
Abstract
Objective
To evaluate the performance and potential of the DeepSeek-R1 in telemedicine consultations for gynecological oncology diseases, comparing its responses with those of human doctors on prominent Chinese online medical platforms.
Methods
A total of 600 online consultation cases covering four gynecological oncology diseases were collected from “Ding Xiang Doctor” and “Good Doctor Online.” After excluding unsuitable cases, 82 were selected. DeepSeek-R1 generated responses based on patients’ questions and information, which were anonymized and evaluated alongside human doctors’ replies by three professional gynecologists. Seven dimensions were assessed: medical accuracy, clinical applicability, communication effectiveness, safety and compliance, popular science translatability, humanistic care, and overall satisfaction. Statistical analysis was performed using non-parametric tests.
Results
DeepSeek-R1 significantly outperformed human doctors across all seven evaluation dimensions (p < 0.0001). Among the seven evaluated dimensions, it scored highest in humanistic care, while human doctors scored highest in medical accuracy. Both groups achieved their lowest scores in popular science translatability. DeepSeek-R1’s responses were more comprehensive and logically structured but tended to be lengthy, which could increase the cognitive load on patients.
Conclusions
DeepSeek-R1 demonstrates strong potential in remote gynecological oncology telemedicine, outperforming human doctors in accuracy, applicability, communication, safety, and humanistic care. However, its responses are often lengthy, potentially increasing patient cognitive load, and both DeepSeek-R1 and human doctors show limitations in effectively translating medical knowledge for public understanding. Future work should focus on optimizing the conciseness of LLM responses and enhancing patient-centered communication to improve telemedicine quality and accessibility.
Keywords
Introduction
Women’s health has always been a major global health concern.1,2 Gynecological oncology diseases are known for being diverse, with different levels of benignity and malignancy, and various presentations. 3 This means that early intervention and treatment, as well as effective care in the late stages of the disease, are essential. For example, ovarian cancer is a malignant gynecological tumor that has always posed a significant threat to women’s lives and health. 4 It has placed a substantial burden on people’s lives and health in various countries and remains one of the most challenging malignancies for medical practitioners to overcome.5–7 Nevertheless, due to atypical early symptoms and rapid disease progression, patients are often diagnosed in advanced stages with a poor prognosis. 4 Therefore, early screening and timely, effective medical advice for suspected cases are essential. However, due to uneven regional economic development, inadequate social infrastructure, and the unbalanced distribution of medical resources, many women in developing countries around the world do not have access to quality healthcare services or timely medical advice. 8 Fortunately, the continuous development of internet technology and the emergence of telemedicine have greatly alleviated this problem.
Telemedicine refers to the medical form in which healthcare providers use an online platform to offer medical consultations, diagnostic recommendations, and therapeutic advice to patients in need, either free of charge or for a fee. 9 Telemedicine enables quality medical resources to reach a wider area, 10 and it is convenient for patients and their families. It also helps medical workers conduct more in-depth disease screening, thus increasing the early detection rate and reducing the death rate. Additionally, it provides valuable data for doctors and epidemiologists to use in epidemiological disease investigations. Studies have demonstrated the importance of telemedicine in chronic disease management.11–16 For example, in the management of atrial fibrillation, telemedicine can connect experts with village doctors. 16 Through this connection, experts can provide consultations and guidance for difficult cases. The platform can also provide continuous education for village doctors, who can conduct in-depth follow-up visits to patients’ homes. 16 The results of the study showed that patient compliance increased and complex cardiovascular events decreased with this format. This program is both sustainable and replicable, representing a new solution to the global problem of rural chronic disease management, as represented by atrial fibrillation. 16 Furthermore, another study has demonstrated that it is useful to utilize mobile CT scanners with remote artificial intelligence (AI) assistance for telemedicine-enhanced lung cancer screening in underserved communities. It not only can reduce barriers to healthcare access for these communities but also promote the early diagnosis and treatment of lung cancer. Furthermore, leveraging AI can significantly enhance the efficiency and quality of processing screening results. 17 Other studies have also revealed the significant value of telemedicine in managing diseases for elderly patients with type 2 diabetes, as well as in providing care services for older adults who are housebound.18,19
In China, “Ding Xiang Doctor” and “Good Doctor Online” are two well-known telemedicine platforms. Through these platforms, patients can access high-quality medical care. Under the platforms’ supervision, most of the doctors’ opinions are valuable. With personal information withheld, the platforms select a series of typical consultations for people’s reference, which are also of high quality. However, accessing medical consultations on both platforms still has a number of limitations. Firstly, telemedicine services on these platforms are costly, and the number of Q&A sessions is limited. Second, doctors are still required to respond online, often at the expense of their rest time. This increases their workload and makes it difficult for them to respond to medical consultations. To solve these problems, people are turning to artificial intelligence, and large language models (LLMs) are playing an increasingly significant role in telemedicine.
