
Abstract
Objective
This study aims to provide a comprehensive bibliometric analysis of model-informed precision dosing (MIPD) research in anti-infective therapy from 2005 to 2025, systematically mapping its evolution from pharmacometric foundations to emerging artificial intelligence applications, and identifying key research trends, institutional contributions, and future research priorities in this rapidly evolving field.
Methods
The terminology related to MIPD and anti-infective drugs was used as a search strategy to retrieved literature from the core collection of Web of Science, and the data obtained were analyzed by VOSviewer, CiteSpace and Bibliometrix.
Results
A total of 4,601 articles were included, the USA published the largest number of documents, Australia had the highest citations per publication. The University of Queensland was the most productive institution. Roberts JA and Lipman J were the most published authors. The field underwent a foundational phase of developing population pharmacokinetic models, a consolidation phase aimed at promoting Bayesian-guided TDM and extending it to special populations, and a frontier phase of parallel advancement involving traditional MIPD and emerging machine learning frameworks. Critically, the divergence between pharmacokinetic metrics used in traditional MIPD and predictive accuracy metrics favored by machine learning approaches represents a principal obstacle to clinical integration.
Conclusion
This study provides the first comprehensive bibliometric map of two decades of MIPD research in anti-infective therapy, documenting its evolution from pharmacometric foundations to emerging AI-assisted applications, and identifies prospective clinical validation, EHR integration, and harmonized ML-MIPD evaluation frameworks as key future priorities.
Keywords
1. Introduction
Infection-related morbidity and mortality remain at an alarmingly high level globally,1,2 encompassing a broad disease spectrum ranging from acute bacterial infections to chronic viral infections—the latter typified by chronic hepatitis B, whose antiviral treatment optimization likewise constitutes an important component of precision anti-infective therapy research. 3 In intensive care, there are physiological changes, including augmented renal clearance, hypoalbuminaemia and organ dysfunction, which offer quite a lot of variability in antibiotic pharmacokinetics.4–6 These modifications often result in the standard dosing regimen falling short of achieving the desired pharmacokinetic/pharmacodynamic (PK/PD) target, either under-exposing or over-exposing. With the growing problem of resistance to antibiotics, optimizing the dosing regimens of these medications has become one of the key components of antimicrobial stewardship strategies. 7
Therapeutic drug monitoring (TDM) has been used for dose adjustment for a long time. It is based on linear extrapolation or the clinician’s experience, which may not be able to keep pace with rapid changes in physiology. 8 A new paradigm in the use of clinical PK data is emerging in model-informed precision dosing (MIPD). 9 By using these data from other patients, the population PK models allow for the analysis of a patient’s likely response to different possible doses.10–12 The operational core of MIPD is Bayesian forecasting—iteratively updating prior pharmacokinetic parameter estimates using observed individual concentration data to yield posterior estimates that more accurately reflect the true pharmacokinetic characteristics of the individual patient. Notably, the methodological versatility of MIPD extends beyond anti-infective therapy, demonstrating capacity to identify drug interactions and optimize initial dosing in other clinical settings such as pediatric and psychiatry, 13 further affirming the broad applicability of population pharmacokinetic modeling and Bayesian forecasting as core tools for precision dosing.
In recent years, artificial intelligence (AI) and machine learning (ML) technologies have begun to enter the MIPD field as complements to traditional pharmacometric approaches. Several methodological categories currently coexist: popPK/PD models constructed on physiological equations; Bayesian forecasting that dynamically adjusts these estimates using individual measured data; ML models that extract patterns directly from data without relying on prespecified mechanistic structures; and reinforcement learning that optimizes dosing sequences through iterative trial and refinement. Demands for data, interpretability, and clinical validation differ in these approaches. The clinical decision support software creating popPK models together with Bayesian algorithms is gradually coming within the regulatory umbrella of software as a medical device (SaMD). From a methodological perspective, the software stays within the conventional boundaries of MIPD. But when it performs automated data integration with electronic health records (EHR), permits real-time concentration entry and instant generation of personalized dosing recommendations, its implementation represents a step toward digital health integration, which characterizes the current frontier phase.
Despite numerous systematic reviews that have summarized drug-specific models or clinical trials,14–16 the field remains devoid of a comprehensive and quantitative analysis of the whole research landscape. The conventional review approach may include selection bias and cannot disentangle the evolution of research themes. For example, how the focus of the field has shifted from theoretical modelling to actual external validation. 17 More critically, with the rapid advancement of digital health technologies, the paradigm is now shifting from traditional TDM toward MIPD as a convergence of pharmacology and health informatics. This evolution translates complex mathematical algorithms into user-friendly software as a medical device, enabling clinicians to input real-time patient data and utilize Bayesian forecasting to predict individualized dosing regimens at the bedside.
To meet these challenges, this paper uses a complete bibliometric technique by employing VOSviewer, 18 Bibliometrix 19 and CiteSpace 20 tools so as to map the knowledge structure of the field and visualise the time-related development of “trending topics” and emerging of “Citation burst” publications. To our knowledge, the present is the first thorough investigation undertaken to analyze the world trends and research frontiers in MIPD research 2005-2025, tracing the scholarly trajectory from pharmacometric foundations to emerging AI applications, with the aim of providing reference for researchers, clinicians, and policymakers.
2. Methods
2.1. Data source and search strategy
The data for this study was drawn from the Web of Science Core Collection (WoSCC), a widely recognized resource acknowledged to be one of the most comprehensive and authoritative sources for bibliometric studies. 21 All literature searches and data exports were conducted on the same day (May 31, 2026). The study period was chosen as January 1, 2005, to December 31, 2025 with the following search strategy:
TS = (“model-informed precision dosing” OR “MIPD” OR “population pharmacokinetic*” OR “PopPK” OR “Bayesian dosing” OR “Bayesian forecast*” OR “MAP-Bayesian” OR “pharmacometric*” OR “NONMEM” OR “probability of target attainment” OR “physiologically based pharmacokinetic*” OR “PBPK” OR “precision dosing” OR “individualized dosing” OR “individualised dosing”) AND TS = (“anti-infective*” OR “antimicrobial*” OR “antibiotic*” OR “antifungal*” OR “antiviral*” OR “beta-lactam*” OR “carbapenem*” OR “aminoglycoside*” OR “glycopeptide*” OR “vancomycin” OR “polymyxin*” OR “colistin” OR “fluoroquinolone*” OR “oxazolidinone*” OR “linezolid” OR “echinocandin*” OR “azole*” OR “therapeutic drug monitoring”)
The initial search retrieved 5,418 records. Document type filtering retained only articles and reviews, excluding editorials, letters, conference abstracts, and other document types (200 records excluded; 5,218 remaining). Language filtering restricted the dataset to English-language publications (71 records excluded; 5,147 remaining). Subsequently, a time range restriction was applied to retain only records within the study period of January 1, 2005, to December 31, 2025 (495 records excluded; 4,652 remaining). All search records were exported in plain text format containing “full records and cited references” for subsequent analysis.
2.2. Data preprocessing
Data preprocessing was performed using CiteSpace (version 6.4.R1). As all records originated from a single database, no duplicate records were identified during deduplication. Additionally, 51 records with a publication year of 2026 were identified and excluded; these records represent online-first or early access articles that had been indexed prior to their formal publication date, and their inclusion would introduce temporal inconsistencies into the analysis. Data cleaning was subsequently performed, including synonym standardization and institutional name normalization (e.g., “population pharmacokinetics”, “PopPK”, and “population PK” were unified as “population pharmacokinetics”; “Bayesian forecasting” and “Bayesian estimation” were merged accordingly) to minimize attribution errors in co-authorship network analysis; the specific thesaurus is provided in Supplemental Table S1. The final dataset comprised 4,601 publications for all subsequent bibliometric analyses.
2.3. Data analysis and statistical analysis
The analysis used three bibliometric tools: VOSviewer (version 1.6.20), CiteSpace and the Bibliometrix R package (version 4.5.2). VOSviewer was used to construct and visualize various network and density maps. CiteSpace was used to capture temporal dynamics and evolutionary trajectories of the research field, including citation burst detection, cluster timeline visualization, and dual-map overlay analysis. The Bibliometrix R package, operated through the Biblioshiny graphical interface, was used to calculate basic bibliometric indicators, analyze annual publication trends, and identify the evolution of research themes over the study period. The general workflow of the bibliometric analysis can be seen in Figure 1. Flowchart of the literature search strategy and bibliometric analysis workflow of MIPD research for anti-infective therapy (2005–2025).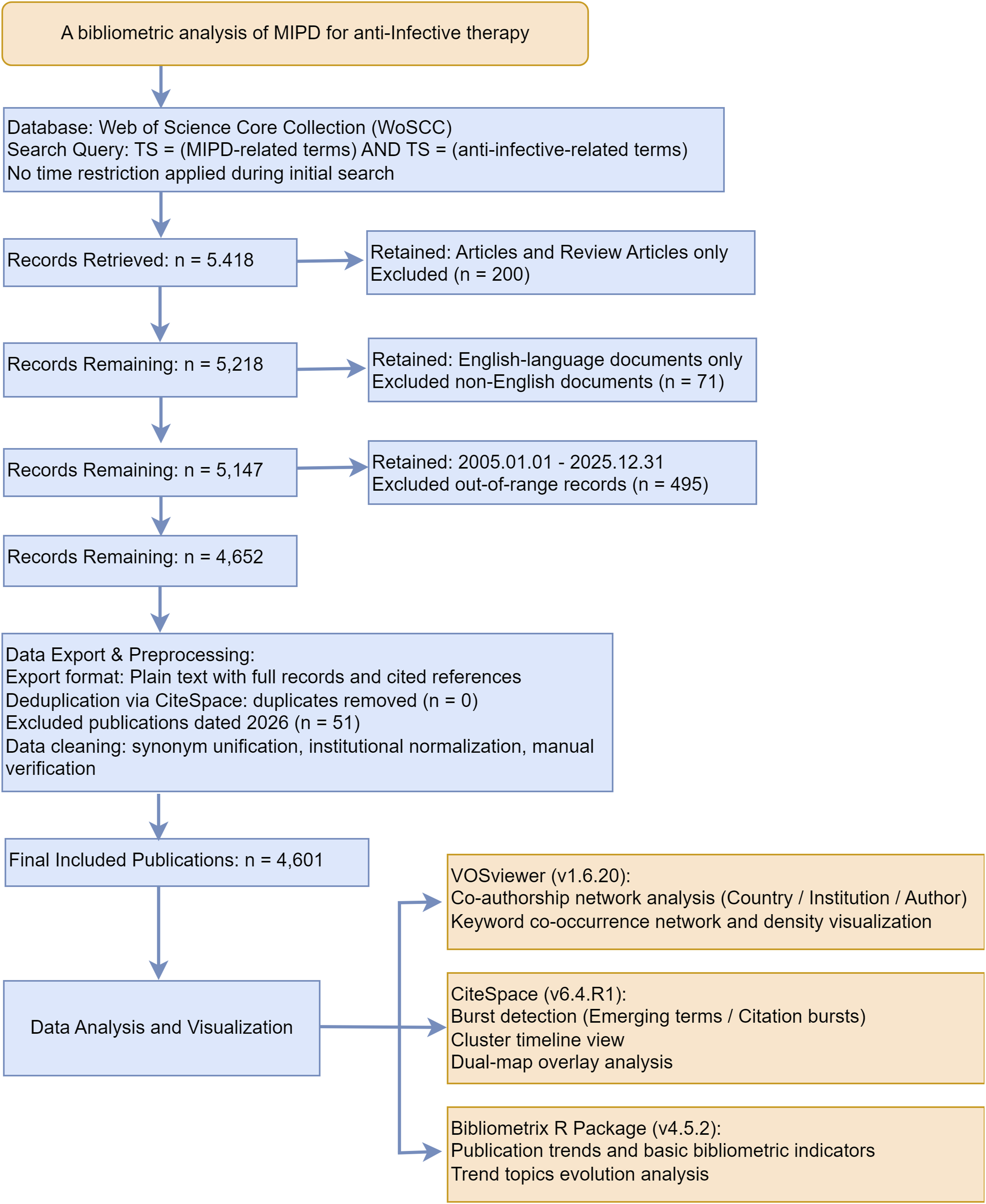
VOSviewer analyses employed full counting, with multiple normalization methods applied to network constructions. Association strength for the country collaboration network, LinLog/modularity for the institution, author, and keyword co-occurrence networks, and fractionalization for the co-citation network. Different minimum thresholds were set for each network: 15 publications for country-level collaboration networks, 35 publications for institutional collaboration networks, 25 publications for author co-authorship networks, 70 citations for reference co-citation networks, and 35 co-occurrences for keyword co-occurrence networks. Clustering employed the Louvain modularity-based algorithm, with a resolution parameter of 1.0 applied to all networks. CiteSpace analysis used annual time slices from 2005 to 2025, with node selection based on the modified g-index (scaling factor k = 25) and network pruning via the Pathfinder algorithm applied to slice networks. Citation burst detection was configured with γ = 1.0, two states, and a minimum burst duration of two years. Country attribution was based on the institutional affiliation of the first author.
