
Abstract
Background
Generative artificial intelligence is increasingly discussed as a tool to support psychiatric practice, particularly by improving clinical workflows. Despite growing interest, little is known about how psychiatrists use genAI and how they assess its usefulness, especially within the German healthcare system.
Objective
This study examines the experiences and attitudes of psychiatrists in a Germany-wide convenience sample, with initial recruitment focused on Berlin and Brandenburg.
Methods
An online mixed methods survey was conducted between September 19, 2024 and March 14, 2025. Psychiatrists working in public psychiatric hospitals, outpatient practices, and members of the German Association for Psychiatry, Psychotherapy, Psychosomatics and Neurology were invited. Of 11,754 contacted psychiatrists, 126 completed the survey, resulting in a response rate of 1.07 percent. The survey assessed sociodemographic characteristics, prior genAI experience, perceived effects on clinical work, and use cases such as documentation, diagnostics, and communication. Quantitative data were analyzed descriptively and qualitative responses using summarizing content analysis.
Results
Slightly more than half of respondents, 52.0 percent, reported using genAI chatbots, most commonly ChatGPT. GenAI was primarily used for administrative tasks, especially writing medical letters and accessing medication information. Many participants reported potential benefits in reducing bureaucratic workload and improving documentation efficiency. At the same time, skepticism regarding clinical usefulness was common. Respondents highlighted clear limitations in diagnostic and therapeutic decision making and emphasized the need for targeted training. Language support was identified as a key advantage, particularly for non native German speakers. The limited sample size restricts generalizability.
Conclusions
Psychiatrists expressed cautious optimism toward genAI, mainly for administrative support, while raising concerns about diagnostic use and insufficient training. These findings underline the need for evidence based integration of genAI in psychiatry, particularly in light of the EU AI Act.
Keywords
1. Introduction
Generative artificial intelligence (genAI) - defined as large language model (LLM) - based systems such as OpenAI’s GPT-4/5, Google Gemini, and Microsoft Copilot - are rapidly reshaping how clinicians across specialties think about day-to-day practice. Emerging studies show that these tools can summarise complex information, support clinical reasoning, translate or adjust communication for different audiences, generate drafts of correspondence or educational material, and interact conversationally with both clinicians and patients.1–4 Such broad capability has positioned genAI as a potentially transformative aid in mental healthcare, where clinical work is deeply text-based, communication-intensive, and characterised by diagnostic uncertainty and high emotional stakes. 5
Early research across medicine suggests that genAI may enhance the completeness of clinical histories, support hypothesis generation for differential diagnosis, assist with empathic phrasing, and streamline workflow in areas such as administrative correspondence and, importantly, clinical note-drafting.1–7 Although these tools remain imperfect - and often error-prone - there is growing evidence that clinicians are experimenting with them across a wide range of tasks, from background research to patient education and decision support. 1
Mental healthcare appears to be an especially early domain of adoption. The conversational nature of LLMs aligns closely with the communicative core of psychiatric work, and uptake by patients has grown at an unprecedented rate. In October 2025, OpenAI reported that more than 1.2 million people per week were using its tools to disclose suicidality - an indicator of both public demand and the shifting digital landscape in which psychiatrists now practise. 6 Against this backdrop, understanding clinicians’ own experiences and attitudes is increasingly urgent.
Yet despite intensifying interest, empirical research on mental health professionals’ use of genAI remains sparse. Existing studies involving general practitioners, psychologists, and other healthcare providers highlight both enthusiasm for potential benefits and concern regarding accuracy, bias, liability, and privacy risks.7–10 However, psychiatrists - who frequently manage complex histories, high-risk presentations, and sensitive patient data - are markedly under-studied. Blease et al. (2024) published research focused specifically on psychiatrists’ attitudes toward genAI. 8 That work provided valuable early insights but did not fully explore the breadth of clinical tasks for which psychiatrists may be adopting these tools, nor how their perspectives compare with those of other mental health or medical professionals.
GenAI systems can produce fluent yet inaccurate or misleading content, and they can encode or amplify gender, racial, disability, and other biases already documented in psychiatric care.8–10 Privacy concerns are especially salient in mental healthcare, where entering identifiable or highly sensitive data into non-secure platforms risks breaches of confidentiality.11,12 Understanding how psychiatrists are engaging with genAI - across documentation, diagnostic reasoning, patient interaction, communication, and administrative work - is therefore essential for developing safe, ethical, and evidence-based guidance for practice.
Regulatory oversight remains in flux. In Europe, the Artificial Intelligence Act entered into force in 2024, with a staged roll-out extending until 2027.11,12 The Act introduces a risk-based framework that classifies AI systems used in healthcare as “high-risk,” imposing stringent requirements for transparency, data governance, and human oversight. However, it remains unclear how these regulations will be operationalized in psychiatric practice or how they will shape day-to-day clinical workflows.
Complementary international work is also advancing rapidly, with proposals for structured implementation pathways, including education strategies and digital navigator support,13,14 as well as technical infrastructures for evaluating genAI tools in clinical mental health contexts. 14 For example, in Germany, early applied research has begun to examine real-world use cases, including studies on genAI-assisted clinical documentation and ambient AI scribes in psychiatric and psychotherapeutic settings.10,15 These emerging studies highlight both usability potential and persistent risks related to accuracy and privacy.
Despite these policy developments, empirical evidence on psychiatrists’ engagement with genAI remains scarce and mostly focus on English-speaking countries.8,16 Only one recent APA-affiliated survey of U.S. psychiatrists found that while awareness was high, clinical use was limited and accompanied by concerns about accuracy, ethics and patient impact. 8 However, little is known about perspectives in other healthcare systems, where regulatory environments, technological adoption rates, and cultural attitudes toward digital innovation may differ. 17
To our knowledge, there are currently no published mixed-methods surveys examining psychiatrists’ engagement with genAI in EU countries. Germany, we argue, presents a highly relevant case, in the EU context, and one ripe for investigation. While efforts to digitalize healthcare are ongoing due to the Digital Healthcare Act, 18 adoption of genAI in psychiatry has been cautious, 19 and the profession operates within strict data protection laws (e.g., GDPR) and a mixed public–private healthcare model. Understanding German psychiatrists’ experiences and attitudes about genAI can inform both national policy and broader international discussions about responsible genAI integration in mental healthcare. Therefore this exploratory mixed-methods study aimed to assess psychiatrists’ experiences with and attitudes toward genAI-based chatbots in psychiatric practice in Germany.
2. Methods
2.1. Subjects
The target population of this study were practicing psychiatrists in Germany. Initial recruitment focused on institutions located in Berlin and Brandenburg to capture both urban and rural care settings. In a second step, recruitment was expanded nationwide via the DGPPN newsletter, resulting in a broader, Germany-wide convenience sample.
Participants in this online survey were recruited using a stepwise sampling approach. In the first step, we contacted public psychiatric hospitals (n = 8), psychiatric departments within general hospitals (n = 30), and outpatient psychiatric practices (n = 57) located in the federal states of Berlin and Brandenburg between September 19 and 25, 2024. These regions were selected to represent both urban (Berlin) and rural (Brandenburg) areas of Germany. Due to the anonymous and open distribution strategy, responses could not be linked to a specific recruitment phase at the individual level.
Institutions were contacted via email and asked to disseminate the survey among their employed psychiatrists. Through this outreach, we aimed to reach approximately 840 psychiatrists. The study used an open convenience sampling strategy based on voluntary participation.
The recruitment list included a range of institutional settings, including large academic centers (e.g., university-affiliated hospitals such as Charité Berlin) as well as non-university hospitals and outpatient practices. However, affiliation with academic institutions was not systematically recorded at the participant level.
