
Abstract
Objectives
This study assessed knowledge, perceptions, and readiness to use e-pharmacy services among adults in Syria, and examined demographic predictors of awareness and readiness.
Methods
A cross-sectional online survey was conducted between November and December 2025 among adults aged ≥18 years residing in Syria. The questionnaire recorded demographic characteristics, prior awareness and use of e-pharmacy, perceived benefits and disadvantages, and readiness to adopt e-pharmacy services.
Results
A total of 600 participants completed the survey. Half (50.2%) had heard of e-pharmacy, while only 14.3% had previously used such services. Perceived benefits received high agreement (mean 3.94/5), especially regarding convenience, time savings, and protection during epidemics. Perceived disadvantages were moderate (mean 3.56/5), with concerns related to privacy, communication errors, and reduced interpersonal interaction. Overall, 53.7% expressed willingness to use e-pharmacy, with the strongest interest in adherence monitoring (79.8%), home medication reviews (78.2%), and side-effect follow-up (74%). In multivariate analysis, higher education, medical-related fields, higher income, female gender, and not having children predicted greater knowledge. Readiness was independently associated only with income and marital status.
Conclusions
Syrian adults show favorable perceptions and moderate readiness toward e-pharmacy despite low actual use. Addressing digital infrastructure gaps, enhancing digital literacy, and strengthening regulatory frameworks may support broader integration of e-pharmacy into Syria’s evolving digital health ecosystem.
Keywords
Introduction
Digital transformation has become a central pillar of modern health systems, with digital health solutions being increasingly integrated into service delivery worldwide. The global expansion of internet access and mobile technologies has accelerated the adoption of online health services, including telemedicine and electronic pharmaceutical services. Digital technologies are considered essential for strengthening health systems, improving access, and promoting equity in healthcare delivery1.
E-pharmacies represent a rapidly growing model for medication distribution, as it enables consumers to order prescription and non-prescription medicines online, often combined with home delivery and remote pharmaceutical consultation. Systematic studies have highlighted that online pharmacy services can enhance accessibility, reduce travel burden, and improve medication continuity, particularly in geographically underserved areas. 2 Moreover, the COVID-19 pandemic increased the adoption of e-pharmacy services, becoming an integral component of modern pharmaceutical care. 3
Despite the potential benefits of e-pharmacy services, significant barriers remain to their adoption. These include concerns regarding medication authenticity, regulatory oversight, cybersecurity, and patient safety. Consumer trust, perceived usefulness, and perceived ease of use strongly influence the intention to adopt online pharmacy services. 4
Syria’s healthcare system operates under a mixed public–private model, with pharmacies widely distributed across urban areas but less accessible in rural regions. Community pharmacies serve as the primary point of care for many citizens, particularly given the limited availability of physicians and the common practice of pharmacist-led counselling. Prescribing and dispensing are not strictly separated in practice, and many patients rely on pharmacists for diagnosis and medication advice. The prolonged conflict has further fragmented service delivery, damaged infrastructure, and widened regional disparities in access to medicines, making e-pharmacy services of great potential. 5
Accordingly, this study aims to assess the level of acceptance and readiness of the Syrian population to use e-pharmacy services, exploring public perceptions, their readiness to utilize these digital platforms, and potential factors influencing their adoption. The findings provide insights into how digital pharmaceutical services can be optimally designed to meet patients’ needs in Syria.
Materials and methods
Study design, setting, and sampling method
In this study, ‘e-pharmacy’ refers to digital pharmaceutical services delivered through online platforms, including 1 online ordering of prescription and non-prescription medications, 2 remote pharmacist consultation, 3 electronic dispensing and home delivery, and 4 digital medication management services such as adherence monitoring and follow-up of side effects.
This cross-sectional survey targeted adults aged 18 years or older residing in Syria. Participants were recruited from multiple regions across Syria. All questionnaire items were mandatory to prevent missing responses. Emails were recorded to avoid duplication. The questionnaire was administered online via Google Forms and shared on social media platforms, namely Facebook and WhatsApp. Data were collected for 60 days between the 1st of November 2025 and the 31th of December 2025.
A convenience sampling approach, supplemented by snowball sampling, was used due to the practical constraints of conducting population-based research in Syria. Limited access to a national sampling frame and regional instability made probability sampling unavailable. At the same time, online distribution through social media platforms allowed efficient recruitment across diverse regions, and snowball sampling helped reach individuals who might otherwise be inaccessible.
At the beginning of the questionnaire, participants received an introductory statement explaining the study objectives and assuring confidentiality. Respondents were also encouraged to share the survey link with others in their network to increase participation.
