
Abstract
Introduction
Recent studies indicated the advancement of Convolutional Neural Networks (CNNs) have facilitated the colon cancer diagnosis process via medical image processing and multi-modality prediction analysis. This paper aims to systematically review the recent notable studies of CNN-based colon cancer classification using histopathological WSI and compare their strengths and limitations as inspirations for future research directions.
Method
This systematic review was conducted under a PRISMA analysis framework. The PICO selection and PROBAST bias assessment tools were used in data selection and validation. The systematic review compared accuracy from notable studies in benchmark architectures (Res-Net, Inception, VGG-Net, Dense-Net, and Efficient-Net) regarding the bi- and multi-classification tasks (2020-2025).
Results
The result showed that Res-Net architecture demonstrated the highest accuracy in both bi- (99.97%) and multi-classification (99.96%) tasks over the past five years. Newer architectures (Efficient-Net, Dense-Net) outperformed older models (VGG-Net, Res-Net) by optimizing depth and feature reuse while minimizing biases. Low computational model were more suitable for real-world deployment and clinical interaction.
Conclusion
This review contributes to the systematic synthesis of knowledge regarding advancements in CNN-based colon cancer classification. Also, this paper provided future research guidelines for further directions (quantum AI, advanced analytics, and lightweight integrations) and implementation in clinical settings.
Keywords
1. Introduction
Colon cancer causes morbidity and mortality worldwide. Emerging Artificial Intelligence (AI) offers significant benefits for patients through more accurate diagnosis. 1 Convolutional neural networks (CNNs) have revolutionized medical image processing and imaging in oncology practices.2,3 In colon cancer histopathological image processing tasks, bi-classification (i.e., adenocarcinoma/benign) and multi-classification (i.e., subtypes of WSI) are the most researched topics. The hierarchical architecture of CNN can identify underlying patterns and structures to facilitate more accurate classification,4,5 segmentation, 6 and registration7,8 than the traditional machine learning approach. 9 By reducing the complexity in manual feature engineering, CNNs accelerate the development of automated tools for a smart and reliable performance in colon cancer diagnosis process.7,10
With the rapid development of CNN applications, Bhatt et al.
11
reviewed CNN architectures, applications, and future scope in general computer vision studies. The Figure 1 indicates a year-by-year increasing research interests in medical CNNs for colon cancer diagnosis from 2000 to 2025. 94,990 out of 481,930 (19.7%) CNN research papers published in Survey results based on related studies.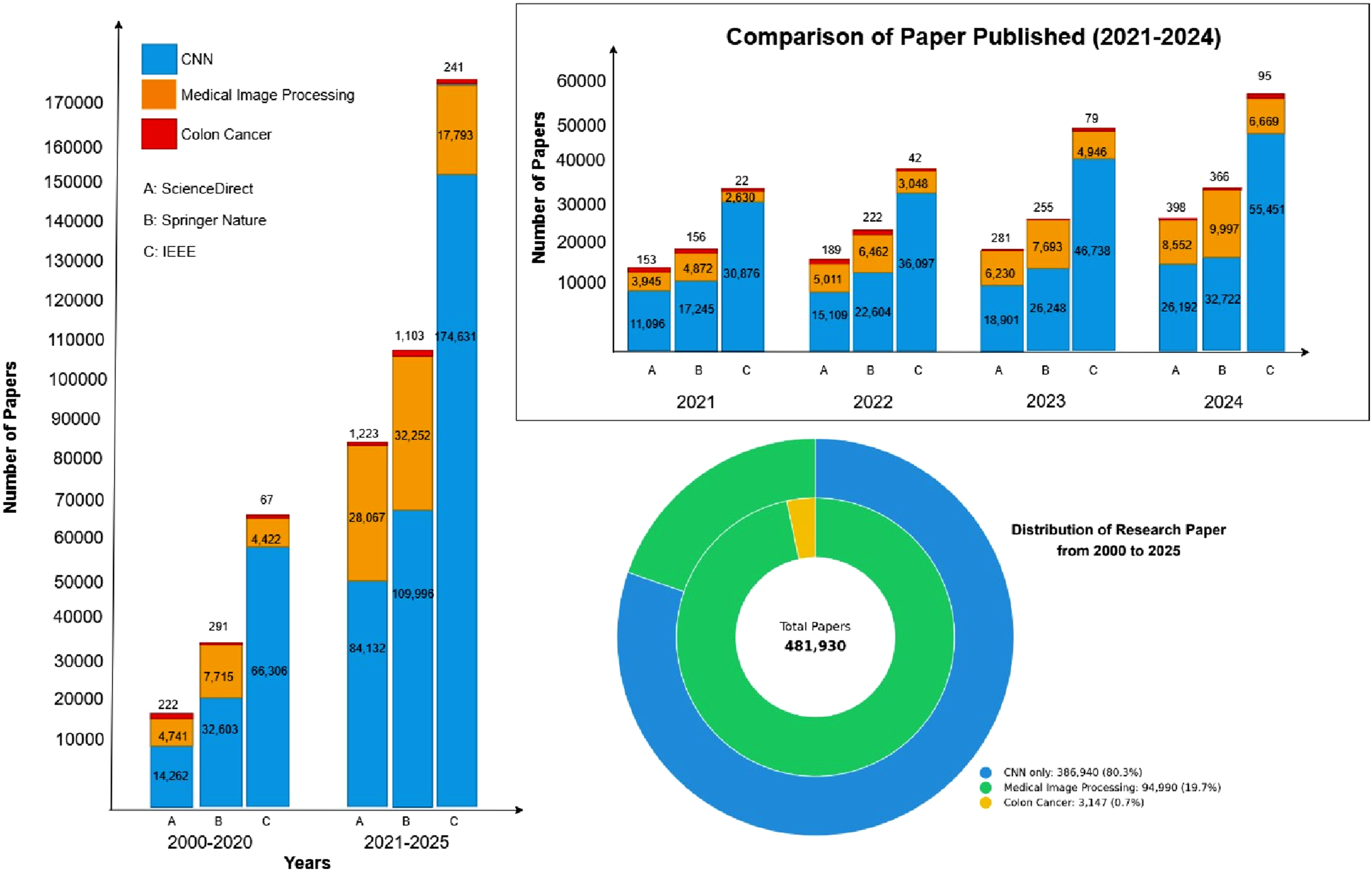
However, only 3,147 (0.7%) of CNN studies particularly looked into colon cancer classification. Specifically, during the last 5 years, 2,567 papers studied state-of-the-art variants of CNN (e.g., Res-Net, Efficient-Net, VGG-Net, Dense-Net, transformer-CNN hybrids, etc.) have been used for the colon cancer diagnosis. 3 In fact, there is a lack of a systematic review with a comparison of the performance of CNN in colon cancer classification tasks. 14 Hence, the aim of the paper is to review the use of various CNN state-of-the-art architectures in colon cancer detection (bi-classification) and multi-classification tasks over the past 5 years.
2. Methodology
2.1. Search strategy
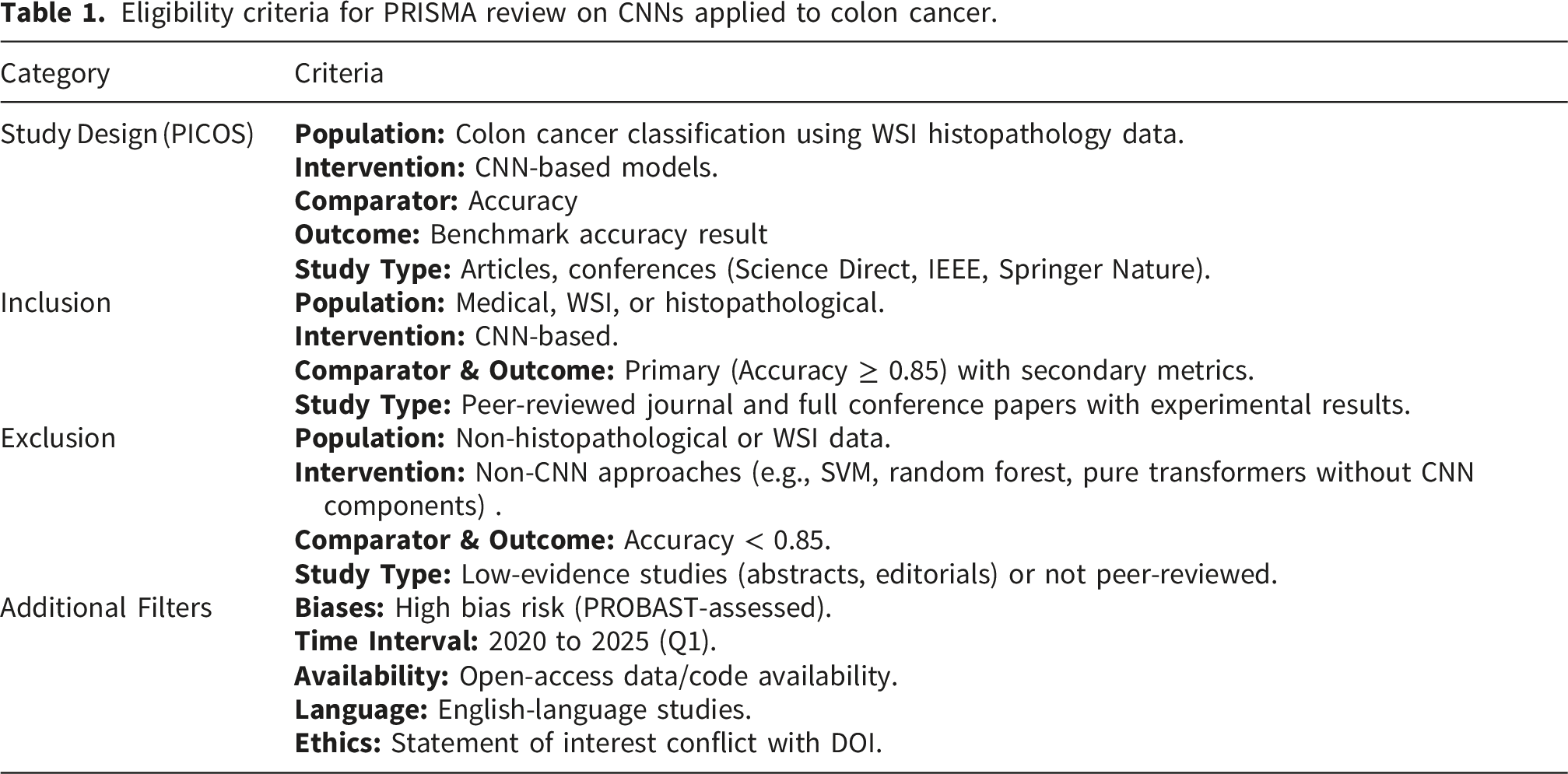
Eligibility criteria for PRISMA review on CNNs applied to colon cancer.
2.2. Data collection, sampling, and selection
We used a stratified two-phase screening process for sampling. First, we investigated the total quantity of related publications from 2000 to 2025. For each included study, we extracted accuracy metrics from text, tables, or figures. Afterwards, this study emphasized the in-depth synthesis. To select qualified sample studies, research title, abstract, and keywords were screened by 2 independent reviewers for relevance, which is the evidence for the further full-text selection in terms of finalization. After the full-text review, the selection was based on the inclusion and exclusion settings in Table 1. The third reviewer validates the results at the end of the selection process.
2.3. Eligibility standard
As shown in Table 1, for the selection of sample articles, the PICOS protocol supervised the process on Population (Medical imaging and image processing data), Intervention (CNN models), Comparator(traditional ML, other DL models, and manual curation), Outcome (Model performance), and Study Type (peer-reviewed journal and conference articles). Inclusion and Exclusion criteria pointed constraint of selection. First, the review processed CNN applications explicitly linking to the PICOS workflow with the PROBAST bias assessment tool.
2.4. Risk of bias and reporting bias assessment
Based on the PICOS design, the PROBAST (Prediction model Risk of Bias Assessment Tool) framework was adopted to systematically evaluate the methodological quality and potential biases of the samples (ResNet, Inception, VGG-Net, Dense-Net, and Efficient-Net) in levels of low, unclear, and high. Each sample was rigorously assessed across four key domains: Participants (representativeness of architecture), Predictors (accuracy in image processing), Outcome (experimental results of accuracy), and Analysis (comparison results). This approach ensured the comparative analysis of CNN architectures accounted for reliable results. 12
2.5. Inclusion and exclusion
The Table 1 outlines clear inclusion and exclusion criteria under the PICOS framework for selecting studies in a systematic review. This selection specifically targets peer-reviewed research published between 2020 and 2025 that uses histopathological whole slide images (WSI) with CNN-based models (including hybrids) to perform classification tasks. Included studies must report a primary accuracy of at least 85%.