In the second step, we collaborated with the German Association for Psychiatry, Psychotherapy, Psychosomatics and Neurology (DGPPN), the largest professional organization for psychiatry in Germany, with 11,754 members as of May 27, 2024. The DGPPN included a link to the survey in its monthly newsletter, distributed on December 18, 2024 and again on March 14,2025.
All invited participants were informed that their responses would remain anonymous and that no identifying information would be shared with the research team. Informed consent was obtained from all participants prior to their participation. The Ethics Committee of the Brandenburg Medical School reviewed the study and issued a waiver of ethical approval (protocol no. 228072024-ANF), as no personally identifiable or sensitive data were collected. Based on a pretest, survey completion took approximately four to five minutes. No compensation was provided for participation.
Inclusion criteria were: (1) being a licensed physician working in psychiatry or a related field and (2) current involvement in clinical practice. Exclusion criteria were incomplete survey responses and participants not working in a psychiatric context.
2.2. Procedures
The online survey was based on an adapted version of a questionnaire originally developed by one of the authors. 8 It was translated into German and adapted to the specific conditions of the German psychiatric care system using a forward-translation approach. To ensure content validity and contextual relevance, three board-certified psychiatrists independently reviewed the translated instrument and provided structured feedback, which was incorporated into a revised version. The core questions from the original instrument remained unchanged to preserve comparability with prior research.
As this was an exploratory study, no formal psychometric validation (e.g., factor analysis or reliability testing) was conducted. However, the questionnaire primarily consisted of descriptive and experience-based items rather than latent construct measures, reducing the need for formal scale validation.
The questionnaire consisted of two parts (see Appendix 1) and 16 Items in total. In the first section, participants provided sociodemographic information. The second section included seven substantive questions. First, participants were asked whether they had prior clinical experience with genAI, such as ChatGPT, Google Gemini, Microsoft Bing AI, or other systems, using a multiple-choice format.
Participants were also asked which specific tasks these AI tools had been used for. Then, participants rated the extent to which AI-powered chatbots might influence six core areas of psychiatric clinical work using a Likert scale. These areas included gathering patient information, diagnostic and prognostic accuracy, treatment planning, conveying empathy, and clinical documentation. Another question used a Likert scale to assess the degree of agreement about the potential impact of genAI use on caring for individuals with mental illness. Five subdomains were addressed: risk of patient harm, potential inequalities in care, genAI as substitute for medical treatment, training needs for clinicians, and potential efficiency gains in the healthcare system. All Likert scales offered four response options: “Strongly disagree,” “Somewhat disagree,” “Somewhat agree,” and “Strongly agree.” Each item also included the options “I don’t know” and “No response.”. An additional closed-ended question asked participants to estimate whether the clinical use of genAI might influence the likelihood of legal action against clinicians. Finally, two open-ended questions invited participants to share additional comments regarding the use of genAI in psychiatric practice and chatbots in general.
We used a four-point Likert scale without a neutral midpoint to encourage respondents to indicate a directional judgment (agreement vs. disagreement) and to reduce central tendency bias.
2.3. Analysis
We used descriptive statistics to analyze the closed-ended questions regarding physicians’ experiences with and attitudes toward genAI in psychiatry. These analyses were conducted using the survey software R (version 4.3.2; R Core Team, 2023) and Microsoft Excel (Microsoft 365, version 2408). Given the exploratory objective and limited sample size, only descriptive statistics were calculated. No inferential statistical models were used, as the study was not powered to detect subgroup differences or predictors. For Likert-scale items, responses of “I don’t know” were treated as a distinct descriptive category and are reported separately where relevant, as they reflect meaningful uncertainty among respondents. “No response” was treated as missing data and excluded from percentage calculations. For transparency, figures and tables report the full distribution of responses, including “I don’t know,” while percentage summaries in the main text refer to valid substantive responses unless otherwise specified.
Given the exploratory objective and limited sample size, analyses were restricted to descriptive statistics. No inferential statistical models were applied, and the study was not powered to detect subgroup differences. Where informative, we report proportions alongside absolute counts to improve interpretability. No formal subgroup comparisons were conducted, and any observed differences should be interpreted descriptively only.
All free-text responses (47 comments; 2,152 words) were analyzed using summarizing content analysis20,21. Due to the limited nature of the dataset – often consisting of brief phrases or sentence fragments – a full thematic analysis was deemed inappropriate (Patton 2023). 22 Two researchers (JS, OG) independently coded all comments; however, no formal blinding between coders was implemented. They developed an inductive codebook (see Appendix 2) through interactive comparison and consensus meeting. Because response length varied, our coding combined two procedures: we assigned a single primary code to each response; for longer responses that contained clearly separable thematic units, the response was segmented and each segment was coded according to a shared response code (for example, comment #150, was split into two code segments). Theme prevalence counts and all quantitative summaries therefore refer to coded segments rather than raw comments counts. Inter-rater agreement for the initial double-coding was substantial (percent agreement = 87%; Cohen´s k = 0.78); remaining disagreements were resolved through discussion. The final codebook comprised three main themes and eight subthemes (see Appendix 2).
Reporting of the online survey followed the Checklist for Reporting Results of Internet E-Surveys (CHERRIES), while reporting of the qualitative components followed the Standards for Reporting Qualitative Research (SRQR). Completed checklists are provided in Appendix 3 and Appendix 4, respectively.
3. Results
3.1. Participant characteristics
Sociodemographic characteristics of the qualitative subsample (n = 47) and the total study sample (N = 126).
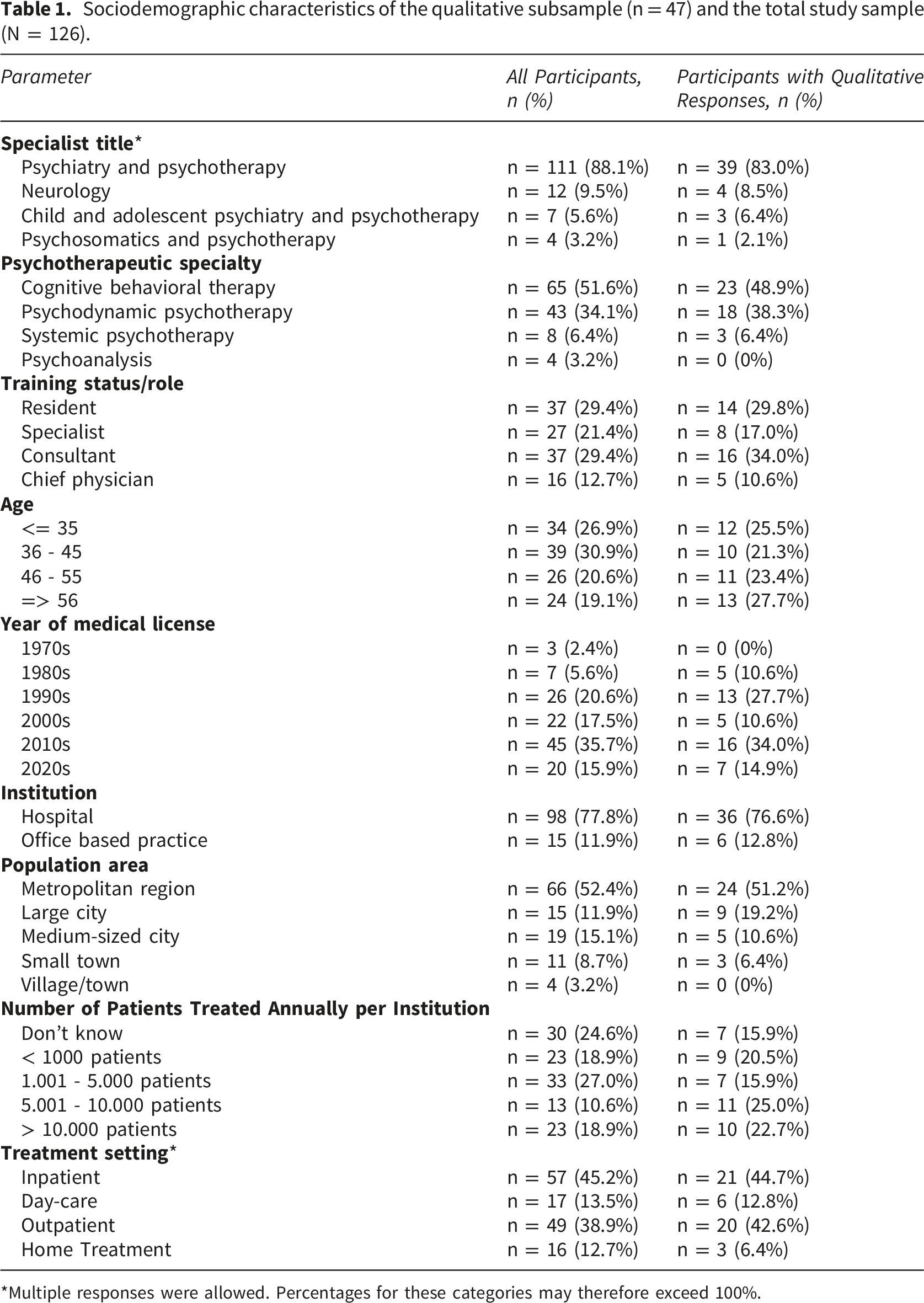
*Multiple responses were allowed. Percentages for these categories may therefore exceed 100%.
