
Abstract
Objectives
To evaluate the feasibility and clinical impact of an IoT-based teleassistance system for remote monitoring of preterm neonates receiving home oxygen therapy.
Methods
A historically controlled cohort study was conducted in Manizales, Colombia, with three phases: (1) baseline data collection from neonates receiving traditional follow-up (n=32), (2) development of an Internet of Things (IoT)-based teleassistance system integrating physiological monitoring, cloud storage, and mobile applications, and (3) pilot testing in a prospective intervention cohort (n=25). The primary outcome was the duration of home oxygen therapy.
Results
Median duration of home oxygen therapy was reduced from 34 days (IQR 25–46) in the control group to 10 days (IQR 7–17) in the intervention group (p<0.001). Reliable communication was achieved through 4G and Wi-Fi, while LoRa performance was limited by geographic constraints.
Conclusions
IoT-based teleassistance was associated with a reduction in the duration of home oxygen therapy in preterm neonates and demonstrated feasibility for remote monitoring in resource-limited settings.
Keywords
Introduction
Premature neonates often require home-based supplemental oxygen therapy after discharge from neonatal intensive care units (NICUs) due to underdeveloped pulmonary systems or chronic conditions such as bronchopulmonary dysplasia and congenital heart disease. 1 This vulnerable population demands continuous and precise physiological monitoring to prevent complications, including retinopathy of prematurity (ROP), neonatal sepsis, and cardiovascular instability.2,3
In Colombia, up to 40% of premature neonates born after 32 weeks receive home oxygen therapy. 2 However, current follow-up approaches—ranging from structured programs like kangaroo mother care to unstructured outpatient visits—lack standardized protocols for continuous data acquisition and timely therapeutic decision-making.
Non-invasive monitoring technologies, particularly photo-plethysmography (PPG), have appeared as promising tools in telemedicine and telecare environments. PPG sensors can measure oxygen saturation (SpO2), heart rate (HR), and, with advanced modeling, estimate blood pressure (BP).4–6 Accurate BP assessment in neonates is clinically significant, as their immature cardiovascular systems present unique hemodynamic characteristics such as high heart rate variability and reduced arterial compliance, which challenge direct adaptation of adult-based algorithms.7,8 Despite advances in PPG-based BP estimation in adult populations,9,10neonatal-specific models are scarce and often limited to NICU environments without integration into portable or IoT-ready platforms. 11
Addressing these gaps requires solutions that combine physiological modeling with embedded computing capable of operating under the constraints of homecare environments—limited connectivity, energy restrictions, and the need for caregiver-friendly interfaces, as shown in previous studies. 12 This platform integrates a wearable module with a MAX30102 PPG sensor for real-time acquisition of SpO2, HR, and PPG-derived BP using a neonatal-adapted Windkessel model. Signal processing algorithms are optimized to manage neonatal motion artifacts and to use on resource-constrained devices, while communication is supported via 4G/LTE and Wi-Fi for reliable data transmission.13–15
Objective: This study aims to evaluate the effectiveness and feasibility of an IoT-based teleassistance system, integrating PPG-based blood pressure estimation and multiparameter physiological monitoring, to reduce the duration of home oxygen therapy and improve clinical decision making for preterm neonates in Manizales, Colombia.
Materials and methods
This historically controlled cohort study was conducted in Manizales and Villamaría, Colombia, between November 2020 and May 2025, and included an embedded technological development phase to evaluate an Internet of Things (IoT)-based teleassistance system for neonatal home oxygen therapy. A three-phase methodological approach was implemented to evaluate the feasibility and effectiveness of an Internet of Things (IoT)-based teleassistance system for neonatal home oxygen therapy (Figure 1). The protocol was approved by a local institutional ethics committee (Act No. 087, 2019). Written informed consent was obtained from the parents or legal guardians of all participants prior to study initiation. Overview of the study design and three-phase methodological approach.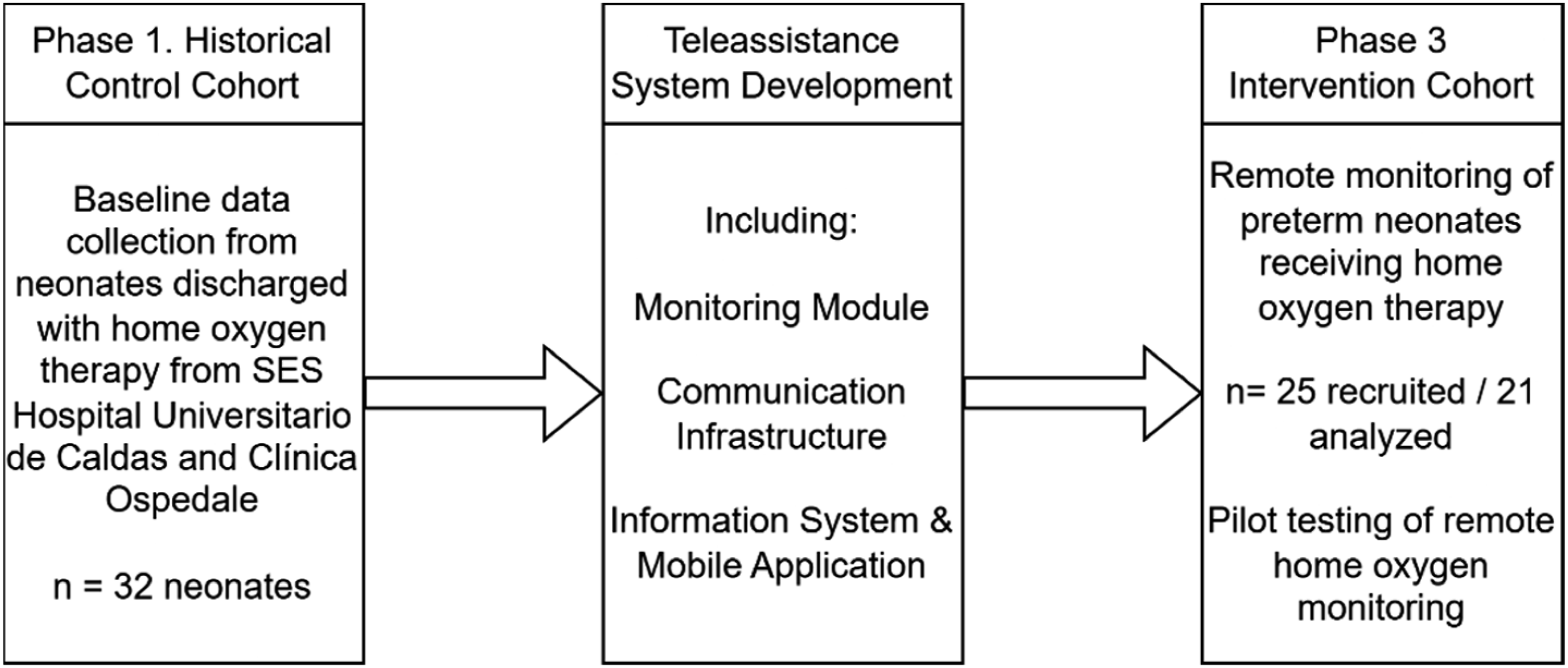
Phase 1: Baseline establishment (historical control cohort)
Between November 2020 and June 2021, prospective data were collected from neonates discharged with home oxygen therapy from the neonatal units of two local hospitals in Manizales, Colombia. Eligible participants were found through hospital discharge records and met the following inclusion criteria: • Clinical indication for home oxygen therapy due to prematurity or chronic neonatal lung disease. • Residence within the municipalities of Manizales or Villamaría. • Discharge to home without access to structured telemonitoring.