2.6. Additional filter
The additional filters (in Table 1) allow the review to prioritize studies with higher quality (using PROBAST evaluation) and relevance beyond the baseline PICOS criteria. The additional filters include restricting the search timeframe of 2020 to early 2025 to capture the latest advancements. The filter include studies with open-access data or code to support transparency and reproducibility to ensure the research specifically addresses tissue classification. Additionally, the filter includes a selection of English-language publications ensures accurate comprehension by the reviewers, while requiring a formal ethics or conflict of interest statement with a DOI ensures the included studies adhere to professional standards of integrity and accountability.
2.7. Reviewer workflow
A three-reviewer workflow is implemented. Reviewer A and B independently conducted the initial screening of titles and abstracts, as well as the subsequent full-text review, based on the predefined PICOS inclusion and exclusion criteria. Then, Reviewer C validated the results at the end of the selection process with PROBAST evaluation (i.e., model development, dataset declaration, result, and validation), additional filters, and disagreements between the two primary reviewers through independent adjudication. The data synthesis was completed by all the reviewers.
2.8. Data synthesis
In this research, quantitative comparisons facilitated data synthesis. Using the most recent five years of research from IEEE Xplore, ScienceDirect, and Springer Nature databases, this research systematically reviewed deeper insights into CNNs architecture designs and applications based on PROBAST evaluation. Reviewers assessed quality of sample studies under the PICOS framework with PROBAST exclusion criteria.
Data synthesis includes accuracy comparison for all 5 state-of-the-art architectures (Res-Net, Inception, VGG-Net, Dense-Net, and Efficient-Net) using a unified formula (in equation (1)). Accuracy
3. Results
3.1. Search results
As shown in Figure 2, the PRISMA flowchart outlines the systematic process of study selection for the review. The process began with the identification of 2,567 records from three databases: IEEE Xplore (344), ScienceDirect (1,124), and Springer Nature (1,099) from 2020 to the first quarter of 2025 without duplicates removed. Flowchart of study selection according to the PRISMA diagram.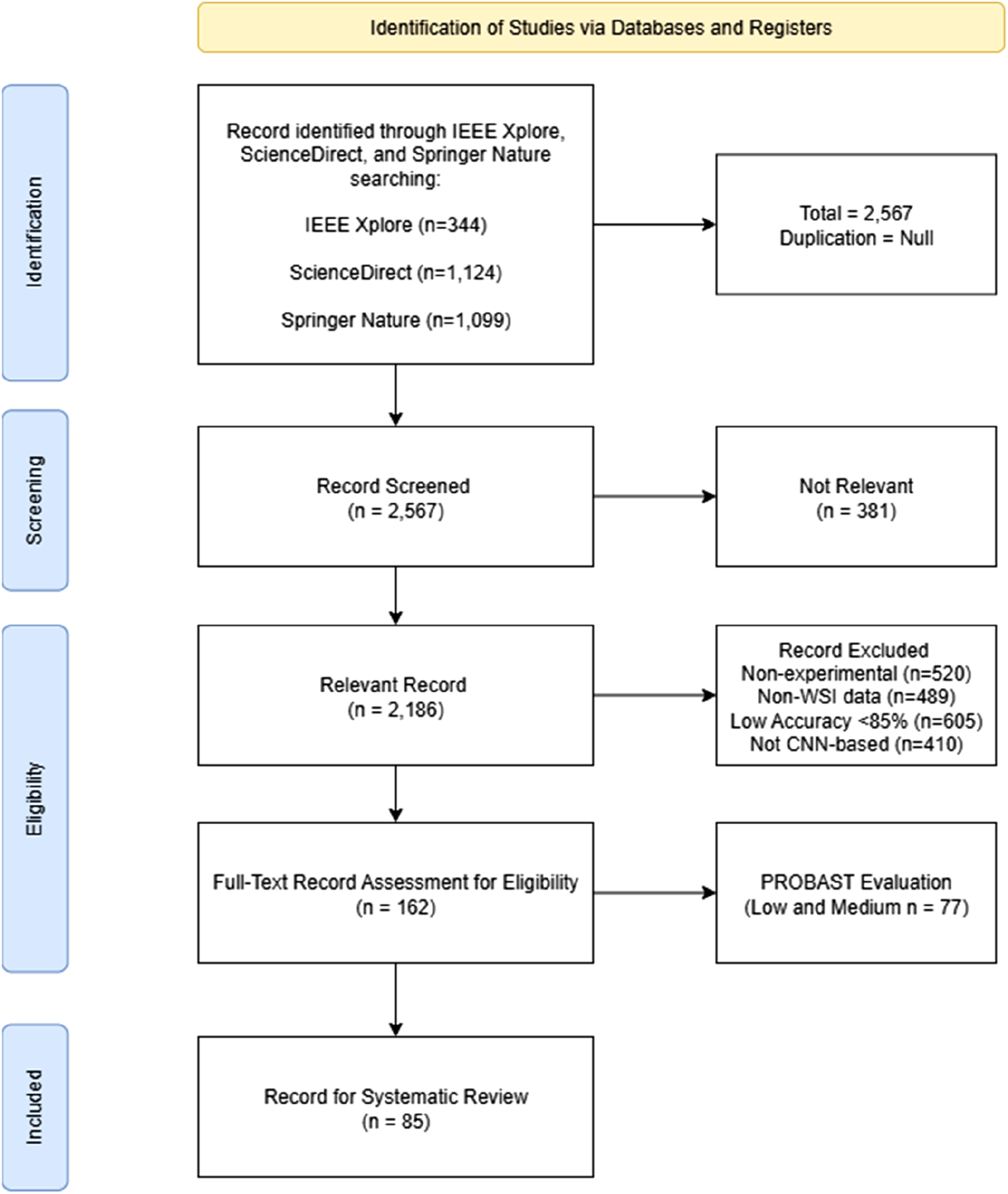
In screening results, 2,186 records were collected, of which 381 were excluded as not relevant. A full-text assessment of 85 records was conducted after the exclusion of non-experimental and non-peer-reviewed design (n = 520), low accuracy below 85% (n = 605), non WSI histopathological (n = 489), and non-CNN-based methods (n = 410). Notably, the sum of these exclusions of full text exceeds the reported 162. After applying the PROBAST tool to evaluate risk of bias, 77 studies with low or unclear risk reliability were ultimately excluded in this review, which is 3.3% of the initially identified sample studies with the consideration of the additional filters (in Table 1). Hence, only the low-risk samples (n=85) were selected in the in-depth review process.
In search results, bi-classification has been achieved at a high level of accuracy using Res-Net, Inception, VGG-Net, Dense-Net, and Efficient-Net architectures. Over the past 5 years, LC25000 (N colon = 10, 000) and Warwick-QU (N = 165) were the most commonly used open datasets for adenocarcinoma/benign issue identification, whereas the multi-classs tasks were realized using NCT-100K (N = 100, 000), CRC-7K (N = 7, 180), TCGA-COAD (N = 192, 312), and EBHI (N = 2, 228) public datasets.
3.2. Residual net
Residual Net (Res-Net) has been successfully applied to medical image classification tasks.
15
Res-Net has been widely adopted for medical image classification tasks, including early work in colon cancer detection.
16
It uses weight layers to train very deep networks that are more accurate in medical image classification, and implemented for colon cancer classification.
17
Res-Net introduced the residual connections or skip connections, allowing information to bypass layers, as shown in Figure 3, H(x) is the output of deep neural network layers based on the residual learning principle (in equation (2)) with x is the original input. Architectural overview of res-net architecture.

BN stands for batch normalization transformation in equation (3). In deep neural layers, μ is mean of the batch with variance (σ2), and the rescaling of the BN requires the learnable parameters γ and β.
The ReLU activation derivatively functions neural networks to improve computational efficiency based on the input x. The key characteristic is in equation (4):
The advantage of Res-Net is driven from its regularizer application. As shown in equation (5), the identity matrix (W
T
) becomes to 0, so it simplifies the workflow and decreases workload of image processing to a
l
.
The addictive feature extraction follows the Residual function (Conv → BN → ReLU stack: 
For the Global Average Pooling l (GAP) ayer, the input x is processed according to equation (7) below:
The final output applied SOFTMAX classification function (in equation 8), Y
c
is the output for channel c (scalar value), β is an inverse temperature parameter (β → ∞ becomes max pooling). The softmax weights sum to 1: 
Thus, Res-Net was introduced in its advantage of skipping connections to solve vanishing gradients, enabling much deeper networks. Average pooling occurs when β = 0, Max pooling means β → ∞, and intermediate β means learned importance weighting.
Performance summary of res-based architectures for bi-/multi- classification.
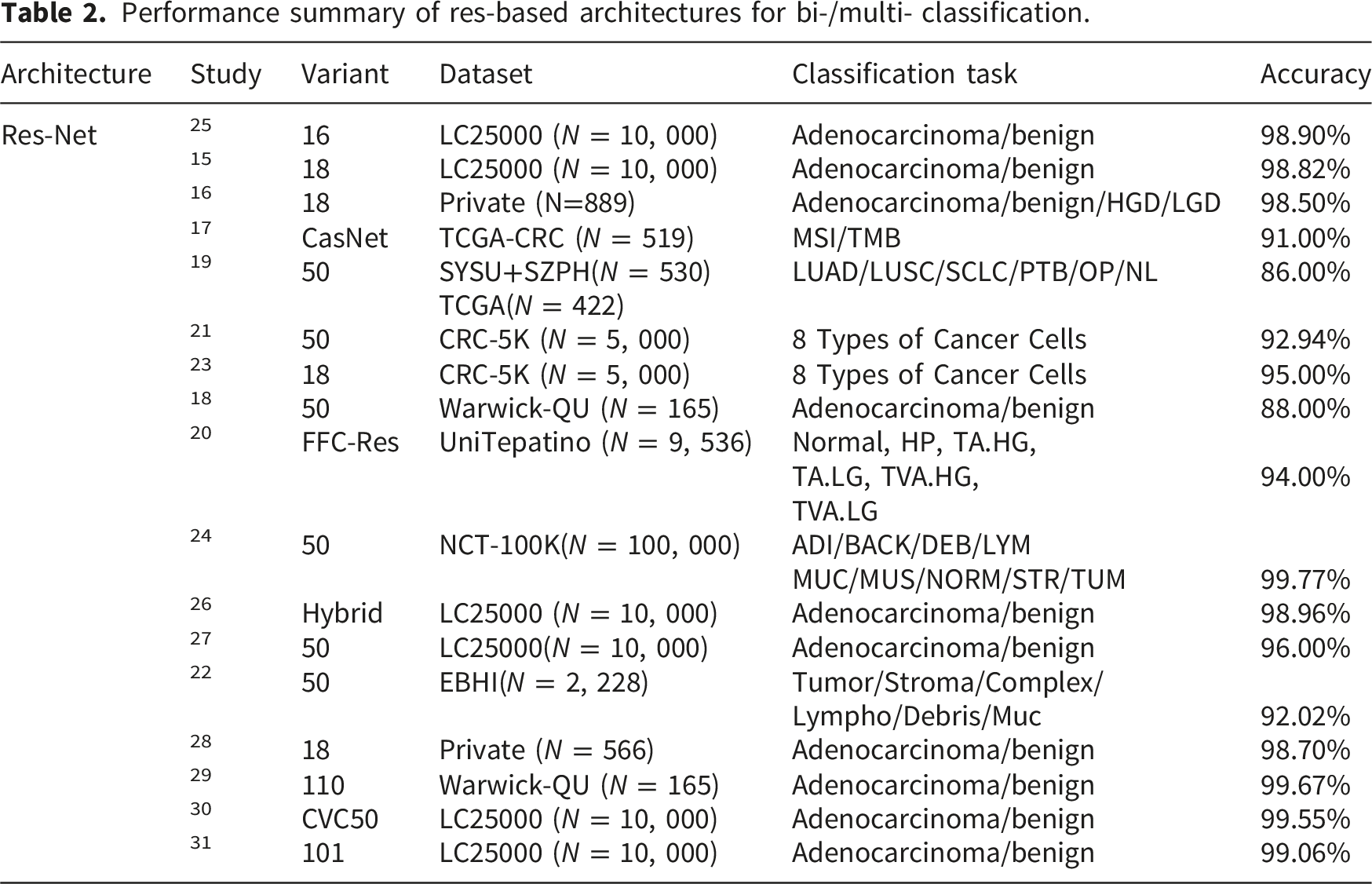
On the other hand, researchers deployed the Res-Net 50 model to realize bi-classification task and improved the accuracy of the model by combining VGG-Net from 83.90% to 96.00%. 27 Another study applied Res-Net 16 and received 98.90% accuracy for lung and colon cancer classification. 25 Res-Net enabled to develop a hybrid model with Xception which surpassed alternative state-of-the-art methods to achieve 98.96% accuracy in cancer classification. 26 In 2024, Haq et al. 28 came up with Res-Net 18 and 50 to deal with colon cancer classification and received 98.70% and 96.66% accuracy. Meanwhile, Alzubaidi et al. 29 received 99.67% accuracy using Res-Net 110 in colon cancer classification. A hybrid model based on the 50 variant achieved 99.50% accuracy. 30 In 2025, research by Deiva et al. 31 used Res-Net achieved the accuracy of classification to 99.06%.