Among all kinds of LLMs, Chat Generative Pre-trained Transformer (ChatGPT) has been attracting a lot of attention, and there have been numerous researches on the use of ChatGPT in telemedicine. In 2024, some researchers analyzed the effectiveness of using ChatGPT in telemedicine for orthopedic-related diseases and found that ChatGPT was more effective than human doctors for popularizing medical knowledge. 20 The scholar also found that ChatGPT was not significantly different from human doctors in other aspects, ultimately concluding that ChatGPT could assist doctors in telemedicine. 20 Recently, China has also made significant progress in developing LLMs. One notable model is DeepSeek, which has received global attention due to its excellent performance and relatively low API price.21,22 The DeepSeek-V3 model is reported to outperform other advanced LLMs, such as Claude-3.5 and GPT-4, in a number of domains, while DeepSeek-R1, which was released on January 20, 2025, is claimed to outperform OpenAI-o1 in a variety of tasks. Studies have explored DeepSeek’s performance in the Chinese National Medical Licensing Examination 23 and in the gastroenterology board examination. 24 However, compared to ChatGPT, the application of DeepSeek-R1 in telemedicine, especially for gynecological oncology diseases, has not been studied in depth.
This study aims to evaluate the performance of DeepSeek-R1 in gynecological oncology telemedicine by comparing its responses with those of human doctors on the platforms “Ding Xiang Doctor” and “Good Doctor Online.”
Methods
Study design
This was a retrospective comparative study designed to evaluate the performance of the DeepSeek-R1 large language model in providing teleconsultations for gynecological oncology diseases, compared with human doctors on online platforms. The study was conducted from April 2025 to October 2025 at the Department of Gynecology, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai, China. This study includes a series of anonymous relevant cases published on the two major platforms, “Ding Xiang Doctor” and “Good Doctor Online”, between 2018 and 2025.
Data sources
“Ding Xiang Doctor” and “Good Doctor Online” are two prominent online medical consultation platforms in China. Both platforms have amassed a substantial corpus of online consultation information related to gynecological oncology diseases on their web pages. Furthermore, both platforms exhibit a range of archetypal and prevalent online consultation dialogues subsequent to the anonymization of patient-related privacy information. This enables doctors and patients to access the information while effectively protecting patient privacy. For each category of diseases, the websites provide detailed classifications, with each disease showcasing approximately 100 typical consultations. A comprehensive consultation information database was compiled, encompassing four prevalent and severe gynecological oncology diseases. The four conditions under consideration are ovarian cancer, endometrial cancer, cervical cancer and vulvar cancer. These four malignancies represent the most prevalent and fatal gynecological oncology diseases in China and globally, with abundant text-based teleconsultation data on the selected platforms, and their distinct clinical characteristics enable a comprehensive evaluation of DeepSeek-R1’s performance in gynecological oncology telemedicine. The total number of consultation cases collected for this study is 600.
Cases screening
However, during the collection process, it was noted that many consultation records contained incomplete basic information, incomplete pathological information, and incomplete laboratory results. Furthermore, numerous consultations entailed the analysis of images; however, the present study is chiefly concerned with evaluating DeepSeek’s capacity to analyze and process textual information. Additionally, a significant proportion of inquiries were addressed through voice responses from doctors. Due to potential inaccuracies in transcription, doctor responses in voice format were excluded. Consequently, inquiry cases were excluded from the study’s scope. After meticulously examining the aforementioned criteria, a total of 82 patient cases were identified as meeting the necessary requirements (Figure 1). We collected the information from these two websites on 82 inquiry cases. This study complies with the provisions of the Health Insurance Portability and Accountability Act (HIPAA) of 1996.