3.2. Quantitative responses
3.2.1. Use of genAI
Approximately half of the respondents (52%, n = 66) reported having used genAI tools at least once to answer clinical questions, with ChatGPT being by far the most commonly used tool (50%, n = 63). Other genAI chatbots mentioned by participants included Perplexity (n = 4), ClaudeAI (n = 2), You (n = 1), Mistral (n = 1), and Aya (n = 1). In total, 48% (n = 60) of respondents stated that they had not used genAI chatbots in psychiatric practice: See Figure 1. Use of generative AI to answer clinical questions. Percentages reflect valid responses (missing data excluded). N may vary by item.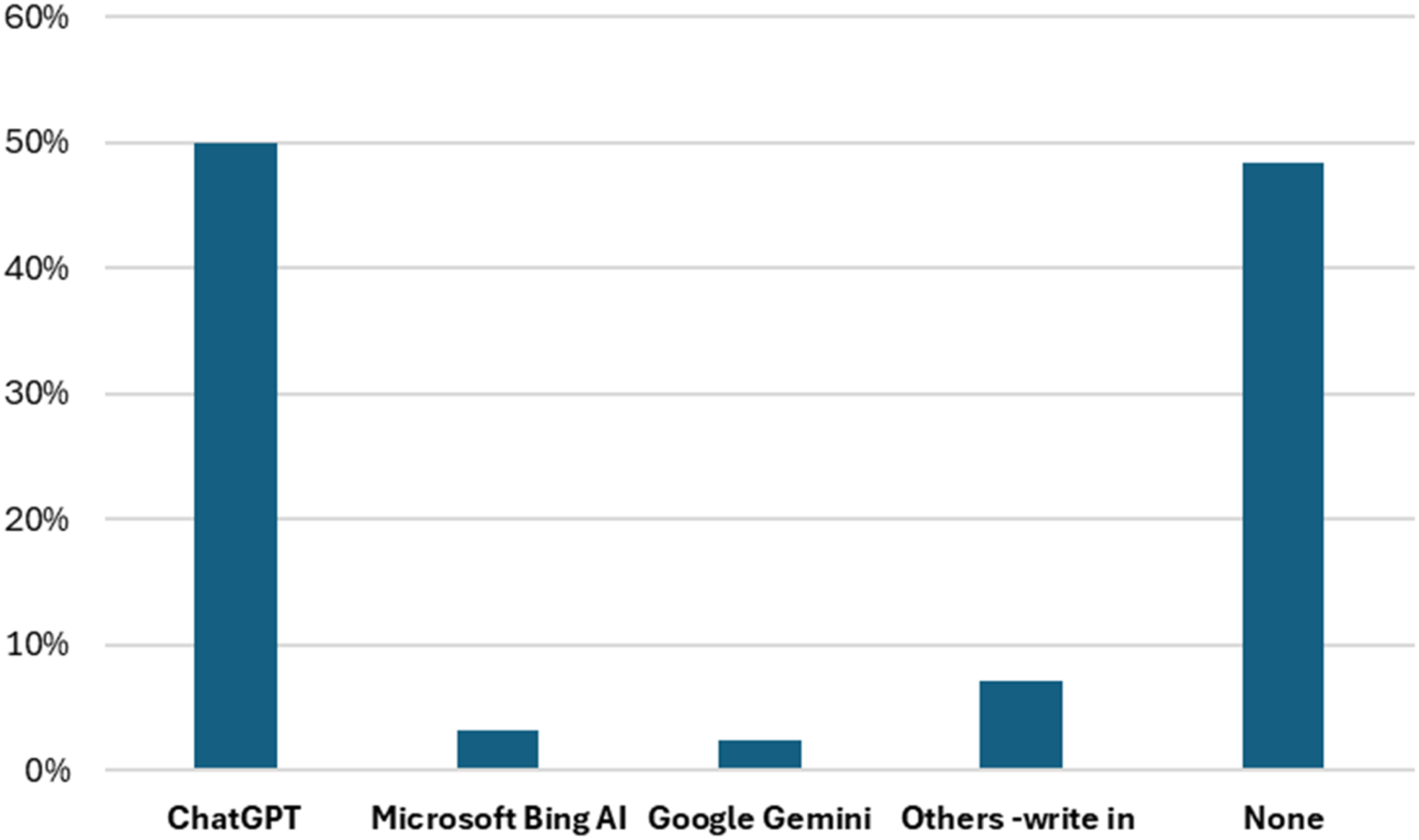
Participants reported using genAI tools for a range of clinical and administrative purposes. The most common uses included obtaining information on medications and potential interactions (n = 33, 22%) and creating medical reports (n = 28, 19%). Other frequently reported applications were suggesting treatment options (n = 15, 10%), supporting differential diagnostic considerations (n = 21, 14%), creating progress entries (n = 15, 10%), and generating clinical summaries from prior documentation (n =18, 12%) (see Figure 2). Clinical tasks supported by genAI by participants. Percentages reflect valid responses (missing data excluded). Multiple responses were allowed. Percentages may therefore exceed 100%.