
Abstract
Objective
Adolescents with spina bifida (SB) often face difficulties in developing self-management skills and forming social relationships, both essential for successful healthcare transition. The metaverse, offering psychological safety through avatar-based interactions, presents a promising approach to address these developmental challenges. This pilot study aimed to develop and evaluate the feasibility and acceptability of a metaverse-based program designed to support healthcare transition and improve quality of life in adolescents with SB.
Methods
Following intervention development and expert validation, eight Korean adolescents with SB (aged 13−15 years) were recruited from a tertiary care center. Feasibility and acceptability were evaluated through pre- and post-intervention assessments and interviews.
Results
All participants completed a four-week program, with a 100% retention rate and high satisfaction scores for both the program and metaverse platform. While quantitative changes were not statistically significant, qualitative findings indicated positive experiences, including increased self-management awareness, emotional support through mentorship, and greater engagement facilitated via avatar-based interactions.
Conclusions
The metaverse-based program effectively met the informational and psychosocial needs of adolescents with SB through peer support and avatar-based anonymity. These findings support the potential of metaverse platforms for enhancing healthcare transition in adolescents with SB.
Introduction
Spina bifida (SB) is a congenital neural tube defect characterized by incomplete closure of the spinal column, often leading to lifelong neurological, musculoskeletal, urological, and sexual dysfunction.1–3 Although advances in medical and surgical care have significantly improved survival into adulthood, individuals with SB continue to face complex, lifelong health challenges.4,5 Healthcare management primarily aims to optimize functional status, prevent complications, and improve health-related quality of life (HRQoL), all of which require effective self-management skills and age-appropriate transition guidance.6–8
Adolescence is a critical period marked by increasing independence, identity development, academic progress, and the pursuit of social connection. 9 To successfully navigate these developmental tasks, adolescents with SB must acquire and practice self-management skills.7,10 This is particularly essential because individuals with SB face ongoing demands related to bladder and bowel management, medication adherence, skin integrity monitoring, and mobility maintenance.11,12 Moreover, successful engagement in adolescent developmental tasks is facilitated through social networks, including peers, friends, and broader community support.13,14 However, adolescents with SB often experience delays in assuming responsibility for their care and report poorer quality of peer relationships compared to their typically developing adolescents.15,16 These challenges adversely affect their overall quality of life (QoL) and complicate the healthcare transition process.17,18 Therefore, innovative interventions are needed to strengthen self-management abilities and enhance social support during this critical developmental period.
The metaverse is a shared immersive digital space accessible via the internet, created through the convergence of physical and virtual worlds. 19 Avatar-based interactions in the metaverse provide therapeutic benefits, such as psychological safety, experiential flexibility, and access to virtual activities that may be difficult in real-world settings.20,21 Avatar anonymity can reduce the stigma and self-consciousness associated with chronic illnesses or physical disabilities, encouraging participants to engage more easily with their peers.22,23 Adolescents’ familiarity with technology and their positive attitudes toward the metaverse are likely to facilitate its integration into healthcare settings.24,25 In South Korea, where digital device use is well-established, the adoption of the metaverse is expanding rapidly across various sectors.26,27 Although the use of the metaverse in healthcare has grown considerably,28–31 no targeted interventions have been developed specifically for adolescents with SB.
The Life Course Model
32
offers a comprehensive framework that considers multiple developmental factors, with a focus on long-term outcomes as children transition into adulthood. Rooted in a biosocial framework, the Life Course Model highlights the interaction between disability and environmental influences, highlighting the importance of a supportive context in facilitating optimal functioning and participation. It identifies three core domains: (1) self-management and health, (2) personal and social relationships, and (3) major life areas such as education and employment. The theoretical framework guiding this study is illustrated in Figure 1. Theoretical framework for this study 
The study aimed to: develop a metaverse-based program for adolescents with SB, grounded in the Life Course Model, to support healthcare transition and improve QoL by addressing self-management, informational, and psychosocial needs; and assess the program’s feasibility and acceptability through descriptive analysis and qualitative inquiry.
Method
Study design
The Medical Research Council (MRC) framework provides systematic guidance for the developing, implementing, and evaluating complex health and social care interventions through four distinct phases: development, feasibility, evaluation, and implementation.
33
This study presents the development and feasibility phases, which represent the first two stages in the MRC framework for developing and evaluating complex interventions,33,34 as applied to a novel metaverse-based intervention for adolescents with SB in South Korea (Figure 2). A single-arm pre-post design without a comparison group was employed, consistent with recommendations for early-phase feasibility studies that prioritize assessing acceptability, demand, and implementation processes over establishing causal effects.35,36 Reporting follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
37
The MRC framework for developing and evaluating complex interventions.
Stage 1: Development of the intervention
The metaverse-based program was systematically developed following the MRC framework for complex interventions, 33 which recommends a structured approach incorporating theory, evidence, and stakeholder engagement.
Theoretical foundation
Structure and components of the Metaverse-based Program.
