
Abstract
Background
Artificial intelligence is influencing healthcare delivery and nursing education; however, its responsible use requires awareness of privacy, accountability, patient safety, and human-centered communication. Evidence concerning ethical awareness among Palestinian undergraduate nursing students remains limited.
Aim
To assess ethical awareness and attitudes toward artificial intelligence among undergraduate nursing students in Palestine and identify factors associated with high ethical awareness.
Methods
A descriptive, analytical cross-sectional study was conducted among 276 undergraduate nursing students at Palestine Polytechnic University, Hebron, Palestine, during March and April 2025. Participants completed an anonymous self-administered questionnaire assessing sociodemographic characteristics, attitudes toward artificial intelligence, and ethical awareness. Ethical awareness was assessed using eight dichotomous items addressing ethical, legal, professional, and relational concerns. Descriptive statistics, independent-samples t tests, one-way analysis of variance, Pearson correlation, and binary logistic regression were applied.
Results
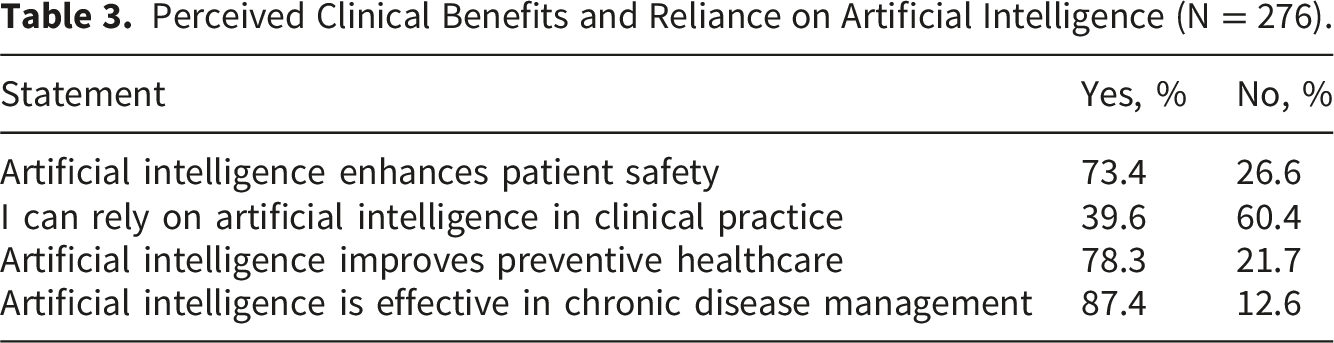
Students demonstrated favorable views regarding the contribution of artificial intelligence to chronic disease management (87.4%), preventive healthcare (78.3%), and patient safety (73.4%). Nevertheless, ethical concerns were evident: 77.1% indicated that artificial intelligence could weaken provider–patient communication, 76.3% considered current legal regulation insufficient, and 66.2% recognized risks of reliance on artificial intelligence over human expertise. Female students reported higher ethical awareness than male students (4.08 ± 1.17 vs. 3.61 ± 1.26; p = .003), and ethical awareness differed by academic year (p = .006). Ethical awareness was positively correlated with attitudes toward artificial intelligence (r = .32, p < .001). Female gender, academic year, and favorable attitudes predicted high ethical awareness, whereas age was not significant.
Conclusion
Palestinian undergraduate nursing students expressed favorable attitudes toward artificial intelligence while recognizing ethical and professional risks. Integrating ethically grounded artificial intelligence education into nursing curricula may support safe, accountable, and patient-centered technology use.
