive habit building was the only overlapping category and was previously discussed in the Self-efficacy category. The remaining six themes that emerged were (1) increased awareness, (2) amplified negative emotions, (3) health monitoring, (4) clinical uses, (5) reduced symptoms, and (6) self-expression and support.
Increased awareness: Ten studies included themes that described an increased awareness of symptoms, behaviours, or feelings as an outcome of wearable device use.29,30,33–35,37,38,45–47 Dewa et al.
33
and Kelley et al.
34
highlighted how self-tracking can help people understand the relationships between their behaviours and mental health status. Participants in Leonard et al. (2017)
37
experienced a greater awareness of the connection between their feelings, physical status, and alcohol use, with one describing that the smartwatch “made [them] realise how [their] body reacts to mood change” (Participant 303, Leonard et al. 2017). Similarly, participants in Leonard et al. (2018)
38
and Van Doorn et al.
46
reported that they were encouraged to take a moment to reflect on their feelings. Participants in McMahon et al.
30
noted that biofeedback helped them become more aware of their breath. Participants in Peuters et al.,
45
Maharjan et al.,
29
and Zhu et al.
47
noted increased awareness of behaviours including healthy lifestyle choices, time spent with infants, and sleep patterns, respectively. Finally, Kleiman et al.
35
shared that Empatica E4 devices helped participants become more aware of their distress: “I was able to be more alert and attentive to when I was having a hard time.” (Kleiman et al. 2019)
Amplified negative emotions: While awareness was often noted as a positive outcome, three papers34,37,47 highlighted how self-tracking could lead to a fixation on negative data and amplify distress. In Leonard et al. (2017), 37 30% of participants noted that alerts of stress sometimes increased their anxiety or stress levels. Notably, Kelley et al. 34 saw that students with mental illness were significantly more likely to report encountering negative data, commonly prompting feelings of guilt and disappointment or revealing unhealthy behaviours for participants.
Health monitoring: Wearable devices were seen as useful for monitoring and investigating health behaviours and symptoms. Participants in Peuters et al.
45
monitored their physical activity, sleep, sedentary time, and breakfast consumption which helped them understand and change their behaviour to work towards their specific goals. Kelley et al.
34
demonstrated that self-tracking was helpful for participants to understand the impacts of their habits: “understanding patterns of what causes me to feel the way I do and further rooting out certainties or uncertainties that drive them.” (Participant 52, Kelley et al. 2017)
Clinical uses: Three studies33,34,43 identified the potential benefits of integrating wearables into treatment pathways. For example, a participant in Dewa et al.
33
emphasised the importance of having actionable and timely supports connected to wearables that monitor and detect mental wellbeing status: “[have] an emergency button where they’re told, ‘This person is either going to hurt themselves or has hurt themselves’… you need to send a medical professional to where they’re registered to.”
Reduced symptoms: Wearables were also seen as useful for providing immediate interventions to reduce symptoms of anxiety and stress. Breathing interventions were emphasised as particularly useful in Millings et al.
39
and Persa et al.,
44
with participants noting that they used the breathing intervention to calm them down when they felt stressed: “I found myself using it more so when like, I was feeling stressed or something had stressed me out, so I thought I'll try that now and see how that goes…I thought the breathing one especially was quite good, because I'd never tried that before…” (Participant 95, Millings et al. 2015) “I use Breathe… because I had to help my dad outside a lot and I got really [stressed out]. (...) Sometimes I use it like three times a day. Mostly because I get really [mad].” (Persa et al. 2023)
Self-expression and support: Finally, wearables were seen as methods of enabling self-expression and helping to foster a sense of support for participants. Dewa et al.,
33
Kleiman et al.,
35
and Zhu et al.
47
revealed that wearables offered a method for participants to express their emotions. In Kleiman et al.,
35
participants were encouraged to press a button on their smartwatch when they experienced distress which 7/47 participants mentioned enjoying as an outlet for expressing distress. Similarly, Zhu et al.
47
discussed how participants noted that the wearable and app helped participants quickly express their negative emotions: “If there is a sudden event, filling out the survey will be used as a method to vent bad emotions.” (Participant 7, Zhu et al. 2024)
Peuters et al.
45
found that fostering social connection, such as sharing progress and goals with friends, increased participant motivation to use the intervention. Additionally, Zhu et al.