As the result of our PRISMA review, the state-of-the-art multi-classification was from a 50 variant application by Peng and Lee. 24 Their study used NCT-100K reaching 99.77% of accuracy in colon cancer multi-classification with F1 from 99.69% to 100.00% and sensitivity (99.56%). A 110 variant application by Alzubaidi et al. 29 used CLAHE preprocessing to Warwick-QU with 99.67% accuracy in detection (adenocarcinoma/benign) with a specificity of 99.56%, sensitivity of 99.57%, and F1-score of 98.34%, respectively.
3.3. Inception net
Inception architecture looks for wider fitness and feasibility in filter layer of neural models. Inception Net employs inception modules comprising of convolutional layers of varying sizes to determine what is interesting in the incoming images. Inception Net is particularly useful for tasks requiring fine-grained feature extraction, where multi-scale patterns matter.
32
As shown in Figure 4 below, the Inception model adopted the network-in-network concept with multi-scale feature processing to effectively extract features from input data. The distinct characteristic of Inception is the use of local response layer, which works as a normalization tool, in equation (9): Architectural overview of inception baseline.
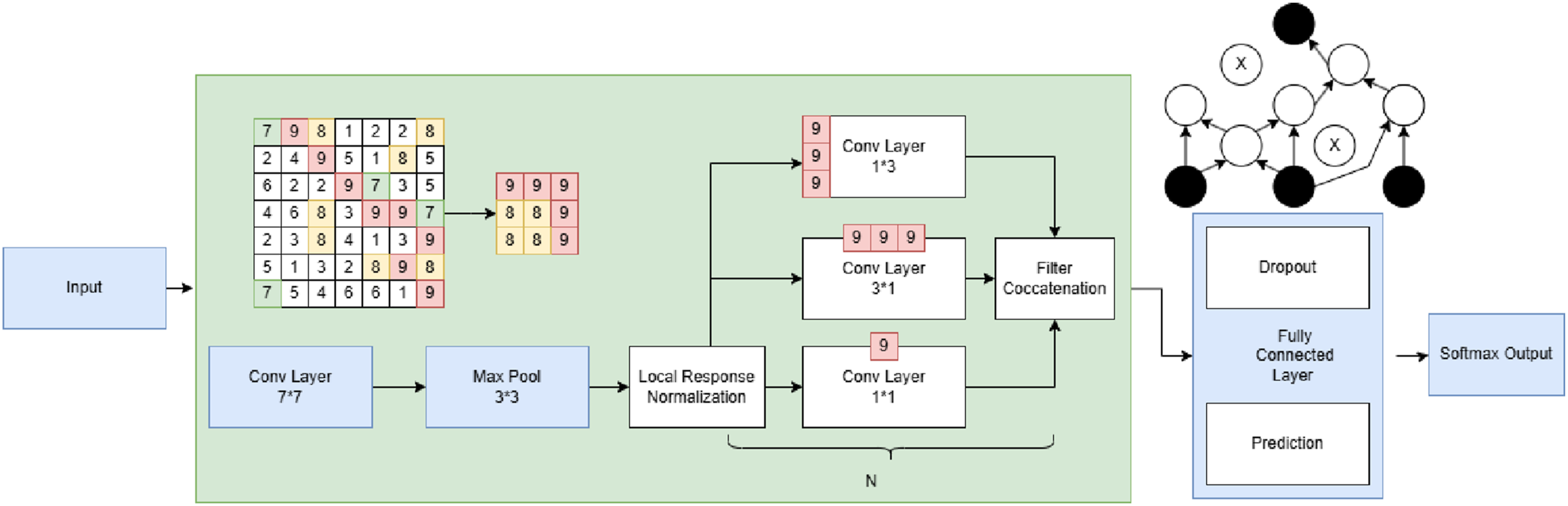
The key characteristic of the Inception model accentuates the use of an auxiliary classifier, which is for loss reduction from the vanishing gradient problem. In equation (10), the L
aux
is the primary loss, N is the batch size, C is the number of classes, yi,c is the ground truth label (1 if sample i belongs to class c, 0 otherwise), with the pi,c is the predicted probability for sample i and class c.
The feature extraction shown in the architecture diagram (Figure 4) of Inception adopted concatenation filter (Eg.11):
Performance summary of inception-based architectures for Bi-/multi- classification.
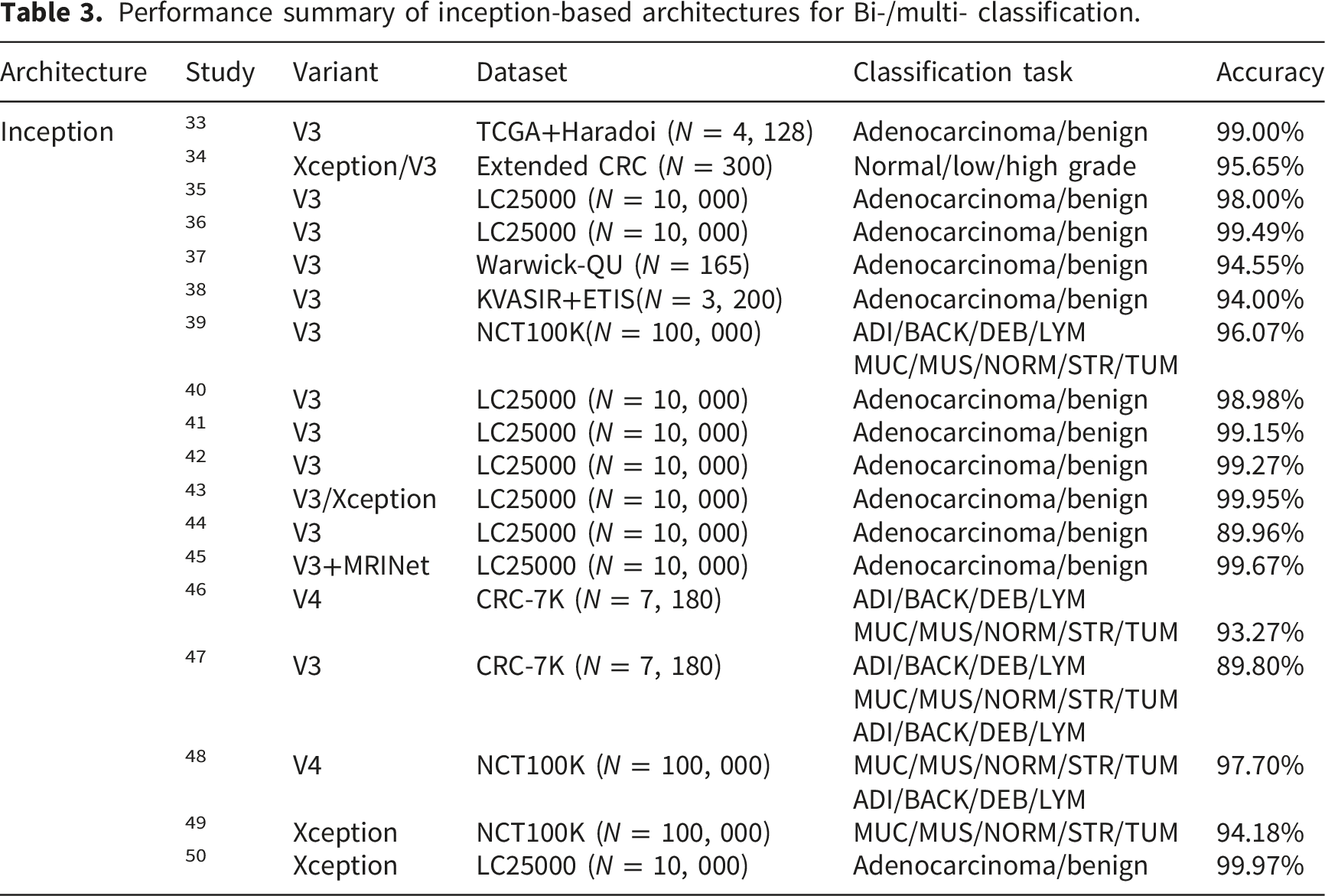
Researchers utilized the V3 variant for bi-classification. The model outperformed multiple competing CNN models with an accuracy of 99.49% 36 on the WSI dataset. Swarna and Hashi 37 designed a model using Inception V3 that achieved 94.55% - 99.40% accuracy on different datasets, while the model 38 resulted in 94.00% accuracy in extensive experiments. Appavu 40 used V3 for colon cancer classification and received a comparatively high accuracy of 98.98%. Ochoa-Ornelas et al. 41 proposed a model for colon cancer classification using the Inception and Res-Net models resulting in 99.15% accuracy, and Merabet, et al. 42 achieved 99.27% accuracy using the same model. Kumar, et al. 43 adopted Inception V3 and their classification result was 99.95%. A hybrid model handling multi-modal data showed 89.96% accuracy for the lung and colon cancer classification. 44 The V3 variant was adopted with MIRNET in 99.67% accuracy. 45 In 2025, the Xception variant outperformed the others with an accuracy of 99.97% by Uyar, et al.
Lastly, Inception V4 model was adopted for colon cancer classification task in 2022 by with 93.27% accuracy. 46 The variant was further improved with 97.70% accuracy by Patnaik, et al. 48 Wang, et al. 39 applied Inception V3 model for colon cancer classification resulting in 96.07% accuracy based on NCT-100K dataset. Gupta, et al. 47 compared Rer-Net, Inception V3, and VGG 16 and 19 variant. Their results showed the best accuracy was achieved by Inception V3 model in 89.80%. Kumar, et al. 49 used Xception achieved 94.18% accuracy in colon cancer classification using the NCT-100K dataset.
As the result of the PRISMA analysis, Kumar, et al. 49 achieved 94.18% accuracy with sensitivity of 92.74%, specificity of 94.80%, F1 of 93.75%, and AUC of 94.48% using the Xception based on NCT-100K dataset for the multi-classification task. Although, Xception model outperformed the traditional Inception variants with 99.97% accuracy, 50 the dataset information is missing without a demonstration of the secondary metrics in terms of low reproducibility. As the result of detection tasks, the most promising accuracy of Inception was observed in the research by Kumar et al., 43 who extensively combined Inception with Res-Net on the LC25000 dataset, resulting in 99. 95% accuracy and a 99.95% F1 score and 100% sensitivity.