Exclusion criteria included congenital heart disease or other major anomalies, incomplete medical records, or transfer to another institution. A total of 32 neonates met these criteria. Infants were discharged with home oxygen therapy when oxygen requirements were ≤0.5 L/min to maintain SpO2 within the predetermined range (90–95%), and when they met additional criteria: weight gain of at least 20–30 grams/day outside the incubator for three days, no evidence of anemia (hematocrit and hemoglobin within the past week), physiological stability without acute illness (or with controlled chronic illness), and no apneas in the last week, following the guidelines of the Colombian Neonatology Association and the Colombian Pediatric Pulmonology Association. 16 They had received supplemental oxygen therapy through unstructured follow-up programs or the kangaroo mother care program.
No teleassistance system was used in this cohort; follow-up was performed via scheduled outpatient visits, subject to appointment availability and authorization from healthcare providers.
Phase 2: Teleassistance system development
The intervention was developed as a comprehensive teleassistance service for remote physiological monitoring. The system included: (a) A wearable monitoring module integrating sensors for oxygen saturation (SpO2) and non-invasive blood pressure estimation using photoplethysmography (PPG);
6
(b) IoT-based communication capabilities (4G/LTE and Wi-Fi, with experimental LoRa). (c) A secure, cloud-based information system for data storage and real-time visualization. (d) A mobile application providing caregivers and healthcare professionals with alerts, patient data, and educational materials.
The system was designed for continuous monitoring and automated generation of visual and auditory alerts when physiological parameters exceeded predefined thresholds. The hospital care team received remote access to the monitoring dashboard to support timely clinical decision-making. The monitoring module was calibrated in neonatal units against standard clinical devices prior to home deployment.
The developed module measures oxygen saturation, heart rate, blood pressure, and temperature. Oxygen saturation, heart rate, and blood pressure estimation are derived from a MAX30102 optical plethysmography sensor (Maxim Integrated Products, Inc) processed via a Raspberry Pi 4 (Sunhokey Electronics Co) running custom Python algorithms. Visual and auditory alerts show abnormal values. Diagnostic reliability testing was conducted between the sensor’s readings and standard ICU monitors. Using Walter et al.’s method, 17 a sample size of 616 observations was calculated to achieve 80% power and 95% confidence, with p0: 0 and p1: 0.1. The Pearson correlation coefficient for SpO2 was 0.87.
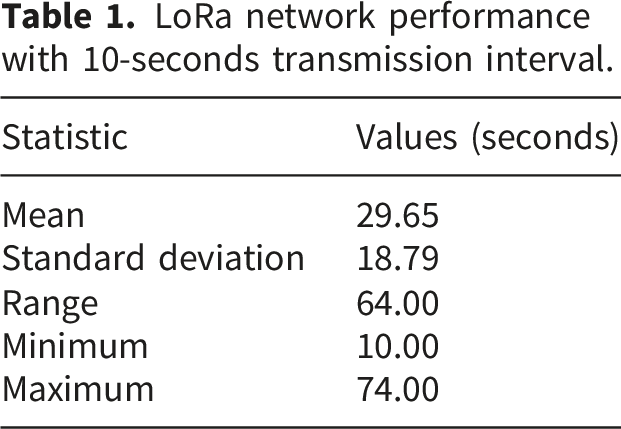
Communication Network: IoT connectivity was enabled through 4G/LTE, Wi-Fi, and experimental LoRaWAN. Ideal LoRa coverage (Figure 2) was simulated for four routers; practical range was limited to 2 km line-of-sight with notable data loss. LoRa was only used when stable message reception under three minutes was confirmed. Mean reception interval for a 10-second send rate is shown in Table 1. Ideal LoRa network coverage map generated using radio mobile (https://www.ve2dbe.com/english1.html), a tool distributed under a creative commons license. LoRa network performance with 10-seconds transmission interval.
