
Abstract
Background
IoT-enabled wearable physiological sensing devices are expanding rapidly into intimate sexual health monitoring contexts, encompassing IoT-enabled sexual wellness instrumentation, sexual health wearables, and related companion technologies, generating pressing digital health governance challenges alongside substantial market growth. Despite a sixfold sector expansion reaching USD 56.8 billion by 2022, the sensing design characteristics governing user acceptance of integrated multi-sensing unit (IMSU)-enabled devices remain empirically uncharacterized, leaving device developers, clinicians, and health informatics policymakers without an evidence base for design standards or biometric data governance frameworks.
Objectives
This research identifies and prioritizes the sensing material characteristics determining anticipated user acceptance of IMSU-enabled intimate physiological health monitoring devices across three psychosocial acceptance pathways: Behavioral functional utility, Desire-based hedonic engagement, and Identity-expressive self-concept alignment.
Methods
A sequential mixed-methods design integrated factor analysis (FA; n = 289 adult participants) with analytic network process (ANP) expert evaluation (n = 30 domain specialists), organized within a theoretical framework synthesizing the Technology Acceptance Model (TAM), Unified Theory of Acceptance and Use of Technology (UTAUT), and Human Determinism Theory of Behavior (HDTB).
Results
Positive anticipated acceptance achieved the highest Standardized Comprehensive Evaluated Weight (SCEW = 0.3449), exceeding negative acceptance by 8.2%. Three sensing characteristics dominated positive acceptance: visual-aesthetic sensing integration (BLMA-STIP, 0.2447), anatomical personalization (APMA-SSC, 0.2376), and auditory-responsive physiological feedback (RPMMC-STIP, 0.2204). Identity dimension characteristics outperformed Behavioral characteristics by 31.5%. Cross-method convergence was confirmed (r = 0.68, p < .01).
Conclusions
Acceptance of IMSU-enabled wearable health devices follows identity-expressive and hedonic pathways that substantially outweigh functional utility logic, extending TAM and UTAUT in domain-specific ways with direct implications for patient-centered device design, digital health communication strategy, and consent-based biometric data governance policy.
Keywords
1. Introduction
1.1. The digital health expansion of wearable physiological Sensing Technologies
The integration of the Internet of Things (“IoT”) and cyber-physical sensing architectures into consumer health infrastructure has fundamentally shifted the operational boundaries of digital health. Continuous physiological monitoring has expanded from institutional clinical settings into the everyday personal contexts of individual users. 1 The convergence of multimodal sensing hardware, wireless data transmission, and AI-driven analytics has generated a new class of wearable digital health devices that capture, transmit, and interpret biometric data streams in real time. Their proliferation carries consequential implications for patients, clinicians, policymakers, and digital health industry stakeholders alike.
Among the least systematically examined application domains within this broader wearable health technology landscape is intimate sexual health monitoring, where multi-modal sensing is embedded within sexual wellness and companion health devices designed to capture continuous bodily data during private activity. This domain encompasses IoT-enabled sexual health instrumentation, including vibrotactile, thermal, and pressure-sensing wearables, a category previously examined in relation to sexual satisfaction, disability support, and psychosocial wellbeing.
Market analysis documents a sixfold sector expansion in this domain, 2 from approximately USD 10 billion in 2016 to USD 56.8 billion by 2022, 3 reflecting accelerating commercial innovation and growing social recognition of intimate well-being as a substantive dimension of digital health. 4 Devices in this category, referred to here as integrated multi-sensing unit (IMSU)-enabled technologies, unify sweat-component analysis, electronic soft-skin pressure sensing, oral saliva biomarker monitoring, and tear-based intraocular pressure detection within a single continuous physiological data collection architecture. AI-driven processing of these multi-modal data streams holds meaningful potential to bridge the functional gap between consumer wellness products and evidence-based digital health instrumentation. 5 At the same time, it generates biometric data governance challenges of a scale and intimacy that existing digital health policy frameworks have not yet adequately addressed.
1.2. Patient acceptability as a determinant of wearable health technology adoption
Patient and user acceptability is a recognized driver of wearable digital health technology adoption. Davis’s technology acceptance model (“TAM”) 6 established that perceived usefulness and perceived ease of use jointly account for the preponderance of variance in adoption intentions, a framework subsequently validated across telemedicine, electronic health records, and consumer wearable platforms.7,8 Venkatesh et al.’s 9 consumer-oriented extension of the unified theory of acceptance and use of technology, designated UTAUT2, reconceptualized adoption dynamics by elevating hedonic motivation, the experiential and pleasure-driven dimensions of technology engagement, to theoretical equivalence with functional utility, a reconceptualization particularly consequential for intimate health monitoring devices, where sensory and experiential qualities constitute primary rather than ancillary value propositions.
Both frameworks, however, require domain-specific extension for the cyber-physical intimate health monitoring context, where the sensing material interface simultaneously functions as the physiological data collection mechanism and the user’s primary aesthetic, tactile, and psychological encounter with the device. Research on personalized and companion technologies consistently demonstrates that users evaluate such devices not only as functional health instruments but as identity artefacts through which personal preferences, self-concept, and subjective experience are expressed and enacted. This dimension is systematically underspecified in both TAM and UTAUT2. It carries direct implications for device design standards, digital health communication strategies, and user-centered governance frameworks.
UTAUT2 introduced seven determinants of consumer technology acceptance: performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, habit, and price value. Of these, hedonic motivation, defined as the pleasure or enjoyment derived from using a technology, holds particular relevance for intimate physiological health monitoring contexts, where sensory engagement and experiential quality constitute primary rather than peripheral value propositions. This construct is therefore foregrounded in the present evaluative framework as the theoretical anchor for the Desire dimension. 10
1.3. Research gap and research contributions
Despite the intersection of user acceptability research, wearable IoT health sensing, and digital health policy, the existing literature has not produced an empirically grounded account of how specific sensing material design characteristics shape acceptance outcomes across behavioral, hedonic, and identity-expressive pathways within intimate physiological health monitoring contexts. This knowledge gap leaves device developers without user-centered design evidence, regulatory bodies without sensor-level benchmark criteria, and potential adopters without the informational foundation required for genuinely autonomous biometric privacy trade-off decisions, a tripartite deficit with direct consequences for patients, clinicians, industry stakeholders, and digital health policymakers alike.
The aim of this research is to identify and prioritize the sensing material design characteristics that govern anticipated user acceptance of IMSU-enabled intimate physiological health monitoring devices, and to determine the relative contribution of behavioral, hedonic, and identity-expressive acceptance pathways to overall adoption orientation, using a sequential FA–ANP mixed-methods design within an integrated TAM, UTAUT2, and HDTB evaluative framework. Three theoretical frameworks are integrated to construct the evaluative architecture of this research. First, HDTB provides the dimensional structure, partitioning user responses into three constitutive dimensions: Behavioral (functional engagement), Desire (affective and hedonic engagement), and Identity (self-concept expression). 11 Second, TAM supplies the functional adoption mechanisms mapped onto the Behavioral dimension, specifically perceived usefulness and perceived ease of use. Third, UTAUT2 supplies the hedonic motivation construct mapped onto the Desire dimension. The Identity dimension extends beyond existing TAM and UTAUT2 formulations, operationalizing the self-concept pathway through which users evaluate intimate devices as identity artefacts. This three-dimensional integration is elaborated in the Literature Review that follows.
This research addresses that gap through a sequential mixed-methods design combining factor analysis (FA; 289 participants) with analytic network process (“ANP”) expert evaluation (30 domain specialists), organized within an integrated theoretical framework extending TAM, 6 UTAUT2, 9 and human determinism theory of behavior (“HDTB”) 12 across three empirically operationalized dimensions: Behavioral (functional sensing utility), Desire (hedonic and sensory engagement), and Identity (aesthetic personalization and self-expressive alignment). Given that the vast majority of participants (96.19%) had no prior awareness or direct experience of IMSU-enabled devices at the time of data collection, the present investigation is explicitly positioned within an anticipated acceptance framework. All findings reflect prospective evaluative orientations toward novel sensing material characteristics rather than post-adoption assessments derived from sustained device use. This distinction is theoretically consequential for interpreting the FA–ANP outputs and is revisited in the limitations section.
The research makes three contributions to digital health scholarship and practice: (1) the first validated sensing material acceptance framework for integrated multi-sensing units (“IMSU”)-enabled wearable health devices, providing an evidence base for design standardization 13 ; (2) identification of Identity and Desire dimension features as the dominant positive acceptance determinants, a finding that diverges substantively from TAM-established functional utility norms and carries direct implications for digital health communication and device development strategy 12 ; and (3) theoretically grounded evidence that acceptance in cyber-physical intimate health monitoring contexts follows psychosocial pathways, with material consequences for biometric data governance policy and user autonomy in digital health contexts. 14
2. Literature Review
2.1. Theoretical framework: integrating TAM, UTAUT2, and HDTB into a unified evaluative architecture
Constructing an empirically grounded evaluation framework for intimate physiological health sensing devices requires synthesizing two complementary theoretical lineages. The first lineage furnishes the dimensional architecture: the HDTB,
12
which partitions human experiential responses into three constitutive dimensions, Behavioral, Desire, and Identity, capturing, respectively, how individuals functionally engage with, are affectively drawn toward, and articulate their self-concept through technology encounters. The second lineage furnishes the adoption mechanisms through which each dimension acquires acceptance-relevant meaning: TAM
6
and its consumer-oriented extension, UTAUT2.
9
This theoretical integration is not merely additive but structurally generative: each HDTB dimension maps onto distinct and empirically validated TAM/UTAUT2 constructs, enabling the framework to translate abstract psychological dimensions into measurable acceptance pathways with direct design and governance implications (Figure 1).
