
Abstract
Background
While integrating digital technology into healthcare is a key strategy to address population aging, robust evidence on the causal impact of large-scale policies is scarce. This study aims to quantify the health effects of China’s smart city policy on older adults and identify the mechanisms driving these outcomes.
Methods
This study employed a multi-period difference-in-differences (DID) model, leveraging China’s national smart city pilot policy as a quasi-natural experiment. The analysis utilized balanced panel data from the China Family Panel Studies (CFPS) for the period 2010–2020. The primary outcomes were self-rated health and mental health among adults aged 60 and over.
Results
Smart healthcare significantly improved older adults’ self-rated health (β = 0.093, p < 0.10) and mental health (β = 0.088, p < 0.10). The policy effect followed an inverted-U shape, peaking at four years post-implementation. Benefits were stronger for rural, younger-old (60-74), and unmarried individuals, suggesting a compensatory effect for underserved groups. These improvements were driven by three mechanisms: increased healthcare utilization, healthier behaviors, and greater health-related investments.
Conclusion
Smart healthcare is an effective tool for improving older adults’ health, but its dynamic and heterogeneous effects highlight the need for adaptive and targeted policies to sustain long-term benefits and ensure equity.
1. Introduction
Population health is a crucial indicator of societal well-being, particularly in aging societies. In October 2016, the Chinese government launched the Healthy China 2030 Plan, officially establishing “Healthy China” as a major national strategy. The strategy marks a fundamental shift from a treatment-centered to a health-centered model. It explicitly targets the health of key populations, including women, children, older adults, and low-income groups. Furthermore, the plan designates healthy aging as a special initiative, underscoring the strategic importance of older adults’ well-being.
Extensive research has identified key health determinants, including socioeconomic status,1,2 lifestyle,3–5 and access to healthcare. Alongside this demographic shift, digital adoption among the elderly is accelerating. As of June 2025, China’s elderly internet penetration rate reached 52.0%, with 161 million users aged 60 and above, according to the China Internet Network Information Center (CNNIC). The integration of digital technology with healthcare services, known as smart healthcare, represents a transformation of traditional healthcare models. Its impact on residents’ health behaviors and health levels warrants further exploration. Existing literature largely supports the positive effects of digital health technologies; for instance, telemedicine improves access to medical resources, 6 and wearable devices enable early disease detection and management. 7 However, current research has two main limitations. First, it predominantly focuses on the micro-level efficacy of specific technologies rather than the macro-level causal effects of policy interventions. Second, it often overlooks the broader social and policy contexts that mediate technology’s impact.
Smart cities are urban development models using next-generation information technologies (e.g., IoT, Big data, AI) to enhance urban planning, governance, and services. As of 2024, over 500 Chinese cities have launched smart city initiatives across various sectors, including healthcare. This study evaluates the health impact of smart city policies on the elderly by employing a multi-period difference-in-differences (DID) model on the 2010-2020 China Family Panel Studies (CFPS) data, treating the policy implementation as a quasi-natural experiment. This quasi-natural experimental design allows for robust causal inference by mitigating potential endogeneity issues. This study makes three primary contributions: First, it provides a robust causal estimate of the health impacts of a large-scale smart healthcare policy by leveraging an exogenous shock to address endogeneity. Second, it investigates the underlying mechanisms by examining changes in healthcare utilization, health behaviors, and health-related investments. Third, it identifies heterogeneous effects across different elderly subgroups, offering targeted evidence for developing more equitable and inclusive digital health policies.
2. Policy context and research hypotheses
2.1. Policy context of smart city pilot programs
China’s smart city pilot policy represents a strategic integration of national new urbanization and informatization goals. Standardized development began in 2012 when the Ministry of Housing and Urban-Rural Development (MOHURD) issued interim administrative measures for national pilots. The primary objective is to optimize urban planning, construction, management, and services using advanced technologies such as the Internet of Things (IoT), cloud computing, and big data. Between 2013 and 2015, MOHURD approved three batches totaling 290 pilot projects across various administrative levels, covering over 80% of China’s prefecture-level cities. These included 90 projects in the first batch (January 2013), 103 in the second (August 2013), and 93 in the third (April 2015), which comprised 84 new and 13 expansion initiatives. This policy context provides a unique quasi-natural experimental setting to identify the causal health effects of large-scale digital infrastructure initiatives. Smart cities provide essential infrastructure, such as regional health platforms and electronic health records, that facilitates smart healthcare development. Furthermore, the phased implementation and specific entry thresholds of smart city policies create a robust quasi-natural experimental setting. Consequently, employing a multi-period difference-in-differences approach allows for the effective identification of causal effects, thereby enhancing the reliability of research conclusions.
2.2. research hypothesis formulation
2.2.1. Smart healthcare and older adults health
The integration of medical Iot, intelligent algorithms, and data analytics reshapes healthcare resource allocation and enables diverse applications for elderly chronic disease management and monitoring. Physiologically, smart wearables continuously monitor critical indicators such as blood glucose and blood pressure. By using machine learning algorithms to detect anomalies, these devices effectively reduce acute complication rates in elderly chronic disease patients. 8 Furthermore, big data-driven personalized management platforms improve treatment adherence via features like smart medication reminders and customized dietary recommendations. These interventions have been shown to enhance patients’ self-rated health outcomes. 9 Smart healthcare technologies also address mental health; social features like online health communities foster connections among older adults, significantly alleviating loneliness and depressive symptoms. 10 This integrated physical and psychological monitoring framework supports a full-cycle elderly health management model. Based on this evidence, we propose the following hypothesis.