3.4. Visual geometry group net
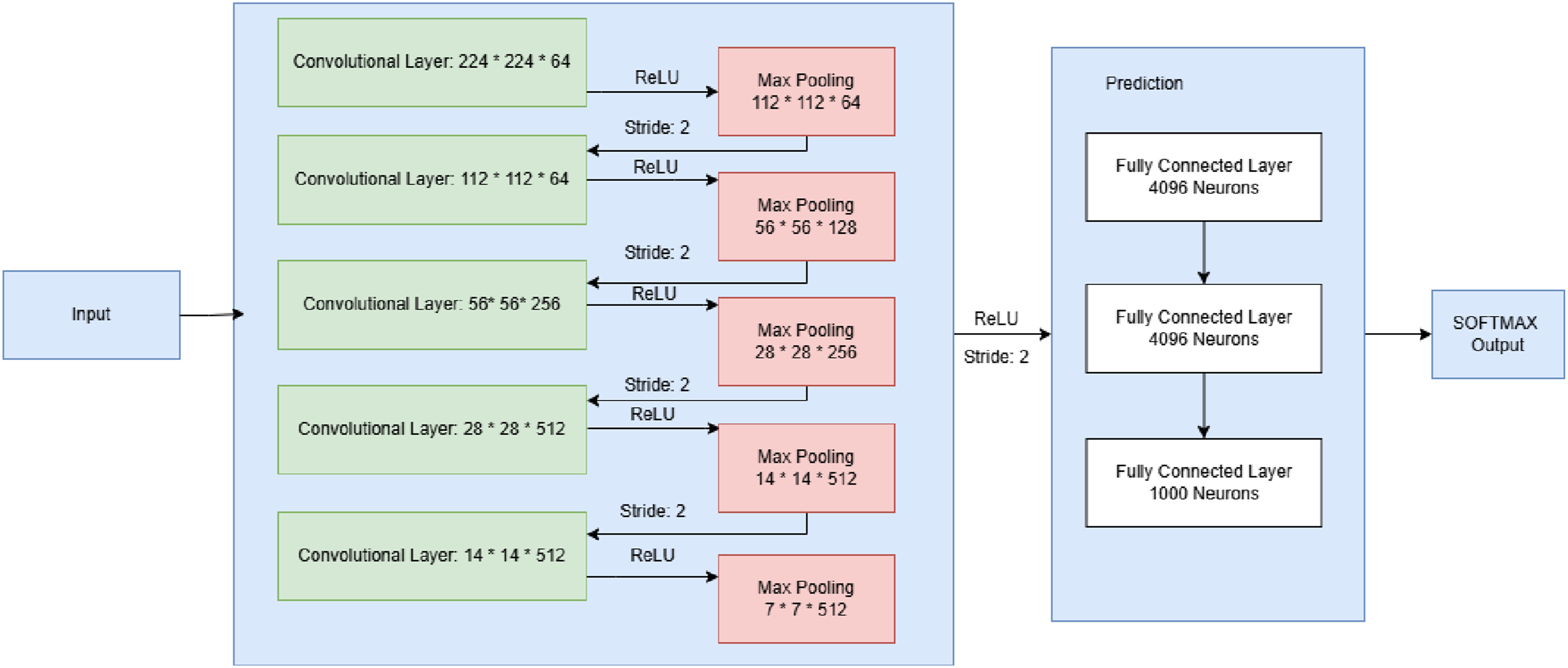
Visual Geometry Group (VGG) works impressively at colon cancer classification tasks. The VGG-Net model was launched in 2014 by academics at Oxford University to outperform AlexNet, the previous state-of-the-art CNN architecture.
51
As shown in Figure 5, VGG-Net stacks multiple convolutional layers in sequence, unlike Inception or Res-Net, which use parallel or skip connections. Comparing to the previous architecture, the distinguishing feature of VGG is the application of chain rule (in equations (12) and (13)) for vanishing gradients in deep layers without cross-layer feature reuse (in equation (14)), where gradients ∏
l
∂f
l
/∂fl−1 → 0 for large L. VGG-net baseline (16) architectural overview. Performance summary of VGG-based architectures for bi-/multi- classification.


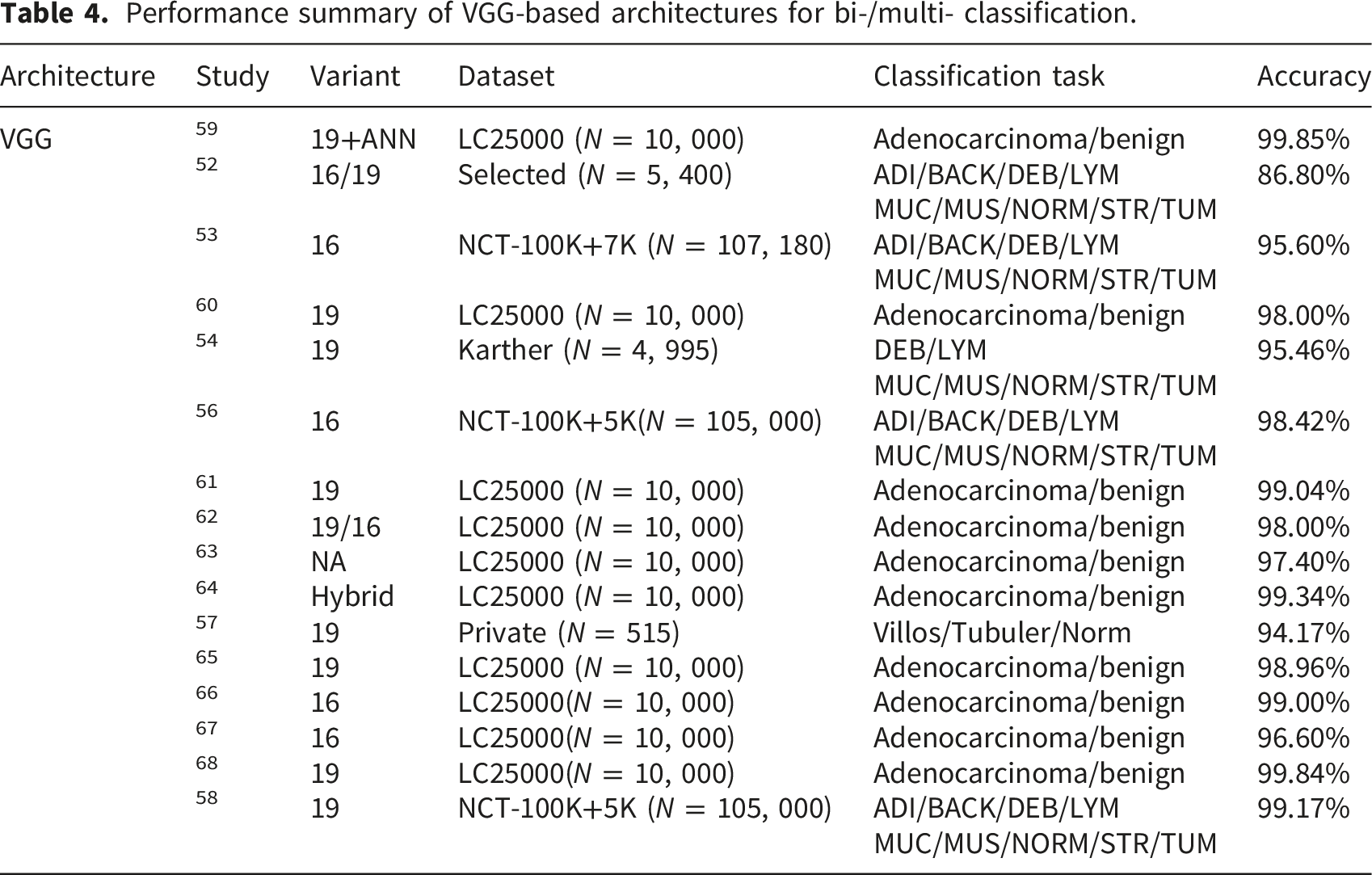
A benchmark on bi-classification reported strong results (99.85% accuracy) by adopting the VGG-Net 19 with ANN structure. 59 Rawashdeh, et al. 61 compared VGG-Net 16 and 19 variant. Their results showed the best accuracy was achieved by the 19 in 99.04%. Yildiz, et al. 62 tested VGG in handling input histopathological data to recognize colon cancer with 98.00% accuracy. Hossain 63 proposed a VGG model to identify lung cancer cells with 97.40% accuracy. Hasan and Oraibi 64 classified colon cancer histopathology photos with a VGG-Net 19 model and published their results in accuracy of 99.34%, more accurate than many competing CNN models. In 2023, a promising result of using VGG-Net to detect colon cancer tissues was obtained by Hadiyoso, et al. 65 in 98.96% using VGG-Net 16. Singh and Singh 66 used VGG-Net 16 achieved 98.00% in the same year with WSI dataset. In 2024, Akar, et al. 67 claimed that the adoption of VGG resulted in 96.60%accuracy, while Singh et al. 60 achieved an accuracy of 98% through the utilization of VGG-Net 19 in colon cancer detection. Lastly, Fahadipour and Aref 68 applied the 19 variant and achieved 99.84% accuracy for colon cancer classification using WSI dataset.
As the PRISMA result, the hybrid ANN + VGG-19 variant
59
achieved the highest accuracy (99.85%) and F1 = 99.92% of the bi-classification among the samples, with a sensitivity of 99.85%, a specificity of 100%, and an AUC of 99.86% using LC25000. The highest accuracy of multi-classification was achieved by the 19 variant model by Khazaee et al.
58
in 99.76% accuracy with F1 ≥ 99.60% using NCT-100K and CRC-5K datasets. Hamida et al.
56
tested the 16 variant, and their result showed 98.42% accuracy with sensitivity
3.5. Dense net
Dense-Net is a CNN model that has been prevalently used in the detection of colon cancer.
69
Being different from the abovementioned CNN architectures, Dense-Net employs multiple dense-blocks to boost non-linear transformational feature learning by adding new features from each concatenation. Meanwhile, Dense-Net addresses vanishing gradients and overfitting through its design, which was intended to optimize CNN architectures (See Figure 6). Densely-linked blocks in this model enhance accuracy by maximizing feature reuse across convolutional layers while optimizing gradient propagation in densely-connected Convolutional Networks.8,70 Architectural overview of dense-net baseline (121) architecture.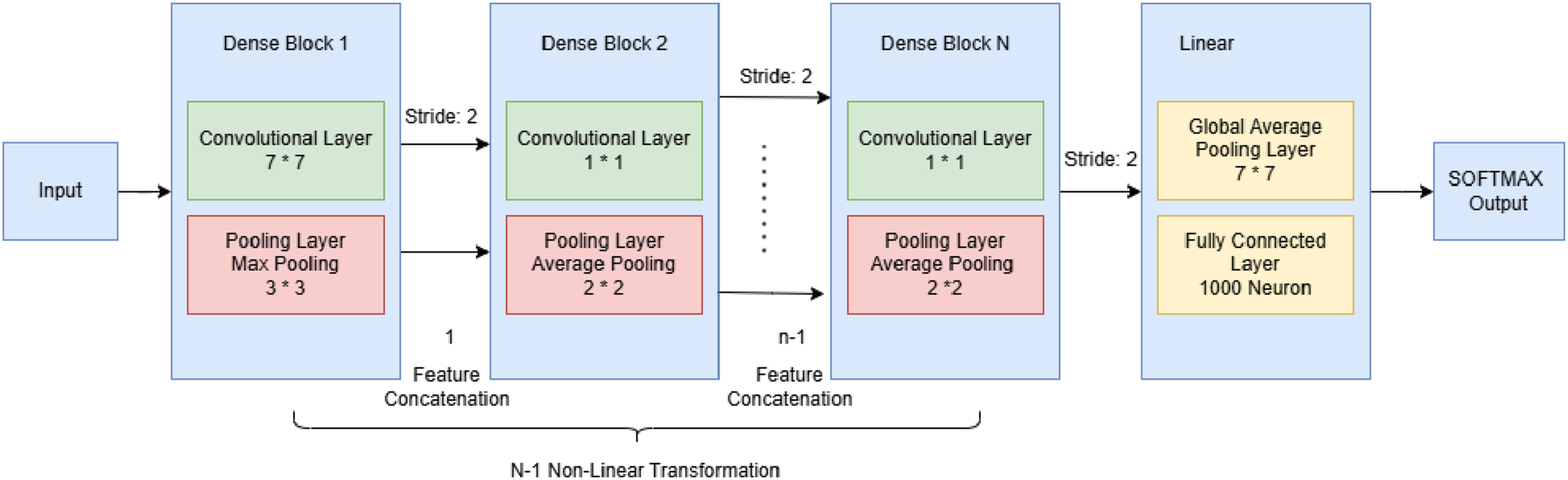
Despite the similar architecture design from previous review, equation (15) interprets the feature transformation at a macro network level of reuse:
Also, Dense-Net differs from other CNNs and has a dense connectivity pattern with a composite function for concatenative feature reuse in equation (16) different from the design of each layer.
Further equation (17) explains Gradient of loss 
Similar logic as Res-Net and VGG-Net, Dense-Net employs global average pooling layer (equation (7)), fully connected layer, and SOFTMAX (equation (8)) for the final linear prediction. The main characteristic of Dense-Net is the feature reuse, which significantly boosts its informational efficiency. However, the size of the architecture varies based on the number of dense blocks in feature reuse.
Performance summary of dense-based architectures for bi-/multi- classification.