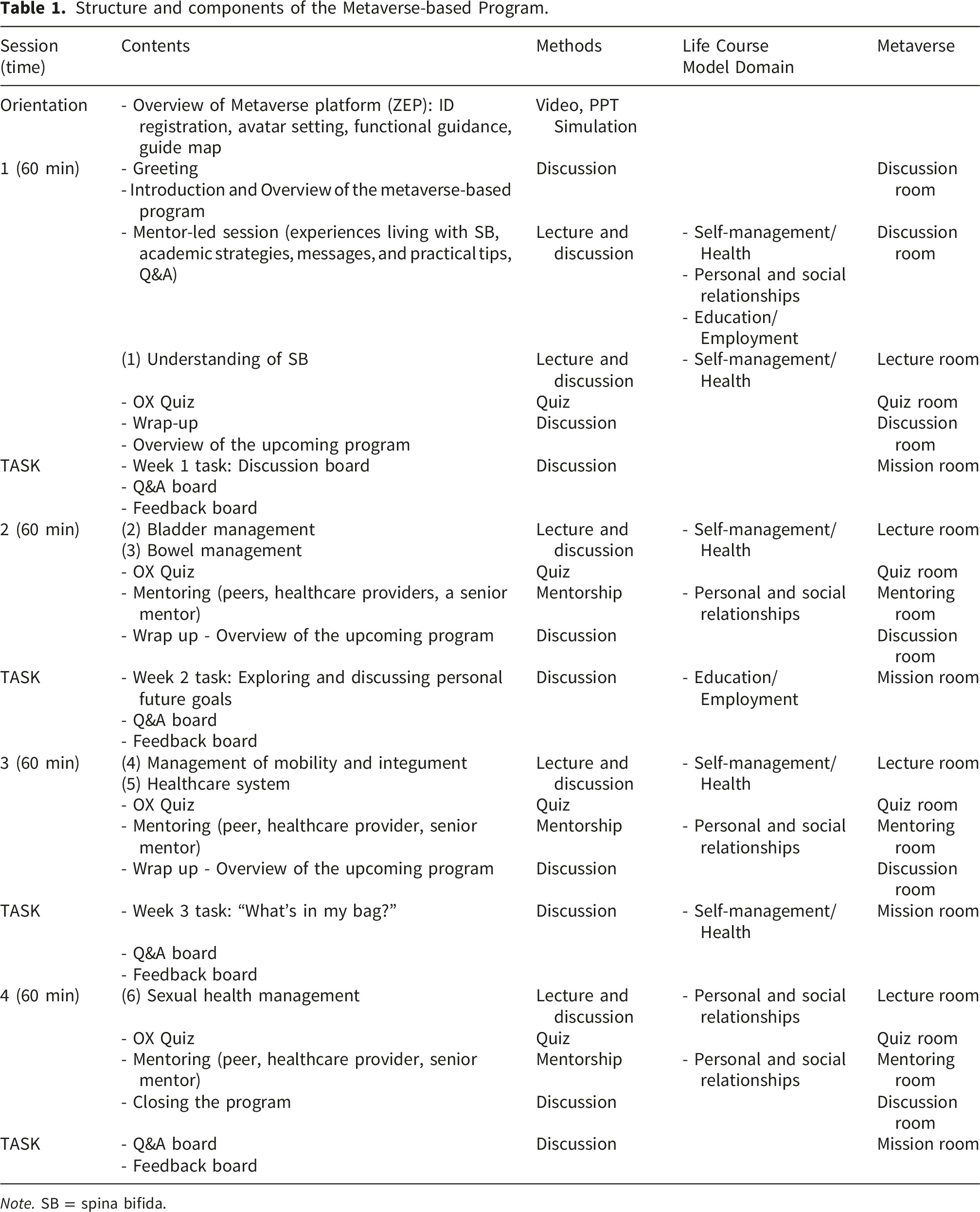
Note. SB = spina bifida.
Content development
Program content was informed by a review of existing effective interventions, including self-management and transition programs for adolescents with SB10,38,39 and the JUMP transition mentorship program, 40 as well as metaverse-based interventions for adolescents with chronic conditions.41,42 Based on this review, the following core components were identified: (1) structured health education addressing SB; (2) peer and professional mentorship to support psychosocial development; and (3) interactive activities to promote engagement and peer connection.
Six Korean-language animated educational videos (9–10 minutes each) were developed in collaboration with an animation director, covering SB self-management topics such as bladder and bowel management, mobility, healthcare systems, and sexual health (Appendix 1). These videos were delivered exclusively via the metaverse platform to program participants and were followed by topic-specific true-or-false quizzes (presented in an O/X format, where ‘O’ indicates ‘true’ and ‘X’ indicates ‘false’).
Mentorship component
Following the Life Course Model’s 32 emphasis on personal development and peer relationships, a mentorship program was incorporated to support participants’ educational interests and employment opportunities, delivered by undergraduate student mentors with SB through individual and group discussions that included time for questions and answers. Mentorship was provided by one undergraduate student mentor with SB and two pediatric nurse practitioners (PNPs). To ensure standardization of mentorship interactions, a structured mentorship guide was developed (Appendix 2) that specified: (1) the roles and responsibilities of each mentor type; (2) discussion topics aligned with the Life Course Model domains; (3) guidelines for responding to participant questions; and (4) strategies for providing emotional support while maintaining appropriate boundaries. Prior to program implementation, all mentors completed a two-hour training session covering the mentorship guide, platform navigation, and procedures for addressing participant concerns. The undergraduate mentor was recruited by the research team from the SB clinic based on their willingness to share lived experiences and ability to serve as a peer role model.
Program structure
The program consisted of four 60-minute sessions delivered over one month, with continuous access to the platform for self-paced activities. The four-week duration was determined based on several considerations: (1) alignment with similar feasibility studies of online psychosocial interventions for adolescents with chronic conditions, which typically range from four to eight weeks10,43; (2) practical constraints including participants’ academic schedules and potential burden associated with longer commitments; and (3) the primary aim of assessing feasibility and acceptability rather than sustained behavior change, consistent with early-phase intervention development. 35 Prior to participation, all participants viewed an instructional video and practiced navigating the metaverse using assigned credentials. Sessions 1–3 incorporated reflective and interactive activities, such as discussion board posts under themes like “Exploring Personal Future Goals” and “What’s in My Bag,” encouraging peer interaction through comments and likes. A dedicated discussion board for questions and feedback remained continuously accessible. The program contents are outlined in Table 1.
Metaverse platform design
The virtual environment was developed on the ZEP platform (https://zep.us/; Naver Z Corp, Seongnam-si, Gyeonggi-do, Republic of Korea), a leading metaverse platform widely used in South Korea. ZEP supports up to 50,000 concurrent users and provides accessibility across various devices with seamless video, audio, and text communication features. Regarding digital access, all participants were required to have an internet-enabled device (e.g., smartphone, tablet, or personal computer; PC) compatible with the ZEP platform. Given the high prevalence of digital device ownership among Korean adolescents,44,45 device access was not anticipated as a significant barrier for the target population. Prior to participation, all participants viewed an instructional video and practiced navigating the metaverse using assigned credentials to minimize technical difficulties.