Smart healthcare implementation positively impacts the health status of older adults.
2.2.2. Smart healthcare and healthcare service utilization
Smart healthcare improves medical access for the elderly by integrating online and offline resources and matching service supply with demand, thereby increasing their utilization of healthcare services. Digital technologies also optimize healthcare resource allocation through intelligent triage and reduced misdiagnosis, which in turn lowers costs and improves efficiency. 11 For instance, smart healthcare has been shown to increase the likelihood of residents choosing large hospitals for their initial consultation. 12 Similarly, patients using online hospitals increase their monthly outpatient visits by 2.4%, an effect more pronounced in rural areas, thus enhancing healthcare accessibility. 13 Based on this evidence, we propose the following hypothesis.
Smart healthcare positively influences the health status of the elderly by increasing their use of healthcare services.
2.2.3. Smart healthcare and health behaviors among older adults
Smart healthcare influences the health behaviors of older adults through real-time feedback and behavioral interventions. For example, wearable devices monitor physiological parameters and metabolic status to support disease diagnosis, 14 while also encouraging increased daily steps and physical activity and reduced sedentary time, thereby promoting healthier lifestyles. 15 Furthermore, integrated social features in health-focused digital communities can enhance cognitive and physical function, reduce vulnerability and social isolation, and improve perceived health among older adults. 16 This evidence leads to the following hypothesis.
Smart healthcare positively influences the health status of older adults by promoting healthier behaviors.
2.2.4. Smart healthcare and health investment among older adults
Smart healthcare encourages increased health investment among older adults through health knowledge dissemination and risk warnings. The development of government-led digital infrastructure creates a supportive environment for such health investments. For example, World Bank report noted that digital innovations in India, such as telemedicine, have enabled over 140 million people to access affordable and efficient healthcare. Health applications and smart devices monitor metrics such as physical activity and sleep quality, encouraging users to adopt healthier habits and increase their investment in preventive care. 17 However, the impact of these health investments is heterogeneous. Higher-income groups can more easily afford smart devices, whereas lower-income individuals may face dual barriers of cost and digital literacy, limiting their access to such health interventions. 18 Accordingly, we propose the following hypothesis.
Smart healthcare positively influences the health status of older adults by increasing their health investments.
3.1. Data sources
This study uses data from the China Family Panel Studies (CFPS), a survey conducted by the Institute of Social Science Survey (ISSS) at Peking University. The CFPS is a large-scale, national longitudinal survey that documents China’s socioeconomic, demographic, educational, and health trends at the individual, household, and community levels. This dataset provides a high-quality foundation for social science research and policy analysis. We extracted data from six survey waves between 2010 and 2020 (conducted in even-numbered years), focusing on individuals aged 60 or older at baseline. To construct a balanced panel, we selected only individuals who participated in all six survey waves. The specific screening process is shown in Figure 1. Participant flow chart.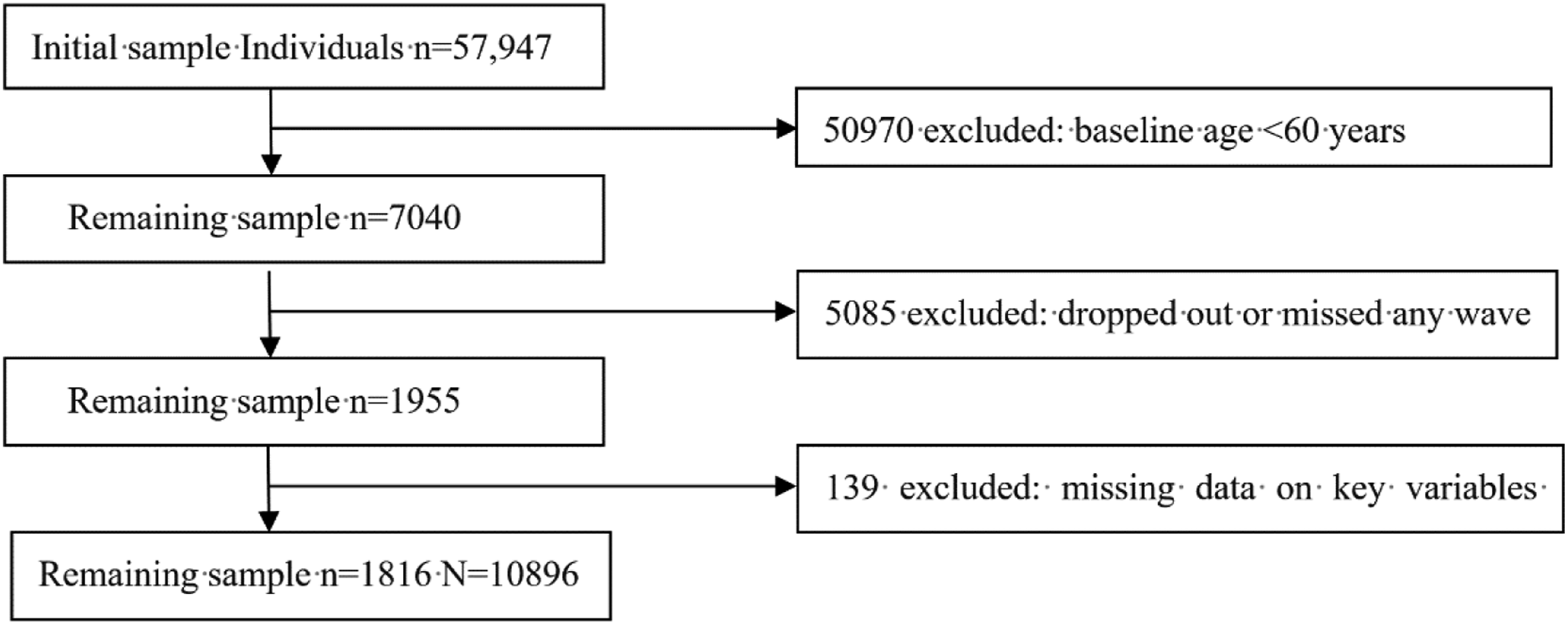
3.2. Variable selection
3.2.1. Dependent variable
This study’s dependent variable is older adult health, operationalized through two dimensions: self-rated health and mental health.
