
Abstract
Objective
Surgery and postoperative complications disrupt circadian rhythms. While clinicians recognize the implicit value of circadian rhythms to evaluate postoperative recovery, the absence of a practical means to measure them has limited their exploration and integration into clinical practice in children.
Methods
Consumer wearable device (Fitbit) was given to children 3-18 years old who underwent laparoscopic appendectomy for complicated appendicitis and data were collected during postoperative days (POD) 1 to 21. Three novel rest-activity rhythmicity (RAR) metrics were computed from minute-by-minute continuous Fitbit data: (1) Periodicity and (2) Amplitude of the 24-hour Activity Rhythm; and (3) Circadian quotient of the 24-hour heart rate (HR) Rhythm. RAR trajectories were aggregated for patients without postoperative complications and compared against trajectories for patients with complications.
Results
Ninety-four patients were included in the analysis (n=13 [14%] with complications). For patients without complications, three RAR metrics gradually increased in intensity until reaching plateaus between POD 11-20 (Periodicity of the 24-hour Activity Rhythm, 95% confidence interval [CI]: POD 9-14; Amplitude of the 24-hour Activity Rhythm, 95% CI: POD 16-24; Circadian quotient of the 24-hour HR Rhythm, 95% CI: POD 9-15). Although the RAR metrics for children with complications increased in intensity, none plateaued during the 21-day study period.
Conclusion
Wearable-derived circadian rhythms demonstrated distinct patterns in RAR metrics for children with and without complications during the 21-day study period following appendectomy. This suggests that the RAR may be relevant digital biomarkers to track postoperative recovery and identify complications in pediatric populations.
Keywords
Article summary
Rest-activity rhythms in wearable-derived physical activity and heart rate may be utilized as biomarkers of normative postoperative recovery and distinguish complications among children following appendectomy.
What’s known on this subject
Clinicians recognize surgery and postoperative complications disrupt circadian rhythms. However, there is currently no practical means to monitor postoperative physiological or behavioral changes at a high resolution, limiting the ability to explore and integrate circadian rhythms to evaluate postoperative recovery in children.
What this study adds
This study utilized physical activity and heart rate data from wearable Fitbits to characterize children’s postoperative recovery using three novel wearable-derived rest-activity rhythmicity (RAR) metrics, as indirect proxies for circadian rhythms. Our findings indicate RAR may be biomarkers for postoperative recovery and complications.
Introduction
The human circadian network, which regulates biological rhythms in the brain and body, is a prime example of a homeostatic system. A central circadian clock within the suprachiasmatic nucleus of the brain aligns external and internal time and ensures multi-organ system coordination with light and darkness.1–11 As a result, countless physiologic processes demonstrate a 24-hour periodicity, or circadian rhythm, such as cycles of sleep/rest at night and wake/activity during the day. The periodicity of an individual’s circadian rhythms reflects their underlying physiologic condition; in cases of pathology, these normal 24-hour rhythms may become misaligned—i.e., occurring on a shorter or longer timescale.12,13 Disrupted circadian rhythms have been associated with diverse conditions,12–20 general anesthetic administration, surgical interventions, and associated complications.21–29
Surgery and postoperative complications induce an acute inflammatory state 30 that temporarily disrupts many natural circadian rhythms, including vital signs such as heart rate (HR),31,32 core body temperature 33 and blood pressure, 34 as well as daily activities. Clinicians have long recognized the value of circadian rhythms as an indicator of health since they play an important role in regulating immune responses, hormonal balance, metabolism, and tissue repair 35 from a molecular standpoint. Disrupted periodicity in vital signs and rest-activity cycles can indicate an underlying pathology, such as prolonged inflammation, pain and impaired healing. Yet, the absence of a practical means to measure circadian rhythms has limited their investigation and clinical utility. 36
Advances in consumer wearable devices have made it possible to reliably collect daily patterns in vital signs, activity, and other biometric data, making it possible to calculate circadian rhythms. 37 For example, rest-activity rhythmicity (RAR) derived from 24-hour patterns of rest and activity from continuous HR and activity data can provide an indirect proxy of circadian organization in real-world settings. 38 Circadian rhythms have been previously investigated in adults, such as patients with Alzheimer’s disease, 39 diabetes, 40 and depression 41 ; however, they have not yet been explored in surgical pediatric populations and may offer a practical means to evaluate children’s circadian disruption caused by surgery and complications.
In a previous study, 42 we investigated the predictive value of 31 RAR metrics (eTable1) derived from a consumer wearable (Fitbit) to differentiate postoperative recovery outcomes (normative vs. complications) in children who underwent laparoscopic appendectomy for complicated appendicitis. Appendectomy is the most common cause of emergency abdominal surgery in children in the United States. 43 Approximately 14% of children experience postoperative complications after appendectomy, 44 which are often difficult to detect early due to reliance on subjective reporting by caregivers. Complications can delay overall recovery,45,46 and may lead to serious health issues, medical expenses, and burden to patients and their families. 47 We found that RAR metrics were promising for early detection in a pediatric cohort, retrospectively predicting complications up to three days before diagnosis with 91% sensitivity. 42
To build on this work and continue addressing current gaps in our ability to monitor postoperative recovery and detect complications using wearables, especially after discharge, we examined the time-course of the three most predictive RAR metrics with clinical interpretation during the first 21 days after pediatric appendectomy. Our objectives were to (1) characterize normative RAR trajectories related to activity and HR, and (2) compare these trajectories for patients who experienced complications against normative recovery.
