
Abstract
Objectives
This study aims to perform a comprehensive visualization-based analysis of the research status, thematic hotspots, and developmental trends in AI-assisted oral disease diagnosis over the past two decades, thereby offering valuable references for future research in this fields.
Material and methods
We conducted a bibliometric study with 2,131 documents extracted from the Web of Science Core Collection (2005-2025) using CiteSpace to systematically analyze publication trends, major countries, institutions, journals and co-citation patterns. Visualizations including collaboration networks, keyword co-occurrence clusters, citation bursts, and topic timelines showed the evolving intellectual structure and emerging research fronts in this area.
Results
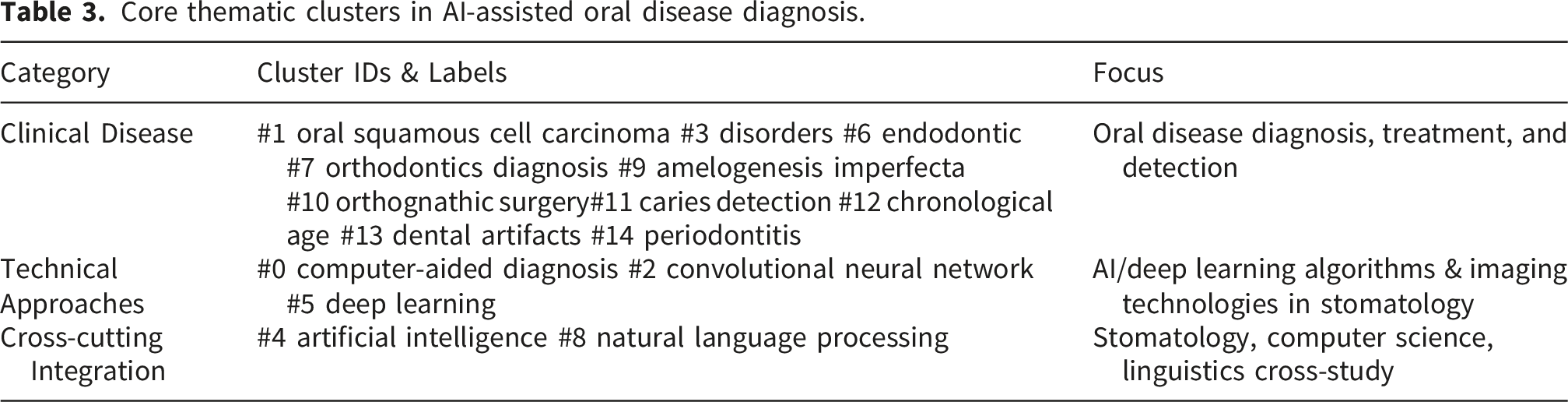
The number of annual publications grew exponentially and peaked at 519 in 2024. China, the United States and India ranked as the top three countries. Berlin-based institutions contributed 224 publications, representing 45.62% of the 491 outputs from the top ten productive institutions. Core keywords were identified through co-occurrence analysis, including “artificial intelligence”, “deep learning”, “machine learning”, and “classification”. Further cluster analysis formed 15 clusters, which were summarized into three major themes: clinical diseases, technical approaches, and cross-cutting integration. Burst analysis showed that “Computer-aided diagnosis” had the strongest burst (5.23), followed by “system” (4.75) and “extractions” (4.69).
Conclusions
In this study, we used bibliometric visualization analysis to explore the evolution process and main research areas of AI-aided diagnosis for oral diseases between 2005 and 2025, identified new research areas, and provided useful guidance on future research and application topics.
Introduction
Oral health is essential to overall health and quality of life, yet oral diseases remain one of the major health threats worldwide. Epidemiological studies have shown that oral diseases are affecting almost 3.5 billion people worldwide, and the prevalence rate is up to 45% in general, significantly higher than any other non-communicable disease. 1 The common oral diseases are dental caries, periodontal disease, tooth loss, oral mucosal lesions, oral cancer, maxillofacial trauma, noma, and congenital malformations like cleft lip and palate. 2 These conditions induce pain and infection, impair nutritional intake and speech function, and may even jeopardize systemic health.3,4
Research demonstrates that most oral diseases are preventable and can be effectively controlled if detected early. 5 Therefore, the accurate and timely diagnosis of oral diseases is of profound significance for patient outcomes. Clinically, traditional diagnosis methods of oral disease include visual examination, probing, percussing, etc. They are usually supplemented with radiographic tools like Cone Beam Computed Tomography (CBCT) or X-rays that offer visual information for a conclusive diagnosis.6,7 However, such methods are highly dependent on the technician’s skill of the doctor performing the test, as well as their subjective judgment, which may compromise diagnostic accuracy and consistency. 8
Given the limitations of conventional diagnostic approaches, artificial intelligence (AI) is considered an effective complement for improving diagnostic objectivity and efficiency. 9 AI was first proposed in the 1950s, with the core objective focusing on machine systems capable of human intelligence simulation for task completion. Notably, over the past decade, the healthcare sector has emerged as a primary focus for AI-related equity investment, surpassing all other industries in capital allocation. 10 Concurrently, with ongoing technological advancements and digital transformation in dentistry, AI has become increasingly integrated into dental practice. Through the application of advanced algorithms and machine learning techniques, AI significantly improves the speed, accuracy, and efficiency of diagnostic processes.11,12 Extensive research has demonstrated that AI plays a crucial role in the diagnosis of dental caries and apical periodontitis,13,14 as well as in the early screening of oral cancer,15,16 and removable dental prostheses. 17
Despite progress in AI-based oral diagnostics, related research remains piecemeal and methodologically limited. Findings are scattered across multiple disciplines, lacking cross-domain knowledge graphs to clarify conceptual relationships.18,19 Two previous bibliometric studies in this field20,21 systematically sorted out the overall application pattern of artificial intelligence technology. Results show that current research hotspots are disease diagnosis, orthodontic intervention, and maxillofacial morphological segmentation, with disease diagnosis being the most prevalent, reflecting strong academic attention. A recent global bibliometric analysis covering 2000-2025 also confirmed the rapid growth and thematic concentration of AI research in dentistry, with major focuses on diagnostic imaging, deep learning, and radiological applications. 22 However, these studies did not focus specifically on AI in dental diagnosis, nor did they analyze key issues such as research trend evolution, key technical methods, and disease identification patterns.
Against this background, this study employed bibliometric analysis to quantitatively analyze the annual publication volume and growth patterns, identifying leading countries, institutions, and core scholars, while mapping collaborative networks. Through keyword clustering, time zone analysis, and burst analysis, it elucidated core themes, traces evolutionary trajectories, and pinpointed emerging frontier fields. The findings provided an overview of the status quo and development trend of AI-based oral disease diagnosis, which can offer some useful guidance both theoretically and practically for further studies.
