
Abstract
Objective
Wearable health devices (WHDs) are increasingly important in supporting personal health goals, yet their effectiveness is mediated by the user experience. This study employs means-end chain (MEC) analysis to map the cognitive pathways through which users transition from perceiving device attributes to attaining core health values.
Methods
We applied a soft-laddering technique to interview 63 adult WHD users. The interview data were analyzed using content analysis to identify key attributes, consequences, and values. A summary implication matrix was constructed to illustrate the linkages between these factors, culminating in the generation of a hierarchical value map.
Results
Results indicate that concrete WHD attributes (e.g., wearability, health tracking, haptic reminders) facilitate positive user consequences, such as a sense of companionship, risk awareness, and self-regulation. These pathways lead to the attainment of high-level health values including mental wellness, safety, self-optimization, and lifestyle improvement. Conversely, we identified significant “broken ladders” in which persistent design flaws (e.g., inaccurate/inconsistent data, black-box algorithms, mistimed prompts, unrealistic goals), lead to negative consequences such as decision paralysis, distress, and motivation crowding. These barriers actively hinder value attainment in WHD usage.
Conclusions
This study provides a comprehensive framework of the WHD user journey, highlighting that user value is not derived solely from the technology but also from psychological and cognitive mediators. Findings suggest that developers must move beyond usability to prioritize data transparency and literacy education, while implementers should monitor for compulsive usage patterns to reduce psychological burdens and support long-term digital health engagement.
Keywords
Introduction
Wearable health devices (WHDs) are sensor-integrated technologies worn on the body that facilitate continuous tracking of physiological and behavioral data—such as heart rate, blood oxygen saturation, physical activity, and sleep—for health-related purposes.1,2 Beyond passive monitoring, these devices typically utilize mobile health (mHealth) applications that leverage persuasive design—including gamified goals, haptic reminders and social comparisons—to educate and nudge users toward better habits and better health.3,4
The commercial and social significance of this sector is undeniable; the global wearable market is projected to reach $114.36 billion by 2028. 5 This proliferation has catalyzed a shift toward proactive health management, empowering the public to engage with their personal health data, thereby enhancing health literacy and autonomy.6,7 Consequently, the integration of WHDs into public health programs has become increasingly common due to their relative affordability and scalability. 8
Despite their technical potential, the deployment of WHDs is currently hindered by a “utilitarian paradox.” Many WHD-based interventions report significant challenges, including low engagement levels, high attrition rates, and a failure to translate the technology affordances into sustained clinical or behavioral benefits.9,10 Emerging evidence suggests that the effectiveness of WHDs is not merely a function of technical affordances but is fundamentally mediated by the user experience. 8
The existing literature characterizes the WHD user experience as inherently complex and ambivalent. 11 Users often reported a spectrum of contrasting psychological states, ranging from reassurance to data-driven anxiety, and from perceived utility to skepticism.12–15 Although existing studies have identified various fragmented elements of this experience, they often lack a cohesive theoretical framework to explain how these divergent outcomes emerge from the same technological affordances. Specifically, the cognitive mechanisms that link low-level device attributes to high-level personal health values remain underexplored.
Our investigation fills in this gap by applying the Means-End Chain (MEC) theory. MEC posits that consumer perceptions are structured as a hierarchical cognitive linkage between perceived product attributes (the “means”), the consequences of use, and the ultimate personal values (the “ends”) that these consequences fulfill. 16 By adopting this framework, we shift the focus from descriptive user experience elements to the relational pathways that define the user journey.
Therefore, this study proposes the following three research questions.
This paper holds both theoretical and practical importance. Theoretically, this study contributes to digital health user experience research by applying MEC theory to wearable health devices, moving beyond superficial usability metrics to uncover the deep cognitive pathways that link device features to users’ core health values. On the practical front, the study provides a clear, actionable roadmap for developers and clinicians to design and deploy WHD-based digital health interventions that are not just technically robust but cognitively aligned with users’ core health values.
In the remainder of this paper, we first introduce the theoretical foundation of this study and then describe data collection and analytical procedures in the methodology section. The subsequent results section details and interprets the factors and linkages derived from the data, followed by a discussion of the whole structure of WHD user c experience ladders. We then critically examine the strengths and limitations of this study and outline promising avenues for future research. Finally, we present a concise conclusion that summarizes the study.
Theoretical foundation
The means-end chain (MEC) framework
The MEC theory, originally conceptualized by Gutman (1982), 16 provides a systematic methodology for modeling the cognitive structures that underpin user preferences and behaviors. The core tenet of MEC is that users do not perceive products as isolated entities; rather, they view them as a “means” to achieve desired “ends”. 17 This relationship is modeled as a hierarchical structure comprising three primary levels: attributes, consequences, and values.
Under the assumption that every interaction with a product yields specific outcomes, users learn to associate attributes of the product with subjective consequences, which in turn satisfy deeply held personal values. These cognitive linkages—often referred to as “ladders”—represent the internal logic through which a user justifies their engagement with a product.
18
To capture more nuanced layers of abstraction, as illustrated in Figure 1, Walker and Olson (1991)
19
expanded this framework into a six-level hierarchy.
In terms of attributes, these represent the fundamental characteristics of a product that are recognized and perceived by users. Concrete attributes refer to the physical, tangible characteristics of a product that can be objectively measured (e.g., screen size, battery life). Abstract attributes are defined as subjective characteristics of a product that normally reside in the minds of users (e.g., ease of use, perceived reliability). 20
In terms of consequences, they are the physiological or psychological effects arising directly from product use. The extended MEC framework distinguishes between functional consequences and psychological consequences. Functional consequences are the practical, immediate user outcomes resulting from product consumption (e.g., convenience, cost savings).21,22 Psychological consequences reflect internalized feelings, emotions, experiences or social perceptions that users connect to product attributes (e.g., a sense of accomplishment, ease of anxiety). 22
In terms of values, they refer to the ultimate “end states” or enduring beliefs that guide a user’s behavior. 16 Instrumental values refer to preferred modes of conduct (e.g., being disciplined), whereas terminal values represent final goals of existence (e.g., longevity). As one moves upward through the means-end hierarchy, the level of abstraction increases, and the focus moves from products to users. This progression allows researchers to move beyond what a technology is (technical specs) to uncover the fundamental psychological drivers that make it matter to the user.
MEC in the digital health context
The MEC framework has gained traction in digital health research due to its ability to map complex user-technology interactions. Recent applications include investigations into user experiences with location-based augmented reality games for physical and mental health, 23 older adults’ perceived values of using smart bracelets, 24 and female fitness app users’ motivations and perceptions. 25
Importantly, MEC offers a distinct advantage over traditional acceptance models (such as TAM or UTAUT), which often focus primarily on “ease of use” and “usefulness” as predictors of adoption. Although these models are effective for measuring intent, they often fail to capture the ambivalence inherent in complex real-world user practices, such as long-term health monitoring in this case. 21 Because MEC allows modeling both desirable and undesirable consequences, it is uniquely suited to investigate the “broken ladders,” in which technical attributes lead to negative psychological states such as decision paralysis or distress. This capacity for neutral, non-binary modeling makes MEC the ideal lens for exploring the multifaceted mechanisms that drive or disrupt value attainment in the wearable ecosystem.
