
Abstract
Background
New digital technologies and platforms have enabled the additional provision of mental health services to counter the increased prevalence of mental health problems among children and adolescents. This real-world retrospective cohort study evaluates engagement levels and symptom improvement among children and adolescents receiving care through one such technology-enabled platform, and examines differences by gender and age group.
Methods
We used descriptive, bivariate, and multiple logistic regression analyses to characterize the number of visits and depressive and anxiety symptom improvements among children and adolescents aged 9 to 17 with elevated depressive symptoms (n=9,853) and/or elevated anxiety symptoms (n=9,996) seen by a Grow Therapy therapist between January 2022 and April 2024. We also examined differences in engagement and outcomes by gender and age group.
Results
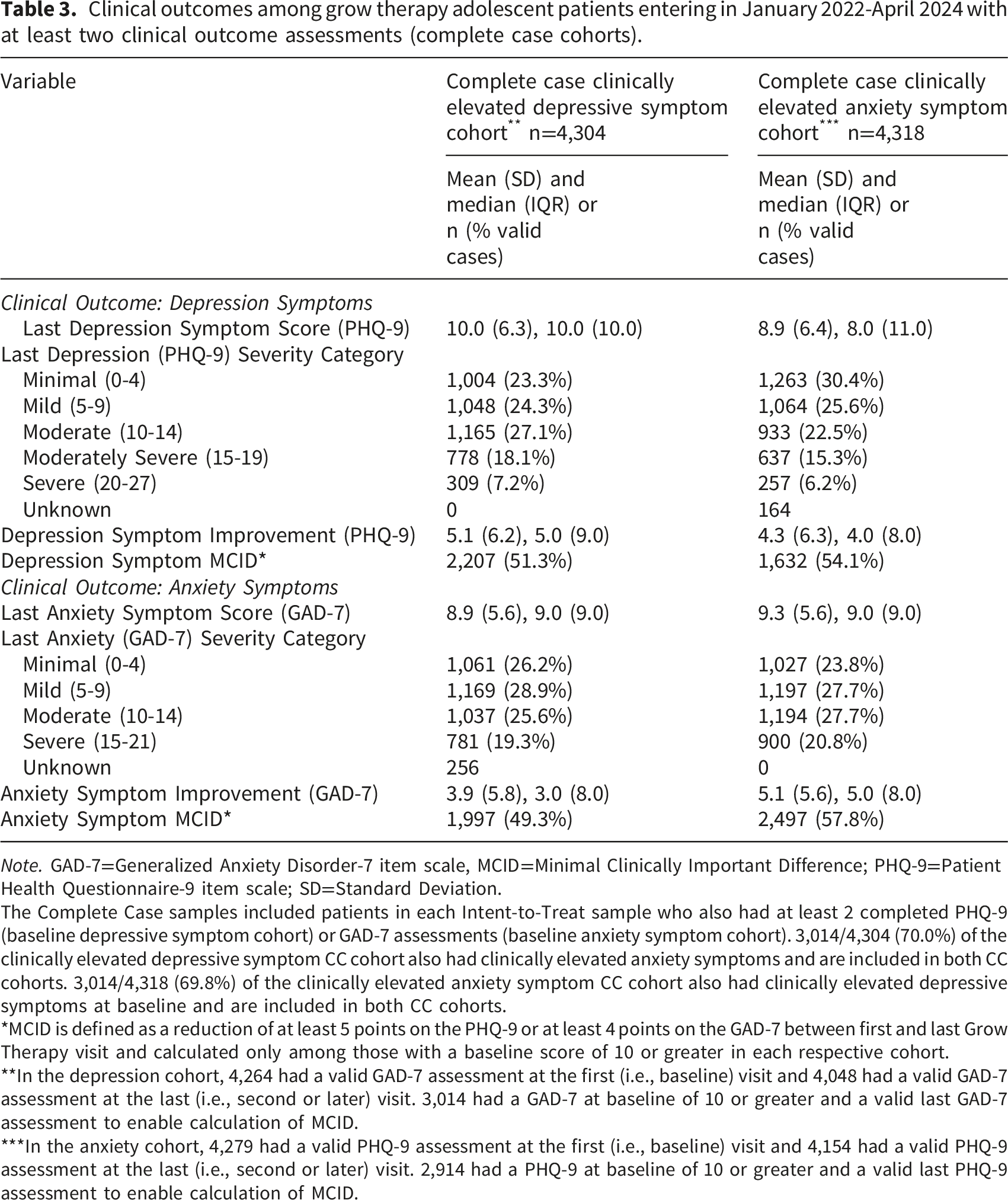
Over half of the depressive and anxiety symptom cohorts, respectively, experienced a minimal clinically significant difference (MCID) in depressive symptoms (51.3%) and anxiety symptoms (57.8%). Although there were no significant interactions between gender and age group, females were less likely than males to meet criteria for MCID in the depressive and anxiety symptom cohorts despite being more likely to attend at least 3 provider visits.
Conclusions
Preliminary findings suggest that therapists employed by Grow Therapy may have the potential to provide effective and engaging treatment for child and adolescent mental health. Gender differences in outcomes suggest the possible need for tailored care considerations for adolescent females.
