
Abstract
Background
Accurate prediction of ICU mortality based on physiological data can significantly facilitate timely interventions and improve patient outcomes. However, patient heterogeneity, including variations in age, disease types, and regional differences, along with the dynamic nature of ICU data, leads to significant limitations in the generalization ability and self-updating capability of existing prediction models. Therefore, developing dynamically adaptive predictive methods is crucial to ensure model adaptability and reliability in real-world clinical settings.
Methods
We propose AdaICU, a novel framework that integrates unsupervised domain adaptation and incremental learning for cross-ICU mortality prediction. The framework first aligns feature distributions between source and target domains using domain-adversarial training, and subsequently updates the model through incremental learning as new target-domain data become available.
Results
Extensive experiments on the PhysioNet 2012 dataset show that AdaICU consistently outperforms baseline models across multiple cross-domain settings. In particular, AdaICU achieves AUROC improvements of approximately 2–6% over the strongest baseline across different transfer tasks. Substantial improvements are also observed in AUPRC, indicating enhanced capability in identifying high-risk patients. In addition, AdaICU improves accuracy by approximately 4–8% and achieves higher positive predictive value, suggesting more reliable positive predictions. Overall, these results highlight the effectiveness of the proposed framework in addressing cross-domain distribution shifts.
Conclusion
By jointly addressing cross-domain distribution shifts and post-deployment model adaptation, AdaICU provides a practical and effective framework for ICU mortality prediction in settings with limited labeled data. This capability makes it particularly promising for real-world application in dynamic clinical environments with evolving data distributions.
Introduction
Intensive Care Units (ICUs) are critical for treating severely ill patients. Physicians rely on continuous monitoring of signals such as heart rate and blood pressure to guide clinical decisions. 1 With the growth of data science, large-scale ICU data now make it possible to build machine learning and deep learning models for mortality prediction.2,3 These models can support early risk stratification and help hospitals allocate limited medical resources more effectively. 4
However, limited generalization across clinical settings remains a key obstacle to deployment. Models trained on data from one ICU setting often perform poorly when applied to a different ICU setting. The reasons include differences in patient populations, monitoring practices, sampling patterns, and treatment protocols. Previous studies have shown that cross-site deployment can reduce predictive performance (AUROC) by 10–20% compared with in-site testing. 5 This drop is more than a technical issue. It can delay clinical interventions, cause patient misclassification, and lead to inefficient use of scarce ICU resources. As a result, limited generalization remains a critical barrier to the reliable adoption of mortality prediction systems in practice.
Most existing approaches are developed and evaluated on a single data source. They implicitly assume that the training and deployment data follow the same distribution,6–8 which rarely holds in practice. ICU settings may differ in patient composition, monitoring practices, sampling patterns, and missing-data characteristics. From a machine-learning perspective, these differences induce a distribution shift between the source domain used for model development and the target domain in which the model is deployed. Such shifts can lead to substantial performance degradation when models are applied to unseen ICU settings, thereby limiting reliable deployment and broader clinical adoption.
To address this challenge, we employ domain adaptation and incremental learning techniques to handle cross-ICU distribution shifts and continual model updating. Through domain adaptation, the model can mitigate environment- and subject-specific variations and extract features that are invariant across ICU subgroups and patient populations. To further adapt to evolving ICU environments, incremental learning allows the model to update as new patient data arrive over time. Despite the straightforward idea, two major research questions remain: (1) How can we learn robust representations from heterogeneous and multi-scale physiological time series? ICU monitoring generates signals with complex temporal dynamics, irregular sampling, and missing values. The challenge is to capture both local patterns and long-term dependencies within these sequences. A well-designed model must represent fine-grained physiological variations while preserving broader temporal trends. (2) How can continuously accumulating ICU data be used to improve mortality prediction? As new ICU data accumulate over time, the model must be updated without losing previously learned knowledge. Without appropriate constraints on the learning process, the mortality prediction model may suffer from catastrophic forgetting, gradually losing previously acquired knowledge as new data is introduced, thereby causing significant deviations in the prediction results.
9
Therefore, effectively integrating newly collected data while preserving essential learned knowledge remains a critical challenge.
In this paper, we present AdaICU, a framework for ICU mortality prediction that integrates domain adaptation and incremental learning to address cross-ICU distribution shifts and continual model updating. The workflow is shown in Figure 1, illustrating the flow from patient data to mortality prediction and model updating. The workflow of AdaICU.
The main contributions of this paper are summarized as follows: • To our knowledge, AdaICU is a novel framework that jointly integrates domain adaptation and incremental learning for ICU mortality prediction. It addresses the challenge of distribution shift across heterogeneous patient populations and evolving clinical environments. • Methodologically, AdaICU employs a CNN–LSTM encoder with a Domain-Adversarial Neural Network (DANN) to capture both local temporal dynamics and long-term dependencies in multivariate physiological time series while learning domain-invariant representations. An incremental learning strategy is further incorporated to enable continuous adaptation to new patient cohorts without catastrophic forgetting. • We performed extensive evaluations using the publicly available PhysioNet 2012 dataset.10,11 We not only validated the effectiveness of the proposed network structure but also demonstrated the performance improvement achieved through domain adaptation in different domains.