Methods
Patient selection and recruitment
This study was approved by the Institutional Review Board at the Ann and Robert H. Lurie Children’s Hospital of Chicago (IRB: #2018-1836). Children 3-18 years old who underwent laparoscopic appendectomy for complicated appendicitis from 2019 to 2022 were approached for inclusion. Patients were excluded if any pre-existing mobility limitations, comorbidities, or doctor-ordered physical activity limits of more than 48 hours post-surgery would impact their postoperative recovery. Patients and/or their caregivers who do not speak English or Spanish were also excluded due to the cost and time associated with translation services.
A research coordinator identified eligible hospitalized patients through the Electric Health Record (EHR) and then approached and recruited pediatric patients and their caregivers after appendectomy. Written consent was obtained from the caregiver for all children under 18 years old. In addition, verbal assents were obtained from children under 12 years old, and written assents from children 12-17. After the consent/assent process, patients were given a wearable fitness tracker (Fitbit: Inspire HR or Inspire 2). The Fitbit application was installed on the caregiver’s smartphone, and a deidentified Fitbit account was set up, ready for wearable data collection via a cloud platform (Fitabase) to occur through postoperative days (POD) 21. Data were collected from POD 1-21, where POD 1 is defined as the first calendar day after surgery, and each day runs from 00:00 to 23:59. The Fitbit was given to the participant as compensation at the end of this period, marking study completion.
Collection of clinical information
The following clinical information was extracted from the patient’s EHR: age, sex, race/ethnicity, postoperative length of stay, and the type and date of any postoperative complications during the recovery period. Phone surveys were conducted on POD 3, 7, 10, 14, and 21 to collect information regarding any new symptoms and healthcare utilization during this period. A panel of five clinicians confirmed the diagnosis of postoperative complications and their corresponding subtypes through EHR and survey results review.
Collection of wearable data
The Fitbit and app automatically synchronized wearable data to the Fitabase cloud platform, including per-minute HR and per-minute step count, as well as daily summaries of resting HR, activity (e.g., total step counts), and sleep (e.g., total sleep minutes asleep). After the study period, per-minute HR, per-minute step count, and daily sleep metrics were downloaded from the cloud platform (Fitabase) and stored on the secure hospital server. Existing studies have validated these Fitbit data with acceptable accuracies for children (3-18 years old) for health monitoring applications.48–54 Fitbit data were collected over a 21-day study period, from POD 1 to POD 21. For all participants, this period included a brief hospital stay following surgery and subsequent discharge to the community. The day of having surgery is defined as POD 0, which is excluded from the study period. The study period starts the first day after surgery day (POD1), which is defined as postoperative day 1, at 0:00 (midnight, or 12:00AM).
Patient groups
After the study period, patients were retrospectively assigned to one of two groups: those who were diagnosed with one or more postoperative complications (e.g., intra-abdominal abscess, surgical site infection, etc.), 44 and those who were not diagnosed with any complication (normative recovery).
Outcome measures of 24-hour activity rhythms
Based on top-ranking Fitbit features in our previous study, 42 we selected Periodicity and Amplitude as the primary RAR measures of interest for the 24-hour Activity Rhythm to maximize clinical interpretability and specifically capture behavioral movement contrast (detailed selection rationale is provided in eMethods 1). Low periodicity and reduced amplitude of 24-hour activity rhythm are significantly linked to disease and disease-related deaths. 55 These two methods and the metrics of activity rhythms were chosen since there is previous evidence to support their use as digital biomarkers for remote patient monitoring, such as for Alzheimer’s disease, 56 cancer, 57 and depression. 58 A moving average was applied to the per-minute step count data using a window size of 15 minutes, as is commonly used by circadian studies.59,60 The moving average starts at time zero for the day (00:00) and stops at the end of the day (23:59). This resulted in up to 96 data points per 24-hour period from which the outcome measures were computed. The Periodicity of the 24-hour Activity Rhythm was extracted from the Periodogram of these data, a non-parametric method for estimating the power spectral density of a time series.61,62 A value above 1.0 indicates the presence of a 24-hour rhythm, whereas a value below 1.0 implies a weaker or less-defined 24-hour rhythm. The greater the value, the stronger the 24-hour rhythm appears to be. Amplitude of the 24-hour Activity Rhythm was derived using Cosinor Regression, a parametric method that estimates the maximum difference in the day from mean activities over the 24-hour period.62,63 A reduction in this measure would indicate circadian disruption.62,64 The methodology for processing per-minute step counts data and detailed metric extraction are presented in the Supplementary (eMethods 2-4 and eFigures 1a, 2a, 3, 4a).