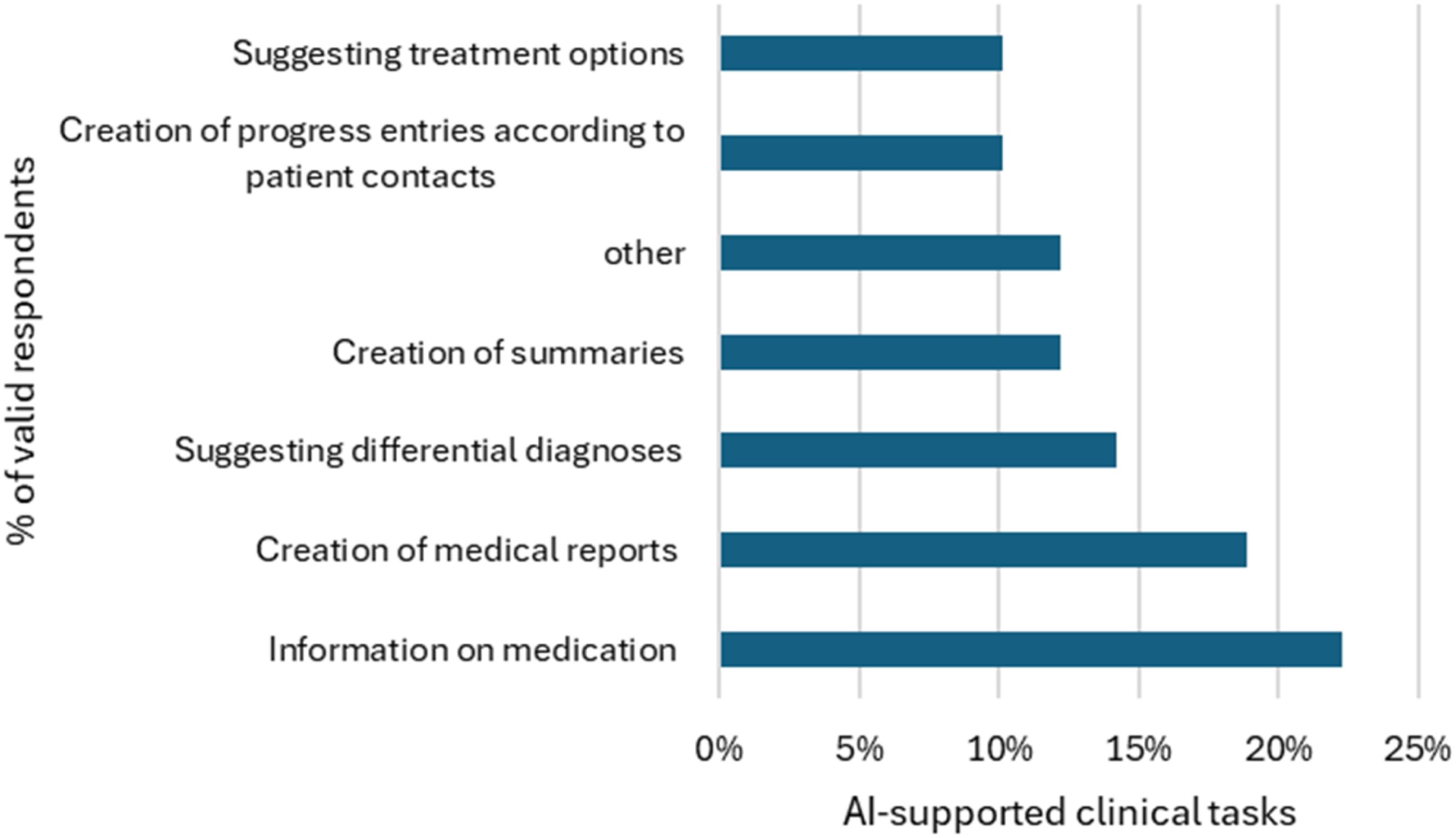
3.2.2. Opinions about effect on practice of genAI
Opinions about effect on practice of generative AI. Percentages reflect valid responses (missing data excluded). N may vary by item.
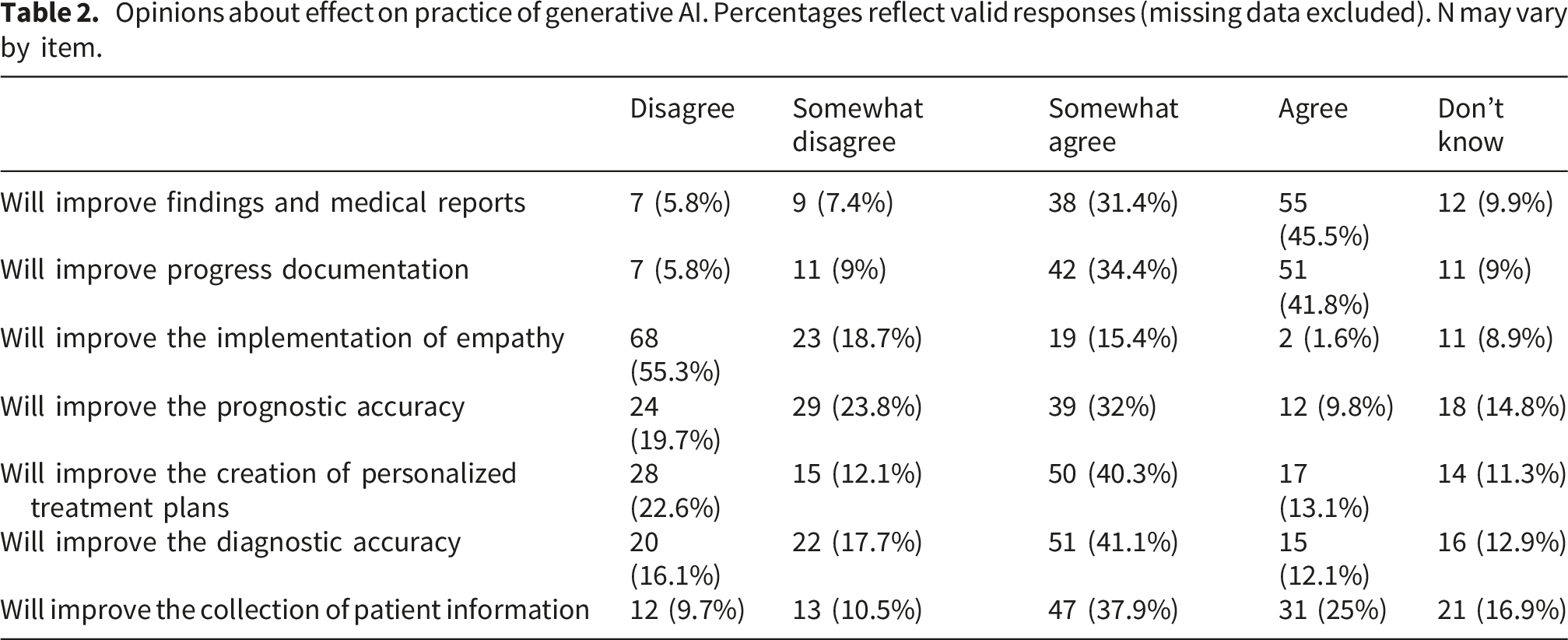
For interpretability, we report both disaggregated Likert-scale responses and, where appropriate, combined agreement categories (i.e.,“somewhat agree” and “agree”). Unless otherwise specified, combined percentages refer to these two categories.
Participants were generally positive about the potential impact of genAI on administrative and informational aspects of psychiatric work. The majority either agreed or somewhat agreed that genAI could improve medical reports (77%) and progress documentation (76%). However, only a small minority (17%) believed that genAI could improve the implementation of empathy in clinical care.
3.2.3. Opinions about patient’s use of genAI
Opinions about patient’s use of genAI. Percentages reflect valid responses (missing data excluded). N may vary by item.
