
Abstract
Objective
This study aimed to summarize the evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems, providing guidance for clinical practice.
Methods
Researchers systematically searched domestic and international databases based on the “5S” pyramid model. Search types included clinical decisions, guidelines, expert consensuses, evidence summaries, systematic reviews, meta-analysis and RCTs. The search scope covered the period from the database’s inception to August 2025(updated on January 2, 2026). For quality assessment, four researchers used the AGREE II assessment guidelines. Two researchers independently assessed expert consensuses, systematic reviews, and RCTs using the evaluation criteria of the JBI Centre for Evidence-Based Healthcare (2016).
Results
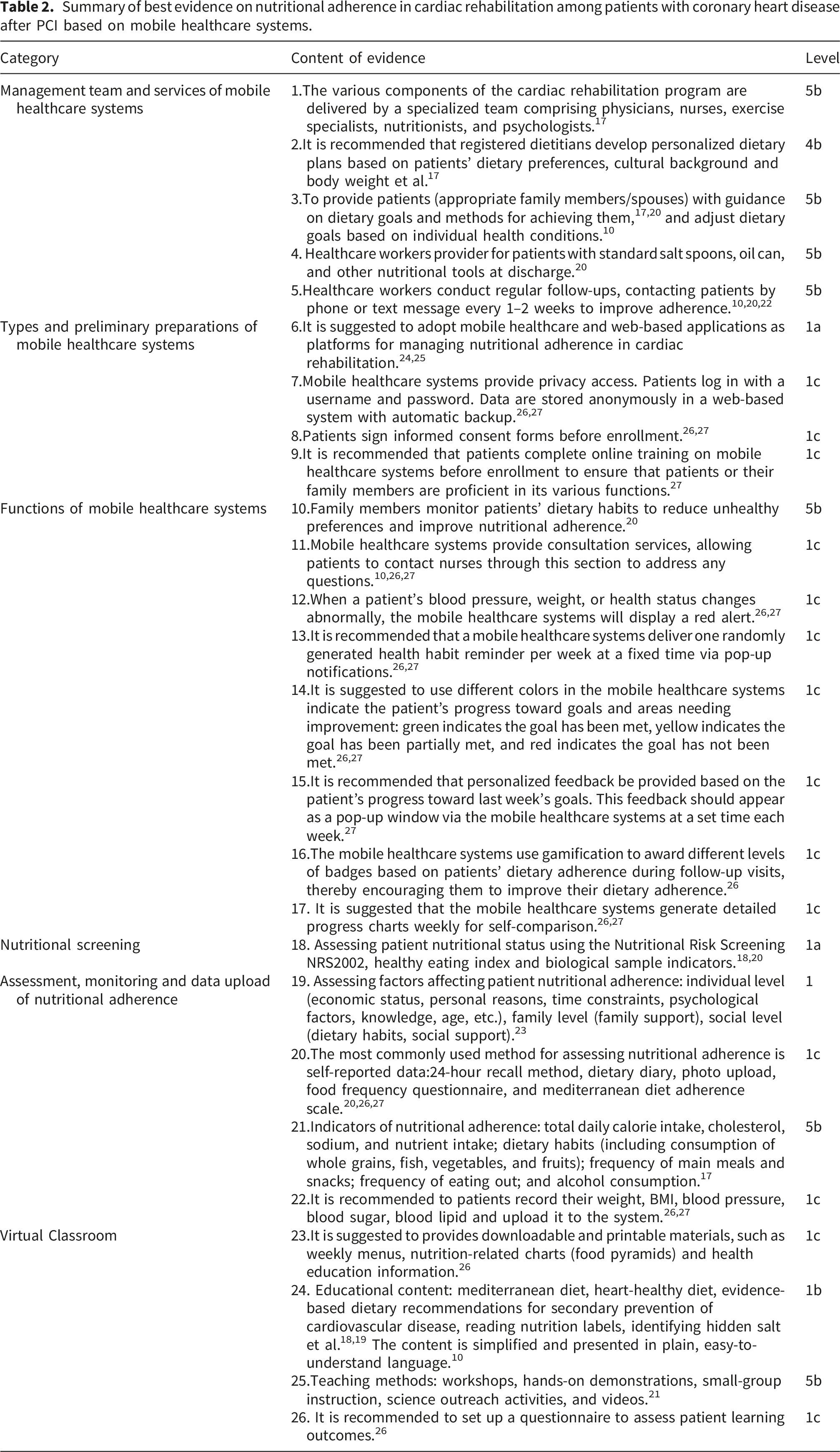
This evidence summary included 12 studies: one clinical decision, two guidelines, four expert consensuses, three systematic reviews, and two RCTs. A total of 26 best evidence items were extracted and categorized into six areas: management team and services of mobile healthcare systems, types and preliminary preparations of mobile healthcare systems, functions of mobile healthcare systems, nutritional screening, assessment, monitoring and data upload of nutritional adherence, and virtual classroom.