Keywords
Introduction
Artificial intelligence (AI) is increasingly incorporated into healthcare delivery, health professions education, clinical decision support, documentation, disease prediction, and patient monitoring. Although these technologies may support efficiency, safety, and improved access to information, their application in healthcare also introduces ethical concerns regarding patient autonomy, privacy and confidentiality, algorithmic bias, transparency, professional accountability, and the preservation of human-centred care. The World Health Organization has emphasized that AI for health should protect autonomy, promote safety and public interest, ensure transparency, foster responsibility and accountability, and promote equity and sustainability. 1 Similarly, ethical frameworks for AI in health professions education identify fairness, transparency, safety, accountability, and collaboration as central conditions for responsible integration. 2
Nursing students are an important population in this transition because they will enter clinical environments in which AI-supported systems may increasingly influence assessment, decision support, patient education, workflow management, and documentation. Future nurses will be required to evaluate AI-supported information while maintaining professional judgment, advocacy, confidentiality, therapeutic communication, and accountability for patient-centred care. Evidence from health professions education indicates that students commonly express positive attitudes toward AI and recognize its potential contribution to healthcare and education; however, their knowledge, preparedness, and confidence in using AI responsibly remain variable.3–5 A systematic review and meta-analysis involving medical, dental, and nursing students reported generally positive attitudes toward AI but also identified gaps in knowledge and preparedness. 3 Similarly, a scoping review of health science students found broad interest in AI education while highlighting concerns regarding insufficient training and uncertainty about professional implications. 4 A multi-country survey further demonstrated that students supported AI integration into health professions education despite reporting limited AI-related knowledge and perceived implementation challenges. 5
In nursing education, the ethical dimensions of AI require particular attention because nursing practice is grounded in relational care, patient advocacy, dignity, confidentiality, safety, and professional responsibility. In the present study,
Recent nursing research demonstrates the relevance of ethical awareness in the context of AI. Migdadi et al. examined AI ethical awareness, attitudes, anxiety, and intention to use AI among nursing students and reported meaningful associations among these variables. 6 Yang found that nursing students’ AI ethics awareness was positively associated with digital literacy and moral sensitivity, emphasizing that responsible engagement with AI requires more than technical familiarity. 7 Collectively, these findings suggest that ethical awareness may help students balance technological innovation with professional responsibility, rather than approaching AI through either uncritical acceptance or unsupported avoidance.
The relationship between ethical awareness and technology acceptance can be conceptually informed by the Technology Acceptance Model and the Unified Theory of Acceptance and Use of Technology. These models emphasize perceived usefulness, perceived ease of use, social influence, and facilitating conditions as factors shaping technology-related attitudes and behavioural intention.8,9 However, they were developed primarily to explain technology adoption and do not independently address privacy, accountability, algorithmic bias, professional responsibility, or patient trust. Accordingly, the present study does not formally test either model; rather, they provide a conceptual background for examining attitudes toward AI, while ethical awareness is considered a distinct nursing-relevant construct requiring specific assessment.
Concerns regarding patient trust and professional accountability are especially important when AI is applied in healthcare. AI-supported decisions may involve sensitive patient information, clinical risk, and recommendations that patients may not readily understand. International ethical guidance emphasizes that AI in healthcare should be governed in ways that preserve patient autonomy, protect privacy, support transparency, and maintain accountability for decisions affecting care. 1 Within nursing education, preparing students to recognize these issues is important because future nurses may be expected to communicate with patients about digitally supported care while ensuring that technology does not compromise dignity, trust, or therapeutic relationships.
Despite increasing international interest, several gaps remain in the literature. Existing studies have frequently examined mixed health profession samples or nursing students outside Palestine, and much of the evidence remains descriptive.3–7,10 Previous studies have also commonly focused on attitudes, intention to use AI, anxiety, or knowledge, whereas fewer investigations have examined predictors of ethical awareness specifically among undergraduate nursing students. Migdadi et al. provided important evidence regarding ethical awareness and AI-related attitudes among nursing students 6 ; however, the present study extends this evidence by examining ethical awareness and attitudes toward AI among undergraduate nursing students in the Palestinian context and by evaluating demographic and academic predictors of high ethical awareness.
The Palestinian context provides an important setting for examining this issue. Evidence concerning AI integration in nursing and health sciences education indicates that curricular preparation, faculty competence, ethical training, and infrastructure are important considerations for responsible implementation. 10 Understanding Palestinian nursing students’ ethical awareness and attitudes may therefore provide an empirical basis for developing curriculum content addressing privacy, accountability, patient safety, bias, appropriate reliance on AI, and the protection of human-centred nursing practice. Such evidence is relevant as nursing programmes prepare graduates for healthcare environments in which digital technologies are expanding while ethical and regulatory safeguards remain essential.
Aim of the study
This study aimed to assess ethical awareness regarding artificial intelligence and attitudes toward artificial intelligence among undergraduate nursing students in Palestine and to identify demographic and academic predictors of high ethical awareness.
Research questions
1. What is the level of ethical awareness regarding artificial intelligence among undergraduate nursing students? 2. What are undergraduate nursing students’ attitudes toward artificial intelligence in healthcare and nursing education? 3. Is there a significant relationship between ethical awareness and attitudes toward artificial intelligence? 4. Do ethical awareness scores differ according to gender and academic year? 5. Which demographic and academic factors predict high ethical awareness among undergraduate nursing students?