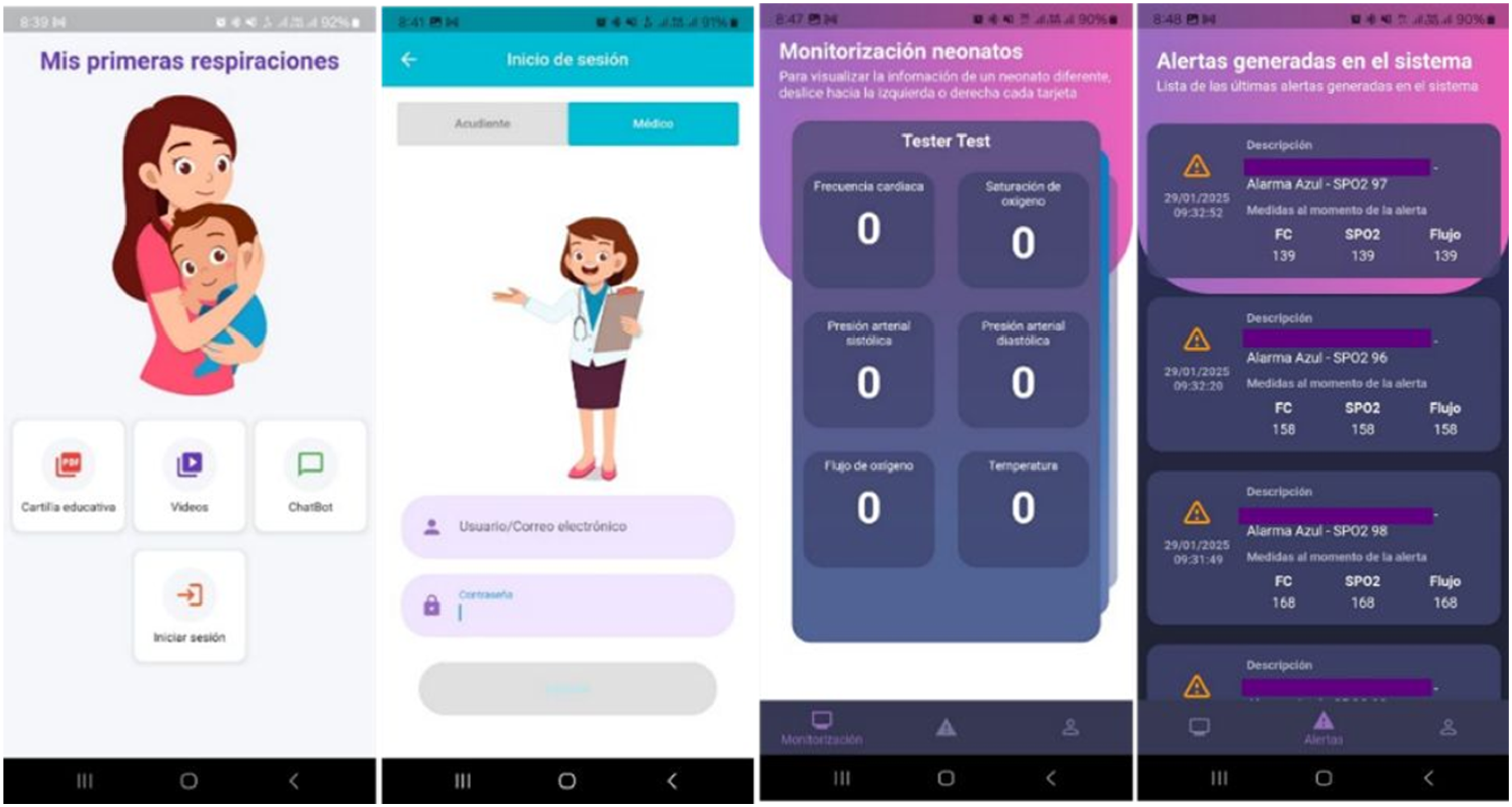
Information System: A web-based platform registers neonates, caregivers, treatment data, and physiological readings (Figure 3). An Android application (Figure 4) provides caregivers and clinicians with real-time alerts, educational materials, and visualizations. Web-based platform interface developed as part of this study for remote monitoring of neonatal patients. The system is part of the project’s original development. Mobile application interface developed within this project, providing real-time alerts, patient data visualization, and educational content.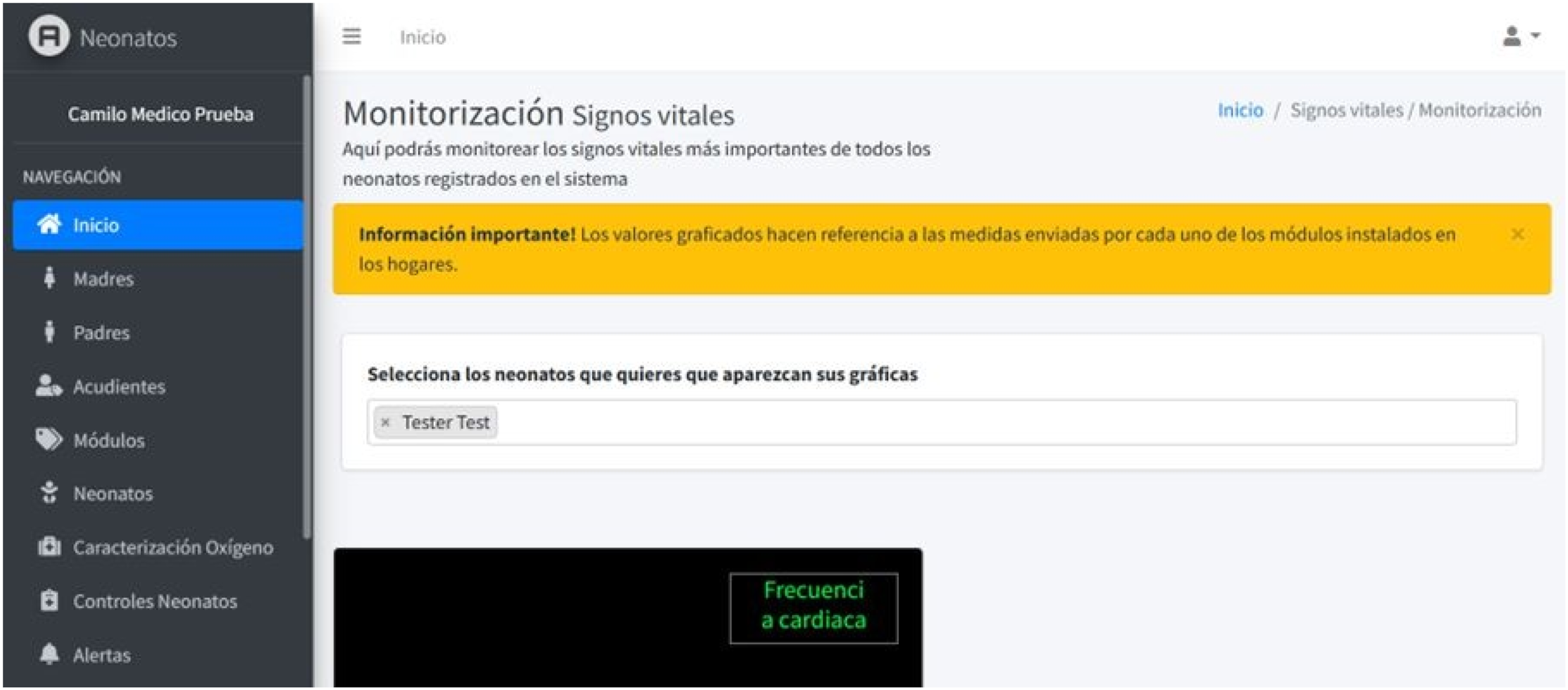
Phase 3: Teleassistance pilot testing (intervention cohort)
From July 2024 to May 2025, a pilot study was conducted with neonates meeting the same inclusion and exclusion criteria as the historical control cohort, with the additional requirement of residence within an IoT network coverage area to ensure real-time data transmission. Recruitment took place at SES Hospital Universitario de Caldas and Clínica Ospedale before discharge, using consecutive sampling of all eligible neonates who met the predefined eligibility criteria. No formal matching procedure was performed between the intervention and historical control cohorts. Instead, participants were recruited consecutively until an intervention cohort of comparable size to the historical control group was achieved.