To address privacy concerns associated with minors in commercial virtual environments, multiple safeguards were implemented: access was restricted to registered participants using unique credentials, all sessions were conducted in private invitation-only rooms with researcher moderation, and participants freely customized their avatars and pseudonyms to maintain anonymity. Data handling practices were disclosed to participants and guardians during the consent process. Although the ZEP platform is a commercial service, no personal health information was transmitted through the platform, and all research-related data were stored separately on secure institutional servers. The research team maintained moderation access to all virtual spaces throughout the program to monitor for potential risks, including unauthorized access and inappropriate interactions.
The virtual environment was collaboratively designed by professional metaverse designers and the SB research team and later customized by nursing faculty and PNPs. The virtual environment reflected the university campus with natural elements and included a lecture hall, discussion areas, and private mentoring rooms to promote participant comfort and familiarity (Figure 3). Implementation of the metaverse-based program in ZEP: (a) Metaverse entrance; (b) Discussion room; (c) OX quiz game; (d) Mentoring room.
Expert validation
An expert panel of seven members—comprising three PNPs and three child health nursing professors with experience in SB care—evaluated the program’s content, feasibility, clarity, and relevance, consistent with recommendations for a valid content evaluation. 46 Experts provided feedback on each item and suggested additional strategies for future program development.
Stage 2: Feasibility
Following MRC guidelines for complex interventions, an initial phase is recommended to assess the feasibility of identifying and addressing potential barriers to the acceptability and delivery of the intervention. 33 At this stage, the primary focus is on determining whether the intervention can be delivered as intended and whether it is acceptable to the target population, rather than on establishing effectiveness between the intervention and outcomes. 47 Accordingly, we conducted a single-arm feasibility study collecting feedback via interviews and self-reported questionnaires from adolescents with SB.
Participants
This study was conducted at the largest SB clinic in Seoul, South Korea, using a convenience sampling technique. Participants were adolescents with SB who met the following criteria: (1) currently enrolled in middle school (aged 13 to 15 years) with SB; (2) ability to use smartphones, tablets or PCs; (3) absence of cognitive impairments; and (4) voluntary assent along with informed consent from a parent or legal guardian. Exclusion criteria included: (1) inability to communicate and respond to the questionnaires; (2) presence of other illnesses or disabilities unrelated to SB.
Participants were recruited through two methods: (1) individuals from a patient dataset used in our previous study 48 who had consented to be contacted for follow-up were invited via text message; and (2) PNPs at the outpatient SB clinic introduced the study to eligible patients during regular visits. Interested individuals contacted the research line via a designated phone line to receive detailed information regarding the study’s aims and methods and to undergo eligibility screening. A total of eight adolescents with SB enrolled in and completed the intervention program. Parents or legal guardians provided written informed consent for participation. Adolescents participated independently in all intervention sessions, in a space separate from their parents, who did not view session content, access the platform, or complete any study questionnaires. Of the eight participants, one adolescent with motor impairment required minimal parental assistance with the initial platform login; the remaining seven logged in independently. No parental assistance was required during subsequent sessions.
Data collection
Adolescents with SB completed two rounds of self-report questionnaires delivered via an online survey platform. All participants completed the questionnaires independently, and full confidentiality was maintained throughout the data collection process. A pre-intervention assessment was conducted one week prior to the initiation of the metaverse-based program.
Sample size
As a feasibility study following the MRC framework for complex interventions, the primary aim was to assess acceptability, identify implementation challenges, and refine the intervention. 33 Previous usability research suggests that a sample of five users can identify approximately 80% of usability issues, with diminishing returns from additional testing. 49 Similar feasibility studies of online and metaverse-based psychosocial interventions have recruited eight to ten participants per group to balance adequate feedback with manageable group dynamics.41,50,51 The chosen sample size was based on limited research funding and keeping the participant group size manageable for effective delivery by the research team.
Measures
Permission to use each questionnaire was obtained from the original developers prior to data collection; the Korean versions of the QUALAS-T 52 and the SB Sexuality Knowledge and SB Worries Questionnaires 10 were translated and validated by members of the present research team. All standardized outcome measures are validated instruments, with original and Korean validation studies cited in the corresponding subsections. Several Korean versions have been previously employed in our research team’s prospective cohort study of children with SB. 48
Feasibility and acceptability
Consistent with recommendations for feasibility research,36,43 feasibility and acceptability were the primary outcomes.
Feasibility was operationalized using three indicators: (1) recruitment rate (proportion of eligible individuals enrolled); (2) retention rate (proportion completing the program); and (3) attendance rate (proportion of sessions attended). Based on prior feasibility studies, predefined benchmarks included ≥75% attendance, ≥80% retention, and <20% survey attrition. 53
Acceptability was assessed using a 16-item questionnaire adapted from a program satisfaction measure used in a prior study 10 and organized into three domains: content (9 items), evaluating perceived helpfulness of each educational video topic and three types of mentorship (PNP, undergraduate student mentor, and peer); delivery methods (3 items), assessing appropriateness of the metaverse platform, session duration, and overall program length; and overall program evaluation (4 items), including attitude toward participation in future healthcare transition programs, willingness to recommend to peers with SB, perceived helpfulness for setting individual transition goals, and overall satisfaction. All items were rated on a 10-point scale (1 = strongly dissatisfied; 10 = strongly satisfied). Cronbach’s alpha for this adapted instrument was 0.98 in this study. Two additional open-ended items assessed the most meaningful program aspects and suggestions for improvement.
Domain 1: Self-management and health
Self-management
Self-management was assessed using the Korean-translated version 54 of Hopson’s (2019) SB-specific self-management scale for adolescents with SB. This 11-item scale includes two domains: self-management behavior (seven items) and knowledge (four items), rated on a 5-point Likert scale. Higher scores indicate greater self-management levels. Cronbach’s alpha was 0.84 in the Korean validation study, 54 and 0.86 in this study.
