
Abstract
Background
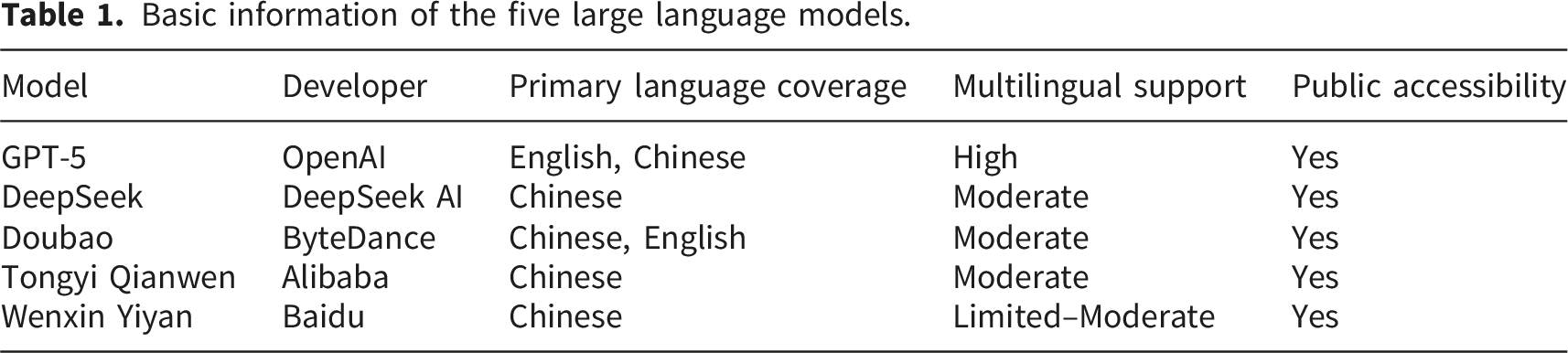
Pulmonary tuberculosis (TB) is a chronic infectious disease that burdens patients and public health systems. Limited reach of traditional education and uneven online information may undermine patients’ understanding, adherence, and trust. Large language models (LLMs) show promise for TB health education, but systematic evaluation is lacking.
Objective
To evaluate five large language models in pulmonary tuberculosis Q&A (Question and Answer) scenarios and examine the effects of different large language models and TB health education themes on response quality, readability, and reliability, thereby supporting standardized artificial intelligence (AI)–assisted health education.
Methods
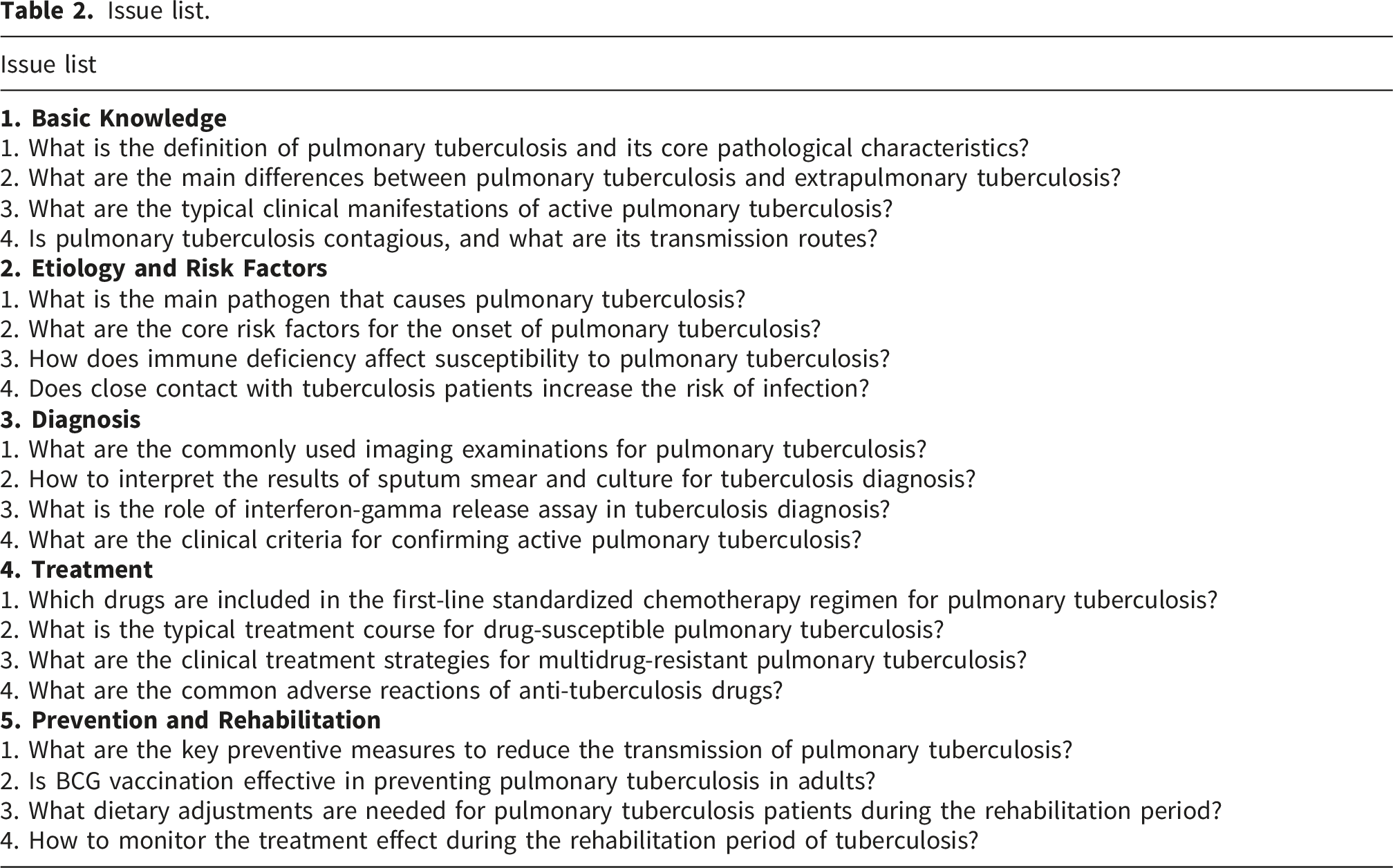
This cross-sectional study was conducted from October 5 to October 11, 2025. Twenty pulmonary tuberculosis–related questions were developed with the assistance of a respiratory physician and categorized into five themes. The questions were entered into five large language models (Doubao, DeepSeek, Wenxin Yiyan, Tongyi Qianwen, and ChatGPT) to generate 100 text responses. Quality was evaluated using patient-education suitability (C-PEMAT-P) and Global Quality Score (GQS), and readability using seven indices, including Automated Readability Index (ARI) and Flesch Reading Ease Score (FRES). Statistical analyses included One-way analysis of variance (One-way ANOVA), Kruskal–Wallis, and correlation analysis.
Results
GPT-5 achieved the highest C-PEMAT-P scores, followed by Doubao, while GQS scores were similar across models. Models showed significant differences on several readability indices, whereas themes had limited effects. Quality indicators were modestly associated with readability, while readability indices were strongly intercorrelated.
Conclusions
Model type is a key determinant of TB health education text quality. Quality and reading difficulty are related but relatively independent and should be jointly considered when selecting large language model (LLM)-generated materials. Further studies should include more models, diseases, and patient-reported outcomes to optimize AI-assisted health education.