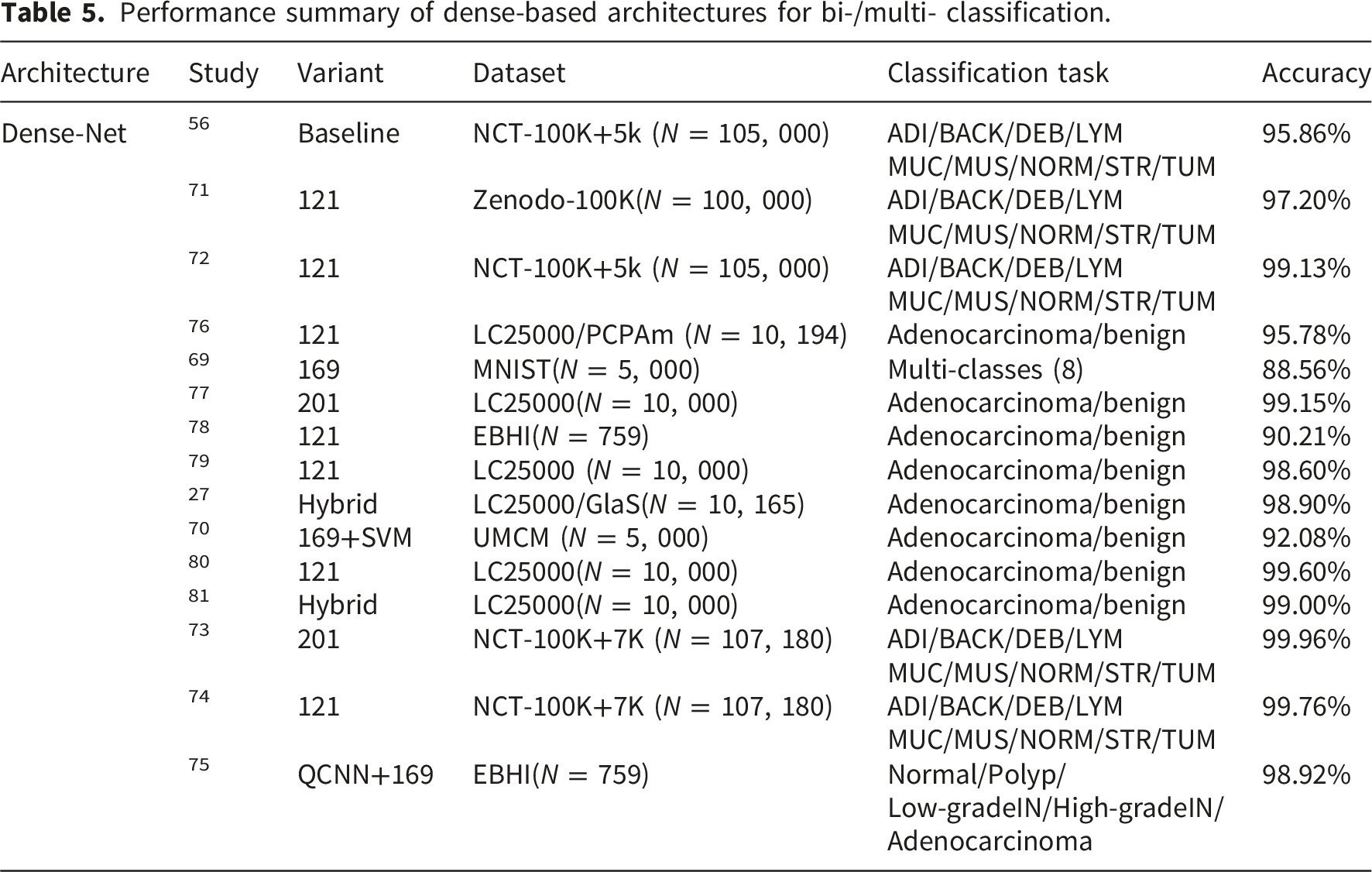
For bi-classification task, a design of Dense-Net 201 model showed 99.15% accuracy. 77 A 4-stage CNN model with a RNN classifier for hyperspectral image processing employed a hybrid model that contained Dense-Net 121 to classify colon cancer histological slides 78 with 90.21% accuracy. Another benchmark study conducted by Kumar et al. 79 showed that 98. 60% in 2022 used histopathological WSI data for the detection of colon cancer. Dense-Net was a widely used in histopathology visualization, such as colon cancer detection. Gowthamy et al. 27 found that their Dense-Net hybrid model for colon cancer histopathology image classification achieved a test accuracy of 98.90%. An application of the hybrid deep and machine learning approach by Dense-Net 169 with SVM was examined by Ohata et al., 70 and their result showed 92.08% accuracy. The same variant was tested by Lauande, et al. 76 resulting in 95.78% accuracy. Sarwinda et al. 18 designed a Dense-Net 121 model as a colon cancer detection tool that had an accuracy of 98.95%. Considering all the aspects described in the previous section, Dense-Net can be considered as a robust architecture for detecting colon cancer. A model based on Dense-Net 121 was examined in colon cancer detection using 10,000 histopathological image, and the result showed 99.60% accuracy in detection. 80 Due to its dense connection structure that favors better gradient flow and re-using features, it may perform well with only a fraction of the parameters. Di Giammarco et al. 81 proposed an experimental model that achieved 99.30% accuracy in colon cancer detection. The performance of Dense-Net still has areas for improvement, and its application in medical image analysis scenarios can be further expanded by extending to other CNN layouts or RNNs.
The results with the potentially near-perfect accuracy were obtained from the research by Hasan et al. 80 with a 99.60% accuracy with 99.44% F1 score in a 121 variant model using the LC25000 dataset in detection tasks. Uddin et al. 73 achieved an accuracy of 99.96% via a self-designed Dense-Net as their noval framework for the multi-classification task with AUC of 1.00, Recall:99.96%, Specificity: 99.99%, and F1 score: 99.96%, alternatively using the datasets of NCT-100K and CRC-7K.
3.6. Efficient net
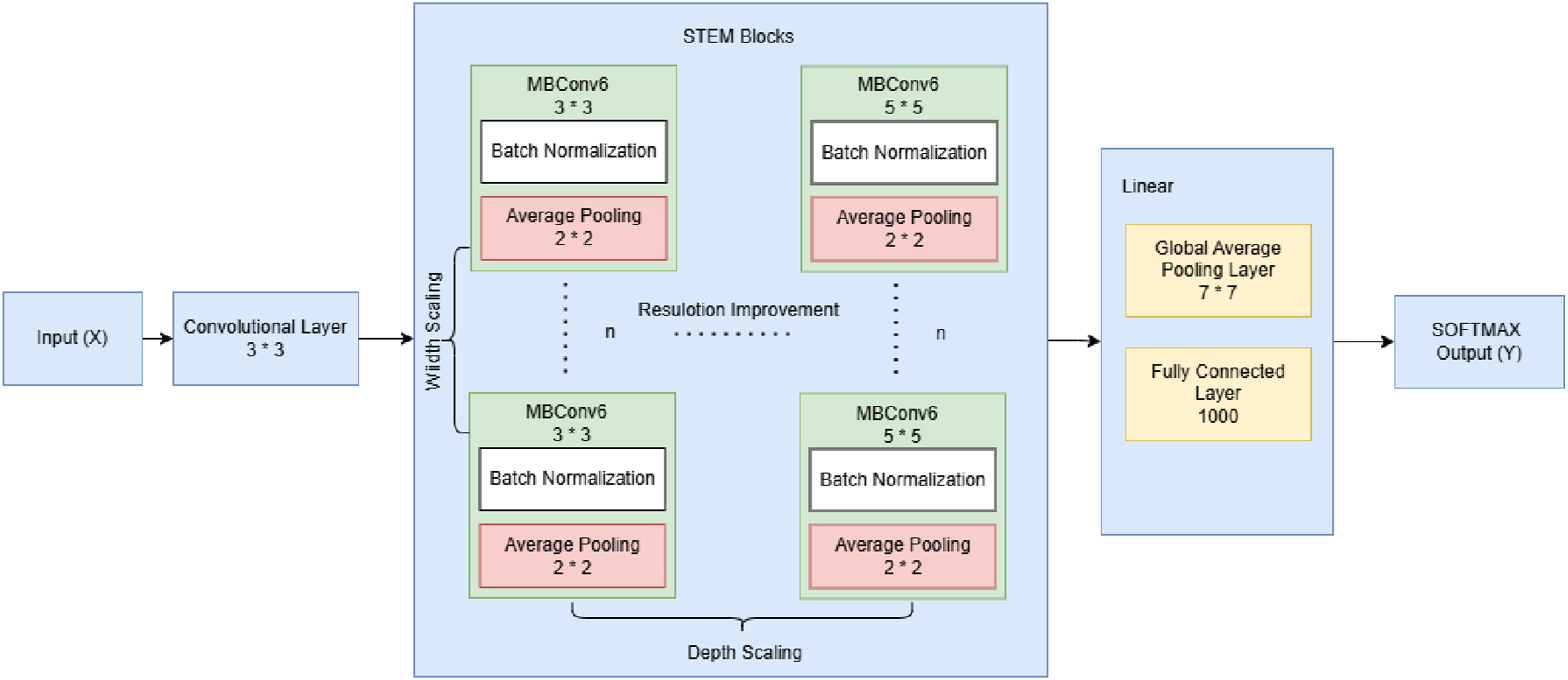
As shown in Figure 7, rather than scaling only one dimension (like depth in VGG-Net or width in Res-Net), Efficient-Net uses a compound scaling method to simultaneously scale to optimize the network architecture depth, width, and resolution concerning accuracy
82
in stem block. The Efficient-Net family of CNN architectures is faster and performs better on the Bidirectional Encoder Representations from Transformers (BERT) machine learning model with fewer parameters.
83
The key characteristic of Efficient-Net is the design of Mobile Inverted Bottleneck Convolutions (MBConv). The Efficient-Net model starts with input normalization (equation (3)) to use RGB standard deviation (σ) and mean (μ) to normalize the input x as x = x − μ/σ. Further, Efficient-Net has a compound scaling layer to calculate the depth (α), width(β), and resolution (γ) of input data in a constraint shown in equations (18) and (19), in the STEM Block shown in Figure 7. Efficient-net baseline (B0) architectural overview.

Then, the STEM block consists multiple MBConv blocks process input x into features
First, a 1 × 1 convolution with weights 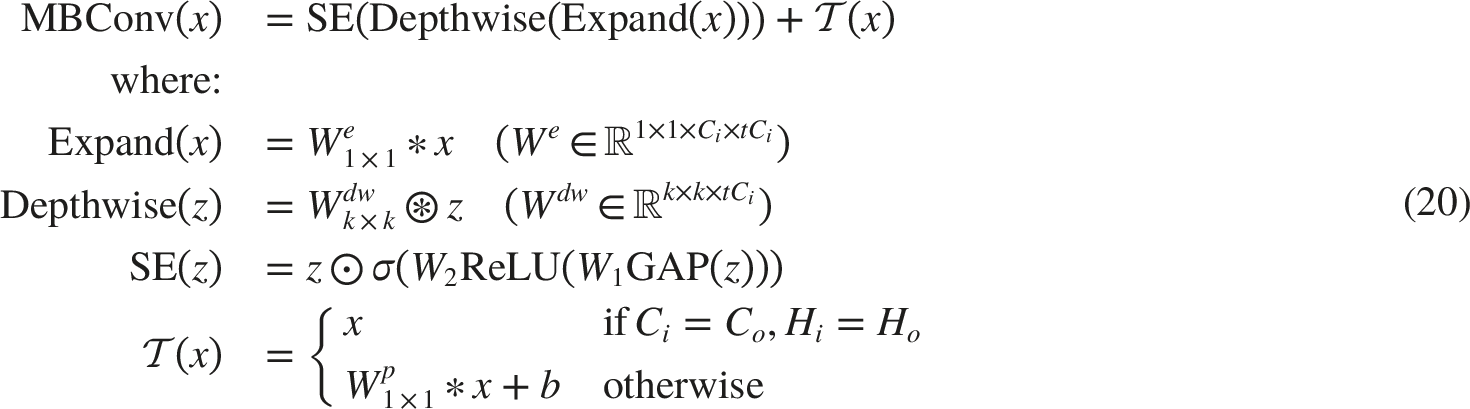
For the multi-classification tasks, Prezja, et al. 84 used V2 model with ViT achieved 99.89% accuracy using the NCT-100K dataset. Another benchmark model adopted the B0 variant 85 achieved 99.87% accuracy using the same dataset. Li, et al. 86 applied V2 with Swin architecture for the multi-classification task achieved 96.00% accuracy also with the NCT-100K dataset.
Performance summary of efficient-based architectures for bi-/multi- classification.