Development of the survey
The study questionnaire was adapted from a previously published Jordanian study, since the Syrian and the Jordanian populations are very similar in terms of culture. 6 The initial draft was reviewed by the supervising professor, who assessed the content, clarity, and design of the questionnaire. Appropriate modifications were made to ensure that the questions were suitable for the Syrian community and understandable for the target population. No major modifications were made.
The finalized Arabic version of the questionnaire (Supplemental File) was structured into four sections. The first section collected participants’ demographic and social information. Monthly income was self-assessed by participants. Students studying medicine, pharmacy, or dentistry were considered students in a medical specialty, while others were considered students of a non-medical specialty. Section two included Knowledge and usage variables assessment via yes or no questions whether the participant had heard or used e-pharmacy before. Sections three and four assessed Perceptions of e-pharmacy using two structured Likert-scale domains adapted from a previously validated questionnaire. The third section measured perceived benefits of e-pharmacy and consisted of ten items evaluating participants’ agreement with potential advantages such as convenience, time savings, improved access, and enhanced safety during epidemics. The fourth section assessed perceived disadvantages using seven items addressing concerns related to privacy, communication quality, reduced interpersonal interaction, and potential risks associated with virtual medication services. All items in both sections were rated on a five-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. For each section, item responses were averaged to generate composite scores, with higher values indicating stronger agreement with the perceived benefits or disadvantages. The Arabic version of the original scales was obtained from the Jordanian study and demonstrated strong internal consistency in prior validation studies, with Cronbach’s alpha coefficients of 0.90 for the benefits domain and 0.867 for the disadvantages domain, indicating acceptable internal consistency. 7 Permission to use and adapt the questionnaire was obtained from the original authors.
Sample size calculation
The sample size for this study was determined based on the recommendations for logistic regression analysis. 8 According to these guidelines, 5–20 participants are required per independent predictor. Considering the upper limit of 20 participants per predictor and a total of 10 predictors, the minimum required sample size was 200 participants.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki to ensure participants’ rights and privacy were protected. Ethical approval to conduct this study was obtained from the Ethical Committee at the International University for Science and Technology (IUST) (ID: PH-26-5). Prior to completing the study questionnaire, all participants provided consent. The questionnaire included a statement explaining the voluntary nature of participation, and participants confirmed their consent by selecting the “Agree to participate” option before proceeding to the study questions. Data were stored on a password-protected device accessible only to the research team. No IP addresses or identifying information were collected.
Statistical analysis
The data collected through Google Forms were downloaded as an Excel file and subsequently imported into IBM SPSS Statistics 26 (Statistical Package for the Social Sciences) for statistical analysis. Data were analyzed using descriptive and inferential statistical methods. Categorical variables such as gender, educational level, field of study, monthly income, marital status, having children, knowledge of e-pharmacy, and readiness to use e-pharmacy were summarized using frequencies and percentages. Continuous variables, including age and Likert-scale scores, were presented as means and standard deviations.
The Pearson Chi-square test was applied to assess relationships between all categorical demographic variables and the outcome measures related to acceptance and readiness. For the variable of age, the Mann–Whitney U test was used to evaluate differences between the two groups due to non-normal distribution.
In addition, univariate logistic regression analysis was conducted to investigate the association between each demographic variable and the study outcomes, including participants’ knowledge, acceptance, and readiness toward e-pharmacy services. Subsequently, multivariate logistic regression analysis was performed to further examine these associations within the same statistical model. All assumptions required for logistic regression were assessed and met. The data showed no evidence of multicollinearity among independent variables, as variance inflation factors were within acceptable limits. Linearity of continuous variables with the logit was verified, and no influential outliers were detected. The sample size was adequate for the number of predictors, ensuring model stability. Therefore, the logistic regression models were considered appropriate and valid for interpretation. Statistical significance was defined as a p-value less than 0.05.