Conclusions
This study summarized the evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems. The findings provide clinical reference for healthcare workers to enhance nutritional adherence in cardiac rehabilitation using mobile healthcare systems.
Keywords
Introduction
Approximately 252 million people worldwide suffer from coronary heart disease, the most common type of cardiovascular disease. 1 According to the China Cardiovascular Health and Disease Report (2023), the number of patients with coronary heart disease in China has reached 11.39 million, with both incidence and mortality rates continuing to rise. 2 Percutaneous coronary intervention (PCI) is an effective treatment for coronary heart disease, improving myocardial perfusion and dilating narrowed arterial lumens. However, it cannot reverse or halt the pathological progression of coronary atherosclerosis. 3 Therefore, primary focus should be on controlling risk factors for cardiac rehabilitation after PCI.
Cardiac rehabilitation is based on a comprehensive medical assessment and provides comprehensive management services for patients with cardiovascular disease through five core components, encompassing physiological, psychological, and social aspects. 4 Among these, nutrition is a core component of cardiac rehabilitation. 5 Nutrition, as a modifiable cardiovascular risk factor, 6 can be improved by intervention, and its effectiveness largely depends on patients’ adherence. Good nutritional adherence reduces cardiovascular mortality. People with higher nutritional adherence exhibit a 14%–28% reduction in cardiovascular death rates. 7 Although the benefits of nutritional adherence have been widely demonstrated. However, in cardiac rehabilitation studies, the issue of nutritional adherence is often overlooked. Study showed that nutritional adherence of patients after PCI during stage I cardiac rehabilitation was less than 32%. 8 Poor nutritional adherence further affects blood pressure and lipid levels, leading to adverse outcomes. 9 Therefore, improving nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI is of great significance and urgent.
Traditional nutritional management is limited by the number of follow-up visits, and patients cannot receive timely feedback between two counseling sessions, affecting adherence and the sustainability of dietary behavior changes. 10 However, mobile healthcare systems change this situation. Mobile healthcare systems are regarded as an effective tool for promoting behavioral changes in patients with coronary heart disease. A previous randomized controlled trial found that SMS intervention based on mobile healthcare systems improved dietary behaviors in patients with coronary heart disease. 11 Mobile healthcare systems enable patients to actively monitor their health and take part in self-management while empowering healthcare workers to provide personalized, continuous care. 12
In past studies, exercise adherence was frequently tracked using digital technologies. However, there are few research investigating nutritional adherence in cardiac rehabilitation for patients with coronary artery disease after PCI using mobile healthcare systems. The existing evidence is somewhat scattered, and research focuses on different areas. Furthermore, changing dietary behaviors faces challenges, influenced by factors such as the complexity of dietary recording, as well as social and cultural aspects. These issues require systematic research to synthesize the evidence. This study aims to summarize evidence using an evidence-based method and make suggestion for healthcare workers to utilize mobile healthcare systems for nutritional adherence management.
Methods
This evidence summary protocol was registered with the Center for Evidence-Based Nursing at Fudan University (registration number:ES20259479).