Materials and methods
Data acquisition
We searched the Web of Science Core Collection (WoSCC, Clarivate Analytics) for relevant publications on AI-assisted diagnosis of oral diseases from January 1, 2005 to November 30, 2025. On December 2, 2025 at 13:00 (UTC+8, China Standard Time), the search and data export were carried out, and all retrieved records were exported in ISI Export Format (Version 1.0). The search strategy was as follows: TS=((“artificial intelligence” OR AI OR “machine learning” OR “deep learning” OR “convolutional neural network” OR “computer-aided diagnosis”) AND (“oral” OR “dental” OR “tooth” OR “Orthodontics” OR “Orthognathic” OR “periodont*” OR “caries” OR “oral cancer” OR “dental implant”) AND (“diagnosis*” OR “detect*” OR “classification” OR “image analysis”)) AND DT=(“article” OR “review”) AND PY=(2005-2025) AND LA=English. Inclusion criteria were: (1)studies on AI-assisted oral disease diagnosis; (2)research or review articles; (3)articles published in English. Two researchers independently screened the articles, with disagreements resolved by a third researcher or through discussion. Inter-reviewer agreement was assessed using Cohen’s kappa coefficient. A total of 3360 records were identified from the WoSCC database, and 2131 studies were ultimately included in the analysis. The retrieval process is shown in Figure 1. The retrieval process.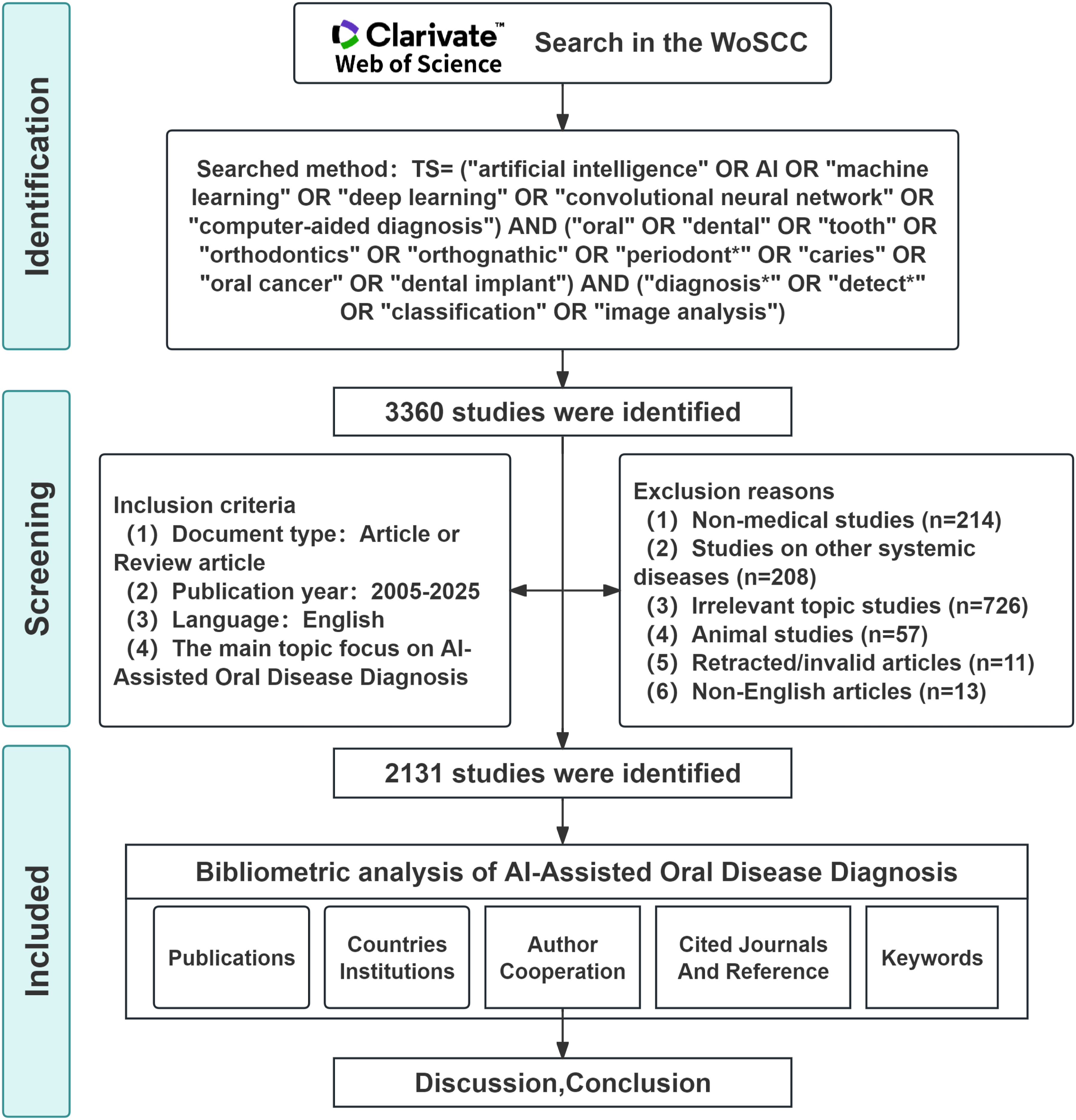
Data analysis
We imported the final dataset into CiteSpace 6.4.R1 (Drexel University, Pennsylvania, USA) in plain text format for bibliometric analysis. Prior to analysis, we standardized keywords, merged synonyms (e.g., deep learning and DL), and removed duplicates from the WoSCC to eliminate redundant nodes. The analysis included publications, countries, institutions, authors, journals, citations, co-occurrence, and keyword clustering. Bibliometric parameters were set as follows: Time Span = 2005-2025, Time Slice = 1, g-index= 25, Top N% = 10, Node types: Country, Institution, Cited journals and reference, Keyword; all other settings remained default. These settings are designed to balance the inclusion of representative nodes with the clarity of the network. To simplify network visualizations and reduce edge density, pathfinder pruning was applied to the author network (sliced only) and to the country, institution, keyword, and cited-reference networks (both sliced and merged); Minimum Spanning Tree (MST) pruning was applied to the cited-journal network across both sliced and merged datasets. In the maps, node size represents term occurrence frequency, and edge width denotes co-occurrence strength. Edge color transitions from purple (earliest publications) to red (most recent ones) to depict the publication timeline. Cluster analysis used the Log-Likelihood Ratio (LLR) algorithm and set γ= 0.65 with a minimum burst duration of two years to detect emerging topics while capturing knowledge base evolution. Sensitivity analysis tested stability using two g-index thresholds (k = 25 and k = 15).