Results
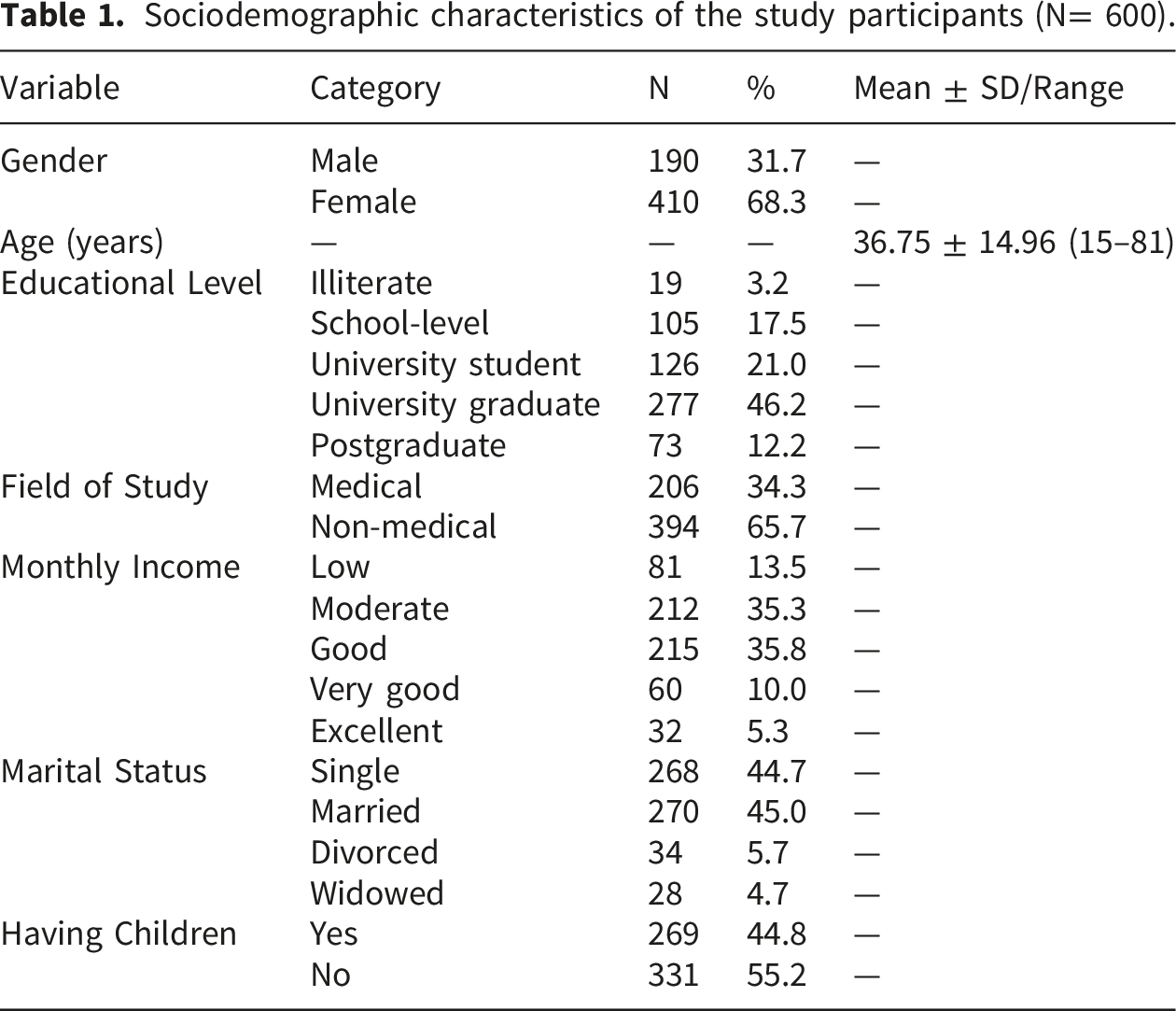
A total of 600 participants responded and completed the questionnaire, most of whom were female (n = 410, 68.3%). Participants had a mean age of 36.75 ± 14.96 years, with ages ranging from 15 to 81 years. Among the participants, 277 (46.2%) were university graduates.
Sociodemographic characteristics of the study participants (N= 600).