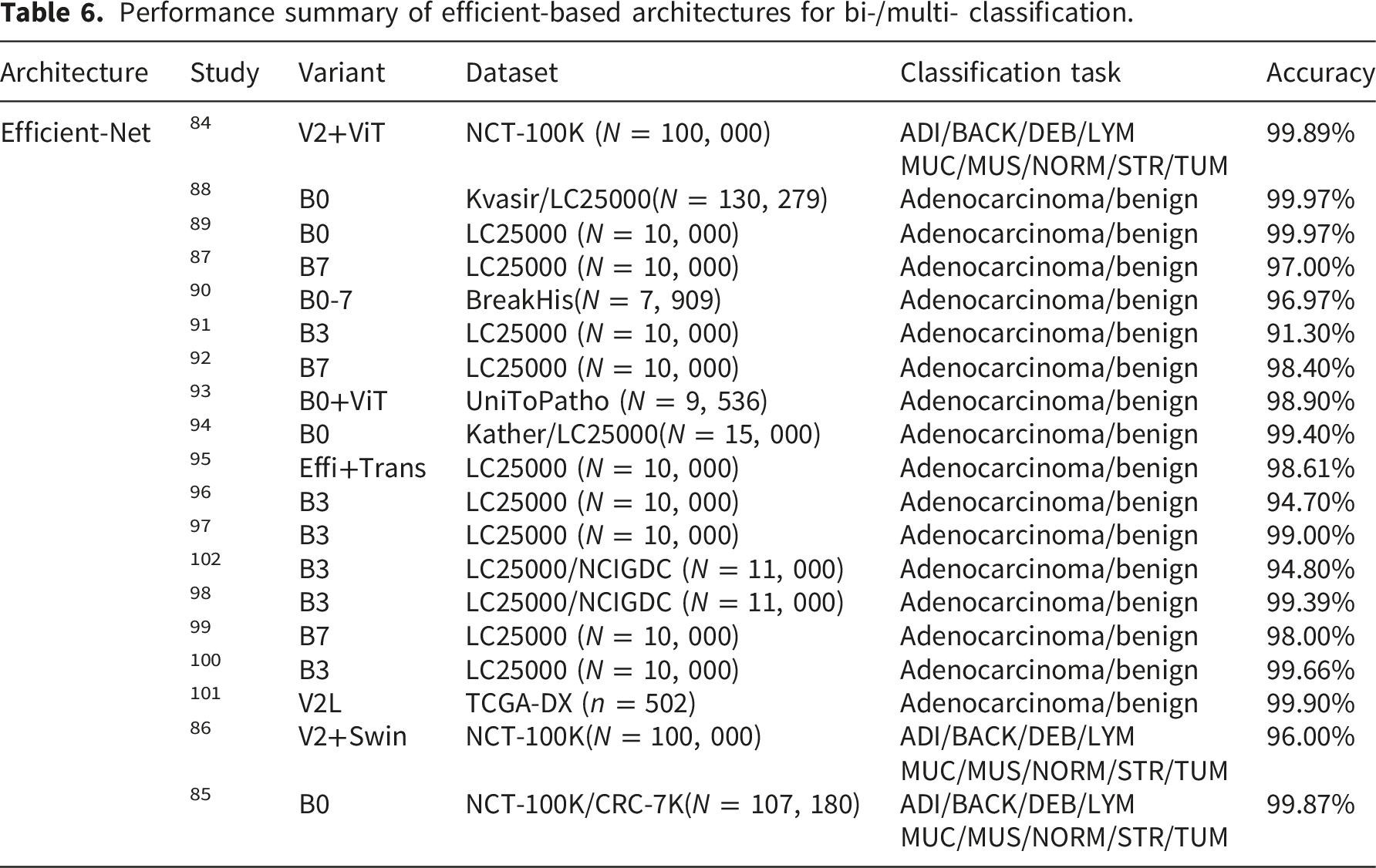
As a result of PRISMA analysis, Efficient-Net demonstrates remarkable effectiveness in classification through its innovative compound scaling approach. The most promising bi-classification result was observed in the application of V2L hybrid variant by Saba, et al. 88 (Recall = 100.00%, F1 =99.93%, AUC = 100.00%) and Taher et al. 89 (Recall =100.00%, F1 = 100.00%) both achieved 99.97% benchmark accuracy based on the LC25000 dataset, while maintaining lower computational requirements compared to traditional CNNs. The highest multi-classification accuracy (99.87%) was achieved by the B0 model 85 (Recall = 94.52% and F1 =94.41%) using NCT-100K and CRC-7K datasets.
4. Discussion
4.1. Benchmark comparison
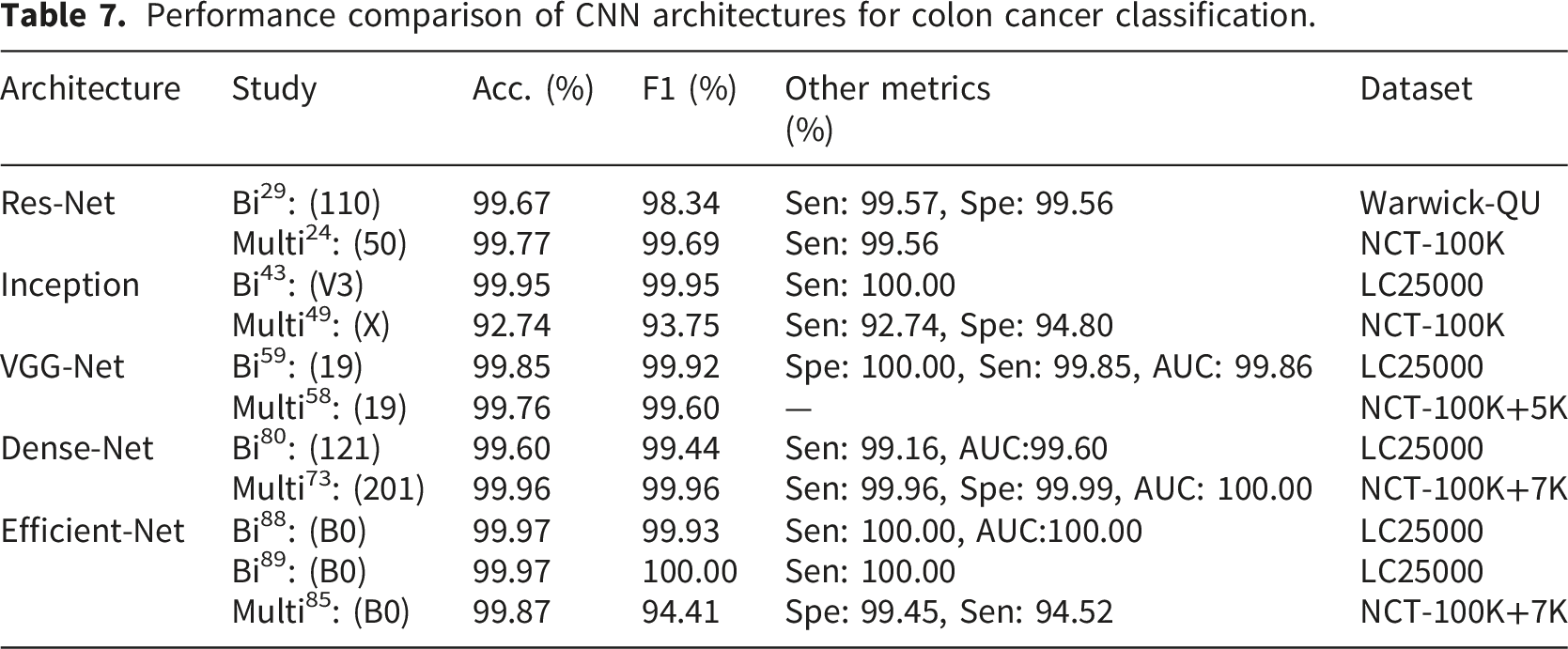
Performance comparison of CNN architectures for colon cancer classification.
Summary and quantitative comparison of CNN architectures for classification tasks.
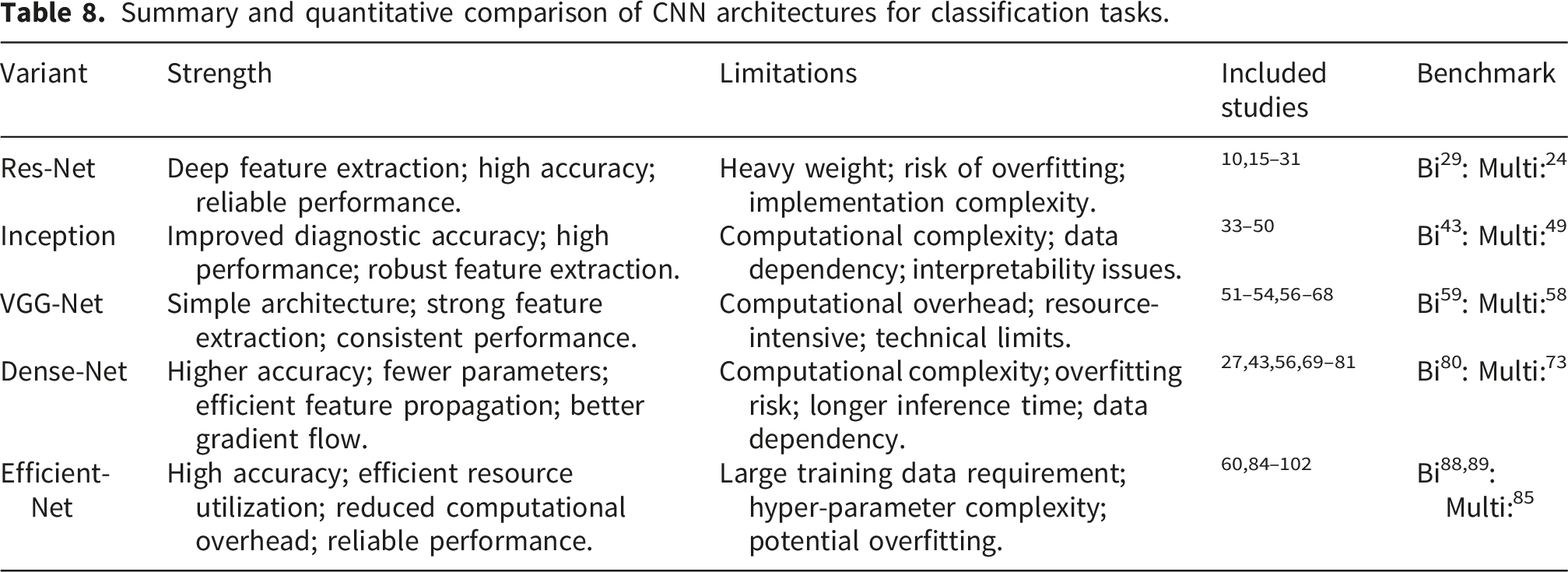
In Table 7, the 110 variant showed the highest accuracy (99.67%) with a remarkable F1 (98.34%) for the bi-classification using the Warwick-QU dataset. 29 Peng and Lee 24 applied the 50 variant model, achieving the highest accuracy (99.77%) with 99.69% F1 and 99.56% sensitivity using the NCT-100K dataset. These remarkable performance metrics indicate the Res-Net excels in deep feature extraction due to its feature of skip connection and mitigates vanishing gradients (equation (6)) for classification tasks. The major limitation of Res-Net application emphasizes on the heavy parameterization, which increases computational costs with overfitting risk, especially in smaller datasets.20,28 Research by Raseena et al. 103 demonstrated that while ResNet50 achieves robust performance across colorectal polyp datasets, regularization techniques are essential to address overfitting concerns, with their proposed model (recall ≥87%) across 4 benchmark datasets.
The benchmark study for bi-classification by Kumar et al. 43 used the V3 variant achieved top-tier accuracy (99.95%), F1 (99.95%), sensitivity (100.00%). For the multi-classification task, Kumar, et al. 49 adopted Xception achieved 94.18% marked as the highest accuracy with 93.75% F1, 92.74% sensitivity, and 94.80% specificity. These performance metrics are lower than its counterparts’ in multi-classification task. The most significant strength of the Inception architecture is its filter design, which optimizes multi-scale feature extraction (see in equation (9)). However, its high computational complexity and dependency on large datasets limit performance in multi-classification.38,47 Recent comparative analyses by Raseena et al. 104 revealed that V3 exhibited relatively poor performance compared to VGG and Res-Net variants, with InceptionResNetV2 ranking as the least effective performer in terms of recall and precision. This finding underscores the need for architectural refinement and optimization for colon cancer image classification.