Methods
Study design and setting
A descriptive, analytical cross-sectional study was conducted among undergraduate nursing students at the College of Nursing, Palestine Polytechnic University, Hebron, Palestine, during the 2024–2025 academic year. Data were collected between March and April 2025. The study examined ethical awareness regarding artificial intelligence (AI), attitudes toward AI integration in nursing education and healthcare practice, and demographic and academic factors associated with high ethical awareness. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidance for cross-sectional studies. 11
Population, sample, and recruitment
The target population comprised all undergraduate nursing students enrolled at the university during the study period (N = 700). 12 Eligible participants were students registered in any of the four academic years of the undergraduate nursing programme, available during data collection, able to understand the questionnaire language, and willing to provide written informed consent. Students were excluded if they declined participation or returned questionnaires with substantial missing data that prevented calculation of the principal variables.
The minimum sample size was estimated using the single-population proportion formula with finite population correction. A 95% confidence level, 5% margin of error, and conservative expected proportion of 50% were applied because no previous Palestinian estimate of high AI-related ethical awareness among undergraduate nursing students was available. The resulting minimum sample size was approximately 248 students. Convenience sampling was used, and eligible students were approached during classroom sessions and clinical briefing meetings. A total of 276 completed questionnaires were included in the analysis. Throughout the manuscript, the population is consistently described as
Instrumentation
Data were collected using a structured, self-administered questionnaire consisting of three sections. The first section collected age, gender, and academic year. These variables were used to describe the sample and examine differences in ethical awareness.
The second section assessed attitudes toward AI using 10 items adapted from the Artificial Intelligence Attitude Scale developed. 13 Items addressed the perceived importance of learning AI, the future relevance of AI in healthcare, integration into education and training, possible replacement of human roles, and perceived diagnostic risk. Responses were rated on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). Negatively phrased items were reverse coded before calculation of the total mean attitude score. The composite score ranged from 1 to 5, with higher scores indicating more positive attitudes toward AI integration.
The third section assessed ethical awareness regarding AI. Ethical awareness was defined as students’ recognition of ethical, legal, professional, and relational concerns associated with AI use in healthcare, including privacy, accountability, reliance on human expertise, public health risk, and provider–patient communication. This definition was informed by previous nursing student research on AI ethics awareness.6,7
The original questionnaire included 12 dichotomous AI-related statements. Following conceptual review, eight items were identified as directly reflecting ethical awareness: recognition of privacy risks; insufficiency of current legal regulation; continuing physician liability for AI errors; developer responsibility for AI mistakes; physician responsibility for AI-supported decisions; risks of relying on AI over human expertise; possible harm to public health; and weakening of provider–patient communication. Responses reflecting recognition of the ethical concern were coded as 1, while responses not reflecting recognition were coded as 0. The total ethical awareness score therefore ranged from 0 to 8, with higher scores indicating greater ethical awareness.
Four items concerning patient safety, preventive healthcare, chronic disease management, and reliance on AI in clinical practice were excluded from the ethical awareness composite score because they measured perceived usefulness or clinical benefit rather than ethical awareness. These items were retained for descriptive reporting only.
For binary logistic regression, ethical awareness was categorized using the eight-item composite score. Participants scoring 6–8, representing recognition of at least 75% of the identified ethical concerns, were classified as having high ethical awareness and coded as 1. Participants scoring 0–5 were classified as having lower ethical awareness and coded as 0.
Validity, reliability, and pilot testing
The questionnaire was administered in
A pilot test was conducted among
Data collection and analysis
Following ethical approval, students provided written informed consent and completed the anonymous questionnaire in 10–15 minutes. Data were analysed using IBM SPSS Statistics version 29. Descriptive statistics summarized study variables. Independent-samples t tests, one-way analysis of variance with Tukey post hoc comparisons, and Pearson’s correlation were used for inferential analysis. Binary logistic regression examined predictors of high ethical awareness, defined as a score of 6–8 on the eight-item scale. Results were reported as adjusted odds ratios with 95% confidence intervals. Model fit was assessed using the Hosmer–Lemeshow test and Nagelkerke R2. Statistical significance was set at p < .05.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee at Palestine Polytechnic University, Hebron, Palestine (EA/177/2025). Written informed consent was obtained from all participants. Participation was voluntary, confidentiality was maintained, and no identifiable information was collected.
Results
Characteristics of Undergraduate Nursing Students (N = 276).