Throughout the analysis, a clear distinction was maintained between traditional MIPD approaches and AI or ML-based methods: mechanistic population pharmacokinetic models and Bayesian forecasting tools were classified as the methodological core of traditional MIPD; machine learning predictive models and reinforcement learning frameworks were classified as emerging AI applications. The study covered EHR integrated clinical decision support systems as an intermediate implementation layer: when their core algorithm is Bayesian they are methodologically within the traditional MIPD framework; when they have machine learning components they display the digital integration features of the current frontier stage. The differences between the pharmacometric foundations of MIPD and the emerging AI applications that are broadening the scope of MIPD is depicted in this classification. It was always maintained that the interpretation of the results of keyword clustering, citation burst detection, and hot topic trend analyses, to ensure conceptual clarity in describing the field’s evolution.
This bibliometric review was reported in accordance with the BIBLIO checklist for reporting bibliometric reviews of the biomedical literature (Supplemental Table S2).
3. Results
3.1. Publications
As depicted in Figure 2, a total of 4,601 publications were covered in this study. The annual publication volume from 2005 to 2012 was very stable, ranging from 54 to 116 articles, reflecting the foundational period of popPK modeling and key anti-infective drug parameter estimation. From 2013 onwards till 2025, the publication entered a phase of rapid growth, increasing from 125 articles to a peak of 469 articles in 2025, more than threefold increase. This growth was driven by the convergence of traditional pharmacometric foundations with emerging AI and ML dosing frameworks, as well as increasingly prevalent antimicrobial stewardship initiatives. Following the citation frequency pattern of publication quantity, it reached its peak in 2019. The slight decline in citation counts after 2020 is not due to the field failing to attract academic attention but rather because the newly published papers have not reached their maximum citation accumulation time. Annual publication output and citation trends in MIPD research for anti-infective therapy (2005–2025).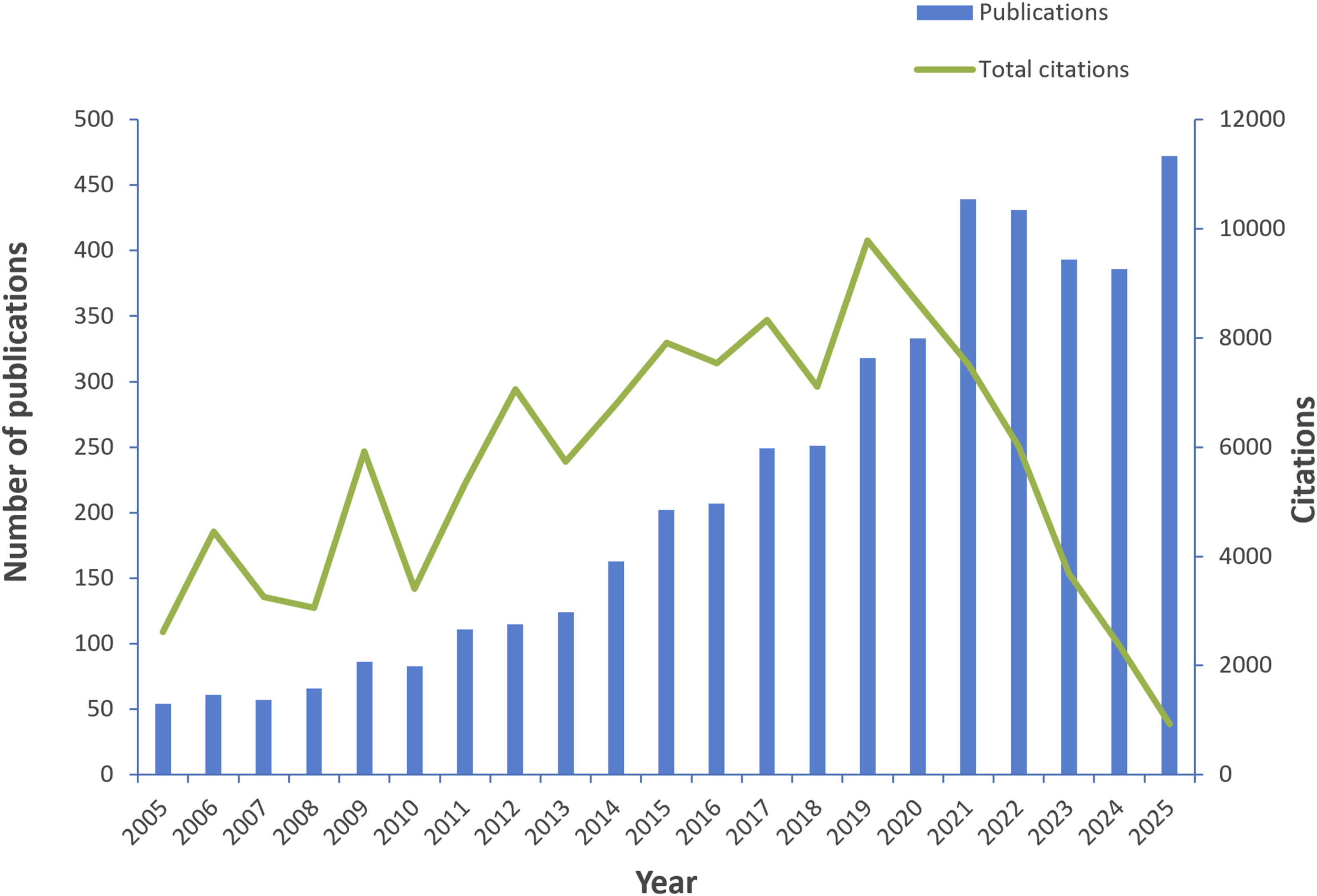
3.2. Country/region contributions
A complete of 99 countries/regions have participated in MIPD research for anti-infective therapy. According to Figure 3(a), research output was predominantly concentrated in North America, Western Europe, and the Asia-Pacific region, while contributions from South America, Africa, and the Middle East remained limited, reflecting persistent global disparities in research capacity. Global distribution and collaboration network of MIPD research for anti-infective therapy (2005–2025). (a) Geographic distribution of publication output by countries/regions. The color gradient reflects the publication volume of each country, where darker shades of blue indicate a higher number of published articles, while grey regions indicate no publications in this field. (b) International collaboration network among countries/regions. Each node represents a distinct country or region, and the size of the node is proportionally scaled to its total publication volume. The lines connecting the nodes signify co-authorship relationships, with the thickness of the lines representing the strength of the collaboration. Different node colors identify distinct collaborative clusters.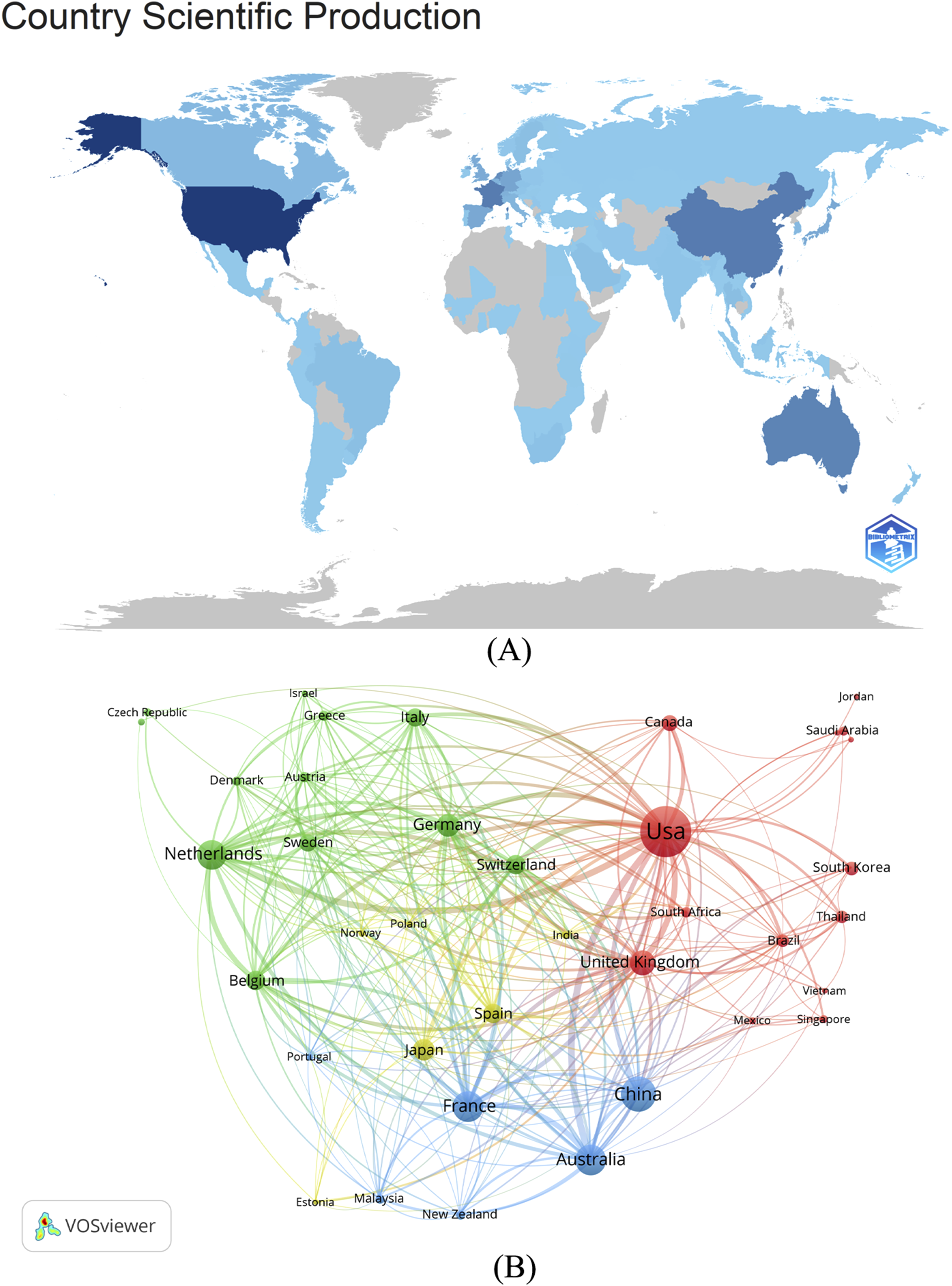
Top 10 countries/regions in MIPD research for anti-infective therapy.