Transition readiness
Transition readiness was assessed using the Korean version of the Revised Transition Readiness Assessment Questionnaire-SB (TRAQ-SB). 54 This 19-item tool includes five domains: Managing Medications (four items), Appointment Keeping (seven items), Tracking Health Issues (three items), Talking with Providers (two items), and Managing Daily Activities (three items), rated on a 5-point Likert scale. Higher scores indicate greater readiness. Cronbach’s alpha was 0.94 at its development, 55 0.90 in the Korean translation, and 0.83 in this study.
Self-efficacy
Self-efficacy was measured using a Korean version of the General Self-Efficacy Scale developed by Jerusalem and Schwarzer (1997), consisting of 10 items rated on a 4-point Likert scale. Higher scores indicate stronger self-efficacy. Cronbach’s alpha of the original scales was 0.75–0.90, 56 0.88 in the Korean version, 57 and 0.87 in this study.
Domain 2: Personal and social relationships
Perceived Social Support
Perceived social support was assessed using the Korean version of the Multidimensional Scale of Perceived Social Support, 58 a 12-item, 7-point Likert scale. The Korean version 59 includes healthcare providers in the “significant others” category. Higher scores reflect greater perceived support. Cronbach’s alpha 0.91 in a previous study, 59 and 0.92 in the current study.
Spina bifida sexuality knowledge
The SB Sexuality Knowledge Questionnaire was developed by Sawin (2002) and translated into Korean by Choi (2022). 10 The 13-item scale is rated on a 5-point Likert scale. Higher scores indicate greater SB-specific sexuality knowledge. Cronbach’s alpha ranged from 0.80–0.83 in the original development, 60 0.83 in the Korean version, 10 and 0.80 in the current study.
Spina bifida worries
The SB Worries Questionnaire was developed by Sawin (2002) 60 and translated into Korean by Choi (2022). 10 The 7-item scale includes two domains: sexuality (five items) and general SB worries about sexuality (two items), rated on a 6-point Likert scale. Higher scores indicate greater SB worries. Cronbach’s alpha of the original scales was 0.83, 60 0.92 in the Korean version, 10 and 0.93 in this study.
Domain 3: Employment and income support
Career preparation behavior
Career preparation behavior was assessed using the Career Preparation Behavior Scale, 61 a 10-item self-report questionnaire rated on a 5-point Likert scale. Higher scores indicate greater career preparation behavior. Cronbach’s alpha was 0.85 in the original study 61 and 0.86 in this study.
Domain 4: Major life area
Health related quality of life (HRQoL)
HRQoL was assessed using the Korean version of the KIDSCREEN-27, 62 a self-report questionnaire measuring HRQoL in children and adolescents aged 8–18 years. 63 This 27-item scale assesses five domains: physical well-being (five items), psychological well-being (seven items), autonomy and parent relations (seven items), social support and peers (four items), and school environment (four items), rated on a 5-point Likert scale. Higher scores indicate better HRQoL. The reliability of the Korean version, as measured by Cronbach’s alpha, ranged from 0.77 to 0.95, 62 and was 0.88 in this study.
SB-specific HRQoL
SB-specific HRQoL was measured using the Korean version of the QUALAS-T, 52 originally developed by Szymanski (2017). 64 This self-report questionnaire includes two domains: family/independence and bladder/bowel management, with five items per domain rated on a 5-point Likert scale. Higher scores indicate better HRQoL. Cronbach’s alpha for the original scales ranged from 0.76 to 0.78, 64 from 0.87 to 0.89 in the Korean version, 52 and 0.88 in the current study.
Qualitative interviews
Following program completion, semi-structured telephone interviews were conducted with all eight participants to explore their experiences and perceptions regarding the intervention’s feasibility and acceptability. Each interview lasted approximately 15 minutes and was conducted by one of three trained researchers using a standardized interview guide based on key feasibility domains (Appendix 3). Interviews were audio-recorded with participant assent and parental consent, and transcribed verbatim by a professional transcription service. Transcripts were reviewed against audio recordings for accuracy prior to analysis.
Data analysis
Quantitative analysis
Quantitative data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize participant characteristics, feasibility indicators, and acceptability ratings. Pre-post differences in outcome variables were examined using Wilcoxon signed-rank tests, appropriate for small sample sizes with non-normally distributed data. Statistical significance was set at p < 0.05.
Qualitative analysis
Interview transcripts were analyzed using reflexive thematic analysis, following the six-phase framework. 65 The first author led the initial phases, including familiarization through repeated reading of transcripts with reflexive journaling, systematic line-by-line inductive coding, and generation of candidate themes. Three authors then independently reviewed the codes and emergent themes to verify the interpretive framework. Themes were iteratively refined through review against the full dataset until final themes were defined and synthesized into a coherent narrative. Trustworthiness was enhanced through investigator triangulation, peer debriefing, and maintenance of an audit trail, guided by established criteria for qualitative rigor.66,67 Regular team meetings were held to challenge interpretive assumptions and discuss coding decisions. Discrepancies were resolved through consensus-based discussion; in cases of persistent disagreement, the senior author made the final determination based on alignment with the data and research objectives.
Ethical Consideration
This study was approved by the Institutional Review Board at the principal investigator’s institution (reference number 4-2024-1505). As all participants were minors (aged <18 years), written informed consent was obtained from parents or legal guardians, and written assent was obtained from each adolescent. Participants and their guardians were informed about confidentiality, secure data storage, and their right to withdraw at any time. Because the intervention was delivered via a commercial metaverse platform, the consent and assent process included an explanation of potential platform-related risks and the safeguards implemented. Participants were advised to avoid sharing personally identifying information, and a protocol for managing inappropriate interactions, including immediate session termination and guardian notification, was established prior to implementation. Study data were limited to what was necessary for research purposes, stored in de-identified form on secure, access-restricted systems, and managed in accordance with IRB requirements. As compensation, each participant received a mobile gift card valued at approximately 42 USD.