Outcome measures of 24-hour heart rate rhythms
Based on previous studies,42,62 the Circadian Quotient (which our prior study termed relative amplitude) 42 was selected as the primary RAR measure of interest for the 24-hour HR Rhythm to provide a clinically interpretable, standardized measure of autonomic regulation (detailed selection rationale in eMethods 1). It is a simple measure of the difference between periods of peak HR and rest HR, allowing for more consistent comparisons across different patients within the study cohort. The same data preprocessing approach of moving average and modeling approaches, including Periodogram and Cosinor Regression, were applied to per-minute HR data (presented in the Supplementary [eMethods 2,5 and eFigures 1b, 2b, 4b]. Then, the Circadian quotient of 24-hour HR rhythm was calculated as the Amplitude of the 24-hour HR Rhythm normalized by mean HR across the day. Lower values of this metric indicate circadian disruption.62,64
Statistical analysis
For analysis, we only included PODs on which the Fitbit computed the daily sleep metrics and resting HR to ensure periods of sleep and wake were both incorporated in the RAR metrics; all other days were excluded. To compare demographic and clinical characteristics between the groups with and without complications, two-sample t-tests were conducted for continuous variables and Chi-square tests for categorical variables. The three RAR metrics were summarized using mean and standard deviation (SD) or the median with interquartile range (IQR) by the groups. Outliers were defined as values exceeding 1.5 times the IQR below the first quartile or above the third quartile to present data distribution and individual differences. 65 Outliers on each POD were incorporated into the curve-fitting processes to account for individual differences. To compare the changes over time, each RAR metric was modeled using smoothing spline regression over the 21-day study period, with the mean of each POD as a knot. Separate models were created for groups with and without complications, and smoothing parameters were estimated using Generalized Cross-Validation (GCV). 66 Next, a nonlinear, cubic-plateau regression was applied to the group without complications to estimate the POD to plateau, along with its 95% confidence interval (CI). Multivariable mixed-effects models were used to compare the main effect of each RAR metric across PODs between the groups with and without complications, accounting for within-subject random effects. The models were also adjusted for sex, age, and race/ethnicity. Statistical analyses were conducted with PyCharm (Python 3.10) and RStudio (R 4.3.3) software (details about packages in eMethods 6). All statistical tests were two-sided, and statistical significance was set as 0.05.
Results
Recruitment, clinical outcomes and wearable data