15
The main triadic reciprocal relationships of the research concept.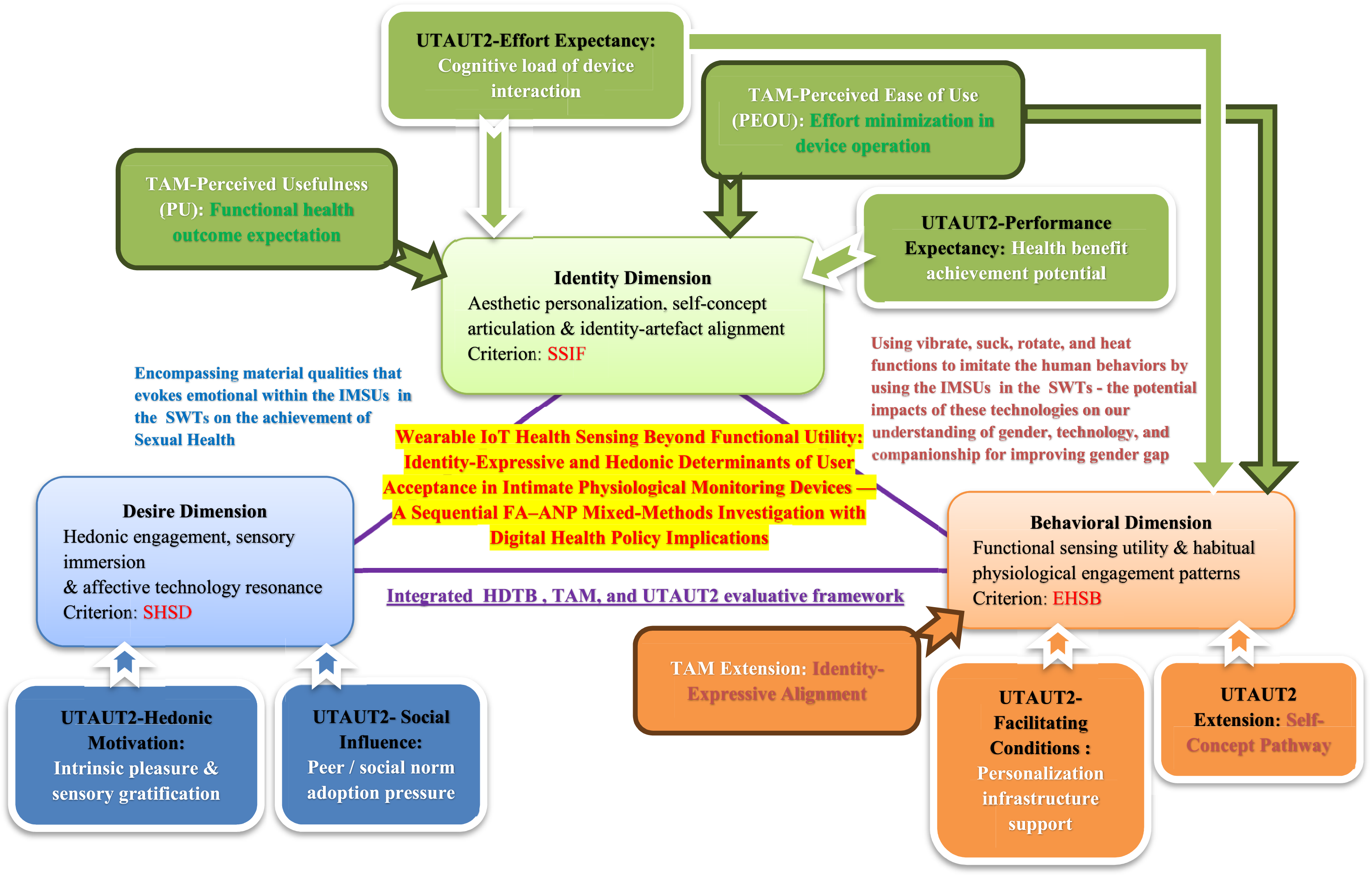
Behavioral dimension: TAM’s perceived usefulness and perceived ease of use integrate into UTAUT2’s performance expectancy and effort expectancy. TAM’s foundational proposition that adoption is driven by users’ cognitive assessments of whether a technology improves task outcomes (perceived usefulness) and whether it demands disproportionate cognitive effort (perceived ease of use), 6 finds its HDTB analog in the Behavioral dimension, which indexes the degree to which sensing material functions facilitate embodied physiological interaction and health-monitoring utility. UTAUT2 further refines this mapping: performance expectancy, the degree to which a technology helps users attain desired health outcomes, directly operationalizes the functional utility pathway, while effort expectancy, the cognitive load associated with device operation, captures the ease-of-use component. 16 Together, these four TAM/UTAUT2 constructs specify the functional adoption logic that the Behavioral dimension operationalizes for intimate physiological health sensing contexts.17,18
Desire dimension: hedonic motivation (UTAUT2). In reconceptualizing technology adoption for consumer contexts, Venkatesh et al.’s 9 elevated the experiential and enjoyment-driven dimension of device engagement, designated hedonic motivation, to theoretical equivalence with task performance utility, a repositioning that carries particular weight for intimate health monitoring contexts where sensory immersion and perceived realism function as primary rather than secondary value propositions. 19 This construct maps directly onto the HDTB Desire dimension, which captures the affective, sensory, and emotionally resonant qualities through which devices engage users beyond functional performance. Within this domain, hedonic motivation is theoretically expected to constitute a more decisive acceptance determinant than in organizational computing contexts, 10 a hypothesis the present empirical design is positioned to directly test.
Identity Dimension: Identity-Expressive Alignment (TAM/UTAUT2 Extension). Neither TAM nor UTAUT2, in their original formulations, incorporates an explicit mechanism for the self-concept pathway through which users evaluate technologies as extensions of personal identity. Research on personalized and companion technologies consistently demonstrates that intimate devices are evaluated not solely as functional instruments but as identity artefacts through which aesthetic sensibility, personal preference, and self-concept are enacted.11,13 The Identity dimension operationalizes this pathway, which the present framework positions as a third theoretically distinct adoption driver supplementing the TAM and UTAUT2 constructs and one potentially dominant in intimate health monitoring contexts where device form constitutes the primary aesthetic and psychological self-encounter. 15
The resulting integrated HDTB, TAM, and UTAUT2 evaluative architecture is illustrated in Figure 1.
2.2. Operationalization: Sensing material criteria and sub-criteria
The criteria defined by reviewing relevant literature.
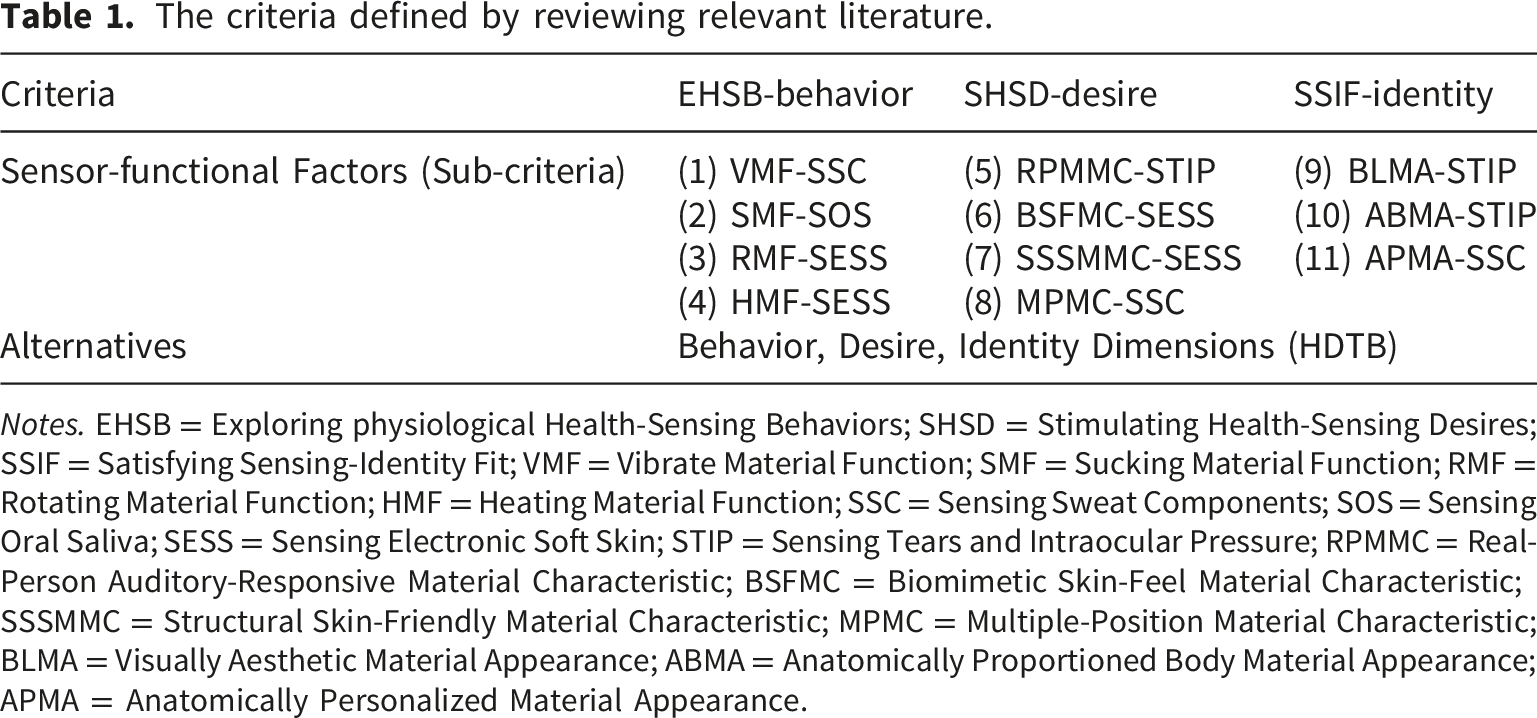
Notes. EHSB = Exploring physiological Health-Sensing Behaviors; SHSD = Stimulating Health-Sensing Desires; SSIF = Satisfying Sensing-Identity Fit; VMF = Vibrate Material Function; SMF = Sucking Material Function; RMF = Rotating Material Function; HMF = Heating Material Function; SSC = Sensing Sweat Components; SOS = Sensing Oral Saliva; SESS = Sensing Electronic Soft Skin; STIP = Sensing Tears and Intraocular Pressure; RPMMC = Real-Person Auditory-Responsive Material Characteristic; BSFMC = Biomimetic Skin-Feel Material Characteristic; SSSMMC = Structural Skin-Friendly Material Characteristic; MPMC = Multiple-Position Material Characteristic; BLMA = Visually Aesthetic Material Appearance; ABMA = Anatomically Proportioned Body Material Appearance; APMA = Anatomically Personalized Material Appearance.