In the intervention cohort, home oxygen therapy was monitored continuously via the teleassistance module. Discontinuation criteria were standardized: maintenance of SpO2 between 90% and 95% for 48 continuous hours on an auxiliary oxygen system. Oxygen weaning was performed by halving the oxygen flow at each step. Upon meeting these criteria, the teleassistance service was ended and the device retrieved. Clinical decisions were made following standardized institutional protocols supported by clinician judgment.
Interoperability testing was performed to integrate the system with existing hospital infrastructure and clinical workflows. Caregivers received on-site training at discharge and ongoing technical support during home use. Response to alerts and compliance with device usage were monitored throughout the study period.
Data analysis
The primary outcome variable was the duration of home oxygen therapy. Secondary outcomes included the corrected age at which home oxygen was stopped, the total home oxygen consumption and system connectivity performance.
A sample size of 23 infants per group was calculated to demonstrate a statistically significant difference of one week in the corrected gestational age at which oxygen was discontinued, with 80% power and a 0.05 significance level, using an average corrected age of 38.5 weeks for discontinuation of home oxygen in preterm infants with mild BPD as a reference. 18
Categorical variables were compared using Pearson chi-square or Fisher’s exact test. Continuous variables with normal distribution according to the Shapiro–Wilk test were compared using the student’s t-test; those without normal distribution were compared with the Mann–Whitney test. Finally, Cox regression and Kaplan–Meier analyses were performed by group (non-intervention vs intervention) and compared using the log-rank test. No multivariable adjustment was performed due to sample size limitations. Data were analyzed using Stata 16.1 (Stata Corp, TX, USA).
Results
Participant flow and recruitment period. A total of 32 neonates met the inclusion criteria for the historical control cohort (Phase 1). For the intervention cohort (Phase 3), 25 neonates were recruited, but 4 parents declined to take part. Recruitment for the control group took place between November 2020 and June 2021, while recruitment for the intervention group occurred between July 2024 and May 2025. Figure 5 summarizes participant recruitment, enrollment, and analysis according to TREND recommendations. Baseline demographic and clinical characteristics were comparable between cohorts. All participants in both cohorts met the same inclusion and exclusion criteria. Participant flow diagram following TREND/CONSORT format.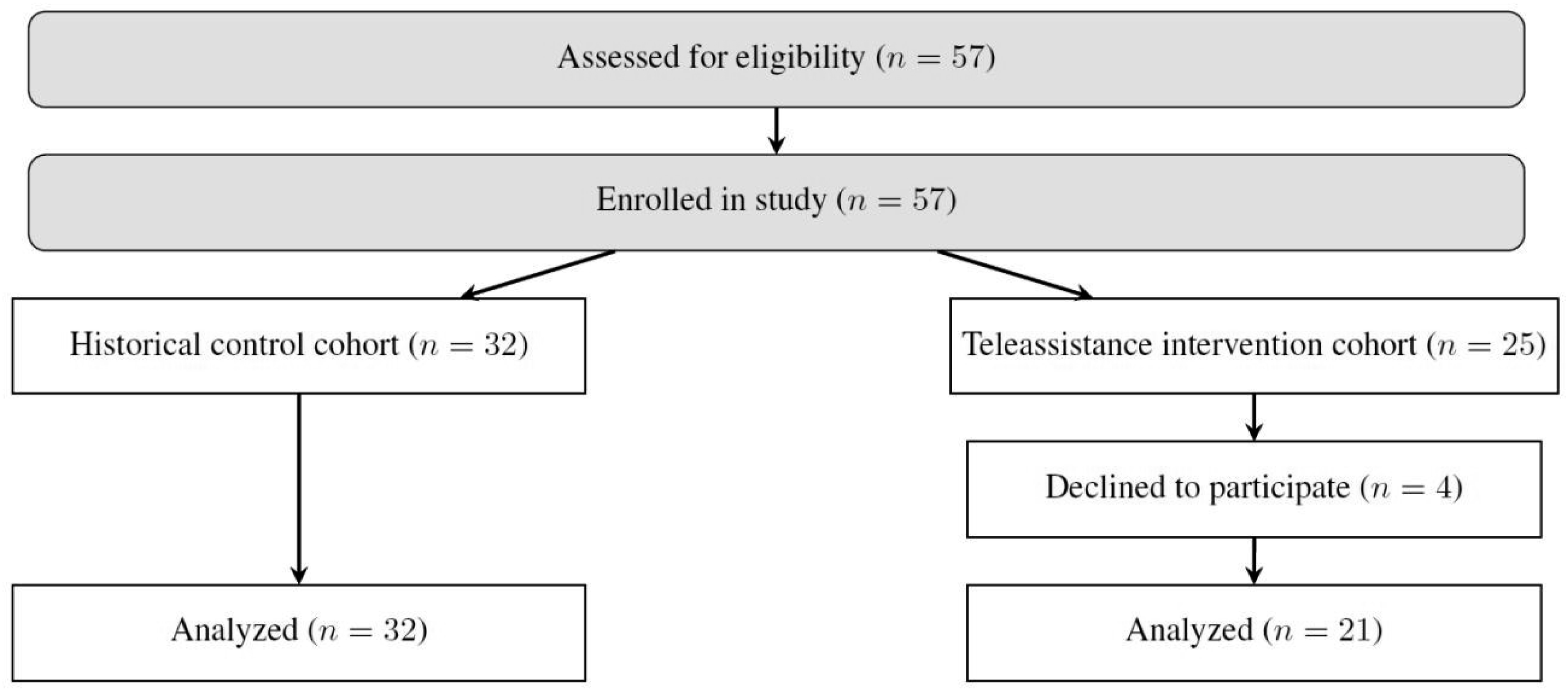
Clinical characteristics of the studied patients by group.