Of the 127 patients approached during study recruitment, 24 (18.9%) declined participation (eFigure 5). Of the 103 enrolled patients, nine were excluded from the analysis because they did not have any sleep metrics, step count, or HR data available from their Fitbit data. Of the 94 patients included for analysis, 81 had no complications during recovery (86%) and 13 had complications (10 with intra-abdominal abscess, 2 with superficial surgical site infections, and one with a small bowel obstruction).
Cohort characteristics and wearable data availability.

Wearable data summary.

Periodicity of the 24-hour activity rhythm
The Periodicity of the 24-hour Activity Rhythm increased over time for both groups following surgery; however, the increase was delayed in the group with complications. The changes in the Periodicity of the 24-hour Activity Rhythm over the 21-day study period for groups with and without complications were shown in Figure 1(a). A significant difference between the groups was observed when comparing the adjusted means of Periodicity on each POD over the 21-day period (p=.008, linear mixed-effect model). Periodicity of the 24-hour Activity Rhythm. (a) Mean and fitted spline curve for postoperative day (POD) 1-21 for patients with no complications and with complications (p=0.008, linear mixed-effect modeling). (b) Fitted normative recovery trajectory for POD 1-21. The trajectory plateaued on POD 11 (95% confidence interval: POD 9-14). (c) Median, interquartile range and outliers for POD 1-21 for patients without and with complications.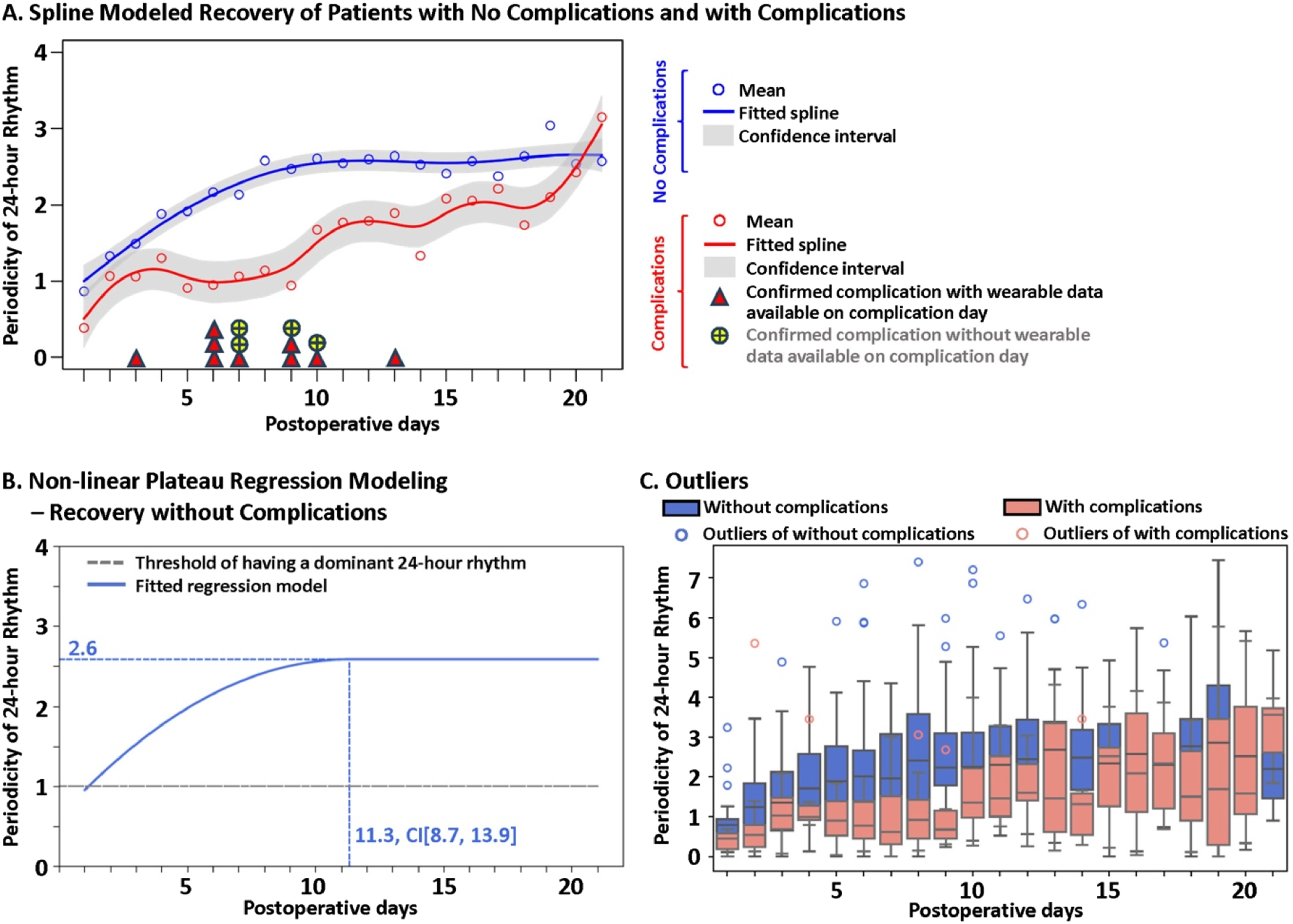
For the normative recovery trajectory, Periodicity of the 24-hour Activity Rhythm reached a plateau at a value of 2.6 on POD 11 (95% confidence interval [CI]: POD 9-14, Figure 1(b)). This suggests that during the early postoperative period, RARs are often absent or weaker than in the later recovery period, with ultradian rhythms (<24-hour period) potentially dominating activity patterns. In contrast, the model failed to converge for the 21-day trajectory of the group with complications, suggesting that the trajectory did not plateau within the 21-day study period or could not be predicted based on the available data. These differences in the recovery trajectories between groups are illustrated in Figure 1(c). Across POD 1-20, a lower proportion of patients with complications exhibited clear RARs compared to those without complications (Figure 2). Proportion of patients with a 24-hour activity rhythm. proportion of patients in each group exhibiting a value >1 for the periodicity of the 24-hour activity rhythm, which indicates a clear 24-hour periodicity in the step count pattern for that day.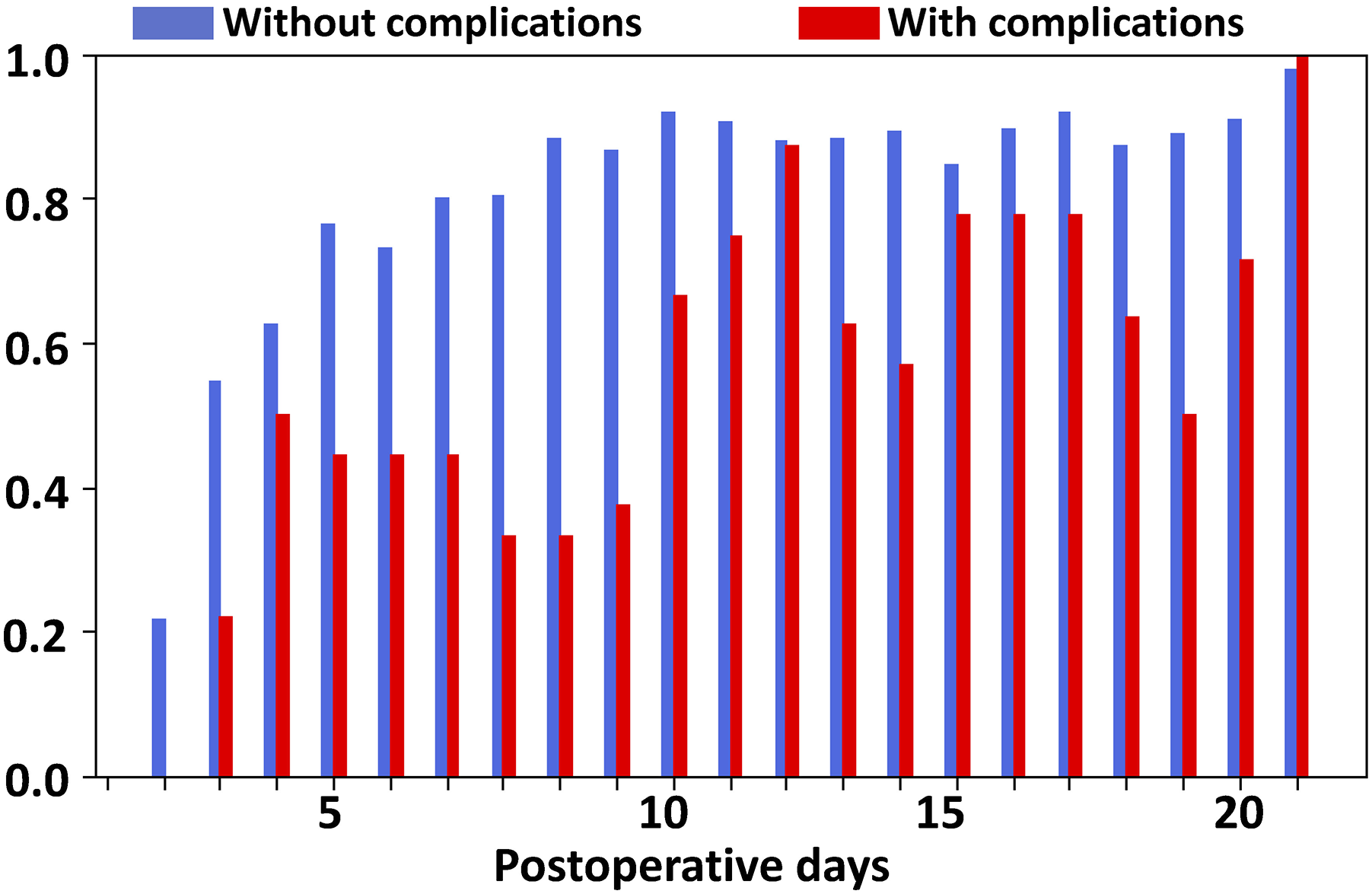
Amplitude of the 24-hour activity rhythm