Results
Stage 1: Development of the intervention
Expert validation results
The content validity index (CVI) for all intervention sessions exceeded 0.8, indicating satisfactory content validity. 68 Preliminary reviews highlighted the program’s clarity and engagement, particularly through the use of diverse visual materials. Based on expert opinions, several expressions were modified for clarity and appropriateness.
Stage 2: Feasibility
Only adolescents with SB participated in the intervention, which was implemented via the metaverse platform by the two researchers who developed this program, supported by research assistants.
Participants characteristics
General and clinical characteristics of adolescents with spina bifida.

Note. AFO = ankle-foot orthosis; CIC = clean intermittent catheterization; FI = fecal incontinence; LMMC = lipomeningomyelocele; MMC = meningomyelocele; SB = spina bifida; SD = standard deviation; TCS = tethered cord syndrome; UI = urinary incontinence; VP = ventriculoperitoneal.
Feasibility and Acceptability
Satisfaction with the metaverse-based program.
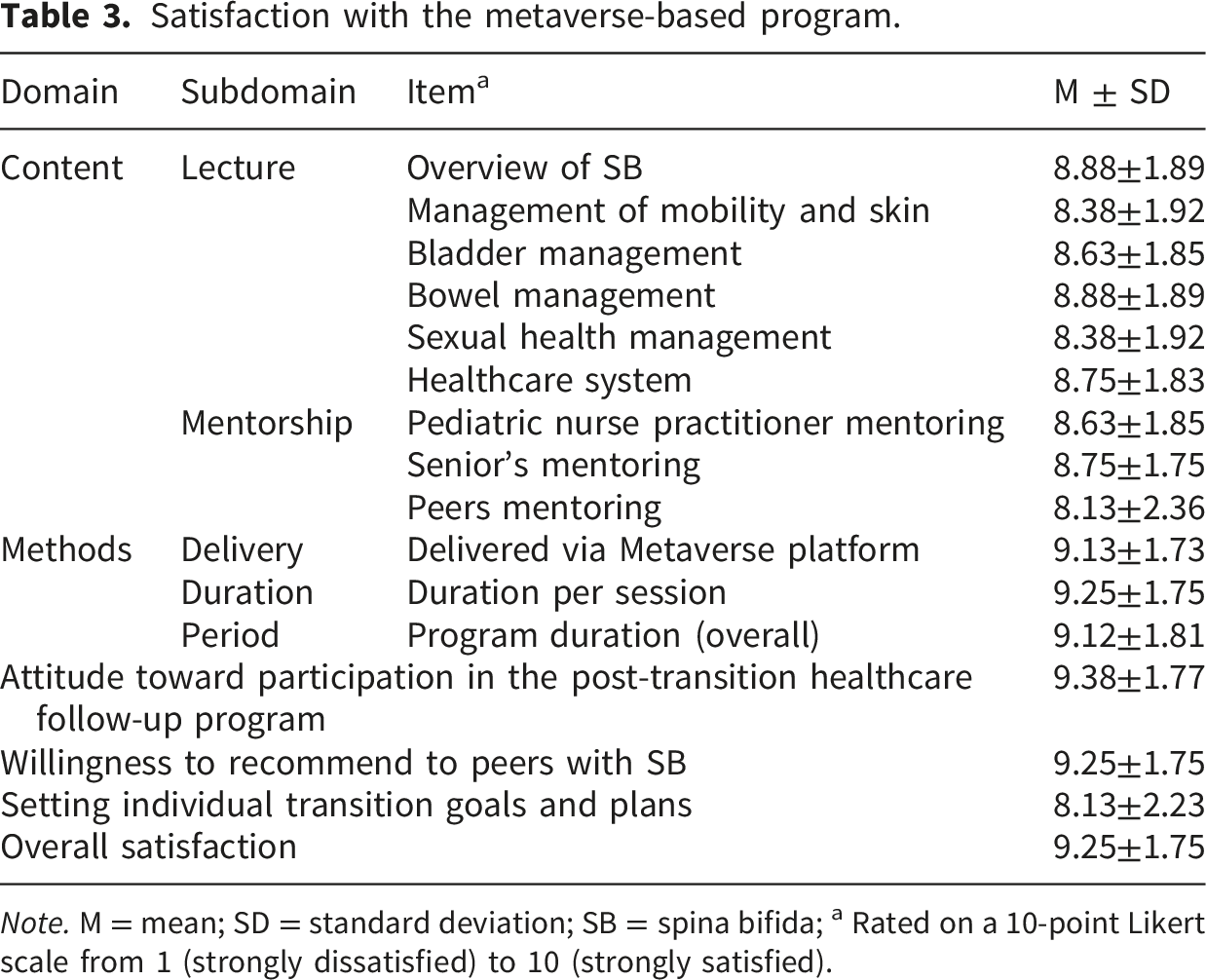
Note. M = mean; SD = standard deviation; SB = spina bifida; a Rated on a 10-point Likert scale from 1 (strongly dissatisfied) to 10 (strongly satisfied).
Difference in outcome variables before and after the metaverse-based program
Satisfaction with the metaverse-based program.