47
revealed that continuous access to these interventions enabled participants to feel cared for throughout their daily life: “During the survey period, I felt cared for when I was upset. However, upon completion, I was reluctant to leave because I still desired that care. I struggle to express my emotions.” (Participant 1, Zhu et al. 2024)
Quantitative
The 10 papers that included quantitative acceptability data used questionnaires to collect participant feedback and are summarised in Appendix E. Custom questionnaires were used by six studies32,36–38,40,41 which asked participants questions specific to the intervention and study context. The System Usability Scale (SUS) 48 was used by three studies,36,43,46 while the Client Satisfaction Questionnaire (CSQ) 49 was implemented in two studies36,37 and used as the basis for one study-specific questionnaire. 38 Other scales used by a single study include the Wearable Computer Comfort Rating Scale, 50 the Questionnaire for the Evaluation of the Treatment (FBB), 51 and the Health Information Technology Usability Evaluation Scale (Health-ITUES). 52
The number of items on the questionnaires ranged from 2 to 50. The details on the questionnaire items and scales used were unclear in Murray et al. 40 Additionally, the number of participants that completed the study questionnaires was not explicitly stated for questionnaires in three studies.36,43,46 For the studies with total respondent numbers listed, respondents ranged from 10 to 60.
The custom, study-specific questionnaires focused on gathering participant experiences with the intervention, perceived effectiveness, and comfort or safety levels. Studies using custom scales reported positive acceptability outcomes including potential help with academic performance through instant wearable feedback, 32 patient satisfaction with remote therapy, 36 and help in managing stress.37,38 However, Chen et al. 32 had minimal methodological detail and data reported which may limit these findings. There were also positive results around feeling “safe” or “very safe” using wearables. 41
Feedback specific to wearable comfort and ease of use were more mixed. Murray et al. 40 reported that 30% of participants experienced minor discomfort, while 80% of participants in Nielsen et al. 41 reported that the devices were “very comfortable” or “comfortable” to use during the day, but less comfortable when using it during the night (68.3%). Additionally, in Murray et al., 40 more than half of participants (14/21) found EMAs helpful, but four found them difficult to complete.
The SUS resulted in overall acceptable scores. Klein et al. 36 and Perego et al. 43 achieved scores higher than 80 (grade “B”, overall acceptable 53 ), while Van Doorn et al. 46 scored 63.78 (grade “D”, marginally acceptable 53 ). Klein et al. 36 collected SUS on each technology component used in the study, finding the ECG chest strap had the highest average SUS score of 84.32 out of the wearables assessed. Additionally, we flagged Perego et al. 43 during the quality assessment in this review due to minimal details reported in the methodology and results.
High satisfaction was reported across studies using the CSQ. Klein et al. 36 noted an average score of 27.5 out of 32, while Leonard et al. (2017) 37 reported average scores of 3.4 out of 4 on individual items, comparable to the satisfaction levels reported from the accompanying surveys in these studies.
Three additional questionnaires were used across studies. Kleiman et al. 35 included the Wearable Computer Comfort Rating Scale with items on this scale ranked from 1 (most comfort) to 10 (least comfort). Most items (10/12) had mean scores less than 5 while the highest mean score was 7.28 in agreement with the statement: “I could feel the device on my wrist”. Kleiman et al. 35 found that those who dropped out of the study were more likely to rate the device as uncomfortable and report feeling the device on their wrist. These findings complement the qualitative theme “complaints about the monitor” noted from participant feedback. Additionally, Klein et al. 36 included the Questionnaire for the Evaluation of the Treatment (FBB), focused on the quality and effectiveness of the online therapy. This demonstrated that on average participants felt therapists were interested in their problems and that their compulsions had not increased during the intervention. Lastly, alongside the SUS, Van Doorn et al. 46 collected participant feedback using the Health-ITUES to evaluate intervention impact, perceived usefulness, ease of use, and user control. Questionnaire items were evaluated from 1 (lowest) to 5 (highest). The average total score was 3.69 with the highest mean score of 3.93 for the impact of the intervention.
Discussion
This systematic review synthesises the findings of 19 studies that collected adolescent acceptability feedback on wearable devices for mental wellbeing applications. A majority (n=14/19) of the studies used wrist-worn devices and heart activity metrics were the most common physiological measurement (n=9), consistent with the common wearable form factors and signals used for stress management. 54 The most common study type was mixed-methods evaluations of adolescent acceptability (n=12). The main factors influencing acceptability that emerged from qualitative synthesis included perceived effectiveness, device comfort, technical reliability, wearable social acceptability, privacy and safety concerns, and contextual adaptation to different settings and participant needs. These overlap with the drivers of acceptability that have been identified in similar investigations of wearable acceptability with adult populations.55,56 Additionally, the quantitative synthesis in this review indicated general high acceptability of wearables for adolescent mental wellbeing, which correspond with strong interest in wearables for mental health seen in adult populations. 55 These measures also mirrored the qualitative data with specific concerns around device comfort, technical reliability, and perceived effectiveness, while revealing some discrepancies, such as for device safety and satisfaction.