Like Periodicity, the Amplitude of the 24-hour Activity Rhythm increased over time for both groups, and the group with complications exhibited a delayed increase, not reaching a plateau during the study period. Figure 3(a) illustrates changes in the Amplitude of the 24-hour Activity Rhythm over the 21-day study period for groups with and without complications. The average standard error of the residuals from the cosinor regression was 0.68 in the group without complications and 0.43 in the group with complications. These values are small relative to the overall range of step count measurements in the dataset (0–120 steps/min), supporting the adequacy of the model fit. A significant difference in amplitude was observed between the groups when comparing the adjusted mean on each POD over the 21-day study period (p=.003, linear mixed-effect model). The normative recovery trajectory for the group without complications, shown in Figure 3(b), reached a plateau at the modeled peak amplitude of 6.5 step counts per minute on POD 20 (95% CI: POD 16-24). The trajectory fit for the group with complications did not converge (Figure 3(c)). Amplitude of the 24-hour activity rhythm. (a) Mean and fitted spline curve for postoperative day (POD) 1-21 for patients with no complications and with complications (p=0.003, linear mixed-effect modeling). (b) Fitted normative recovery trajectory for POD 1-21. The trajectory plateaued on POD 20 (95% confidence interval: POD 16-24). (c) Median, interquartile range and outliers for POD 1-21 for patients without and with complications.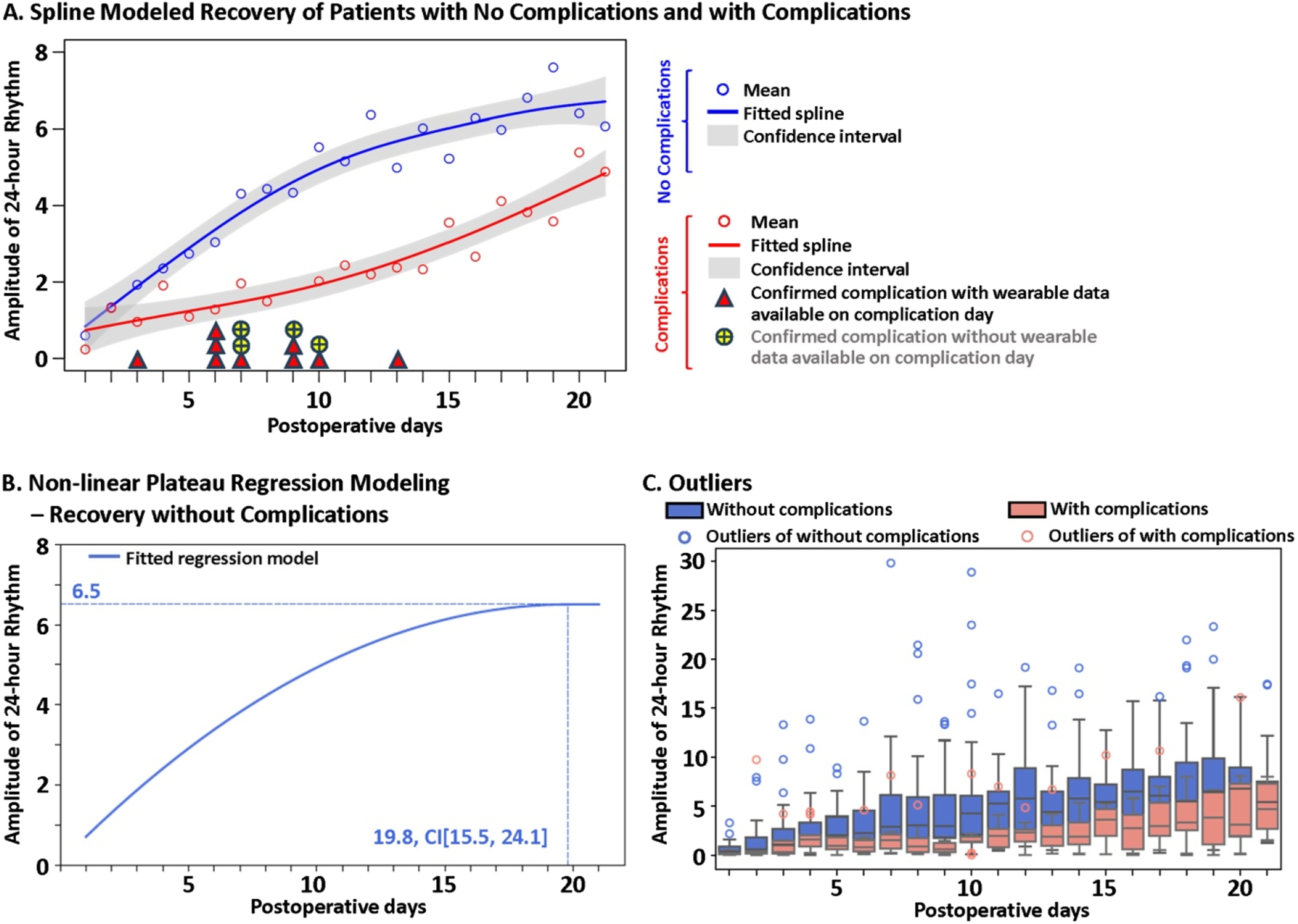
Circadian quotient of the 24-hour heart rate rhythm
Like the activity rhythm metrics, the Circadian quotient of the 24-hour HR Rhythm over the 21-day study period increased for both groups (Figure 4(a)). However, the group with complications exhibited a slower increase than the group without complications and did not reach a plateau during the study period. The mean of standard errors on residuals of the cosinor regression fit was 0.96 for the group without complications, compared to 2.18 for the group with complications. These values are small relative to the overall range of HR measurements in the dataset (40–150 bpm), supporting the adequacy of the model fit. A significant difference was observed between the groups when comparing the adjusted mean values on each POD over the 21-day study period (p<.001, linear mixed-effect model). The normative recovery trajectory fit, shown in Figure 4(b), reached a plateau at the modeled peak amplitude of 0.16 on POD 12 (95% CI: POD 9-15), while the trajectory fit for the group with complications did not converge (Figure 4(c)). Circadian quotient of the 24-hour heart rate rhythm. (a) Mean and fitted spline curve for postoperative day (POD) 1-21 for patients with no complications and with complications (p<0.001, linear mixed-effect modeling). (b) Fitted normative recovery trajectory for POD 1-21. The trajectory plateaued on POD 12 (95% confidence interval: POD 9-15). (c) Median, interquartile range and outliers for POD 1-21 for patients without and with complications.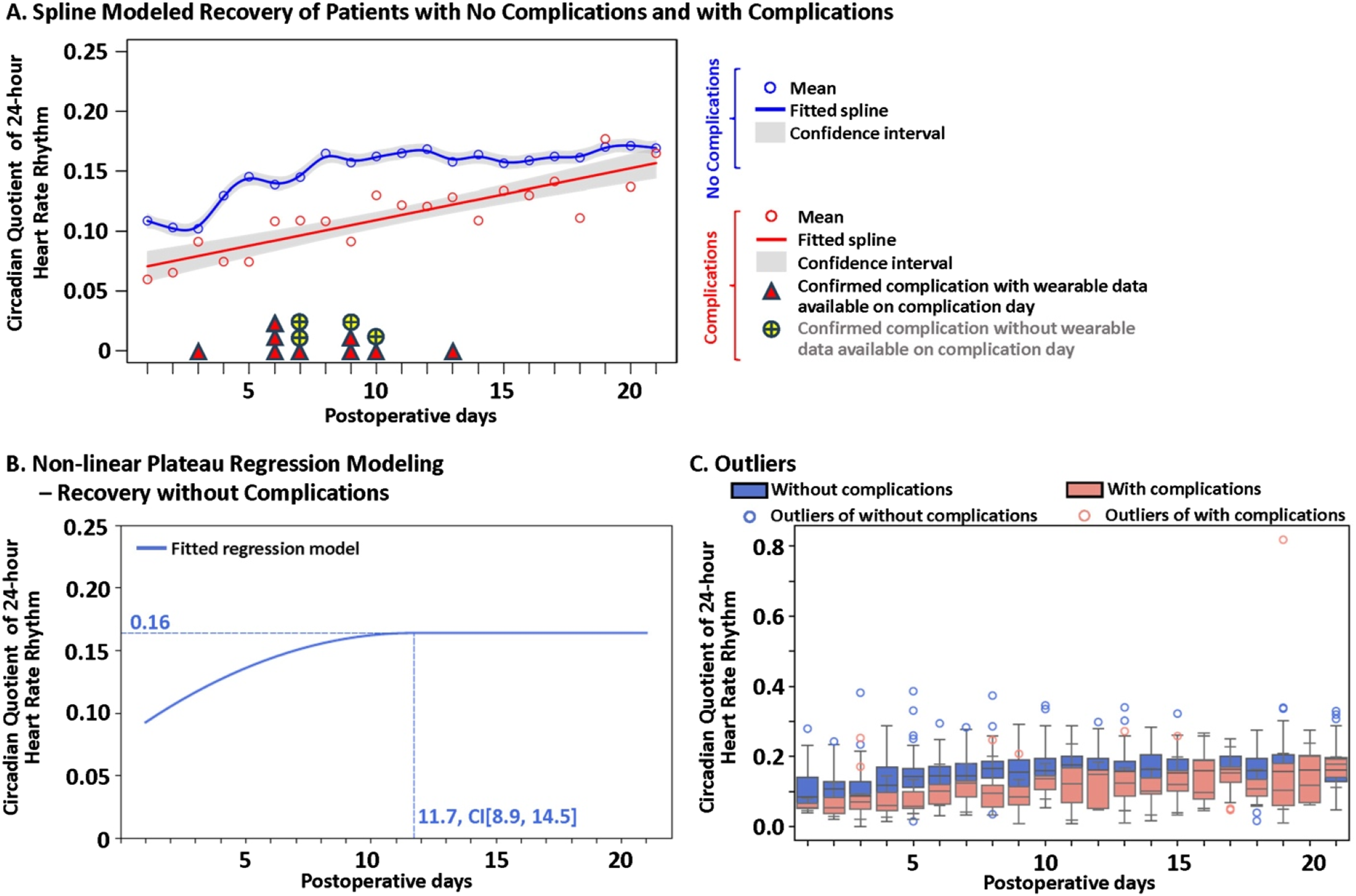