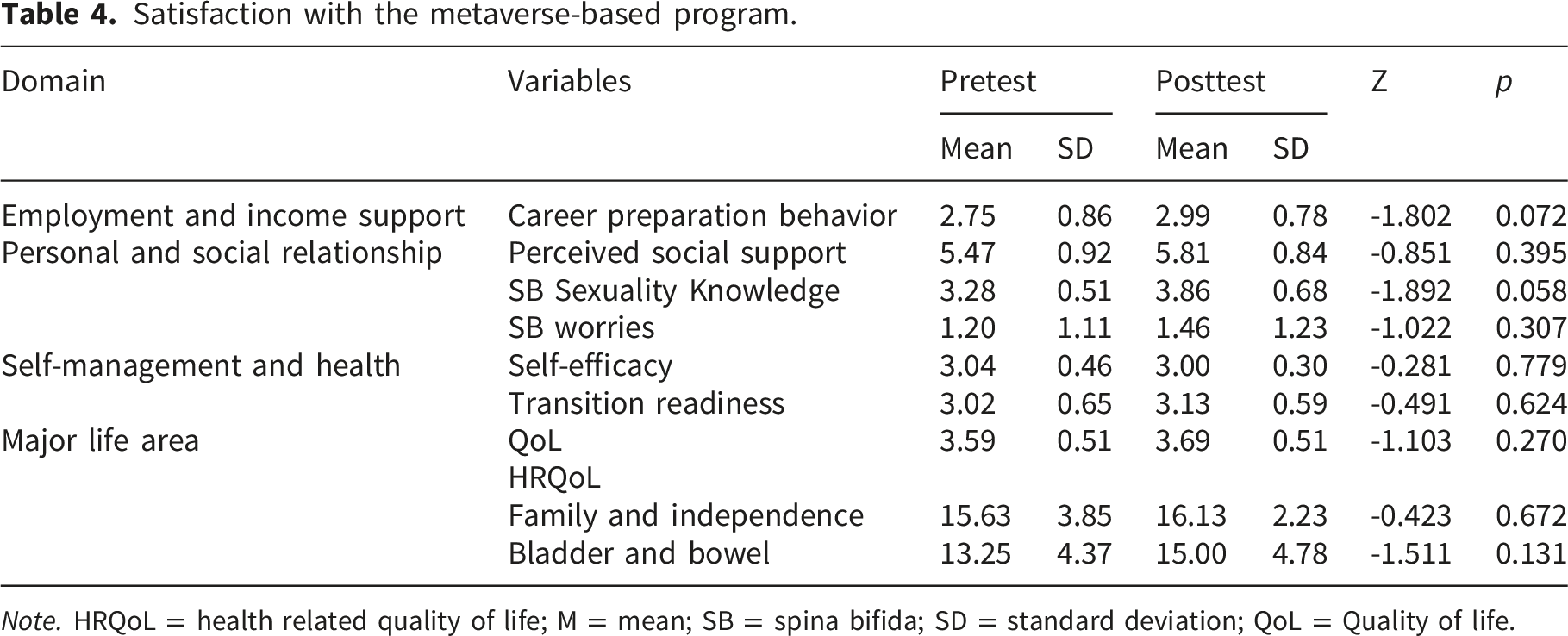
Note. HRQoL = health related quality of life; M = mean; SB = spina bifida; SD = standard deviation; QoL = Quality of life.
Qualitative findings
Qualitative findings: Themes and representative quotes.
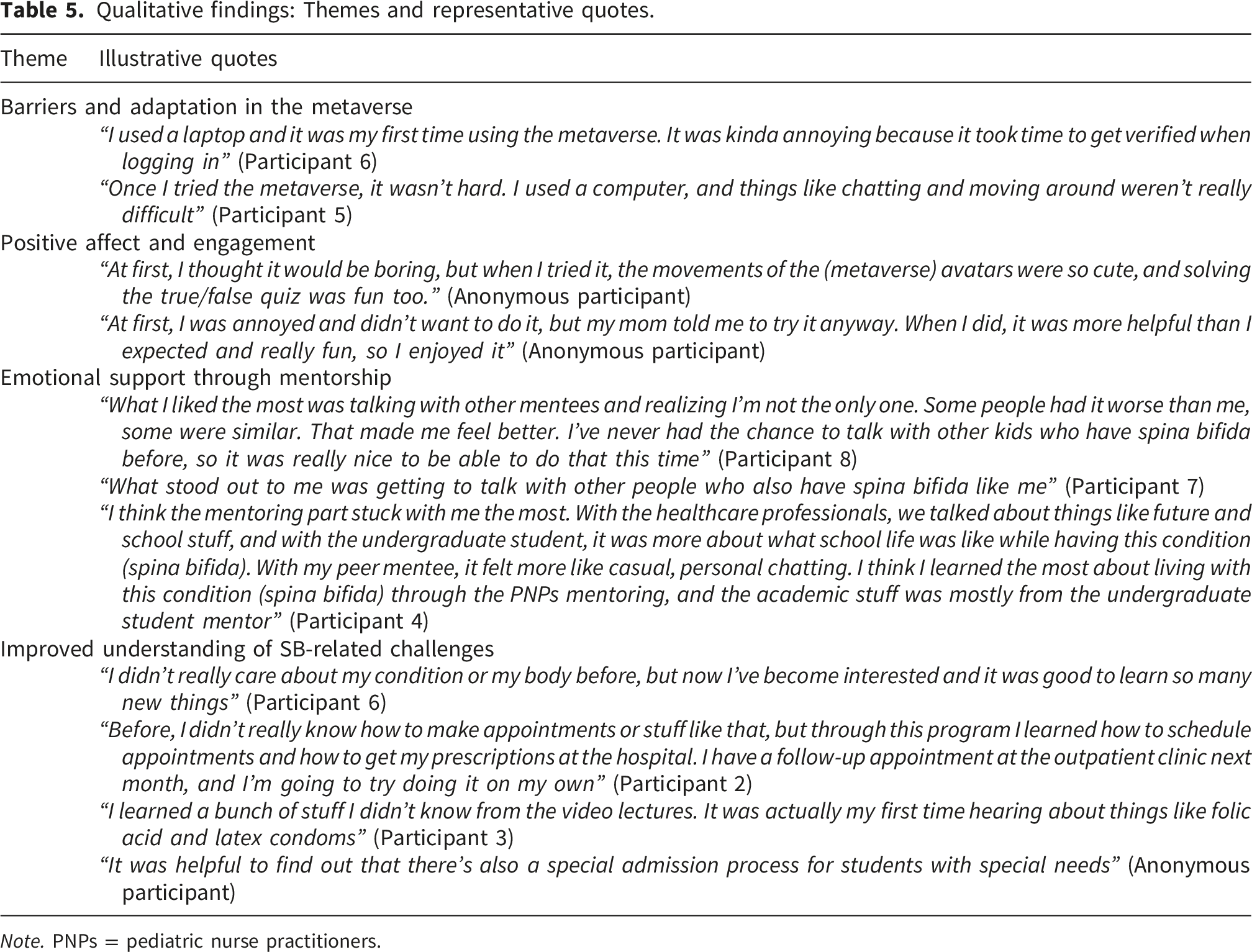
Note. PNPs = pediatric nurse practitioners.