The rest of this paper is organized as follows: In Section 2, we review the related work on mortality prediction, domain adaptation, and incremental learning. In Section 3, we detail the design and implementation of AdaICU. We present the experimental results in Section 4. In Section 5, we discuss limitations and potential improvements. Finally, Section 6 concludes the paper.
Related work
ICU mortality prediction
Summary of representative ICU mortality prediction models.
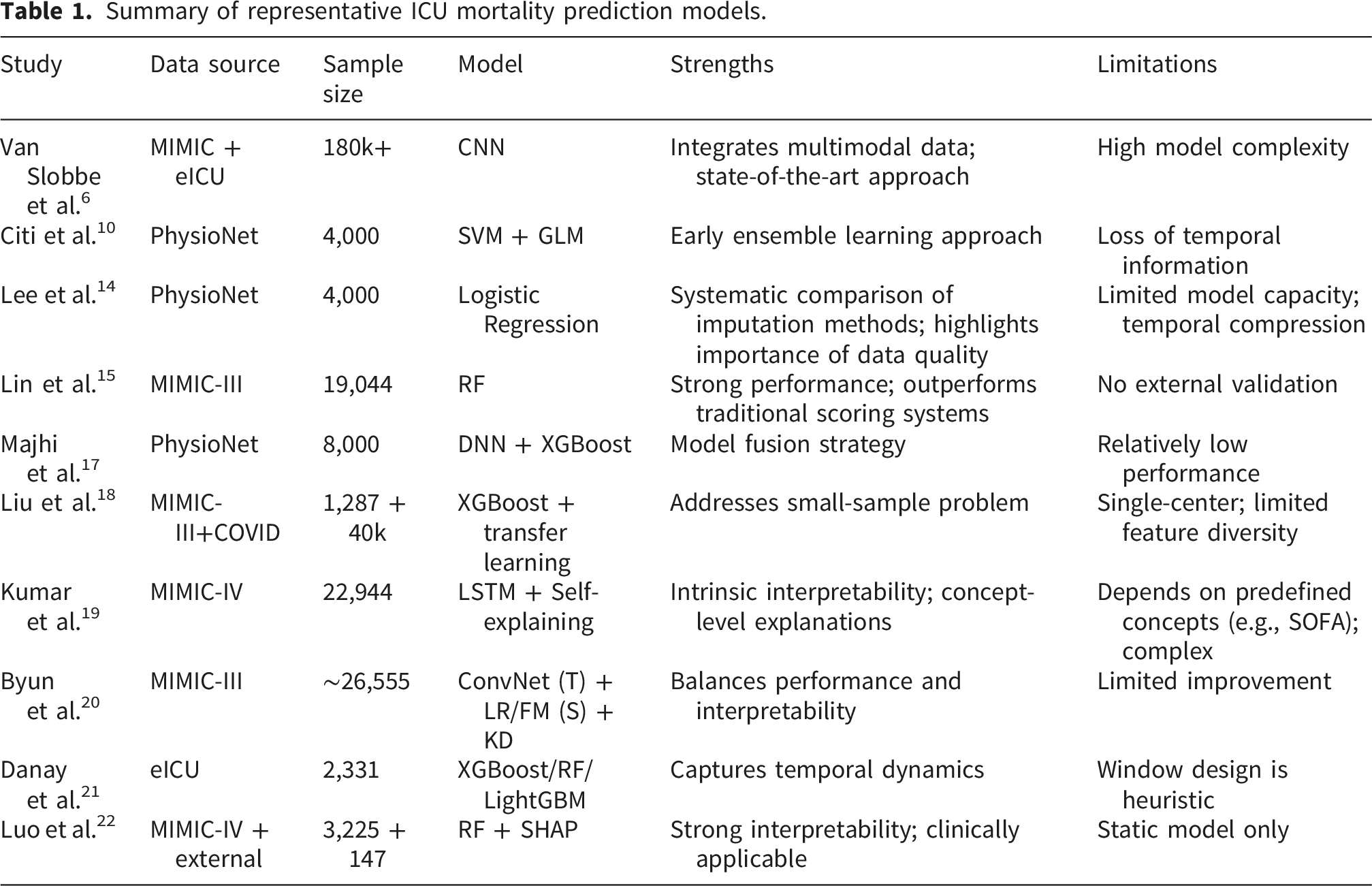
Deep learning approaches, including CNNs, LSTMs, and hybrid architectures, have been applied to multivariate physiological time series to improve mortality prediction performance.6,9,23–25 These models capture complex temporal dynamics and inter-variable relationships, often outperforming traditional ML models within the same ICU. However, their reliance on large labeled datasets limits their applicability in scenarios where target-domain labels are scarce.
Recent studies have explored domain adaptation, transfer learning, and incremental learning to enhance cross-ICU generalization.8,26–29 These works demonstrate that models trained on one ICU or hospital may perform poorly on others due to distribution shifts in patient populations, monitoring protocols, and clinical practices. Domain adaptation and incremental learning strategies have been proposed to mitigate this degradation, particularly when labeled data in the target ICU are limited.30–33 Our study builds on this line of work by integrating domain adaptation with incremental learning to maintain performance across heterogeneous ICU subgroups while avoiding catastrophic forgetting.