Methods
Study design
Given the exploratory nature of this study, a qualitatively dominated approach was adopted. Data were collected using laddering interviews and were analyzed following the methodology proposed by Reynolds and Gutman. 26 The study design was approved by the Northeast Normal University Ethics Review Committee on March 18, 2023 (R-2023-03-001). This study is reported according to the COREQ (Consolidated Criteria for Reporting Qualitative Research) guidelines. 27
Participants and recruitment
This study targeted individuals with experience using WHDs. As acquiring qualitative data is constrained by time, place, and circumstance, sample relevance is considered more critical than sample statistical representation in qualitative-dominated research. 28 Accordingly, we employed purposive sampling, a form of nonprobability sampling in which sample selection is based on the researcher’s judgment of which elements best fit the study’s criteria. Considering that social media has a high penetration rate in China (80% by 2025, according to CNNIC) and that users of WHDs significantly overlap with social media users, 29 we implemented a low-cost recruitment campaign through leading Chinese social media platforms, including WeChat, QQ and Baidu Tieba, which ran from October 6, 2024 to February 11, 2025. The recruitment campaign advertised the researchers’ roles and the aims of the study. Interested individuals completed an online questionnaire, which collected information on whether they currently used a WHD, the last time they interacted with their device(s), and their age. Inclusion criteria required that participants be 18 years of age or older and have experience using at least one WHD. Exclusion criteria included: a washout period of more than three months for former users (to minimize recall bias) and inability to comprehend written or spoken Mandarin. A total of 71 respondents were initially recruited, of whom 63 were deemed eligible according to the inclusion and exclusion criteria.
Interviews were conducted and coded concurrently with the recruitment process, with the final sample size determined by the achievement of data saturation. By the time the interview reached the 51st respondent, no new themes had emerged. Following established practices in prior research,22,26 we conducted an additional 12 interviews (about one-fourth of the sample) to test for saturation. Data saturation was considered achieved in this study since no new themes emerged from these additional interviews, resulting in a final sample size of 63 participants.
Laddering interview
A laddering interview is an in-depth, one-on-one interviewing technique used to develop an understanding of how users translate the attributes of products into meaningful associations with respect to the self. 26 The laddering method supports two approaches: hard and soft laddering. Hard laddering requires interviewees to generate ladders one-by-one, whereas soft laddering follows their natural flow of speech and allows forks, loops and blind alleys. 17 As this study is exploratory, we employed soft laddering to elicit rich information from participants.
The outline of a semi-structured interview.

The interviews were conducted by CL (a research fellow specializing in Health Informatics), who has expertise in interviewing in general and the specific laddering approach. No prior relationship was established between the researcher and the participants before the commencement of the interviews, and participants were informed of the researcher’s role and purpose through the recruitment and consent process. The interviews took place on the campus of Northeast Normal University, China, from October 2024 to February 2025. Participants were provided with light refreshments during the interview, and no other compensation was offered. All interviews were conducted face-to-face, audio recorded, and transcribed verbatim. The transcripts were not returned to participants for review; however, the researcher checked them against the original recordings to ensure accuracy. Non-verbal cues and the researcher’s initial reflections were documented in field notes. On average, the interviews lasted 25 minutes, with 4 elicited attributes and 3 rungs on a ladder.
Data analysis
Samples of content coding.

*[R1] denotes the first interview respondent.
All procedures were conducted independently by CL and XC, and disagreements between them were reconciled through discussion together with LW. In brief, a total of 1056 codes emerged from open coding. Through consolidation, the total number of first-level codes was reduced to 668, represented by 42 distinct factors. These distinct factors were then categorized into 20 attributes, 18 consequences, and 4 values. The intercoder reliability was assessed by calculating Cohen’s Kappa, which is a coefficient that compares the observed agreement between two coders to the agreement expected by chance. A Cohen’s Kappa score above 0.60 is considered substantial agreement. For codes, factors, and categories, the Cohen’s Kappa scores were 0.73, 0.80, and 0.78, respectively, demonstrating substantial reliability.
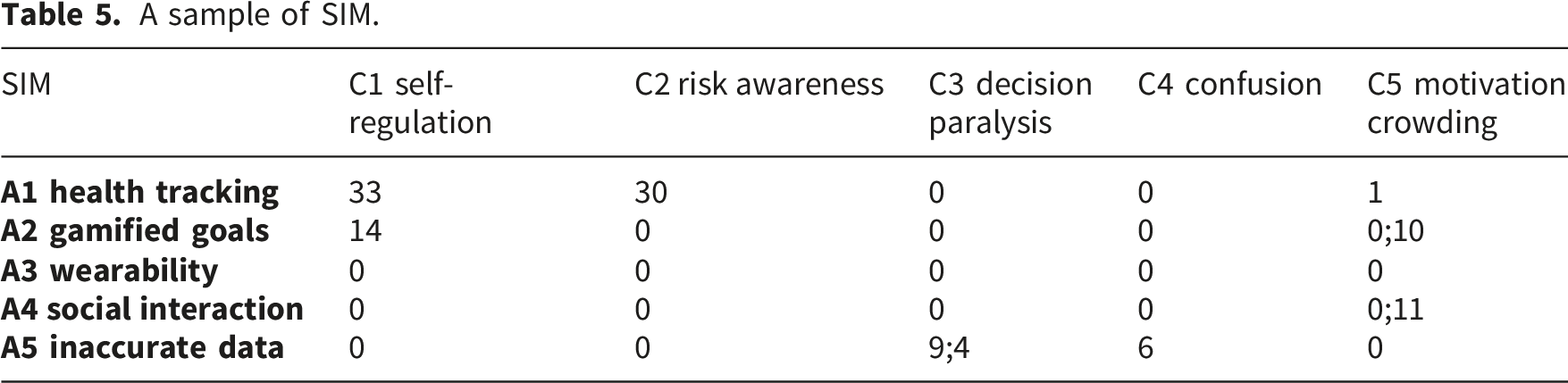
Construction of the Summary Implication matrix (SIM). The SIM summarizes the linkages between factors identified in the content analysis, effectively transforming qualitative data from the interviews into quantitative data. The linkages were identified from the coded responses to the laddering questions. Two types of linkages existed between factors: direct and indirect. A direct linkage exists when one factor is mentioned directly after another factor in the same ladder. An indirect linkage between two factors exists when they are mentioned in the same ladder, separated by one or more intermediary factors. For example, if a respondent mentioned that the goal setting and feedback features helped him/her schedule and control daily activities, thereby supporting an energetic lifestyle, then a hierarchical linkage is generated: from gamified goals to self-regulation, then to lifestyle improvement. Direct linkages existed between gamified goals and self-regulation and between self-regulation and lifestyle improvement, while indirect linkages existed between gamified goals and lifestyle improvement.