Raising questions
This study employed the PIPOST model proposed by the JBI Evidence-Based Nursing Center at Fudan University to formulate evidence-based questions. Population (P): Patients with coronary heart disease after PCI; Intervention(I): Provide nursing interventions related to nutritional adherence in cardiac rehabilitation using mobile healthcare systems; Professional (P): healthcare workers; Outcome (O): nutritional adherence, completion rate, participation rate, etc. Setting (S): Home, community or outpatient clinic; Type of evidence (T): Clinical decisions, Guidelines, expert consensuses, evidence summaries, systematic reviews, meta-analysis, randomized controlled trials (RCTs).
Search strategy
According to the “5S” pyramid model, 13 the search was conducted from top to bottom. This study prioritizes high-level evidence from the top tier of the evidence pyramid, including clinical decision support systems, comprehensive evidence summaries, evidence-based guidelines, and systematic reviews. Where high-level evidence is insufficient or not fully applicable to the research question, primary studies are included to supplement the evidence. The search databases were as follows: BMJ Best Practice, Up To Date, JBI Evidence-Based Healthcare Database, Guidelines International Network (GIN), New Zealand Guideline Group (NZGG), National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), National Guidelines Clearinghouse (NGC), American Heart Association, Japan Heart Association, Cochrane Library, PubMed, Web of Science, Embase, CINAHL, Yimaitong, CKNI, Wanfang, VIP, Sinomed. Search term:(coronary heart disease OR acute myocardial infarction OR acute coronary syndrome OR percutaneous coronary intervention OR PCI) AND (cardiac rehabilitation OR diet OR nutrition OR food OR dietary adherence OR dietary management OR nutrition prescription OR dietary intervention) AND (guideline OR expert consensus OR clinical decision OR evidence summary OR systematic review OR meta-analysis OR randomized controlled trial OR RCT). This study adopted search strategy that combines medical subject headings and free-text terms, which is adjusted according to the search syntax of different databases. The search strategies for each database were presented in the supplementary material. The search time ranged from the database’s creation to August 2025. (updated on January 2, 2026).
Inclusion and exclusion criteria
Inclusion criteria: Patients aged ≥18 years with coronary heart disease after PCI; The study content focuses on measures to improve nutritional adherence in cardiac rehabilitation using mobile healthcare systems; The types of literature include clinical decisions, guidelines, expert consensuses, evidence summaries, systematic reviews, meta-analyses, and RCTs; Chinese or English literature. Exclusion criteria: Duplicate publications or references without full-text access; Literature that did not pass quality assessment; Meeting summaries or meeting reports; Expert consensus statements that have not been revised or updated.
Literature screening
Two trained researchers independently screened the literature. In the event of any disagreement, the matter will be discussed with a third researcher until a consensus is reached. This study used EndNote 21 to manage the literature. After removing duplicate references, the researchers conducted an initial screening of the article titles and abstracts, then read the full texts and included those that met the predefined inclusion and exclusion criteria.
Quality evaluation
Quality evaluation criteria varied according to the type of research and are listed as follows: Guideline quality was assessed independently by four researchers using the Appraisal of Guidelines for Research and Evaluation II (AGREE II), 14 which contains six domains, 23 items, and two overall evaluation items rated on a 7-point scale. If the percentage of standardization in all fields exceeds 60%, it is classified as grade A; If the standardized percentage in ≥3 domains falls between 30% and 60%, it is classified as grade B; If the standardized percentage in three or more domains is less than 30%, it is classified as grade C. Two researchers evaluated expert consensuses, systematic reviews, and RCTs using the JBI Centre for Evidence-Based Healthcare (2016) evaluation tool standards. 15 The quality of the included studies was independently assessed by researchers who had completed evidence-based nursing training. In cases of disagreement, a third researcher was consulted to reach consensus.
Evidence summary and grade
Evidence was independently extracted and summarized by two researchers, with a third verifying the content. Evidence summary adheres to the following principles: When evidence content is complementary, it should be combined. When evidence content is conflicting, prioritize the highest-quality, most recently published literature. Evidence grading using the JBI Evidence Pre-Grading System (2014). 16 This tool categorizes evidence levels into five tiers, with Level 1 the highest and Level 5 the lowest.