The double-edged sword of self-tracking
One dynamic that emerged from this review was the tension between positive and negative psychological impacts of wearables. For instance, participants outlined several benefits of wearables including qualitative reports from ten studies of increased awareness of thoughts, feelings, and behaviours,29,30,33–35,37,38,45–47 often linked to increased motivation and positive behaviour change. Simultaneously, participants in three studies34,37,47 highlighted that self-tracking amplified feelings of stress or anxiety, and participants in four studies29,31,42,47 worried about increased surveillance. In Kelley et al., 34 the college students diagnosed with mental illnesses were more likely to report encountering negative self-tracking data. This underscores the importance of custom methods of sharing data about mental wellbeing and adapting wearables to account for people’s mental health status.
This double-edged sword aligns with previous research demonstrating that wearables are used beyond tools for habit tracking to satisfy people’s emotional and social needs. 57 While self-tracking can encourage feelings of self-efficacy, achieving wellbeing goals, and connecting to communities, it can also lead to obsessions with data, issues with privacy and surveillance, and a lack of transparency in wearable metrics, among other concerns. 58 Therefore, it is particularly important that these tools are designed and implemented carefully for adolescent populations who may be particularly vulnerable to negative self-judgements 59 and heightened stress responses. 60
Future studies should further investigate design approaches to mitigate the potential risks related to self-tracking in this age group and how this varies based on context. Rather than maximising data collection or adherence, effective interventions should incorporate adaptive biofeedback based on people’s personality and mental health status. These could include methods like just-in-time adaptive interventions (JITAIs) to tailor interventions to respond in moments of heightened need based on real-time wearable data.61,62 Future interventions could also include methods of identifying signs of obsessive self-monitoring patterns, limiting data tracking, providing transparent wearable metrics and avenues for communication, and facilitating connection with mental health professionals.
Contextual considerations
The importance of considering how wearables fit into participants’ daily lives in specific contexts was another major theme revealed in this review. Participants in low-income settings, such as the studies in high-risk communities in Nepal 29 and Uganda,41,42 highlighted safety concerns, strong reactions from their community, and speculations about the impacts of the wearables used. Interestingly, these results conflicted with quantitative reports indicating that most participants felt safe when wearing the device. 41 Still, these outcomes contrast starkly with social acceptability in middle- to higher income settings where participants focused on device aesthetics and classmate perceptions.
Additionally, participants in Dewa et al. 33 suggested that wearables for detecting mental health deterioration should be able to react to real-life scenarios through timely interventions and offering quick connections to professional support. These findings align with a review by Kang and Exworthy 63 stressing the importance of providing wearable interventions that can adapt to different situations and needs. Additionally, Rieder et al. 64 describes both external and internal contextual factors from people’s environment or personal state that can either facilitate or inhibit feelings of self-efficacy for wearable users. When implementing wearable interventions, careful consideration should be given to several elements including the wearable form factors, which signals are collected, the method and frequency of feedback, and the training information provided to participants.
As demonstrated in Maharjan et al. 29 and Persa et al. 44 partnership with local organisations and participatory design processes can facilitate better contextual alignment of these interventions. While acceptability assessments are beneficial methods of gauging people’s perspectives on technology, methods of participatory design and community engagement involve participants in the process of adapting digital interventions to best suit them. Relevant stakeholders such as adolescents, caregivers, teachers, psychologists, technologists, and policy makers should work together to co-create digital interventions and plan how they can be effectively used. Policy makers should consider guidelines that encourage ethical, safe, and context-specific digital mental health interventions for young people.
Implications for design
Several qualitative themes, related to device usability, satisfaction, and perceived benefits, were echoed in the quantitative feedback reported in this review. In particular, device comfort was assessed as part of custom questionnaires in three studies36,40,41 and one study 35 used the Wearable Computer Comfort Rating Scale. Kleiman et al. 35 found that participants who rated the device as less comfortable had lower adherence. Technical challenges with the wearable were another common frustration and barrier to engagement across quantitative and qualitative findings. For example, participants in Van Doorn et al., 46 despite sharing perceived benefits of the intervention, noted that battery life and complicated login process kept them from engaging, which was reinforced by a low SUS score. Focus group feedback in Leonard et al. (2017) 37 also called attention to both perceived benefits and technical challenges. In this case, the high satisfaction score on the CSQ revealed that the perceived benefits likely outweighed the technical barriers faced by participants in this study. These findings align with prior research demonstrating that perceived benefit has a greater impact on the perceived value of wearables than perceived risks. 65 Therefore, wearable designs should minimise the levels of technical barriers and maximise potential benefits because participants consider this trade-off when determining the acceptability of interventions.