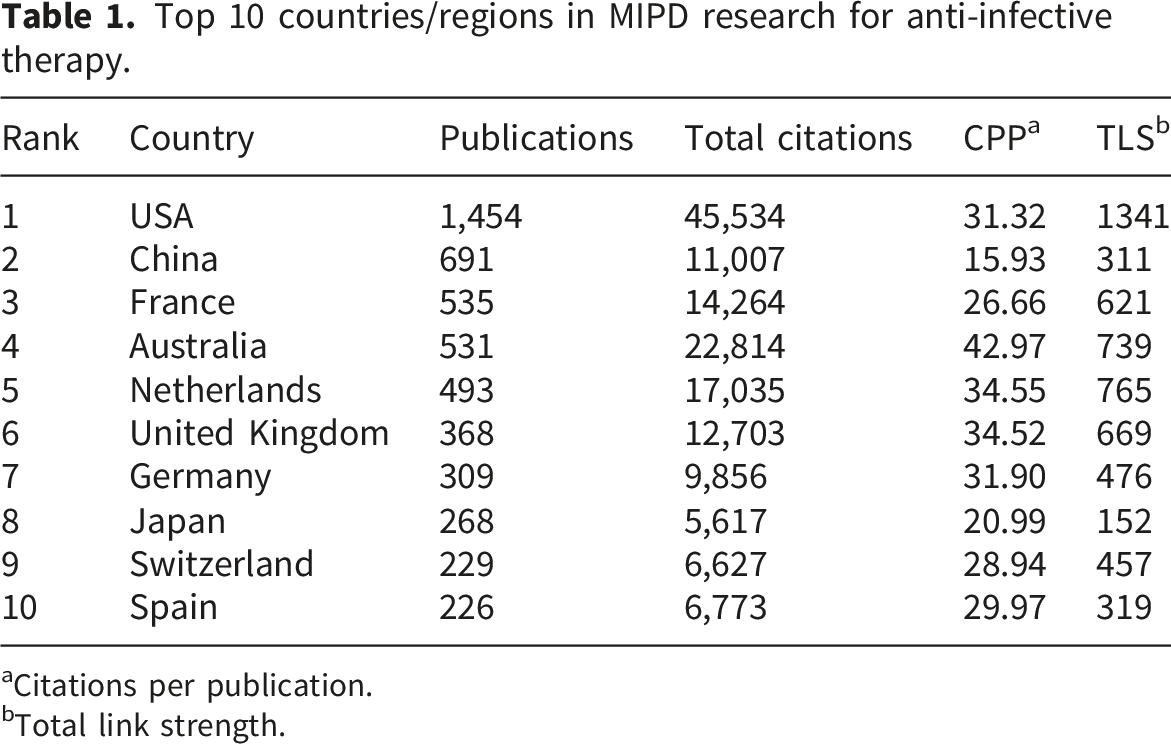
aCitations per publication.
bTotal link strength.
The collaboration network among countries/regions is shown in Figure 3(b). The size of the node indicates a larger publication volume, and a thicker line indicates a stronger collaboration. The USA located in the middle of the network, acts as the core hub for cooperation especially with China and Australia. Geographic differentiation was seen in the focus of research among major contributing countries. In the USA, there was mainly a focus on the development and validation of software for Bayesian dosing and pharmacokinetic modelling. This is most of all related to the strength in computational pharmacology and the concentration of major academic software development teams in that country. In Australia and several European countries, there was a greater focus on the clinical assimilation of TDM protocols and MIPD into everyday use. This geographic differentiation may be attributed to differences in healthcare system structures, regulatory environments, and research funding priorities, 22 with the United States tending toward methodological innovation 23 while Australian and European institutions prioritize clinical translation and real-world application. 10
3.3. Institutional contributions
MIPD study was participated by more than 2,200 institutions. Figure 4(a) shows the leading 10 institutions in volume of publication, of which four are located in Australia, five in Europe, and one in the USA. The University of Queensland ranked first with 247 publications, reflecting Australia’s leading position in popPK model development and Bayesian dosing guidance for anti-infective therapy. In terms of citation impact, Monash University had the highest average citations per publication, followed closely by Uppsala University, reflecting the important contributions of both institutions to PK/PD target attainment analysis and TDM-guided dosing optimization. We also assessed network map of institutional collaborations (Figure 4(b)). Australia’s domestic collaborative effort is highly cohesive, with a strong focus on the University of Queensland and Royal Brisbane & Women’s Hospital. At the same time, Monash University is deepening its international collaborations, notably with the University of Florida (US). Europe has a strong internal collaborative network spearheaded by Erasmus MC and Uppsala University whereas China has evolved a relatively independent research ecosystem. Overall, cross-cluster linkages among the Australian, European, and American research communities remain relatively sparse, indicating scope for expanding global collaboration in MIPD implementation. Institutional contributions and collaboration patterns in MIPD research for anti-infective therapy (2005–2025). (a) Top 10 institutions ranked by publication output. (b) Inter-institutional collaboration network. Each node represents an individual institution, with the node’s size being proportional to its total publication output. The curved lines connecting the nodes denote collaborative relationships, and the thickness of these lines indicates the strength of the collaboration. Different color-coded clusters represent different collaborative groups or consortia.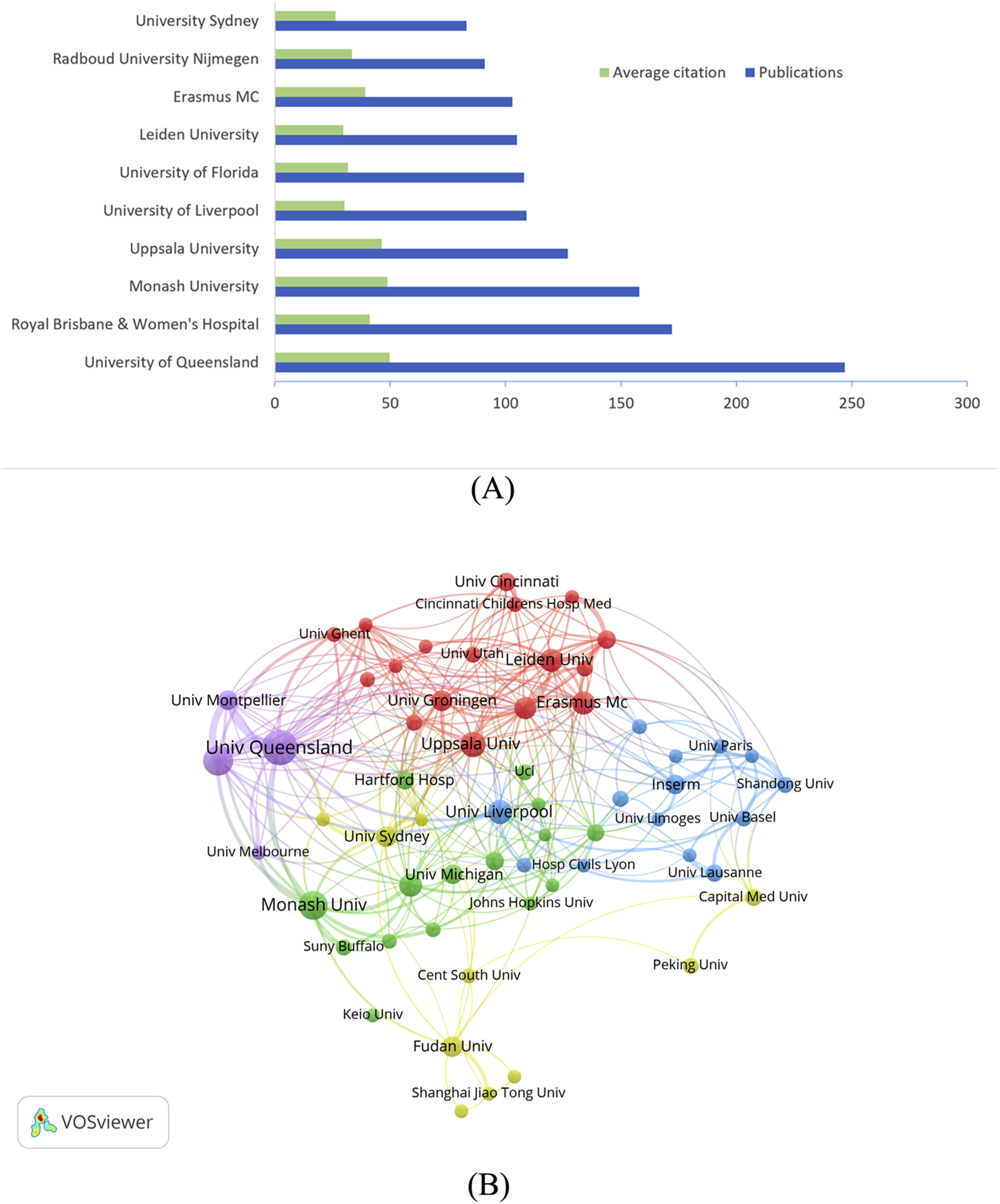
3.4. Author impact and collaboration network
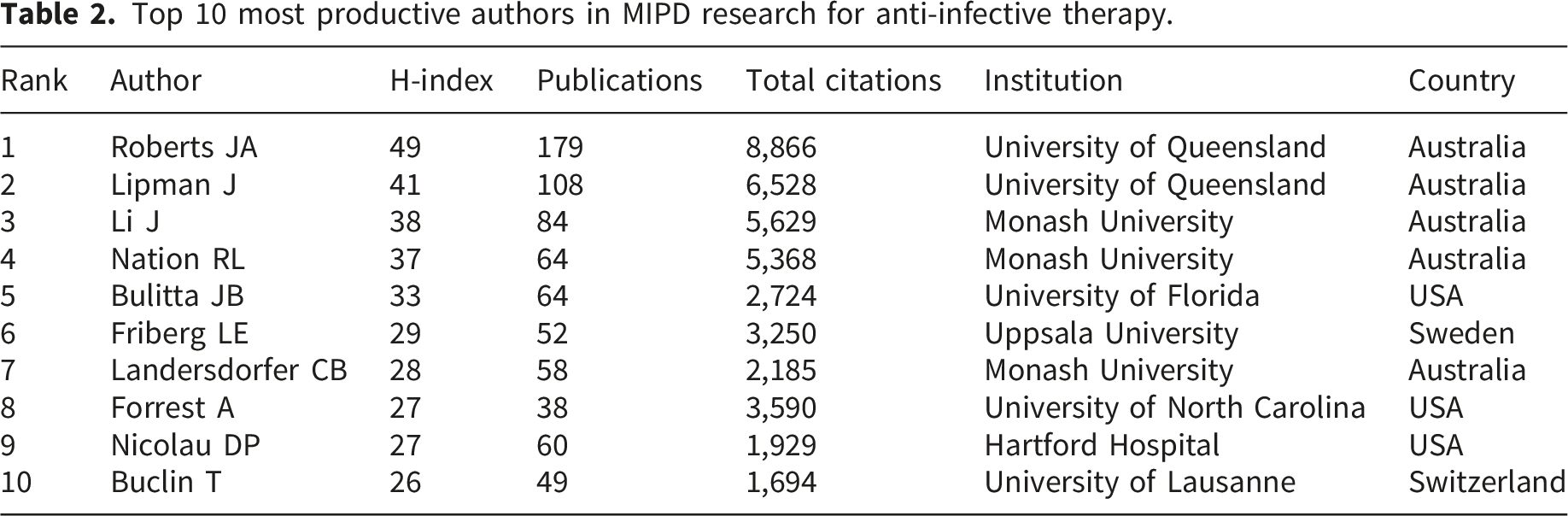
Top 10 most productive authors in MIPD research for anti-infective therapy.