Keywords
There has been a marked increase in mental health problems among adolescents over the past few decades.1,2 Moreover, these issues have disproportionately affected female adolescents and younger adolescents relative to their male and older counterparts, respectively. 3 Hypotheses made to explain the alarming rates have included the corresponding increasing rates of sedentary behavior, obesity, screen time,4–7 and particularly problematic use of social media.8–10 These increases were further accelerated by the isolation imposed by COVID-19. 11 As a result of the pandemic, the American Academy of Pediatrics together with the American Academy of Child and Adolescent Psychiatrists and the Children’s Hospital Association declared a United States national state of emergency, 12 and the Surgeon General issued an urgent public health advisory about youth mental health. 13 Despite the increased attention paid to adolescent mental health problems, however, only about half of those in need receive treatment. 14 Parents and guardians historically have been the main driver of adolescent mental health treatment seeking behaviors, with their preferences influencing the type of treatments sought and received by their adolescent children. Nevertheless, barriers including cost, provider shortages, stigma, and communication difficulties between parents and adolescents continue to limit access to necessary treatment.14–16
The explosion of virtual and digital mental health treatments has provided additional methods and modalities of providing mental health services. One such new model of care focuses on connecting patients with providers and payers (e.g., insurers) using a technology-enabled platform to deliver a choice of remote, digital services tailored to the patient’s preferences. Some of these newer entities allow an interested patient or, in the case of care sought for an adolescent, one of their parents or guardians to select the characteristics of a preferred provider based on their preferences and insurance carrier.
Despite rapid growth in teletherapy and digital mental health services, engagement patterns and clinical outcomes in newer technology-enabled, platform-based models of care for adolescents remain poorly characterized.17–19 Existing evidence for telemental health treatment in youth largely derives from traditional telepsychiatry or protocolized telehealth interventions, which have generally demonstrated comparable engagement and modest but clinically meaningful improvements in depression and anxiety symptoms under controlled conditions.20–22 The supporting literature, however, has primarily relied on small samples, focused on clinician- or intervention-driven models rather than commercial platforms that encourage patient choice of provider characteristics, and been conducted largely in research or pilot settings rather than real-world care environments.22–24
Moreover, few studies have described engagement trajectories or symptom change among adolescents receiving care through large-scale commercial technology-enabled platforms. This gap persists despite adult digital mental health research documenting substantial real-world variability in engagement and outcomes outside of clinical trials.25,26 Understanding these trajectories is particularly salient for adolescents, given well-documented gender- and age-related differences in mental health presentation, care-seeking, and treatment response during this developmental period.27–29