25
Amount of included cases for each gynecological oncology diseases.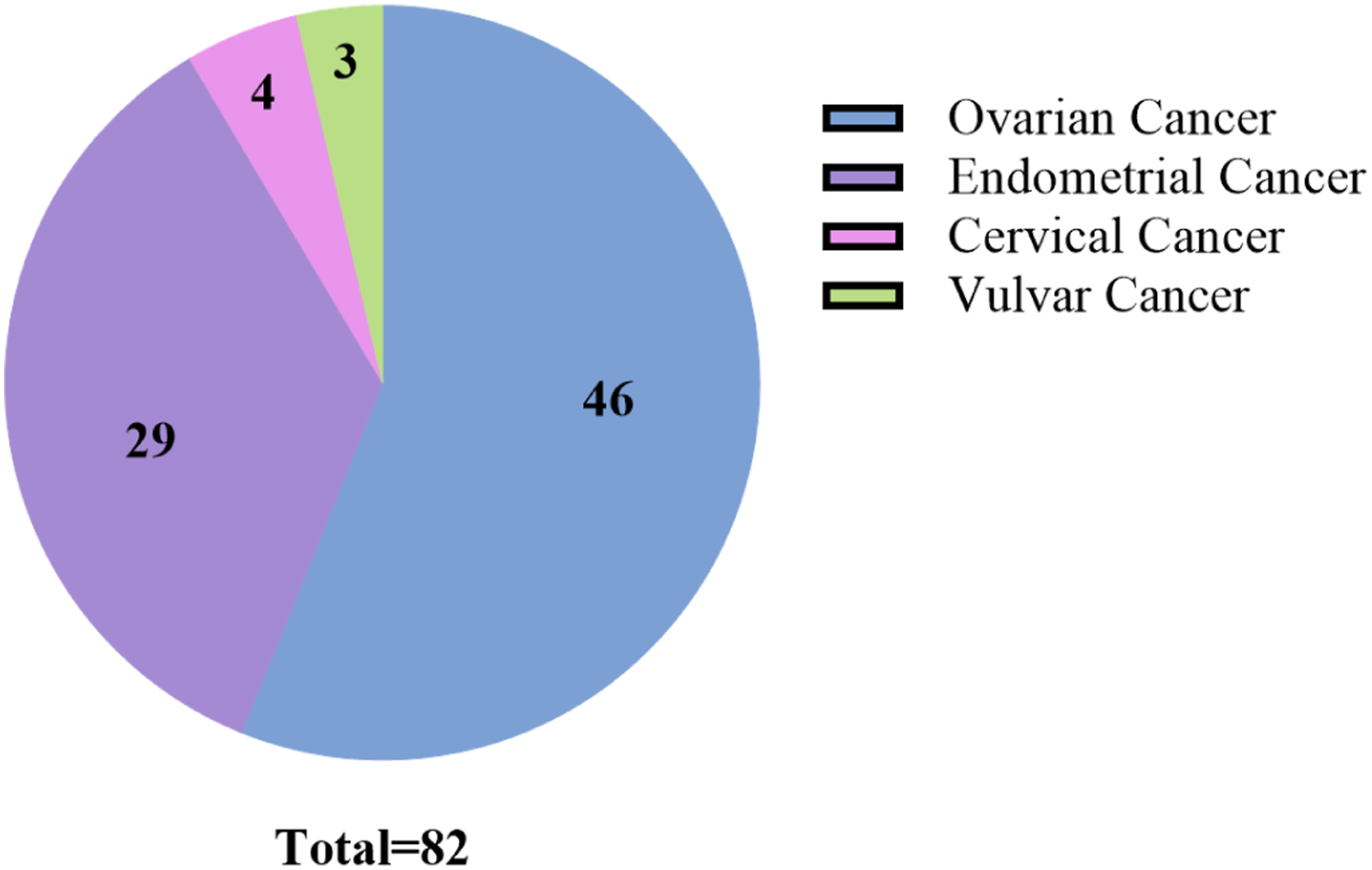
Data collection
Following the compilation of case information, the aforementioned inquiries were directed to the DeepSeek-R1 model for response. In order to prevent interference between different cases, a new conversation was initiated for each case’s response. Furthermore, to optimize the quality of the responses, a prompt was provided at the commencement of each conversation. “You are an expert in the field of obstetrics and gynecology. Assume you are currently conducting an online telemedicine consultation as a doctor. I will now provide you with a patient’s medical information from an online consultation. Please respond based on the information provided. Please note that the response should be precise, concise, and reflect a humanistic touch, expressing care for the patient.” Subsequent to receiving a response from DeepSeek-R1, the original doctor’s response on the website and DeepSeek-R1’s response were submitted to three professional obstetricians and gynecologists for evaluation. To reduce potential errors, the source of the responses was anonymized. To minimize potential unblinding due to formatting differences, all AI-generated responses were stripped of Markdown elements, bulleted lists, and other visual formatting cues. Specialists did not know whether the answers they were evaluating came from human doctors or DeepSeek-R1. We asked them to evaluate each response from seven perspectives: medical accuracy (MA), clinical applicability (CA), communication effectiveness (CE), safety and compliance (SAC), popular science translatability (PST), humanistic care (HC), and overall satisfaction (OS), with a scoring range of 1-10 points. The OS is the mean of the initial six items.
Evaluation criteria
The MA primarily evaluates the accuracy of basic medical knowledge, the alignment of treatment recommendations with the latest clinical guidelines, and the comprehensiveness of differential diagnosis coverage. The CA focuses on the applicability of responses to specific patient circumstances, such as age, medical history, and allergic history. CE primarily evaluates the logical organization of information, the prominence of key information, and the clarity of content. SAC assesses whether responses pose medical risks, such as misguidance or delayed treatment. PST assesses the ability to translate relevant medical knowledge into understandable content for the general public. HC assesses the degree of attention paid to patients’ emotional and psychological needs. OS reflects the overall acceptance of the response.