Knowledge and use of E-Pharmacy
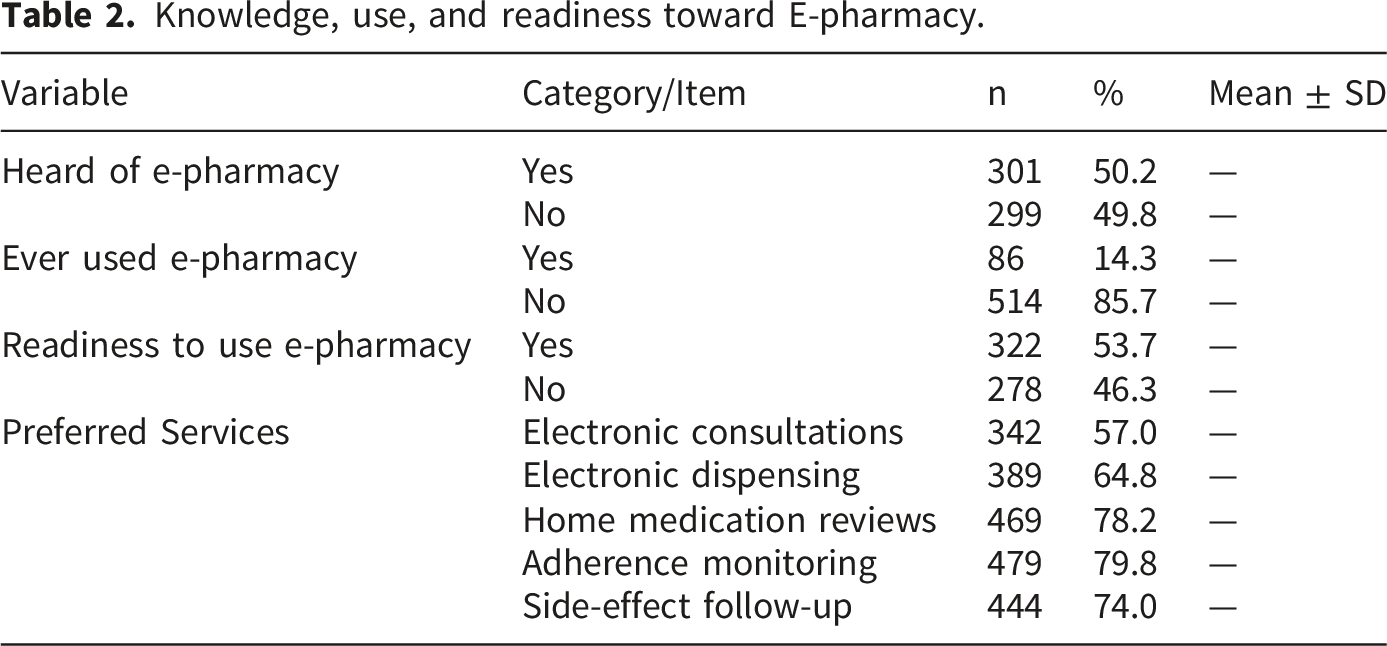
A total of 301 participants (50.2%) reported having heard of e-pharmacy, while 299 (49.8%) had not. Only 86 participants (14.3%) had previously used e-pharmacy services, whereas 514 (85.7%) had never used them.
Readiness to use E-Pharmacy
Knowledge, use, and readiness toward E-pharmacy.
Perceptions of E-Pharmacy
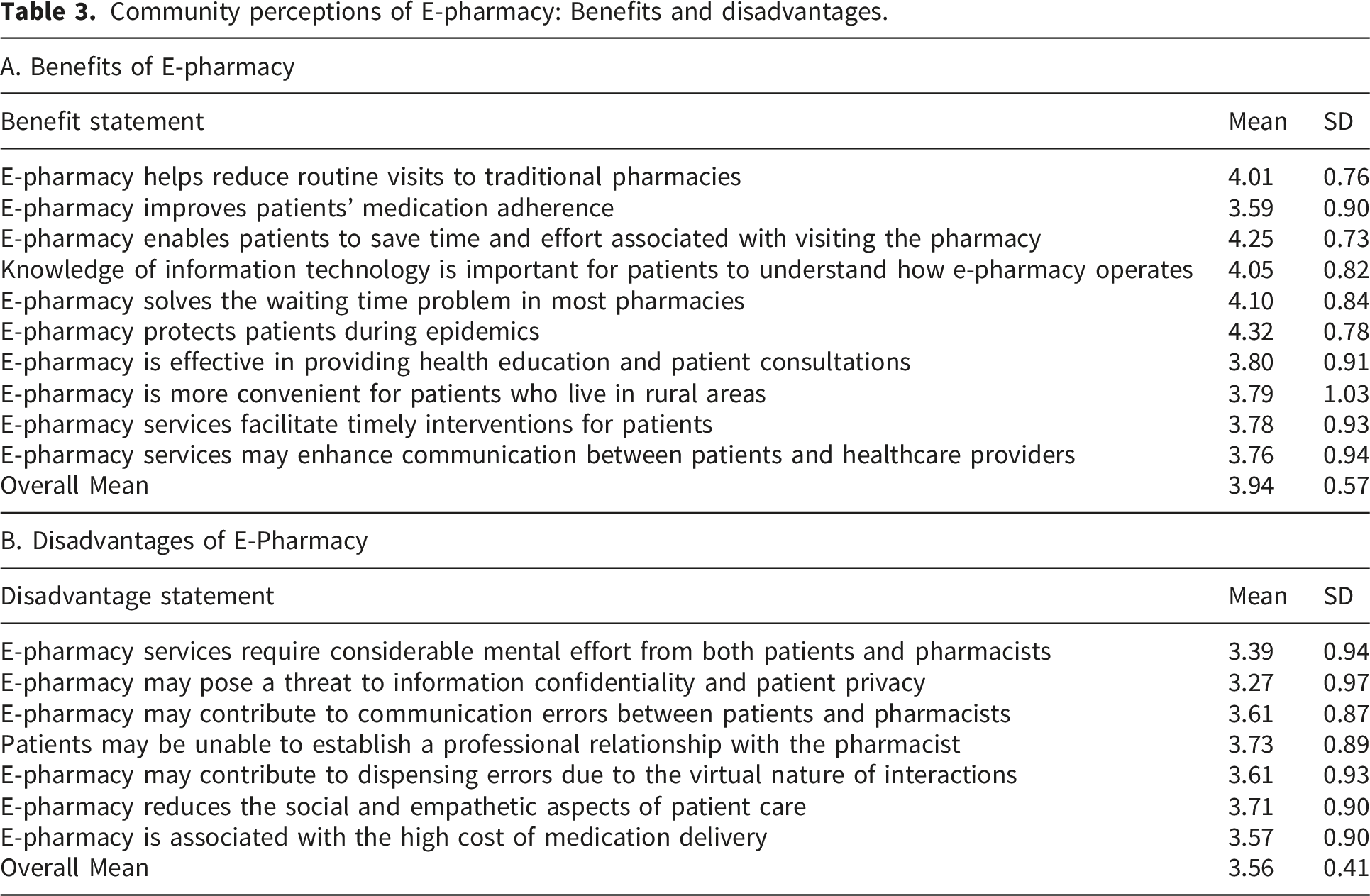
Community perceptions of E-pharmacy: Benefits and disadvantages.
Knowledge of e-pharmacy varied across demographic groups. Females demonstrated higher knowledge than males, and participants with knowledge were younger on average than those without knowledge. Educational level showed a clear gradient, with knowledge increasing