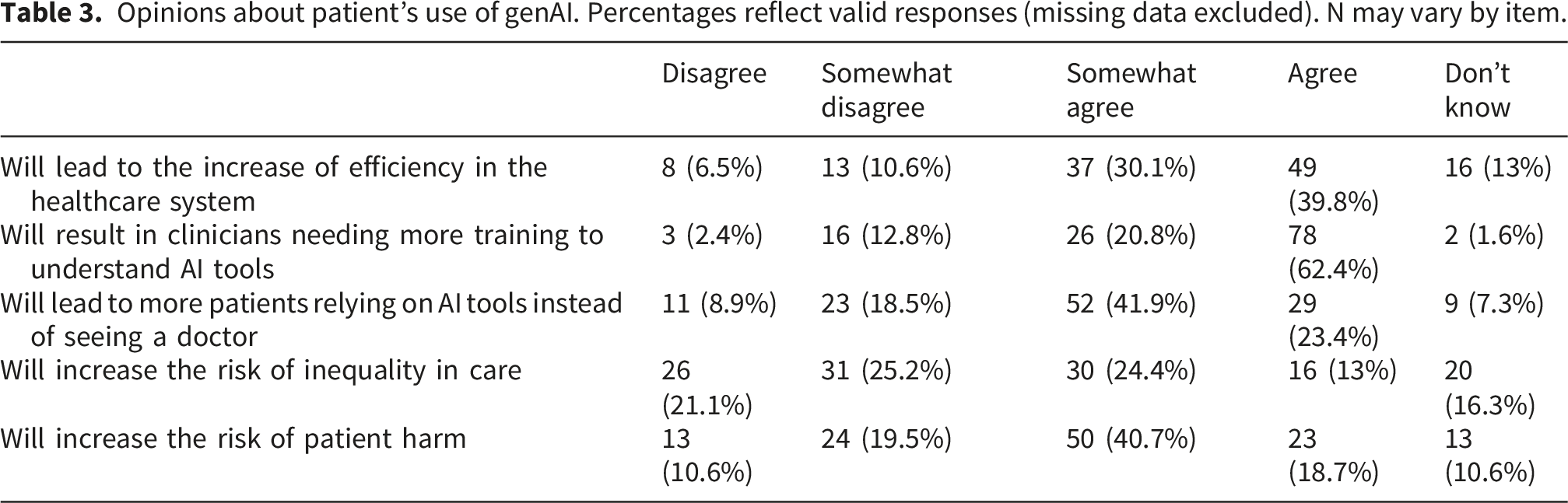
Regarding patients’ use of genAI tools, responses reflected mixed attitudes. 70% of respondents (combining “somewhat agree” and “agree”) indicated that clinicians would require additional training (20.8% somewhat agree; 62.4% agree) to handle genAI use in clinical contexts, and 63% believed that patients may increasingly rely on genAI instead of consulting a physician. Concerns about potential risks were common, with 59% agreeing that genAI use could increase the risk of patient harm.
3.2.4. Connection Between GenAI Use and Legal Action
See Figure 3. Connection Between genAI Use and Legal Action. Percentages reflect valid responses (missing data excluded). Multiple responses were allowed. Percentages may therefore exceed 100%.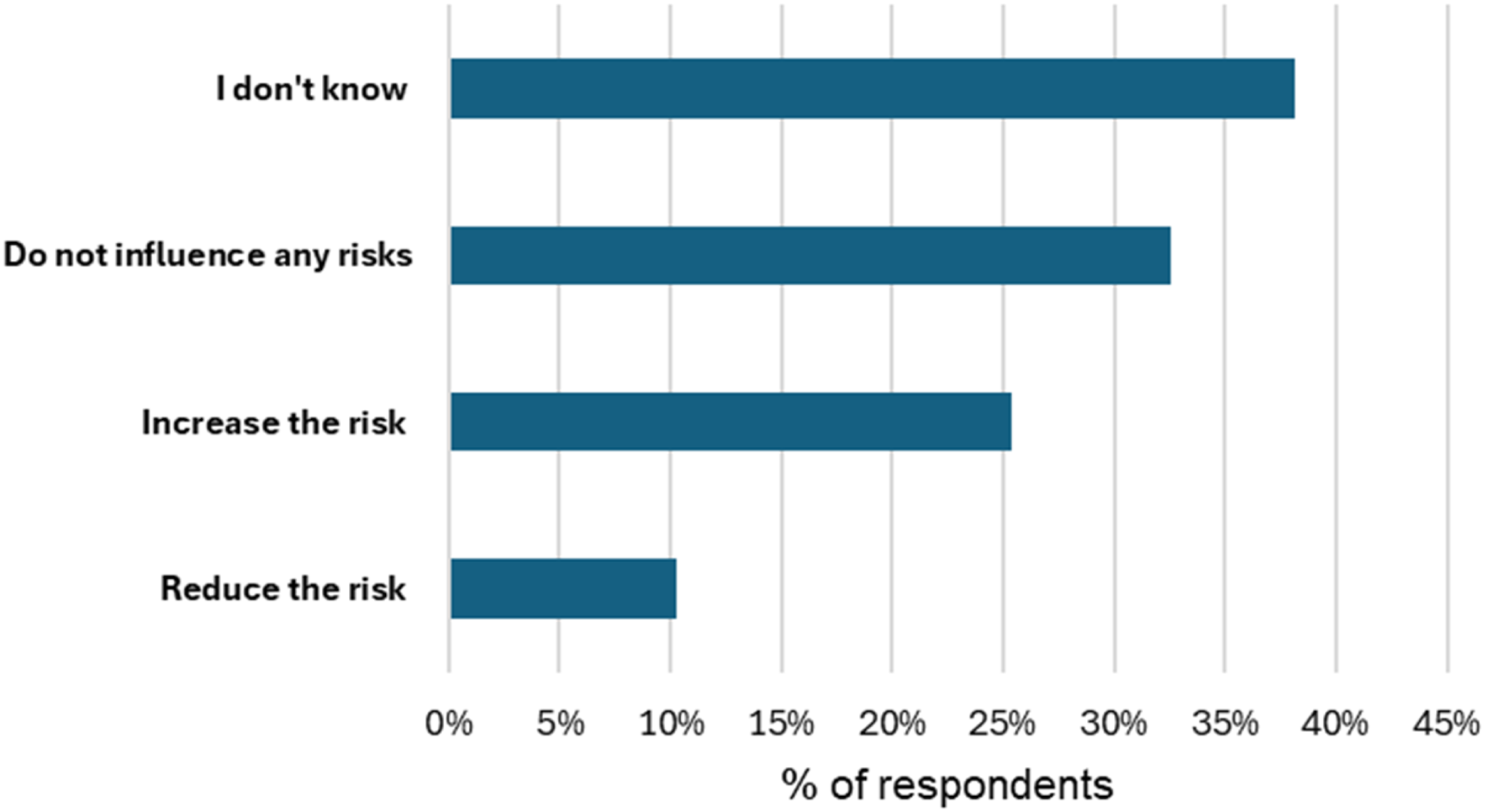
Participants were uncertain about the legal implications of genAI use in psychiatric care. Approximately one quarter of respondents believed that genAI use would increase the likelihood of legal action against clinicians (n = 32; 25%), while a third expected no change (n = 41; 32%). Notably, more than one third of participants indicated uncertainty (n =48; 38%), suggesting that medico-legal risks of genAI remain unclear among psychiatrists. This uncertainty is therefore reported as a substantive finding rather than treated as missing data.