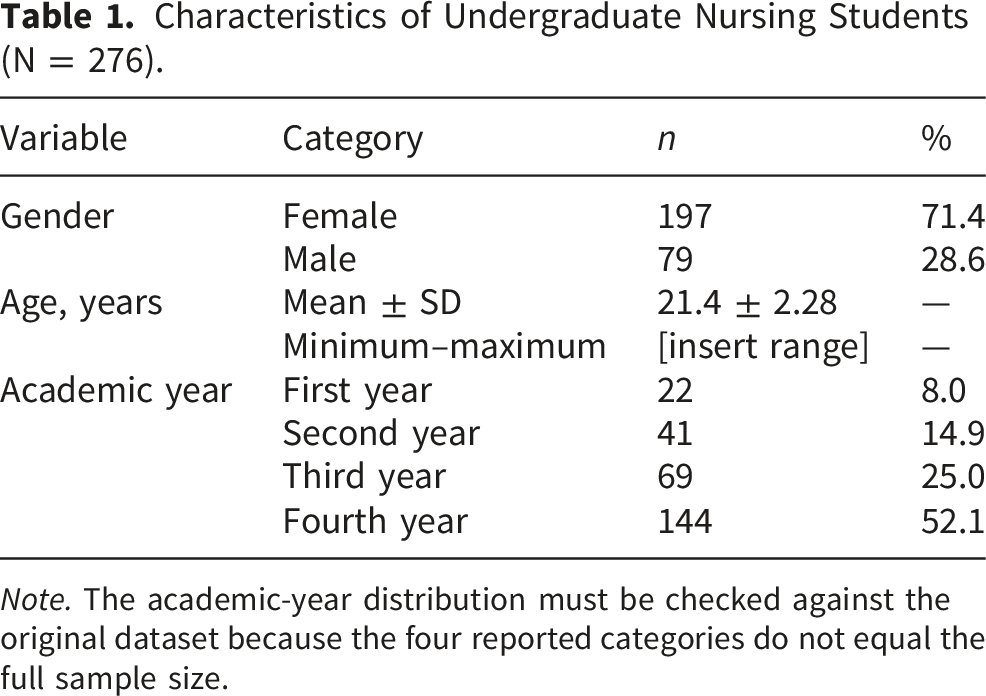
Note. The academic-year distribution must be checked against the original dataset because the four reported categories do not equal the full sample size.
Responses Indicating Ethical Awareness Regarding Artificial Intelligence (N = 276).
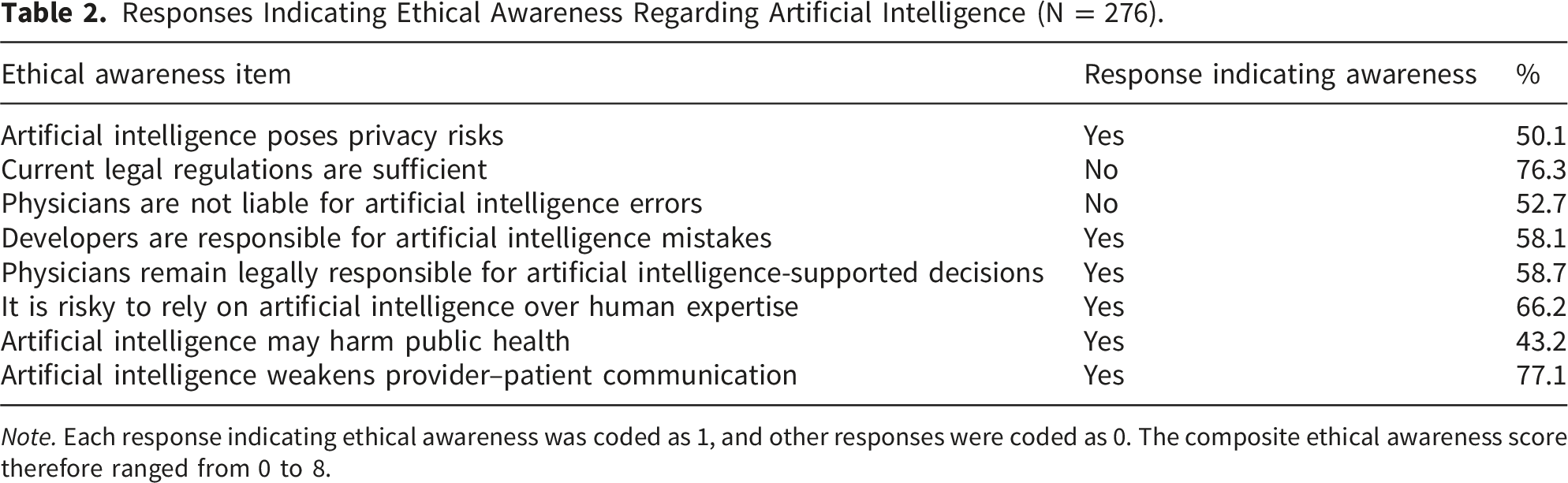
Note. Each response indicating ethical awareness was coded as 1, and other responses were coded as 0. The composite ethical awareness score therefore ranged from 0 to 8.