Self-Rated Health. Self-rated health provides a holistic assessment of an individual’s health, integrating physiological, psychological, and social factors.19,20 This was measured on a five-point Likert scale, ranging from “Very unhealthy” (1) to “Very healthy” (5), where higher scores indicate better self-rated health.
Mental Health. A primary challenge for longitudinal analysis of mental health in the China Family Panel Studies (CFPS) is the use of different measurement scales across waves. The 2010 and 2014 surveys used the Kessler Psychological Distress Scale (K6), while the 2012 and subsequent waves used the 8-item Center for Epidemiologic Studies Depression Scale (CES-D8). Despite their different names, both are established instruments for screening psychological distress. They share substantial construct overlap, as K6’s core symptoms (e.g., sadness, nervousness, hopelessness) align with CES-D8’s dimensions (e.g., depressed mood, anhedonia). Previous research supports their comparability. For instance, studies show high classification agreement at clinical thresholds 21 and comparable screening efficacy in general populations. 22 Moreover, prior research using the CFPS dataset has successfully integrated both scales, confirming their consistency for longitudinal modeling. 23 To ensure cross-wave comparability, we performed a two-step harmonization. First, we reverse-coded the negatively worded items in the CES-D8 so that higher scores on both scales consistently represent better mental health. Second, to account for the different Likert scales (5-point for K6, 4-point for CES-D8), we standardized the raw total scores from each wave into Z-scores.
3.2.2. Explanatory variables
Lacking direct city-level data on smart healthcare development, this study uses the implementation of smart city pilot policies as a proxy variable, a common approach in the literature. This choice is justified on three grounds. First, their policy objectives are closely aligned: smart healthcare is explicitly designated as a core component within the government’s National Smart City Pilot Indicator System, implying that pilot implementations directly accelerate the digital transformation of local healthcare. Second, smart city initiatives provide critical technical infrastructure—including big data and cloud computing platforms—that constitutes a fundamental prerequisite for the delivery of intelligent healthcare services. Third, empirical studies show that smart city development significantly improves the quality and accessibility of local healthcare, with one estimate documenting an approximate 21.7% increase in overall service levels. 24 Accordingly, this policy proxy represents an effective and reliable indicator of the advancement in smart healthcare. Methodologically, to mitigate potential biases from this proxy, we employ a multi-period difference-in-differences (DID) model. This approach controls for confounding factors related to time-invariant city characteristics and common time trends. We also conduct a parallel trends test and a series of robustness checks to validate our model.
3.2.3. Control variables
Variable settings and descriptive statistics.

3.3. DID model
We employ a multi-period difference-in-differences (DID) model to evaluate the impact of smart healthcare on the health of older adults. The model is specified as follows:
Here, Y ict denotes the self-rated physical or mental health of individual i in city c at time t. The term policy ic ⋅ timeit is the interaction between the policy dummy and the time dummy. Policy ic equals 1 if the individual resides in a pilot city. For the first two batches of pilot cities announced in January and August 2013, timeit equals 1 starting in 2014. For the third batch announced in April 2015, timeit equals 1 starting in 2016. β captures the average treatment effect of smart healthcare. X ict includes control variables at the individual and household levels. η i and λ t represent individual and time fixed effects, respectively, and ε ict is the error term. Standard errors are clustered at the city level.
4. Empirical analysis
4.1. Baseline regression
Baseline regression results.

Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
Among the control variables, marital status significantly affects mental health (β = 0.266, p < 0.001) but shows no significant association with self-rated health. This finding suggests that the psychological toll of widowhood or divorce may outweigh its direct effects on physical health in this demographic. Both per capita net household income (β = 0.026, p < 0.10) and financial support from children (β = 0.049, p < 0.10) are positively associated with self-rated health. This is consistent with Grossman’s health capital theory, which posits those greater financial resources ease budget constraints on health investments, thereby slowing the depreciation of an individual’s health capital. Economic capital can improve health by: (1) enabling access to preventive care, (2) improving living conditions and nutrition, and (3) reducing stress-induced chronic inflammation. 27 In addition to financial aid, caregiving support from children is also significantly associated with better mental health (β = 0.058, p < 0.05), as tangible assistance can alleviate daily life pressures. 28 From a social participation standpoint, employment status is positively associated with both self-rated health (β = 0.087, p < 0.05) and mental health (β = 0.071, p < 0.05). This aligns with findings that structured, meaningful employment is particularly beneficial for mental health. 29 Interpersonal relationships formed through social participation exhibit a strong predictive power for self-rated health (β = 0.042, p < 0.001) and mental health (β = 0.034, p < 0.001) among older adults. This finding underscores the applicability of social support theory to the elderly population, indicating that high-quality social networks can generate health benefits via neuroendocrine mechanisms. 30
4.2. Robustness tests
4.2.1. Parallel trends test
A key assumption of the DID model is the parallel trends hypothesis, which requires that the treatment and control groups exhibited similar trends in the outcome variable prior to the policy intervention. To test this assumption, we use an event study approach with the following specification:
Here, Yict denotes the event-time dummy variable. It equals 1 if individual i in city c is in period t that falls k periods before or after the implementation of the Smart City Pilot Policy; otherwise, it equals 0. The implementation period is defined as the CFPS survey wave closest to the time when city c launched the pilot. For example, a city that initiated the pilot in April 2015 corresponds to the fourth CFPS wave. Xict represents the control variables used in the baseline regression. βk captures the dynamic effects of smart healthcare on the health of older adults before and after the policy intervention.
The results of the parallel trends test are illustrated in Figure 2. Using one wave prior to the implementation period (k = -1) as the reference category, the horizontal axis represents the number of survey waves relative to the implementation period, while the vertical axis reports βk estimates with 95% confidence intervals. Prior to policy implementation, all coefficients cluster around zero, indicating no significant differences in self-rated and mental health between the treatment and control groups—thus satisfying the parallel trends assumption. Post-implementation, the effects follow an inverted U-shape: insignificant in the implementation wave, significantly positive in the following two waves, and subsequently declining. This suggests a potential time-bound effect. Such a dynamic pattern aligns with Rogers’ “S-curve” in the theory of technology diffusion. The initial phase of smart city policy implementation focuses on infrastructure development, platform creation, and user awareness. However, immediate health benefits for the elderly are limited due to factors like the digital literacy gap and the time required for technology adoption
31
Consequently, significant health improvements are not typically observed during this early stage. After one to two years, as the adoption of services like remote health monitoring and online consultations increases, tangible health improvements among the elderly emerge. This trend aligns with the standard technology adoption cycle. However, these gains often exhibit diminishing marginal returns. Systemic challenges—such as funding constraints, poor interdepartmental coordination, and waning media attention—can hinder long-term policy sustainability.
31
As a result, user engagement may decline, causing the initial health benefits to plateau. Parallel trend test.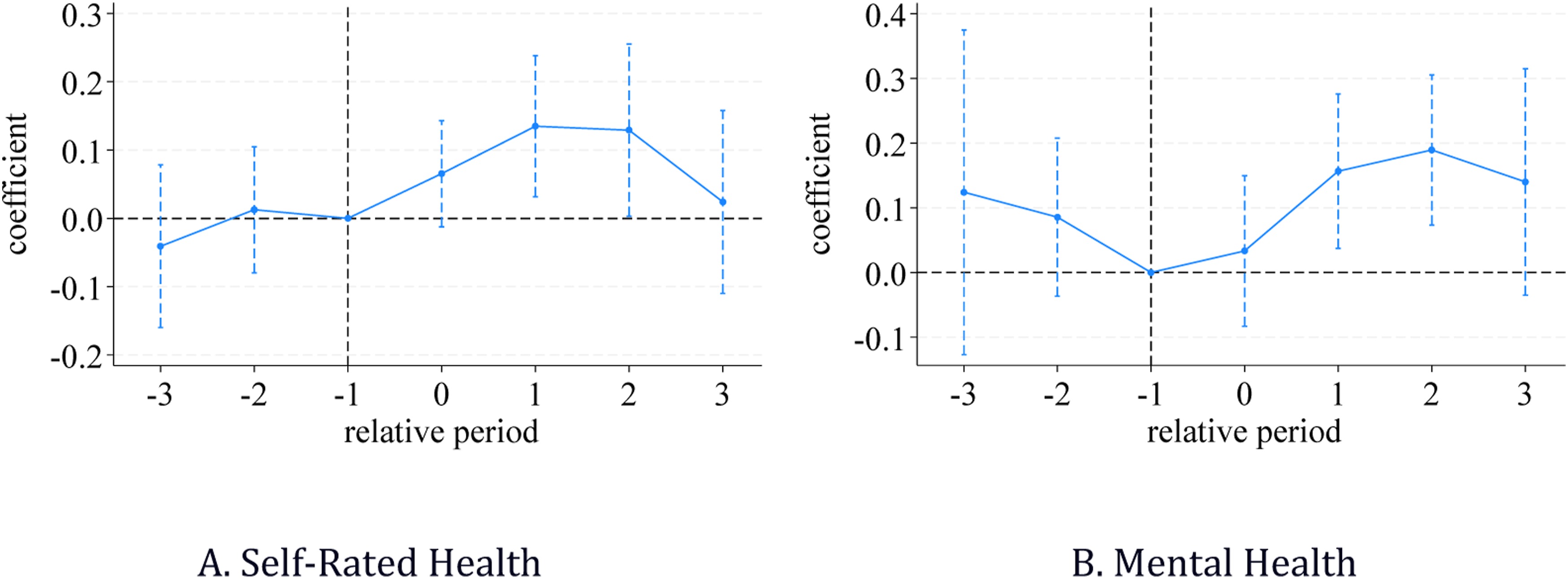
4.2.2. Placebo test
To ensure our results are not driven by unobserved confounders or random chance, we conducted a placebo test. The logic is that if the estimated effect is genuine, a randomly assigned “placebo” treatment should yield an effect centered around zero. Specifically, we randomly assigned a falsified treatment status to a subset of cities and a random implementation time. We repeated this process 500 times, creating a distribution of placebo coefficients to test the null hypothesis of no effect. As shown in Figure 3, the distribution of these 500 placebo coefficients is centered at zero and follows a normal distribution, which is the expected outcome if the true policy effect were zero. In contrast, our actual estimated coefficient (the vertical dashed line) falls far outside this distribution. This result strongly suggests that our findings are not due to chance or unobserved factors, reinforcing the validity of the baseline estimates. Placebo test.