Overall, the Related Work highlights that while traditional and deep learning models perform well within a single ICU, cross-ICU deployment requires strategies such as domain adaptation and incremental learning to achieve robust generalization.
Domain adaptation
Distribution shift is a well-known challenge in machine learning. Models trained on a source domain often fail to generalize to unseen target domains. 34 In ICU settings, such shifts may arise not only from differences in monitoring devices, sampling protocols, and treatment practices, but also from differences in clinical focus and patient populations across ICUs. For example, the same physiological parameter may carry different clinical implications depending on the ICU context; elevated blood pressure may be interpreted differently in a surgical ICU than in a medical ICU. Domain adaptation aims to address this problem by aligning feature distributions across domains. In Unsupervised Domain Adaptation (UDA), the target domain lacks labeled data. Most UDA methods therefore attempt to learn a shared feature space through distribution alignment.35,36
In early ICU mortality prediction research, most models assumed that a single training dataset could generalize to all hospitals. Nori et al. questioned this assumption, showing that patient heterogeneity can undermine performance. 37 Subsequent work began to address domain-related issues. Alves et al. explored domain adaptation strategies for mortality prediction. 26 Gong et al. applied transfer learning to mitigate data scarcity in cardiac surgery risk models. 38 Liu et al. used prediction scores from MIMIC-III as additional features for COVID-19 mortality prediction, alleviating the cold-start problem. 18 These studies suggest that domain adaptation and transfer learning can improve robustness when models are transferred across clinically heterogeneous settings. More recently, Kumari et al. employed deep domain adaptation to improve cross-hospital generalization. 30
These studies confirm the potential of domain adaptation to mitigate distribution shifts. However, most methods only handle static settings with fixed source and target domains. They rarely consider that ICU data change over time. By contrast, AdaICU combines domain adaptation with continual learning. This design allows the model to handle distributional shifts across hospitals while also adapting to new data as it arrives.
Incremental learning
Incremental learning updates models with new data while retaining previously acquired knowledge. 39 In the clinical deployment scenario considered in this paper, a predictive model may first be adapted from a source ICU domain to a target ICU domain and then need to be updated as new patient data gradually accumulate in the target ICU over time. In such settings, repeatedly retraining the model on all available data may be inefficient or impractical. Moreover, historical ICU data may not always remain fully accessible because of privacy, data-governance, and storage constraints. 31 Incremental learning therefore provides a practical mechanism for updating the deployed model while reducing the need for repeated access to all previously collected data.
Prior studies have explored incremental learning in medical time-series analysis. Sun et al. proposed MAPIC, a few-shot incremental learning framework for medical time-series classification. 32 Shi et al. designed an incremental learning system for atrial fibrillation detection and validated it on real ECG data. 33 These studies demonstrate that incremental learning can be useful for handling evolving medical data streams, but they mainly focus on standalone medical time-series tasks rather than the deployment setting considered here.
In our setting, the key challenge is that a model deployed in a target ICU may need to handle both initial cross-domain adaptation and subsequent updating as new target-domain data become available. Existing studies usually address either continual updating or cross-domain adaptation in isolation. By contrast, AdaICU combines domain adaptation with incremental learning in a unified framework, with ICU mortality prediction serving as a representative application scenario. This design allows the model to support post-deployment updating in evolving ICU settings while reducing catastrophic forgetting.
Methods
The overview of our proposed AdaICU is shown in Figure 2. The model first takes physiological data from both the source domain and the target domain as input, where labeled data are available in the source domain and unlabeled data are used from the target domain during domain adaptation training. These data (e.g., blood pressure, heart rate, and urine output) are encoded into a shared representation through a feature encoder. A classifier is then employed to predict patient mortality, while a domain discriminator is introduced to minimize distributional discrepancies between domains via adversarial training. After the initial source-to-target adaptation stage, incremental learning is used to update the model as new target-domain data become available over time. The overall framework of AdaICU.
To facilitate the description of the ICU mortality prediction task, the physiological data and survival status of a patient at time t are denoted as ⟨P t , O t ⟩.
Domain adaptation model
As mentioned earlier, patient data obtained in real ICU wards can be highly heterogeneous. These data may contain complex temporal patterns and domain-specific variations that are not directly relevant to mortality prediction. The model’s ability to predict the risk of mortality may be compromised by these factors, resulting in reduced performance when applied to new patients or deployment settings. Domain adaptation can efficiently resolve this problem by aligning different domains. In this study, we consider an unsupervised domain adaptation setting, where labeled data are available in the source domain, while only unlabeled data are available in the target domain during adaptation training. 40 Under this setting, our method uses unlabeled target-domain data to encourage alignment between source and target representations while reducing domain-specific variation.
We developed a DANN-based CNN-LSTM architecture as our domain adaptation model. DANN can suppress domain-specific information while preserving task-relevant features for mortality prediction. The three basic components of the network architecture: the feature encoder, the classifier, and the domain discriminator—are illustrated in Figure 3. The goal of this model is to provide domain-adaptive mortality prediction by learning task-relevant representations while suppressing domain-specific ones. AdaICU deep learning architecture.
Feature encoder
As illustrated in Figure 3, the feature encoder extracts deep features from the clinical data. x i ∈ X denotes the ith input sample. The mortality label y i ∈ Y indicates the corresponding outcome. Furthermore, every piece of input data is accompanied by a domain label, which originates from either the labeled source domain space D s or the unlabeled target domain space D t , creating a total of D.