Results
A total of 3360 articles were initially retrieved from the WoSCC database. After screening, 2131 studies were included in the final analysis. The inter-reviewer agreement for study selection was high (Cohen’s kappa = 0.876), demonstrating the reliability of the screening process.
Annual publication volume
Figure 2 showed that from 2005 to 2025, the number of published papers has generally been on the rise. Moreover, before 2017, the number of papers published each year was very low (fewer than 10). Starting from 2018, the number of papers increased rapidly, reaching a peak of 519 in 2024, followed by a slight decline in 2025, which may be associated with incomplete data retrieval. Annual publication volume of AI-assisted oral disease diagnosis (2005–2025).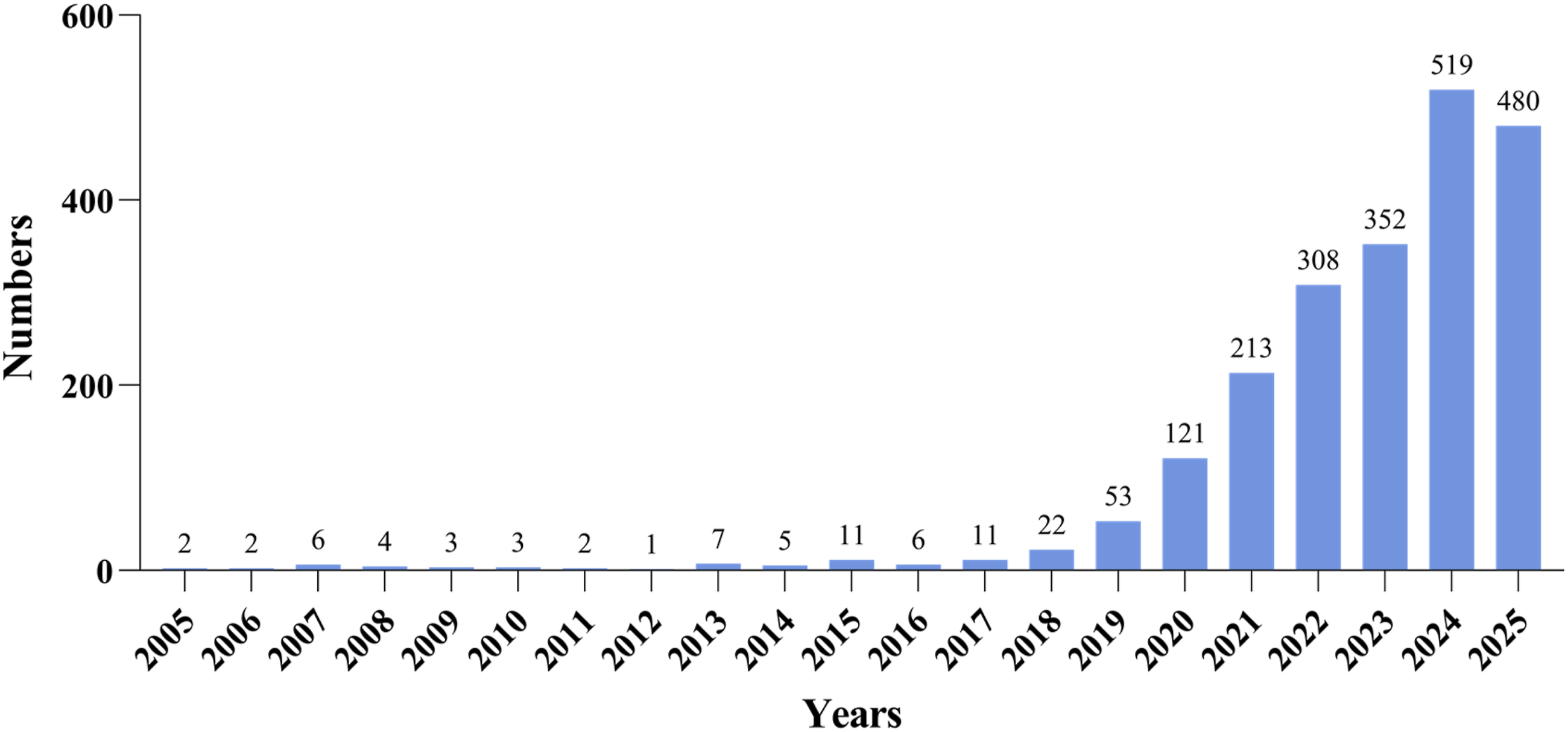
High-output countries and institutions
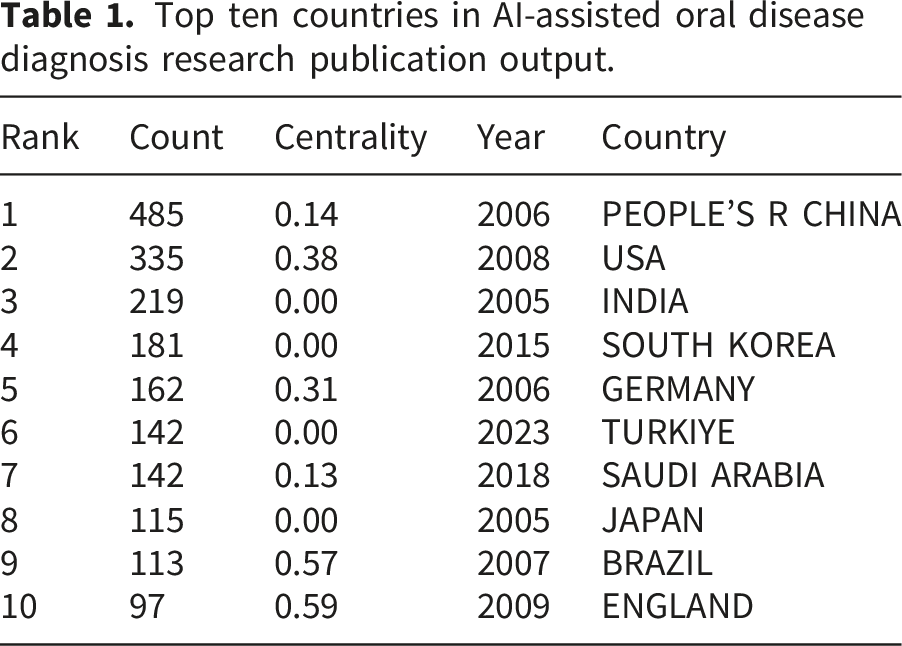
In terms of countries/regions (Figure 3(a)), China ranked first with 485 papers, leading research on AI-assisted diagnosis of oral diseases. This was followed by the USA, India, South Korea, and Germany. England occupied the highest position in betweenness centrality among these top ten countries/regions (Table 1), indicating its prominent role in global research collaboration. The top ten institutions published 491 papers, accounting for 23.04% of the overall publications. Four institutions in Berlin (Humboldt University of Berlin, Free University of Berlin, Charité-Universitätsmedizin Berlin, and the Berlin Institute of Health) published 224 papers, making up 45.62% of the top ten output. The institutional collaboration network (Figure 3(b)) supported this, as the nodes of these four Berlin institutions are large with distinct purple outer rings, showing high publication volume, centrality, and strong collaborative ties. Sichuan University and Peking University followed closely. Overall, universities contributed more publications than hospitals. Collaboration network of high-output countries and institutions in AI-assisted oral disease diagnosis: (A) Countries; (B) Institutions. Top ten countries in AI-assisted oral disease diagnosis research publication output.