Introduction
Pulmonary tuberculosis, also called “lao bing” in Chinese, is a chronic disease caused by infection with Mycobacterium tuberculosis.1,2 It can be traced back to about six thousand years ago in Italy and Egypt.3,4 Tuberculosis has high infectivity. 5 It is one of the top ten causes of death worldwide and the leading cause of death from a single infectious agent. 6 According to global epidemiological surveys, in 2024, the incidence of pulmonary tuberculosis was 134 per 100,000 population, and among newly diagnosed patients, 54% were male, 35% were female, and 11% were children. 7 Since treatment is a prolonged process, patients experience not only the physical burden of the disease but also considerable psychological stress, which brings continuous challenges to the health care system and to public mental health.8,9
In the treatment of pulmonary tuberculosis, pharmacotherapy is the primary treatment, and it must be combined with long-term management and follow-up.10,11 Previous studies have shown that patients’ level of knowledge about pulmonary tuberculosis has a marked impact on their adherence to treatment and on clinical outcomes.12,13 Therefore, it is particularly important to provide health education that is accurate, reliable, and easy to understand.14,15 Traditional health education methods are limited in terms of both the scope of content delivered and the size of the population reached. 16 With the development and widespread use of the internet, especially online question-and-answer platforms and various social media, people can obtain health information through multiple channels. However, the uneven quality, partial coverage, and insufficient accuracy of online information may weaken patients’ trust in making medical decisions and negatively affect their psychological state.17,18
In recent years, AI has developed rapidly and has shown obvious advantages in many fields.19–22 As one type of AI, Large language models have strong semantic understanding, broad knowledge coverage, and the ability to integrate information, which brings new opportunities for health education.23,24 Traditional health education mainly relies on professionals, such as physicians, nurses, and pharmacists. 