Perceived Clinical Benefits and Reliance on Artificial Intelligence (N = 276).
Attitudes Toward Artificial Intelligence Among Undergraduate Nursing Students (N = 276).
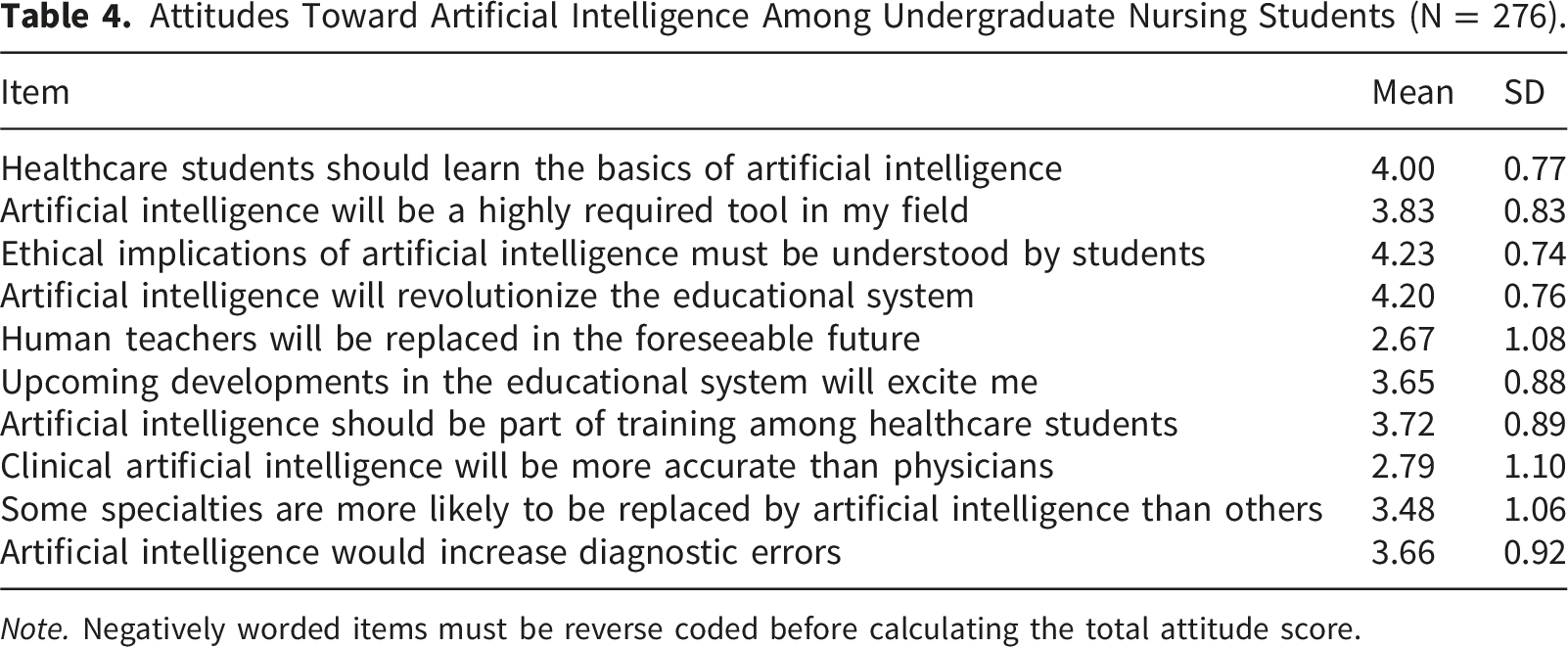
Note. Negatively worded items must be reverse coded before calculating the total attitude score.
Ethical Awareness Scores According to Gender and Academic Year Among Undergraduate Nursing Students (N = 276).

Note. The original manuscript reported significant differences according to gender and academic year but did not report post hoc comparisons. These comparisons must be inserted from the SPSS output. Academic-year findings should be interpreted cautiously because of unequal group sizes.
Correlation Between Ethical Awareness and Attitudes Toward Artificial Intelligence Among Undergraduate Nursing Students (N = 276).

Binary Logistic Regression Predicting High Ethical Awareness Among Undergraduate Nursing Students (N = 276).