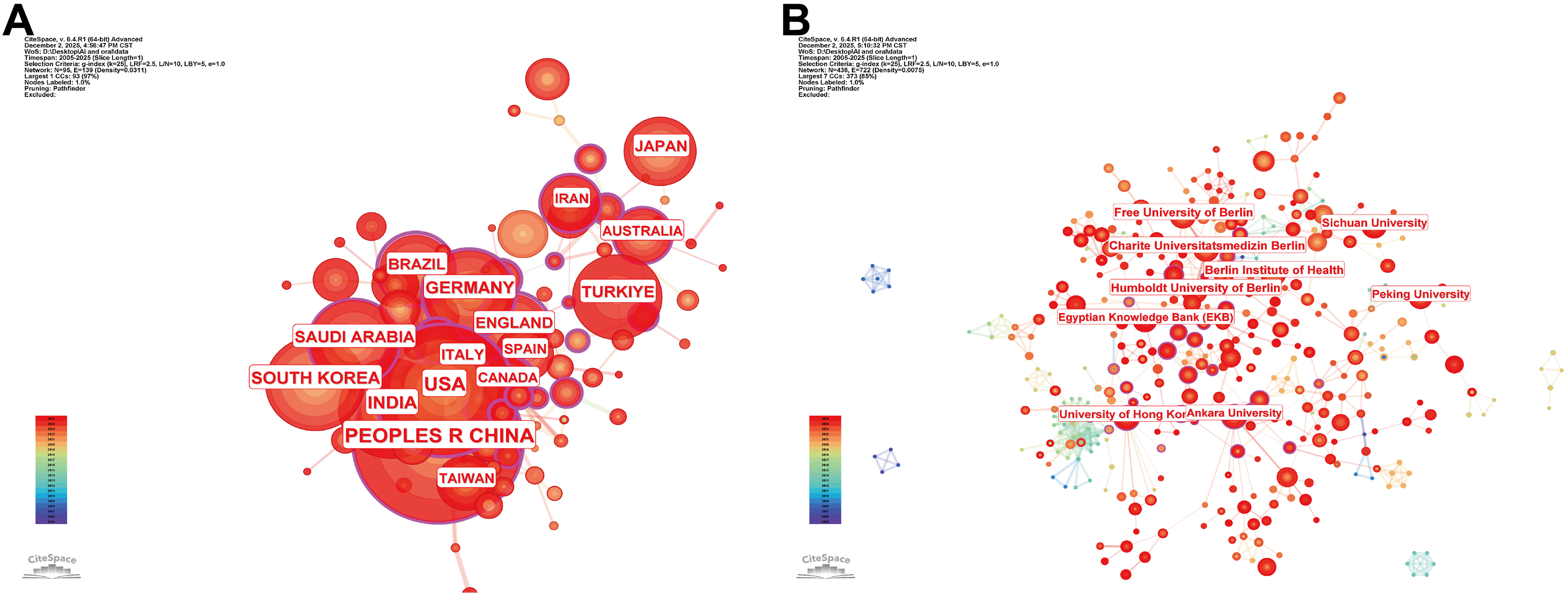
Author cooperation network map analysis
The author’s co-occurrence network built with CiteSpace 6.4.R1 has 801 nodes, 1,778 links, and a density of 0.0055 (Suppl.Figure S1). Falk Schwendicke was the most published author (45 articles). According to Price’s Law (M=0.749√Nmax), 23 the core author threshold was M≈5.02, so authors with >5 publications were core authors. Fifty met this criterion(26.8%), below the 50% benchmark, indicating no stable core author group in AI-assisted oral disease diagnosis.
Cited analysis of journals and references
Citation analysis is a valid criterion for evaluating academic paper quality.
24
Figure 4(a) showed the top three journals in co-citation: Scientific Reports (1,164), Journal of Dentistry (816), and Journal of Dental Research (764) (Suppl.Table S1). Seven journals are in medical/comprehensive sciences, and three are in computer science. Suppl.Table S2 listed the top 10 most cited papers, with visualizations in Figure 4(b). The most cited article by Lee JH (Journal of Dentistry, 2018)
25
designed a convolutional neural network (CNN) for caries diagnosis in periapical radiographs, achieving high AUC values, notably 0.917 for the premolar model, indicating good clinical relevance and supporting CNNs as effective tools. The second most cited paper by Schwendicke F (Journal of Dental Research)
11
provided a comprehensive review of AI applications in dentistry, exploring limitations and future prospects. The third study applied CNNs to tooth detection and numbering in panoramic X-ray images for dental chart digitization.