Statistical analysis
Following the acquisition of specific scores, the data underwent processing with GraphPad Prism 10.3.1 software. For each evaluation perspective, the mean score of the three doctors’ evaluations for each case was first calculated. This process yielded a total of 82 scoring data points for each perspective, encompassing both the doctors’ responses and those provided by DeepSeek. Subsequently, a comparative analysis was conducted on the scoring data for the doctors’ answers and DeepSeek’s answers within the same perspective.
We used GraphPad Prism 10.3.1 to perform the Kolmogorov-Smirnov test and Wilcoxon matched-pairs signed rank test.
Initially, the Kolmogorov-Smirnov test was employed to ascertain whether each set of data followed a normal distribution. The results indicated that none of the variables exhibited a normal distribution. Next, given the paired design (each case evaluated by both DeepSeek-R1 and human doctors) and the non-normal distribution of the data, we employed the Wilcoxon matched-pairs signed rank test as the primary analytical approach to assess whether the median of paired differences significantly deviated from zero. When the p-value obtained from the Wilcoxon matched-pairs signed rank test was less than 0.05, the difference was considered statistically significant. Subsequently, we further utilized GraphPad Prism 10.3.1 to generate column bar charts, thereby more vividly demonstrating the differences between the two sets of data across various perspectives. Furthermore, the mean values of the 82 scoring data points under each perspective were calculated, and a radar chart was plotted using RStudio (Version: 2026.01.1+403) and R (version 4.5.0). This method enabled a more intuitive comparison of the performance differences between the two sources of answers. We calculated the effect size (r) using the Z-value obtained from the Wilcoxon matched-pairs signed rank test to verify sample size sufficiency. A value of r ≥ 0.5 indicates a large effect, supporting that the sample size was adequate to identify the significant differences observed. Intraclass Correlation Coefficient (ICC, two-way mixed effects, absolute agreement) was calculated using RStudio (Version: 2026.01.1+403) and R (version 4.5.0) to assess inter-rater reliability across all seven dimensions, where ICC > 0.75 indicated high agreement, 0.40-0.75 indicated moderate agreement, and ICC < 0.40 indicated poor agreement.