Results
Results of literature screening and basic characteristics of included studies
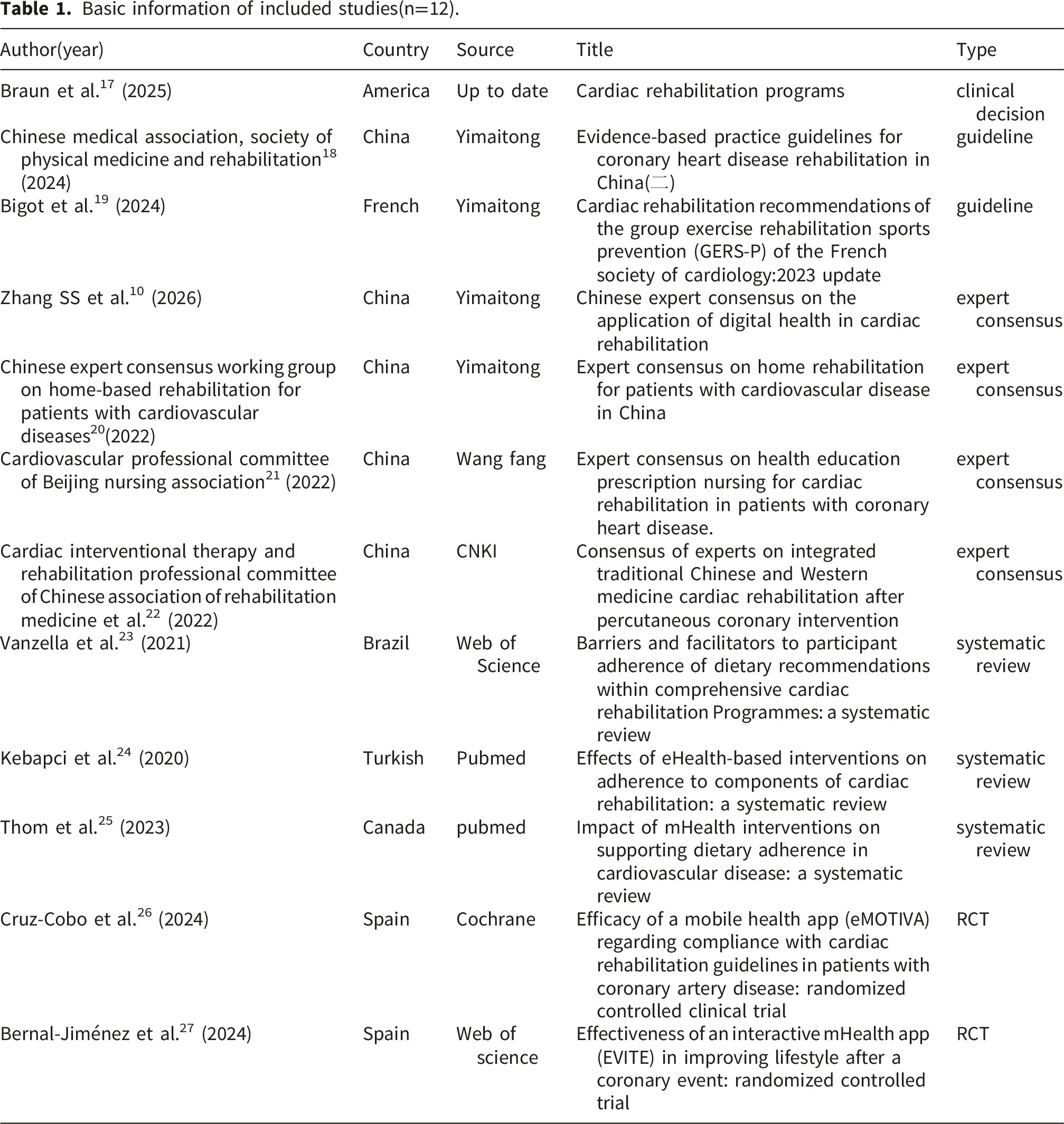
The initial search yielded a total of 4,990 studies, of which 1 was identified through snowball sampling. After removing 1,106 duplicate records, 3,884 studies remained. After reading the titles and abstracts, 78 studies remained. After full-text review,12 studies were eventually included: one clinical decision, two guidelines, four expert consensuses, three systematic reviews, and