Behavioral dimension (EHSB): four sensing material functions constitute this dimension. The vibrate material function (“VMF”) 24 operates through sweat-component sensing (“SSC”), transducing biochemical signals into tactile feedback; the sucking material function (“SMF”) 25 operates through oral saliva sensing (“SOS”), enabling oral biomarker acquisition; the rotating material function (“RMF”) 26 operates through electronic soft-skin sensing (“SESS”), integrating mechanical actuation with dermal conductance monitoring; and the heating material function (“HMF”) 27 similarly employs SESS technology to deliver thermal stimulation paired with skin-surface sensing. Collectively, these functions constitute the tactile, thermal, and mechanical interface through which users form habitual engagement patterns and arrive at TAM-aligned assessments of physiological utility and ease of use.
Desire dimension (SHSD): four sensing material characteristics address the hedonic and emotionally resonant facets of device engagement. The real-person auditory-responsive material characteristic (“RPMMC”) 28 employs tear and intraocular pressure sensing (“STIP”) to generate dynamic auditory feedback contingent on real-time physiological signals; the biomimetic skin-feel material characteristic (“BSFMC”) 29 uses SESS technology to approximate dermal tactile realism; the structural skin-friendly material characteristic (“SSSMMC”) similarly draws on SESS technology to deliver anatomical comfort and postural adaptability and the multiple-position material characteristic (“MPMC”) 30 employs SSC technology to accommodate postural variability. Collectively, these characteristics converge on perceived sensory immersion and biomimetic realism; precisely the hedonic motivation constructs that UTAUT2 identifies as disproportionately influential in consumer health technology adoption.
Identity dimension (SSIF): three sensing material appearances define this dimension. The visually aesthetic material appearance (“BLMA”) 31 and anatomically proportioned body appearance (“ABMA”) both employ STIP technology to achieve visually integrated aesthetic coherence; the anatomically personalized material appearance (“APMA”) 32 employs SSC technology to enable individualized physiological interface customization. By aligning device form with user self-concept, these characteristics activate the identity-expressive acceptance pathway that distinguishes intimate physiological health sensing evaluation from general-purpose wearable health technology assessment, a distinction theoretically consequential for device design standards, digital health communication strategy, and privacy-sensitive governance frameworks applicable to biometric data generated outside clinical oversight. 33
Figure 1 illustrates how this integrated framework connects TAM, UTAUT2, and HDTB theoretical constructs through evaluative criteria to specific sensing material sub-criteria, linking design-level decisions to the distinct psychological mechanisms through which they acquire acceptance-relevant meaning across functional performance, hedonic engagement, and identity-expressive pathways. 34
3. Research design
This section describes the methods employed to achieve the research aim stated in Section 1.3: identifying and prioritizing the sensing material characteristics governing anticipated user acceptance of IMSU-enabled intimate physiological health monitoring devices across Behavioral, Desire, and Identity acceptance pathways.
3.1. Sequential mixed-methods research architecture
This research adopts a sequential mixed-methods architecture integrating two analytically distinct phases, large-scale quantitative survey assessment and expert-weighted qualitative evaluation, to address dual research objectives: isolating the latent constructs governing user evaluations of sensing material characteristics, and establishing hierarchical priority relationships among those characteristics for anticipated digital health technology acceptance. Quantitative data from 289 survey participants and qualitative judgments from 30 domain experts are treated as complementary evidence streams, with each phase informing the interpretive structure of the other across the Behavioral, Desire, and Identity analytical dimensions of the integrated HDTB, TAM, and UTAUT2 framework.
First process — quantitative analysis FA approach: FA approach serves as the primary data-reduction instrument, isolating latent constructs accounting for covariation patterns among eleven sensing material characteristics distributed across three HDTB evaluation criteria (EHSB, SHSD, SSIF). By distilling correlated observed variables into theoretically coherent factors, FA generates communality estimates quantifying how completely each characteristic is captured within the extracted factor solution, providing empirically weighted inputs that anchor the expert evaluation phase. 35
Second process — qualitative analysis ANP method: ANP method, an extension of the Analytic Hierarchy Process (AHP) that explicitly models feedback and interdependency among criteria rather than assuming hierarchical independence, 31 receives FA-derived communality weights as structured inputs and subjects them to systematic pairwise comparison by domain experts. This yields priority weights reflecting each sensing characteristic’s relative contribution to acceptance outcomes, with consistency ratio (“C.R.”) and consistency index (“C.I.”) values below 0.10 confirming the logical coherence of expert judgments. 36
Third process — integration and triangulation: the sequential FA–ANP connection achieves methodological triangulation by subjecting the same phenomena to structurally distinct analytical logics, statistical dimension reduction and expert-weighted decision modeling. and quantifying the degree of output convergence.
37
Divergence between FA-derived communalities and ANP-derived priority weights would indicate method-dependent artifact; convergence signals stable, replicable acceptance indicators warranting theoretical interpretation and evidence-based policy inference. Figure 2 maps the complete data flow from instrument administration through both analytical phases to final acceptance evaluation.
38
Main research design and steps.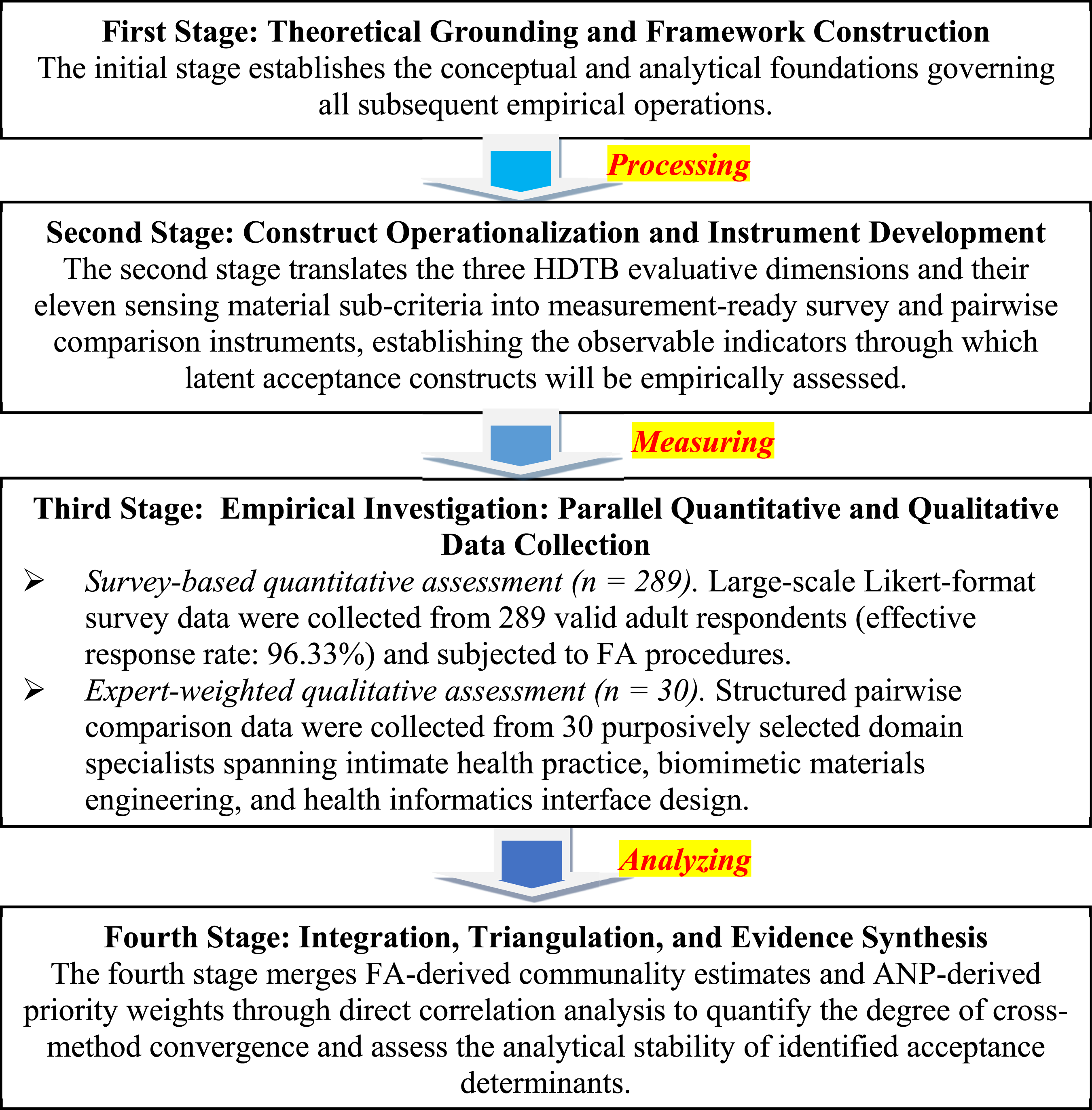
3.2. Research steps
This research adopts a sequential mixed-methods design that integrates quantitative FA with qualitative ANP evaluation to systematically investigate how sensing material characteristics of IMSU-enabled intimate physiological health monitoring devices govern anticipated user acceptance across three theoretically grounded evaluative dimensions: Behavioral functional utility, Desire-based hedonic engagement, and Identity-expressive self-concept alignment. The investigation proceeds through four methodologically distinct yet analytically interdependent stages, the structure of which is depicted in Figure 2.
First Stage — Theoretical Grounding and Framework Construction: the initial stage establishes the conceptual and analytical foundations governing all subsequent empirical operations. Two parallel tasks are executed. First, the integrated HDTB, TAM, and UTAUT2 evaluative architecture is constructed by mapping TAM’s perceived usefulness and perceived ease of use constructs onto the Behavioral dimension; UTAUT2’s hedonic motivation construct onto the Desire dimension; and the identity-expressive alignment mechanism, a theoretical extension introduced in this research, onto the Identity dimension.