25 In contrast, large language models are built on deep learning and trained on large amounts of text, so they can quickly generate answers that are logically clear and well-structured in natural language interactions.26,27 Representative systems in China and abroad, such as DeepSeek and ChatGPT, have already shown potential for clinical support applications in supporting medical diagnosis, patient consultation, and medication education.28–30 At the same time, other models with similar functions have emerged globally, and their scope and depth of application are continuously expanding. 31 However, the language style, readability, comprehensibility, and accuracy of citations differ across models; all of these differences may affect users’ understanding of and trust in the popular science content. At present, there is still a lack of systematic evaluation studies on the performance of large language models in science popularization related to pulmonary tuberculosis.
Basic information of the five large language models.
Materials and methods
Ethical considerations
All data used in this study were generated by artificial intelligence large language models. No human or animal experiments were involved, and no real personal information or biological samples from humans were included. According to relevant academic and ethical guidelines, this type of study does not require ethics committee review.
Research procedure
Issue list.
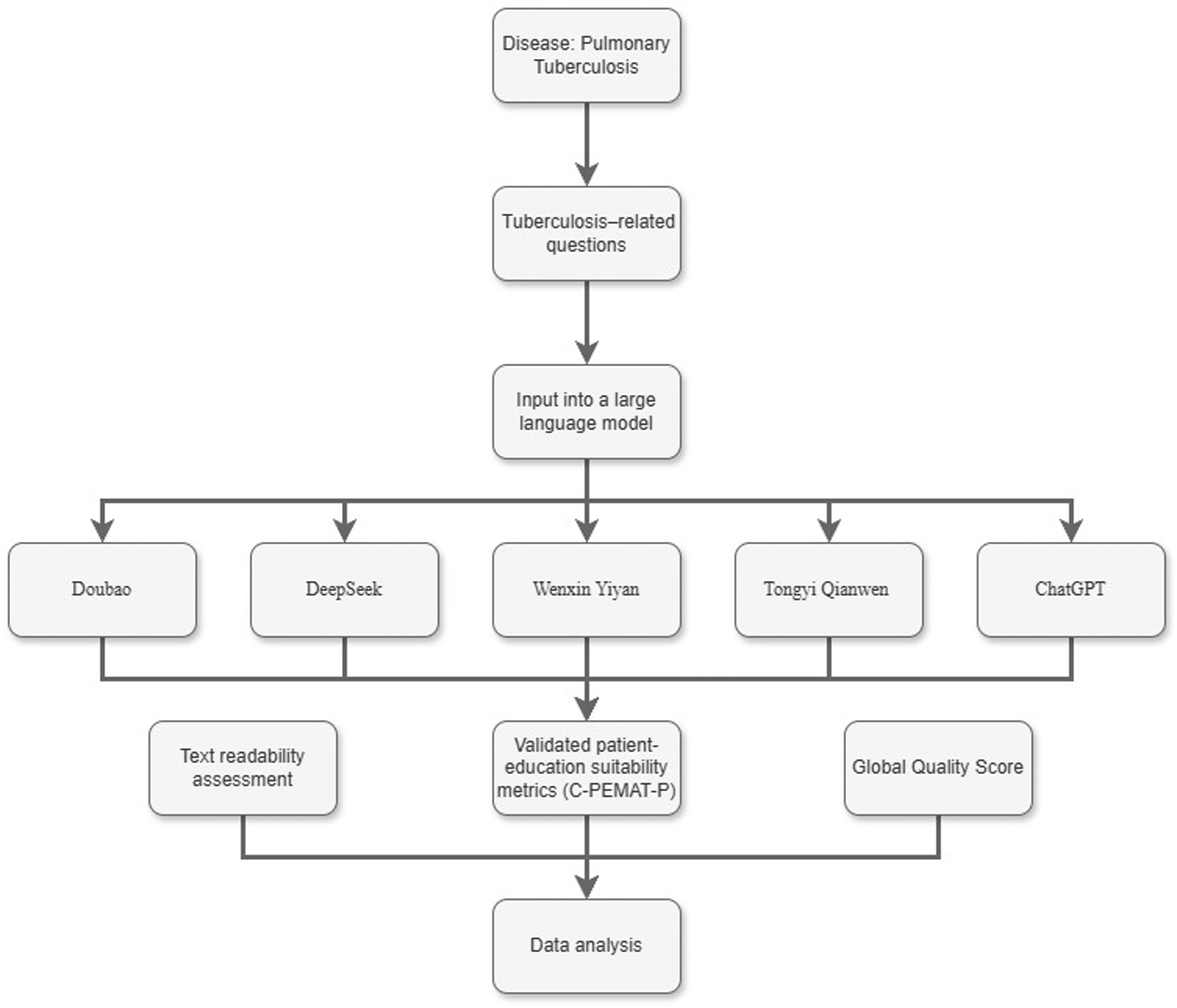
Flowchart of the study.
Readability evaluation
We used several formulas provided by an online text readability assessment tool (https://readabilityformulas.com/) to analyze the answers generated by the large language models. Currently, as there is no internationally accepted standard indicating which readability index is the most accurate and reliable, this study adopts mainstream indicators that are widely used in prior research.
Indicators of an online text readability assessment tool.
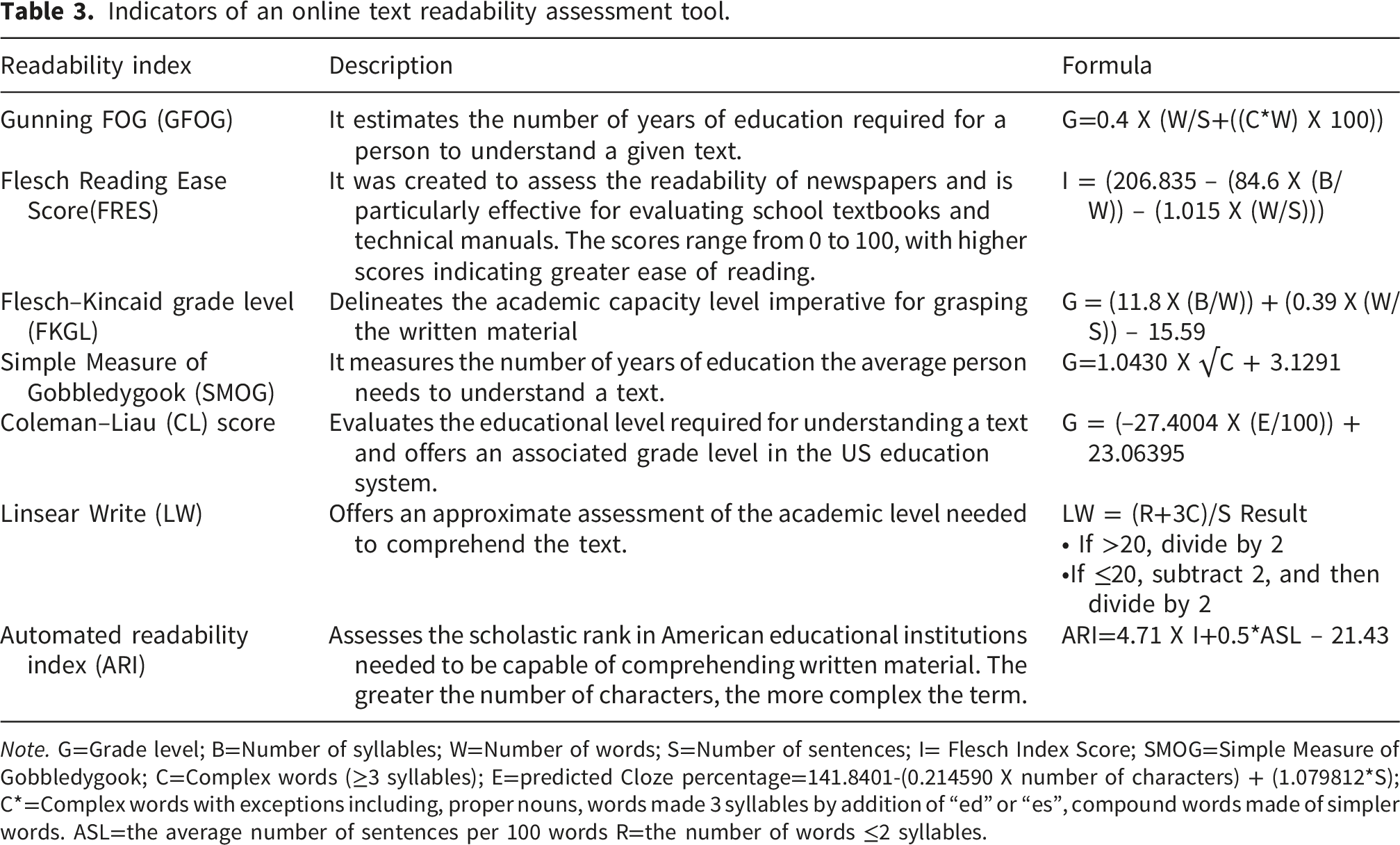
Note. G=Grade level; B=Number of syllables; W=Number of words; S=Number of sentences; I= Flesch Index Score; SMOG=Simple Measure of Gobbledygook; C=Complex words (≥3 syllables); E=predicted Cloze percentage=141.8401-(0.214590 X number of characters) + (1.079812*S); C*=Complex words with exceptions including, proper nouns, words made 3 syllables by addition of “ed” or “es”, compound words made of simpler words. ASL=the average number of sentences per 100 words R=the number of words ≤2 syllables.