The feature encoder, G
f
, takes the raw, intricate, high-dimensional clinical data as inputs, and converts them into a simpler, low-dimensional representation, z. To perform feature extraction, we stack three 2D CNN (Convolutional Neural Network) layers, where each convolutional layer is followed by batch normalization and ReLU activation. This structure allows the model to extract localized spatial correlations across the temporal feature grid, while the intermediate dropout helps prevent overfitting. The CNN output is then flattened and passed through two fully connected layers to generate a compact representation. Although the convolutional layers compress the input characteristics for prediction, they are less effective at capturing time-series data correlations. To capture both spatial and temporal features from the data, we introduce an additional branch consisting of one LSTM layer with tanh activation functions. The raw input sequence is directly processed by the LSTM layer to model long-term temporal dependencies. To integrate the complementary strengths of the two branches, the features derived from the CNN and LSTM pathways are concatenated and passed through a learnable fusion gate. Specifically, a linear layer followed by a sigmoid activation generates an attention-like coefficient α, which adaptively balances the contributions of the CNN and LSTM outputs. The final feature representation is computed as a convex combination:
Classifier
As shown in Figure 3, the classifier G
y
takes the output feature z from the previous stage as input. Three fully connected layers with activation functions are employed to extract discriminative features related to patient mortality. Subsequently, these features are projected into a latent space aligned with the mortality label dimensions via a final sigmoid layer. This design enables the model to output a probability distribution over the predicted mortality labels for the input x, as follows:
The Binary Cross-Entropy loss with logits is computed between the actual and predicted labels. The label prediction loss is defined as follows:
M denotes the number of mortality labels, while |D
s
| signifies the total number of samples in the source domains. During training, the feature encoder G
f
and the classifier G
y
collaborate to maximize prediction performance by minimizing the label prediction loss
Domain discriminator
The domain discriminator G
d
uses the feature representation z and the predicted mortality output 

Optimization objective
The objective of the AdaICU model is to reduce the loss of label prediction, denoted as 
λ is the hyperparameter that balances two objectives and mediates their trade-off during model optimization. Our model’s objective in the training phase is to minimize the combined loss function, ensuring that mortality risk prediction remains domain-independent.
Incremental learning
After the initial source-to-target adaptation stage, the deployed model may need to be updated as new target-domain data gradually accumulate over time. In this work, incremental learning is introduced as an updating mechanism for this post-deployment stage, rather than as the only possible alternative to full retraining. This design is motivated by practical settings in which repeated retraining on all previously collected data may be inefficient or undesirable, for example because of computational cost or limited access to historical data. However, incremental learning is associated with the issue of catastrophic forgetting. 41 This phenomenon occurs when learning a new task causes the model to overwrite knowledge acquired from previous tasks. The forgetting problem is addressed through the application of the Elastic Weight Consolidation (EWC) method. 42 EWC is an algorithm designed to preserve knowledge from previous tasks while learning new ones.
Specifically, we assume that new target-domain data become available in batches after deployment. We set a threshold τ as the minimal amount of new data for model updating with incremental learning. Once the amount of newly accumulated target-domain data reaches this threshold, the model is incrementally updated using these data. To ensure an appropriate update frequency of the model, τ is set to 300 to maintain a balanced update frequency.
The detailed procedure of the EWC algorithm is as follows: We consider the initial dataset training (base model) as task A and the subsequently collected dataset training as task B. The fundamental concept of EWC is to constrain modifications to the crucial parameters of the previous task. This is achieved by incorporating a quadratic penalty on the parameter differences into the loss function:
Datasets
We use the publicly available PhysioNet Challenge 2012 dataset, 43 as it provides clearly defined ICU-type subgroups along with multivariate physiological time-series data. Such a structure enables a controlled and reproducible evaluation of cross-ICU distribution shifts, which is central to our study. The dataset contains multivariate clinical time-series data from 12,000 patients, including age, gender, height, weight, ICU type, and 37 physiological variables recorded during the first 48 hours of ICU stay.
General characteristics of patients across ICU domains.

Note. Cardiac, cardiac surgery recovery unit; Coronary, coronary care unit; Medical, medical ICU; Surgical, surgical ICU.
The PhysioNet 2012 dataset was selected because it offers a clearly defined and standardized partition of patients into multiple ICU types (e.g., Medical, Surgical, Coronary, and Cardiac), thereby naturally supporting controlled cross-domain evaluation. This explicit domain structure enables a systematic and reproducible investigation of domain adaptation under well-defined experimental conditions.
While more recent datasets such as MIMIC-IV contain larger and more diverse patient populations, they do not explicitly provide a standardized domain partition aligned with ICU types. Constructing such domain splits in MIMIC-IV would require additional assumptions or preprocessing steps (e.g., hospital unit mapping or cohort redefinition), which may introduce confounding factors and reduce experimental reproducibility.
Therefore, the PhysioNet 2012 dataset is particularly suitable as a benchmark for evaluating cross-domain adaptation methods in a controlled and interpretable setting. Future work will extend the proposed framework to larger and more heterogeneous datasets, such as MIMIC-IV, to further assess generalizability in real-world multi-center scenarios.