This mapping transforms abstract psychological constructs into operationalizable evaluative criteria (EHSB, SHSD, SSIF) capable of anchoring both the large-scale participant survey and the expert pairwise comparison instrument. Second, the statistical and decision-analytic methodologies are selected and justified relative to research objectives: FA approach is designated as the quantitative data-reduction instrument for isolating latent constructs from large-scale survey covariance structure, and ANP model is designated as the qualitative priority-weighting instrument for modeling non-hierarchical interdependency relationships among acceptance criteria, a selection justified by the demonstrated unsuitability of strictly hierarchical AHP mode structures for acceptance contexts involving cross-dimensional feedback effects. 39
Stage 2 — Construct Operationalization and Instrument Development: the second stage translates the three HDTB evaluative dimensions and their eleven sensing material sub-criteria into measurement-ready survey and pairwise comparison instruments, establishing the observable indicators through which latent acceptance constructs will be empirically assessed. For the large-scale participant instrument, eleven Likert-scaled items are constructed, one per sensing material characteristic, each item anchored to its designated evaluative dimension (EHSB, SHSD, or SSIF) and its specific sensing technology (SSC, SOS, SESS, or STIP). Item wording is deliberately calibrated to elicit evaluative judgments of perceived importance within the intimate physiological health sensing context, rather than general attitudinal endorsement, in order to generate dimensional scores directly comparable across the Behavioral, Desire, and Identity acceptance pathways. For the expert ANP instrument, pairwise comparison items are constructed at two hierarchical levels: dimension-level comparisons (e.g., EHSB versus SHSD) and sub-criteria-level comparisons within each dimension. 40
New measurement items were constructed rather than adopting existing validated instruments for two reasons. First, no previously validated instrument addresses the specific sensing material characteristics of IMSU-enabled devices across the three HDTB dimensions operationalized in this research. Second, the intimate physiological health monitoring context introduces domain-specific constructs, including anatomical personalization, biomimetic skin-feel, and auditory-responsive physiological feedback, that have no direct equivalents in existing TAM or UTAUT-based wearable health technology scales. Item wording was therefore developed from the theoretical framework and reviewed by the expert panel prior to full-scale administration to ensure face validity and content validity within this novel domain.
Stage 3 — Empirical Investigation: Parallel Quantitative and Qualitative Data Collection: the third stage executes the dual empirical assessment through two simultaneously structured but analytically independent data collection procedures. Data collection was conducted through in-person administration in private interview settings between February and December 2025. The extended collection period accommodated purposive regional sampling across all four geographic zones of Taiwan (northern, central, southern, and eastern) and facilitated thorough expert panel scheduling across three disciplinary cohorts. Survey-based quantitative assessment (289 participants): large-scale Likert-format survey data were collected from 289 valid adult respondents (effective response rate: 96.33%) and subjected to FA procedures. Sampling adequacy was verified through KMO testing (threshold: ≥ 0.6) and Bartlett’s Test of Sphericity (threshold: p < .001) prior to factor extraction. Communality estimates were computed for all eleven sensing material sub-criteria to quantify the degree to which each characteristic is captured within the extracted latent factor solution, providing both construct validity evidence for the HDTB dimensional architecture and empirically weighted inputs for subsequent ANP model integration. Construct validity was further evaluated through factor loading magnitudes and the structural coherence of the three-dimensional solution relative to the theoretical HDTB, TAM, and UTAUT2 framework.
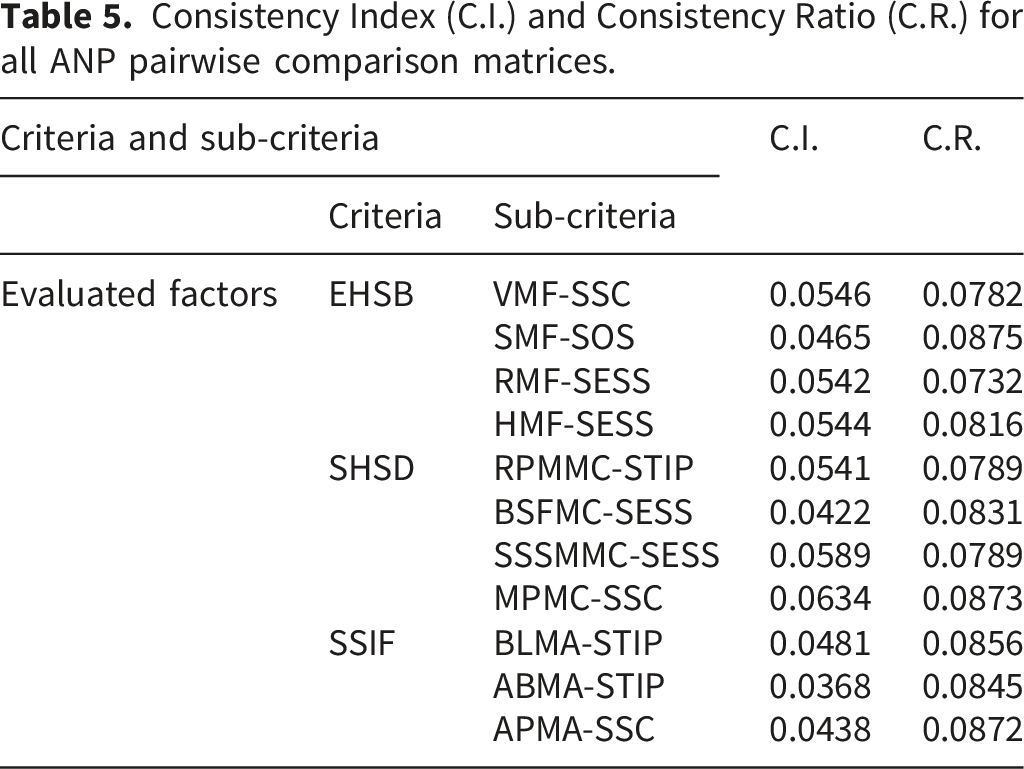
Additionally, expert-weighted qualitative assessment (30 experts): structured pairwise comparison data were collected from 30 purposively selected domain specialists spanning intimate health practice, biomimetic materials engineering, and health informatics interface design. ANP priority weights were derived for all eleven sensing material characteristics across three acceptance outcome categories (NAI-SH, NeuAI-SH, PAI-SH), with FA-derived communalities embedded as weighted inputs within the ANP supermatrix structure to achieve systematic cross-method integration. Judgment consistency was verified through Consistency Index (C.I.) and Consistency Ratio (C.R.) computation for each pairwise comparison matrix, with C.R. < 0.10 constituting the acceptance threshold for all matrices. Expert panels yielding mean C.R. values substantially below this threshold, with no individual matrix requiring revision, satisfy the reliability standard for ANP priority weight interpretation. 41
Stage 4 — Integration, Triangulation, and Evidence Synthesis: the fourth stage merges FA-derived communality estimates and ANP-derived priority weights through direct correlation analysis to quantify the degree of cross-method convergence and assess the analytical stability of identified acceptance determinants. A Pearson correlation coefficient between FA communalities and ANP priority weights at or above r = 0.6 constitutes a moderate-to-large convergence signal, indicating that the acceptance rankings generated by statistically emergent user preference patterns and independently derived expert judgments are mutually reinforcing rather than method-dependent artifacts. 42
Convergence at this level supports three integrated inferential outputs: (i) standardized comprehensive evaluated weights (“SCEW”) for the three acceptance outcome categories, quantifying the aggregate directional orientation of the participant sample toward positive, neutral, or negative adoption; (ii) ranked dimensional profiles for Behavioral, Desire, and Identity acceptance pathways, establishing the relative primacy of identity-expressive and hedonic versus functional utility drivers in this domain; and (iii) evidence-based design priorities and digital health governance recommendations synthesized from the method-triangulated acceptance signals, outputs directly actionable for IMSU device developers, health informatics policymakers, clinicians, and regulatory bodies engaged with IoT intimate physiological health monitoring technologies. Figure 2 depicts the complete four-stage research architecture and inter-stage data flow. 43
3.3. Statistical methods
The analytical strategy of this research proceeds in two sequentially integrated phases. In the first phase, FA approach is applied to large-scale survey data (289 participants) to identify the latent dimensional structure underlying participants’ evaluations of eleven sensing material characteristics, yielding communality estimates that quantify the degree to which each characteristic is captured within the three-factor HDTB solution. In the second phase, ANP modeling is applied to structured expert pairwise comparison data (30 experts) to derive interdependency-adjusted priority weights for each characteristic relative to three acceptance outcome categories. FA-derived communalities are embedded as weighted inputs within the ANP model supermatrix, enabling systematic cross-method integration. Triangulation is assessed through Pearson correlation between FA approach communalities and ANP model priority weights, with convergence at r ≥ 0.60 supporting integrated interpretation of the combined outputs.
3.3.1. Measurement instrument: Five-point Likert scale
Attitudinally, the graduated five-point response continuum enables participants to express differentiated perceptions of sensing material importance, a measurement requirement that binary categorical formats cannot satisfy without systematic loss of inter-criterion discriminability. 44 Statistically, Likert-structured responses generate interval-approximating ordinal data that satisfy the input assumptions of the FA and ANP analytical procedures constituting the core of this research’s mixed-methods architecture, while simultaneously producing standardized item scores that are directly comparable across all 289 participant responses and 11 sensing material characteristics without instrument-specific recalibration.45,46 Practically, the structured response format substantially reduces the response burden and interpretive variability associated with open-ended qualitative items, a consideration directly relevant to a survey instrument administered across four geographic regions of Taiwan through face-to-face interview protocols requiring participant and researcher time efficiency.
3.3.2. Quantitative phase: Factor analysis (FA)
FA approach serves as the primary data-reduction instrument in the quantitative phase, isolating the latent constructs that account for covariation patterns among the eleven sensing material sub-criteria distributed across the three HDTB evaluation dimensions. The FA approach is appropriate for this purpose because high factor loadings and communality values provide direct empirical evidence that observed items accurately represent their designated theoretical constructs, contributing to both construct validity and the empirical coherence of the HDTB, TAM, and UTAUT2 integrated framework.
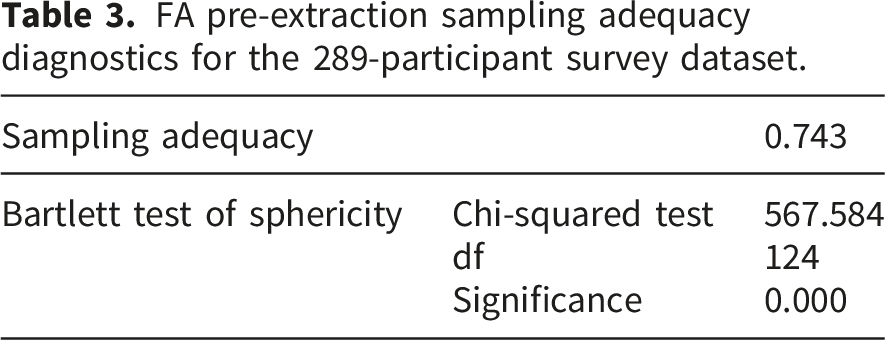
Sampling adequacy: Kaiser-Meyer-Olkin (“KMO”) test. Before extracting factors, the KMO statistic was computed to assess whether the inter-variable correlation matrix is suitable for factor analysis. The KMO index ranges from 0 to 1; values approaching 1 indicate that the pattern of correlations is sufficiently compact and that shared variance among variables derives substantially from underlying common factors rather than unique or error variance, rendering FA both appropriate and likely to yield stable factor solutions. Following established interpretive conventions, KMO values in the 0.70–0.79 range are considered adequate; values of 0.80 and above indicate meritorious suitability. Values below 0.6 indicate that the variable set is insufficiently intercorrelated to support meaningful factor extraction and requires reconceptualization before FA is attempted.