steadily from illiterate participants to those holding postgraduate degrees. Participants in medical fields reported higher knowledge than those in non-medical fields, and higher monthly income was also associated with increased knowledge. Marital status showed notable variation, with divorced and single participants demonstrating higher knowledge levels than married or widowed individuals. Participants without children also showed higher knowledge than those with children.
Associations between demographic variables and knowledge and readiness to use E-pharmacy.
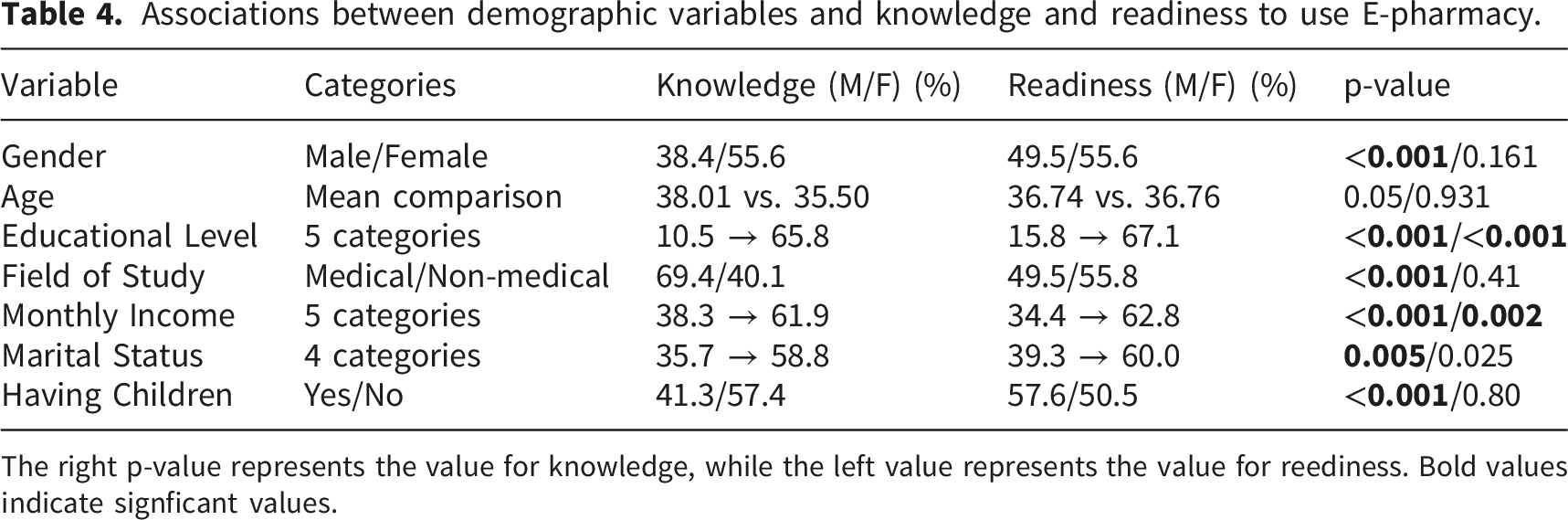
The right p-value represents the value for knowledge, while the left value represents the value for reediness. Bold values indicate signficant values.