Table 2 presents general information regarding patients across various ICU domains. The dataset includes four ICU domains: Cardiac, Coronary, Medical, and Surgical. It is evident that the mortality prevalence was low across all four domains, resulting in class imbalance.
Average physiological indicators across the four ICU domains.

Note. DiasABP, diastolic arterial blood pressure; MAP, mean arterial pressure; NIDiasABP, non-invasive diastolic arterial blood pressure; NIMAP, non-invasive mean arterial pressure; NISysABP, non-invasive systolic arterial blood pressure; PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; SaO2, arterial oxygen saturation; SysABP, systolic arterial blood pressure.
For data preprocessing, we addressed missing values by applying forward filling followed by backward filling. If a particular feature of a sample was missing across all time points, the global mean value was used for imputation. To mitigate the impact of outliers, we performed percentile-based truncation, retaining values between the 1st and 99th percentiles. For normalization, we employed min-max scaling. Data preprocessing was largely consistent between machine learning and deep learning approaches. The only difference is that deep learning models employed hourly sampling of patient features, whereas machine learning models relied on feature values averaged over the entire observation period.
Results
Evaluation settings
We use six metrics in AdaICU’s evaluation, including AUROC, AUPRC, Brier score, Accuracy, PPV, and Sensitivity.6,15 Higher AUROC, AUPRC, Accuracy, and PPV values indicate better performance, while a lower Brier score reflects more accurate probabilistic predictions. Sensitivity highlights the model’s ability to correctly identify critical cases, which is especially important in mortality prediction. For threshold-dependent metrics, the classification threshold is determined based on the F1 score to balance precision and recall. Additionally, for each model, the best-performing checkpoint is selected according to validation set performance. • AUROC: Measures the model’s ability to distinguish between classes across all classification thresholds. A higher value indicates better discriminatory performance. • AUPRC: Focuses on the trade-off between precision and recall, especially useful for imbalanced datasets. A higher AUPRC suggests better performance in identifying the positive class. • Brier score: Evaluates the accuracy of probabilistic predictions by measuring the mean squared difference between predicted probabilities and actual outcomes. Lower Brier scores indicate better-calibrated and more accurate probability estimates. • Accuracy: Represents the overall correctness of the model by calculating the proportion of true results (both true positives and true negatives) among the total number of cases. A higher accuracy implies better overall classification performance. • PPV: Indicates the proportion of predicted positive cases that are actually positive. A higher PPV suggests greater reliability in identifying true positive outcomes. • Sensitivity: Measures the model’s ability to correctly identify actual positive cases. A higher sensitivity is critical in clinical settings to ensure high-risk patients are not overlooked.
Overall performance
Here, we present a comprehensive performance comparison of AdaICU against four benchmarks: Var-CNN, 6 SVM-GLM, 10 DNN-XGB, 17 and RF. 15 These baseline models were selected to represent a diverse set of commonly used approaches in ICU mortality prediction, including traditional machine learning, deep learning, and hybrid methods. In addition to the four primary baseline models, we also included two neural-network-based baselines, namely LSTM and CNN-LSTM. The LSTM model consists of a standalone LSTM network and serves as a representative recurrent architecture for ICU time-series prediction. The CNN-LSTM model combines convolutional and recurrent layers and corresponds to the feature-extraction backbone used in AdaICU, but without the domain adaptation and incremental learning components. These additional baselines were included to evaluate the contribution of the proposed adaptation framework beyond the underlying network architecture. Notably, these models do not incorporate domain adaptation mechanisms. The comparison is therefore designed to evaluate the effectiveness of introducing domain adaptation under cross-ICU transfer settings, rather than to benchmark against all existing domain adaptation approaches.
In this study, all available samples from the PhysioNet 2012 dataset were included without additional manual exclusion criteria, ensuring consistency with the benchmark setting. The number of patients in each ICU subset is summarized in Table 2. To ensure robust evaluation and mitigate overfitting, we employed 5-fold cross-validation, with 80% of the data allocated for training and the remaining 20% for testing. Within each training fold, 20% of the data was further split as a validation set for model selection and hyperparameter tuning. All deep learning models were trained for 100 epochs using the Adam optimizer, with a batch size of 128 and an initial learning rate of 0.0001. The experimental setup was consistent across all models to ensure a fair comparison.
Cross-domain performance (AUROC ± std).

Note. AdaICU results are shown in bold, and the best non-AdaICU baseline is underlined. AdaICU is only applicable to cross-domain transfer settings and is therefore not reported when the source and target domains are identical.
Compared with the source-trained CNN_LSTM model without domain adaptation, AdaICU attains additional AUROC gains in 10 of the 12 cross-domain tasks, with improvements ranging from 0.011 to 0.083. The largest improvements are observed in Surgical → Cardiac (+0.083), Medical → Surgical (+0.062), Medical → Cardiac (+0.058), and Surgical → Medical (+0.054), highlighting the effectiveness of the domain adaptation module in facilitating knowledge transfer.