Inter-variable correlation structure: Bartlett’s Test of Sphericity (“BTS”) 47 complements the KMO measure by providing a formal statistical test of whether the observed correlation matrix departs significantly from an identity structure, that is, whether any meaningful inter-variable relationships exist beyond chance-level covariation. A statistically significant result (p < .001, as adopted in this research given the sample size of 289 participants) confirms sufficient inter-variable correlation to support factor extraction and justifies proceeding to communality estimation. Importantly, BTS significance establishes a necessary rather than sufficient condition for FA approach appropriateness; its interpretation must be integrated with KMO adequacy values and the theoretical coherence of the extracted factor solution to constitute a complete pre-extraction validity assessment. In this research, a significance threshold of p < .001 was adopted, consistent with the large sample size (289 participants) and the multivariate nature of the HDTB evaluative framework.
Communality estimation and construct representation. Following factor extraction, communality values were computed for each of the eleven sensing material sub-criteria. Communality quantifies the proportion of each observed variable’s total variance explained by the extracted factor solution; that is, how completely each sensing characteristic is captured within the latent dimensional structure of the HDTB framework. All communality values exceeding 0.50 are regarded as acceptable, indicating that the factor solution accounts for the majority of each variable’s variance; values approaching or exceeding 0.7 indicate strong latent construct representation. 48 Uniform elevation of communalities across all eleven characteristics would confirm that no sensing sub-criterion is systematically underrepresented within the Behavioral, Desire, or Identity dimensional architecture, providing a reliable empirical foundation for the subsequent ANP priority-weighting phase. The statistical relationships governing FA extraction are expressed in Equations (1), (2) and (3) (Appendix B-1 and B-2).49,50
3.3.3. Qualitative phase: Analytic network process (ANP)
Following quantitative FA, the ANP serves as the qualitative priority-weighting instrument, translating FA-derived communality estimates into hierarchically structured, expert-validated acceptance weights for each of the eleven sensing material characteristics relative to the three acceptance outcome categories: NAI-SH, NeuAI-SH, and PAI-SH. The ANP was selected over the conventional Analytic Hierarchy Process (AHP) 39 on grounds directly pertinent to this research’s analytical requirements: where AHP assumes strict top-down hierarchical independence among decision criteria, ANP explicitly models feedback and interdependency relationships among criteria within and across levels, a structural necessity when evaluating acceptance determinants whose influence pathways are mutually reinforcing across Behavioral, Desire, and Identity dimensions rather than strictly sequential.
Pairwise comparison matrix construction: expert evaluations were structured through systematic pairwise comparisons within a matrix architecture, where each element aij represents the relative importance ratio of criterion i over criterion j, expressed as the weight ratio Wi/Wj. Three structural constraints govern the matrix: diagonal elements equal unity (aij= 1), reciprocal symmetry holds throughout (aij× aij= 1), and all off-diagonal elements are strictly positive. Priority vectors, the eigenvectors representing each criterion’s relative importance weight, are derived through the vector quantities method (AW= nW) in conjunction with the maximum eigenvalue principle (Rw= λ_max), yielding the relative priority weight vector W= [W1, …, Wj, …, W n ] for all evaluated sensing characteristics. The complete pairwise comparison matrix formulation, priority vector derivation, and consistency verification procedures are expressed formally in Equations (4)–(6) respectively (Appendix C-1 and C-2).41,42
Consistency verification: the logical coherence of expert pairwise judgments was assessed through a two-stage consistency algorithm producing two complementary diagnostics. The Consistency Index (“C.I.”) quantifies the degree of transitivity violation in expert judgments by relating the maximum eigenvalue (λ_max) to matrix dimension n, while the Consistency Ratio (“C.R.”) normalizes C.I. against the Random Index (“R.I.”), the expected C.I. value for a randomly generated matrix of equivalent dimension, yielding a scale-invariant coherence indicator interpretable across matrices of different sizes. 43 The threshold C.R. < 0.10 is the universally adopted acceptance criterion in ANP applications: matrices satisfying this threshold demonstrate internally coherent expert judgments in which transitivity is substantially preserved; matrices exceeding it indicate excessive judgment inconsistency and require expert re-evaluation before their priority weights can be treated as analytically credible. A mean C.R. substantially below 0.1 across all pairwise comparison matrices, with no individual matrix requiring revision, constitutes the reliability benchmark for the expert evaluation phase of this research. 51
FA–ANP integration architecture: rather than treating FA and ANP as sequential but analytically independent procedures, this research embeds FA-derived communality values as weighted criteria inputs within the ANP supermatrix structure, enabling each sensing characteristic’s priority weight to reflect both its statistically demonstrated latent construct representation, quantified through communality, and the expert-assessed relative importance of that construct within the broader acceptance hierarchy. This integration architecture ensures that ANP priority weights are empirically anchored rather than relying exclusively on expert judgment, and that FA communalities acquire acceptance-category-specific interpretive significance rather than remaining context-neutral statistical descriptors. SCEW values represent the standardized aggregate priority weight per acceptance category across all eleven sensing characteristics, computed as the normalized sum of ANP priority scores within each acceptance alternative column, and therefore sum to unity, reflecting the proportional distribution of anticipated acceptance orientations across negative, neutral, and positive adoption categories. 52
3.3.4. Methodological integration: FA–ANP triangulation
The sequential integration of FA and ANP achieves methodological triangulation by subjecting equivalent evaluative phenomena, user and expert assessments of the same eleven sensing material characteristics, to two structurally distinct analytical logics operating on different data sources, thereby enabling empirical assessment of whether identified acceptance signals are stable across methods or contingent on any single analytical procedure.
Triangulation rationale and validity logic: FA approach operates on large-scale survey covariance structure (289 participants), extracting latent dimensions from patterns of inter-variable correlation through a statistical procedure that is entirely data-driven and independent of any individual judgment. ANP, by contrast, operates on systematically elicited expert pairwise comparisons (30 experts), deriving priority weights through a judgment-aggregation procedure that is explicitly value-laden and discipline-informed. The two procedures therefore represent not merely different methods but epistemically distinct approaches to the same evaluative question, making their convergence or divergence a theoretically meaningful validity signal rather than a methodological redundancy. Convergence between FA-derived communalities and ANP-derived priority weights indicates that acceptance signals are stable across both data-driven statistical inference and expert-weighted decision modeling, warranting confidence that they reflect genuine and replicable user evaluative orientations rather than instrument-specific response tendencies or analytical artifacts of any single phase. 48
Cross-method convergence quantification: convergence between FA communalities and ANP priority weights is quantified through Pearson correlation analysis applied to the paired values for all eleven sensing material characteristics. A correlation coefficient at or above r = 0.60 constitutes a moderate-to-large convergence signal, consistent with established benchmarks for mixed-methods triangulation in health technology acceptance research, and sufficient to support the theoretical inferences drawn from integrated FA–ANP outputs. 37 Divergence below this threshold would indicate method-dependent artifact, requiring separate interpretation of FA and ANP outputs rather than integrated synthesis.
Convergence at or above the threshold supports three integrated inferential products: (i) Standardized Comprehensive Evaluated Weights (SCEW) for the three acceptance outcome categories, quantifying the aggregate directional orientation of the combined participant and expert sample toward positive, neutral, or negative adoption; (ii) ranked dimensional profiles for the Behavioral, Desire, and Identity acceptance pathways, establishing the relative primacy of psychosocial versus functional utility drivers in this domain; and (iii) method-triangulated evidence-based design priorities and digital health governance recommendations directly actionable for IMSU device developers, health informatics policymakers, clinicians, and regulatory bodies.
Internal validity evidence: the cross-method triangulation architecture serves a second validity function beyond convergence testing: it guards against the most consequential threats to internal validity in this research context. Social desirability bias, the tendency of participants in sensitive health technology contexts to misrepresent their evaluative orientations, would produce divergent FA and ANP outputs if present, because survey respondents and expert panelists are subject to structurally different social pressures and respond through entirely different instrument formats. The correspondence between FA communality structure and ANP priority weights therefore constitutes evidence not only of method stability but of freedom from the systematic response distortion that sensitive-topic acceptance research is particularly susceptible to generating.37,44 The complete FA–ANP integration architecture, data flow, and convergence assessment procedure are depicted in Figure 2.
3.4. Participant recruitment, ethical procedures, and data collection
3.4.1. General participant recruitment and sample characteristics
General participant sample: a total of 300 adults were recruited through purposive sampling across Taiwan. Following exclusion of 11 invalid responses (8 lacking documented informed consent; 3 substantially incomplete), 289 valid questionnaires were retained (effective response rate: 96.33%). Inclusion criteria were: aged 18 years or older, capacity to comprehend the questionnaire instructions, and voluntary provision of informed consent. Exclusion criteria were: age below 18 years, inability to comprehend the questionnaire content, refusal to confirm informed consent, and substantially incomplete questionnaire responses. The sample comprised 157 males (54.05%) and 132 females (45.95%), drawn from four geographic regions: central Taiwan (n = 96, 33.21%), northern Taiwan (n = 93, 32.17%), southern Taiwan (n = 91, 31.51%), and eastern Taiwan (n = 9, 3.11%).
The descriptive statistics of the questionnaire survey responses.