26
Co-citation networks of journals and references in the field of AI-assisted oral disease diagnosis, (A) Journal co-citation network, (B)Reference co-citation network.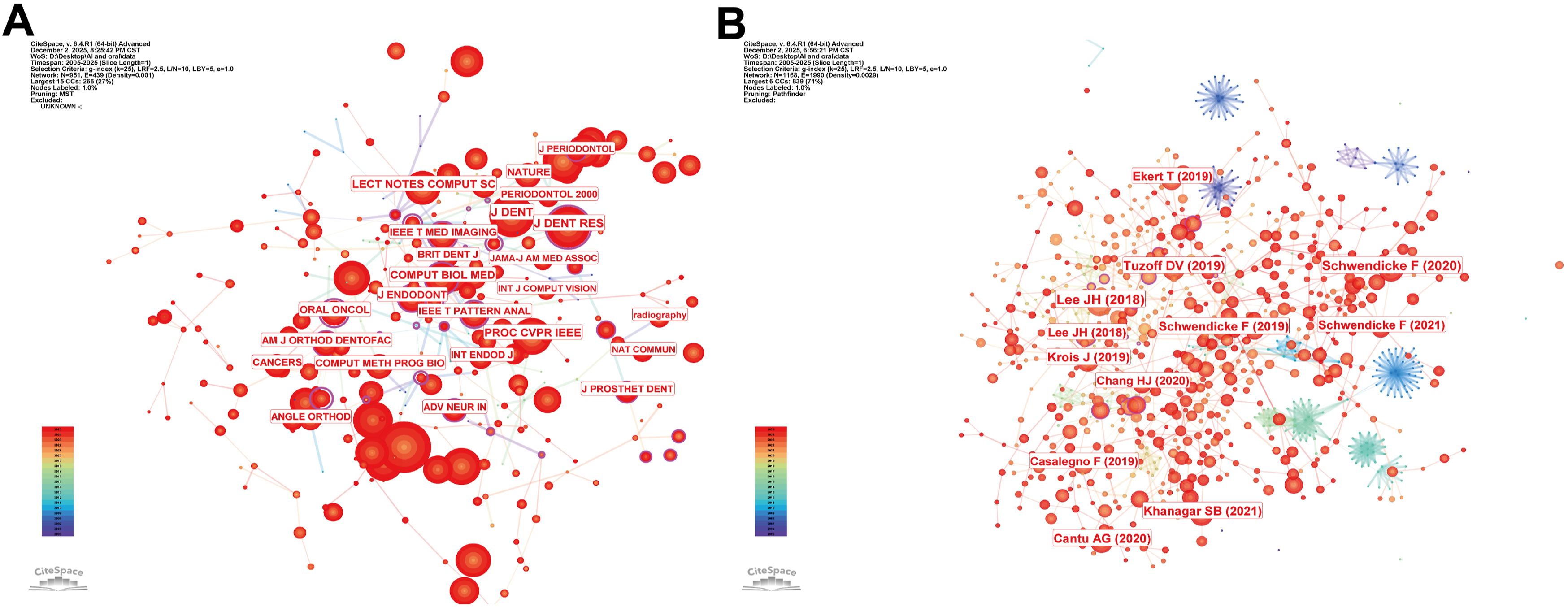
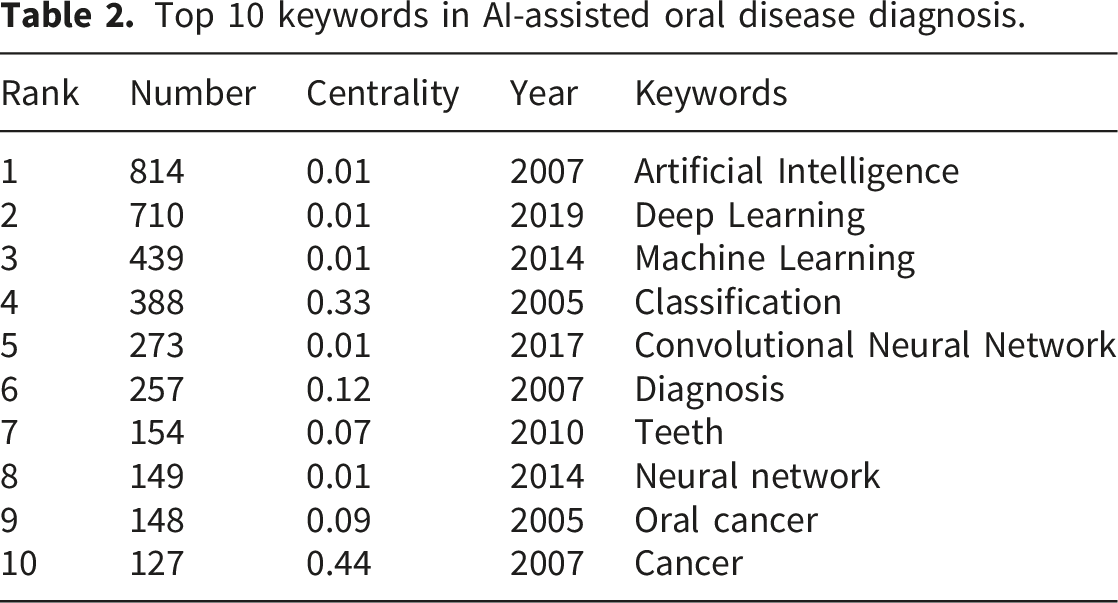
Keyword co-occurrence analysis
The Price formula (M = 0.749√Nmax) identifies core academic keywords,
27
highlighting those with over 21 occurrences as core keywords with larger nodes in the visualization, indicating research hotspots. Figure 5(a) showed CiteSpace’s co-occurrence and coverage, and Table 2 listed the Top 10 cited keywords. The top five core keywords were artificial intelligence, deep learning, machine learning, classification, and convolutional neural networks. Cancer, as a high-center disease, also received significant attention. Visualization maps of keywords in the field of AI-assisted oral disease diagnosis. (A) Keyword co-occurrence network, (B) Keyword cluster analysis. Top 10 keywords in AI-assisted oral disease diagnosis.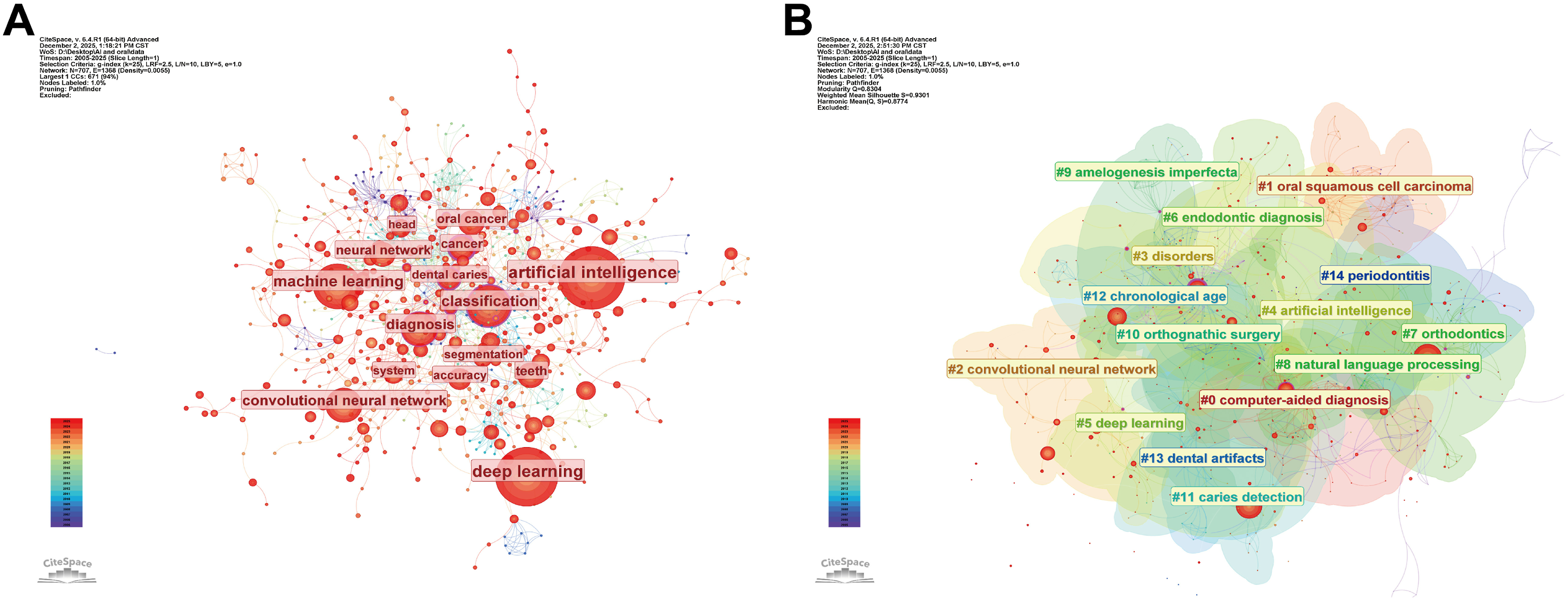
Keyword cluster and timeline map analysis
Core thematic clusters in AI-assisted oral disease diagnosis.