Results
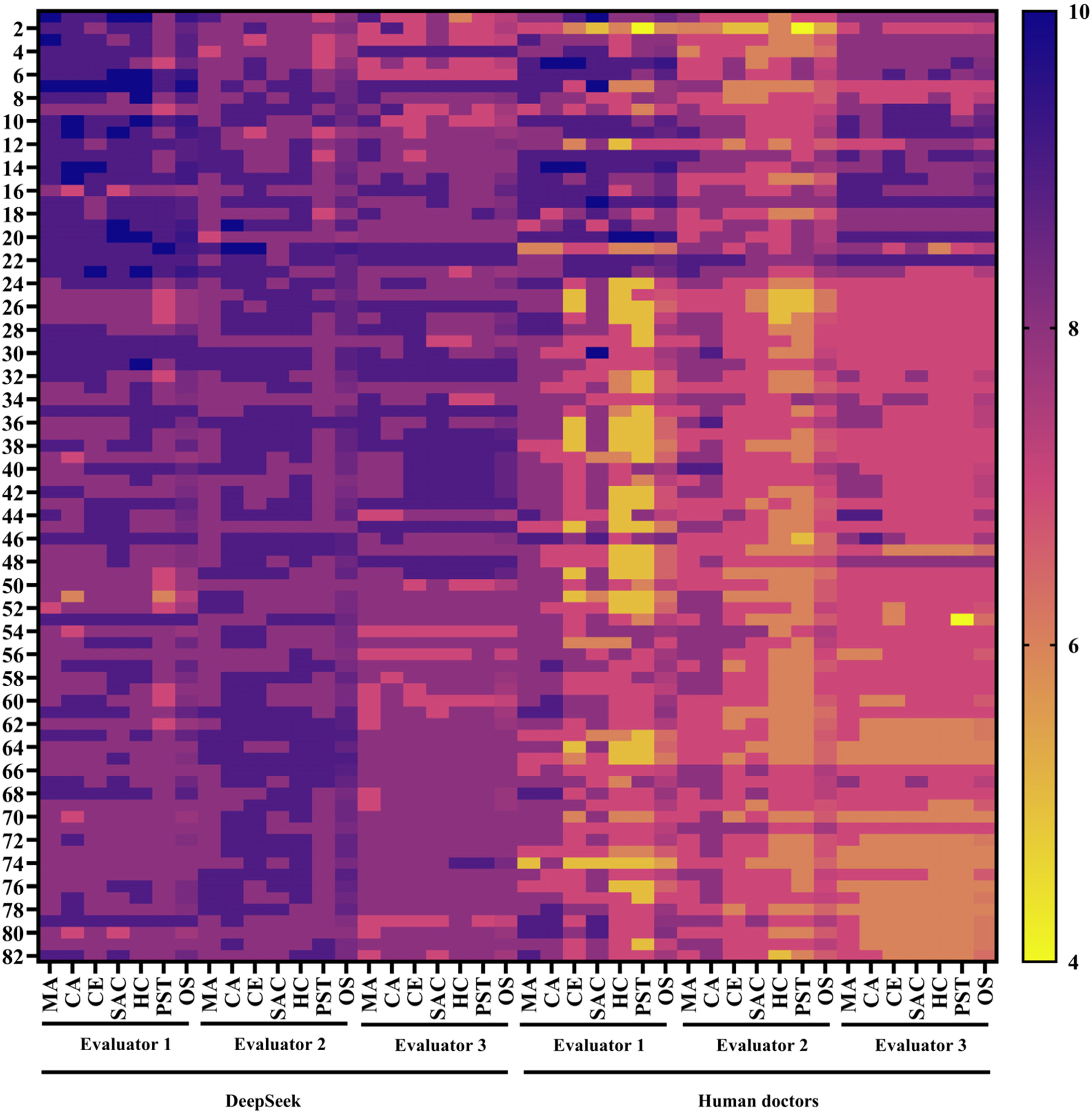
We selected four common gynecological oncology diseases from “Ding Xiang Doctor” and “Good Doctor Online,” totaling 600 cases, including ovarian cancer, endometrial cancer, cervical cancer and vulvar cancer. Many of these cases included voice responses, while others contained images or required image analysis. We used these two criteria to screen out 489 cases at the outset. We then assessed the completeness of related information, such as personal basic information, pathology reports, and laboratory reports. We removed 29 cases with incomplete information, leaving 82 cases that met the requirements. After anonymizing the sources, we provided the doctors’ responses and the corresponding DeepSeek responses for the cases that met the criteria to three professional obstetricians and gynecologists for evaluation. Figure 2 illustrates this process completely. Figure 3 presents all scoring results in the form of a heatmap. We then conducted a statistical analysis to derive a series of results. Flowchart of the study. Heatmap of the all scoring results.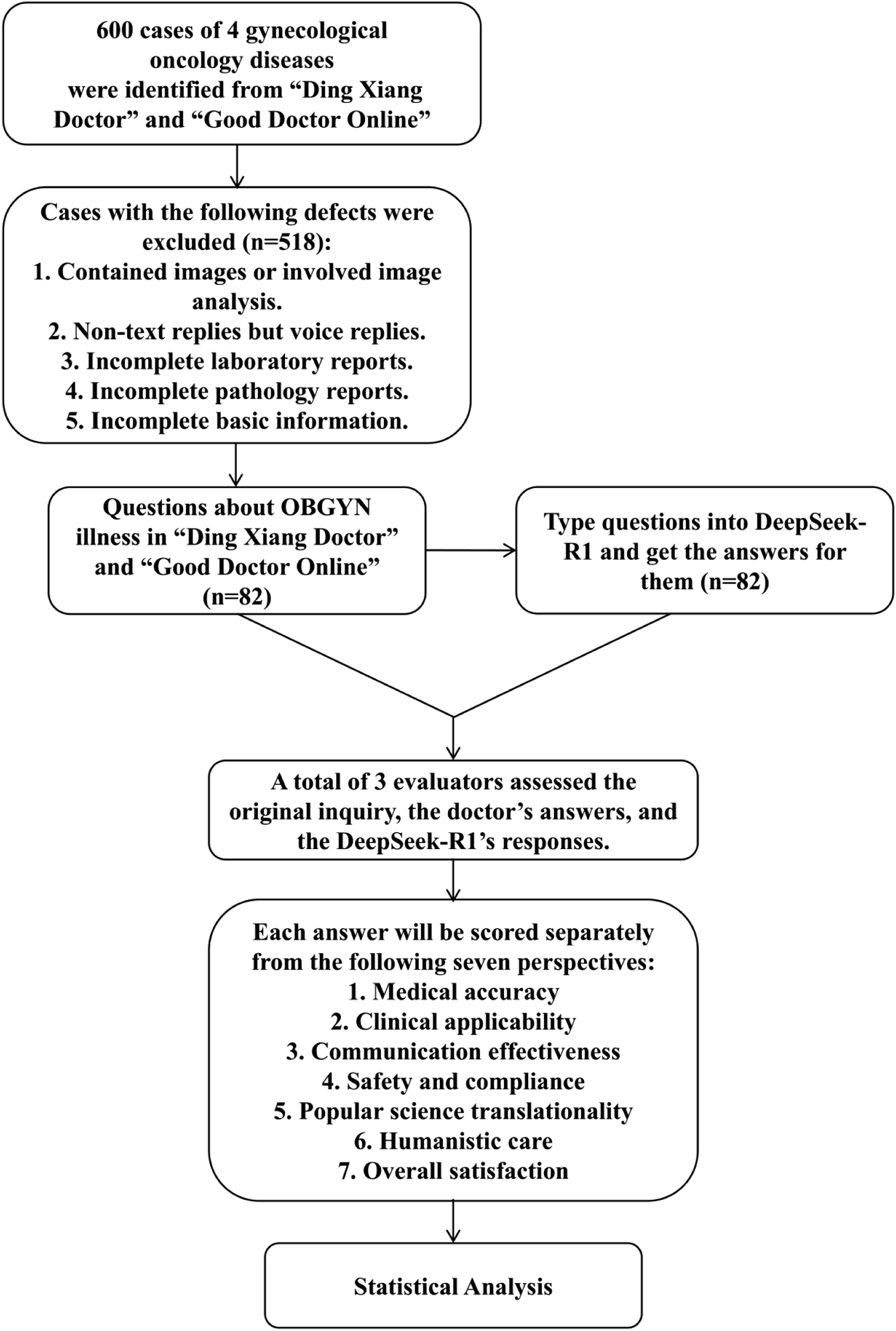
It is found that DeepSeek’s responses scores were higher than that of human doctors across all seven perspectives. For MA, DeepSeek’s mean score is 8.276 with a standard deviation of 0.3695, while human doctors’ mean score is 7.654 with a standard deviation of 0.5252. And the difference is statistically significant (p < 0.0001). For CA, DeepSeek’s mean score is 8.439 (SD = 0.3845), compared to 7.650 (SD = 0.4623) for human doctors, with p < 0.0001. For CE, DeepSeek’s mean score is 8.406 (SD = 0.3745), whereas human doctors score 7.159 (SD = 0.7848), p < 0.0001. For SAC, DeepSeek’s mean score is 8.407 (SD = 0.3553), versus 7.317 (SD = 0.6016) for human doctors, p < 0.0001. For PST, DeepSeek scores a mean of 8.114 (SD = 0.3997), while human doctors score 6.695 (SD = 0.8610), p < 0.0001. For HC, DeepSeek’s mean score is 8.447 (SD = 0.3680), compared to 6.748 (SD = 0.7743) for human doctors, p < 0.0001. For OS, DeepSeek achieves a mean score of 8.348 (SD = 0.2884), while human doctors score 7.204 (SD = 0.6023), p < 0.0001.