3.3. Qualitative responses
Responses to the open-ended questions were optional. A total of 47 participants (37.3% of the sample) provided qualitative comments, which form the basis of the following analysis. or example: “Can simplify regulated processes, such as writing doctor’s letters”. These comments were generally concise, often consisting of a short phrase or one to two sentences (total word count of qualitative responses = 2,152). Through an iterative process of content analysis, three primary themes were identified regarding the perceived impact of genAI on mental healthcare: See Figure 4. Figures in parentheses refer to participant identification numbers, gender (M, F, or Prefer Not to Say) and whether the respondent reported using genAI to assist in with clinical tasks (Yes or No). Qualitative themes and sub themes concerning psychiatrists expectations towards genAI.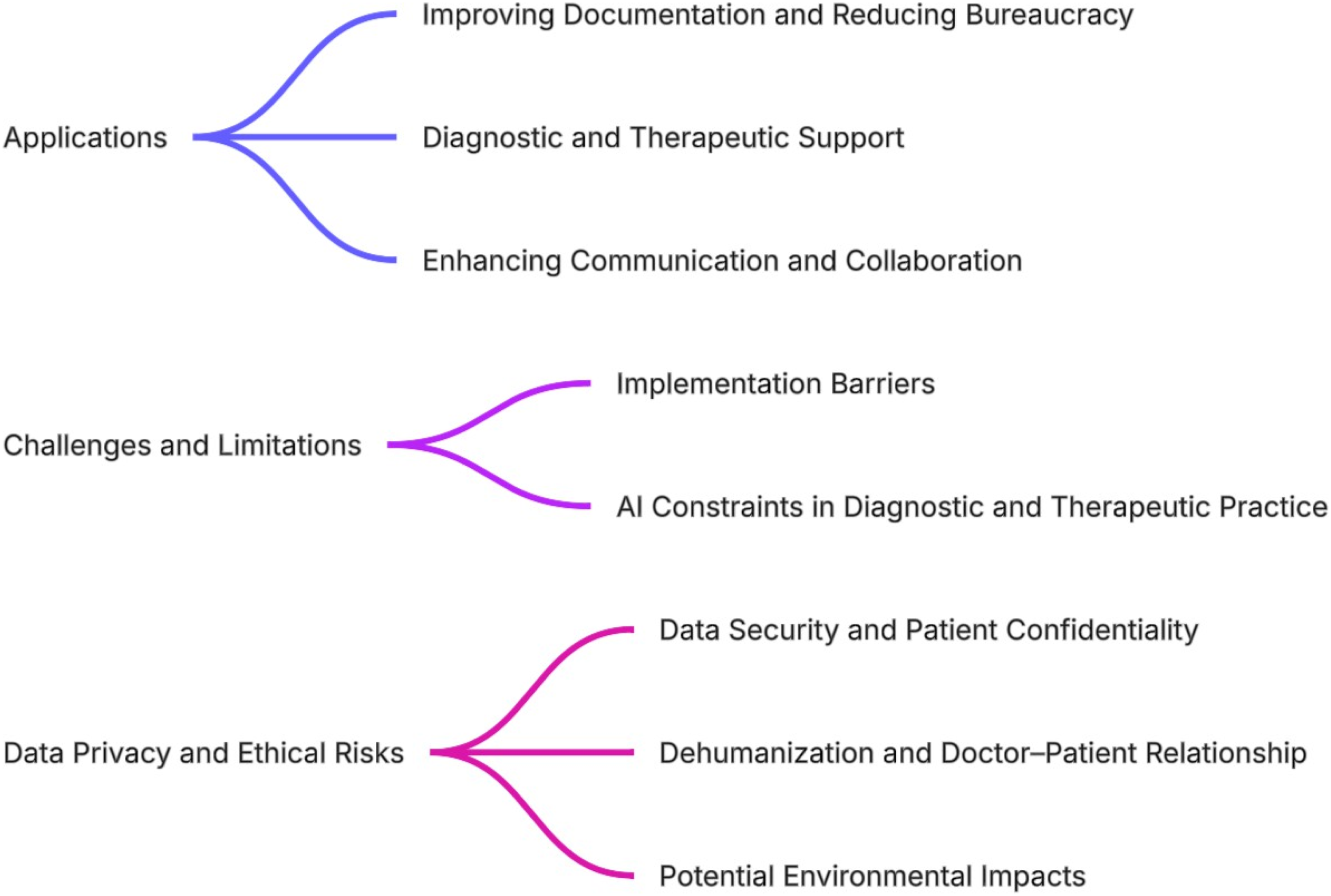
3.3.1. Applications
3.3.1.1. Improving documentation and reducing bureaucracy
The potential for genAI to alleviate the documentation burden in psychiatric practice was a recurrent theme among respondents. Several participants expressed optimism about the integration of genAI into administrative processes, particularly regarding its potential for saving time: “I consider the use of AI tools in our field to be absolutely sensible and desirable. The administrative tasks alone, for which there is usually little time, would be made much easier. I very much hope that it will be used more widely soon” (#68, F, No). Another participant shared a similar perspective on the topic: “I see a particular opportunity for AI in creating and revising documentation, findings, objection forms, etc., which currently account for too much of the bureaucratic work involved in psychiatric practice” (#52, F, No). A broader perspective on the time-saving potential was provided by one of the responders, highlighting the importance of time in the doctor-patient relationship: “AI tools should improve information processing for diagnostics, progress monitoring, standardized therapy-accompanying self-observation, and medication management, make bureaucratic requirements more efficient to process, and thus create space and time for qualitatively meaningful personal encounters between doctors and patients” (#40, F, Yes).
Some respondents acknowledged genAI’s potential to streamline workflows but emphasized the importance of understanding its limitations: “It can definitely simplify and speed up bureaucratic work and also optimize clinical work in terms of AI oversight, provided you know the limits of AI.” (#148, M, Yes). This perspective was echoed in a related comment: “They can be very helpful for creating practical texts/everyday correspondence if the problem with server locations could be solved” (#105, M, No).
However, not all respondents shared this enthusiasm. Some expressed skepticism regarding the practical benefits of genAI in documentation: “Never used because I would have to enter as much data as I write in the doctor’s letter, because psychiatric epicrisis reports are so individual.” (#127, N/A, No). Another participant voiced concern about inefficiencies: “I have only used ChatGPT once for a medical report as part of my work, but I had to make too many corrections and didn’t feel comfortable doing so. Otherwise, I don’t have any ideas for using it in my everyday life at the moment” (#67, F, Yes).
3.3.1.2. Diagnostic and therapeutic support
Only a minority of respondents viewed genAI positively in the context of diagnostic and therapeutic decision-making. One participant highlighted the need for targeted training for psychiatric professionals: “I have already used ChatGPT privately on various occasions and have been repeatedly pleasantly surprised – I am therefore fundamentally positive about the use of AI in a clinical context and would be very pleased to see specific applications combined with appropriate training” (#174, M, No).
Some respondents welcomed the use of genAI for clinical support, particularly in differential diagnosis: “Fast and differentiated information about diseases; complex questions possible” (#164, M, Yes). Still, limitations were acknowledged: “I already use the Plus version of ChatGPT every day, for example to create handouts for lectures. However, there are significant shortcomings in literature research, e.g., invented source entries. I find it helpful for differential diagnostic considerations” (#147, M, Yes). Another respondent perceived genAI’s diagnostic utility to be confined to early-career clinicians: “AI applications may increase diagnostic certainty among beginners, but are not useful in therapy” (#23, M, No).
3.3.1.3. Enhancing communication and collaboration
Language barriers remain a significant challenge in clinical communication, particularly for physicians who are not German native speakers. Several participants highlighted the role of genAI in addressing these challenges by offering linguistic support and improving the efficiency of written communication.
A non-German respondent reflected on how genAI facilitated his professional duties: “I and many of my non-German colleagues benefit enormously from the time saved by linguistic support in the preparation and correction of reports and discharge letters that concern diagnostic limitations. I personally anonymize the names of patients and other personal information” (#128, M, Yes).
The value of genAI in collaborative clinical contexts was further emphasized: “Complete anonymization is necessary when working with patient-related data. I see considerable time savings, especially when working with foreign colleagues in connection with dictations. AI is also a good way to question your own findings and expert opinions” (#142, M, Yes).
Another participant was unequivocal in their support: “Given the quality of the assistant doctors, especially their lack of German language skills, I can only see positives in AI” (#169, M, Yes).
3.3.2. Challenges and limitations
3.3.2.1. Implementation barriers
Participants shared a wide range of reflections on the potential and limitations of genAI in psychiatry, often drawing on analogies and broader societal concerns. For example: “From the attempt to compose Beethoven’s Tenth with AI – that probably sums it up: everything serial, mechanical, and involving a lot of hard work becomes easier and more precise; individual and creative work is not yet possible, it’s just the nature of the system; but then again, it also depends on the users, because some are satisfied with a lot of superficial and untested information” (#36, M, Yes). With this analogy, one participant emphasized the perceived lack of creativity in genAI-generated output.
For others, technical and organizational restrictions posed greater challenges. One respondent criticized the limited access to genAI tools in clinical environments: “Hospital operators and software manufacturers should urgently open up to the possibilities. Currently, our hospital IT even blocks ChatGPT” (#54, M, Yes). This practical concern was echoed in broader reflections about systemic readiness. As another participant expressed: “AI will have a massive impact on our lives, especially the world of work. It is doubtful whether Germany is prepared for this” (#169, M, Yes).