4.2.3. Robustness test based on PSM-DID
PSM-DID test results.
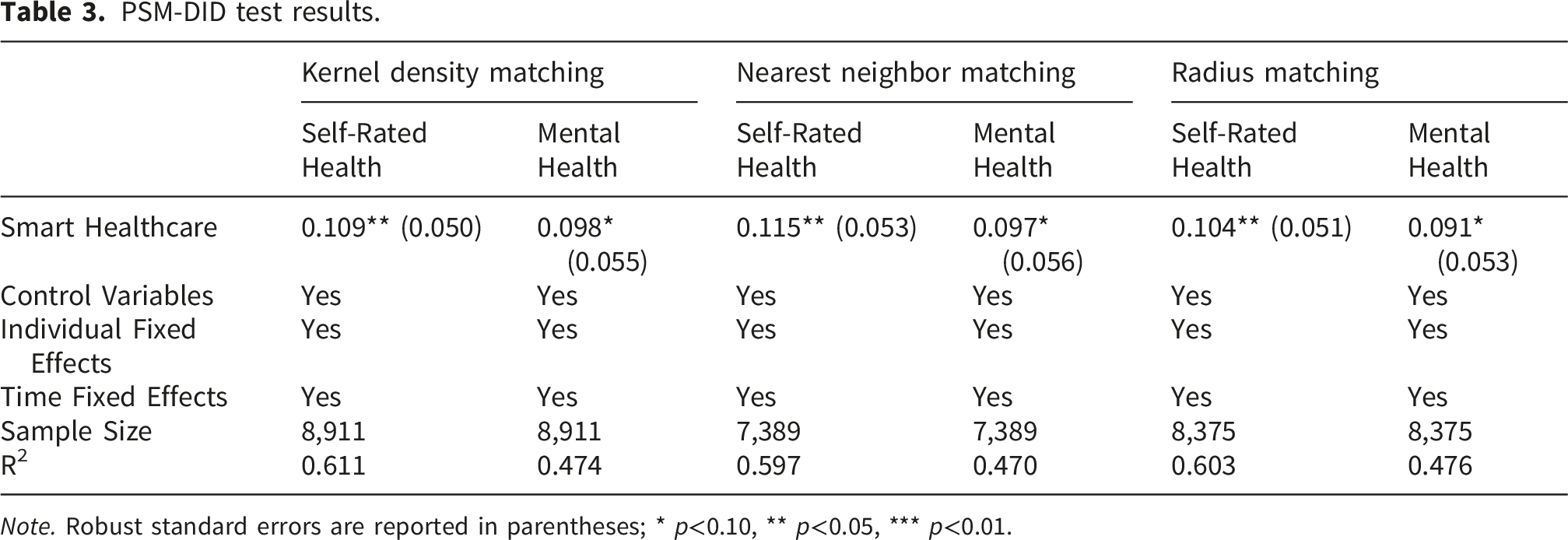
Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
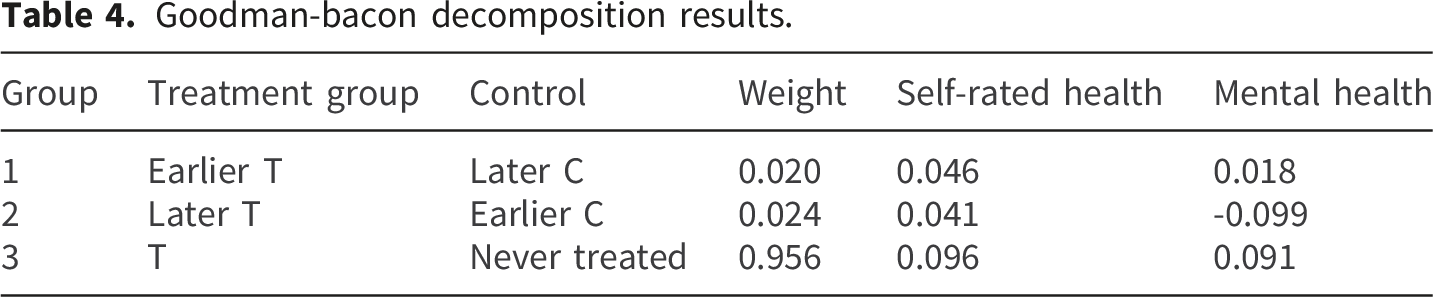
4.2.4. Testing heterogeneous treatment effects
Goodman-bacon decomposition results.
Robust estimator under heterogeneous treatment effects.

Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
4.2.5. Controlling for other policy factors
Test Results after Controlling for other Policy Interferences.
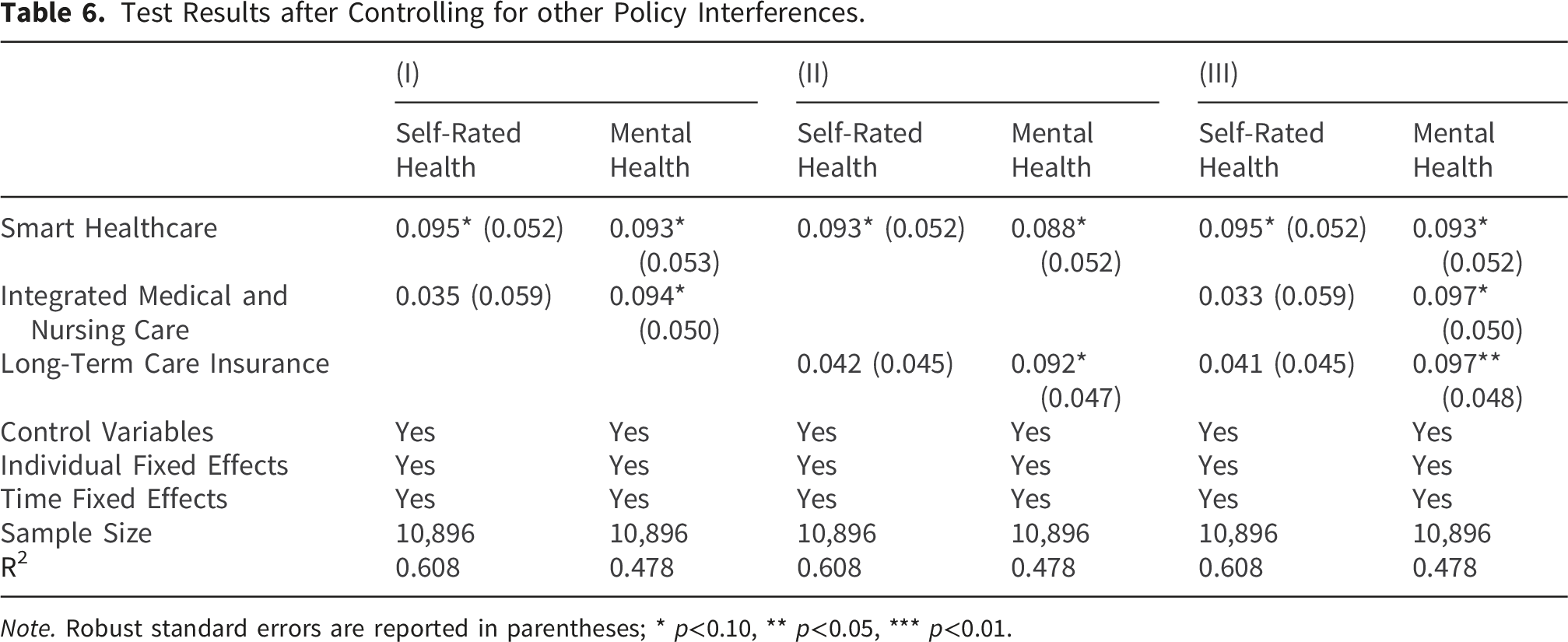
Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
4.3. Heterogeneity analysis
Heterogeneity test results.

Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
By age, the policy benefits those aged 60–74 in both self-rated health (β = 0.088, p < 0.10) and mental health (β = 0.082, p < 0.10). No significant effects were found for individuals aged 75 and over. This may be due to lower digital literacy and adoption rates among this older cohort, limiting the policy’s reach and effectiveness. Regarding marital status, while married seniors show significant improvements in self-rated health (β = 0.134, p < 0.05), the policy has a stronger positive effect on the mental health of unmarried seniors (β = 0.266, p < 0.05). This suggests smart healthcare may offer compensatory emotional and social support for those who are widowed or living alone.
4.4. Analysis of mechanisms of action
Having established that smart healthcare improves health outcomes for older adults, we now explore potential mechanisms, focusing on healthcare utilization, health investment, and lifestyle changes.
4.4.1. Enhancing healthcare service utilization
Healthcare service utilization serves as a key mediating variable for improving the health of older adults. This can be observed through two primary pathways. On one hand, enhanced primary and preventive services help achieve early intervention and disease prevention. Specifically, regular check-ups, health education, and chronic disease management are effective in slowing disease progression and lowering the risks of incidence and complications among the elderly. 35 On the other hand, innovative service models improve healthcare accessibility. Telemedicine and integrated medical-elderly care increase the continuity and convenience of services, ultimately improving older adults’ health by mitigating barriers to receiving care. 36
Results of mechanism testing.

Note. Robust standard errors are reported in parentheses; * p<0.10, ** p<0.05, *** p<0.01.
4.4.2. Guiding healthy behaviors
Healthy behaviors, including reduced alcohol consumption, smoking cessation, and increased physical activity, are critical for older adults’ health. Research confirms that limiting alcohol, 37 quitting smoking, 38 and increasing physical activity39,40 significantly improve health outcomes.