These results indicate that among the seven metrics, the lowest scores for both human doctors and DeepSeek occur in the PST perspective. Human doctors perform best in the MA perspective, whereas DeepSeek attains its highest score in the HC perspective. Figure 4 presents the score values for MA, CA, CE, SAC, HC, PST and OS. Figure 4 also includes a radar chart summarizing the scores of human doctors and DeepSeek across all seven perspectives comprehensively. Table S1 and Table S2 show the results of the Wilcoxon matched-pairs signed rank test and ICC respectively. The results of the Wilcoxon matched-pairs signed rank test and ICC demonstrate the reliability of the study conclusions. (A) Medical Accuracy scores of the 2 groups. (B) Clinical Applicability scores of the 2 groups. (C) Communication Effectiveness scores of the 2 groups. (D) Safety and Compliance scores of the 2 groups. (E) Popular Science Translatability scores of the 2 groups. (F) Humanistic Care scores of the 2 groups. (G) Overall Satisfaction scores of the 2 groups. (H) The radar chart of the scores of the 7 perspectives of the 2 groups.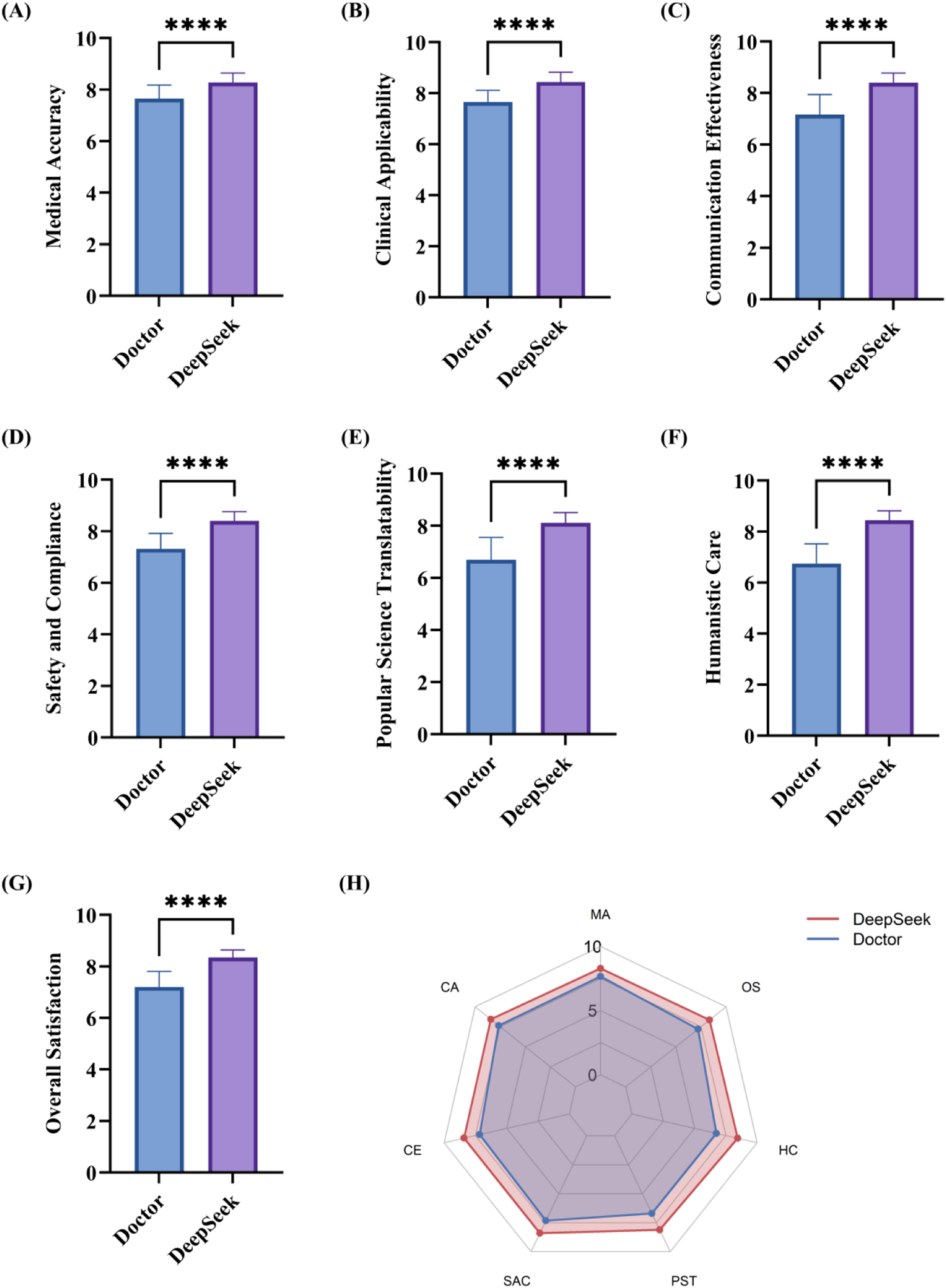
Discussion
Our study demonstrates that DeepSeek-R1 performs excellently in online remote consultations for obstetric and gynecological oncology diseases, surpassing human doctors across all evaluated metrics. We consider that DeepSeek’s high scores are closely related to its response style. Its answers are characterized by templated, modular, and formulaic structures, which produce standardized and highly logical responses. This standardization facilitates evaluators in tracing the logical flow of the answers, thereby enabling more accurate scoring. Furthermore, DeepSeek’s responses tend to be highly detailed and require longer generation times, covering a broad and comprehensive range of content. Such thoroughness significantly reduces potential omissions and flaws, making higher scores more attainable. However, excessively lengthy responses substantially increase the cognitive burden on patients and their families during online consultations and may also result in important information being overlooked. Therefore, further development by relevant practitioners is warranted to produce generated texts that are more targeted and appropriately concise.