In Figure 5(a), the collaboration network of the authors is shown. The size of the node indicates the amount of publications while the colour of the same indicates clustering taking collaboration into account. The network arranged five research groups. The purple cluster, centered on Roberts JA and Lipman J, focuses on PK/PD-guided TDM in the ICU setting, establishing the clinical framework for MIPD in severe infections. The blue cluster led by Li J encompasses the theories behind popPK and PK/PD target attainment especially for last-line antibiotics. The red cluster has been put together by Nicolau DP, Kuti JL, and Kloft C, which refers to the development and validation of Bayesian dosing software in hospital pharmacy practice. The green cluster projecting theoretical pharmacometrics and its extension in pediatric popPK and in antimicrobial stewardship is headed by Friberg LE Mouton JW Allegaert K. A new yellow cluster is beginning to emerge showing that a growing number of researchers are directing efforts towards digital TDM platforms and new AI/machine learning-assisted dosing decision support. The proximity of the clusters indicates that the researchers held frequent co-authorship relations. Figure 5(b) presents the active time periods of core researchers. Blue nodes identify early pioneers, an emerging yellow cluster includes researchers such as Buclin T and Guidi M, suggesting newer collaborative groups that may be linked to recent clinical implementation and digital dosing research. The temporal overlay in Figure 5(b) confirms this trajectory: early contributors established the popPK and PK/PD foundations; an intermediate generation consolidated Bayesian forecasting and TDM protocols; and the most recent generation of researchers is driving early integration of machine learning and EHR-linked clinical decision support. Author productivity, collaboration networks, and temporal activity patterns. (a) Co-authorship network of core researchers. The node size proportional to publication count and colors representing collaboration clusters identified through modularity optimization. (b) Temporal distribution of author activity. Blue nodes represent early pioneers, while yellow nodes denote recent contributors, reflecting generational shifts in research of MIPD.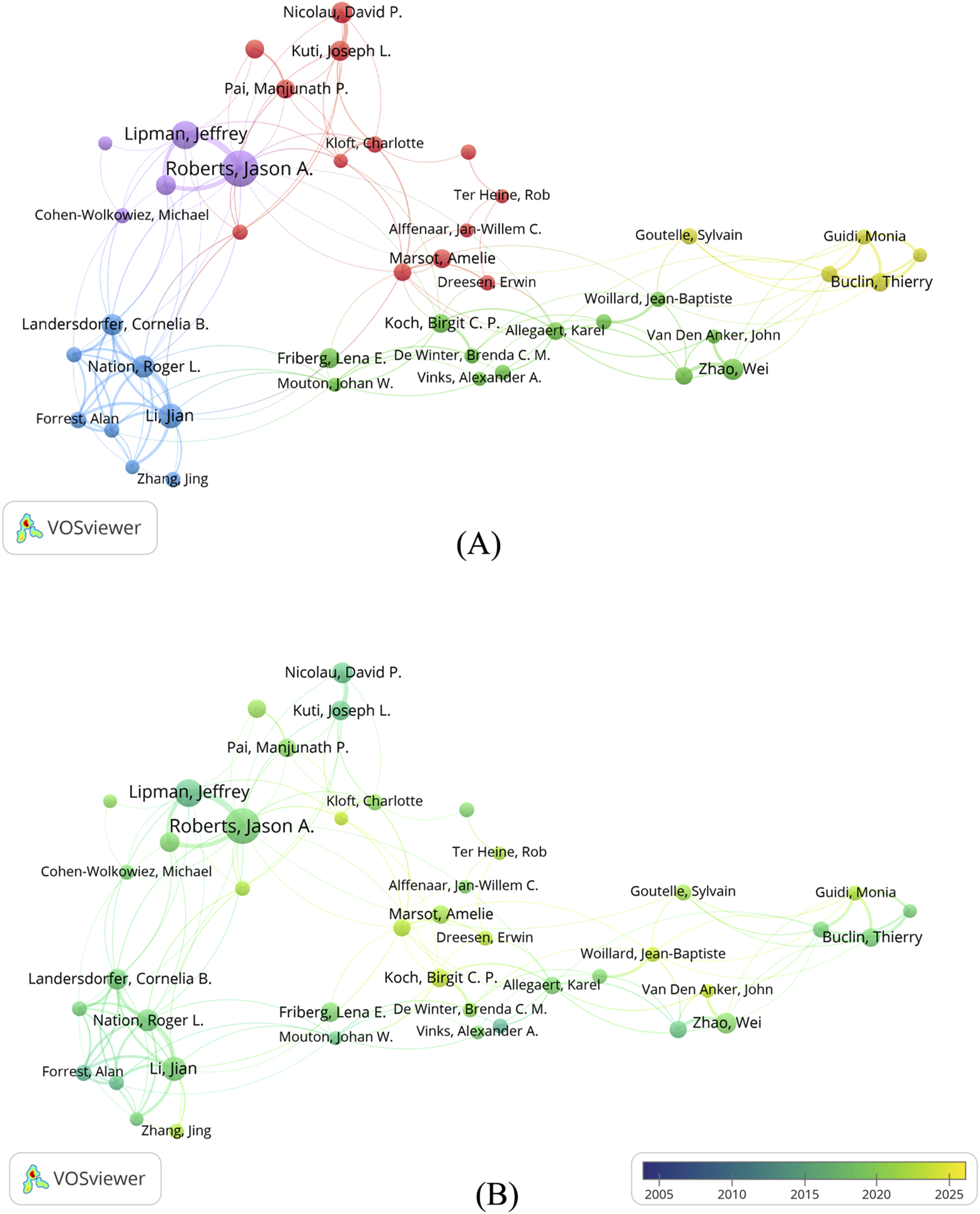
3.5. Journal contributions
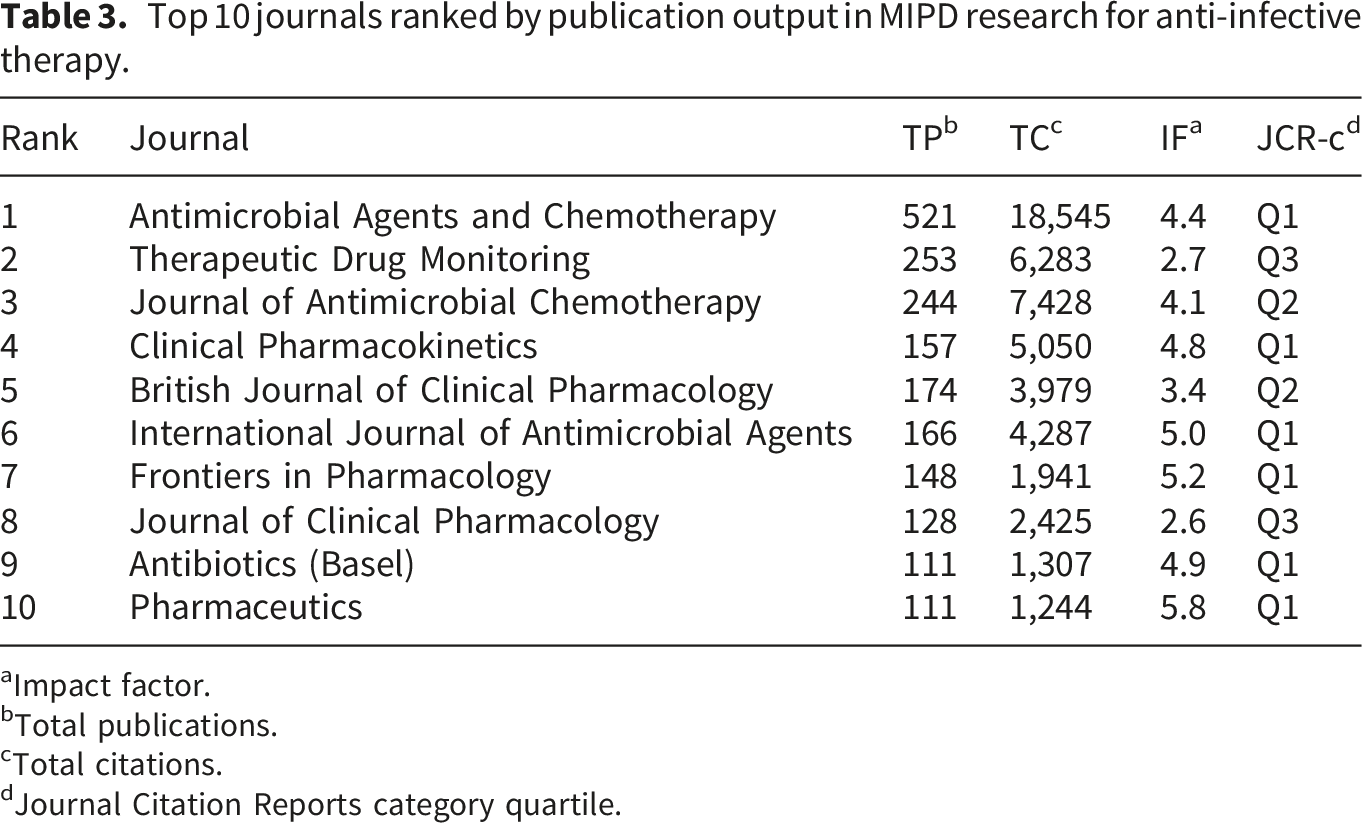
Top 10 journals ranked by publication output in MIPD research for anti-infective therapy.
aImpact factor.
bTotal publications.
cTotal citations.
dJournal Citation Reports category quartile.