In light of these limitations, the objectives of this retrospective cohort analysis were to descriptively characterize engagement and symptom change among adolescents receiving care through a single commercial technology-enabled mental health care platform, and to examine whether these patterns differed by gender and age group. By leveraging large-scale, real-world data, this study extends prior telehealth research by providing descriptive evidence from a care setting that more closely reflects contemporary mental health treatment delivery.
Methods
Sample and study design
This retrospective cohort study included two intent-to-treat (ITT) cohorts of adolescent patients aged 9 to 17 years with a first Grow Therapy provider visit between January 1, 2022 and April 30, 2024. Cohort 1 comprised patients with at least moderate depressive symptoms (n=9,853) and Cohort 2 comprised patients with at least moderate anxiety symptoms (n=9,996), as detailed below. There was sizable overlap in the two ITT cohorts, with 7,153/9,853 (72.6%) of the clinically elevated depressive symptom ITT cohort also having clinically elevated anxiety symptoms and 7,153/9,996 (71.6%) of the clinically elevated anxiety symptom ITT cohort also having clinically elevated depressive symptoms at baseline. The CC samples used for clinical symptom analyses required at least two PHQ-9 or two GAD-7 assessments to enable the computation of a change score and included 4,304 patients in the depressive symptom cohort (43.7% of the corresponding ITT sample) and 4,318 patients in the anxiety symptom cohort (43.2% of the corresponding ITT sample). Again, there was sizable overlap in the two ITT cohorts, with 3,014/4,304 (70.0%) of the clinically elevated depressive symptom CC cohort also having clinically elevated anxiety symptoms and 3,014/4,318 (69.8%) of the clinically elevated anxiety symptom CC cohort also having clinically elevated depressive symptoms at baseline. (Figure 1). Adolescent patients aged 9 to 17 with a first grow therapy visit in January 2022-April 2024 with elevated baseline depressive or anxiety symptoms.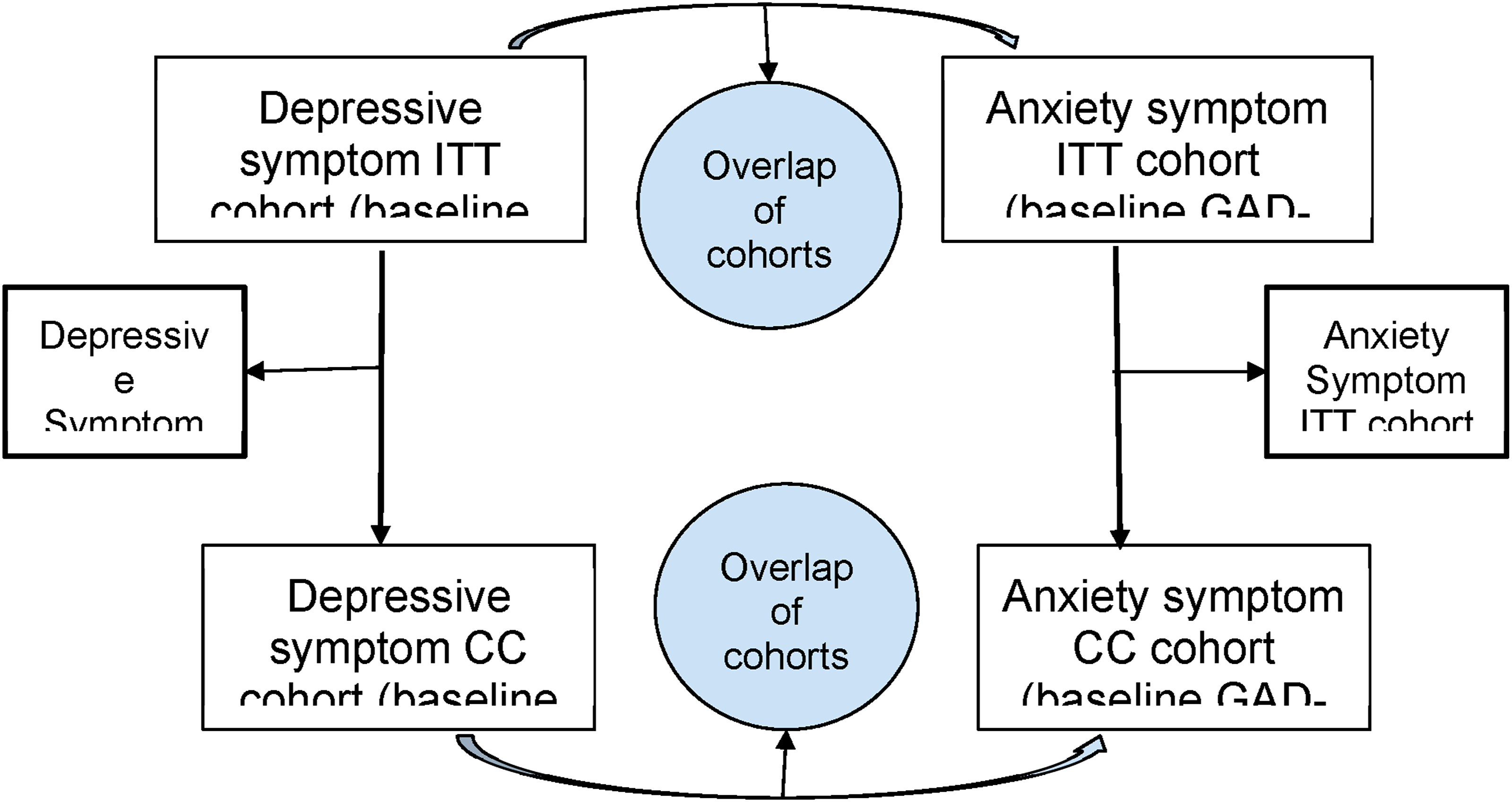
Deidentified data included demographic and clinical data collected as part of treatment engagement as well as the number of visits each patient had with a Grow Therapy mental health provider. Data collected through April 30, 2025 were included to allow at least 12 months of follow-up per patient. A parent or guardian of each eligible adolescent Grow Therapy patient signed a privacy policy agreement that allowed the conduct of research using de-identified collected data in cases that followed a prescribed review protocol to ensure that both privacy and research needs were met.
Grow Therapy treatment
Grow Therapy is a commercial, technology-enabled mental health platform integrated with commercial insurance companies. Mental health treatment from a Grow Therapy provider consisted of mostly telehealth-delivered psychotherapy, pharmacotherapy, or both. Providers were licensed providers such as professional counselors, social workers, psychologists, and psychiatric prescribers such as psychiatric mental health nurse practitioners (PMHNPs) and medical doctors (MDs). Parents or guardians visited the Grow Therapy website to enroll their adolescent in treatment. Site visitors were able to select preferred provider characteristics (i.e., clinical specialty, provider demographic and identity characteristics). Grow’s algorithm then matched the prospective patient with providers who fit their search criteria and who had availability in the upcoming days. The total number of visits varied by patient based on what was clinically indicated.
Data, including protected health information, collected as part of Grow Therapy provided care is stored in Health Insurance Portability and Accountability Act-compliant electronic medical records. The WCG IRB granted approval of the study as exempt under 45 CFR § 46.104(d) (4).