All linkages among factors were summarized in a matrix, with direct linkages appearing on the left of the semicolon and indirect linkages on the right. CL first coded linkages for each respondent and counted them into the SIM. Thereafter, XC performed a reexamination. Based on the SIM, we calculated the abstractness and centrality of each factor. Abstractness of an element is the ratio of in-degree (i.e., the column sum of the element in the SIM) divided by in-degree plus out-degree (i.e., the row sum of the element in the SIM). Factors with higher abstractness scores occupy higher layers in a means-end hierarchy, thus providing an objective method to validate the validity of categorization in content analysis. 31 Centrality of a factor is calculated by dividing total degree (i.e., in-degree plus out-degree) by the sum of all active cells in the SIM, which indicates the relative importance of each factor.
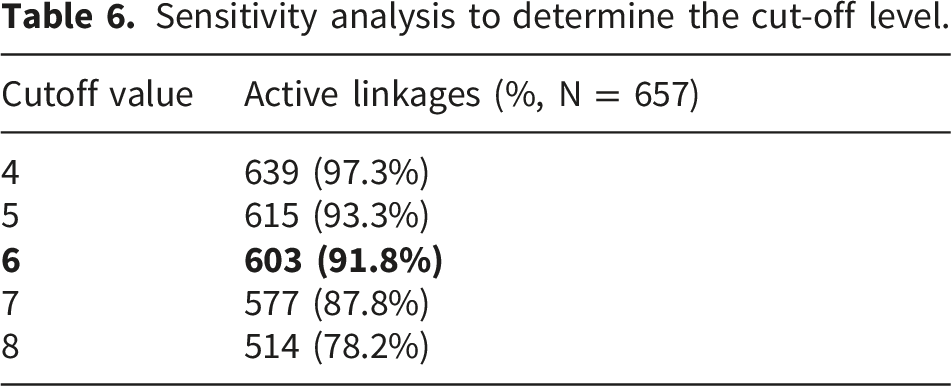
Generating the hierarchical value map (HVM). The HVM visually illustrates the relationships between factors and is built up by considering the linkages in the SIM. By inspecting the HVM, the dominant value attainment paths can be identified. 26 Usually, the HVM does not display all the factors and linkages in the SIM because a trade-off must be made between retaining sufficient information and creating a clear concise structure. This study follows a common practice proposed by Bagozzi and Dabholkar (1994) 32 to determine the cut-off value through sensitivity analysis. In this approach, only factors and links above the cut-off value are represented in the structure. The cut-off value is determined by comparing the proportion of selected linkages to the total number of linkages in the SIM. As a guideline, the HVM should cover more than two-thirds of all linkages in the SIM. 26
Results
Participant characteristics
Participant characteristics (N = 63).

Factors of WHD user experience
Factors of WHD user experience.
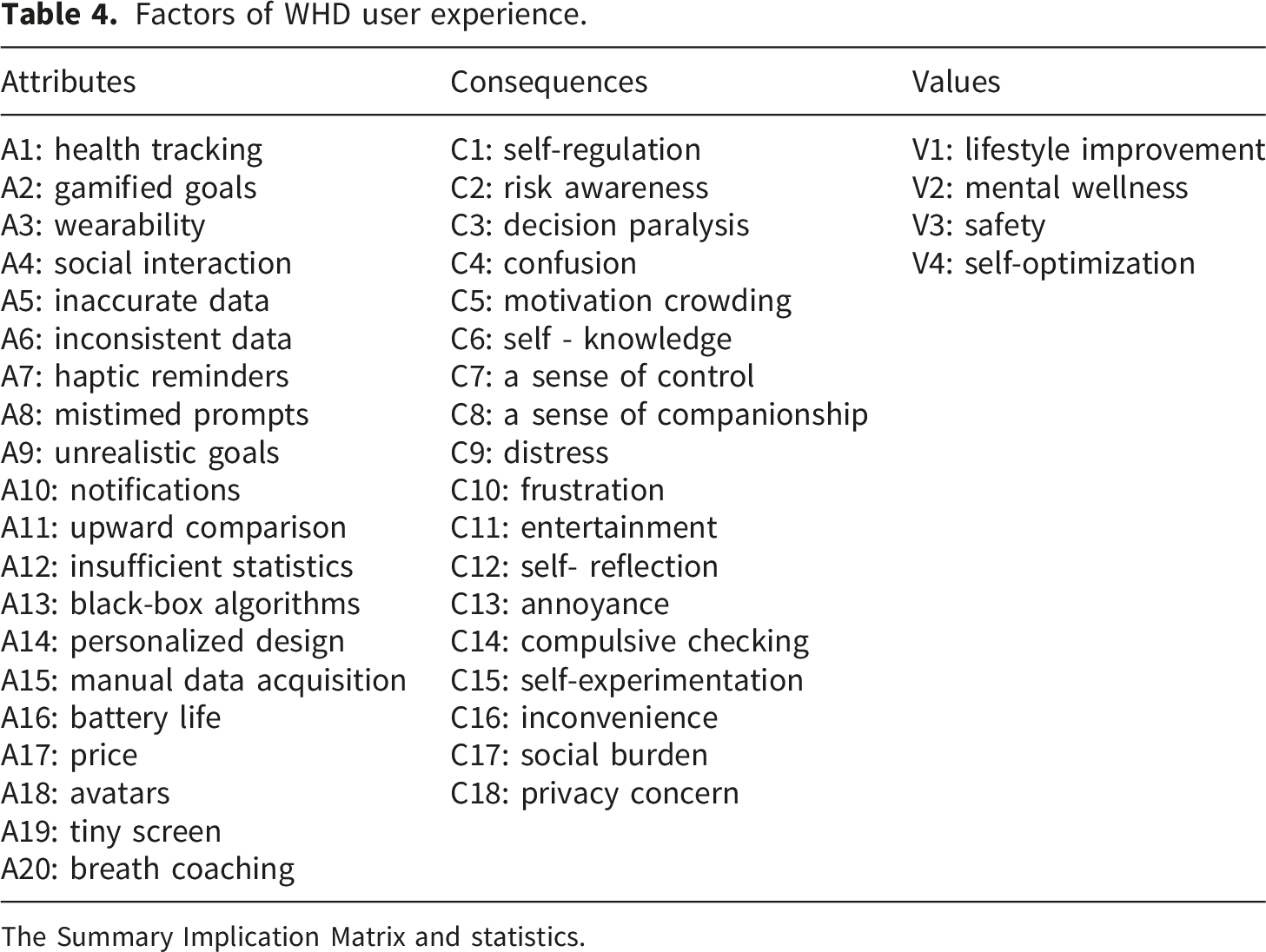
The Summary Implication Matrix and statistics.