two RCTs. The screening process for this study is presented as a PRISMA flowchart in Figure 1. Table 1 shows the basic characteristics of the included research. PRISMA flowchart for literature screening. Basic information of included studies(n=12).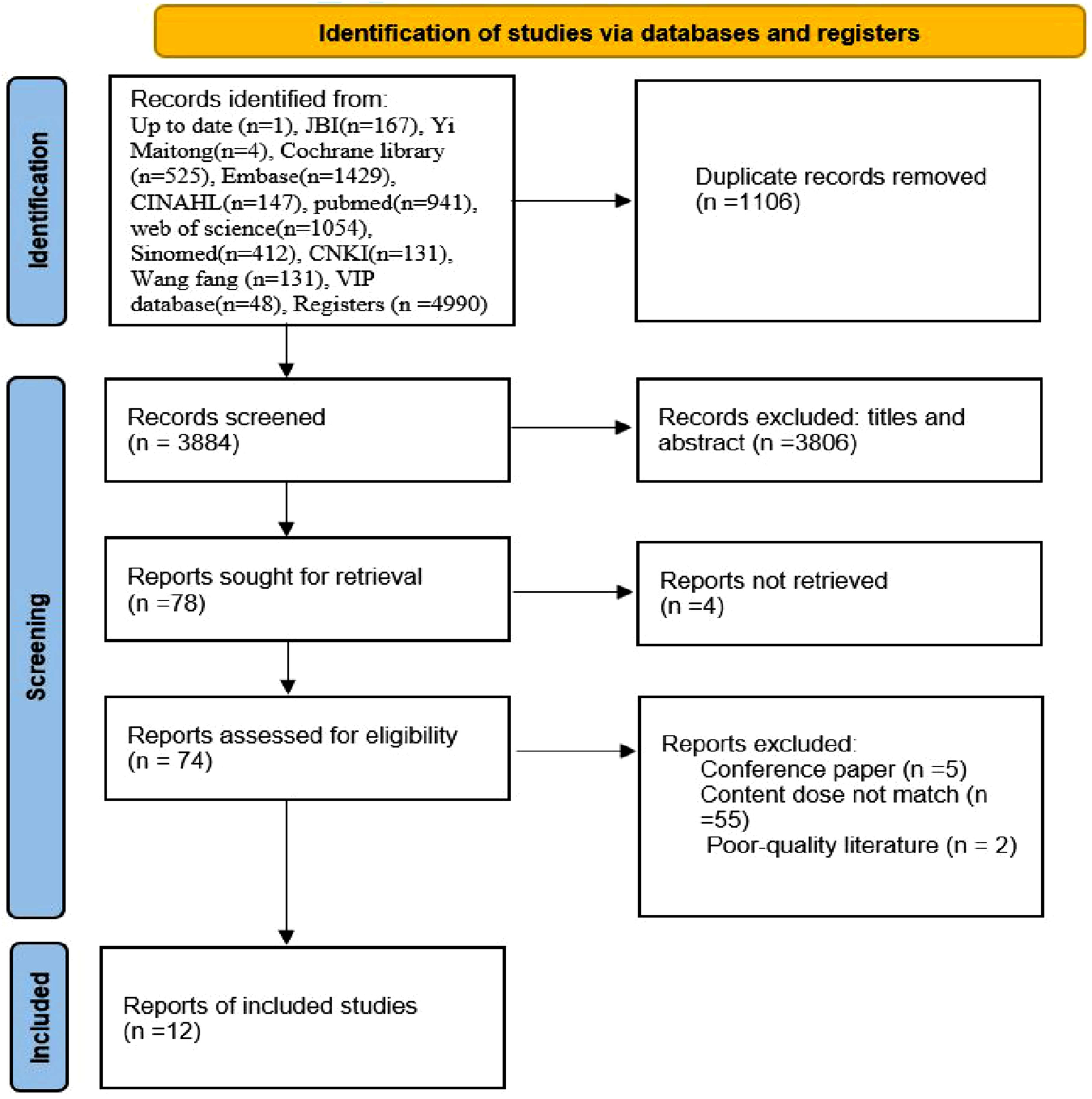
Quality evaluation results of literature
Quality evaluation result of clinical decision
This study included one clinical decision 17 from UpToDate, which was regarded as high quality and was directly included in the analysis.