The state-of-the-art VGG-Net study by Al-Jabbar et al. 59 achieved the highest accuracy (99.85%) with F1 (99.92%), specificity(100.00%), sensitivity(99.85%), and AUC (99.86%) in bi-classification tasks using the 19 variant. For the multi-classification task, 99.76% accuracy was achieved by Khazaee, et al. 58 using the 19 variant with 99.60% F1. The advantage of the architecture is its uniform 3*3 convolutional layers that simplify the architecture but remain effective in feature extraction due to the applied chain rule (in equations (12) and (13)) for vanishing gradients in deep layers without cross-layer feature reuse (in equation (14)). Nevertheless, the limitation of the architecture accentuates the excessive resource consumption due to high parameter count and computational cost.56,58 The performance hierarchy established by Raseena et al.103,104 confirmed VGG19 as the top-performing model and demonstrated superior accuracy across benchmark datasets. However, this superior performance comes with substantial computational demands, as documented in comparative complexity analyses. 58
The benchmark study in Dense-Net used the 121 variant by Hasan et al. 80 achieved highest accuracy (99.60%) in bi-classification with sensitivity in 99.16%, F1 in 99.44%, and AUC in 99.60%. Uddin et al. 73 in multi-classification resulted 99.96% accuracy with 99.96% F1, 99.96% sensitivity, 99.99% specificity, and 100.00% AUC. The strength of Dense-Net is feature reuse (in Equation (16)), which improves parameter efficiency and gradient flow, achieving the near-perfect accuracy (99.99%) among all the samples reviewed. However, the limitation of Dense-Net is obvious in memory-intensive training and slower inference times.76,78 Haryanto et al. 105 successfully optimized DenseNet121 through hyperparameter tuning, achieving 98% accuracy with 19.5 seconds training time using NVIDIA A100 accelerator. Hence, careful parameter selection can partially mitigate computational demands. Their research concluded that Dense-Net 121 with a 75% freeze rate, zero hidden layers, a learning rate of 0.001, and the RMSProp optimizer achieves optimal performance.
Lastly, the Efficient-Net highlights suitability for resource-constrained environments. In bi-classification tasks, Saba et al. 88 and Taher et al. 89 both achieved 99.97% benchmark accuracy based on the LC25000 dataset. Both of them demonstrated remarkable F1 and sensitivity. For the multi-classification task, the B0 model achieved 99.87% with 99.45% specificity and 94.52% sensitivity. 85 The advantage of using the architecture is the depthwise separable convolutions with compound scaling optimize accuracy with minimal computational cost (in equation (20)). However, its limitation indicates the architecture sensitivity to hyperparameter and requires extensive data augmentation.91,93 Novel lightweight architectures continue to emerge, with Dabass et al. 106 proposing a clinically comparable CNN framework incorporating Enhanced Convolutional Learning Modules (ECLMs) and attention learning modules that achieved 97.7% accuracy on NCT-100k and 98.83% on Kather-5k datasets, with validation scores exceeding 9.0 from expert pathologists. Similarly, EL-CNN architectures 107 with spatial pyramid pooling and enhanced convolutional block attention modules (ECBAM) have demonstrated 99.48% accuracy on NCT-CRC-HE-100K with only 3.72 million parameters, proving that robust performance and low complexity can coexist for clinical applications.
4.2. Result synthesis
Further summarization indicated Dense-Net architecture achieved the highest accuracy in both bi- and multi-classification tasks. The Figure 8 further synthesized findings based on the analysis results into a comparative matrix on the dimensions of depth of feature extraction, simplicity, efficiency, robustness, and resource intensity. Comparison matrix.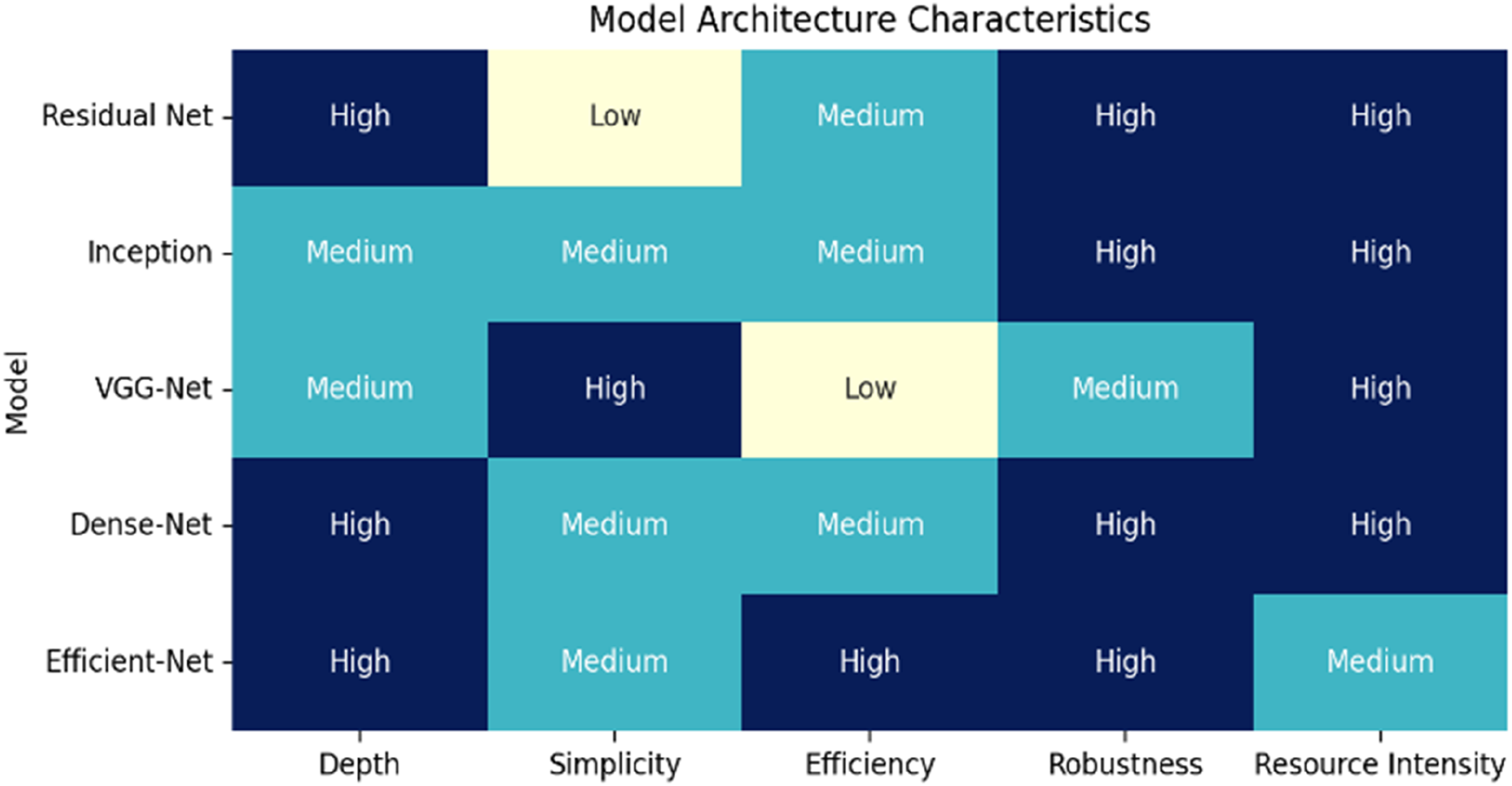
Res-Net demonstrates high depth and robustness due to its skip connections enabling deep networks, but suffers from low simplicity and high resource intensity.
29
Inception offers medium depth and simplicity through its multi-scale branches,
43
with high robustness but also high computational costs.
37
VGG-Net stands out for its high simplicity from uniform 3× 3 convolutions,
65
yet has low efficiency and medium robustness.
60
Dense-Net achieves high depth and robustness via dense connections,
74
though its medium efficiency comes with high resource demands.
18
Efficient-Net excels with high depth, efficiency, and robustness,
73
balancing these with medium resource intensity despite requiring large datasets. Together, these results highlight the trade-offs between architectural complexity, computational efficiency, and performance, with newer models like Efficient-Net and Dense-Net offering superior balances for colon cancer classification tasks. The synthesis highlighted two critical trends, which are
However, the review’s reliance on accuracy as the primary comparative metric, necessitated by inconsistent reporting of secondary metrics across benchmark studies, points to a broader issue of reproducibility in the field. A significant portion of the high-performing studies identified in this review, particularly those utilizing the LC25000 dataset, risk overfitting to dataset-specific artifacts rather than learning genuine disease morphology. The LC25000 dataset, while large and well-annotated, consists of carefully curated, tiled images from a limited number of sources. As highlighted in studies on domain shift,7,13 models trained on such homogeneous data often fail to generalize to external clinical populations. For instance, a model achieving 99.9% accuracy on LC25000 might see its performance drop precipitously when tested on whole-slide images from a different hospital system using a different scanner or staining protocol—a challenge underscored by the cross-dataset validation issues in Yang et al., 19 where ResNet-50 accuracy varied widely from 54% to 86% across different datasets (SYSU1, SYSU2, TCGA, and SZPH). The reliance on a few public datasets (LC25000, NCT-100K, Warwick-QU) creates a risk of ”benchmark overfitting,” where the research community collectively optimizes for performance on these specific data distributions, potentially neglecting the vast heterogeneity of real-world clinical data. 13
5. Implications
5.1. Architecture design
CNN architecture and hyperparameter optimization strategies.
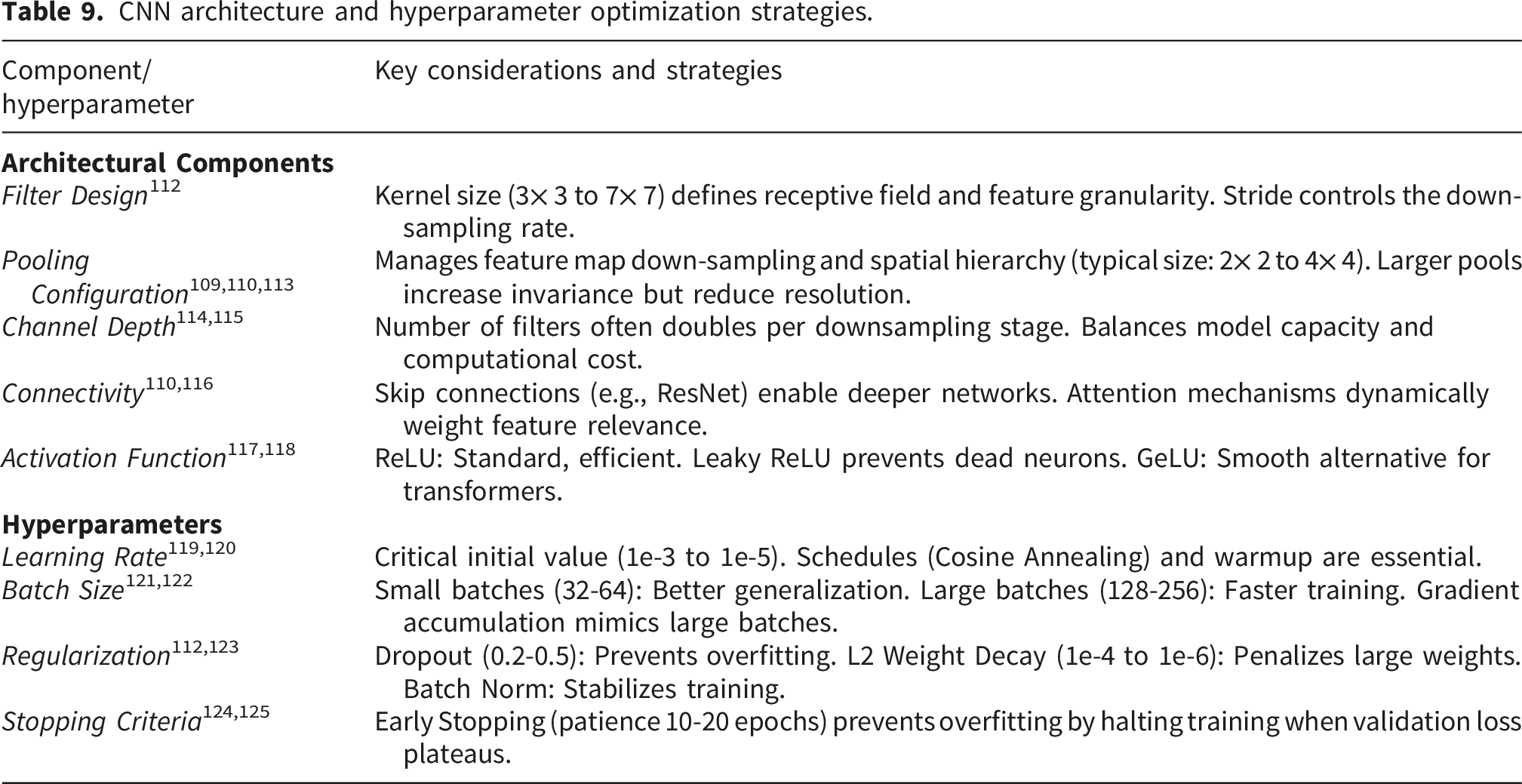
Among these factors, the convolutional filter settings determine the model’s complexity levels as well as the total number of feature learned. 114 The size and resolution of output feature maps depend on pooling layers that use stride and size parameters to compress data over space.111,117 Through the insertion of activation functions, models become nonlinear, which enhances their ability to detect subtle characteristics within the data.113,118 The colon cancer image classification requires distinct combinations of convolutional, pooling, activation, dropout, and fully-connected layers. 116
The efficiency of a CNN model depends on the correct activation selection 118 during both training and validation processes. An appropriate choice of activation function enables neural networks to execute continuous function approximation, so as to realize medical image processing with tumor classification. 126 During the learning process, the training and updating methods employed for the model determine its ability to achieve solution convergence and its algorithm for optimal performance.115,127 Lastly, the number of convolutional filters within architecture serves as a critical element feature extraction from input data. 128
In summary, architecture design of CNN models requires balancing complexity of task with available resources, as well as a mechanism to extract meaningful data patterns (features) from input histopathological images for classification tasks.