Discussion
To identify practical means for describing circadian rhythms in children post-surgery, we examined daily circadian patterns in HR and activity in children who underwent laparoscopic appendectomy for complicated appendicitis and examined changes in these patterns during the postoperative recovery period. We characterized their normative recovery trajectories using wrist-worn consumer wearable devices over 21 PODs and found differences in children who experienced complications. Our findings highlight the potential of circadian rhythms, quantified through three RAR metrics – Periodicity of the 24-hour Activity Rhythm, Amplitude of the 24-hour Activity Rhythm, and Circadian quotient of HR Rhythm – as novel digital biomarkers for tracking postoperative recovery. Together, these findings have important implications for continuous monitoring of pediatric postoperative recovery remotely in both inpatient and outpatient settings and for the early detection of complications to facilitate precise, efficient, and early treatment for this population.
Our previous studies42,67,68 have demonstrated the potential of machine learning models to analyze patterns of biometric data from consumer wearables and predict postoperative complications during the recovery period. While these studies have offered techniques generate daily predictions about a child’s recovery status, they did not provide insights into underlying data patterns or their changes over time. By characterizing the trajectories of the most predictive circadian metrics during the postoperative period, we sought to further examine the utility of these metrics and increase their interpretability. Other studies have defined procedure-specific normative postoperative recovery trajectories using daily physical activity metrics collected by consumer wearable devices, such as total daily step count, peak step cadence or pulse rate variability69–74; however, cumulative daily step count metrics are limited as they only measure activity volume without accounting for the timing of activity throughout the day. In contrast, we modeled RARs using a 15-minute sampling window to capture activity variation with more precise timestamps. This approach allows us to detect activity patterns throughout the day and night; wherein nighttime activity may indicate poor sleep and would not be reflected by total daily step counts. Furthermore, circadian metrics related to HR may have additional practical value since HR is commonly considered during clinical evaluations. 