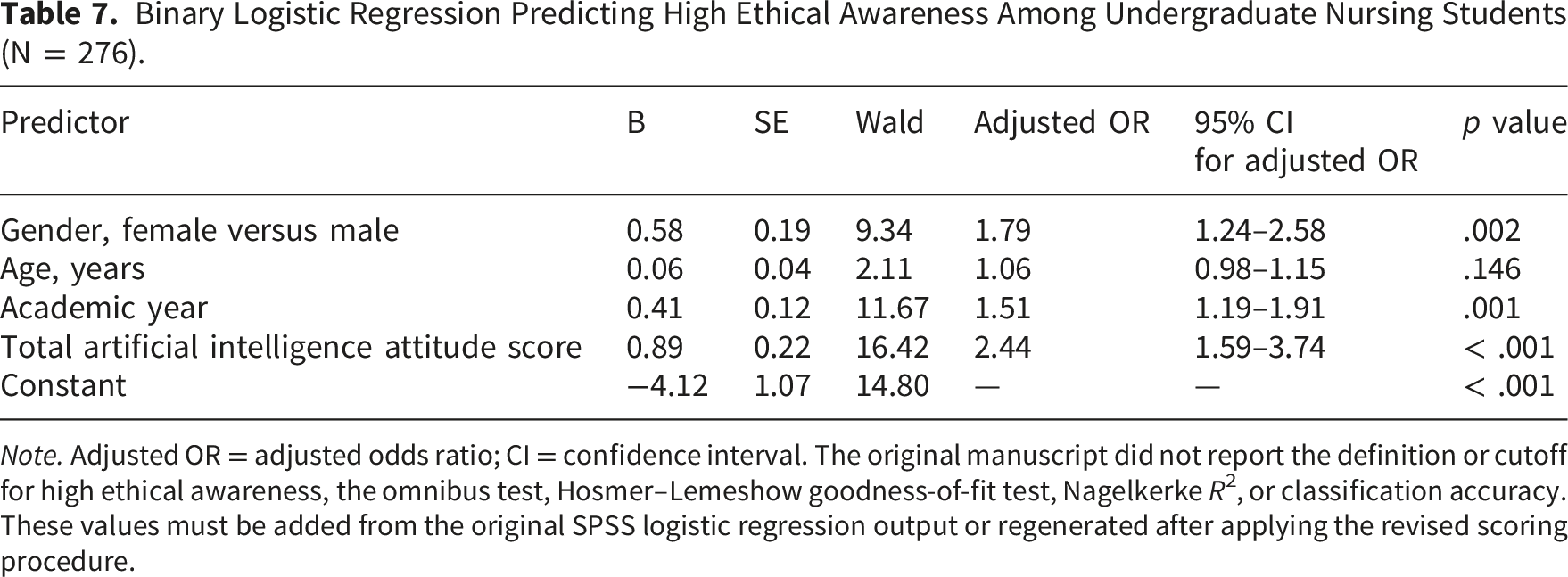
Note. Adjusted OR = adjusted odds ratio; CI = confidence interval. The original manuscript did not report the definition or cutoff for high ethical awareness, the omnibus test, Hosmer–Lemeshow goodness-of-fit test, Nagelkerke R2, or classification accuracy. These values must be added from the original SPSS logistic regression output or regenerated after applying the revised scoring procedure.
Discussion
This study examined ethical awareness regarding artificial intelligence (AI), attitudes toward AI, and predictors of high ethical awareness among undergraduate nursing students in Palestine. Overall, the findings demonstrated a pattern of cautious acceptance. Students recognized the potential contribution of AI to chronic disease management, preventive healthcare, and patient safety, while also identifying important ethical concerns related to inadequate legal regulation, reliance on AI over human expertise, and the possible weakening of provider–patient communication. Students also reported generally favourable attitudes toward learning about AI and integrating it into nursing education.
Ethical awareness was significantly higher among female students and differed according to academic year, with more senior students reporting higher scores. In addition, ethical awareness was positively correlated with attitudes toward AI. The regression findings indicated that gender, academic year, and more positive AI attitudes were significant predictors of high ethical awareness, whereas age was not significant 12 . Collectively, these findings suggest that ethical concern does not necessarily represent rejection of AI; rather, it may reflect a more informed and professionally responsible orientation toward its use.