5.2. Hyperparameter finetuning
After the architecture design, a CNN model achieves its best results based on the quality and extent of the training data it receives.121,124 The CNN model requires diverse and representative training datasets which include different colon cancer types at multiple status. In this case, a proper finetuning strategy on the hyperparameters, which are listed in Table 9, is equally critical as architecture design in terms of performance improvement.
To be specific, a minimum number of epochs leads to the model underfitting, but an excessive number of epochs increases the risk of overfitting. 125 Batch size is the number of samples combined for processing in each training iteration. Larger batch sizes applied during model training accelerates the learning process but also consume memory resources increasingly. The approach leads to higher memory needs and potentially weakens gradient precision. 121 Furthermore, dropout rate (i.e., percentage of inhibitory nodes) selected for random removal from the network for overfitting reduction purposes. 123 The training process with this technique helps the model learn stronger features that show improved generalization potential for new and unknown data points in medical image processing tasks with high data variability. 112
Models uses dropout method to attain superior test-retest results than models without dropout regardless of Monte Carlo testing. 129 Accurate disease detection and prediction becomes essential during medical image processing tasks. A model learning rate determines the speed of weight updates during training. The stability of a model stands in opposition to training speed of convergence while applying a high learning rate. Lower learning rate values create both slower convergence and worse model results.119,120 The process of tuning CNN model hyperparameter remains equally important to CNN architecture development when developing efficient CNN models. These methods, like grid search, random search, and even Bayesian optimization, are often automated or done by hand to fine-tune the hyperparameters. 122
6. Recommendations to future research
This section provides a load of recommendations to future research (Figure 9). As indicated in the discussion, model architectures, data quality, and model optimization determine the performance of a CNN model. Further, the integration of a model regarding particular clinical setting also challenges onsite performance of a model. Lastly, as a supportive tool in diagnosis, the predictive result needs to be reinforced in the current diagnosis process by clinicians in terms of result visualization and interpretability improvement. Future research.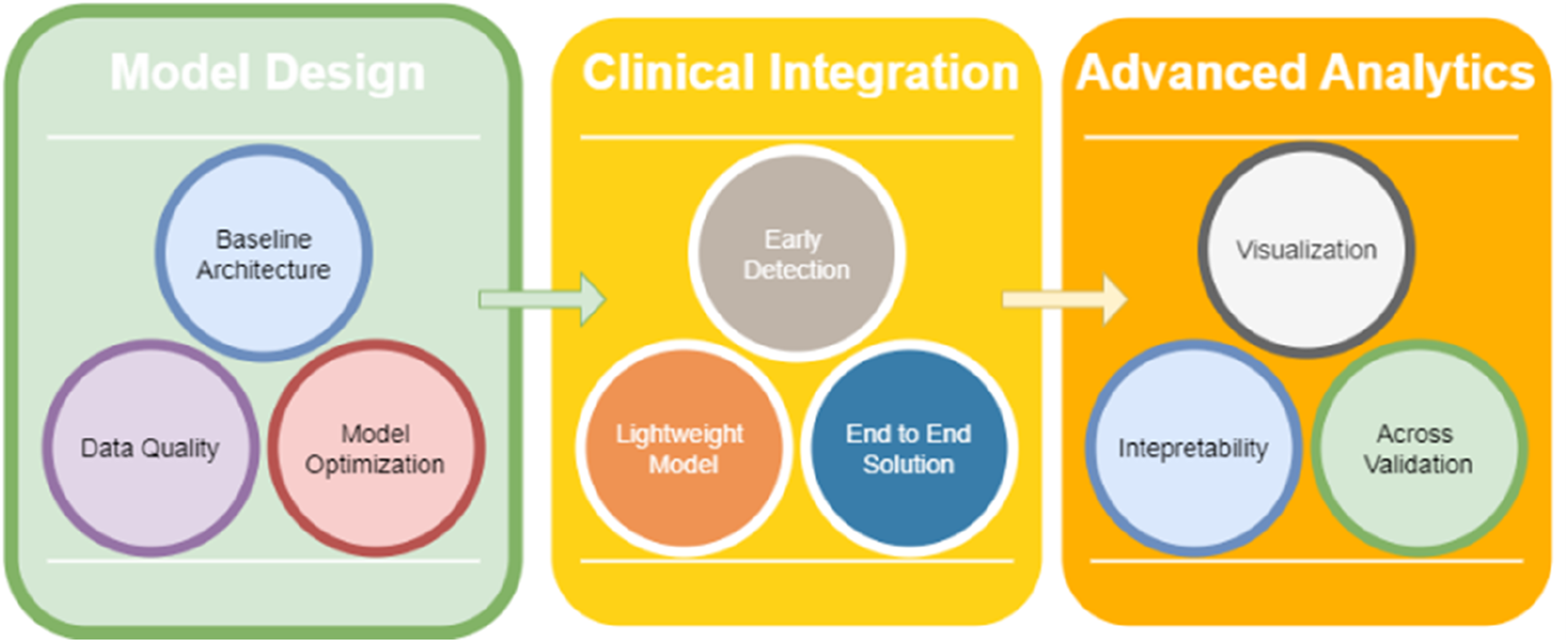
6.1. Quantum computing
In this review paper, the importance of model architecture design and hyperparameter finetuning were discused. From 2020, scholars130,131 have discussed the revolutionary emerging quantum computing in model development.
For imaging and image processing tasks, quantum-based innovation (e.g, QCNN) has been used for certain image processing tasks. In the case of QCNN, models are able to overcome the challenges from small-sized datasets. 132 Limited size and high variety in clinical sample influence the performance of model application. Quantum computing has shown its potential performance in corresponding medical imaging and image processing tasks by improving learning efficiency.
For the classification task, the potential improvement could occur from data pre-processing to the end of hyperparameter fine-tuning. Parameterized quantum circuits can represent certain complex decision boundaries more compactly than classical CNNs. Some studies131,133 suggest quantum models can be more resilient to certain types of noise or adversarial perturbations. In this case, quantum computing could help with major challenges faced by pathologist in terms of variability across scanners, staining protocols, and sites.
6.2. Advanced analytics
Recent studies134,135 identified the need for better interpretability in CNN models, an area of research that is likely to be fulfilled in future work. The inability to interpret the functioning of these models is a major problem for their therapeutic use. There is a need to develop CNN models along with interpretation methods that clinicians can understand so that they can better understand the model with prediction reasoning in a supportive decision-making process. Regarding result visualization, future efforts should focus on developing sophisticated visualization tools that can effectively display detection results through interactive heatmaps, region-specific confidence scores, and annotated overlays that highlight suspicious areas in real-time during colonoscopy and histopathological procedures.5,136
Cross-validation for CNNs is essential for several critical reasons. First, it ensures the robustness and generalizability of AI models across diverse patient populations and clinical settings. Through rigorous cross-validation across different medical centers, patient cohorts, and time periods, researchers can validate that their models maintain consistent performance beyond their initial training environment. A model with high overall accuracy might still have clinically unacceptable false-negative rates, which misclassify malignant cases as benign. Focusing solely on accuracy overlooks other clinically vital measures (sensitivity, specificity, precision, and the AUC). True reproducibility requires not only open data and code, but also comprehensive documentation of all preprocessing steps (e.g., CLAHE augmentation in Ref. 29, hyperparameter tuning processes (as detailed in Table 9 regarding learning rates, batch sizes, and regularization strategies), precise architecture definitions, and the clinical measures.
6.3. Lightweight clinical integrations
Colon cancer outcomes are highly dependent on the stage at which the disease is diagnosed. For the proper integration of CNN-based CDSS into clinical settings, linking them to existing healthcare systems is required for smart medication development. 136 Studies108,109 suggested that researchers should modify CNN variant model structures to improve early-stage detection performance. However, early-stage lesions are often small, subtle, and easily missed by both human observers and current automated systems. The identification of tiny and early-stage colon cancer lesions remains challenging for CNN models. Small lesions in low-resolution images can escape both human and CNN model detection because current models either overlook them or issue false positive identifications. Early detection aligns with the broader trend in medicine toward preventive care and minimally invasive intervention. By catching cancer earlier, clinicians can intervene sooner, often with less aggressive treatments, reducing patient morbidity and healthcare costs.
The lightweight CNN models delivered a 99.6% accuracy rate in diagnosing lung and colon cancer images while showing their capacity to process histopathological image. 102 Future work should focus on developing lightweight architectures that maintain high diagnostic performance while reducing computational demands, enabling real-time analysis and deployment in resource-limited settings. Lightweight CNN architectures such as Mobile-Net, Efficient-Net, and Shuffle-Net demonstrate powerful performances in identifying colon cancer. The models excel in performance efficiency and accuracy levels suitable for mobile utilization and real-time applications.
Future end-to-end solutions should encompass the entire pipeline from image acquisition through automated analysis to result visualization and clinical decision support. 4 Research efforts should focus on creating unified systems that automatically handle preprocessing steps, apply optimized CNN models for detection and classification, and present results in an interpretable format directly within existing hospital information systems. The end-to-end approach should emphasize real-time processing capabilities, robust error handling, and automatic quality control measures to ensure reliable performance in clinical settings.
7. Conclusion
Key findings of the paper contribute the following points. First, the paper survey statistically pointed to an increasing research interest in CNN applications to medical imaging and image processing and further in colon cancer classification from 2000 to early 2025 (Figure 1).
Using the PRISMA framework, 85 studies were included in the final review (Figure 2). Comparison revealed bi-and multi-classification benchmark studies among state-of-the-art CNN architectures (Table 8) with their best accuracy results. For bi-classification tasks: Res-Net (99.77%) in Ref. 24, Xception (99.95%) in Ref. 43, VGG-Net (99.85%) in Ref. 59, Dense-Net (99.60%) in Ref. 80, and Efficient-Net (99.97%) in Ref. 88 and 89. For the multi-classification task, Res-Net (99.67%), 29 Inception (92.74%), 49 VGG-Net (99.76%), 58 Dense-Net (99.96%), 73 and Efficient-Net (99.87%). 85
Furthermore, the potential challenges in current CNN development were summarized as aiming for a simple and efficient architecture and effective hyperparameter fine-tuning (Table 9). Lastly, the future research recommendations were proposed including quantum AI advancement, lightweight model design, and advanced analytics (Figure 9).
This review has several limitations. First, restricting the search to three databases may have excluded relevant studies. Second, due to the inconsistency of the secondary metrics adopted in benchmark studies over the past years, accuracy was the only widely used metric for comparison. However, focusing primarily on accuracy as the comparative metric overlooks other clinically important measures. The heterogeneous reporting of these metrics across the literature highlights the need for standardized evaluation protocols in future research. Third, the inclusion threshold of
Footnotes
Acknowledgement
This study is supported by TIRGS-ILG/1/2023/SCS/001 Taylor’s Internal Research Grant Scheme - Impact Lab Grant. Special thanks to Hebei Academy of Fine Arts for the collaborative support.
Ethical considerations
This study is a systematic review of previously published literature. Therefore, direct ethical approval from an institutional review board was not required. The review was conducted in accordance with established scholarly principles for systematic reviews.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Taylor’s Internal Research Grant Scheme - Impact Lab Grant (TIRGS-ILG/1/2023/SCS/001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The PROBAST protocol and result in PRISMA review can be accessed via: https://doi.org/10.7910/DVN/ZQYLAL (![]() )
)
Contributorship
Jie Li collected data and composed the manuscript. Weiwei Goh and Noor Zaman Jhanjhi validated PROBAST review result and proofread the manuscript. Ting Li coordinated the references.
Guarantor
Jie Li (
Weiwei Goh (
Noor Zaman Jhanjhi (
School of Computer Science, Taylor’s University.