Figure 6 shows a dual-map overlay of citing and cited journals. The dominant green citation trajectories indicate that the research frontiers (citing journals) mainly come from “Medicine, Clinical Medicine” categories, whereas the knowledge base (cited journals) primarily comes from “Molecular, Biology, Genetics” and “Health, Nursing, Medicine” on the right. This pattern confirms the characteristic nature of MIPD as a translational medicine discipline linking basic biology and clinical application. The directional citation pathways further reveal knowledge flows from theoretical pharmacometrics toward Bayesian-guided TDM and digital decision support. Dual-map overlay of journals in MIPD research for anti-infective therapy (2005–2025), depicting knowledge flow from citing journals (left) to cited journals (right), with ellipses representing journal clusters and colored paths indicating citation trajectories. The green main path reveals that research frontiers are primarily published in “Medicine, Medical, Clinical” journals (left ellipse), while the knowledge base draws predominantly from “Molecular, Biology, Genetics” and “Health, Nursing, Medicine” disciplines (right ellipses).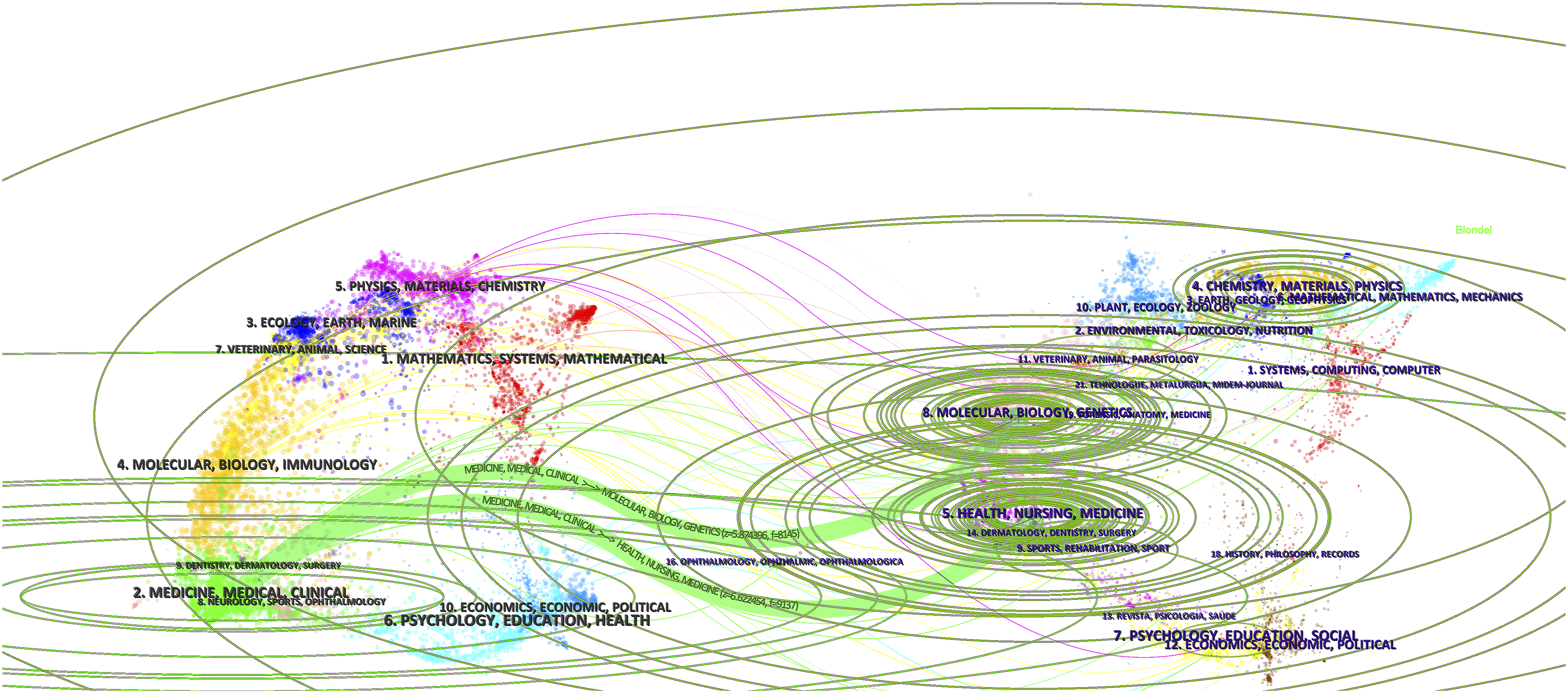
3.6. Reference co-citation
Top 10 most commonly cited references creating the knowledge base of MIPD research in anti-infective therapy.
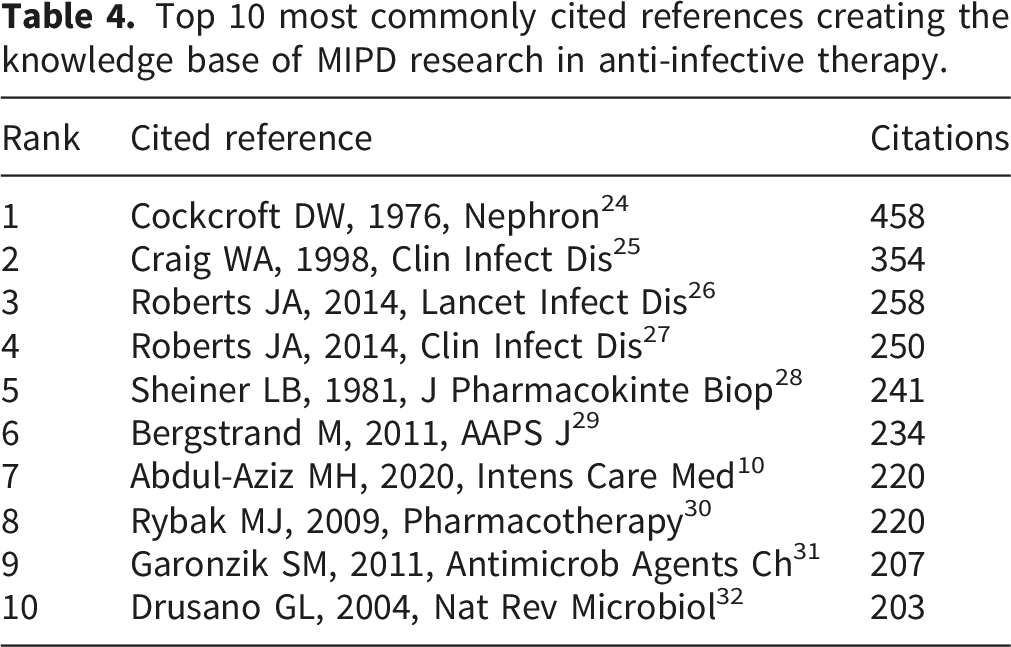
The document co-citation network view is shown in Figure 7(a). The sizes of the nodes are related to the number of citations. The network reveals four distinct clusters: a large red cluster anchored by Cockcroft and Craig, representing PK/PD and renal function foundations; a blue cluster representing popPK methodology; a green cluster representing the evolution of vancomycin TDM guidelines; and a yellow cluster representing dosing optimization for last-resort antibiotics (polymyxins/colistin). In the density view (Figure 7(b)), the foundational works of Cockcroft, Craig, and Drusano appear as bright yellow “hotspots,” with Garonzik SM forming a secondary high-density region, reflecting the field’s sustained focus on renal function-adjusted dosing and polymyxin pharmacokinetics. Co-citation analysis of foundational literature in MIPD research. (a) Network visualization of co-cited references, with node size proportional to citation frequency and colors representing thematic clusters. (b) Density visualization highlighting citation hotspots, using color intensity to indicate citation concentration, with bright yellow “hotspots” marking seminal works (c) Timeline view of research evolution and clustering.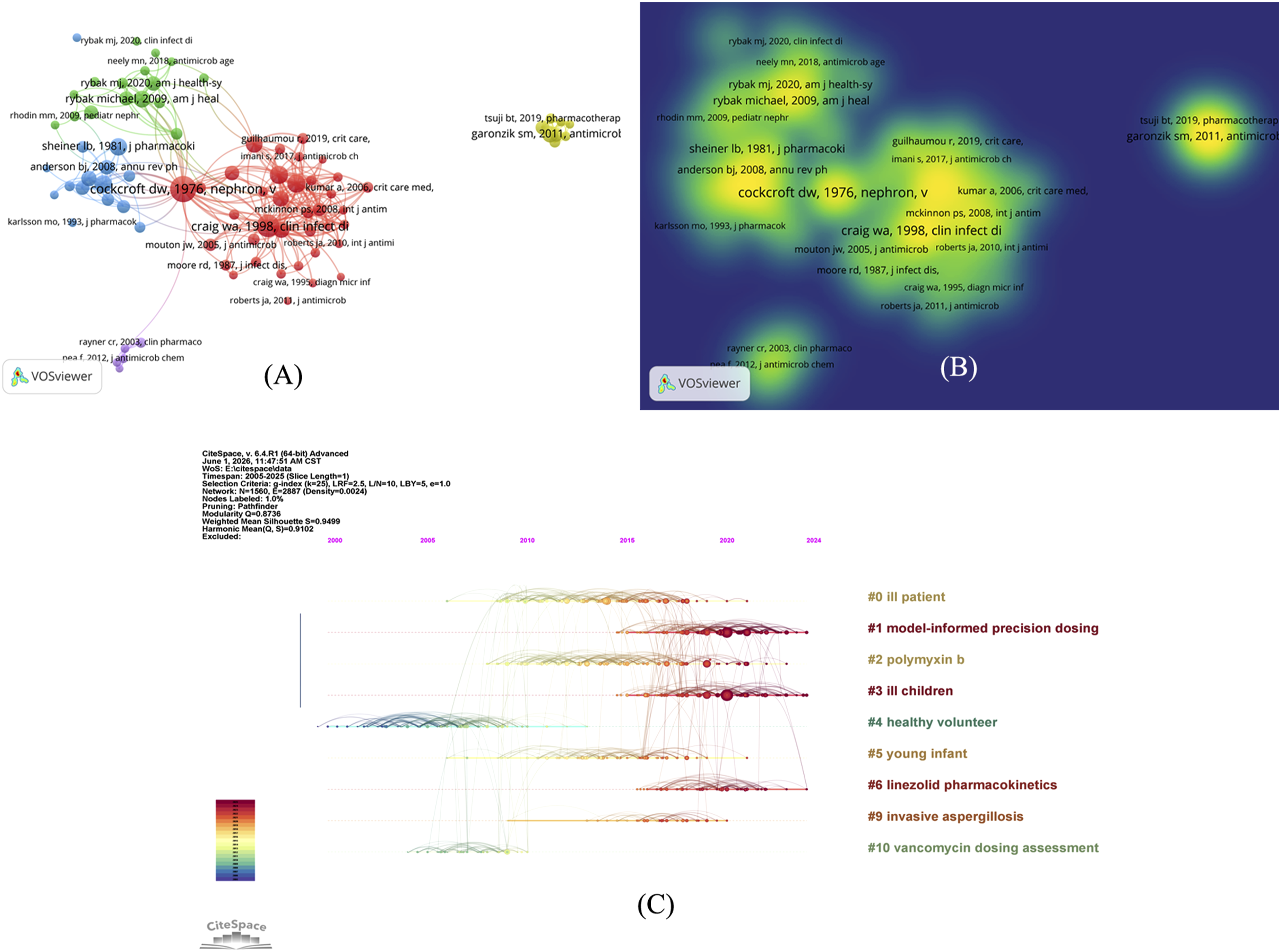
We performed the timeline view analysis using CiteSpace in order to reflect the evolution of research hotspots (Figure 7(c)). The Modularity Q value (0.8736 > 0.3) shows a significant clustering structure. Furthermore, the Weighted Mean Silhouette S value (0.9499 > 0.7) indicates a high homogeneity degree of clusters, thus confirming the high reliability of the clustering result.