Quality evaluation results of guidelines
This study included two guidelines.18,19 One guideline 18 has a recommendation level of A, with an intraclass correlation coefficient of 0.963. Another guideline 19 has a recommendation level of B, with an intraclass correlation coefficient of 0.960. Detailed results are provided in supplementary table 1.
Quality evaluation results of expert consensuses
This study included four expert consensuses.10,20–22 Four expert consensuses10,20–22 were assessed as “No” for item 6, and “Yes” for all other items. The overall quality of the studies was high, making it appropriate for inclusion. Detailed results are provided in supplementary table 2.
Quality assessment results of systematic reviews
This study included three systematic reviews.23–25 One systematic review 25 was rated “Yes” for all items. Two systematic reviews23,24 were assessed as “No” for item 9, and “Yes” for all other items. The included studies were of good quality and deed eligible for inclusion. The detailed results are shown in supplementary table 3.
Quality assessment results of RCTs
This study included two RCTs.26,27 Two RCTs26,27 were assessed as “unclear” for item 2, “No” for item 4, “unclear” for item 5 and “No” for item 8. The studies were of high overall quality and were considered appropriate for inclusion. Detailed results are provided in supplementary table 4.
Summary of evidence
Summary of best evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems.
Discussion
Management team and services of mobile healthcare systems
Coronary heart disease is frequently accompanied by conditions such as hypertension and hyperglycemia, leading to a clinical course that is complex and prone to change. Therefore, it requires collaboration across disciplines. 28 Mobile healthcare systems provide a platform for enhancing communication and information sharing among medical teams, thereby fostering more informed decisions and delivering high quality care services. 29 Nutrition plans formulated by dietitians are a crucial component in assessing the quality of cardiac rehabilitation. When formulating a nutrition plan, dietitians should take into account the patient’s dietary culture, preferences, and set specific, achievable goals to enhance the patient’s sense of self-efficacy, thereby improving nutritional adherence. 30 The achievement of more significant results is achieved by setting goals that include short-term and long-term aims. 31 It is worth noting that patients often find it difficult to control their salt intake at home. To improve the accuracy of salt intake assessments, experts recommend providing patients with standardized salt spoons at discharge. This recommendation is particularly pertinent given findings by Zhang et al. 32 that only 10.7% of Chinese residents use salt spoons, highlighting a significant opportunity for educational intervention and tool distribution by the mobile healthcare team. In addition, telephone follow-ups are an important way to reinforce patients’ target behaviors, thereby promptly identify and address potential barriers that arise during the implementation of interventions. However, this method involves higher labor costs. It is necessary to explore AI-based automated follow-up systems to optimize resource allocation.
Types and preliminary preparations of mobile healthcare systems
Mobile healthcare systems take various forms, including remote monitoring, telephone, and telemedicine. Mobile healthcare and web-based applications have been shown to improve nutritional adherence.24,25 Data security, privacy and confidentiality remain the primary concerns for patients using mobile healthcare systems. 33 According to statistics, 34 between 2009 and 2024, the United States experienced a cumulative total of 392 million healthcare data breaches. To reduce potential risks, it is recommended that mobile healthcare systems strengthen user security management and system-level data protection. Future research should validate the effectiveness of artificial intelligence technologies in identifying and dynamically managing potential data risks, with the aim of establishing a data security protection system. Additionally, we respect patients’ autonomy and protect them from harm. Therefore, patients sign an informed consent form before enrollment. To further enhance patients’ understanding of informed consent content, researchers use digital tools such as videos and interactive media. 35 For patients, mobile healthcare systems are new tool. Therefore, patients should be trained via pre-recorded online courses before using it to ensure they are proficient in its features.