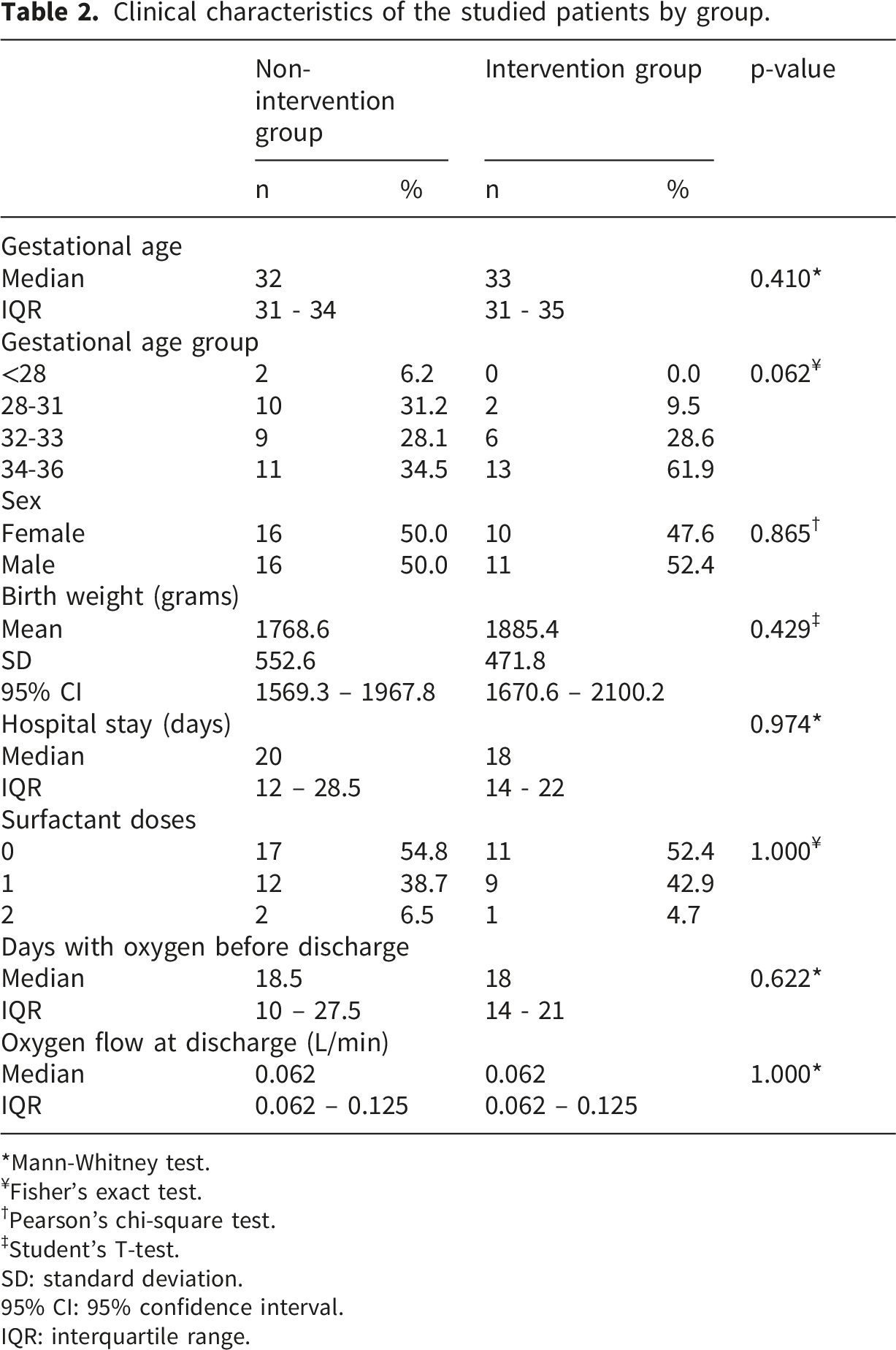
*Mann-Whitney test.
¥Fisher’s exact test.
†Pearson’s chi-square test.
‡Student’s T-test.
SD: standard deviation.
95% CI: 95% confidence interval.
IQR: interquartile range.
Outcomes by group.
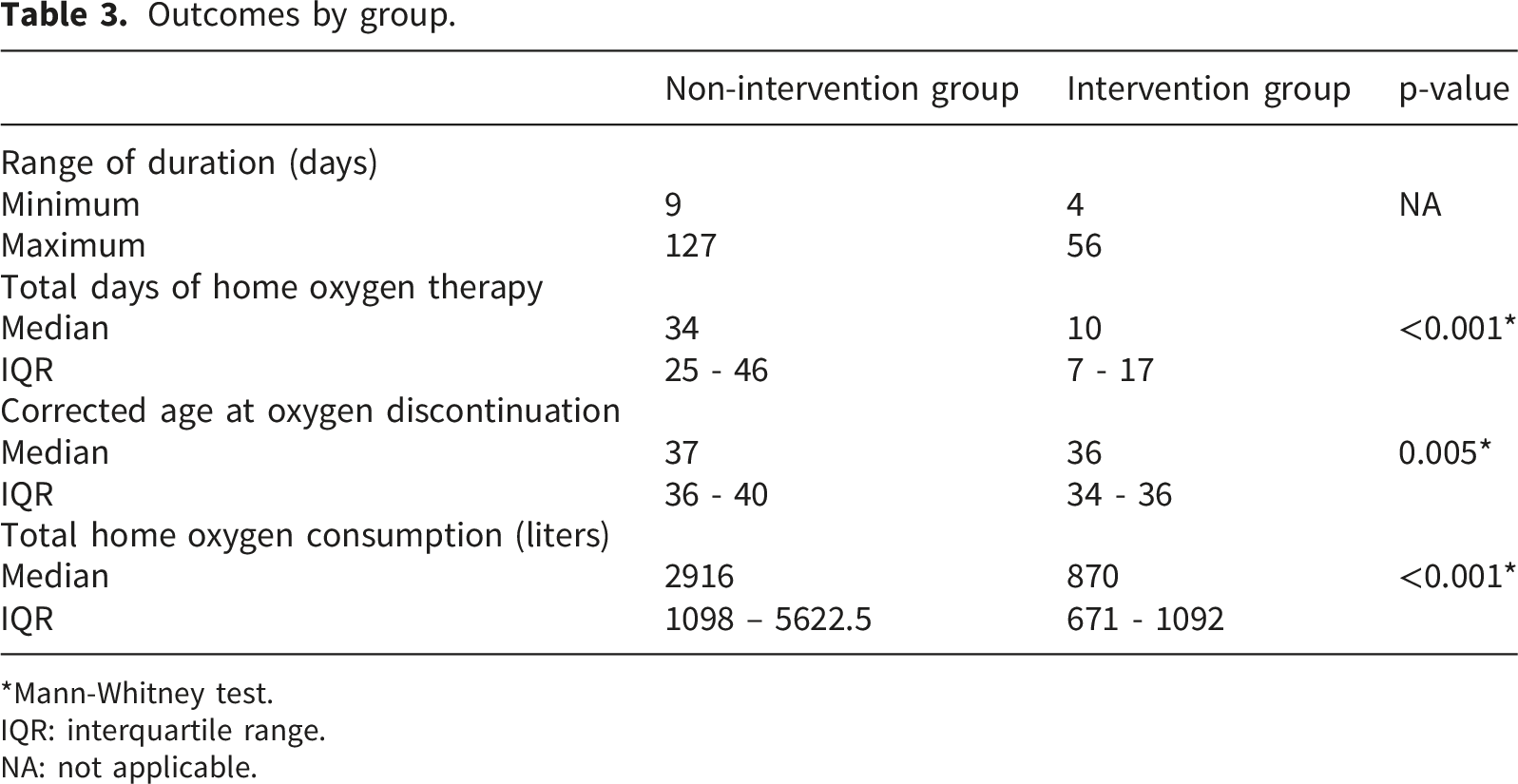
*Mann-Whitney test.