The simultaneous recognition of AI benefits and ethical concerns is particularly relevant in nursing education. Nursing practice requires the use of clinical knowledge and technological information while preserving professional accountability, therapeutic communication, advocacy, confidentiality, and respect for patient dignity. Consequently, students may support AI as a useful clinical and educational tool while remaining cautious about its limitations and risks. International ethical guidance similarly emphasizes that AI in healthcare should preserve autonomy, transparency, accountability, safety, and equity. 1
The positive relationship between ethical awareness and favourable AI attitudes may indicate that students who recognize ethical concerns are not necessarily resistant to innovation. Instead, ethical awareness may enhance students’ confidence in engaging with AI responsibly because they are better prepared to identify when privacy, accountability, human oversight, or patient communication may be compromised. Previous evidence among nursing students has shown that ethical awareness, attitudes, anxiety, intention to use AI, digital literacy, and moral sensitivity are interconnected dimensions of responsible technology adoption.6,7
This interpretation is also consistent with technology acceptance perspectives. Perceived usefulness and perceived ease of use may support favourable attitudes toward AI, but nursing education must extend beyond technology acceptance to address ethical responsibility and human-centred care.8,9 A systematic review guided by the Technology Acceptance Model found that nursing students’ perceptions of usefulness and ease of use were important influences on AI acceptance; however, it also highlighted the need for educational preparation to support appropriate adoption. 14 Therefore, favourable attitudes should not be interpreted as sufficient readiness for clinical use unless accompanied by ethical competence and critical judgment.
The higher ethical awareness reported among female students should be interpreted cautiously. Although gender-related differences may reflect variations in sensitivity to relational and ethical aspects of care, the present study did not investigate the underlying reasons for this finding. Similarly, the higher ethical awareness among senior students may reflect greater clinical exposure and increased contact with ethical issues during professional training. Nevertheless, because academic-year groups were unequally represented, particularly with fewer first-year students, this finding should not be interpreted as definitive evidence that ethical awareness improves progressively across the nursing programme.
The present findings are consistent with Palestinian evidence showing that nursing students generally hold positive attitudes toward AI integration in nursing practice and healthcare. A recent Palestinian study reported favourable attitudes toward AI benefits and willingness to use AI, while also identifying the need for structured AI-focused training in nursing curricula. 15 The current study adds to that evidence by focusing specifically on ethical awareness and by examining demographic and academic predictors associated with high ethical awareness.
The findings also complement Palestinian evidence concerning emotional and professional responses to AI. A study among Palestinian nursing students found that positive attitudes toward AI could coexist with AI-related anxiety, indicating that students may value AI while simultaneously experiencing uncertainty about its future educational and professional implications. 11 This is relevant to the present findings because ethical concerns regarding legal responsibility, communication, and reliance on AI may represent informed caution rather than negative attitudes toward technology.
Concerns about AI were not limited to students. Studies among intensive care unit nurses and neonatal intensive care unit nurses in the West Bank identified perceived worries regarding AI adoption in clinical practice, particularly in relation to professional roles, patient care, awareness, and previous experience with AI.13,12 These clinical findings reinforce the importance of preparing nursing students before graduation, as concerns surrounding accountability, human oversight, and patient safety may become more significant in high-acuity clinical settings.
The present findings are also aligned with broader international evidence. Systematic reviews of health professions students have reported generally positive attitudes toward AI, accompanied by gaps in knowledge, confidence, and readiness for ethically appropriate use.3–5 A review of AI-based technologies in nursing found that much of the existing evidence remains concentrated in early development and validation phases, with limited evidence regarding implementation and impact in nursing practice. 16 Similarly, international nursing scholarship has emphasized that nurses should actively contribute to AI design, implementation, governance, and education to ensure that these technologies remain aligned with nursing values and patient needs. 15
Recent reviews focused specifically on nursing education have highlighted similar ethical and educational priorities. Evidence indicates that AI may support simulation, individualized learning, assessment preparation, clinical reasoning, and access to educational content; however, concerns persist regarding privacy, bias, accountability, academic integrity, dependency on automated outputs, and the need for educator oversight.17,18,19 Thus, the present Palestinian findings reflect a wider international pattern while also providing locally relevant evidence for nursing education within a resource-constrained healthcare and educational context.
Implications for nursing education, practice, and policy
The study findings have direct implications for undergraduate nursing education. Nursing programmes in Palestine should integrate structured AI education that combines technical understanding with ethical and professional preparation. Curriculum content should address privacy and confidentiality, algorithmic bias, legal and professional accountability, patient safety, documentation integrity, communication with patients, and appropriate human oversight of AI-supported decisions. Such content may be delivered through case-based learning, simulation, clinical scenarios, reflective discussions, and interprofessional ethics activities.