Theme 1. Barriers and adaptation in the metaverse
Participants initially experienced minor technical difficulties, particularly among first-time metaverse users: “It was kinda annoying because it took time to get verified when logging in” (Participant 6). However, most adapted quickly after brief exposure to the platform: “Once I tried the metaverse, it wasn’t hard. Things like chatting and moving around weren’t really difficult” (Participant 5). These findings indicate that initial technical barriers were manageable and did not impede overall program engagement.
Theme 2. Positive affect and engagement
Despite initial hesitation, participants consistently described the program as enjoyable and engaging. One participant noted: “At first, I thought it would be boring, but when I tried it, the movements of the avatars were so cute, and solving the true/false quiz was fun too.” Another reflected: “At first, I was annoyed and didn’t want to do it, but my mom told me to try it anyway. When I did, it was more helpful than I expected and really fun.” These responses suggest that the interactive, avatar-based format contributed to sustained motivation and positive attitudes toward participation.
Theme 3. Emotional support through mentorship
Participants described the mentorship component as emotionally meaningful, particularly valuing connections with others who shared similar experiences. One participant stated: “What I liked the most was talking with other mentees and realizing I’m not the only one. Some people had it worse than me, some were similar. That made me feel better. I’ve never had the chance to talk with other kids who have spina bifida before” (Participant 8). Another noted: “What stood out to me was getting to talk with other people who also have spina bifida like me” (Participant 7). Participants also differentiated the unique contributions of each mentor type: “With the healthcare professionals, we talked about things like future and school stuff, and with the undergraduate student, it was more about what school life was like while having this condition. With my peer mentee, it felt more like casual, personal chatting” (Participant 4). These findings suggest that the multi-layered mentorship structure addressed diverse psychosocial needs and reduced feelings of isolation.
Theme 4. Improved understanding of SB-related challenges
Participants reported increased understanding of SB and greater awareness of self-management strategies. Several described a shift from passive awareness to active interest: “I didn’t really care about my condition or my body before, but now I’ve become interested and it was good to learn so many new things” (Participant 6). Participants also gained practical healthcare navigation skills: “Before, I didn’t really know how to make appointments or stuff like that, but through this program I learned how to schedule appointments and how to get my prescriptions at the hospital. I have a follow-up appointment at the outpatient clinic next month, and I’m going to try doing it on my own” (Participant 2). Additionally, participants reported acquiring new knowledge about sexual health: “I learned a bunch of stuff I didn’t know from the video lectures. It was actually my first time hearing about things like folic acid and latex condoms” (Participant 3). Information about educational pathways was also valued: “It was helpful to find out that there’s also a special admission process for students with special needs.” These findings suggest that the educational content addressed informational needs and fostered greater interest in future planning, particularly regarding education and employment pathways.
Discussion
In this study, we developed the metaverse-based intervention designed to address the informational and psychosocial needs of adolescents with SB while supporting their self-management and transition to adult healthcare. To the best of our knowledge, this is the first intervention of its kind utilizing a metaverse platform for adolescents with SB. The intervention consisted of structured health education and mentorship, reinforced by ongoing peer engagement, and delivered via an adapted metaverse platform to enhance engagement among adolescents with SB. The absence of dropouts throughout the program suggests strong preliminary evidence supporting the feasibility and acceptability of this approach. Consistent with previous research,10,38 adolescents with SB who participated in the intervention described a broad range of SB-related challenges and expressed a need for tailored support. Participant feedback indicated that the intervention was well received and met many of their identified needs.
While initial technical barriers, such as login delays were reported, participants quickly adapted and appreciated the platform’s interactive features, including chat functions and avatar-based engagement. This may be attributed to the fact that the participating mentees belong to Generation Z, 69 who have been exposed to digital technologies since early childhood and are likely to show high affinity for the metaverse. In the metaverse, users are immersed in a virtual environment through avatars, enabling real-time interaction without spatial or temporal constraints, while maintaining full anonymity.70,71 Given the tendency within Korean society to conceal health-related differences, adolescents with SB often refrain from disclosing their condition. 17 In this context, the anonymity afforded by the metaverse platform may provide a supportive environment for more open engagement in self-management and peer interaction.
Peer support, particularly from individuals with similar conditions, has been shown to reduce isolation and promote identity reconstruction in adolescents with chronic illnesses.72,73 In this study, sharing experiences within the metaverse environment helped participants develop greater self-understanding and resilience, consistent with the critical role of social interactions in adolescent development. 74 Supportive peer relationships have been associated with better treatment adherence and HRQoL.73,75 Adolescents with SB, especially females, often report challenges related to body image and self-esteem,76,77 which is consistent with the present findings. However, peer interaction, along with normative changes in the emphasis on physical appearance during the transition to adulthood, may mitigate these concerns over time. 78 These findings support the value of peer-supported, developmentally appropriate interventions to enhance QoL and promote positive identity development in adolescents with SB.
An understanding of condition-specific challenges, including bladder and bowel management, sexual health, and healthcare navigation, is essential for fostering autonomy and facilitating a successful healthcare transition in adolescents with SB.8,79,80 In this study, participants demonstrated substantial informational needs related to SB, particularly regarding self-management, sexuality, and future planning (Appendix 4), consistent with previous research.39,81 Although adolescence is typically a time of increasing curiosity about sexuality and romantic relationships, adolescents with SB often lack adequate opportunities to explore these topics.78,82 Given the increased risk of sexual health challenges in adulthood among individuals with SB, 81 it is essential to provide adolescents with accurate, SB-specific sexual and reproductive health education within a safe and supportive environment to ensure adequate preparation and healthy romantic development.