IQR: interquartile range.
NA: not applicable.
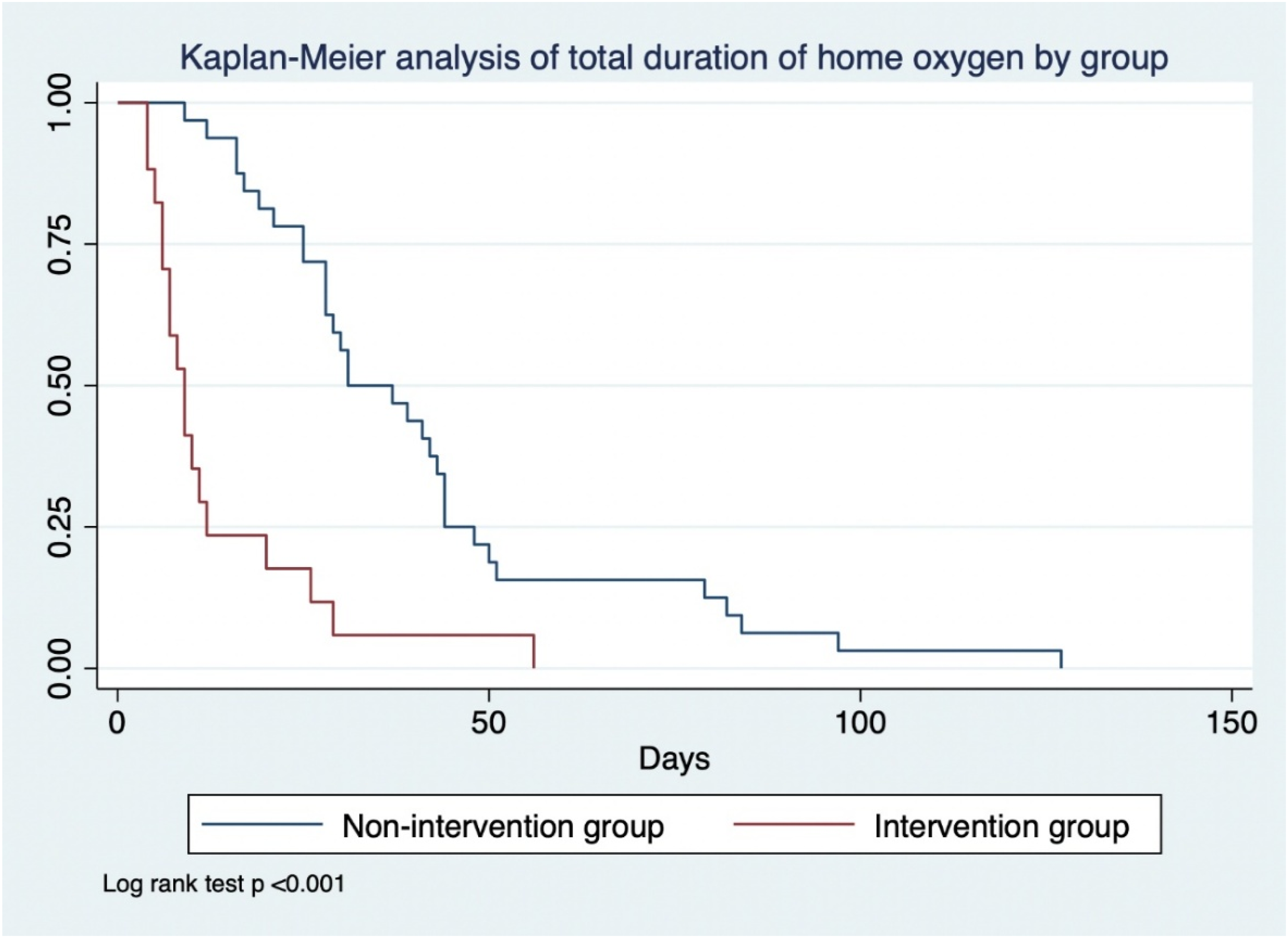
Figure 6 compares the duration of home oxygen therapy between the two groups (Mann Whitney p: <0.001), and Figure 7 shows the Kaplan-Meier curves for the duration of home oxygen therapy according to group (log-rank test p: <0.001). The hazard ratio was 4.29 (95%CI: 2.34-7.89). Total duration of domiciliary oxygen therapy. Kaplan-Meier analysis of total duration of home oxygen by group.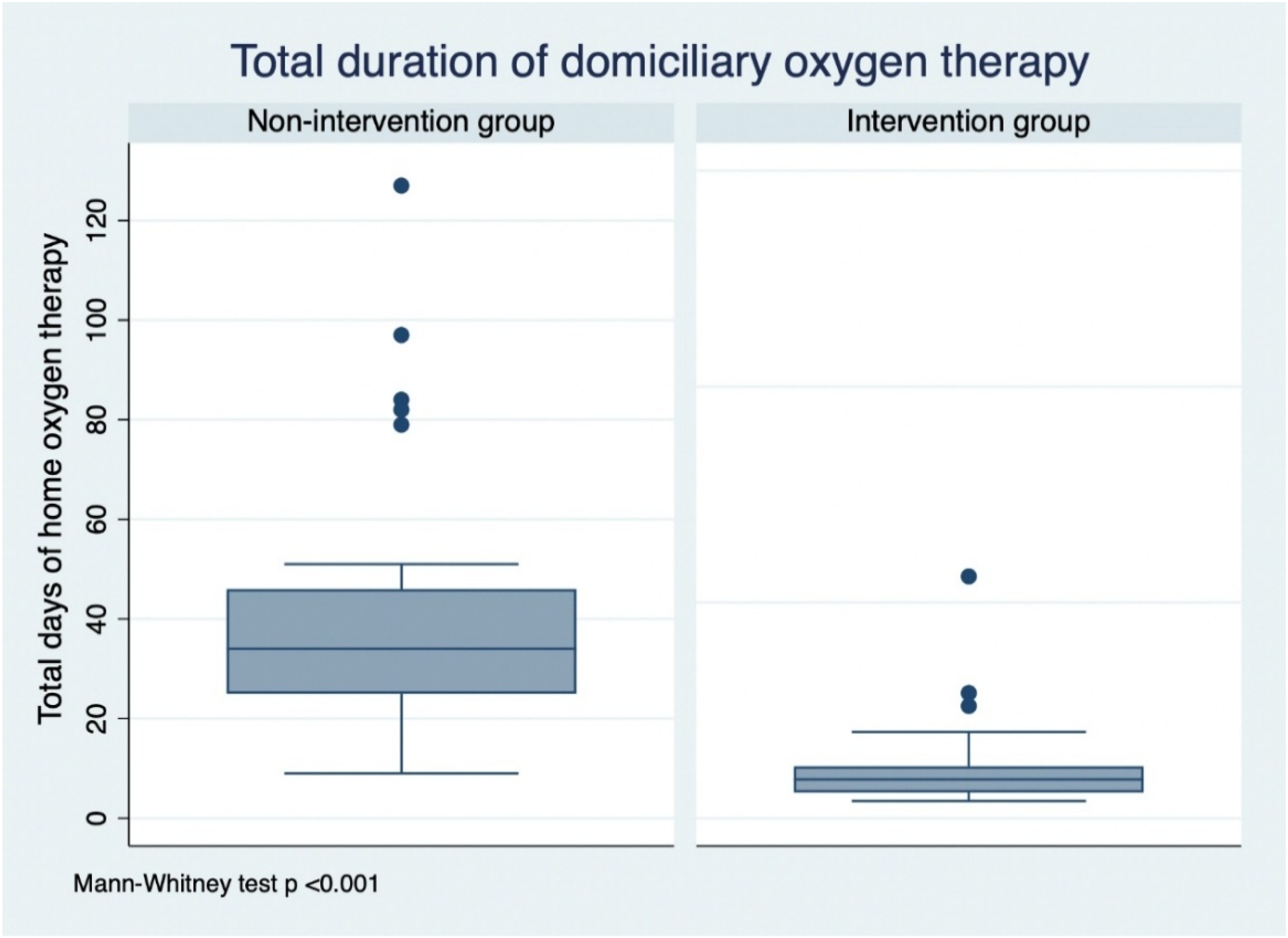
Adverse events
No adverse events or safety incidents related to device use were reported in the intervention cohort.
Discussion
This study aimed to evaluate the feasibility and clinical impact of an IoT-based teleassistance system for remote monitoring of preterm neonates on home oxygen therapy. The primary finding was a meaningful reduction in the duration of oxygen therapy in the intervention cohort, with a median of 10 days compared to an estimated 34 days in the historical control group. This reduction is clinically relevant, as it ensures that neonates receive only the duration of supplemental oxygen needed. These results reinforce our first hypothesis that continuous remote monitoring through IoT-enabled systems can improve therapy duration while supporting clinical safety and improving care efficiency.
The corrected gestational age at which home oxygen was discontinued was 36 weeks in the intervention group, in contrast to the study by Charpak and colleagues in Bogotá, 18 who found a corrected gestational age of 38.5 weeks at the time of discontinuation and an average of 101 days of supplemental oxygen from birth. Bogotá is found at 2600 meters above sea level (masl). It has been proven that at altitudes above 2100 masl, oxyhemoglobin saturation begins to decline rapidly, increasing the likelihood that preterm newborns will be discharged with home oxygen and that its duration will be longer. 16 Manizales is situated at 2130 masl, an intermediate altitude according to the World Health Organization. 19