Outcomes and analyses
Data collected prior to program enrollment included demographics of the patient’s gender (female, male, “other”) and age (categorized into 9-11, 12-14, and 15-17). Engagement data consisted of the number of individual or family outpatient psychotherapy, medication evaluation, or medication management non-cancelled visits (i.e., number of visits). This variable was dichotomized in two ways: (1) 3 or more versus fewer than 3 visits, to approximate the threshold for establishing peak therapeutic alliance, 30 and (2) 12 or more versus fewer than 12 visits, to approximate the length of a typical adolescent mental health intervention. 31
Clinical outcome measures collected prior to the first visit and then upon provider request or at every third visit consisted of the Patient Health Questionnaire-9 item scale (PHQ-9) to measure depressive symptoms 32 and the Generalized Anxiety Questionnaire-7 item scale (GAD-7) to measure anxiety symptoms. 33 Both patient-reported outcome instruments are reliable and validated measures of respective symptomatology for depression 34 and anxiety. 35 Both PHQ-9 and GAD-7 scores were classified by severity as follows: minimal (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20+) depressive symptoms measured by the PHQ-9 31 and minimal (0-4), mild (5-9), moderate (10-14), and severe (15+) anxiety symptoms measured by the GAD-7. 33 Thus, the depressive symptom cohort included patients with a score of 10 or greater on the PHQ-9 and the anxiety symptom cohort included patients with a score of 10 or greater on the GAD-7. The change between the first and last assessments were categorized into having a minimum clinically important difference (MCID) yes versus no, defined as a reduction in symptoms of 5 or more points among those starting with a score of 10 or higher for the PHQ-9 and a reduction of 4 or more points among those starting with a score of 10 or higher for the GAD-7.36–38
Analyses were conducted in R software 39 separately for each cohort (depressive and anxiety symptom cohorts) using either the ITT or CC sample, depending on the outcome of interest. The ITT sample cohorts include all adolescents with at least moderate levels of depressive and/or anxiety symptoms who had at least one visit with a Grow Therapy provider. The CC sample cohorts included those in the ITT respective cohorts who had at least two PHQ-9 assessments (in the depressive symptom cohort) or two GAD-7 assessments (for the anxiety symptom cohort).
Demographics and baseline clinical characteristics were summarized using simple descriptive statistics in each cohort (the depressive and the anxiety symptom cohorts) and each sample (ITT and CC). Engagement analyses included patients in each ITT sample cohort and consisted of (1) chi-square tests, or Fisher’s Exact tests when expected cell sizes were low, and Bonferroni post-hoc comparisons to test unadjusted associations and (2) logistic regression to test adjusted associations between gender, age group, and having at least 3 visits with a Grow Therapy provider. Clinical outcome analyses consisted of the same unadjusted and adjusted analyses for whether each patient experienced depressive symptom and anxiety symptom changes that met criteria for MCID in the CC samples for each cohort. Regression models adjusted for baseline symptom levels, gender, age group (and number of visits in the clinical outcome models) yielded odds ratios with 95% confidence intervals (CIs). An interaction term was included in each model to examine whether associations differed by gender/age group combination. If interaction was not significant, main effects of both gender and age group were examined. Additional ANOVA and Bonferroni post-hoc tests were conducted for gender and age group differences of significant main effects identified. A 2-sided P ≤ .05 was considered indicative of statistical significance. Logistic regression diagnostics were conducted to assess multicollinearity, influential observations, and linearity of continuous predictors with the logit. No violations were identified that materially altered model estimates.