The clusters reveal a coherent three-phase knowledge evolution. Clusters #4 “healthy volunteer” and #10 “vancomycin dosing assessment” reflect early efforts to establish popPK models and PK/PD targets under controlled conditions, providing an evidence base for clinical TDM protocols. 33 Clusters #2 “polymyxin B” and #6 “linezolid pharmacokinetics” represent the extension of MIPD principles to last-resort and time-dependent antibiotics with extremely narrow therapeutic windows, where Bayesian-guided dosing is critical for balancing efficacy with toxicity.34,35 Cluster #1 “model-informed precision dosing,” as the most active dominant cluster, reflects the formal consolidation of the field into a clinical framework combining popPK models with Bayesian forecasting for real-time dose individualization. 22 Clusters #0 “ill patients,” #3 “ill children,” #5 “young infants,” and #9 “invasive aspergillosis” further indicate that research is expanding MIPD validation to high-complexity populations, including critically ill adults, 10 pediatric and neonatal patients, and invasive fungal infection settings, collectively reflecting the field’s transition from model development to clinical deployment. 36
3.7. Keywords and research hotspots
3.7.1. Keyword analysis
The co-occurrence network of high-frequency keywords was perform with the aid of VOSviewer software which produced four thematic (Figure 8(a)). The red cluster, whose core terms were “popPK,” “TDM,” “vancomycin,” “MIPD,” “NONMEM,” and “external evaluation”, represents the methodology of MIPD and TDM implementation. The appearance of the keywords “pediatrics,” “neonates,” “tacrolimus,” “voriconazole,” and “linezolid” demonstrates that Bayesian-informed dosing is now extending to multiple narrow-therapeutic-window drugs and patient populations. The green group, which consists of “PK,” “PD,” “critical care,” “Monte Carlo simulation,” “beta-lactams,” and “PTA,” encompasses the PK/PD-guided dosing optimisation in critical care, where the Monte Carlo simulation is applied in the prediction of probability of target attainment for time-dependent antibiotics in patients with abnormal physiology. The “CRRT” and “RRT” nodes further illustrate how renal replacement therapy affects the intensity of pharmacokinetic variability in critically ill patients. The blue cluster contains “aminoglycosides,” “gentamicin,” “neonates,” and “antifungal agents,” reflecting the need for dedicated popPK models in neonatal and pediatric populations, in whom pharmacokinetic changes during maturation render simple weight-based dose extrapolation from adults scientifically untenable. The yellow cluster, which mainly features “colistin” and Pseudomonas aeruginosa,” is representative of PK/PD-guided doses for carbapenem-resistant gram-negative bacterial infections: these are agents of last resort with an extremely narrow therapeutic window and nephrotoxicity. Consequently, model-informed dosing are particularly important. It is important to note that the node “AI” is located on the periphery of the red cluster, which also contains the terms “popPK” and “MIPD”. Its present low co-occurrence frequency and marginal position in the network suggest that the incorporation of artificial intelligence with established pharmacometric frameworks is still in its early stage – that is, it is not mainstream yet. This finding is consistent with the classification of AI in this study as an “emerging application” which is further corroborated by citation burst analysis. Keyword analysis revealing research structure, temporal evolution, and emerging frontiers. (a) Co-occurrence network and clustering of keywords. (b) Temporal overlay of keyword emergence, using color gradients to visualize research evolution, blue represent early and yellow means recent. (c) Trend topics over time, the bubble size represents research volume. (d) Top 25 keywords with strongest citation bursts, the red bars indicate burst periods, with intensity reflecting the strength of increased attention.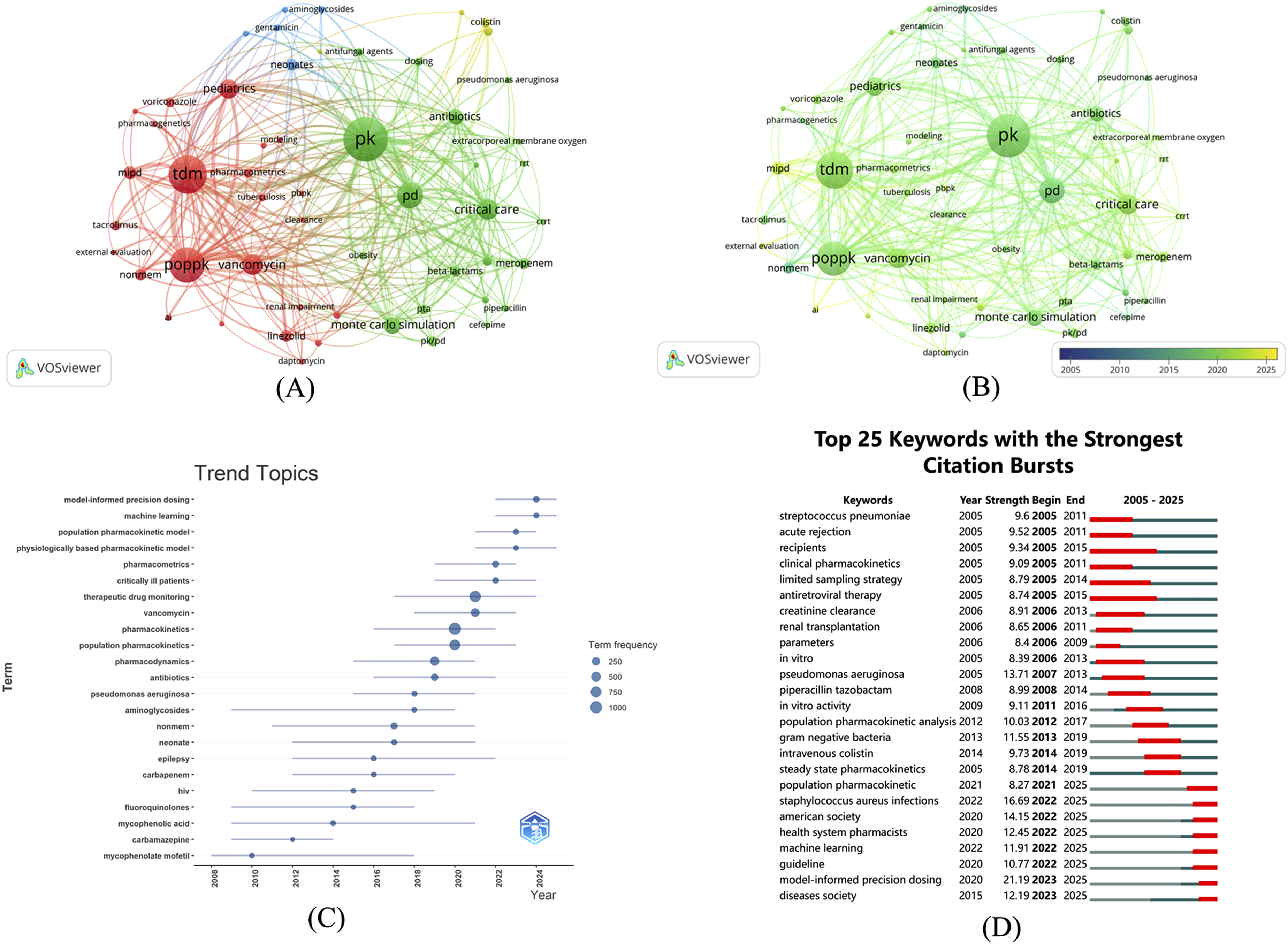
3.7.2. Research hotspots
Both the time-overlay map presented in VOSviewer (Figure 8(b)) and the trend graph illustrated in Bibliometrix (Figure 8(c)) delineate the evolutionary course over the last twenty years, which can be categorized into three principal phases.
Early research was dominated by foundational pharmacometric methods, with “aminoglycosides,” “NONMEM,” “neonate,” “carbapenem,” “fluoroquinolones,” and “HIV” among the high-frequency terms of this period. The early appearance of “mycophenolate mofetil” and “carbamazepine” indicates that popPK modeling had begun to extend into transplant anti-rejection and neuroscience domains, accumulating methodological experience that would subsequently inform anti-infective precision dosing applications. During the intermediate period, more interest was paid to the clinical application of PK/PD, characterized by increased use of terms including “population pharmacokinetics,” “pharmacokinetics,” “pharmacodynamics,” “vancomycin,” “therapeutic drug monitoring,” and “Pseudomonas aeruginosa”. The term “critically ill patients” and “pharmacometrics” appeared to be concentrated together as there were many clinical references to individual pharmacokinetic variability. In the ICU, disease states can significantly alter drug disposition which often results in standard dosing regimens being inadequate. As a result, model-informed dosing becomes most important. In recent years, “model-informed precision dosing” and “machine learning” have simultaneously emerged as the two most persistently growing high-heat topics, with concurrent increases in citations of “population pharmacokinetic model” and “physiologically based pharmacokinetic model” (PBPK), indicating that the field’s research methods are no longer confined to conventional compartmental models. The simultaneous emergence of these two themes reflects the extension of research from pharmacometric foundational methods toward emerging AI applications, with machine learning representing an active emerging direction that currently remains methodologically distinct from mainstream MIPD practice and has yet to achieve deep integration.
3.7.3. Citation bursts and future trends
The sequence of research frontiers is further revealed by the Top 25 burst keywords list (Figure 8(d)). In the early burst phase (2005–2014), terms such as “Pseudomonas aeruginosa,” “recipients,” and “limited sampling strategy” clustered prominently, reflecting popPK modeling work for immunosuppressants, antiretroviral drugs, and anti-pseudomonal agents during this period, alongside methodological exploration of practical TDM sampling strategies. In the intermediate burst phase (2012–2020), “population pharmacokinetic analysis,” “gram-negative bacteria,” and “intravenous colistin” successively intensified, reflecting systematic scholarly attention to the PK/PD characteristics of multidrug-resistant pathogens and the pharmacology of polymyxins. In the present burst phase (2021–2025), “model-informed precision dosing” registered the highest burst intensity in the entire dataset. Thus, MIPD has progressively transitioned from early investigational exploration to clinical consensus and standardised practice. Simultaneously, “machine learning” also shows substantial intensity of bursts which confirms this as an active emerging direction which is methodologically distinctive from a traditional MIPD framework but is nevertheless the subject of research increasingly seeking to combine the two.
Concerning evaluation frameworks, classical MIPD commonly utilizes Bayesian posterior predictive performance, the proportion of patients reaching PK/PD targets, and pharmacokinetic metrics, notably bias and precision, as the primary evaluation criteria; machine learning dosing models more often utilize data-driven performance measures such as area under the receiver operating characteristic curve, cross-validated prediction accuracy, and feature importance rankings. Not having an identical, clinically relevant common endpoint between the two evaluation paradigms also limits regulatory acceptance of machine learning tools and clinical uptake. Addressing this issue requires the establishment of harmonized validation standards that simultaneously account for pharmacokinetic accuracy and patient clinical outcomes. The concurrent bursts of “american society,” “health system pharmacists,” “diseases society,” and “guideline” reflect active efforts by international academic bodies such as ASHP and IDSA to advance the development of MIPD-related guidelines and standards.