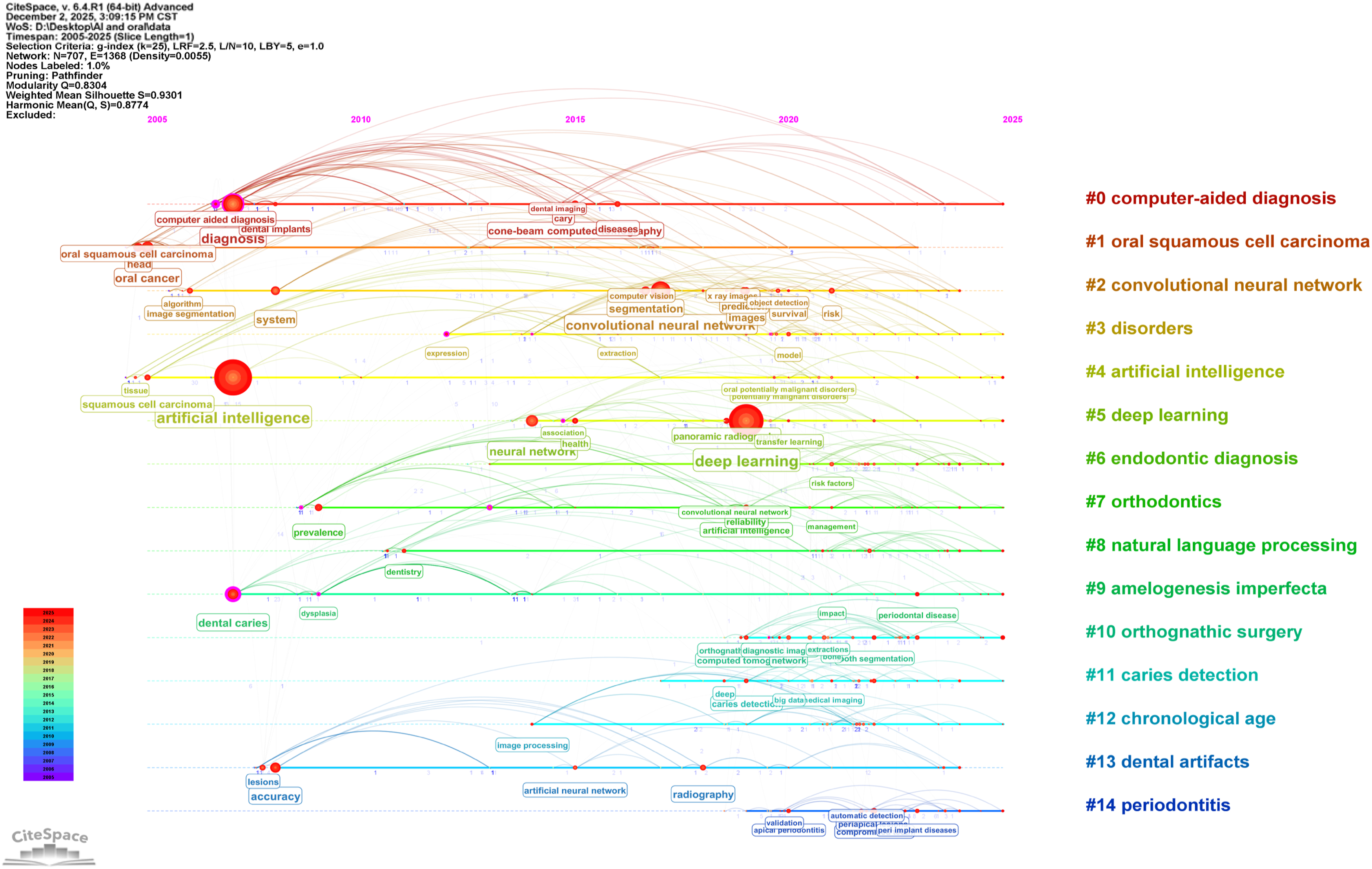
Timeline map of keywords in the field of AI-assisted oral disease diagnosis.