Regression analysis
In the univariate logistic regression model for knowledge of e-pharmacy, all demographic variables were significant predictors. Females had higher odds of knowledge compared with males, and younger age was associated with slightly higher odds. Higher educational levels and being in a medical field both increased the likelihood of knowledge, as did higher monthly income. Marital status also showed an effect, with non-married groups having higher odds of knowledge, and participants without children were more likely to have knowledge than those with children. In the multivariate model, all variables remained significant except age and marital status.
Univariate and multivariate logistic regression for predictors of knowledge and readiness to use E-pharmacy.
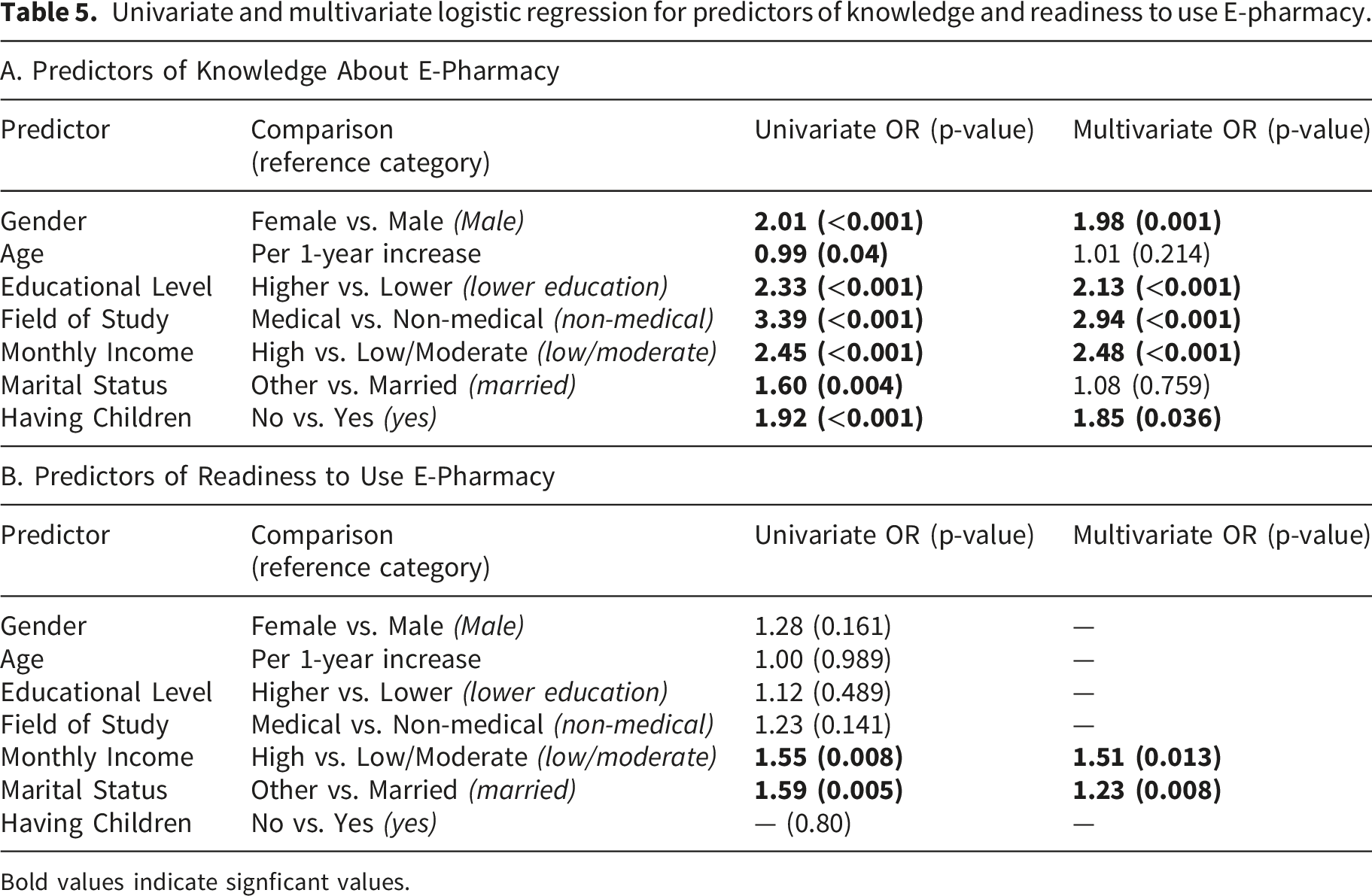
Bold values indicate signficant values.