When compared to earlier studies in similar contexts,18,20 the reduction observed in our cohort is notable. While kangaroo mother care and other structured follow-up programs have shown benefits in neonatal outcomes, their ability to promptly stop oxygen therapy is still constrained by scheduling and authorization processes inherent in traditional care models. By enabling real-time physiological data acquisition and automated alerts, our system supported timely clinical decision-making and facilitated earlier and safer discontinuation of oxygen therapy.
The present findings should also be interpreted within the broader context of telemedicine and remote patient monitoring. A growing body of evidence suggests that digital health interventions can improve access to specialized care, support continuity of care after hospital discharge, and facilitate timely clinical decision-making through the availability of real-time patient data. Telemonitoring has demonstrated benefits across multiple clinical domains, including chronic disease management, cardiovascular care, respiratory disorders, and pediatric follow-up programs. In neonatal care, however, the implementation of home-based telemonitoring systems remains comparatively limited. Our study contributes to this emerging field by demonstrating the feasibility of integrating physiological monitoring, IoT connectivity, and clinical teleassistance into a single platform for managing home oxygen therapy in preterm neonates. These findings support the growing role of digital health technologies in extending specialized neonatal care beyond the hospital setting and into the home environment.
Our results on the reduction in the duration of home oxygen therapy are consistent with those obtained by Rhein and colleagues 21 in the United States, in their controlled clinical trial evaluating whether analysis of home oximetry data compared to standard care would reduce the duration of home oxygen therapy. Patients in the control group had an average of 100.1 days with oxygen, compared to 78.1 days in the intervention group. Their study was conducted in nine academic centers at altitudes ranging from 18 to 298 meters above sea level, but with extremely preterm newborns (average 26.8 weeks) and extremely low birth weight (average 938 grams), which differs from our population (33 weeks and 1885 grams), explaining the differences in the duration of home oxygen therapy.