Keywords with the strongest citation bursts
Burst detection with fixed model coefficients(α=2.0, γ=0.65, Minimum Duration=2), 31 burst keywords identified and top 25 displayed. Figure 7 showed the burst detection and trend of the top 25 keywords since 2005, which detects keywords that have a statistically significant increase over time by identifying temporal patterns, capturing changes in research interests, and emerging research frontiers. “Computer-aided diagnosis” had the strongest burst (5.23), lasting from 2007 to 2017, followed respectively by “system” (4.75) and “extractions” (4.69). The top six high-burst keywords all emerged in 2020 (“human identification,” “recognition,” “big data,” “mathematical modeling,” “pattern,” and “object detection”), possibly due to the accelerated progress of AI technology. The burst of new keywords such as “periodontal bone loss” and “extractions” indicates a rising trend in applying artificial intelligence techniques to aid the diagnosis of other oral diseases, which could be potential research directions for further study. Top 25 keywords with the strongest citation bursts.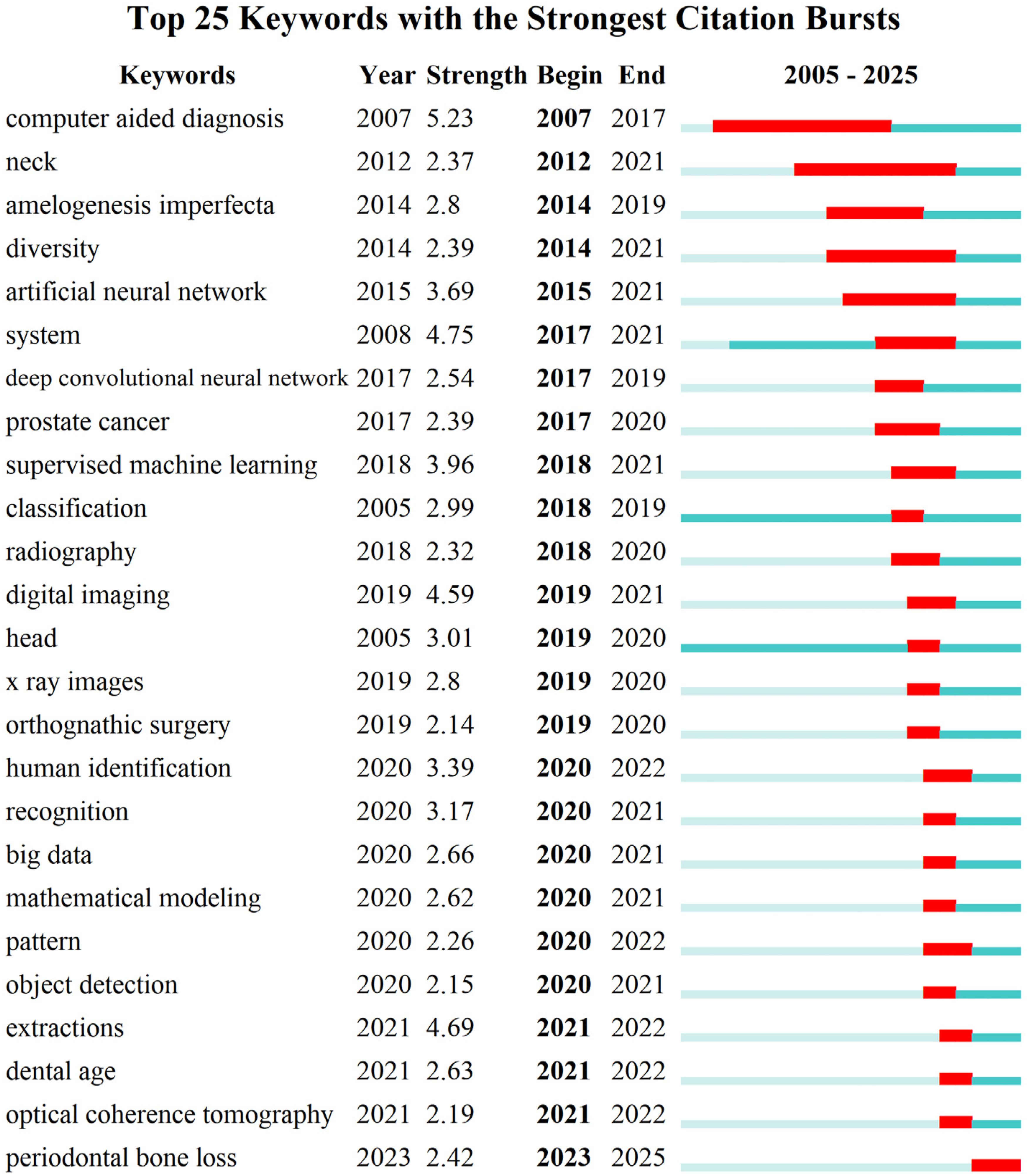
Sensitivity analysis
Sensitivity analysis indicated that lowering the g-index from 25 to 15 filters out low-frequency keywords and reduces the number of nodes from 707 to 486. Meanwhile, core clusters and top burst keywords remain stable, with only minor peripheral variations, which confirms the robustness of the results.
Discussion
This study conducted bibliometric and trend analyses of 2,131 WoSCC papers on AI-assisted diagnosis of oral diseases, identifying key authors, papers, institutions, and countries. Publications showed a sustained upward trend from 2005 to 2025. Similar to the findings of Özbey, F et al., 22 this developmental trajectory can be divided into three phases: slow and modest publication growth before 2018, followed by exponential growth across relevant indicators from 2018 to 2024. A temporary drop was observed in 2025 because literature collection ended in November. Nevertheless, the overall rising trend is expected to persist. This growth trend aligns closely with key milestones in AI development. The breakthrough of AlexNet in the 2012 ImageNet competition demonstrated the transformative power of CNNs in image recognition, marking the dawn of the deep learning era. 29 Subsequently, the widespread application of CNN in medical imaging analysis laid the technical foundation for AI research in dentistry. 25 Meanwhile, the maturation of generative AI and multimodal learning technologies is driving significant advancements in AI-assisted dental diagnosis research.30,31
Regarding national and institutional contributions,China, the U.S., and India ranked top 3 in publication volume due to high researcher activity and efficient funding. 32 Despite China’s high output, its global collaborative role was weak. In contrast, the US had higher intermediary centrality and served as an international cooperation hub. To promote the development of AI-assisted disease diagnosis, global scholars should enhance communication and foster interdisciplinary collaboration. Among the top ten high-output institutions, four are located in Berlin, with Humboldt University of Berlin leading in publications. The university has conducted AI research since 2002, when Dietmann S utilized feedforward neural networks to predict adjacent regions of protein molecular surface plaques, 33 indicating that Berlin’s universities started early and made significant contributions to the development of AI-assisted diagnosis.
Author co-occurrence analysis showed that only 50 core authors were responsible for a little more than half of all publications, revealing no well-established, coherent research community within the area of AI-assisted oral disease diagnosis and suggesting a large potential space to expand disciplines and promote academic exchanges. Most papers were published in journals including Scientific Reports (IF=3.9), Journal of Dentistry (IF=5.5), Journal of Dental Research (IF=5.9), and Dentomaxillofacial Radiology (IF=4.1), which primarily focus on dentistry or computer science, with a relatively low proportion of interdisciplinary publications. Among the top ten cited studies, six utilized AI-assisted image recognition technology, highlighting its critical role in clinical diagnostic decision support. In terms of oral disease types, highly cited studies predominantly focused on periodontal disease and dental caries, likely due to their high prevalence and reliance on imaging examinations.