Analyses also were performed on each ITT sample cohorts (depressive symptom cohort n=9,853 and anxiety symptom cohort n=9,996) to compare those included (n=4,304 and n=4,318, respectively) versus not included (n=5,549 and n=5,678, respectively) in the CC sample (see Figure 1) to determine differences in the ITT and CC samples that would impede the generalizability of the findings. Chi-square tests were used to determine differences in those in versus not in the CC cohorts by gender and by age group, and Wilcoxon Rank Sum tests were used to determine differences in those in versus not in the CC cohorts by baseline levels of PHQ-9 and GAD-7 because of non-normality of that data. Medians and interquartile ranges (IQRs) were reported for any significant Wilcoxon Rank Sum tests by included status, as well.
Results
Sample
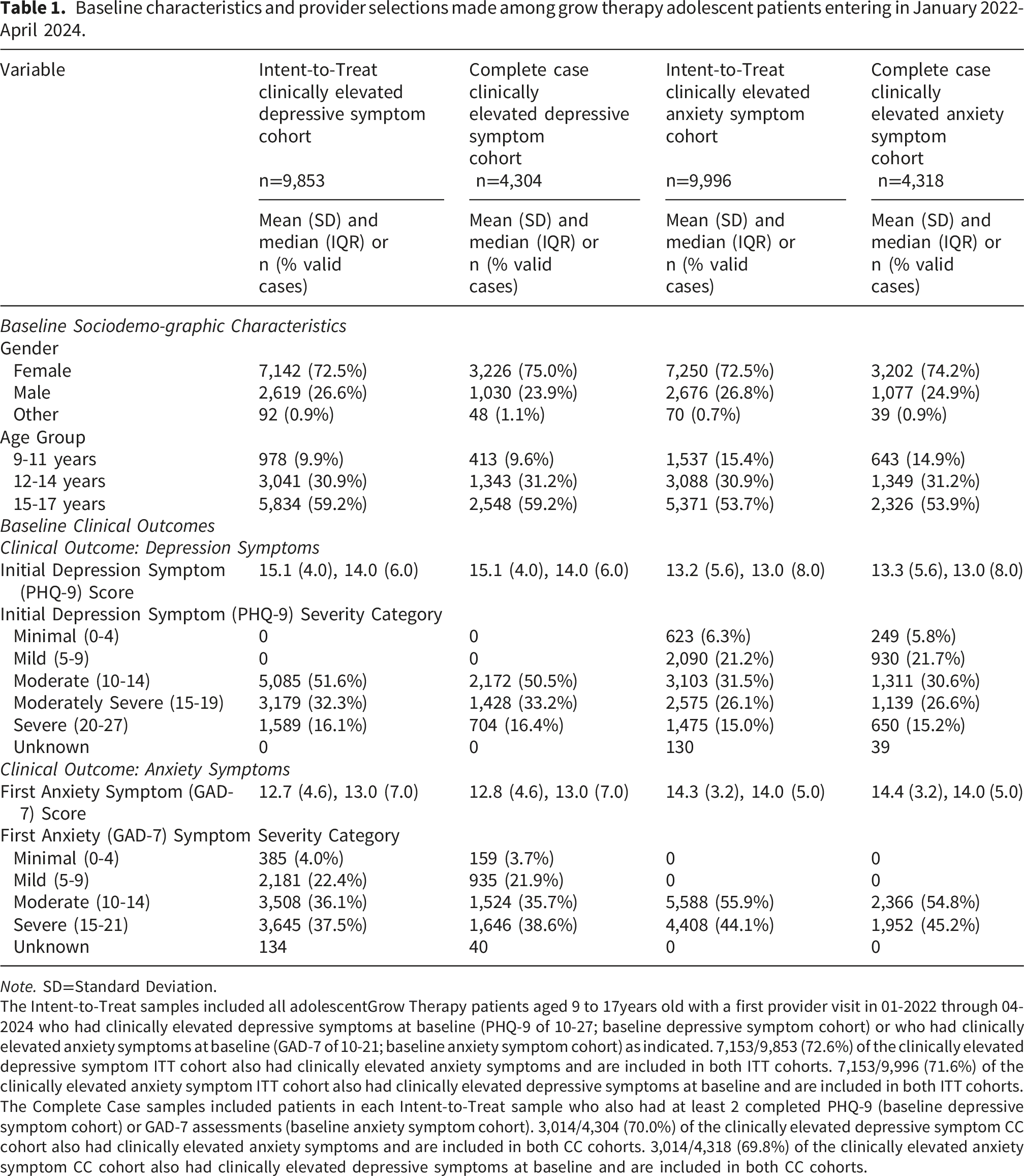
Baseline characteristics and provider selections made among grow therapy adolescent patients entering in January 2022-April 2024.
Note. SD=Standard Deviation.
The Intent-to-Treat samples included all adolescentGrow Therapy patients aged 9 to 17years old with a first provider visit in 01-2022 through 04-2024 who had clinically elevated depressive symptoms at baseline (PHQ-9 of 10-27; baseline depressive symptom cohort) or who had clinically elevated anxiety symptoms at baseline (GAD-7 of 10-21; baseline anxiety symptom cohort) as indicated. 7,153/9,853 (72.6%) of the clinically elevated depressive symptom ITT cohort also had clinically elevated anxiety symptoms and are included in both ITT cohorts. 7,153/9,996 (71.6%) of the clinically elevated anxiety symptom ITT cohort also had clinically elevated depressive symptoms at baseline and are included in both ITT cohorts. The Complete Case samples included patients in each Intent-to-Treat sample who also had at least 2 completed PHQ-9 (baseline depressive symptom cohort) or GAD-7 assessments (baseline anxiety symptom cohort). 3,014/4,304 (70.0%) of the clinically elevated depressive symptom CC cohort also had clinically elevated anxiety symptoms and are included in both CC cohorts. 3,014/4,318 (69.8%) of the clinically elevated anxiety symptom CC cohort also had clinically elevated depressive symptoms at baseline and are included in both CC cohorts.
Baseline patient characteristics, provider selection, and differences between the ITT and CC samples of each cohort
Females were more likely to be in the CC samples than males of both the depressive and anxiety symptom cohorts (Table 1), indicating that data were not missing completely at random and the findings of the CC cohorts are not completely representative of the ITT samples. No significant differences were determined by included status in the CC samples for age group or for baseline PHQ-9. The Wilcoxon Rank Sum test comparing those in the anxiety cohort by included status in the CC sample was significant (p=0.03), however, the means and SDs were nearly identical for those included and not included in the CC sample (15.3±3.2 and 15.4±3.2, respectively) and the medians and IQRs were the same (14(5)).