In terms of consequences, users reported both positive effects and unintended negative effects. On one hand, WHDs fostered positive effects including enhanced self-regulation (n = 36), self-experimentation (n = 9), self-reflection (n = 12), improved risk awareness (n = 30), self-knowledge (n = 18), sense of control (n = 17), sense of companionship (n = 15), and increased entertainment (n = 12). On the other hand, users experienced side effects like confusion (n = 26), decision paralysis (n = 29), compulsive checking (n = 10), annoyance (n = 10), motivation crowding (n = 23), frustration (n = 13), and distress (n = 15).
There are mainly four main types of health-related values that users achieve through the appropriation of WHDs, including lifestyle improvement (n = 49), mental wellness (n = 40), safety (n = 29), and self-optimization (n = 23).
A sample of SIM.
Based on the SIM, we calculated the abstractness and centrality of each factor (see Appendix B). As shown in Figure 2, a scatter plot of factors’ abstractness scores by category, the abstractness level of factors tends to increase from attributes to consequences, then to values. Exceptions are A5, A8, A9, A12, A13 and A14, with abstractness scores of 0.5. These are discussed further with reference to relevant literature,25,33,34 and are retained in their original category considering their inherent meaning (Figure 3). Abstractness scores of factors. Centrality scores of factors.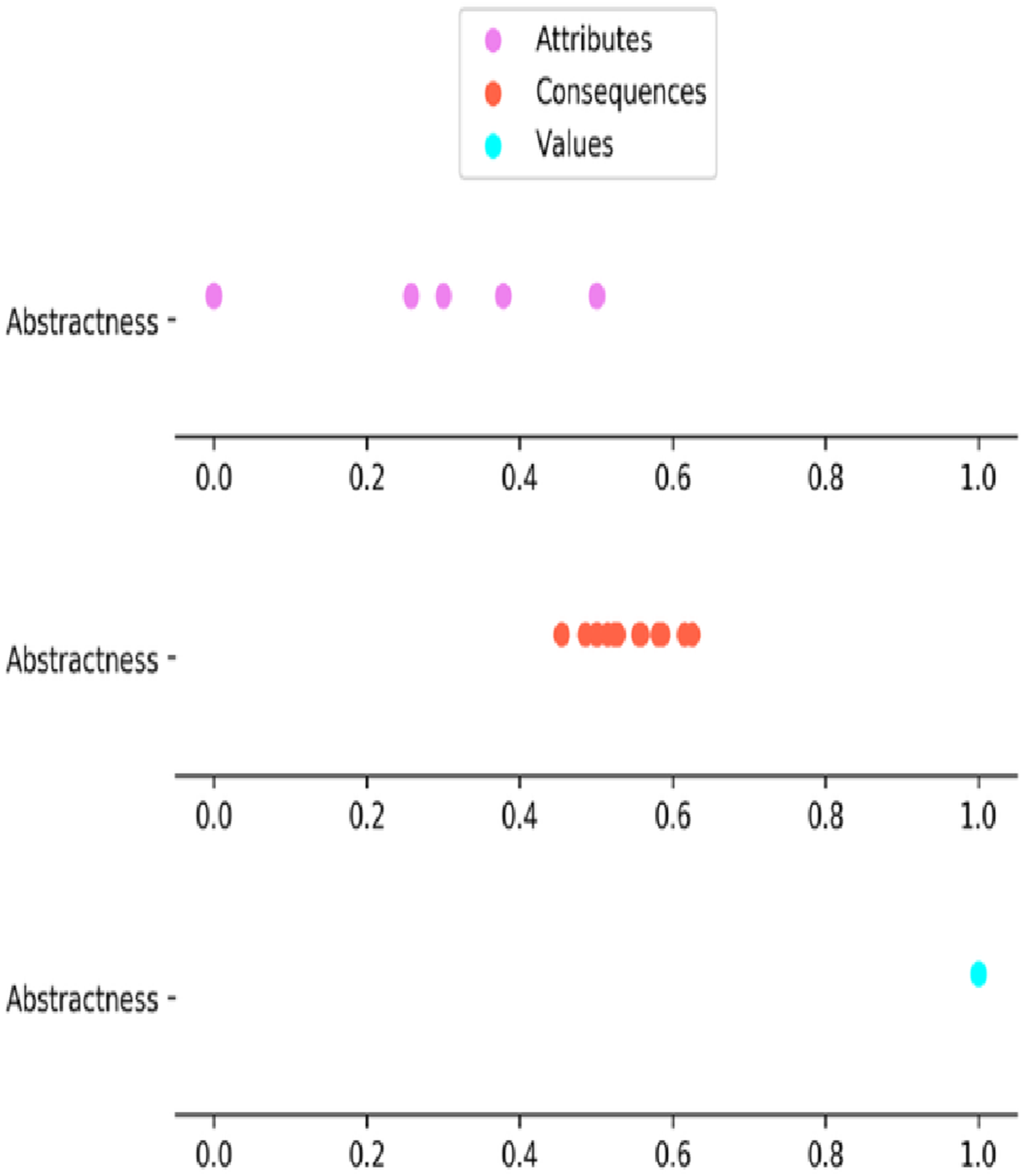
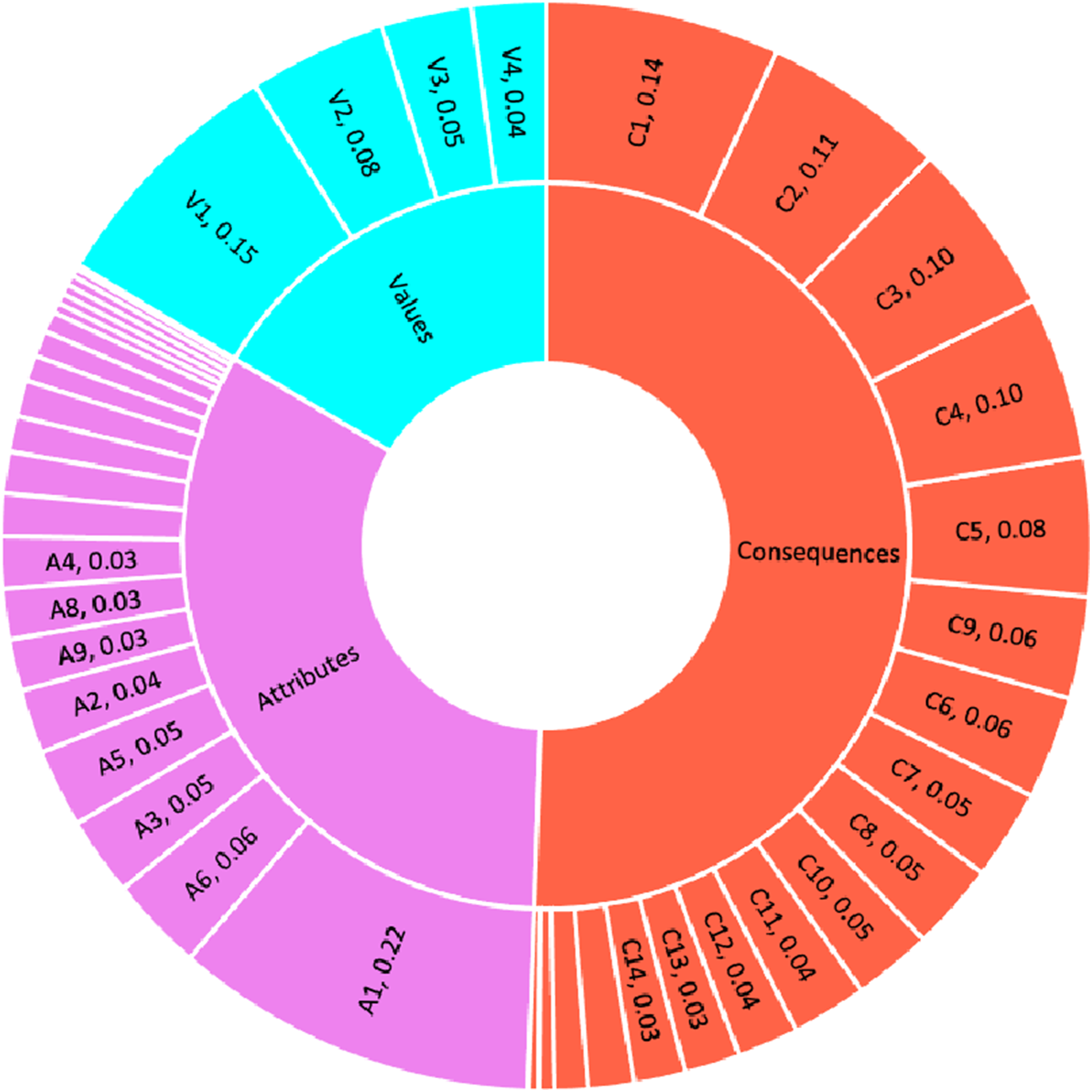
According to the centrality scores of the factors, A1 (health tracking), V1 (lifestyle improvement), C1 (self-regulation), C2 (risk awareness), C3 (decision paralysis), and C4 (confusion) play predominant roles in the structure, collectively accounting for 81% of all links in the implication matrix.
Mapping WHD users’ value attainment paths via HVM
Sensitivity analysis to determine the cut-off level.

The HVM of WHD user experience.
This study initially adopted a three-level HVM comprising attributes, consequences, and values. However, data analysis revealed significant hierarchical relationships within both attributes and consequences; therefore, the basic levels of attributes and consequences were further divided into two sublevels, drawing on concepts from previous studies. 19 As a result, the final model comprised five structural level, labeled as “Concrete attributes,” “Abstract attributes,” “Functional consequences,” “Psychosocial consequences,” and “Values.” In total, 33 elements with 48 distinct linkages provide a graphical summary of the hierarchical structure pertinent to WHD user experience (Figure 4).
Discussion
The HVM of WHD user experience
In the HVM of WHD user experience, four critical values exist at the top: lifestyle improvement, mental wellness, safety and self-optimization. First, lifestyle improvement emerged as the most significant value across the whole HVM, with the highest number of linkages. In the existing literature, WHDs are frequently employed in interventions targeting key lifestyle elements, such as regular exercise, good sleep hygiene, and a balanced diet, 35 although their effectiveness remains controversial. 