When benchmarked against models trained directly on the target domain (i.e., diagonal entries in Table 4), AdaICU remains competitive despite not using target-domain labels. The gap between the best cross-domain AdaICU result and the best target-trained model is 0.044 for Medical, 0.010 for Cardiac, 0.060 for Coronary, and 0.018 for Surgical. In particular, for the Cardiac and Surgical target domains, AdaICU approaches the performance of the best target-trained models very closely, indicating that the proposed framework can substantially narrow the performance gap between cross-domain adaptation and target-specific training.
Nevertheless, AdaICU performs slightly below the best baseline in two tasks targeting the Coronary ICU, namely Cardiac → Coronary and Surgical → Coronary. This underperformance may be related to the limited sample size of the target Coronary ICU, which may restrict the model’s ability to fully exploit transferred knowledge. In addition, the relatively small domain discrepancy in these transfer settings may reduce the potential benefit of adaptation, making strong non-adaptive baselines more competitive.
To further visualize the cross-domain performance of AdaICU, we compare AdaICU with several strong baselines through ROC and precision–recall curves. As shown in Figure 4, AdaICU achieves the highest AUROC values across the three transfer tasks shown in the figure, with scores of 0.8556, 0.8996, and 0.8349, respectively, consistently outperforming Var-CNN (0.8400, 0.8529, and 0.7999), SVM-GLM (0.7221, 0.7719, and 0.7306), DNN-XGB (0.6984, 0.7339, and 0.7122), and RF (0.7995, 0.8212, and 0.7992). The ROC curves further demonstrate that AdaICU maintains stronger discriminative ability under varying decision thresholds across different cross-domain settings, highlighting its superior robustness to distribution shifts between source and target ICU domains. ROC curves of different models across three cross-domain transfer tasks.
We further assess model performance using the area under the precision–recall curve (AUPRC), which is particularly informative in imbalanced clinical settings where positive cases are relatively rare. As shown in Figure 5, AdaICU consistently achieves the highest AUPRC values across the three transfer tasks, with scores of 0.4968, 0.4421, and 0.3896, respectively. These results substantially outperform all baseline models, including Var-CNN (0.3609, 0.2694, and 0.2388), SVM-GLM (0.2451, 0.2352, and 0.2321), DNN-XGB (0.1503, 0.1387, and 0.1253), and RF (0.2626, 0.2156, and 0.1877). The consistent advantage of AdaICU in the precision–recall space indicates that its superiority is not limited to overall ranking performance, but also extends to a more favorable balance between detecting positive cases and limiting false positives. This property is particularly important in ICU prediction tasks, where both missed detections and excessive false positives may have serious clinical implications. Precision–recall curves of different models across three cross-domain transfer tasks.
Domain adaptation
Performance comparison across three cross-domain transfer tasks.

Note. AdaICU results are shown in bold, and the best non-AdaICU baseline is underlined. Medical ICU → Cardiac Surgery Recovery Unit, using the Medical ICU as the source domain and the Cardiac Surgery Recovery Unit as the target domain. The other two settings follow the same meaning.
In Table 5, AdaICU achieves AUROC values of 0.8556, 0.8996, and 0.8349, as well as AUPRC values of 0.4968, 0.4421, and 0.3896, respectively, all of which are higher than those of the best-performing baselines. Relative to Var-CNN, AdaICU yields corresponding relative improvements of 1.9%, 5.5%, and 4.4% in AUROC, and 37.7%, 64.1%, and 63.1% in AUPRC across the three tasks. These results further support the superiority of AdaICU in cross-domain prediction, especially under clinically imbalanced settings.
For threshold-dependent metrics, AdaICU also achieves the highest Accuracy and PPV in all three transfer tasks. Specifically, its Accuracy reaches 0.9300, 0.9387, and 0.9217, while its PPV reaches 0.3895, 0.4052, and 0.3545, respectively. Compared with the strongest baselines, AdaICU improves Accuracy by 5.3%, 4.5%, and 8.4%, and improves PPV by 60.9%, 56.0%, and 84.9%, respectively. These results indicate that AdaICU not only improves overall classification accuracy, but also produces substantially more reliable positive predictions, which is particularly important for ICU risk stratification and clinical decision support.
By contrast, AdaICU does not consistently achieve the best performance in Sensitivity or Brier score. In the Medical ICU → Cardiac Surgery Recovery Unit task, the highest Sensitivity is achieved by RF (0.7203), whereas in the Surgical ICU → Cardiac Surgery Recovery Unit and Coronary Care Unit → Cardiac Surgery Recovery Unit tasks, the best Sensitivity is obtained by SVM-GLM (0.5854) and DNN-XGB (0.6016), respectively. Nevertheless, AdaICU maintains competitive Sensitivity values of 0.5960, 0.5800, and 0.5860 across the three tasks, suggesting a favorable balance between detecting positive cases and limiting false positives. Similarly, because lower Brier scores indicate better calibration, the underlined baseline models rather than AdaICU achieve the best calibration performance in these experiments. Therefore, the primary advantage of AdaICU lies in its superior cross-domain discrimination, stronger positive predictive performance, and better overall predictive utility, rather than in calibration alone.
To evaluate the impact of the amount of unlabeled target-domain data on the performance of the AdaICU model, we conducted experiments using the Surgical ICU as the source domain and the Cardiac Surgery Recovery Unit as the target domain. Specifically, the proportion of target-domain samples was gradually increased from 0.1 to 0.9. The corresponding changes in model performance were assessed using the AUROC. The results are visualized in Figure 6. Effect of the proportion of unlabeled target-domain data on AdaICU performance.