Engagement in the ITT samples of each cohort
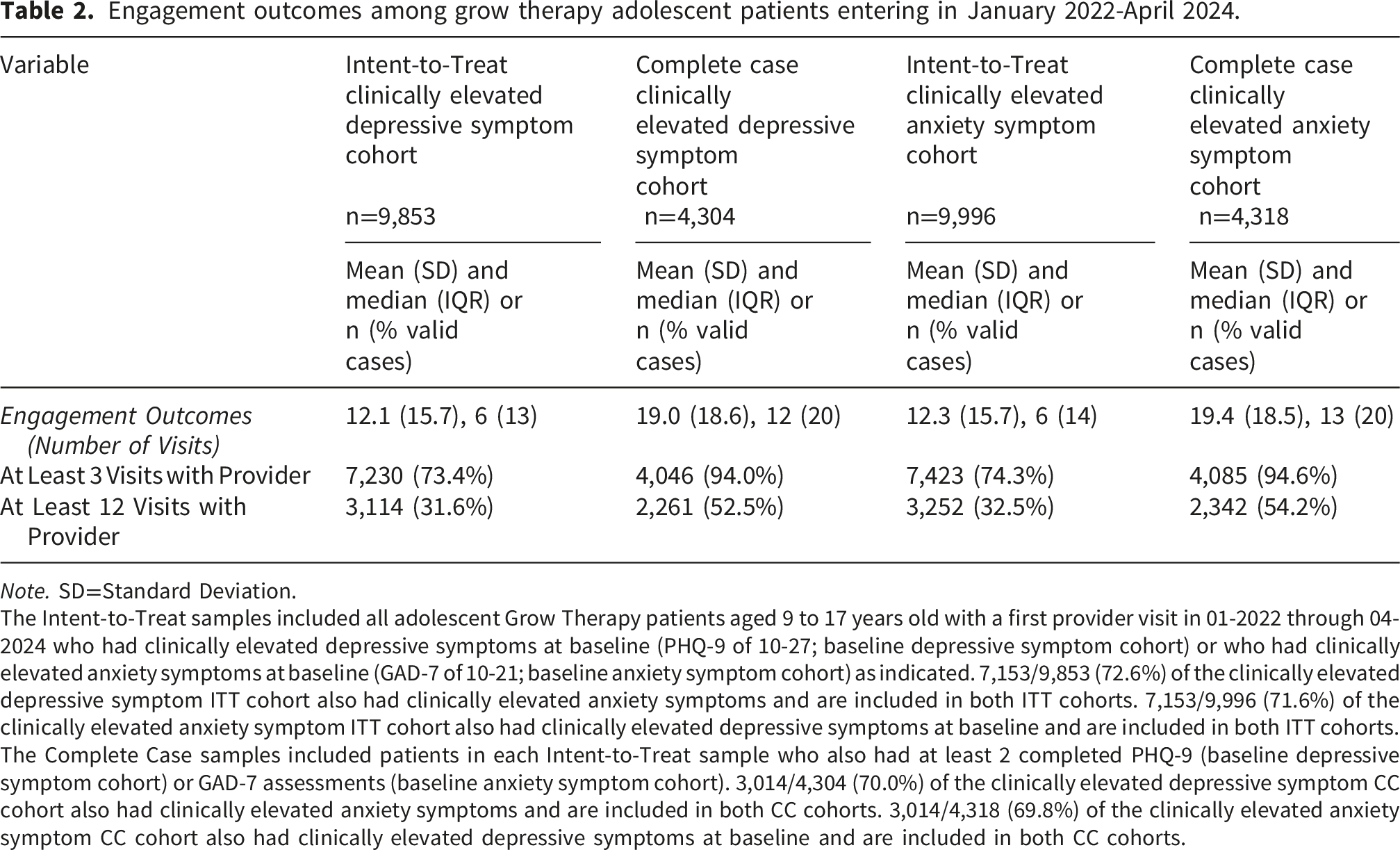
Engagement outcomes among grow therapy adolescent patients entering in January 2022-April 2024.
Note. SD=Standard Deviation.
The Intent-to-Treat samples included all adolescent Grow Therapy patients aged 9 to 17 years old with a first provider visit in 01-2022 through 04-2024 who had clinically elevated depressive symptoms at baseline (PHQ-9 of 10-27; baseline depressive symptom cohort) or who had clinically elevated anxiety symptoms at baseline (GAD-7 of 10-21; baseline anxiety symptom cohort) as indicated. 7,153/9,853 (72.6%) of the clinically elevated depressive symptom ITT cohort also had clinically elevated anxiety symptoms and are included in both ITT cohorts. 7,153/9,996 (71.6%) of the clinically elevated anxiety symptom ITT cohort also had clinically elevated depressive symptoms at baseline and are included in both ITT cohorts. The Complete Case samples included patients in each Intent-to-Treat sample who also had at least 2 completed PHQ-9 (baseline depressive symptom cohort) or GAD-7 assessments (baseline anxiety symptom cohort). 3,014/4,304 (70.0%) of the clinically elevated depressive symptom CC cohort also had clinically elevated anxiety symptoms and are included in both CC cohorts. 3,014/4,318 (69.8%) of the clinically elevated anxiety symptom CC cohort also had clinically elevated depressive symptoms at baseline and are included in both CC cohorts.
Clinical outcomes in the CC samples of each cohort
Clinical outcomes among grow therapy adolescent patients entering in January 2022-April 2024 with at least two clinical outcome assessments (complete case cohorts).
Note. GAD-7=Generalized Anxiety Disorder-7 item scale, MCID=Minimal Clinically Important Difference; PHQ-9=Patient Health Questionnaire-9 item scale; SD=Standard Deviation.
The Complete Case samples included patients in each Intent-to-Treat sample who also had at least 2 completed PHQ-9 (baseline depressive symptom cohort) or GAD-7 assessments (baseline anxiety symptom cohort). 3,014/4,304 (70.0%) of the clinically elevated depressive symptom CC cohort also had clinically elevated anxiety symptoms and are included in both CC cohorts. 3,014/4,318 (69.8%) of the clinically elevated anxiety symptom CC cohort also had clinically elevated depressive symptoms at baseline and are included in both CC cohorts.
*MCID is defined as a reduction of at least 5 points on the PHQ-9 or at least 4 points on the GAD-7 between first and last Grow Therapy visit and calculated only among those with a baseline score of 10 or greater in each respective cohort.
**In the depression cohort, 4,264 had a valid GAD-7 assessment at the first (i.e., baseline) visit and 4,048 had a valid GAD-7 assessment at the last (i.e., second or later) visit. 3,014 had a GAD-7 at baseline of 10 or greater and a valid last GAD-7 assessment to enable calculation of MCID.
***In the anxiety cohort, 4,279 had a valid PHQ-9 assessment at the first (i.e., baseline) visit and 4,154 had a valid PHQ-9 assessment at the last (i.e., second or later) visit. 2,914 had a PHQ-9 at baseline of 10 or greater and a valid last PHQ-9 assessment to enable calculation of MCID.