Synthesizing the patterns of bursts described above, the current research frontier is concentrated on prospective clinical validation of MIPD and machine learning-assisted dosing tools, integration with electronic medical record systems, clinician comprehension and use of model outputs, and alignment with antimicrobial stewardship daily workflows.
4. Discussion
4.1. Global challenges in anti-infective therapy and key drivers of MIPD
Antimicrobial resistance (AMR) contributed to approximately 5 million deaths in 2019,a figure projected to increase substantially before 2050. 37 Most often inter-patient pharmacokinetic (PK) variability is ignored in traditional empirical dosing. As a result, part of critically ill patients do not achieve the anticipated pharmacodynamic target when receiving the usual doses of β-lactam antibiotics. 38 To overcome this challenge, a model-informed precision dosing paves the path from “empirical medicine” to “precision medicine” through the integration of population pharmacokinetic (PopPK) models, patient characteristics and monitoring in real time.17,39,40
The year 2013 was a turning point for explosive growth in this area (Figure 2), owing to the interplay of technical, clinical and regulatory factors. On the one hand, the growing maturity of pharmacometric modeling software (e.g., NONMEM) and related open-source tools (e.g., R packages) has greatly lowered the technical barriers. 41 The burst strength of “Monte Carlo simulation” was extremely high during that period. The United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA), on the other hand, successively published guidelines in favour of the use of PopPK/PD modelling for the development of novel medicines, which coincides temporally with the worldwide advent of multidrug-resistant pathogens.42,43
The global research landscape exhibits pronounced geographic disparities in both output and impact. The continued underrepresentation of South America, Africa, and the Middle East warrants particular attention from the international community, underscoring the urgent need for greater investment in research capacity building and resource sharing.
4.2. Evolution of MIPD in core anti-infective drug classes
The development of β-lactams, vancomycin, and polymyxins is central to MIPD evolution. The co-citation network (Figure 7(a)) reveals four thematic clusters reflecting this evolution: a PK/PD and renal function foundation cluster anchored by Cockcroft and Craig; a popPK methodology cluster; a vancomycin TDM guideline evolution cluster; and a last-resort antibiotic dosing optimization cluster—collectively tracing the trajectory from theoretical modeling to clinical standardization.
Beta-lactams have dominated antibiotic PK/PD modeling research owing to their well-defined time-dependent PK/PD relationships. Despite solid theoretical models supporting continuous infusion strategies, various physical and operational hurdles remain specifically, drug stability, line compatibility and lack of reliable TDM used in practice. 10
In contrast with other antibiotics, vancomycin is the prime example of MIPD. The success of vancomycin’s therapeutic monitoring is mainly attributed to the narrow therapeutic index and the clear pathway recommendations such as the recommendations in the 2020 Infectious Diseases Society of America (IDSA) and the American Society of Health-System Pharmacists (ASHP) consensus which specifically says the dosing target should shift from trough-guided to AUC guided. 44 Additionally, the FDA approval of Bayesian Forecasting Software has also increased its widespread availability. The concurrent citation bursts of “american society,” “health system pharmacists,” “diseases society,” and “guideline” in the citation burst analysis (Figure 8(d)) represent pivotal milestones marking the standardization of vancomycin MIPD, and exemplify how regulatory recognition and professional society consensus can accelerate clinical translation. The success of MIPD will not only rely on scientific data, but also necessitate standardized protocols, regulatory approval, and integration into routine clinical practice, reflecting the deeper dynamics of clinical translation. This shows a deep law of clinical translation.
Moreover, we have recognized an intensive citation burst for polymyxins (2015–2020), 35 coinciding with the emergence of cluster #2 “polymyxin B” in the timeline view (Figure 7(c)), reflecting the urgent need for MIPD in agents with an extremely narrow margin between efficacy and nephrotoxicity. Of note, cluster #6 “linezolid pharmacokinetics” showed an active period on the timeline closely paralleling that of cluster #2; together, they represent a key consolidation phase during which MIPD principles were extended to last-resort antibiotics with extremely narrow therapeutic windows, where drug exposure is closely associated with serious adverse effects such as thrombocytopenia and Bayesian-guided individualized dosing holds important clinical value for optimizing the efficacy-toxicity balance. Continued attention on antifungals (e.g., voriconazole), which indicate that MIPD is indispensable for treating the immunocompromised, those with severe infection or drugs that have a narrow therapeutic index. 45
4.3. Crucial role in special populations
Critically ill patients are the most important target population of MIPD. In the ICU, the pathophysiological changes like capillary leak, hypoalbuminemia, augmented renal clearance (ARC), or continuous renal replacement therapy (CRRT) applications make the pharmacokinetics of patients very unstable, directly reflected in the tight co-clustering of “critically ill patients,” “crrt,” “monte carlo simulation,” and “pta” in the keyword co-occurrence analysis (Figure 8(a)).
Many investigations have shown the serious clinical effects of these pathophysiological alterations. Part of those patients with ARC who have severe sepsis are still on underdosing of antibiotics in spite of maximal recommended dose. The underdosing is associated with higher treatment failures and prolonged stay. 46 While prospective trials show that Bayesian-guided MIPD can improve target attainment rates while reducing nephrotoxicity, 47 gaps in evidence remain.
Pediatric populations, especially neonates, represent another important frontier. The co-citation timeline (Figure 7(c)) identifies clusters #3 “critically ill children” and #5 “very young infants” as active frontiers, while the clustering of “aminoglycosides,” “gentamicin,” and “neonates” in the blue cluster of the keyword co-occurrence network (Figure 8(a)) collectively reflects sustained scholarly investment. Given that glomerular filtration rates and hepatic metabolic enzymes are undergoing active maturation in children, direct extrapolation of adult doses is scientifically untenable, 48 and dedicated popPK models integrating gestational age and birth weight have been used to support aminoglycoside dosing interval optimization. 49 The future goal of expanding MIPD to frail elderly and patients with severe hepatic impairment is an important target requiring good prospective validation.
4.4. Specific barriers to clinical translation: From bedside operations to system integration
Despite significant academic advances, specific operational barriers to routine bedside application of MIPD persist. With regard to sampling design, the accuracy of the Bayesian posterior estimates relies heavily on the timing of the concentration sample collection; sampling windows are often interrupted by nursing care activities in critically ill patients, and the development and validation of limited sampling strategies (LSS) represent an important pathway for reducing operational burden. Regarding clinician acceptance, decision-making dilemmas arising when model recommendations conflict with clinical intuition are commonplace, necessitating enhanced pharmacometric training and improved interpretability of software interfaces. 50 Regarding interpretability and accountability, the decision-making processes of black-box machine learning algorithms lack transparency; when model recommendations lead to adverse outcomes, the boundaries of accountability among developers, prescribing physicians, and healthcare institutions remain unclear under current regulatory frameworks, and the establishment of clear accountability frameworks, concurrent with tightening FDA/EMA regulation of SaMD is urgently needed. 51 Regarding antimicrobial stewardship integration, embedding MIPD into AMS daily workflows, including Bayesian assessment triggered by TDM results and recommendation delivery at the point of order entry is an organizational prerequisite for scaled implementation, and the long-term impact on patient outcomes requires confirmation through prospective studies. 52 At the technical level, EHR integration represents a critical technical bottleneck for scaled application. Most MIPD software cannot as yet interface automatically with hospital EMRs, requiring manual data entry by pharmacists, a substantial burden in busy ICU environments. 50 The dual citation bursts for “guideline” and “diseases society” in Figure 8(d) reflect a shared clinical imperative for standardization and integration.
4.5. The emerging role of AI and ML
Synthesizing the bibliometric findings of this study, the field exhibits a clear three-phase evolutionary trajectory. In the foundational phase, the seminal works of Cockcroft, Craig, and Drusano in the co-citation network established the theoretical PK/PD foundations; NONMEM modeling and aminoglycoside/vancomycin parameter estimation constituted the core work; and Rybak’s (2009) vancomycin TDM consensus marked the transition from empirical practice toward evidence-based standards. In the consolidation phase, Roberts JA’s DALI study systematically demonstrated the systematic inadequacy of standard dosing in the ICU; Bayesian dosing software progressively entered the regulatory scope of SaMD; and the IDSA/ASHP 2020 consensus shifting the vancomycin target from trough concentration to AUC represented an important breakthrough for the MIPD concept at the guideline level. In the current phase, “model-informed precision dosing” recorded the highest citation burst intensity in the dataset, with standardization entering an accelerated period; “machine learning” burst simultaneously but with lower network centrality, reflecting AI integration at a nascent rather than mature stage, with prospective clinical validation representing the current core gap.
4.6. Future research priorities
Based on our analysis, future research should prioritize the following three directions: (1) Responsible integration of emerging AI applications: Deep learning holds promise for capturing complex physiological relationships, but prospective clinical validation, regulatory-grade interpretability, and clear accountability frameworks are necessary prerequisites for safe deployment. Developing harmonized validation frameworks that simultaneously incorporate pharmacokinetic fidelity and patient clinical outcomes is key to bridging the methodological gap between the two paradigms. (2) Redefining Clinical Endpoints: Large-scale pragmatic RCTs and real-world EMR studies are needed to confirm the substantive impact of MIPD on clinical cure rates and mortality, thereby supporting fundamental changes in clinical pathways and reimbursement policies.
53
(3) Frontloading Drug Development: For novel beta-lactam/beta-lactamase inhibitor combinations, early introduction of the MIDD framework is recommended, with MIPD integrated concurrently with Phase II/III study designs rather than applied retrospectively post-approval.