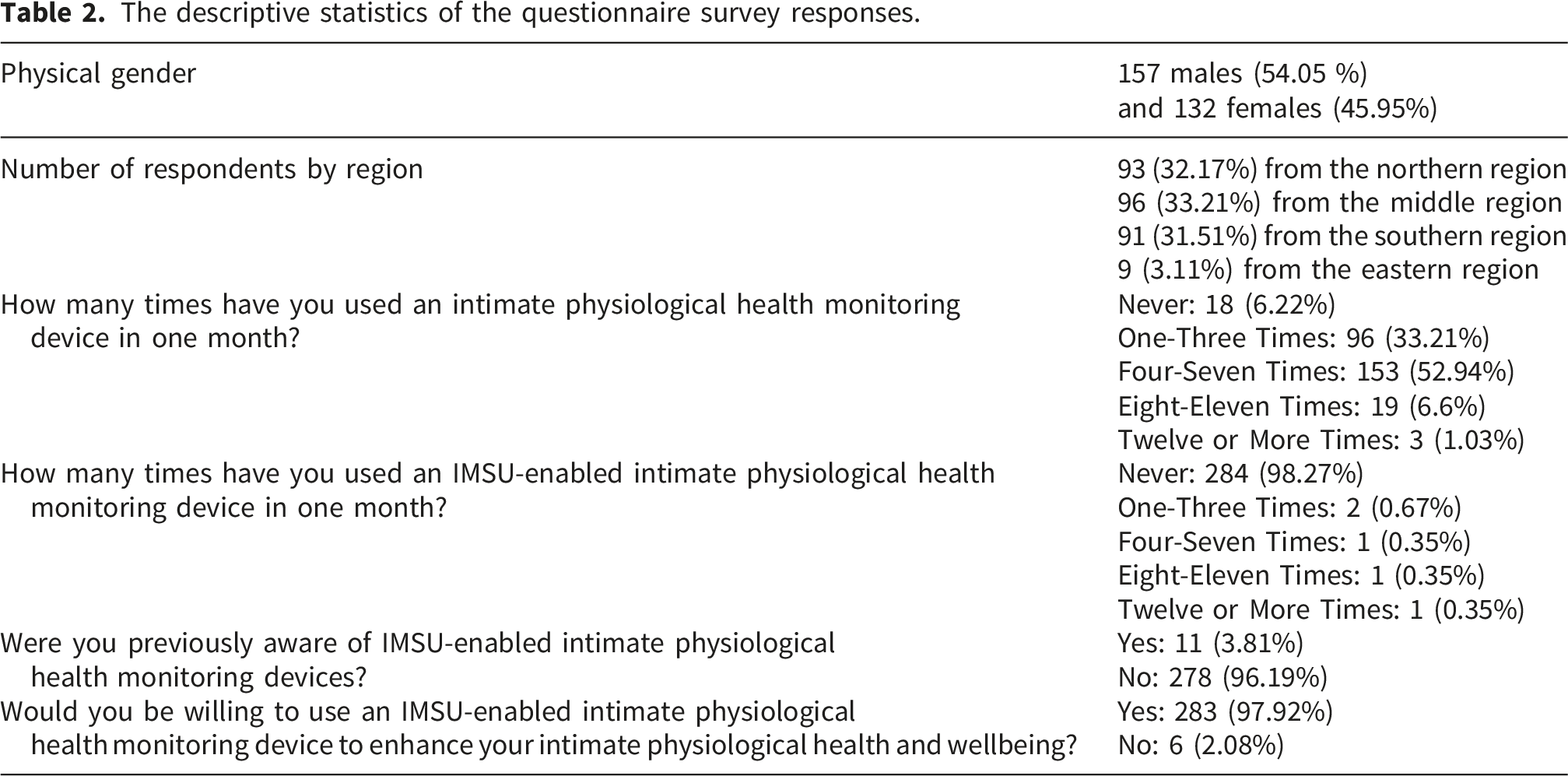
Three patterns in Table 2 are analytically consequential. First, 86.15% of participants reported monthly use of conventional intimate health devices, with 52.94% reporting four to seven monthly uses, establishing meaningful category-level familiarity that lends credibility to evaluative judgments about novel IMSU-enabled features despite limited direct experience with sensing-integrated variants. Second, the contrast between near-total prior unfamiliarity with IMSU technologies (3.81% prior awareness) and near-universal expressed adoption willingness (97.92%) firmly positions this investigation within an anticipated rather than experienced acceptance framework, a distinction embedded in the TAM and UTAUT2 theoretical assumptions adopted and revisited in the limitations section. Third, the gender-balanced sample supports demographic representativeness within Taiwan’s adult population. However, the eastern Taiwan subsample was substantially smaller (9 participants, 3.11%) than the other three regional subsamples, reflecting the considerably lower population density of eastern Taiwan relative to northern, central, and southern regions. This regional imbalance limits the representativeness of findings for eastern Taiwanese adults and is acknowledged as a sampling constraint in the limitations section. The single-country design additionally constrains cross-cultural generalizability.
Expert panel: the ANP evaluation phase engaged a purposively assembled panel of 30 domain specialists across three stakeholder cohorts, selected according to established ANP panel standards: minimum five years of domain-relevant professional experience; verifiable expertise through academic publication, professional practice, or product development; and availability for approximately 60 minutes of structured pairwise comparison. The panel comprised intimate health practitioners and certified health educators (12 participants, 40%; mean experience 11.2 years, SD = 5.3); materials science and biomedical engineering specialists with expertise in biomimetic materials and wearable sensing systems (8 participants, 26.7%; mean experience 9.8 years, SD = 4.6); and human-computer interaction researchers specializing in health informatics and privacy-sensitive interface design (10 participants, 33.3%; mean experience 8.4 years, SD = 3.9). Formal qualifications included doctoral degrees (18 participants, 60%), master’s degrees (10 participants, 33.3%), and professional certifications (2 participants, 6.7%). This disciplinary composition ensured that priority weights integrated clinical, engineering, user experience, and governance perspectives across the full spectrum of considerations relevant to emerging IoT intimate health sensing technologies, strengthening the ecological validity of derived expert judgments.
Measurement instruments. Two five-point Likert instruments (5 = very important; 1 = very unimportant) 46 were developed for the respective cohorts. The general participant survey measured perceived importance of eleven sensing material characteristics relative to three HDTB evaluation criteria. A representative item: “How important is the vibrating material function (VMF) with sweat-component sensing (SSC) for exploring physiological health-sensing behaviors and achieving intimate health satisfaction?” The expert instrument employed a pairwise comparison format aligned with ANP requirements. A representative item: “How important is the physiological health-sensing behavior criterion (EHSB) compared to the health-sensing desire criterion (SHSD) in determining user acceptance?”
3.4.2. Ethical compliance and IRB waiver justification
This research does not require Institutional Review Board (“IRB”) 53 application or review. All research procedures were conducted in full accordance with the World Medical Association Declaration of Helsinki. 54 Specifically, this research does not require full IRB review under the social science research waiver principles established by Academia Sinica, the Center of Taiwan Academic Research Ethics Education, 55 and the Taiwanese Ministry of Science and Technology and Ministry of Education, on the following six grounds:
(1) all participants were directly interviewed in person with full comprehension of research content and objectives confirmed prior to participation; (2) all participants voluntarily consented to their questionnaire responses being utilized for research purposes 54 ; (3) all participants were aged 18 years or above, satisfying Taiwan’s legal adult threshold for research participation; (4) direct informed consent, including unconditional withdrawal rights at any point, was obtained from every participant without exception; (5) no personally identifiable information was collected or retained at any stage of the research process; all responses were assigned non-linked numerical codes prior to analysis. Given that data collection involved in-person administration, the procedures employed constitute functional de-identification rather than absolute anonymity; no names, contact details, or other direct identifiers were recorded by research assistants at any point. All data was stored in encrypted, access-restricted systems, with records to be retained for five years post-publication and thereafter securely destroyed. 56
And (6) the research was assessed as presenting minimal risk, with no potential for harm or discomfort exceeding that ordinarily encountered in daily life or during routine psychological assessment, fully consistent with the minimal risk standard established under 45 CFR 46.102 of the U.S. Common Rule and the NIH Federal research protection framework. 56
Furthermore, no vulnerable populations, including minors, persons under coercion, individuals with cognitive impairments, or others with compromised decision-making capacity, were enrolled at any stage of data collection. Accordingly, this research does not require IRB application or review under the social science research waiver classification established by Academia Sinica and the Center of Taiwan Academic Research Ethics Education. All procedures were implemented in full accordance with the Declaration of Helsinki. 57
The research involved only anonymous questionnaire responses from consenting adults, with no collection of personally identifiable information, no invasive procedures, and no participation of vulnerable populations, satisfying all conditions under which IRB review is not required. Written informed consent was obtained from all participants prior to data collection. 58
3.4.3. Expert panel recruitment: Composition, size justification, and Delphi framework
The ANP qualitative evaluation phase engaged a purposively assembled expert panel of 30 domain specialists, recruited and evaluated through structured in-person interviews aligned with Delphi method principles. 59 The Delphi framework governs expert data collection for three reasons specific to this research’s evaluative context. Within ANP pairwise comparison settings, the structured anonymity that Delphi protocols enforce is not merely a procedural preference but a validity requirement: without anonymity, priority weight distributions risk systematic inflation toward the positions of institutionally senior panel members, a distortion mechanism documented in multi-expert health technology evaluation literature as the halo effect which would undermine the ecological validity of derived weights as representations of genuine disciplinary consensus. 60 Beyond anonymity, Delphi’s iterative consultation structure enables panelists to arrive at more considered and internally consistent judgments than single-round methods permit, directly supporting the consistency ratios that ANP requires for priority weight credibility. Finally, the independence of individual expert responses from group social dynamics, a structural feature of Delphi that distinguishes it from focus group and consensus conference formats, ensures that the 30-member panel’s pairwise judgments reflect authentic domain expertise rather than socially negotiated compromise positions. 61 The three-cohort panel composition, intimate health practitioners (12 participants, 40%), materials science and biomedical engineering specialists (8 participants, 26.7%), and health informatics researchers (10 participants, 33.3%), is described in full in Section 3.4.1. This disciplinary configuration ensured that ANP priority weights integrated clinical, engineering, user experience, and policy perspectives across the full evaluative spectrum, while the direct professional stakes of panel members in real-world technology development, deployment, and adoption strengthen the ecological validity of the derived expert judgments.
The expert pairwise comparison instrument employed a five-point Likert-format response scale (1 = negligible significance; 5 = paramount importance) 46 within structured ANP pairwise comparison matrices. A representative expert item reads: “How important is the physiological health-sensing behavior criterion (EHSB) compared to the health-sensing desire criterion (SHSD) in determining user acceptance of IMSU-enabled intimate health monitoring devices?” Expert interview sessions required approximately 25–30 minutes and were conducted in private settings to maintain response confidentiality and eliminate social influence on individual evaluative judgments, consistent with Delphi anonymity principles. 62
4. Results
4.1. FA measurements: Sampling adequacy and communality structure
FA pre-extraction sampling adequacy diagnostics for the 289-participant survey dataset.