45 Using affordable consumer wearables and simplified metrics to track daily fluctuations in activity and HR fills a current gap in the ability to examine circadian rhythms in clinical and community settings. These trajectories can inform additional modeling techniques, such as near-real-time anomaly detection, with the goals of strengthening early detection and providing more interpretable, actionable insights to clinicians about the relationship between circadian disruption and complication onset.
Our results demonstrate that circadian rhythms can function as references for normative recovery and highlight differences in children experiencing a complication. The three novel RAR metrics showed delayed recovery in the presence of complications. This aligns with our prior studies that found that wearable-derived metrics, such as total daily step counts and cadence, were shown to predict postoperative complications before clinical diagnosis.70,72 Deviations from normative trajectories may serve as early alerts for developing complications and enable more timely interventions. Incorporating these insights into clinical practice could reduce the need for emergency department visits, hospitalization, or repeat intervention.70,72
This study also introduces a digital phenotyping methodology, which provides continuous, objective quantification of human behavior, physiology, and health-related functioning using data collected from wearables, for extracting RAR rhythms as digital biomarkers and exploring their clinical utility with potential applications in other pediatric populations. Activity and heart rate rhythms have been recently proposed by multiple studies as digital biomarkers for adults to compare and monitor the progression of Alzheimer’s disease, 56 Parkinson’s disease, 75 depression, 58 infectious diseases such as COVID-19, 76 and mood disorders.77–79 To our knowledge, this study marks the first step in investigating circadian rhythms in both activity and HR as biomarkers for postoperative monitoring in children. Future work should consider extending this methodology to monitor postoperative recovery in children undergoing other surgical procedures, such as pectus excavatum, 80 tonsillectomy, 81 orthopedics, 82 oncologic resections, 83 and postoperative pain management. 84 It could be applied to assess other physiological changes (e.g., body core temperature) during postoperative recovery, allowing wearables to provide additional clinical value for continuous vital sign monitoring in children. These concepts align with prior work employing mathematical and statistical models to predict circadian markers from wrist-worn wearables and activity data,85,86 offering a practical alternative to traditional markers such as dim light melatonin onset, which are challenging to assess continuously or in real time.