36 This study finds that lifestyle improvement is directly facilitated by self-regulation, entertainment, and risk awareness, but hindered by motivation crowding and decision paralysis, as unintended consequences of WHD usage. The HVM further reveals that the positive consequences supporting the ultimate value of lifestyle improvement stem from concrete technological attributes, notably the core feature of health tracking and interaction features such as notifications, haptic reminders, gamified goals, and social interaction. For instance, one respondent described the benefits of using WHDs for lifestyle improvement, “One fun feature is the (virtual) medals awarded for celebrating exercise goals. They make exercise more entertaining, and earning each one keeps me motivated to stay active in daily life” [R2]. The HVM further reveals critical breakdowns in the pathway to lifestyle improvement, rooted in persistent data quality issues and interaction design flaws. Data quality issues, including inaccurate/inconsistent data, insufficient statistics, and black-box algorithms, collectively lead to decision paralysis in lifestyle adjustment. Interaction design flaws—such as mistimed prompts, unrealistic goals, and upward comparison—crowd out motivation for lifestyle improvement. The path-specific discussion of the ambivalent effect of WHD usage on lifestyle improvement is conducted in subsequent sections.
Second, safety emerged as a key value sought by WHD users. The HVM indicates that one prerequisite for safety is risk awareness, which is enhanced through the continuous monitoring of critical health metrics (i.e., health tracking), paired with real-time notifications of abnormal events. Safety and health risk assessment is an important area in which wearable technology contributes. Previous studies have proposed wearable technologies as solutions for detecting and alerting users to falls, 37 extreme glucose levels, 38 fatigue 39 and heart disease. 40 However, the reliability of wearables in supporting safety and health risk management is often compromised by data quality issues. Specifically, health data quality issues, including inaccurate/inconsistent data, insufficient statistics, and black-box algorithms, first confuse users, then lead to decision paralysis, and ultimately undermine the value of safety. One respondent recounted an experience in which WHDs failed to provide adequate safety protection: “I had a severe low blood sugar episode. The monitor displayed 4.7 mmol/L, but a fingerstick test showed a much lower reading of 2.4 mmol/L. I cannot understand why the numbers don’t match… this uncertainty increases the risk” [R31].
Users also seek to improve mental wellness with the help of WHDs. The mental effects of WHDs have become an increasing focus in digital health literature. 41 Some researchers have applied WHDs in the treatment of anxiety and depression, suggesting that WHDs can offer mental wellness-related values.42,43 However, other studies indicate that WHDs may also provoke adverse psychological reactions. 44 Drawing on the mechanisms revealed by the HVM, mental wellness as a terminal value is positively influenced by a sense of companionship and a sense of control, while being negatively affected by the unintended consequence of distress. Notably, the attribute of wearability, which fosters a sense of companionship can also intensify distress by encouraging compulsive checking.
Studies on the quantified-self movement have noted that people are increasingly participate in digital monitoring of their health and fitness for self-optimization. 45 In the HVM analysis, self-optimization emerges as a significant value for WHD users. As one respondent explained, “I value the recorded data on my running activity; it helps me gauge my progress in increasing my speed” [R36]. From the vantage point of the whole HVM, the value of self-optimization is positively influenced by self-knowledge derived from practices of self-experimentation and self-reflection based on health tracking, while it is negatively affected by decision paralysis caused by data quality issues.