Relationship of engagement and clinical outcomes to gender and age group in the ITT and CC samples of each cohort, respectively
Unadjusted and adjusted analyses predicting having at least three provider visits, minimum clinically important difference change in depressive symptoms, and minimum clinically important difference change in anxiety symptoms from age group and gender among grow therapy adolescent patients entering in January 2022-April 2024.

Note. GAD-7=Generalized Anxiety Disorder-7 item scale, MCID=Minimal Clinically Important Difference; PHQ-9=Patient Health Questionnaire-9 item scale; SD=Standard Deviation.
The Intent-to-Treat samples used for the engagement models (models 1 and 3) included all adolescentGrow Therapy patients aged 9 to 17 years old with a first provider visit in 01-2022 through 04-2024 who had clinically elevated depressive symptoms at baseline (PHQ-9 of 10-27; baseline depressive symptom cohort) or who had clinically elevated anxiety symptoms at baseline (GAD-7 of 10-21; baseline anxiety symptom cohort) as indicated. 7,153/9,853 (72.65%) of the clinically elevated depressive symptom ITT cohort also had clinically elevated anxiety symptoms and are included in both ITT cohorts. 7,153/9,996 (71.6%) of the clinically elevated anxiety symptom ITT cohort also had clinically elevated depressive symptoms at baseline and are included in both ITT cohorts. The Complete Case samples included patients in each Intent-to-Treat sample who also had at least 2 completed PHQ-9 (baseline depressive symptom cohort) or GAD-7 assessments (baseline anxiety symptom cohort). 3,014/4,304 (70.0%) of the clinically elevated depressive symptom CC cohort also had clinically elevated anxiety symptoms and are included in both CC cohorts. 3,014/4,318 (69.8%) of the clinically elevated anxiety symptom CC cohort also had clinically elevated depressive symptoms at baseline and are included in both CC cohorts. The Complete Case samples used for the clinical symptom models (models 2 and 4) included patients in each Intent-to-Treat sample who also had at least 2 completed PHQ-9 (baseline depressive symptom cohort) or GAD-7 assessments (baseline anxiety symptom cohort). Models adjusted for patient age group (all models), gender (all models), baseline depression symptoms (all models models), baseline anxiety symptoms (all models), and number of visits (models 2 and 4). Unadjusted comparisons done via chi-square tests.
*Fisher’s Exact Test used instead of Chi-Square Test due to low expected counts in the “Other” gender cells.
**MCID is defined as a reduction of at least 5 points on the PHQ-9 or at least 4 points on the GAD-7 between first and last Grow Therapy visit and calculated only among those with a baseline score of 10 or greater in each respective cohort (n=4,304 for depressive symptom MCID in the depression cohort and n=4,318 for anxiety symptom MCID in the anxiety cohort).
1Male vs. Female pairwise Fisher’s Exact Test is significant p=.02 but neither other pairwise comparison is significant (Male vs. “Other” p=0.19 and Female vs. “Other” p=0.40.
2Male vs. Female pairwise Fisher’s Exact Test is significant p<0.01 but neither other pairwise comparison is significant (Male vs. “Other” p=0.24 and Female vs. “Other” p=0.89.
3Pairwise chi-square test is significant for 9-11 years vs. 15-17 years p=0.03 but the other pairwise comparisons were not (9-11 years vs. 12-14 years p=0.77 and 12-14 years vs. 15-17 years p=0.27).
4Male vs. Female pairwise Fisher’s Exact Test is significant p=0.04 but neither other pairwise comparison is significant (Male vs. “Other” p=0.45 and Female vs. “Other”=0.77).
Discussion
Summary of findings
To our knowledge, this is among the first study to describe the typical levels of engagement and clinical outcomes observed by children and adolescents aged 9-17 receiving treatment for elevated depressive and/or anxiety symptoms by therapists employed by a technology-enabled mental health treatment platform, Grow Therapy, both overall and by gender and age group. Children and adolescents in the study cohorts exhibited high levels of engagement and showed meaningful changes in standardized measures of depression and anxiety symptoms. As hypothesized, females had higher representation in the analytic file, as did older children aged 15-17, possibly because post-hoc analyses determined that baseline levels of symptomatology was higher for females relative to males and also higher with each progressive age group in both depressive and anxiety symptom cohorts.
Although no significant interactions were observed between gender and age group, several main effect analyses yielded significant findings. Males were more likely than females to have symptom improvements meeting criteria for an MCID in both the depressive and anxiety cohorts and, in the depressive cohort, this was despite being less likely to have 3 or more provider visits. In addition, adolescents in the anxiety cohort ages 15-17 were less likely than children ages 9-11 to have at least 3 provider visits, but no differences were found in meeting criteria for anxiety symptom MCID. In addition, children and adolescents identifying as a gender other than male or female appeared more likely to have at least 3 provider visits compared to males and less likely to meet criteria for MCID, although these analyses did not yield statistical significance because of the low sample sizes of those identifying as having a gender identity “other” than male or female. Additional studies focused specifically on children and adolescents identifying as having a non-binary gender identity that have sufficient power to identify significant differences are needed.