The mechanism underlying these results likely involves a combination of continuous monitoring, caregiver engagement through the mobile application, and the availability of accurate, real-time data for clinicians. Continuous access to oxygen saturation and other physiological parameters allowed the healthcare team to identify stabilization earlier, reducing unnecessary days on supplemental oxygen. Furthermore, integrating photoplethysmography (PPG)-based blood pressure estimation 6 within the teleassistance module provided additional hemodynamic insights, which may contribute to more comprehensive neonatal monitoring. While photoplethysmography has been widely studied in clinical and adult monitoring settings, its application in neonatal home-based monitoring stays limited. To our knowledge, few systems have integrated PPG-derived parameters into teleassistance platforms for remote monitoring of preterm neonates, highlighting the novelty of our approach in this context.
No significant differences were found about birth weight or oxygen flow at discharge, unlike the study by Yeh and colleagues, 22 who found that patients with oxygen flow >0.5 L/min at discharge had longer durations of home oxygen therapy.
A key strength of this study is the real-world implementation of a digital health solution in a resource-limited setting with challenging geographical conditions. The teleassistance module, supported by a hybrid communication infrastructure (4G/LTE, Wi-Fi, and experimental LoRaWAN), functioned reliably in most households, with 4G proving to be the most consistent communication method. This integration of IoT and mobile health technologies aligns with global trends in digital transformation of healthcare and proves the potential for scalability. Experimental LoRaWAN testing revealed significant data loss and transmission delays under real-world conditions. With a transmission interval of 10 seconds, approximately 33% of transmitted messages were successfully received, and delays of up to 160 seconds were seen. These limitations reduced its suitability for reliable real-time monitoring, leading to the prioritization of 4G and Wi-Fi connectivity.
However, several limitations should be acknowledged. First, the nonrandomized, historically controlled design introduces the potential for selection bias and confounding, making it difficult to definitively attribute the observed differences solely to the telemonitoring intervention. Although no major changes in national guidelines for home oxygen withdrawal occurred during the study period and baseline demographic and clinical characteristics were comparable between cohorts, residual confounding related to unmeasured temporal changes in clinical practice cannot be completely excluded. Second, the sample size in the intervention cohort was relatively small, and recruitment was limited to households within IoT network coverage, which may affect the generalizability of the findings. Third, long-term outcomes beyond oxygen therapy discontinuation, such as respiratory readmissions or late-onset complications, were not assessed. Finally, LoRa coverage was substantially lower than theoretical estimates due to the mountainous geography of Manizales, which restricted its practical deployment and limited its suitability for reliable real-time monitoring.
Despite these limitations, the findings have important implications for neonatal care in similar settings. The system could be integrated into national or regional health programs to support structured, technology-enabled home follow-up, potentially reducing hospital readmissions, optimizing resource use, and improving caregiver confidence. Further studies should aim to confirm these results in larger, multicenter cohorts, explore the cost-effectiveness of the intervention, and assess its integration with electronic health record systems.
Conclusion
The IoT-based teleassistance service presented in this study offers a feasible and effective approach for remotely monitoring preterm neonates receiving home oxygen therapy. The intervention was associated with a reduction in the duration of home oxygen therapy, from a median of 34 days in the historical control cohort to 10 days in the intervention group, while supporting safe and evidence-based clinical decision-making. Continuous access to real-time physiological data, combined with automated alerts, facilitated earlier identification of clinical stability and timely discontinuation of oxygen therapy. These findings suggest that teleassistance systems may improve the efficiency of neonatal follow-up programs and help reduce the risks associated with prolonged oxygen exposure in this vulnerable population.
Beyond the immediate clinical benefits observed, the proposed teleassistance approach demonstrates the potential of IoT-enabled remote monitoring to support broader digital transformation strategies in neonatal care. From a technological perspective, the platform demonstrated the feasibility of integrating physiological monitoring, cloud-based information systems, and remote communication technologies into a unified teleassistance ecosystem capable of supporting home-based neonatal care. Hybrid connectivity based on 4G/LTE and Wi-Fi provided reliable communication, whereas LoRaWAN performance was limited by the mountainous geography of the study area, highlighting the importance of context-specific connectivity strategies in digital health deployments. The scalability and adaptability of the system make it particularly relevant for low- and middle-income countries where access to specialized follow-up and continuous physiological monitoring may be limited. Future research should evaluate long-term clinical outcomes, healthcare utilization, cost-effectiveness, implementation at larger scales, and integration with routine neonatal care pathways and electronic health records. These findings support further evaluation of teleassistance technologies as a strategy to improve access, continuity of care, and clinical outcomes for vulnerable neonatal populations.
Footnotes
Acknowledgments
The authors would like to thank Universidad Nacional de Colombia – Manizales campus, Universidad Autónoma de Manizales, S.E.S Hospital Universitario de Caldas, Clínica Ospedale, and the Ministerio de Ciencia, Tecnología e Innovación for their support during the project.
Ethics considerations
The study was conducted following the Declaration of Helsinki and approved by the Bioethics Committee of the Universidad Autónoma de Manizales (approval record No. 087 of 2019). The project was classified as involving more than minimal risk due to the inclusion of a vulnerable population, by Resolution 8430 of 1993 on research involving human subjects in Colombia.
Consent to participate
Written informed consent was obtained from the parents or legal guardians of all neonates before enrollment in the study.
Author contributions
Conceptualization: Santiago Murillo-Rendón; Isabel C. Echeverri-Ocampo; Carolina Márquez-Narváez; Fernando Arango-Gómez; Belarmino Segura Giraldo; Camilo Salgado Jiménez; Oscar Julián López-Uribe. Methodology: Santiago Murillo-Rendón; Isabel C. Echeverri-Ocampo; Belarmino Segura Giraldo. Data curation: Carolina Márquez-Narváez; Fernando Arango-Gómez. Formal analysis: Santiago Murillo-Rendón; Camilo Salgado Jiménez. Writing—original draft: Santiago Murillo-Rendón; Isabel C. Echeverri-Ocampo. Writing—review and editing: All authors. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Ministerio de Ciencia, Tecnología e Innovación de Colombia (MINCIENCIAS), project No. 121984468173, “Teleasistencia para Monitoreo de Oxígeno Domiciliario en Neonatos”, under Announcement 844-2019: “Convocatoria pacto para la generación de nuevo conocimiento a través de proyectos de investigación”.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figure statement
All figures included in this manuscript are original and were created by the authors.
Use of artificial intelligence tools
The authors used artificial intelligence (AI) tools to support language editing and improvement of clarity and coherence of the manuscript. All scientific content, analysis, and conclusions were developed and confirmed by the authors.