Several considerations remain to successfully incorporate wearables into the postoperative continuum of care. In this study, although the importance of continuously wearing the Fitbit was emphasized to participants and their caregivers throughout the data collection (i.e., during recruitment and follow-up phone calls), non-adherence and missing data were still prevalent in the dataset, which is likely reflective of real-world deployment scenarios. Thus, educational materials, as well as technical and clinical support systems, will be critical to build for widespread implementation, which are suited for families of varying digital and medical literacy. Furthermore, while data were deidentified in the current study, data security and privacy regulations must be developed for the pediatric population, since it is possible that these data could also be integrated into EHR.
In addition to monitoring, RAR metrics could be used to guide the timing of treatments, an approach known as chronotherapy. For example, recent work has indicated that the timing of chemotherapy 87 and cardiac surgery 88 during the day may affect patient outcomes. These metrics can also inform personalized interventions to realign the circadian clock, such as bright light exposure or structured activity regimens. 89
Limitations
The limitations of this study should be considered when interpreting the findings. From a study design perspective, the comparison between patients with and without postoperative complications is constrained by our cohort’s small number of complications. Spline curves could only be generated for the cohort with complications since the recovery trajectory did not converge. It remains unclear whether this is due to the nature of the wearables data related to the complications or our cohort’s size. This study also followed patients through POD 21 only. While we assume that the cohort with complications will eventually reach stability in RAR values, this was not demonstrated within the 21-day period and warrants further study. Moreover, relying on the proposed metrics to detect complications may not capture all cases due to individual variability in postoperative recovery. However, the normative recovery trajectories can serve as a reference for generating threshold-based alerts for clinical check-ins after hospital discharge, during the early postoperative time when complications are likely to develop.
In terms of device and data limitations, the devices and data export used in this study did not provide estimates of sleep onset, midpoint, or wake times, limiting our ability to directly calculate sleep-specific circadian misalignment. 90 In the future, next-generation wearables and validated sleep estimation methods91–93 could be leveraged to further characterize potential circadian or RAR misalignment in pediatric populations. Furthermore, because appendectomy is often an emergency procedure, preoperative data were unavailable for comparisons to a per-participant baseline. Future studies incorporating preoperative baselines can offer greater insights into circadian differences during recovery, and should also explore other circadian metrics such as acrophase. 94
Finally, several external and analytic factors should be considered. There are many factors that can influence circadian rhythms, such as postoperative recovery, stress, pain, medication, light exposure, feeding schedules, exercise, and social activities. Due to the practical limitations of unconstrained, real-world data collection in this study, it is nearly impossible to isolate the effect of each factor on the wearables data in this study. Further studies or methods may be needed to evaluate how these and other factors affect circadian rhythms during recovery to develop more personalized approaches to monitoring and intervention. Similarly, we did not attempt to decouple the effect of physical activity from heart rate in the recorded signals. Although other studies have estimated this using predictive models, 95 we determined this was not feasible given the amount of missing data in the daily time series recordings and its unknown impact on the generalizability of such an approach. Future work may consider imputation based on the correlated or prior data to address this issue, but additional validation would be needed given the high level of variability in pediatric populations. Future work should also assess the applicability of our findings across additional surgical procedures, at diverse institutions, and within adult surgical populations.
Conclusion
We examined changes in RAR extracted from HR and activities for children who underwent laparoscopic appendectomy for complicated appendicitis using consumer wearable devices during hospitalization and post-discharge. We characterized normative trajectories over a 21-day postoperative period and observed delayed RAR recovery in patients who experienced complications. These trajectories offer a new method for evaluating postoperative recovery, positioning RAR derived from wearables as digital biomarkers for the remote monitoring and early identification of complications.
Supplemental material
Supplemental material - Rest-activity rhythmicity as digital biomarkers of postoperative recovery and complications in children
Supplemental matraial for Rest-activity rhythmicity as digital biomarkers of postoperative recovery and complications in children by Michela Carter, Rui Hua, Megan K. O’Brien, Hangil Lee, J. Benjamin Pitt, Soyang Kwon, Renee C. B. Manworren, Austin Chen, Arianna Edobor, Jane Holl, Arun Jayaraman, Hassan MK Ghomrawi, MPH and Fizan Abdullah in Digital Health.
Supplemental material
Supplemental material - Rest-activity rhythmicity as digital biomarkers of postoperative recovery and complications in children
Supplemental matraial for Rest-activity rhythmicity as digital biomarkers of postoperative recovery and complications in children by Michela Carter, Rui Hua, Megan K. O’Brien, Hangil Lee, J. Benjamin Pitt, Soyang Kwon, Renee C. B. Manworren, Austin Chen, Arianna Edobor, Jane Holl, Arun Jayaraman, Hassan MK Ghomrawi, MPH and Fizan Abdullah in Digital Health.
Footnotes
Acknowledgments
Thank you to Angie Figueroa for her contributions to patient recruitment for this study.
Ethical considerations
The Institutional Review Board at the Ann and Robert H. Lurie Children’s Hospital of Chicago approved the study (IRB: #2018-1836).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute Of Nursing Research of the National Institutes of Health under Award Number R01NR020918. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.