Discussion
This study examined knowledge, perceptions, and readiness to use e-pharmacy services in Syria, along with the demographic factors influencing these outcomes. Compared with traditional pharmacies, e-pharmacy may improve access for individuals in remote areas, reduce travel costs, and support continuity of care. However, in settings like Syria where face-to-face pharmacist interaction substitutes for physician care, the shift to digital platforms may raise concerns about communication quality and trust.
The findings reveal a population that is moderately aware of e-pharmacy and generally receptive to its potential benefits, yet actual utilization remains low. The current situation in Syria regarding digital health integration is complex. The country’s infrastructure before the war in 2011 was not built with digital health services in mind, and was later destroyed during the war. On the other hand, the transitional government has shown promising interest in shifting focus to health sector modernization as a part of its national recovery strategy through integrating digital health systems, rebuilding infrastructure, and securing international partnerships, 9 with further facilitation of e-pharmacy by the Ministry of Communications lifting previous restrictions on electronic applications, 10 allowing tech startups to launch via simple notification rather than a lengthy licensing process. However, the results of these efforts are likely to take years before being visible. Moreover, E-pharmacy applications are only currently active in Damascus, Aleppo, Idlib, and Lattakia, leaving most Syrian cities out of E-pharmacy coverage.
Although half of the participants had heard of e-pharmacy, only a small proportion had ever used such services. This gap between awareness and actual use is consistent with patterns observed in other low- and middle-income settings, where digital health services remain underdeveloped. Limited availability of e-pharmacy platforms, insufficient digital infrastructure, and lack of regulatory frameworks may contribute to low adoption, all of which are present in the Syrian context as mentioned before. Additionally, cultural preferences for face-to-face interactions with pharmacists, an important factor for the elderly looking for social interaction, may discourage individuals from transitioning to online services despite being aware of them.11,12
Participants expressed strong agreement with the benefits of e-pharmacy, particularly regarding convenience, time savings, and enhanced safety during epidemics. These findings align with global evidence showing that convenience and reduced exposure to infectious environments are major drivers of e-pharmacy acceptance, along with variety, home delivery, and competitive prices. 13 The high rating for epidemic-related protection is especially relevant in the post-COVID-19 context, where digital health solutions gained prominence. 14
In contrast, participants reported moderate concerns about disadvantages, including privacy risks, communication errors, and reduced personal interaction. These concerns are well-documented barriers to digital health adoption and may reflect limited trust in online systems and fear of data breaches. 15 Addressing these concerns through clear regulations, secure platforms, and pharmacist training in telecommunication could improve public confidence. 16 Examples of these measures is Ministry of Health Decision No. 4 of 2026, which sets conditions for the registration and digital tracking of pharmaceutical products, 17 but e-pharmacy environment in Syria is still far from perfect.
More than half of the participants indicated willingness to use e-pharmacy services, suggesting substantial potential demand. The highest acceptance was observed for clinical support services such as adherence monitoring, home medication reviews, and follow-up of side effects. This pattern indicates that participants value pharmacist involvement in ongoing medication management and may view e-pharmacy as a tool to enhance—not replace—traditional care. 18 Lower acceptance of electronic dispensing and consultations may reflect concerns about accuracy, trust, or the perceived need for in-person evaluation. 16 The latter is important in Syria, where people with low incomes depend on pharmacists instead of doctors as primary counselors, making giving up face-to-face interactions unfeasible for this demographic. 19
Knowledge of e-pharmacy varied significantly across demographic groups. Women demonstrated higher knowledge than men, which may reflect their greater involvement in family health decisions and medication management. 20 Younger participants were more knowledgeable, likely due to higher digital literacy and greater exposure to online services. Education showed a clear gradient, with higher levels strongly associated with greater knowledge, consistent with evidence linking digital health literacy to educational attainment. 21
Participants in medical fields had substantially higher knowledge, which is expected, given their professional exposure to healthcare technologies. 22 Higher income was also associated with greater awareness, possibly due to better access to digital devices and internet connectivity, a factor that is also very important in the Syrian context. 23 Marital status and having children were associated with knowledge in univariate analysis, but these associations disappeared in the multivariate model, suggesting that their effects were mediated by other demographic factors such as education and income.