By analyzing the significant factors, linkages, ladders and chains, we divided the overall HVM structure into three sub-structures to facilitate a more in-depth discussion. These sub-structures are presented separately in Figures 5–7 and are discussed in-detail to provide deeper understanding and insights. The sub-structure of psychological feelings in the HVM. The sub-structure of cognitive processing in the HVM. The sub-structure of motivational dynamics in the HVM.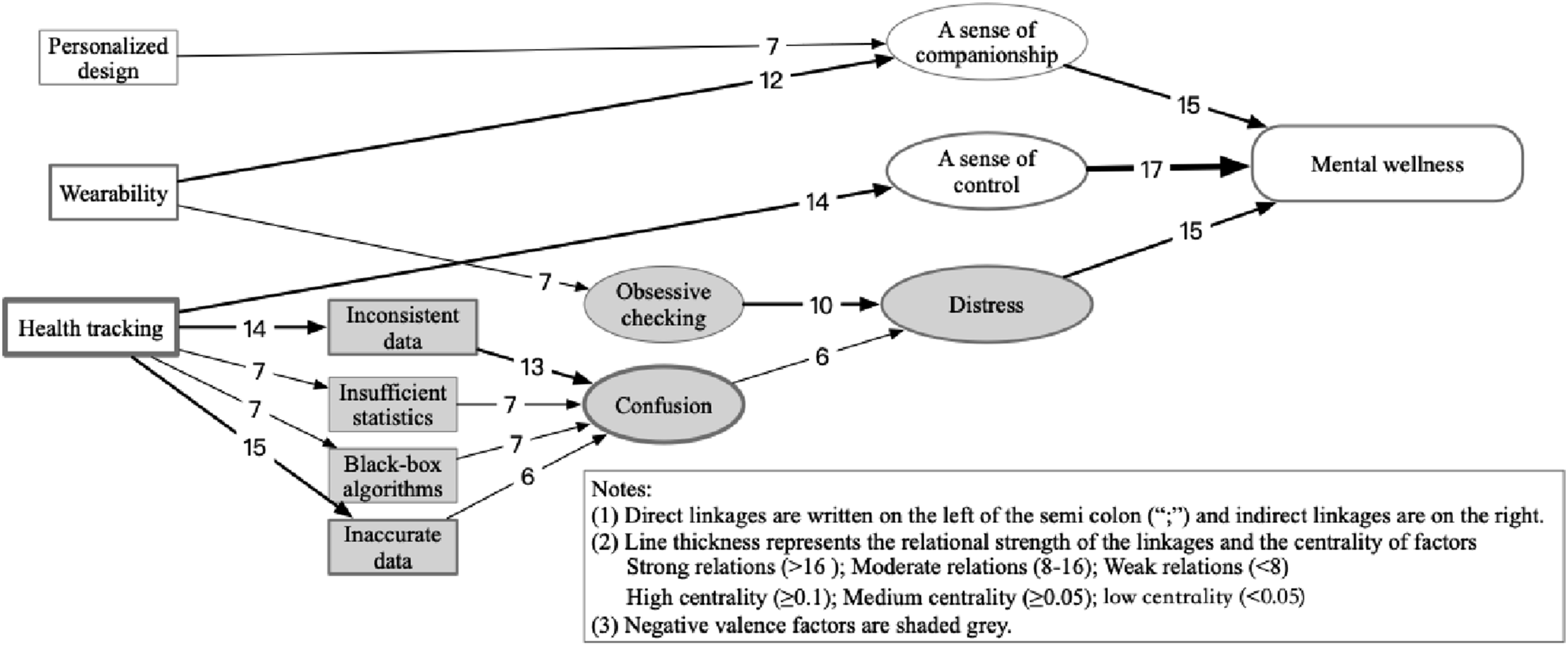

The sub-structure of psychological feelings in the HVM
In the sub-structure of psychological feelings of WHD user experience (Figure 5), two pairs of conflicting user experience paths emerge from the same attributes of WHDs: wearability and health tracking. We provide a detailed description and discussion of ambivalent user experiences regarding these two attributes, as follows.
The wearability feature of WHDs, characterized by their proximity to the body and a ubiquitous presence, 46 can influence mental wellness in both positive and negative ways, depending on users’ psychological patterns. On the positive side, wearability, along with personalized design, can foster a sustained sense of companionship, which, in turn, enhance mental wellness. Jang and Kim 46 scrutinized companion-like experiences with WHDs through the lenses of relational and extended-self. Consistent with the present study, their findings demonstrated the significant effect of personalized design on perceived companionship. Conversely, wearability can also have negative mental effects: it may encourage compulsive checking behaviors, leading to increased distress and ultimately undermining mental wellness. This pattern is often observed among anxious patients, for whom the ubiquitous presence of WHDs serves as a constant reminder of their condition. 47 To cope with the fear of disease progression, these users may resort to compulsive checking, which in turn reinforces a cycle of distress. For instance, one respondent who was recently diagnosed with diabetes stated, “I feel the sensor all the time. It is implanted in my body and invades my mind. I can’t help but constantly think about my disease. Checking my glucose level hundreds of times a day… It’s just so exhausting” [R38]. While researchers and practitioners have primarily focused on issues of discontinuance and low engagement with WHDs, this study suggests that overuse and excessive dependence may also arise under certain conditions.
In contrast to the vague and implicit perception of one’s own health status, the precise, objective health tracking data provide users with a positive sense of control, which can ultimately foster mental health. A sense of control refers to the belief that one’s life is controllable by his/her own actions rather than being a consequence of chance. 14 Numerous studies have demonstrated a strong relationship between perceived control and positive mental health outcomes. For example, Precht et al. 48 found that perceived control positively related to emotional well-being during the COVID-19 pandemic. In this study, a sense of control serves as an important psychological resource for individuals in coping with stressors arising from various health challenges. However, new stressors are introduced by health data quality issues (i.e., inconsistent/inaccurate data, insufficient statistics, and black-box algorithms), which first lead to confusion and then to distress, ultimately undermining mental wellness. One respondent who diagnosed with atrial fibrillation and experiencing anxiety described his interaction with health monitoring data as follows, “I need to reassure myself that my heart is doing okay. While the device is somewhat useful, it frequently detects AFib despite me feeling no discomfort. This confuses me and only makes me more anxious than before” [R43]. These findings indicate that although health tracking has significant potential to support mental wellness, their benefits are largely compromised by data quality issues. A detailed discussion of data quality issues is presented in the following section, which focuses on the cognitive processing structure of WHD user experiences.