Additionally, social acceptability was a common theme in the qualitative synthesis, however, it was largely absent from the quantitative reports. This may be due to the lack of questionnaires that captured social impacts related to the device used. Researchers in the future could explore the use of quantitative methods to assess this element of acceptability, such as the Wearable Acceptability Range (WEAR) scale 66 that focuses specifically on social acceptability. Device comfort, ease of use, and social acceptability should all be considered when designing wearables and wearable-based interventions to encourage acceptability.
Limitations and future directions
Of the few studies identified in this review, there was a large range in quality which may limit the reliability of the findings. Additionally, there was significant heterogeneity in the interventions, the methodology of both qualitative and quantitative data collection, and the comprehensiveness of data reported in the results. Studies were also largely carried out in developed countries. The considerable intervention variability, such as study duration and reported participant incentives, also complicates the synthesis of consistent findings across included studies. The limited number of studies, lack of consistency in methodology, and limited diversity across the included studies make it challenging to identify factors which affect the acceptability of wearable interventions for mental wellbeing that are generalisable to adolescent cohorts not captured in this review.
Limitations of this review process include a lack of meta-analysis of the quantitative acceptability metrics due to the heterogeneity of the study designs, limiting our ability to synthesise quantitative metrics across the included studies. Similarly, the use of thematic analysis rather than meta-ethnography for qualitative synthesis may limit the depth of analysis and interpretation of participant feedback. The 72.8% agreement between researchers in TFA theme mapping suggested subjectivity in the interpretation of the extracted codes and final categories. Additionally, existing relevant studies could have been missed if they were outside the scope of the databases searched in this review. Although the selected databases were chosen to capture research across health, engineering, and social science, expanding the databases further to focus on human factors research could have yielded additional studies.
A consideration for future research is the integration of AI features into wearable interventions based on recent advances, such as “stress scores” and conversational health agents. There was limited mention in reviewed literature of AI integration into wearable interventions. Future research could examine how AI integration into wearables and connected apps may impact the identified acceptability factors, such as data accuracy and transparency, surveillance concerns, methods of communication, and personalised interventions.
Conclusion
Wearable devices present promising yet complex opportunities to support adolescents with pressing mental health needs. Further research is needed to promote adolescent-centred digital supports, including evaluating their psychological impact, minimising potential risks, and adapting to diverse contexts. This review offers novel insights into the factors that influence the acceptability of wearables for adolescent mental wellbeing, which can inform further development of interventions to provide scalable, accessible, and context-specific support to counter the growing mental health crisis in adolescents.
Supplemental material
Supplemental material - The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review
Supplemental material for The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review by Justin Laiti, Rhieya Rahul, Merinda Mundadan, Elaine Byrne, Pádraic J. Dunne in DIGITAL HEALTH
Supplemental material
Supplemental material - The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review
Supplemental material for The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review by Justin Laiti, Rhieya Rahul, Merinda Mundadan, Elaine Byrne, Pádraic J. Dunne in DIGITAL HEALTH
Supplemental material
Supplemental material - The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review
Supplemental material for The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review by Justin Laiti, Rhieya Rahul, Merinda Mundadan, Elaine Byrne, Pádraic J. Dunne in DIGITAL HEALTH
Supplemental material
Supplemental material - The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review
Supplemental material for The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review by Justin Laiti, Rhieya Rahul, Merinda Mundadan, Elaine Byrne, Pádraic J. Dunne in DIGITAL HEALTH
Supplemental material
Supplemental material - The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review
Supplemental material for The acceptability of wearable devices for promoting adolescent mental wellbeing: A systematic review by Justin Laiti, Rhieya Rahul, Merinda Mundadan, Elaine Byrne, Pádraic J. Dunne in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank RCSI for supporting this systematic review and the Fulbright program for facilitating the partnership to make this research possible.
Ethical considerations
No ethical approval was sought due to all the research included in this review being publicly available.
Consent to participate
Not applicable as there were no participants in this study.
Consent for publication
Not applicable since all data included in this review is public.
Author contributions
JL conceptualized this review, performed data curation, analysis, and synthesis, and drafted the manuscript. RR and MM supported data analysis and synthesis while also editing the final manuscript. EB helped in the conceptualization and supervision of this review and in the editing of the manuscript. PD acquired the funding, provided supervision, and revised the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author of this study is funded by a PhD grant partnership between the Royal College of Surgeons in Ireland and the U.S. Fulbright Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data extracted from included studies in this review is available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.