Besides, it is observed that, regardless of whether responses originate from human doctors or DeepSeek-R1, the scores for the PST perspective were the lowest among the seven evaluated dimensions. This indicates a notable deficiency in both DeepSeek and human doctors in translating specialized medical knowledge into language that is readily understood by the general public.This issue has also been highlighted in existing research. For instance, studies addressing AI-assisted cardiopulmonary resuscitation (CPR) education have noted that DeepSeek’s responses contain numerous technical terms. 26 Several factors contribute to this phenomenon. For human doctors, daily clinical rounds, medical record documentation, and professional communications foster a habit of using dense professional terminology and concise logical structures. This habit may lead to an implicit assumption that remote consultation recipients possess a certain level of medical knowledge. Moreover, compared with online consultations, face-to-face interactions enable doctors to provide more detailed and vivid explanations through facial expressions, body language, and visual aids, which are constrained in virtual settings. Regarding DeepSeek, although its responses are logically coherent and detailed, they tend to be templated and formal. This templated style employs extensive academic expressions, which may cause comprehension difficulties for patients during online remote consultations. To address this issue, it is recommended that healthcare providers consciously explain essential terms or concepts before delivering responses in future online consultations. For DeepSeek, further development by relevant practitioners is anticipated, or alternatively the design of more precise prompts could enhance the translation of professional content into language understandable by the general public.
Additionally, human doctors scored highest in the MA compared to the other six perspectives, indicating that human doctors possessed a solid foundation of medical knowledge and extensive clinical experience, and can promptly incorporate the latest clinical guidelines into clinical practice. As a result, MA stands out relative to other indicators.