One participant questioned the long-term implications of investing in genAI while neglecting staffing needs: “A lot of money is being invested in AI instead of personnel. Standardized processes can be simplified, but many patients cannot be standardized. What good is it if AI creates doctor’s letters but the secretarial office remains unstaffed? Who is legally responsible for mistakes? Is it desirable to have robots driving through hospital rooms instead of hiring people?” (#59, M, No).
3.3.2.2. GenAI constraints in diagnostic and therapeutic practice
A further significant issue related to the perceived limitations of genAI in supporting psychiatric diagnosis and treatment planning. Some participants warned that genAI cannot be fully trusted in clinical contexts due to the risk of misinformation and fabricated data. One respondent raised this concern emphatically: “ChatGPT does not provide medical evidence, only the most likely answer! ChatGPT ‘invents’ alleged sources that do not exist, without this being apparent at first glance. ‘Medical’ recommendations are therefore in no way reliable and should never be accepted without verification. Even ‘scientific research’ via ChatGPT carries considerable risks of false or at least unfounded statements!” (#64, M, Yes) This viewpoint was shared by others who had also encountered limitations, particularly when using AI for in-depth or highly specialized queries. As one participant put it: “I use ChatGPT for research questions, including writing reports and similar documents. Unfortunately, if you have in-depth knowledge of the research area or methods, you quickly reach ‘hallucinatory’ limits. Limits – critical if this is not noticed! Unfortunately, it is a disappointment (at least for now) when it comes to really in-depth questions” (#85, F, Yes).
Another respondent elaborated on the same issue, pointing out the superficiality of answers and the absence of verifiable sources: “At least in the free version, ChatGPT only provides superficial answers to medical questions; answers cannot be properly evaluated due to a lack of references” (#131, M, Yes).
Linking these concerns, participants warned that gen AI’s shallow, poorly referenced answers undermine clinicians’ critical skills and professional judgement. One respondent highlighted the risk of professionals becoming overly reliant on genAI: “I expect that the ability to make a diagnosis and/or write a doctor’s letter independently will decline. The task of checking the recommendations/reports generated by AI for errors is tedious and not very creative, so I think the probability of errors is likely to increase, especially if colleagues don’t put much effort into critical review” (#74, F, No). In a similar vein, another participant reflected on the broader ethical and professional consequences of deferring to machines: “Personally, I would prefer to see the use of AI limited to this context or, more generally, to specific functions such as writing or editing. If humans stop memorizing information and thinking for themselves, they become machines and are no longer therapists” (#150, M, Yes).
Others adopted a more moderate position. While supportive of AI-assisted clinical tools, one respondent emphasized that these should not replace human judgment: “The use of AI for diagnosis and therapy recommendations should be supported, but not replaced” (#87, F, No).
3.3.3. Data privacy and ethical risks
3.3.3.1. Data security and patient confidentiality
Data privacy emerged as one of the most sensitive and frequently cited concerns in this study. Several participants expressed strong reservations about the use of genAI in clinical practice. As one respondent emphasized: “A topic of utmost relevance would be data protection when transferring patient cases, files, and reflections, especially when transferring them to AI outside the EU. For these and ethical reasons, the use of AI in psychiatry must be very well supported and thought through in order to take advantage of the great opportunities without creating new risks” (#163, M, No).
Some participants adopted a more categorical stance, rejecting the involvement of systems with insufficient transparency or international safeguards: “Procedures with non-transparent algorithms have no place in direct patient care, nor do those that involve the processing of personal health data in countries without reliable data protection regulations” (#105, M, No).
“Not resolved. Use of real patient data is not yet possible. No funding available. This would therefore be a purely unfunded hobby project with virtual dummy data that is not protected by data protection laws” (#88, M, Yes). Others pointed not only to legal and ethical issues but also to structural barriers such as lack of funding.
Still, a note of cautious optimism was expressed by one of the respondents who acknowledged the potential benefits of genAI, particularly in documentation and support for non-native speakers, but noted infrastructure as a key limiting factor: “I believe that ChatGPT&Co can be an enormous help, especially when it comes to documentation and creating documents. This also applies to dictations and for non-native speakers. Processing in the cloud is (still) problematic. If the servers could be located securely in Europe or even in the clinic, this would dramatically expand the possibilities” (#42, M, Yes). Another participant added that with appropriate safeguards, such as strict anonymization, the use of genAI in clinical contexts could be feasible: “Complete anonymization is necessary when working with patient-related data” (#142, M, Yes).
3.3.3.2. Dehumanization and doctor–patient relationship
Ethical concerns were also raised regarding the potential impact of genAI on the therapeutic relationship and on clinical training. One participant articulated this apprehension directly: “I fear a deterioration in the doctor-patient relationship and communication. I fear poorer training in the ’clinical eye’” (#81, F, No). The relational and cognitive dimensions of care were further questioned in another statement, which addressed the broader role of human engagement in medical practice: “I would not feel entirely comfortable being treated by a doctor who draws their knowledge from AI…” (#150, M, Yes).
3.3.3.3. Potential environmental impacts
The topic of the potential environmental impacts of using genAI was brought up several times by the participants. While one participant viewed the potential environmental impacts as negative and limiting the use of genAI: “In addition, the use of AI consumes considerable amounts of energy and water. Therefore, at this point in time, I am against the use of existing AI systems in the medical field” (#122, F, No), the other held an opposing viewpoint on the matter: “…But letting it [AI] help you promotes efficiency and saves energy” (#150, M, Yes).
4. Discussion
4.1. Main findings
This is, to our knowledge, the first mixed methods survey in an EU country to examine psychiatrists’ experiences and attitudes toward genAI–based chatbots. Administered approximately one year after the public release of ChatGPT, this exploratory study in Germany found that just over half of respondents had used a genAI in clinical work, most often ChatGPT. Usage was concentrated in administrative and informational domains, such as drafting letters and retrieving medication information, rather than in direct diagnostic reasoning or therapeutic interactions. This quantitative pattern was mirrored in the qualitative data, where many respondents emphasized genAI’s potential to reduce documentation burden and streamline bureaucratic workflows, while only few mentioned diagnostic or therapeutic applications.
Participants were most positive about potential documentation efficiency gains, with nearly seven in ten agreeing that genAI could make documentation more efficient. This aligns with international findings that administrative relief may be perceived as a primary opportunity for genAI in psychiatry. 23 However, only around one in five respondents believed genAI could help convey empathy, and concerns were common about patient-facing use, particularly the risk of misinformation. The scepticism was echoed in free-text comments highlighting risks of “hallucinated” information and fears that reliance on genAI might erode clinicians’diagnostic judgement or the therapeutic relationship. Nearly nine in ten agreed that psychiatrists require more training to use these tools responsibly, a sentiment reinforced by qualitative statements advocating for structured education and institutional guidance.
Views on medico-legal implications were mixed: a quarter of respondents anticipated increased legal risk, a third expected no change, and over a third were unsure. Correspondingly, several qualitative comments underscored uncertainty about legal accountability, especially in cases where genAI-assisted documentation might contain errors or unverified information. These findings are notable given that the EU AI Act, implemented in early 2025, 12 formally categorizes healthcare AI as “high-risk” and requires transparency, human oversight, and robust data governance (European Parliament, 2024). Our results suggest that German psychiatrists have yet to see concrete guidance on how these requirements will apply in day-to-day psychiatric care.
Taken together, the integration of quantitative frequencies and qualitative narratives reveals a consistent pattern: in this sample, genAI primarily perceive as a tool for administrative support rather than clinical reasoning, balancing optimism about efficiency gains with significant ethical and legal concerns. The qualitative insights therefore extend and enrich the quantitative findings by explaining why psychiatrists express caution - linking efficiency expectations to documentation pressures, and concerns about empathy to fears and dehumanization. However, these quantitative findings should be interpreted with caution given the limited and sometimes fragmentary nature of the responses, while offering contextual insight that complements the quantitative findings.