Functions of mobile healthcare systems
The functions of mobile healthcare systems are monitoring, consultation, alerts, reminders, identification, feedback, rewards, and charts. Patients are more likely to choose unhealthy foods on weekdays or when dining out with friends. 23 Using the mobile healthcare systems, family members can remotely monitor patients’ dietary behaviors, provide behavioral guidance and emotional support to promote nutritional compliance. Family members or patients can also consult experts for personalized nutrition advice. Research shows that personalized dietary counseling improves metabolic outcomes and may lower risk of complication. 36 Indicators such as blood pressure, blood glucose, and body weight are closely associated with the occurrence of adverse cardiovascular events. 37 For these indicators, a tiered alert system is recommended to accurately identify high-risk patients by setting clear thresholds. 38 However, warning systems that rely on fixed thresholds have limitations in complex data analysis and struggle to capture dynamic changes. In comparison, machine learning algorithms have better predictive accuracy and are more effective at identifying high-risk patients.39,40 Reminders assist patients focus on nutritional issues, and make healthier food choices, thereby reducing risk. 41 However, frequent reminders might cause information overload and notification fatigue, reducing patient compliance. 42 Thus, it is recommended that mobile healthcare systems reminder be scheduled weekly, with automatic delivery within a fixed time window to improve read rates and avoid excessive disruption. Reminders also help reinforce patients’ behavioral memories and improve nutritional adherence, 43 thereby promoting the achievement of dietary goals. To make progress toward goals more easily identifiable, a striking color scheme is used, such as traffic light color coding. Moreover, the mobile healthcare systems are suggested to give kind and encouraging comments weekly based on the patients’ nutrition target achievement status. Such feedback enhances the emotional bond between the participants and target behavior, forming a positive feedback loop that fosters compliance. 44 However, current evidence on feedback frequency is limited. 45 Future study will explore the dose-response relationship between feedback frequency and nutritional adherence. Patients may feel annoyed if feedback is frequent. Gamification features make the process more entertaining, increasing adherence and motivating patients to improve their nutrition habits. 46 Research has found that coupons, points, and ranking systems are favored by patients. 46 However, the effectiveness of gamification shows differences in various age groups. 47 More importantly, overreliance on external rewards may undermine patients’ intrinsic motivation, affecting the long-term maintenance of behavioral change. 44 When developing gamification, it is recommended to adjust game elements based on age differences and emphasize the cultivation of intrinsic motivation to promote long-term adherence by strengthening autonomy-based support, providing continuous feedback, and setting phased goals. In addition, presenting information clearly and effectively is important to help patients understand it. Visualization enables complex data to be presented in a more intuitive way. Among other, charts are one of the most used visualizing methods with 24%. 48 Vibrant colors attract attention and enhance the readability of chart information. 48 The technology acceptance model suggests that perceived usefulness and perceived ease of use increase patients’ willingness to adopt mobile healthcare systems. Visual design reduces the difficulty of understanding information and enhances visual intuitiveness, thereby improving patients’ perceived usefulness and perceived ease of use. 49 For the design of mobile healthcare systems, it is important to consider the preferences of colors and styles of charts for patients from different age groups. 50
Nutritional screening, assessment, monitoring and data upload of nutritional adherence
Malnutrition is associated with adverse clinical outcomes, including higher morbidity and mortality, prolonged hospital stays, and an increased risk of complications. 51 A study reported that approximately two-thirds of elderly patients undergoing PCI exhibit varying degrees of malnutrition. 52 Early identification and intervention of patients’ nutritional status play a crucial role in improving prognosis. Therefore, it is suggested that patients undergo nutritional screening after PCI to assess their nutritional status. The European Society for Enteral Nutrition recommends the Nutritional Risk Screening Tool 2002 (NRS-2002) as the preferred screening tool due to its ease of use, and it has been endorsed by multiple expert consensus groups.20,53,54 Biological parameters such as serum albumin and urine analysis provide a more objective reflection of a patient’s nutritional status and are relatively reliable, serving as an important supplement to screening results. 55 In addition, nutritional adherence in cardiac rehabilitation patients is influenced by a variety of personal, family, and social factors, so we ought to take these factors into account when implementing interventions. To gain a more comprehensive understanding of a patient’s nutritional adherence, multiple indicators are usually required for assessment. Currently, the most commonly used assessment methods rely primarily on subjective reports, such as dietary diary, 24-hour recall, and questionnaire surveys. 56 These methods are low-cost but are affected by participants’ memory biases and subjective judgments, limiting data reliability. Among them, the dietary diary provides detailed information, but the recording process is time-consuming, resulting in low participant acceptability. 57 Standardized questionnaires are commonly used to evaluate nutritional adherence. However, existing scales are designed for the general population, and there is currently no scale specifically for assessing nutritional adherence in cardiac rehabilitation patients. With the development of machine learning and image recognition technologies, artificial intelligence plays a significant role in assessing nutritional intake and adherence. 58 Participants use their phone cameras to take photos. Food features are extracted by AI technology, which then utilizes web databases to identify food types, portion sizes, and calorie counts, making dietary records more convenient and efficient. 59 But the accuracy of AI recognition of food still needs further study.