Moreover, among the seven evaluated metrics, DeepSeek was observed to achieve the highest score in HC. This outcome is evidently related to the explicit inclusion of “humanistic care” content in its responses. In contrast, human doctors’ provision of humanistic care is often implicitly integrated within their replies, making it less overt and more difficult to capture. In some cases, it may even be overly simplified, resulting in relatively lower scores. However, it should be noted that although DeepSeek’s explicit presentation of humanistic care contributes to its favorable scoring, the effectiveness and meaningfulness of such formalized expression remain questionable. Much of the humanistic care content generated by DeepSeek consists of generic statements lacking personalization tailored to the specific circumstances of the patients. Furthermore, the segregation of this content into a separate paragraph places excessive emphasis on politeness and formality, weakening its connection to the preceding medical information. This generates a sense of detachment and perfunctoriness, casting doubt on whether it truly provides the comfort and reassurance expected from authentic humanistic care for patients and their families. For future research, it is recommended that patients and their families participating in remote online consultations should be involved in the evaluation of the “humanistic care” metric to better assess its emotional soothing effect. Additionally, these findings highlight the need for human doctors to place greater emphasis on delivering emotional value, thereby providing more comprehensive physiological and psychological support.
Undoubtedly, this study has several limitations. First, all evaluating experts are drawn from a single institution, which may introduce bias into the assessment results. Therefore, multicenter studies will be pursued in future research. Second, the study is confined to four gynecological oncology diseases, leaving many prevalent conditions unexamined. Whether evaluation results differ among diseases within the same specialty warrants further investigation. Additionally, diseases from other medical specialties are not included. Given the considerable differences in severity, treatment complexity, and clinical approaches across disciplines, future studies should incorporate multiple specialties to provide a more comprehensive understanding. Furthermore, this study only included text-based teleconsultation cases and excluded those involving clinical imaging analysis, which is critical for gynecological oncology diagnosis and management. Therefore, exploring the multimodal analysis capability of the model that integrates imaging and text represents an important direction for future research.
Conclusions
In conclusion, this study systematically evaluated the performance of the DeepSeek-R1 in remote consultations for gynecological oncology diseases across seven dimensions: medical accuracy, clinical applicability, communication effectiveness, safety and compliance, humanistic care, popular science translatability, and overall satisfaction. The results demonstrate that DeepSeek-R1 outperforms human doctors on all assessed metrics. However, despite its comprehensive content, rigorous logic, and clear structure, the length of its responses may increase patients’ cognitive burden, and both the form and substance of its humanistic care require further refinement. Human doctors excelled in providing personalized consultations but are limited by workload constraints and still need to enhance their expression of humanistic care. This study highlights the promising potential of advanced large language models, exemplified by DeepSeek-R1, in remote gynecological oncology healthcare, particularly in medically underserved regions. Future research should pursue multi-center, multi-disciplinary comprehensive evaluations to further optimize the model’s response specificity, conciseness, clarity, and patient-centered humanistic care expression, thereby improving the quality of remote medical services and patient outcomes.
Supplemental material
Supplemental material - Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors
Supplemental material for Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors by Haojie Cai, Yaqian Zhao, Yongsong Wu, Yilin Liu1, Shanshan Cheng, Yu Wang in DIGITAL HEALTH
Supplemental material
Supplemental material - Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors
Supplemental material for Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors by Haojie Cai, Yaqian Zhao, Yongsong Wu, Yilin Liu1, Shanshan Cheng, Yu Wang in DIGITAL HEALTH
Supplemental material
Supplemental material - Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors
Supplemental material for Evaluating DeepSeek-R1 for gynecological oncology disease consultation in telemedicine: A comparative study with human doctors by Haojie Cai, Yaqian Zhao, Yongsong Wu, Yilin Liu1, Shanshan Cheng, Yu Wang in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Good Doctor Online, DingXiangYuan and the Ding Xiang Doctor website’s public display of gynecological oncology remote consultation cases. During the preparation of this manuscript, the authors used DeepSeek-R1 for the purposes of polishing the language. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Ethical considerations
This study was approved by the Ethics Committee of Shanghai First Maternity and Infant Hospital (KS22335).
Author contributions
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (2024YFA0917700), the Shanghai Municipal Commission of Science and Technology (25TS1412200), the National Natural Science Foundation of China (Grant No. 82272888), Shanghai Hospital Development Center Foundation (Grant No. SHDC12022106, 2022SKLY-12), Tongji University (2026-0555-YB-05), Shanghai First Maternity and Infant Hospital (Grant No. 2023B01、2023A01、2024A05、2024B20) and Health Commission of Shanghai Pudong District (Grant No. PWZxq2022-03、PW2023D-14).
Declaration of Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.