Although cross-national comparisons should be interpreted cautiously, as available surveys differ in sampling frames, survey timing, and question wording, it is still worth exploring what we know currently about national differences in genAI adoption. Our findings echo those of the recent APA-affiliated U.S. survey, 8 which also reported limited direct clinical use, a focus on administrative applications, and high demand for training. However, engagement with diagnostic or treatment-planning uses appeared even lower in our German sample, possibly reflecting a more cautious adoption climate, institutional restrictions, or lower integration of approved genAI tools in psychiatric settings.
Our findings are also broadly consistent with an Australian survey of 107 community members and 86 mental health professionals, which reported that 43% of professionals had used genAI – most often for research and report writing – while simultaneously expressing mixed attitudes about its future role in mental health care, balancing perceived efficiency and accessibility benefits against concerns about privacy, ethics, and reduced human connection. 24 Similarly, a 2025 UK survey of 1,005 general practitioners found that 25% reported purposeful use of genAI tools in clinical practice. 25 In this survey, 69% anticipated improved documentation and 79% agreed that training may be needed, figures that are broadly similar to those in our German psychiatrist sample (70% and 89%, respectively). 7 However, UK respondents were more likely than their German counterparts to expect that patients might rely on genAI instead of seeking medical care (59% vs. 42%), and both groups were similarly sceptical about genAI’s capacity to enhance empathic communication suggesting that adoption remains incremental across high-income countries, with variability in uptake likely reflecting differences in regulatory environments, institutional readiness, and cultural attitudes toward genAI in healthcare. We stress that, against these prevailing opinions, emerging findings suggest that genAI tools are showing significant capacity to detect emotional states and to communicate information in ways perceived as compassionate—indeed, in some studies even outperforming clinicians.20,21 Again, however, we emphasize that when it comes to national comparisons, apparent differences may reflect methodological variation rather than underlying adoption differences. We interpret this limitation as yet further reason for more robust national surveys into genAI adoption.
4.2. Strengths and limitations
A key strength of this study is that it expands research on psychiatrists’ perspectives to a non-English-speaking, European context with a distinctive healthcare structure and strict data protection laws. The questionnaire was adapted from prior international work 8 and reviewed by German psychiatrists to ensure contextual appropriateness. Recruitment across both urban (Berlin) and rural (Brandenburg) regions, supplemented by national DGPPN newsletter distribution, broadened reach across different practice environments.
Several limitations must be acknowledged. The response rate was low, limiting generalizability, and self-selection bias may have led to overrepresentation of psychiatrists with stronger interest in genAI. Because open professional dissemination prevents a precise denominator of invited participants and recruitment only took place in one region of Germany, representativeness cannot be ensured. In addition, partial responses were excluded without formal attrition analysis, which may have introduced additional bias. Recruitment occurred in two widely separated phases (September 2024 and December 2024–March 2025), during which awareness, capabilities, and media coverage of genAI evolved rapidly; temporal variation in exposure and attitudes cannot be excluded. As in similar surveys, some items did not distinguish between current experiences and anticipated future effects, introducing interpretative ambiguity. The limited, non-stratified sample precluded subgroup analyses by demographic or professional characteristics. Because of the exploratory design and sample size, the study did not examine predictors of genAI use or attitudes using multivariable modeling. Future studies should be powered to conduct regression analyses to identify determinants of adoption.
The use of a four-point Likert scale without a neutral midpoint may have influenced response distributions by encouraging directional responses, potentially overestimating agreement or disagreement. We also did not systematically collect data on academic affiliation (e.g., employment in university hospitals), which may influence familiarity with and attitudes toward emerging technologies such as genAI. Recruitment occurred across two temporally separated phases during a period of rapid development in genAI technologies and public awareness. As responses could not be linked to specific recruitment phases, potential temporal effects cannot be assessed and may have influenced the findings.
Future studies should employ stratified or probability-based sampling, incorporate richer qualitative components, and explore variations across psychiatric subspecialties. Furthermore, little is known about patients’ use of these tools in Germany – an area that warrants much more targeted survey research. Patients’ perspective will be particularly critical regarding trust, stigma, and the perceived benefits or harms of genAI integration into mental healthcare including by psychiatrists. 26 Finally, to explore adoption in different countries, we call for more harmonised, robust, cross-national, longitudinal research into the uptake of genAI among key stakeholders.
4.3. Conclusions
While our findings suggest that some German psychiatrists are beginning to integrate genAI-based chatbots into their work – mainly for administrative and informational tasks – we cannot infer that this reflects broader national practice. Efficiency gains were widely anticipated, yet significant uncertainty remains regarding clinical applications, medico-legal implications, and how the EU AI Act will be operationalized in psychiatric settings, particularly given the widespread use of general purpose, largely non-EU-based tools. The strong call for training underscores the urgent need for structured, evidence-based guidance. This transitional moment offers an opportunity for policymakers, professional bodies, and developers to work with clinicians to ensure that any potentialfuture expansion of genAI adoption in psychiatry is both ethically sound and aligned with patient care priorities.
Supplemental material
Supplemental material - Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany
Supplemental material for Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany by Julian Schwarz, Vera Goer, Olga Guzhova, Lena Holtz, Felix Mühlensiepen, Charlotte Blease in DIGITAL HEALTH
Supplemental material
Supplemental material - Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany
Supplemental material for Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany by Julian Schwarz, Vera Goer, Olga Guzhova, Lena Holtz, Felix Mühlensiepen, Charlotte Blease in DIGITAL HEALTH
Supplemental material
Supplemental material - Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany
Supplemental material for Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany by Julian Schwarz, Vera Goer, Olga Guzhova, Lena Holtz, Felix Mühlensiepen, Charlotte Blease in DIGITAL HEALTH
Supplemental material
Supplemental material - Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany
Supplemental material for Psychiatrists’ experiences and opinions of generative AI: An exploratory online mixed methods survey in Germany by Julian Schwarz, Vera Goer, Olga Guzhova, Lena Holtz, Felix Mühlensiepen, Charlotte Blease in DIGITAL HEALTH
Footnotes
Acknowledgement
The authors thank all participating psychiatrists for taking part in the survey and sharing their experiences and perspectives. We also acknowledge the support of the institutions and professional networks that assisted with the distribution of the survey. We would also like to thank Lena Holtz for editorial assistance in the submission process.
Author contributions
Charlotte Blease: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. Vera Goer: Writing – review & editing. Olga Guzhova: Qualitative data analysis, Writing – original draft, Writing – review & editing. Lena Holtz: Data collection, quantitative data analysis, software, visualization, writing – original draft. Felix Mühlensiepen: Writing – review & editing. Julian Schwarz: Conceptualization, supervision, data collection, qualitative data analysis, resources, Writing - original draft, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Brandenburg Medical School publication fund supported by the German Research Foundation and the Ministry of Science, Research and Cultural Affairs of the State of Brandenburg.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JS is a co-author on related concurrent work in this field, however JS declares no conflict of interest. All other authors declare no conflict of interest.
Data Availability Statement
Due to GDPR and ethics constraints, the original non-anonymized dataset and analysis scripts cannot be shared. The individual-level survey dataset has been fully anonymized by removing all free-text responses, geographic information, and any potentially identifying details to ensure participant privacy in accordance with GDPR and institutional ethics requirements. The anonymized dataset, along with the full survey instrument (German original version and English translation), is openly available in a persistent repository on the Open Science Framework (OSF) at: ![]() .
.
Trial Registration
This study was reviewed by the Ethics Committee of the Brandenburg Medical School, which issued a waiver of ethical approval (protocol no. 228072024-ANF).
Guarantor
JS
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.