Keyword clustering and timeline analyses revealed that the initial stage of AI-assisted oral disease diagnosis research primarily focused on disease classification, particularly oral cancer. Aubreville et al. developed a deep learning model for automatically classifying cancerous tissue in subsurface microanatomical images obtained via confocal laser endomicroscopy(CLE). 34 This model outperformed traditional CLE image interpretation methods with 88.3% average accuracy. However, AI applications were limited in scope and technical advancement, reflecting a conservative, foundational development stage. Per the China ICT Academy, since early 2018, AI-enabled healthcare has emerged as one of the most prominent vertical application domains for artificial intelligence. 35 AI technology in the field of oral disease diagnosis has made both quantitative and qualitative progress. Current applications cover a wide range of diagnostic tasks, including deep learning-based periodontal disease screening image analysis, 36 three-dimensional digital phenotyping for periodontal and peri-implant tissue assessment, 37 and CBCT-based temporomandibular joint disorder detection. 38 Recent studies have further demonstrated that AI-assisted pathological analysis significantly enhances sentinel lymph node (SLN) metastasis detection in melanoma and head and neck cancers (HNC), reducing reliance on time-consuming and costly immun-ohistochemistry (IHC) procedures.39,40 Based on these findings, Sreeram et al. 41 proposed that AI has transformative potential for early lymph node metastasis detection across multiple cancer types, including oral cancer, by improving both diagnostic accuracy and clinical efficiency through computational pathology. Collectively, these advances indicate AI’s role in dentistry extends beyond imaging assistance, enabling deeper integration into diagnostic workflows and clinical decision-making.
From 2007 to 2017, “computer-aided diagnosis” dominated early AI research in dentistry with the strongest burst strength, driven by advances in “digital imaging” and “artificial neural networks,” which established the foundation for image-based automated diagnosis. After 2020, advances in deep learning and big data drove surges in “recognition,” “object detection,” “big data,” and “mathematical modeling,” marking a shift from single-task image classification to intelligent multimodal systems for full clinical workflows. This aligns with natural language processing (NLP), which parses clinical notes and integrates imaging data through knowledge graphs to support personalized treatment planning. 42 Furthermore, recent advances in NLP and large language models (LLMs) have facilitated the development of multimodal artificial intelligence systems capable of integrating imaging data, clinical records, and textual information, thereby providing more comprehensive support for clinical decision-making. Recently, growth in “optical coherence tomography” and “periodontal bone loss” burst strength indicates a shift in digital dentistry from 2D imaging to 3D microstructural quantification. 43 This technology provides a high-quality data foundation for AI-assisted diagnosis. Existing studies have demonstrated that deep learning models achieve an accuracy rate of 97% in detecting periodontal bone loss, with some models performing even better than clinicians in specific scenarios. 44 However, translating research findings into clinical practice remains challenging. While most models exhibit excellent accuracy, sensitivity, and specificity under standardized conditions, variability in image quality and significant individual patient heterogeneity in real-world clinical settings significantly compromise their actual performance. 45 Models with high specificity and low sensitivity are prone to missed diagnoses, delaying treatment; conversely, models with high sensitivity and low specificity are susceptible to misdiagnosis, leading to unnecessary diagnostic procedures. 46 Therefore, it is essential to enhance model calibration, external validation, and interpretability to promote the clinical application of AI in oral diagnosis.
Moreover, the privacy and security of large-scale imaging datasets require careful consideration, particularly when multi-center data sharing is involved. Strict protection of patient information from leakage must be ensured through standardized informed consent procedures, data anonymization, and federated learning techniques. In addition, differences in demographic characteristics, geographic regions, and clinical settings may affect the representativeness of training datasets and potentially introduce algorithmic bias. 47 The limited interpretability of certain deep learning models may also reduce clinician trust and hinder clinical implementation. 48 These challenges highlight the importance of improving fairness, transparency, explainability, and standardized validation in future AI research and clinical applications.
Future oral diagnosis AI systems will not be limited to image data analysis. They will integrate large language models like ChatGPT-5.2 with reasoning capabilities. 49 These models can combine imaging findings, patient records, and clinical descriptions to improve diagnostic accuracy and reduce misdiagnosis. 50 Besides integrating imaging and clinical data, researchers should create standardized, publicly accessible oral imaging datasets with diverse demographics and samples from multiple centers, along with unified evaluation criteria. Additionally, regular multi-center external validation and optimization of model interpretability are crucial for the reliability and fairness of AI-based oral diagnosis technologies, enabling their clinical application.
Limitations
This study has several methodological limitations. First, it only used WoSCC for literature retrieval, excluding Scopus and PubMed, which may have caused missed publications and reduced dataset comprehensiveness and representativeness. Second, despite using a combined search strategy, some dental-specific terms were not systematically included, possibly leading to underrepresentation of specific diagnostic themes. Third, biases in CiteSpace’s parameter settings and measurement algorithms may have affected the objectivity of co-occurrence and clustering analyses. Fourth, theme clustering mainly relied on high-frequency keyword distribution with manual interpretation, introducing subjective bias. Fifth, including only English-language literature causes language bias and may reduce the representation of non-English-speaking countries’ research. Sixth, as a retrospective bibliometric analysis, conclusions are limited by the literature’s temporal scope and disciplinary evolution, making it hard to reflect recent advancements.
Conclusions
In summary, AI applications in medical diagnosis are now widespread and a key research area in the interdisciplinary field of medicine and information science. CiteSpace analysis shows AI research in oral disease diagnosis is expanding. Studies have evolved from basic models to advanced algorithms, with current efforts focused on clinical needs. Future research should prioritize multimodal data and explainable algorithms to develop precise, transparent AI systems, advancing oral healthcare toward personalization, precision, and universal access. Additionally, for complex clinical decisions, manual verification must be retained to enable AI to better assist oral diagnosis and treatment.
Supplemental material
Supplemental material - Visualization of artificial intelligence applications in oral disease diagnosis: A bibliometric analysis
Supplemental material for Visualization of artificial intelligence applications in oral disease diagnosis: A bibliometric analysis by Fangfang Liang, Ziyi Wang, Haonan Li, Panpan Zhang, Jing Shen in DIGITAL HEALTH
Footnotes
Ethical consideration
Only public bibliographic metadata were analyzed without involving human or identifiable data, so ethical approval was not needed.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Tianjin Natural Science Foundation Project (24JCZDJC00880) and Project of Tianjin Nursing Association (tjhlky2024QN12).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no relevant conflicts of interest. No conflict of interest exists in the submission of this manuscript, and the manuscript is approved by all authors for publication. I would like to declare on behalf of my co-authors that the work described was original research that has not been published previously, and not under consideration for publication elsewhere, in whole or in part. All the authors listed have approved the manuscript that is enclosed.
Data Availability Statement
Data is provided within the manuscript or supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.