The sub-structure of cognitive processing in the HVM
The sub-structure of cognitive processing in the HVM illustrates how WHD users’ information practices add value to health-related decision-making (Figure 6). First, by observing and assessing health tracking data, users can promptly identify potential health risks. In addition, advanced WHDs send notifications to report the automatically detected abnormalities. The resulting increase in risk awareness often encourages users to participate further in formal medical tests and interventions, thereby supporting health and safety. For example, one respondent stated: “The ECG provided by the Apple Watch showed that I had sinus rhythm and ventricular premature beats ... so I went to the hospital for further examination and was diagnosed with myocardial ischemia” [R30]. This process following paths summarize this process: from notifications/health tracking to risk awareness, and then to safety. In traditional contexts, health risks or subhealth conditions are often neglected by individual before obvious symptoms appear. 49 Consistent with Baumann and Weinberger, 50 and Charlton and Kyriaco, 51 who argue that WHDs can foster preventive healthcare, this study’s findings suggest that WHDs can enhance risk awareness and support health and safety. Kirubakaran 52 advocates a more direct approach: sharing health tracking data with healthcare providers for safety purposes. This approach is especially valuable for at-risk populations but less feasible for the general population due to the limited computing resources in healthcare systems.
Second, through self-experimentation and self-reflection, health tracking data are transformed into self-knowledge, ultimately contributing to self-optimization. This pathway illustrates how WHD users integrate information practices with concrete health practices. In self-experimentation, users aim to identify relationships between behavior and physiological responses. 53 For instance, one respondent noted, “I figured out how sensitive my body is to energy drinks through simple experiments. After drinking coffee, my resting heart rate went up from around 65 to 75. But with tea and Red Bull, the effect wasn’t as noticeable”[R5]. Through self-reflection, users review historical health records and develop rational explanations for data fluctuations. As one respondent explained, “After riding the spinning bike for an hour, I checked the exercise record and found that most of the effort went into endurance training. To improve calory-burning efficiency, I increased the resistance to the highest level I could sustain” [R52]. Self-experimentation and self-reflection represent two distinct modes of knowledge discovery—deduction and inference—both of which require a relatively high level of data literacy and scientific literacy. 54
Users often experience confusion when processing health data from WHDs, leading to decision paralysis across contexts. These negative consequences are linked to health data quality issues including inconsistent/inaccurate data, insufficient statistics and black-box algorithms. First, users compare different brands of WHDs when measuring the same health metric and often notice significant inconsistencies. As one respondent noted, “I use a Huawei and a Xiaomi band to track my sleep, and there is about an hour’s difference between the two … I’m not sure which to trust” [R62]. Such discrepancy stems in part from the lack of standardized data processing across the wearable industry. 55 Second, users frequently compare WHD outputs with “gold standards”, such as direct observations or formal medical tests, and identify clear measurement errors. Prior validation studies suggest that commercially available WHDs sacrifice accuracy in favor of convenience and low cost, and their estimation of sleep, heart rate and physical activity are susceptible to environment noise. 56 Third, some users expressed disappointment with the lack of potentially valuable statistical analysis, such as time-series or correlation analysis. For example, a respondent stated, “The sleep data hasn’t really helped with my insomnia, mainly because the wearables don’t connect it with my daily activities, which seems like a key factor” [R1]. Fourth, some users complain that sleep scores and physical activity index are difficult to interpret due to black-box algorithms. The complex synthetic process underlying these measures raise doubts about their meaning and reliability. 2 In summary, these negative experiences in the cognitive processing highlight the unmet information needs of WHD users in managing their personal health. As wearable technologies continue to evolve, emerging solutions in academia hold promise for addressing data quality issues raised by users. For instance, Weed et al. 57 and Kim et al. 58 have proposed different approaches for wearable-based circadian phase estimation using light exposure, activity, and body temperature data. These approaches not only have the potential to provide a new type of health indicator to general users, but also to enhance the accuracy and interpretability of downstream health metrics, such as sleep scores.
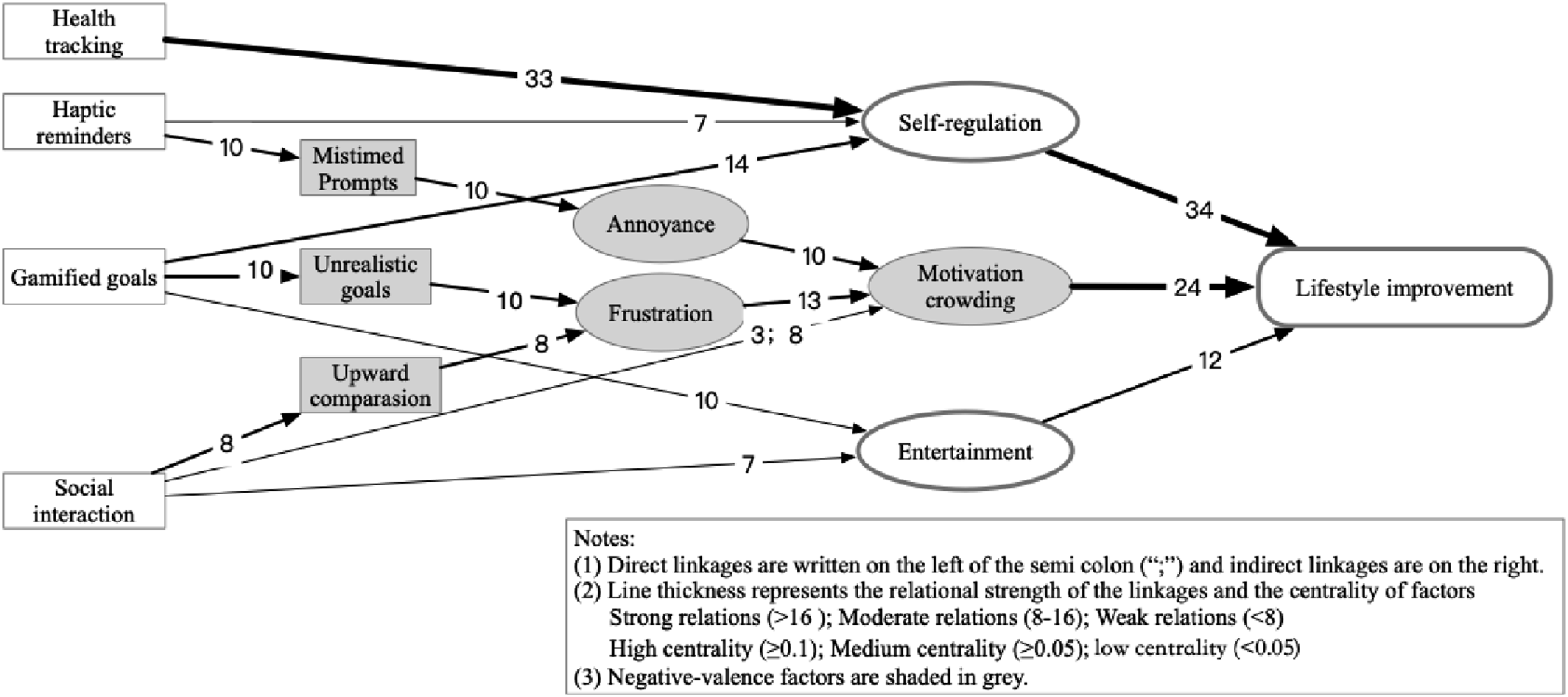
The sub-structure of motivational dynamics in the HVM
Within the HVM, the motivational substructure includes two positive pathways that encourage WHD users to engage in lifestyle improvement, while two negative pathways hinder their participation. First, WHDs empower users to self-regulate key elements of their lifestyle, summarized as the chains: from health tracking/gamified goals/haptic reminders to self-regulation, and then to lifestyle improvement. For instance, a respondent said, “The calorie consumption data from my tracker is really helpful …I use it to manage my diet and avoid overeating” [R10]. Second, the interaction features of WHDs contribute to a more entertaining environment, which encourages sustained commitment to lifestyle improvement, captured by the chains: from gamified goals/social interaction to entertainment, and then to lifestyle improvement. As one respondent noted, “Apple Watch provides (virtual) medals for celebrating daily exercise goal attainment. It is fun. Getting medals is both the motivation and encouragement for exercise” [R11]. Similarly, existing studies show that WHD use is positively associated with enjoyment. 59 Lifestyle improvement requires long-term commitment to deliver health benefits, and the lack of immediate incentives makes it difficult for individuals to sustain motivation. 60 This study suggests that WHDs supplement this process by enabling timely self-regulation and offering immediate, entertainment-based incentives that support sustained lifestyle improve.