This study evaluated domain adaptation performance using different proportions of target-domain samples for adaptation. The AUROC generally increased as the proportion of target-domain data used for adaptation increased, reaching its highest value at a ratio of 0.8 (AUROC = 0.866). However, when the ratio was further increased to 0.9, the AUROC decreased markedly to 0.829. One possible explanation is the reduced number of samples remaining for evaluation, as allocating more target-domain data to adaptation leaves fewer cases for testing, which may reduce the stability and reliability of the performance estimate.
Based on Table 4, AdaICU demonstrated strong adaptation capability even when only a limited amount of target-domain data was available. Specifically, when 2,530 target-domain samples were available, the model achieved effective adaptation using only a few hundred unlabeled target-domain samples and substantially outperformed the non-adaptive baseline.
This finding is of practical importance because it reduces reliance on large labeled target-domain datasets, the collection of which is often costly and labor-intensive. By leveraging a limited amount of unlabeled target-domain data, domain adaptation methods such as AdaICU may achieve strong performance in real-world settings where labeled data are scarce.
To further investigate the feature distributions after domain adaptation, t-distributed stochastic neighbor embedding (t-SNE) 44 was used to project the learned representations into a low-dimensional space for visualization. Figure 8 and Figure 9 in Appendix present the feature visualizations before and after domain adaptation, respectively. As shown in the t-SNE visualizations, prior to domain adaptation, source and target samples form distinct clusters for each class, reflecting the model’s effective separation of source domain features. Following domain adaptation, source and target features become highly aligned, resulting in an overall intermixing of the two domains. Consequently, class-specific clusters appear less pronounced in the low-dimensional t-SNE projection. This does not imply a degradation of classification performance; rather, it indicates that the domain adaptation process primarily focuses on aligning the global distributions across domains. Importantly, the high-dimensional feature space continues to maintain class separability, allowing the model to correctly classify target domain samples.
Ablation study
Ablation study.

Note. w/o CNN, AdaICU model without CNN; w/o LSTM, AdaICU model without LSTM. Values in bold indicate the best performance for each evaluation metric.
Specifically, removing either the CNN or LSTM module leads to a decline in discriminative performance. Without the CNN module, the AUROC decreases from 0.8996 to 0.8865 and the AUPRC decreases from 0.4421 to 0.4215. Without the LSTM module, the AUROC similarly drops to 0.8866, while the AUPRC decreases to 0.4303. These results indicate that both components contribute meaningfully to the performance of AdaICU.
Compared with the removal of the LSTM module, removing the CNN module results in a slightly larger reduction in AUPRC and a comparable reduction in AUROC, suggesting that the CNN component may contribute slightly more to discriminative feature extraction in this task. This finding highlights the importance of CNN layers in capturing local patterns and correlations in ICU data, whereas the LSTM module complements the model by encoding temporal dynamics and sequential dependencies.
In terms of calibration, however, AdaICU does not achieve the best Brier score in this ablation study. Although the full model yields a Brier score of 0.1500, the w/o CNN and w/o LSTM variants obtain 0.1490 and 0.1474, respectively, with the lowest value achieved by w/o LSTM. Since lower Brier scores indicate better calibration, these results suggest that the primary advantage of the full AdaICU model lies in stronger discriminative performance and improved AUPRC rather than calibration. Overall, the ablation study confirms that the integration of CNN and LSTM enables AdaICU to learn more effective spatiotemporal representations, leading to better overall performance in terms of discrimination.
Incremental learning
We further investigate the effectiveness of our incremental learning approach in adapting to new ICU environments. As shown in Figure 7, we present the overall performance of AdaICU after applying incremental learning. Initially, the model is trained using source domain data along with a small portion of the target domain data. Subsequently, the remaining target domain data is divided into two portions. One part is used for incremental learning, and the other part is reserved for testing. The incremental learning process was conducted over ten batches, with the proportion of target domain samples in each batch progressively increasing from 0.1 to 1.0 of the total incremental learning dataset. Following the training of each batch, the model’s performance was evaluated on a fixed target domain test set using three metrics: AUROC, AUPRC, and Brier score. Incremental learning performance of AdaICU under different remaining target data ratios.
As illustrated in Figure 7, all three metrics show consistent improvement as more target domain data is introduced through incremental training. Specifically, the AUROC increases steadily from 0.8776 to 0.9093, indicating enhanced discriminative ability of the model over time. The AUPRC rises from 0.4496 to 0.5554, reflecting progressively better identification of positive (high-risk) cases, which is particularly critical for imbalanced datasets. Meanwhile, the Brier score decreases from 0.0532 to 0.0330, suggesting increasingly well-calibrated and reliable probability outputs.
These results demonstrate the effectiveness of our incremental learning approach in progressively adapting to the target domain while avoiding catastrophic forgetting. The model maintains stability throughout the incremental updates and achieves improved generalization as more domain-specific information becomes available. Moreover, the complementary trends of AUROC, AUPRC, and Brier score validate the robustness and practical utility of our strategy in real-world ICU mortality prediction scenarios. Minor fluctuations observed in AUPRC during intermediate stages may be attributed to variations in batch composition, but they do not disrupt the overall upward trend.