Relationship of findings to prior research
Our study findings appeared similar to those from prior published research. First, the ITT sample cohorts each had a mean over 12 visits with a Grow Therapy provider, which is slightly higher than the average of 9.0 visits with a private mental health clinician in 2017-2018 among U.S. adolescents ages 12-17 reported in the literature. 40 Possible contributors may include provider matching, insurance integration, and visit accessibility, though these were not directly tested. Second, like prior studies, our collective study analyses found that female children and adolescents had disproportionately higher levels of baseline symptomatology than their male counterparts,29,41,42 higher levels of engagement (although not significant in the anxiety cohort), but smaller levels of symptom decline that met depressive or anxiety symptom MCID criteria than males. Additional studies are needed to better understand why, despite engagement being higher, female children and adolescents do not have as favorable outcomes as their male counterparts. Although, despite some literature showing a dose-response relationship between engagement and outcomes,43,44 our post-hoc analyses did not reveal significant differences in clinical outcomes by the number of visits like other published research. 29
Implications of findings
Our findings show that technology-enabled platforms that connect patients, providers, and payers such as the Grow Therapy program are utilized by children and adolescents and may lead to significant improvements in depressive and anxiety symptoms, perhaps both statistically and clinically. As compared to males, the greater representation of females and their smaller symptom declines in adjusted models suggest that gender should be considered in treatment planning, although, as previously mentioned, more rigorous study designs are needed to make definitive conclusions.
Limitations and future research directions
This study is not without several limitations that have implications for the need for additional research to fully understand the degree of engagement and symptom changes across different types of sociodemographic characteristics. First, the use of real world data and not a prospective, randomized controlled trial design precludes the confirmation that symptom declines observed were greater than what could have been observed by regression to the mean or spontaneous remission. 45 Thus, no causality can be inferred between use of the Grow Therapy platform and clinical outcomes. Second, less than half of children and adolescents in our ITT cohorts had at least two measurements of both the PHQ-9 and the GAD-7 assessments and were therefore excluded from our CC cohorts. The extent of missingness limited the use of standard imputation techniques. The large proportion of missing data precluded the valid use of missing data techniques to account for the differences between ITT and CC cohorts.46,47 The children and adolescents in the CC dataset were more likely to be female than those in the ITT dataset, so conclusions about males and older adolescents may not generalize to all youth served by the platform. Third, data on treatment modality (psychotherapy vs pharmacotherapy vs combined care or teletherapy vs in-person), medication use, treatment duration, and provider-level clustering were not available in the shared analytic dataset and therefore could not be modeled. In addition, the data do not allow for the possibility that treatment provided outside the Grow Therapy platform could be responsible for the symptom changes experienced. Thus, the findings of the study cannot be attributed to the Grow Therapy platform alone. Grow Therapy has recently implemented several improvements to its data collection processes in order to provide better measurement informed care, so these analyses can be replicated in the future using more robust sample sizes after the data has a chance to mature. Additional investigation of other sociodemographic and clinical characteristics such as race/ethnicity, residential status with respect to living in a mental health provider shortage area or medically underserved area, or other types of mental health challenges experienced and how these factors might influence engagement and clinical outcomes are needed to ensure that the equitability of care provided across a wider range of children and adolescents needing mental health care.
Conclusion
Newer mental health treatment modalities and delivery systems such as technology-enabled platforms that connect patients, providers, and payers are needed to address the increase in mental health challenges and subsequent increase in demand for services provided to children and adolescents observed in recent years. This study shows that Grow Therapy providers offer one such platform to treat depressive and anxiety symptoms that appears to be engaging and associated with significant clinical symptom changes, at least among the sample engaging long enough to have at least one post-baseline mental health visit where the patient completed a repeat PHQ-9 and/or GAD-7 assessment. Exploratory analyses suggested that gender differences in several of the metrics studied support a potential need to consider increased demand for treatment by adolescent females when making treatment decisions. Additional studies are needed to confirm the findings and explore associations with other sociodemographic characteristics of children and adolescents to ensure health equity in care delivery. Our findings should be interpreted cautiously and primarily as descriptive real-world evidence.
Footnotes
Ethical considerations
Data, including protected health information, collected as part of Grow Therapy-provided care is stored in Health Insurance Portability and Accountability Act-compliant electronic medical records.The WCG IRB granted approval of the study as exempt under 45 CFR § 46.104(d) (4).
Consent to participate
A parent or guardian of each eligible adolescent Grow Therapy patient signed a privacy policy agreement that allowed the conduct of research using de-identified collected data in cases that followed a prescribed review protocol to ensure that both privacy and research needs were met.
Consent for publication
A parent or guardian of each eligible adolescent Grow Therapy patient signed a privacy policy agreement that allowed the conduct of research using de-identified collected data in cases that followed a prescribed review protocol to ensure that both privacy and research needs were met.
Author contributions
V.F.H. conceptualized the study, led the analytic plan, conducted the analyses, interpreted findings, and drafted the manuscript. E.H., M.C., and A.G. contributed to data preparation. I.D. and C.G. provided clinical interpretation and contextual input. M.K. contributed to study conceptualization, platform context, and critical manuscript review. All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is a paid consultant to Grow Therapy. All co-authors are employees, earning a salary, benefits, and options from Grow Therapy.
Declaration of conflicting interests
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is a paid consultant to Grow Therapy. All co-authors are employees, earning a salary, benefits, and options from Grow Therapy.
Data Availability Statement
Deidentified data is available from the first author upon reasonable request.