Limitations
This study has several limitations. First, the small sample size of eight participants, while appropriate for an initial feasibility assessment, limits generalizability and restricts the ability to draw statistically meaningful inferences. The unique nature of SB combined with the narrow age range (middle school students aged 13–15 years) contributed to recruitment challenges. Additionally, convenience sampling from a single tertiary care center in South Korea further limits the external validity of these findings. All participants in this study had reliable internet access and demonstrated adequate digital literacy, which may not reflect the circumstances of adolescents from lower socioeconomic backgrounds or regions with limited digital infrastructure. Second, the single-arm design without a comparison group precludes causal inferences regarding intervention effects. While this design is consistent with the exploratory nature of feasibility research, which primarily aims to assess acceptability and identify implementation challenges, future studies should incorporate randomized controlled designs to establish causal effects. Third, the four-week intervention period may have been insufficient to detect meaningful changes in outcomes such as self-management, transition readiness, and health-related quality of life, which typically require sustained skill-building over time. Fourth, the exclusive reliance on self-reported measures introduces potential sources of bias, including social desirability and recall bias. These concerns may be heightened in a novel and engaging environment such as the metaverse, potentially leading to inflated satisfaction ratings or overly favorable self-assessments. Additionally, the acceptability questionnaire was adapted from prior work and not formally validated, which may limit the precision of acceptability ratings. Finally, this pilot study did not account for potential confounding variables such as personal, familial, or environmental factors that could have influenced outcomes. In particular, although parental involvement in the intervention was minimal, the potential influence of broader parental engagement, such as post-session parent-adolescent discussions, on study outcomes was not formally assessed. Future iterations may consider incorporating parent-oriented components and examining parental engagement as a moderator of intervention effects.
Conclusions
This study presents the first metaverse-based intervention specifically designed to support healthcare transition and quality of life among adolescents with SB. The findings suggest that virtual reality platforms are a feasible and acceptable modality, with high program adherence and participant satisfaction. Qualitative results revealed enhanced understanding of SB-related challenges, increased emotional support, and sustained engagement despite initial technical difficulties. The successful use of avatar-based interactions to address sensitive topics such as sexuality and self-management suggests that metaverse platforms may have potential to complement traditional healthcare services. These preliminary findings indicate that virtual platforms may offer a developmentally appropriate method for delivering psychosocial support and health education, particularly by overcoming geographical constraints and reducing stigma-related barriers to peer connection.
Implications for practice
The findings from this pilot study suggest that metaverse-based interventions can be integrated into routine transition care for adolescents with SB. Healthcare providers should consider incorporating avatar-based virtual platforms as complementary tools to traditional face-to-face services, particularly for addressing sensitive topics such as sexuality and self-management that adolescents may find difficult to discuss in conventional clinical settings. The high engagement levels observed indicate that virtual environments may enhance participation in transition programs, especially for adolescents who face geographical or mobility barriers to accessing in-person peer support groups. Implementation requires minimal technological infrastructure, as most adolescents already have access to internet-enabled devices, making this approach both practical and scalable across different healthcare settings. However, adolescents with significant mobility limitations may require initial technical support during platform onboarding, and implementation planning should incorporate accessibility considerations to ensure equitable participation. Future research should extend the intervention duration and incorporate longitudinal follow-up assessments to evaluate the sustained effects of the program. Given that self-management skill acquisition and QoL improvements require ongoing reinforcement, subsequent trials might consider implementing booster sessions or maintenance phases following the initial intervention period. As digital health technologies continue to evolve, metaverse-based approaches may play an increasingly central role in adolescent chronic healthcare management, emphasizing the need for interprofessional collaboration and platform usability training in clinical practice.
Supplemental material
Supplemental material - Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study
Supplemental material for Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study by Hooyun Lee, Hyeseon Yun, Kyua Kim, Eunjeong Bae and Eun Kyoung Choi in DIGITAL HEALTH.
Supplemental material
Supplemental material - Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study
Supplemental material for Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study by Hooyun Lee, Hyeseon Yun, Kyua Kim, Eunjeong Bae and Eun Kyoung Choi in DIGITAL HEALTH.
Supplemental material
Supplemental material - Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study
Supplemental material for Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study by Hooyun Lee, Hyeseon Yun, Kyua Kim, Eunjeong Bae and Eun Kyoung Choi in DIGITAL HEALTH.
Supplemental material
Supplemental material - Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study
Supplemental material for Development and feasibility of a metaverse-based program for health care transition and quality of life in adolescents with spina bifida: A pilot study by Hooyun Lee, Hyeseon Yun, Kyua Kim, Eunjeong Bae and Eun Kyoung Choi in DIGITAL HEALTH.
Footnotes
Acknowledgments
The authors acknowledge the adolescents with SB and their families for their participation and for sharing their experiences in this study.
Ethical considerations
This study was approved by the Institutional Review Board at the principal investigator’s institution (reference number 4-2024-1505), and the study was conducted in accordance with the Declaration of Helsinki. As all participants were minors (aged <18 years), informed consent was obtained from parents or legal guardians, and assent was obtained from each adolescent. Participants and their guardians were informed about confidentiality, secure data storage, and their right to withdraw at any time. As compensation, each participant received a mobile gift card valued at approximately 42 USD. Written informed consent was obtained from all participants and their guardians
Author contributions
All authors made substantial contributions to the manuscript, in accordance with the National Academy of Sciences guidelines. Specifically, the authors had the following roles: H.L.: Conceptualization, Data curation, Methodology, Formal Analysis, Writing–Original Draft, Writing Review and Editing, Visualization, Project Administration. H.Y.: Data management and analysis, data interpretation. K.K.: Data management and analysis, data interpretation. E.B.: Data management and analysis. E.K.C.: Conceptualization, Methodology, Formal Analysis, Writing – Review and Editing, Supervision, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT [MSIT]) (No. 2022R1A2C1008573), and supported by the Brain Korea 21 FOUR Project, Yonsei University College of Nursing. The funders did not play any role in the data collection, interpretation, or reporting in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.