Discussion
In this study, we propose AdaICU, an ICU mortality prediction framework that combines unsupervised domain adaptation with incremental learning to address patient heterogeneity and variations across ICU settings. By leveraging unlabeled target-domain data during adaptation, AdaICU aligns the feature distributions of the source and target domains, improving cross-ICU generalization. The integration of incremental learning enables post-deployment updating. This allows the model to refine its predictions as new target-domain data accumulate over time.
Experimental results demonstrate that AdaICU improves robustness under cross-ICU transfer settings. It consistently outperforms conventional baseline models, demonstrating the benefit of leveraging unlabeled target-domain data. Notably, the AUROC achieved by AdaICU is comparable to those reported in prior ICU mortality prediction studies. This is particularly encouraging, as externally validated models often report AUROCs of approximately 0.87–0.89, whereas higher values are typically observed in more favorable single-center settings.
The variability across transfer tasks may be partially explained by the clinical heterogeneity among ICU types. Cardiac and Surgical ICUs contain more homogeneous perioperative populations, whereas Medical ICUs include patients with diverse disease etiologies and severity levels. Consequently, transfer performance tends to be higher when source and target ICUs share similar clinical characteristics and lower when substantial differences exist in patient composition, mortality prevalence, and physiological profiles.
However, this comparison should be interpreted with caution, because AdaICU is the only model that has access to unlabeled target-domain data during training, whereas the baseline models are trained without any target-domain information. As a result, the comparison is not fully balanced and does not constitute a head-to-head evaluation against alternative domain adaptation methods. Therefore, the observed performance gains should be understood primarily as evidence of the potential value of incorporating unlabeled target-domain data through adaptation and incremental updating, rather than as definitive proof that AdaICU is universally superior to all competing modeling strategies.
We also acknowledge that ICU mortality prediction may not fully demonstrate the framework’s potential, as mortality labels are often available and relatively reliable. The practical value of AdaICU is expected to be higher in settings with limited, delayed, or unavailable target-domain labels, in which unsupervised adaptation and post-deployment updating are most relevant.
Despite these promising results, the study has several limitations. First, it is retrospective, and missing values in ICU datasets may reduce robustness because real-time ICU monitoring often introduces irregularities that standard imputation cannot fully capture. Second, the comparative evaluation has an inherent limitation: since AdaICU uniquely exploits unlabeled target-domain data, while the baseline models do not, part of its performance advantage may reflect differences in available information rather than differences in model architecture alone. Future studies should therefore include stronger and fairer comparators, particularly domain adaptation or semi-supervised methods that are also allowed to access unlabeled target-domain data. Third, the current work focuses on adaptation between a single source and a single target domain. Multi-source or multi-target adaptation scenarios, which better reflect real-world hospital networks, remain to be explored. Fourth, experiments rely on four ICU subgroups from the PhysioNet 2012 dataset, which share a common collection protocol; thus, the studied domain shifts may not fully represent inter-institutional or cross-regional variability. Finally, prospective validation in actual clinical workflows is necessary to evaluate the impact on decision-making and patient outcomes.
Future work will extend AdaICU in several directions. First, we will evaluate the framework in multi-source and multi-target adaptation settings to better capture complex hospital networks. Second, external validation on larger and more heterogeneous cohorts is essential to test robustness across collection protocols and regional practices. Third, methodological improvements, such as richer temporal-feature representations and advanced sequence models, could enhance the capture of physiological patterns. Fourth, incorporating multimodal data, including laboratory results, imaging, medications, and clinical notes, may improve robustness against missing modalities and enhance interpretability. Finally, integrating federated learning could enable collaborative model training across institutions while preserving patient privacy.
Conclusion
Predicting ICU patients’ mortality risk based on their physiological data has been a long-standing research focus. However, the diversity of patients and the differences in ICUs make the ”train once, fit all” paradigm ineffective. To address this problem, we present AdaICU, an incremental domain adaptation-based ICU patient mortality prediction framework. By using unsupervised domain adaptation, we align the feature distribution of the source and target domains to improve the generalization ability of the model. In addition, we also apply incremental learning to enable AdaICU to adapt and refine its predictions continuously. We have demonstrated the effectiveness of the proposed model through extensive evaluations. AdaICU’s strong generalization and continual adaptation capabilities highlight its potential for clinical deployment.
Footnotes
The authors would like to thank the National Key R&D Program of China (2021ZD0140405).
Ethical considerations
This study was an analysis of third-party deidentified publicly available databases with pre-existing ethical review board approval.
Author Contributions
Equal contribution: Xinqiang Xie and Ting Lyu contributed equally to this work and are co-first authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key R&D Program of China (2021ZD0140405).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data utilized in this study are publicly available from the PhysioNet repository under the title ”Mortality in Intensive Care Unit Patients: the PhysioNet Computing in Cardiology Challenge 2012”.
43
The data can be accessed at: ![]() .
.
AI usage statement
AI-based language tools were used to assist with translation and language refinement during manuscript preparation. These tools were applied only to improve clarity and readability. The authors take full responsibility for the content of the manuscript.
Reporting guideline
This study was reported in accordance with the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD+AI) recommendations.
Footnote
Guarantor Xie XQ.