43
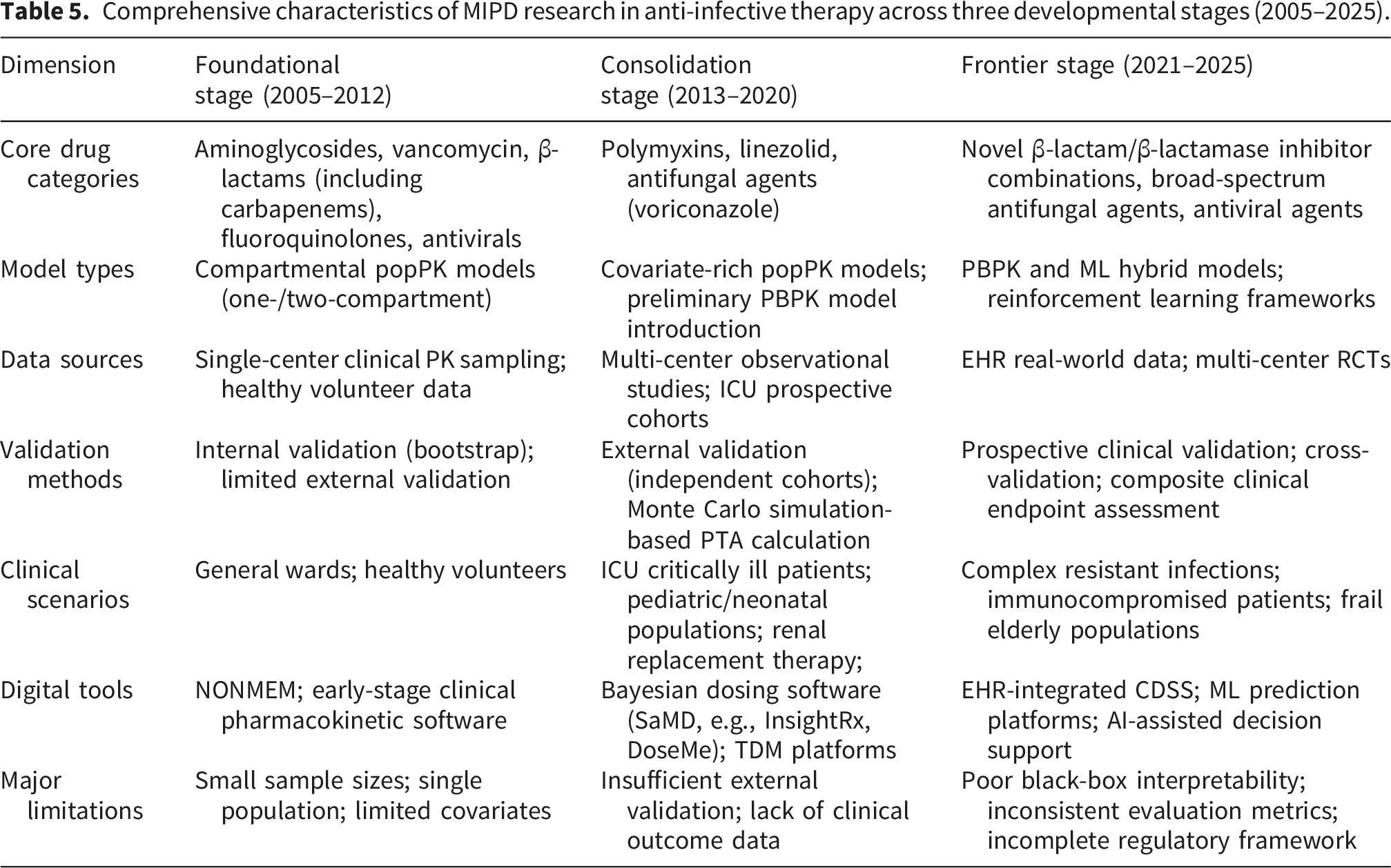
To synthesize these findings, Figure 9 provides a comprehensive timeline mapping the evolution of MIPD research from methodological foundations to AI integration. Furthermore, Table 5 systematically outlines the three-stage research characteristics across seven dimensions including drug classes, model types, data sources, validation methods, clinical settings, digital tools, and main limitations to enhance the practical clinical value of this review. Comprehensive timeline of Model-Informed Precision Dosing (MIPD) research evolution (2005–2025). This timeline integrates bibliometric data with key methodological and clinical milestones to illustrate the three-stage evolution of MIPD research: the foundational Phase (2005–2012), the consolidation Phase (2013–2020), and the frontier Phase (2021–2025). Comprehensive characteristics of MIPD research in anti-infective therapy across three developmental stages (2005–2025).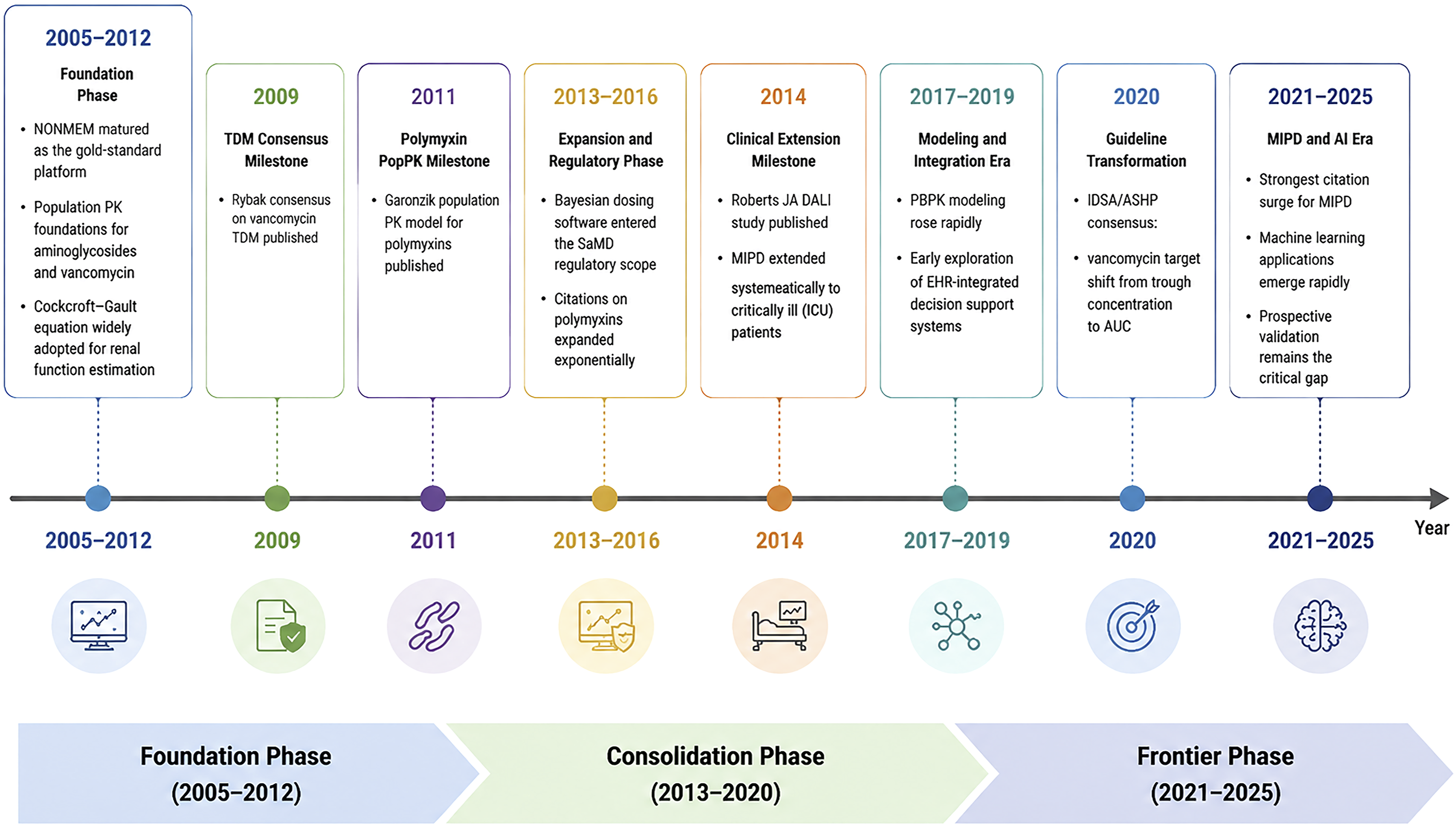
4.7. Limitations
Initially, we performed the bibliometric analysis solely on the WoSCC database, which may have excluded some grey literature as well as full texts of clinical guidelines in languages other than English or that are not indexed. Despite enhancements made to the search strategy to optimize disciplinary relevance, the broad nature of popPK terminology means some records at the edges of the disciplines may have inconsistently made the inclusion and exclusion decisions. Moreover, citation network analysis suffers from temporal lag effects; studies published within the past two years of high quality may be missing from network visualization due to not gaining enough citations especially true for emerging AI/ML clusters. As the search strategy was centred on established terminology for MIPD and anti-infectives and not on terminology peculiar to AI, studies utilising machine learning or deep-learning methods but not explicitly referring to the MIPD framework may have been missed. Future bibliometric studies with AI-specific search strategies would be useful. Ultimately, this research was aimed at the identification of macro level developmental trends; future works should comprise a systematic review focused on specific multidrug resistant organisms or innovative computational approach.
5. Conclusion
This bibliometric analysis provides a comprehensive mapping of MIPD research for anti-infective therapy spanning two decades. By analyzing 4,601 publications from the WOSCC using CiteSpace, VOSviewer, and Bibliometrix, the following was established: the United States led global output with 1,454 publications; Australia demonstrated the highest citation impact with the greatest CPP (42.97); the Netherlands played a key bridging role in the European collaboration network with the highest TLS (765); the University of Queensland and Roberts JA were the most productive institution and author, respectively; and *Antimicrobial Agents and Chemotherapy* served as the most central publication platform in the field. Geographically, research participation from South America, Africa, and the Middle East remains markedly insufficient, reflecting persistent global imbalances in research capacity.
This study documents a coherent three-phase developmental trajectory. The foundational phase centered on population pharmacokinetic model construction and PK/PD parameter estimation; the consolidation phase saw systematic promotion of Bayesian forecasting in clinical TDM practice; and the current frontier phase has witnessed MIPD transition from investigational exploration to clinical consensus and standardized practice, with machine learning frameworks simultaneously emerging as a complementary direction that currently remains methodologically distinct from the traditional MIPD framework and has yet to achieve deep integration.
There are key barriers to further progress identified in this study. First, traditional MIPD and new machine learning developments have different paradigms for what constitutes validation. Second, automated integration between MIPD software and hospital electronic medical records is immature and further limits access within everyday clinical workflows.
Regarding future research directions, this study identifies the responsible integration of emerging AI applications, the prospective redefinition of clinical endpoints, and the systematic front-loading of model-informed approaches into early drug development as the priority tasks for the field.
Achieving these goals and ensuring that the clinical translation of MIPD yields quantifiable improvements in patient survival will require sustained, in-depth, and globally coordinated multidisciplinary collaboration among pharmacometricians, clinicians, informaticists, and regulatory agencies.
Supplemental material
Supplemental material - From pharmacometric foundations to emerging artificial intelligence applications: A bibliometric analysis of model-informed precision dosing for anti-infective therapy (2005–2025)
Supplemental material for From pharmacometric foundations to emerging artificial intelligence applications: A bibliometric analysis of model-informed precision dosing for anti-infective therapy (2005–2025) by Xuejing Li, Wenfeng Chen, Xuan Wang, Xiang Li in DIGITAL HEALTH.
Supplemental material
Supplemental material - From pharmacometric foundations to emerging artificial intelligence applications: A bibliometric analysis of model-informed precision dosing for anti-infective therapy (2005–2025)
Supplemental material for From pharmacometric foundations to emerging artificial intelligence applications: A bibliometric analysis of model-informed precision dosing for anti-infective therapy (2005–2025) by Xuejing Li, Wenfeng Chen, Xuan Wang, Xiang Li in DIGITAL HEALTH.
Footnotes
Acknowledgments
The authors would like to thank those individuals who made the VOSviewer, Citespace and the R package “bibliometrix” opensource software available.
Ethical considerations
No patients were involved in this research, so the ethical approval is not required.
Author contributions
Xuejing Li: Conceptualization, Methodology, Visualization, Writing - original draft. Wenfeng Chen: Methodology, Investigation. Xuan Wang: Methodology, Data curation, Formal analysis, Software, Visualization. Xiang Li: Conceptualization, Project administration, Writing - review & editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets analyzed during this study are available in the Web of Science core collections.
Guarantor
The guarantor of this manuscript is XL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.