Virtual classroom
Research indicates that patients recovery to unhealthy eating habits six months after completing a cardiac rehabilitation program. 36 Given this, it is recommended that mobile healthcare establish a virtual classroom and provide downloadable educational materials to enable patients to learn about nutrition at any time. Kumar et al. confirmed that virtual education enhances adherence to the Mediterranean diet. 60 Moreover, current health education lacks theoretical guidance to explain changes in nutritional adherence behavior. The Health Belief Model is a theoretical framework for promoting behavioral change in health. It systematically explains the relevant behavioral mechanisms, with its core components being perceived susceptibility, perceived severity, perceived benefits, perceived barriers, behavioral cues, and self-efficacy. 61 Therefore, virtual classroom design is recommended to combine the Health Belief Model. Additionally, nurses are the primary providers of nutrition education. 62 Educational content is evidence-based, ensuring scientific rigor and standardization of information. But depending simply on static educational resources may not be sufficient to meet patients’ diverse needs. We employ more dynamic and interactive digital education strategies, such as using short animated videos to improve understanding for people with low health literacy, incorporating quizzes into mobile healthcare to reinforce knowledge retention, and implementing AI-powered chatbots to provide personalized nutrition counseling around the clock.
Limitations
This study has the following limitations: First, because most of the evidence comes from English-language literature, there are differences between China’s dietary patterns and those of Western countries, as well as differences in cultural backgrounds.
The Chinese population generally has a high sodium intake. 63 These differences in dietary patterns may reduce the applicability of the Mediterranean diet in our country.
Furthermore, despite the high penetration rate of smartphones. Yet, the prevalence of coronary heart disease is relatively high among the elderly. The group lacks digital health literacy and may have reservations about recommendations regarding mobile healthcare systems, which affect adherence to the intervention. 64 Therefore, during the process of clinical translation, medical professionals are advised to adapt the protocol to local conditions by taking into account the characteristics of the Chinese diet, the patients’ specific circumstances, and expert judgment in order to enhance its feasibility and applicability. Secondly, the limited number of studies and RCTs may restrict the generalizability of the conclusions. Furthermore, due to significant heterogeneity among the studies (interventions and outcome measures), this study did not conduct a meta-analysis. Further large-scale randomized controlled trials and meta-analysis are needed in future research. Thirdly, although this study has taken steps to control for methodological bias, there remains a risk of publication bias.
Conclusions
This study summarized the evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems. The evidence summary provides recommendations for clinical practice guidance for healthcare workers. However, the feasibility and effectiveness of these strategies still need to be validated in clinical practice.
Supplemental material
Supplemental material - Summary of evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems
Supplemental material for Summary of evidence on nutritional adherence in cardiac rehabilitation among patients with coronary heart disease after PCI based on mobile healthcare systems by Yaqin Hu, Dongyan Lu, Jinghua Yi, Mengying Wang, Jingya Liang, and Jing Li in Digital Health.
Footnotes
Acknowledgements
We extend our gratitude to all experts who took the time to guide this study.
Author contributions
HYQ: Drafting, literature search, assessing the quality of the literature, extracting and grading evidence, reviewing.
LDY: Literature search, assessing the quality of the literature, extracting and grading evidence.
YJH: Assessing the quality of the literature, extracting and grading evidence.
WMY: Assessing the quality of the literature.
LJY: Assessing the quality of the literature.
LJ: Evidence extraction and grading, methodological guidance, review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Lishui Municipal Science and Technology Bureau Public Welfare Project (2024GYX54).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Guarantor LJ.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.