The findings also have implications for nursing practice. Graduating nurses may increasingly encounter AI-supported systems in clinical decision support, documentation, patient monitoring, risk prediction, and patient education. Ethical preparation during undergraduate education may enable future nurses to assess AI-generated information critically, recognize unsafe reliance on automated recommendations, communicate transparently with patients, and preserve professional accountability. This is particularly important in critical care and neonatal settings, where inaccurate decisions or reduced human oversight may have substantial consequences for vulnerable patients.13,12
At the policy level, nursing faculties, healthcare organizations, and regulatory bodies should develop clear guidance for responsible AI implementation. Such guidance should clarify professional accountability, patient data protection, transparency, acceptable educational use, faculty responsibilities, and procedures for evaluating AI tools before clinical or educational adoption. Evidence syntheses emphasize that effective AI integration requires governance, ethical standards, staff preparation, and institutional policies rather than technology introduction alone.14–20
Strengths and limitations
This study has several strengths. First, it addresses an emerging and highly relevant issue in nursing education: the relationship between AI attitudes and ethical awareness. Second, it contributes evidence from Palestine, a context that remains underrepresented in international research concerning AI and nursing education. Third, the study focused specifically on undergraduate nursing students, who represent a future workforce likely to encounter AI-supported healthcare technologies. Fourth, the study used a structured questionnaire, expert content validation, pilot testing, reliability assessment, and multivariable analysis to address its objectives. Finally, distinguishing ethical-awareness items from general perceived-benefit items strengthens the conceptual clarity of the revised manuscript.
Several limitations should be considered when interpreting the findings. The cross-sectional design limits causal interpretation; therefore, the relationship between ethical awareness and attitudes cannot establish whether one construct influences the other over time. Convenience sampling may have introduced selection bias and may limit generalizability beyond the participating institution. Self-reported responses may also be influenced by social desirability or by students’ perceptions of academically desirable answers.
The unequal distribution of participants across academic years limits interpretation of academic-year differences. In addition, the study included only age, gender, and academic year as predictors. Other potentially influential variables, including previous AI education, digital literacy, clinical exposure to AI tools, previous ethics education, access to digital resources, anxiety, and intention to use AI, were not assessed. Finally, although the revised ethical awareness measure reflects recognition of selected ethical concerns, it should not be interpreted as measuring the full complexity of ethical reasoning, ethical decision-making, or clinical competence.
Conclusion
Undergraduate nursing students in Palestine demonstrated generally positive attitudes toward AI while recognizing significant ethical, legal, and professional concerns. The positive association between ethical awareness and attitudes suggests that ethical preparation may facilitate responsible acceptance of AI rather than discourage innovation. Integrating ethically grounded AI education into nursing curricula is therefore essential to prepare future nurses to engage with emerging technologies while preserving accountability, patient safety, therapeutic communication, and human-centred care.
Supplemental material
Supplemental material - Ethical awareness and attitudes toward artificial intelligence among undergraduate nursing students in Palestine: A cross-sectional study
Supplemental material for Ethical awareness and attitudes toward artificial intelligence among undergraduate nursing students in Palestine: A cross-sectional study by Mohammad Qtait in DIGITAL HEALTH.
Footnotes
Acknowledgements
The author would like to thank all undergraduate nursing students who participated in this study. The author also acknowledges the experts who contributed to the content validity assessment of the questionnaire.
Ethical consideration
Ethical approval for this study was obtained from the Research Ethics Committee at Palestine Polytechnic University, Hebron, Palestine (Approval No. EA/177/2025).
Consent to participate
All participants were informed about the purpose of the study, the voluntary nature of participation, confidentiality of their responses, and their right to withdraw without any consequences. Written informed consent was obtained from all participants before data collection. No personally identifiable information was collected, and all data were handled confidentially and used solely for research purposes.
Consent for publication
Not applicable. This manuscript does not contain any individual participant’s identifiable information, images, or personal data requiring consent for publication.
Author contribution
Mohammad Qtait was solely responsible for the conceptualization of the study, methodology development, questionnaire preparation, data collection, data curation, formal analysis, interpretation of findings, preparation of the original manuscript draft, critical revision of the manuscript, supervision, project administration, and final approval of the version submitted for publication. The author accepts full responsibility for the integrity and accuracy of all aspects of the work.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and subject to relevant ethical and institutional requirements. The questionnaire used in this study is provided as a supplementary file accompanying the manuscript.
Data guarantor
Mohammad Qtait is the data guarantor for this study and accepts full responsibility for the integrity of the data and the accuracy of the data analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.