In contrast to knowledge, readiness to use e-pharmacy was influenced by fewer demographic variables. Only monthly income and marital status remained significant predictors in both univariate and multivariate analyses. Higher income may facilitate access to digital tools and reduce concerns about delivery costs, an important factor for low-income Syrians, where there is a general perception that electronic services are more expensive, while single individuals may be more open to adopting new technologies. 24 The lack of association with gender, age, education, field of study, and having children suggests that readiness is shaped more by perceived usefulness and trust than by sociodemographic characteristics.
An interesting finding was that participants in medical fields showed lower readiness than those in non-medical fields, despite having higher knowledge. This may reflect greater awareness of potential risks, such as medication errors or communication challenges, among healthcare professionals. This discrepancy highlights the need for targeted engagement with medical personnel to ensure their support for e-pharmacy implementation.
The findings indicate strong potential for expanding e-pharmacy services in Syria, provided that key barriers are addressed. Policymakers should prioritize developing regulatory frameworks that ensure patient safety, data privacy, and quality of care. Public awareness campaigns and digital literacy initiatives may help bridge the gap between knowledge and readiness. Pharmacists should receive training in telepharmacy communication to maintain the quality of patient interactions in virtual settings. Improving internet infrastructure and ensuring affordable access to digital tools will also be essential for equitable adoption.
Conclusion
These findings have important implications for Syria’s post-conflict digital health recovery. The moderate readiness observed suggests that e-pharmacy could expand meaningfully, but only if structural barriers are addressed. Years of conflict have damaged telecommunications networks, created regional disparities, and limited digital health initiatives to major cities such as Damascus, Aleppo, Idlib, and Lattakia. As a result, large segments of the population remain without access to online pharmaceutical services. Strengthening digital infrastructure and implementing secure, regulated platforms will be essential to build public trust. Because many Syrians rely on community pharmacists as their primary source of medical advice, e-pharmacy models should complement existing pharmacy roles rather than replace face-to-face interactions. The strong interest in adherence monitoring and home medication reviews indicates that e-pharmacy could help address gaps in chronic disease management, particularly in underserved regions. A national digital health strategy that integrates e-pharmacy, improves digital literacy, and ensures equitable access would support safer and more effective implementation as Syria continues rebuilding its health system. The same principles could be of use for other low income countries.
Limitations
This study has a few limitations that should be considered. Because the survey was distributed online using convenience and snowball sampling, the sample may not fully represent the entire Syrian population in every governorate. Moreover, because participation required internet access, individuals with limited connectivity—particularly older adults, rural residents, and lower-income groups—may be underrepresented. This may have resulted in a sample with higher digital literacy than the general population, potentially inflating awareness and readiness estimates. The cross-sectional design also limits the ability to draw causal conclusions from the observed associations. Finally, the study relied on self-reported responses, which may be influenced by recall or social desirability tendencies.
Supplemental material
Supplemental material - Knowledge, perceptions, and readiness to use electronic pharmacy services among the Syrian population: A cross-sectional study
Supplemental material for Knowledge, perceptions, and readiness to use electronic pharmacy services among the Syrian population: A cross-sectional study by Mohammad Basheer Alameer, Zahra Kabbani, Reem Alsamara, Rana Habeeb and Kenda Jawich in Digital Health.
Footnotes
Acknowledgements
The authors would like to thank the participants.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki to ensure participants’ rights and privacy were protected. Ethical approval to conduct this study was obtained from the Ethical Committee at the International University for Science and Technology (IUST) (ID: PH-26-5).
Consent to participate
Prior to completing the study questionnaire, all participants provided consent. The questionnaire included a statement explaining the voluntary nature of participation, and participants confirmed their consent by selecting the “Agree to participate” option before proceeding to the study questions. A clinical trial number is not applicable.
Authors contributions
MBA and ZK wrote the manuscript, RA collected the data, RH and KJ supervised the whole process. All authors revised and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, 18 Sage UK House Style and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are available under reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.