We investigated the role of smart healthcare in promoting healthy behaviors among older adults. This study incorporated variables for alcohol consumption, smoking, and physical exercise frequency. The results are presented in Table 8 (columns III–V). The findings show that smart healthcare significantly reduced alcohol consumption (β = -0.022, p < 0.10). This suggests that health monitoring and risk alerts are effective in discouraging unhealthy drinking habits. This result is consistent with Kelly, who found that digital interventions can lower alcohol intake. 41 The results also revealed that smart healthcare significantly promoted physical exercise (β = 1.070, p < 0.10), likely by motivating users through exercise-tracking apps and goal-setting features. We did not find a significant impact on smoking behavior.
4.4.3. Promoting health investment
Drawing on Health Investment Theory, 42 health capital can be augmented through investments in health. Empirical studies support this, showing that internet use increases household health investment and fosters a shift from passive treatment to active prevention. 43 Health investments can be categorized as either preventive (e.g., medical insurance, regular check-ups) or curative (e.g., medical consumption, rehabilitation services), both of which improve health outcomes by reducing risk exposure and enabling faster disease intervention. 44
To test whether smart healthcare improves health by increasing health investment, we measured two variables: participation in basic medical insurance and the logarithm of per capita household health expenditure. The results, shown in columns (VI) and (VII) of Table 8, indicate that smart healthcare has a significant positive effect on both participation in basic medical insurance (β = 0.040, p < 0.05) and per capita health expenditure (β = 0.309, p < 0.05). These findings suggest that smart healthcare encourages older adults to increase their investment in health, thereby improving their health status.
5. Discussion
5.1. Smart healthcare effectively enhances older adults’ health
Our baseline regression results indicate that smart healthcare has a significant positive effect on both self-rated health and mental health among older adults. This finding aligns with existing research, confirming a strong link between the adoption of smart healthcare and health improvements in this population.
For physical health, the mechanism can be explained by technological advancements. Personalized medical platforms, powered by big data, support precise and individualized health management. 9 Furthermore, smart wearables like electronic blood pressure monitors and health watches enable real-time monitoring of vital signs. This facilitates risk prediction and continuous tracking, thereby reducing acute episodes and unnecessary medical visits. 8
Regarding mental health, smart healthcare can mitigate loneliness and depression by fostering emotional companionship and social connection. For example, digital health tools with social features enhance social support, which improves emotional well-being and cognitive function. 10 Research has also identified a discernible link between data from smart devices and users’ psychological states, further supporting this connection. 45 Additionally, features like video calls and remote monitoring directly bridge generational gaps, enhancing feelings of belonging and security and thus boosting psychological resilience. 46
However, smart healthcare also presents challenges. The reliance on data sharing raises privacy concerns, as the risk of data breaches can increase anxiety. Moreover, low digital literacy and technological accessibility barriers can cause psychological discomfort for some older adults. Thus, a key policy challenge lies in mitigating issues like the digital divide, information overload, and privacy risks for the equitable distribution of technological benefits.
5.2. Significant heterogeneity in the positive impacts of smart healthcare
The heterogeneous effects of smart healthcare on the health of older adults likely arise from the interplay of social resources, technology adoption capabilities, and social support.
First, regarding residential location, our subgroup analysis indicates that smart healthcare more effectively improves health in rural areas, particularly mental health. This is likely due to urban-rural disparities in healthcare access. Rural areas often face shortages of professional resources and geographical barriers to care. 47 Smart healthcare mitigates these challenges through telehealth and digital interventions, creating significant opportunities for health improvement. In contrast, urban old adults have better access to an established healthcare network, so the compensatory effect of smart healthcare is less pronounced.
Second, age-based heterogeneity was evident. Smart healthcare showed a stronger positive effect on the health of younger-old adults (60–74 years) but no significant effect on older-old adults (75+). This difference can be attributed to age-related variations in the ability and willingness to adopt new technologies. This aligns with the theory of the “Third Age” (active and capable) and “Fourth Age” (frailty and cognitive decline). 48 Smart healthcare is better suited for the active aging goals of the “Third Age,” whereas its role in the “Fourth Age” is often limited to emergency response and care support. High learning costs and lower self-efficacy often reduce technology adoption among the oldest-old. 49 This is consistent with studies in China, which found that health interventions have diminishing marginal effects with increasing age. 50
Third, we observed heterogeneity by marital status. Smart healthcare significantly improved self-rated health for partnered adults but had a more pronounced positive impact on the mental health of unpartnered adults. This divergence may be because spousal support can amplify the effectiveness of digital health tools, enhancing adherence and thus improving physical health outcomes. Conversely, unpartnered adults, who face a higher risk of loneliness and social isolation, 51 benefit more from the social connectivity features that improve mental well-being. However, it is crucial to note that marital quality may be more important than marital status itself. An adult in a low-quality marriage may experience greater psychological distress than an unpartnered one, and technology may fail to improve their mental health if it does not address underlying family conflict. 52 Therefore, a simple partnered/unpartnered dichotomy may mask the complex role of relationship quality as a core determinant of health.
5.3. Smart healthcare influences health through multiple pathways
Our analysis suggests that smart healthcare improves older adults’ health through three interconnected pathways: enhancing service accessibility, guiding healthy behaviors, and promoting health investment.