Communality values for all sensing material characteristics.
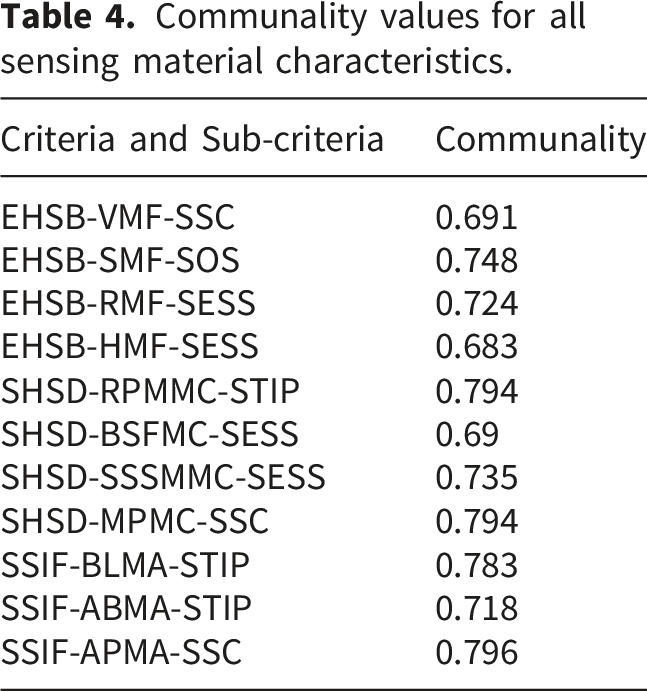
It should be noted that the original factor loading matrix per item is no longer retrievable, precluding full reporting of individual factor loadings. Communality values are therefore presented as the primary evidence of construct representation within the extracted factor solution. Future replications of this framework should preserve and report complete factor loading matrices to strengthen analytical transparency and reproducibility.
4.2. ANP measurements: Priority weighting and consistency verification
Building on FA-derived communality structure, an ANP hierarchical model was constructed to quantify interdependency-adjusted priority weights for each sensing characteristic relative to three acceptance health outcomes: negative acceptance and health influence (NAI-SH), neutral acceptance and health influence (NeuAI-SH), and positive acceptance and health influence (PAI-SH). FA communalities were embedded as weighted criteria within the ANP structure, enabling systematic cross-method integration of statistically derived user perceptions and expert-weighted judgments. The ANP model’s four-level hierarchy, goal, dimension, criteria, and acceptance alternative, maps from overall acceptance assessment through the three HDTB dimensions to individual sensing characteristics, as illustrated in Figure 3. The ANP Analytical Model.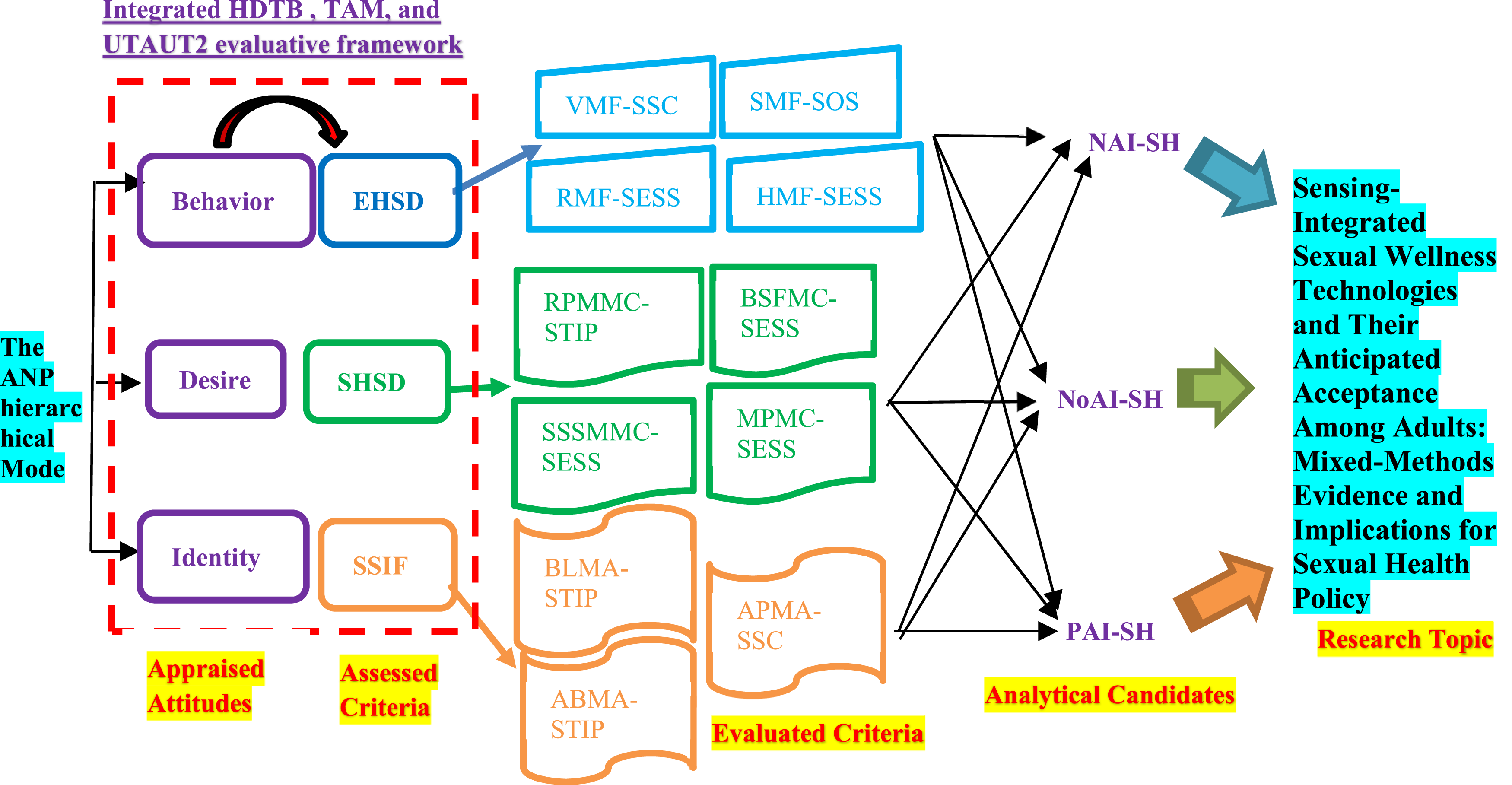
Consistency Index (C.I.) and Consistency Ratio (C.R.) for all ANP pairwise comparison matrices.
FA communalities and ANP priority weights for all sensing material characteristics across acceptance categories.
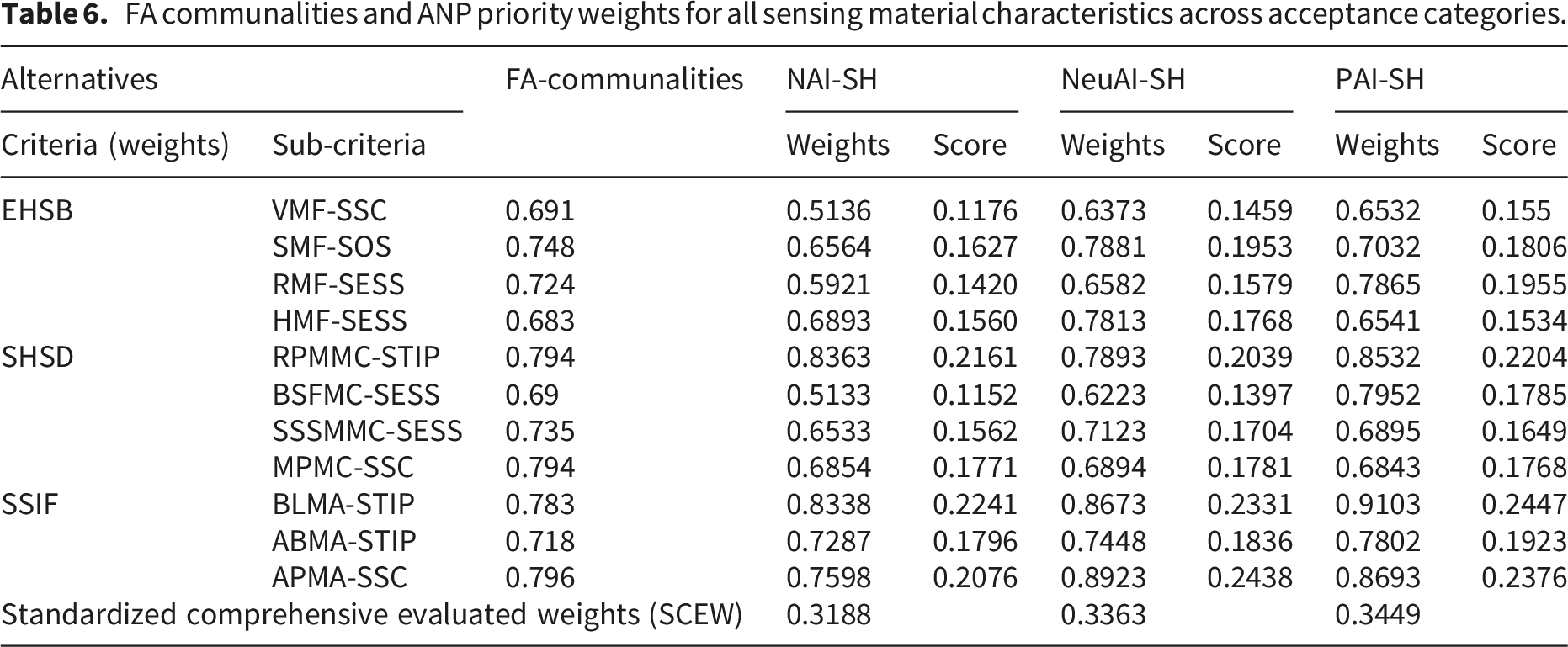
PAI-SH recorded the highest aggregate Standardized Comprehensive Evaluated Weight (SCEW = 0.3449), surpassing NeuAI-SH (0.3363) by 2.5% and NAI-SH (0.3188) by 8.2%. The compressed margin between categories suggests that user orientations toward IMSU technologies are graduated rather than polarized, carrying important implications for digital health governance strategies targeting the substantial ambivalent user segment. Among individual characteristics, the three highest PAI-SH scorers, BLMA-STIP (0.2447), APMA-SSC (0.2376), and RPMMC-STIP (0.2204), all belong to the Identity or Desire dimensions, indicating that personalization and experiential engagement features carry greater acceptance weight than functional physiological monitoring properties. A moderate-to-large cross-method correlation (r = 0.68, p < .01) between FA communalities and ANP priority weights confirms these acceptance signals are stable and replicable, validating the integrated analytical framework.