However, when external incentives from WHDs are not successfully internalized by users, they may lead to unintended negative consequences and ultimately undermine users’ self-determined motivation for lifestyle improvement. Specifically, two negative chains exist in the sub-structure of motivational dynamics. First, reminders are frequently perceived by users as mistimed prompts, triggering annoyance, and consequently producing a motivation crowding-out effect on lifestyle improvement. For instance, one respondent said, “It is really annoying getting the vibration from my wristband reminding me to stand up when I’m in an important meeting. I actually think it is intrusive and makes me feel like I’m losing autonomy over my own schedule” [R4]. Addressing this concern requires context-aware prompt timing. One promising avenue is to integrate circadian phase estimation into prompt-timing algorithms—an approach supported by Kim et al., 58 who emphasize that accurate circadian phase estimation is a prerequisite for delivering timely interventions.
Second, some users experienced frustration arising from unrealistic goals and upward comparison in social interaction, which, in turn, threatened their self-determined motivations for lifestyle improvement. For example, one respondent lamented, “The 10,000-step goal feels unrealistic for me; it leaves me feeling frustrated and discouraged about trying to live an active life” [R11]. While WHDs provide users with other-determined motivation for lifestyle improvement, 15 they may crowd out more self-determined forms of motivation, which are associated with better adherence to health behaviors. 61 To mitigate those potential negative effects, we propose that WHDs should be further developed in three key areas: context-sensitive reminders that respond to users’ dynamic schedules, personalized goal setting, and a supportive, encouraging social interaction environment.
Strengths, limitations and future research
The main strength of the current study lies in the construction of a means-end chain structure of WHD user experience factors, which adequately captures the entire pathway from WHD attributes to the intermediate user consequences and ultimately to personal health values. By modeling both positively and negatively valence factors within the MEC framework, this study addresses the inherent complexity and ambivalence of WHD user experience. Moreover, while WHD user experience has been explored qualitatively in previous studies, the combined qualitative, quantitative and visual data analysis approach used in this study represents an additional strength.
There are however several limitations to the current study that could pave the way for future research. First, this study may be subject to sample bias given that the sample consisted solely of Chinese participants. The use of WHDs is profoundly shaped by contextual factors such as health beliefs, digital literacy, social norms, and trust in technology, 62 which can differ significantly across cultures. Therefore, it is important to note that this study was conducted within the Chinese cultural context—a highly digitized society with a population of moderate health literacy levels. Future research that adopting a cross-cultural lens would be a valuable extension of this work. Second, the present study applied a qualitatively dominated approach, which does not allow for strict statistical generalization of the findings. While the sample size adhered to Reynolds and Gutman’s 26 guidelines for generating valuable insights into WHD user experiences, it does not permit a robust quantitative analysis. Future research can adopt a quantitative approach with a larger sample to validate the hierarchical structure of WHD user experience identified in this study and offer more generalizable implications regarding wearable technology development and application. Third, while our sample includes users with varying levels of experience, the group sizes limit our ability to conduct robust comparative analyses. To adequately capture how users’ perceptions of WHDs change over time, a longitudinal design should be considered in future research.
Conclusions
This study is among the first to investigate WHD user experience from a means-end chain perspective. Through systematic analysis, this study identifies not only positive user outcomes but also critical breakdowns in the technology-health chain. Specifically, our findings indicate that users generally undergo a complex multistage process to achieve personal health values, including lifestyle improvement, safety, mental wellness, and self-optimization, through their interactions with WHDs. This study reveals that the attributes and functions of WHDs contribute to health values by providing various intermediate benefits, such as fostering a sense of companionship and control, enhancing risk awareness, improving self-knowledge and self-regulation, and increasing entertainment. It also highlights the technological and user barriers that hinder the attainment of value. To cope with the negative user experiences, WHDs need to be further developed to address data quality issues, including inaccurate/inconsistent data, insufficient statistics, and black-box algorithms, as well as interaction design problems including mistimed prompts, unrealistic goals, and stressful upward social comparison. In addition, special attention should be given to compulsive use behaviors, which are likely to occur in vulnerable populations.
Supplemental material
Supplemental material - Ladders to better health? Identifying the cognitive pathways and barriers to value attainment in wearable health device usage
Supplemental material for Ladders to better health? Identifying the cognitive pathways and barriers to value attainment in wearable health device usage by Caining Li, Xiaoyu Chen and Lai Wei in Digital Health.
Supplemental material
Supplemental material - Ladders to better health? Identifying the cognitive pathways and barriers to value attainment in wearable health device usage
Supplemental material for Ladders to better health? Identifying the cognitive pathways and barriers to value attainment in wearable health device usage by Caining Li, Xiaoyu Chen and Lai Wei in Digital Health.
Footnotes
Ethical considerations
The study received ethical approval from the Northeast Normal University Ethics Review Committee on March 18, 2023 (R-2023-03-001). Written informed consent was obtained from all participants prior to study initiation.
Author contributions
CL and LW designed the study framework. CL and XC conducted the interviews, the data analysis and interpretation. CL drafted the manuscript. All authors provided input into manuscript preparation and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Natural Science Foundation of China (No. 72404053). CL is supported by the Social Science Research Project of Jilin Provincial Department of Education (No. JJKH20241438SK), the Fundamental Research Funds for the Central Universities (No. 2412024QD030), the Postdoctoral Fellowship Program of CPSF (No. GZC20230415).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized dataset supporting the conclusion of this article is available upon reasonable request for bona fide researchers with an established scientific record and bona fide organizations.
Guarantor
CL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.