Smart healthcare enhances accessibility to medical services in two key dimensions: spatial and economic. First, it improves spatial accessibility by overcoming geographical barriers. E-Health enables older adults in remote, rural, or underserved areas to receive virtual consultations, granting them access to high-quality medical resources that were previously out of reach. 53 Telemedicine projects in remote Chinese regions have already demonstrated success. For example, in Xinjiang and Qinghai, telemedicine stations connect border villages with top-tier tertiary hospitals, after 43 remote medical stations were built in Milin, Tibet, the local clinic consultation rate increased by 20.6%. Second, smart healthcare improves economic accessibility by streamlining service processes and increasing efficiency. The World Health Organization’s Universal Health Coverage framework emphasizes that financial affordability relies on appropriate payment mechanisms and efficient allocation of resources. Smart healthcare serves as a key technological means to support these goals. In practice, Electronic Health Records enable real-time information sharing and reduce repeated tests caused by incomplete information. Remote consultation modules allow older adults to receive expert diagnoses from higher-level hospitals without long-distance travel, thereby reducing transportation, accommodation, and other non-medical costs. 12
Regarding health behaviors, smart healthcare is associated with reduced alcohol consumption and increased physical activity among older adults. This aligns with the Health Belief Model, which posits that an individual’s readiness to adopt healthy behaviors depends on perceived susceptibility, perceived severity, and a balance between perceived benefits and barriers. 54 First, smart healthcare enhances older adults’ access to health knowledge and their capacity for behavioral decision-making. Smart city pilot policies, through public service campaigns and community health education, deliver personalized health management advice. These initiatives significantly improve health literacy. Studies show that higher health literacy helps older adults change their health attitudes, increase their use of preventive medical services, and adopt healthier behaviors. 55 Second, smart healthcare improves adherence to chronic disease management, facilitating a shift from passive treatment to proactive intervention. Smart health devices can track data such as daily activity, sleep, and blood pressure. This information allows older adults to better assess their own behaviors. Consequently, they can improve their self-management by exercising more frequently, adhering to medical check-ups, and modifying their health habits. 56 Notably, the effect of smart healthcare on smoking behavior was not statistically significant (p > 0.10). This may suggest that changing addictive behaviors requires more intensive interventions. It also implies that future smart healthcare designs should employ differentiated strategies tailored to the specific characteristics of different health behaviors.
In terms of health investment, smart healthcare significantly increases older adults’ participation in basic medical insurance and raises household healthcare expenditure. Smart healthcare may stimulate health investment through two primary mechanisms. First, health monitoring data enhances older adults’ perception of health risks, which in turn stimulates demand for preventive investment. Older adults using smart health devices show greater adherence to health screenings and behavioral interventions for chronic disease management. This shifts spending from acute treatment to long-term and preventive health investments, such as rehabilitation equipment and home care. 46 Second, smart healthcare spurs the development of novel health products and promotes the growth of the senior health industry. The rising adoption of devices like smart wristbands and electronic blood pressure monitors has driven investment in emerging markets. These markets include rehabilitation equipment and remote health management services. At the policy level, pilot programs in China integrating long-term care insurance with smart elderly care have unlocked substantial investment opportunities, such as in home-based care beds and smart community wellness centers. These initiatives both stimulate individual health investment and invigorate the senior health industry.
6. Implications for further research
This study employed a multi-period difference-in-differences (DID) model to systematically evaluate the causal effect of smart healthcare on the health of older adults. It provides empirical evidence from China on the role of digital technology in healthy aging. Our findings offer valuable insights for promoting the inclusive development of smart healthcare and optimizing health resource allocation. However, this study has several limitations that future research should address. First, although using the Smart City Pilot Policy as a quasi-natural experiment mitigates endogeneity bias, data limitations prevented a deeper analysis of heterogeneity in technology use at the individual level. This includes variations in usage frequency, depth, and the specific functional modules employed. Future research could use targeted survey data to clarify the moderating mechanisms within the “technology use–behavior change–health outcome” pathway. Meanwhile, a binary policy proxy cannot fully capture variations in the intensity and quality of local smart healthcare implementation. To refine these causal estimates, future research should utilize granular, continuous indicators, such as the number of smart clinics or regional digital health penetration rates. Second, our study found that the health benefits of smart healthcare were less pronounced for vulnerable populations, such as the oldest-old and unmarried individuals. This highlights the complexity of achieving digital inclusion. Future research should move beyond the access-level digital divide. It should explore how to enhance technology adoption and effective use among vulnerable groups through multiple pathways, such as age-friendly design, intergenerational support, and community-based training. This would help ensure that the benefits of smart healthcare are shared more equitably among all older adults. Finally, smart healthcare is a rapidly evolving technological system. Its long-term health effects and sustainability models require continuous observation. Future research should conduct longitudinal studies to assess the long-term impacts of smart healthcare on health trajectories, medical burdens, and quality of life. Attention should also be paid to new digital barriers and ethical challenges that may emerge as technology evolves. This will provide a scientific basis for building a more robust and equitable governance framework for smart aging.
Footnotes
Ethical Considerations
Ethical approval for all the CFPS waves was granted from the Peking University. During the fieldwork, each respondent who agreed to participate in the survey was asked to sign two copies of the informed consent, and one copy was kept in the CFPS office, which was also scanned and saved in PDF format.
Author contributions
Wang, B. and Gong,R.G. analyzed the data, wrote the manuscript, and interpreted the data. Huang,R.Y amendments and suggestions. All the authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is supported by National Social Science Fund Youth Project “Research on Rural Mutual Support Eldercare Service Models from the Co-production Perspective; National Social Science Fund Youth Project 24CGL”.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from Peking University, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Peking University.