5. Discussion
5.1. Graduated acceptance hierarchy: Implications for digital health adoption strategy
FA–ANP integration reveals a graduated acceptance hierarchy for IMSU-enabled digital health technologies rather than a sharply bifurcated distribution. The 8.2% gap between PAI-SH (0.3449) and NAI-SH (0.3188) signals a meaningful directional preference toward positive adoption, while the narrow 2.5% differential between positive and neutral acceptance categories (0.3363) indicates that a substantial proportion of users occupy an evaluative middle ground, the governance-relevant ambivalent segment. For digital health policymakers, clinicians, and technology developers, this graduated distribution implies that adoption barriers are neither structural nor dispositional but are more likely attributable to insufficient transparency in biometric data governance and inadequate communication of physiological health utility, both tractable intervention targets.
5.2. Identity and Desire dimensions as primary digital health acceptance drivers
Dimensional decomposition of PAI-SH scores reveals a theoretically consequential ordering within the integrated HDTB, TAM, and UTAUT2 framework: Identity dimension characteristics achieved the highest mean positive acceptance score (0.2249), followed by Desire (0.1852) and Behavioral (0.1711), a 31.5% performance gap between highest and lowest dimensions that directly validates the theoretical extension this research introduces. In this domain, identity-expressive and hedonic features displace perceived functional utility, TAM’s foundational adoption determinant, as the dominant acceptance drivers.
Three characteristics most concretely embody this pattern. BLMA-STIP, visually integrated aesthetic design combined with intraocular pressure physiological tracking, achieved the highest individual PAI-SH score (0.2447), establishing aesthetic coherence as a primary rather than supplementary device attribute in user evaluation. APMA-SSC, anatomically individualized device form paired with sweat-component biometric sensing, ranked second (0.2376), positioning personalization capacity as a core design requirement with direct implications for patient-centered digital health device development. RPMMC-STIP, auditory-responsive physiological feedback generating a sense of interactive presence, ranked third (0.2204), representing the affective and immersive dimension of hedonic engagement that UTAUT2’s hedonic motivation construct identifies as disproportionately influential in consumer health technology contexts. By contrast, purely functional Behavioral characteristics (VMF, SMF, RMF, HMF) consistently scored below all three Identity and Desire leaders despite their greater direct relevance to physiological health-monitoring utility.
This inversion of the functional utility hierarchy extends TAM and UTAUT2 in domain-specific and policy-consequential ways. Davis 6 positioned perceived usefulness as the dominant adoption determinant in organizational computing contexts; Venkatesh et al.’s 9 elevated hedonic motivation to co-equal standing with functional utility in consumer technology settings. The present findings argue for a further domain-specific elaboration: intimate physiological health monitoring devices are evaluated simultaneously as health instruments and as identity artefacts through which users express aesthetic sensibility, personal preference, and self-concept. For digital health communicators, policymakers, and device developers, this implies that technology communication strategies and governance frameworks framed exclusively through functional health-monitoring utility logic are likely to systematically underperform relative to approaches that substantively engage users’ identity-expressive and experiential motivations.
5.3. Cross-method validity and biometric data governance implications
The r = 0.68 (p < .01) correlation between FA communalities and ANP priority weights, derived from entirely independent analytical procedures applied to structurally distinct data sources, constitutes the research’s primary internal validity evidence. Three conclusions follow. First, the alignment between statistically emergent user preference patterns and independently derived expert judgments indicates that identified acceptance signals reflect genuine, replicable evaluative orientations rather than instrument-specific tendencies. Second, the correspondence between aggregated user perceptions and expert-weighted priorities validates both panel domain competence and multidisciplinary representativeness. Third, the cross-method consistency of key findings; particularly, the convergence of elevated FA communalities and ANP priority weights for BLMA-STIP (0.783; 0.9103), APMA-SSC (0.796; 0.8693), and RPMMC-STIP (0.794; 0.8532), confirms that these characteristics represent method-stable design priorities rather than artifacts of any single analytical phase.
Beyond methodological validity, these findings carry direct biometric data governance implications for the digital health policy community. IMSU-enabled devices continuously collect intimate physiological data streams, including dermal biomarkers, intraocular pressure, and oral saliva composition, outside clinical oversight, generating governance challenges that existing digital health frameworks have not yet systematically addressed. The compressed PAI-SH/NeuAI-SH differential (2.5%) suggests that the substantial ambivalent user segment’s adoption trajectory will likely be determined by the transparency, user-controllability, and institutional legitimacy of biometric data governance architectures, rather than by device functionality or clinical evidence alone. This governance-acceptance interface represents a critical intervention point for digital health regulators and health informatics policymakers.
6. Conclusions and recommendations
This research applied a sequential FA–ANP framework within an integrated HDTB, TAM, and UTAUT2 evaluative architecture to identify sensing material characteristics governing anticipated user acceptance of IMSU-enabled intimate physiological health monitoring devices. Three principal contributions emerge for digital health scholarship and practice. First, the research delivers the first multi-dimensional, theory-grounded acceptance framework explicitly connecting discrete IoT sensing design characteristics to the distinct psychosocial pathways, Behavioral, Desire, Identity, through which they acquire adoption-relevant meaning, providing an evidence base for device design standardization and user-centered health informatics governance. Second, three method-stable positive acceptance determinants are identified: visual-aesthetic sensing integration (BLMA-STIP, 0.2447), anatomical personalization (APMA-SSC, 0.2376), and auditory-responsive physiological feedback (RPMMC-STIP, 0.2204). Third, acceptance in this domain follows identity-expressive and hedonic pathways that outweigh functional utility by 31.5%, diverging substantially from TAM-established norms and carrying direct implications for device design strategy, digital health communication, biometric data governance policy, and user autonomy frameworks.
Four evidence-based recommendations are offered for researchers, clinicians, device developers, and policymakers engaged in the digital health ecosystem. IMSU device development should treat Identity and Desire dimension features; particularly, aesthetic coherence, anatomical individualization, and multi-modal sensory feedback, as primary design requirements rather than optional enhancements. User-centered physiological personalization should be integrated as a foundational patient-centered design principle. Pending longitudinal validation with experienced users, these findings provisionally suggest that transparent, user-controlled biometric data governance architectures may be critical for converting the substantial ambivalent user segment into sustained adopters. Based on anticipated acceptance data, digital health communication strategies may benefit from framing IMSU value through holistic experiential and identity-expressive discourse, supplementary to rather than replacing evidence-based health-monitoring utility messaging, though this inference requires confirmation through longitudinal deployment research.
Six limitations constrain generalizability. First, the single-country Taiwanese sample restricts cross-cultural applicability. Second, near-universal absence of prior IMSU experience (98.09%) positions all findings within an anticipated rather than experienced acceptance framework. Third, self-report methodology carries social desirability risk in sensitive health technology contexts. Fourth, the original factor loading matrix is no longer retrievable, precluding full reporting of factor loadings per item; future replications should present complete factor loading matrices to strengthen analytical transparency and reproducibility. Fifth, the expert panel excluded data governance specialists and bioethicists whose perspectives are consequential given IMSU’s intimate biometric data collection implications, a compositional gap that future expert evaluation studies should address. Sixth, the disproportionately small eastern Taiwan subsample (n = 9, 3.11%) relative to the northern (n = 93), central (n = 96), and southern (n = 91) subsamples limits regional representativeness within the study’s own sampling frame. Future research should ensure proportional regional representation across all geographic zones to strengthen intra-national generalizability.
Future research priorities include: longitudinal deployment studies assessing whether pre-adoption preference structures predict sustained physiological health monitoring engagement; experimental governance transparency manipulations to identify policy architectures most effective in resolving adoption ambivalence; clinical efficacy trials establishing health outcome evidence beyond acceptance measurement; and cross-cultural comparative investigations delineating the boundary conditions of the present findings. As IoT-enabled physiological sensing continues its expansion into intimate digital health contexts, constructing governance frameworks and design standards that honor users' identity-expressive acceptance logic while protecting biometric data rights and individual health autonomy constitutes one of digital health informatics' most consequential and pressing emerging challenges.
Supplemental material
Supplemental material - Wearable IoT health sensing beyond functional utility: Identity-expressive and hedonic determinants of user acceptance in intimate physiological monitoring devices — A sequential FA–ANP mixed-methods investigation with digital health policy implications
Supplemental material for Wearable IoT health sensing beyond functional utility: Identity-expressive and hedonic determinants of user acceptance in intimate physiological monitoring devices — A sequential FA–ANP mixed-methods investigation with digital health policy implications by Ai-Chieh Chang, Jiin-Chyuan Mark Lai, Shu-Hui Peng, Chun-Ming Shih and Ming Yuan Hsieh in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all participants and domain experts for their time and contributions to this research.
Ethical considerations
All research procedures were conducted in full accordance with the World Medical Association Declaration of Helsinki. In accordance with the social science research waiver principles established by Academia Sinica and the Center of Taiwan Academic Research Ethics Education, this research does not require IRB application or review. The study involved only anonymous questionnaire responses from consenting adults aged 18 or above, with no collection of personally identifiable information, no invasive procedures, and no participation of vulnerable populations, satisfying all conditions under which IRB review is not required. Written informed consent was obtained from all participants prior to data collection. No vulnerable populations were enrolled at any stage.
Consent for publication
Not applicable. This research collected only anonymous questionnaire responses. No personally identifiable information was collected or retained at any stage. All responses were assigned non-linked numerical codes prior to analysis. IRB review was not required under applicable Taiwanese social science research regulations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Taiwanese Ministry of Education (MOE-114-TPRBM-0039-017Y1), Taiwanese National Science and Technology Council (NSTC 113-2629-H-142-001-), National Taichung University of Education (NTCU114106).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this research are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.