Quality assessment
This study used the Patient-education suitability (C-PEMAT-P) scale and the Global Quality Score (GQS) to assess the reliability of the model-generated answers. The C-PEMAT-P includes 24 items, divided into two dimensions: “understandability” (16 items, including the logical organization of information and the extent to which technical terms are explained in plain language) and “actionability” (8 items, including the clarity of action guidance and the appropriateness for the target population). Each item is scored 0 or 1 (0 = does not meet the criterion at all, 1 = fully meets the criterion), giving a total score from 0 to 24; higher scores indicate better accessibility of the material for users. 35
The GQS is a 5-point global rating scale. A score of 1 indicates “poor quality, with disorganized content, missing key information, and no practical value for users”; 2 indicates “overall poor quality, with weak logical structure, incomplete core information, and limited practical value”; 3 indicates “moderate quality, with some important information adequately discussed and basic practical value”; 4 indicates “good quality, with clear logical structure, coverage of most relevant information, and relatively high practical value”; and 5 indicates “excellent quality, with rigorous logic, smooth flow, and high practical value for users”. 36
On 20 October 2025, two pharmacists, each with more than three years of relevant professional experience, used these two scales to evaluate the answers separately. When discrepancies in scoring occurred, a third expert was consulted to determine the final rating, and reviewers reached consensus through detailed discussion. Inter-rater agreement was quantified using Cohen’s kappa coefficient. 37 According to commonly used criteria, κ > 0.75 indicates excellent agreement, 0.40 ≤ κ ≤ 0.75 indicates acceptable agreement, and κ < 0.40 indicates poor agreement. All disagreements were resolved through consensus to ensure the rigor and reliability of the assessment. In this study, Cohen’s kappa coefficients for both the C-PEMAT-P and GQS ratings were greater than 0.75, indicating excellent inter-rater agreement.
Statistical analysis
This study selected appropriate statistical methods according to the distribution characteristics of the data. For measurement variables with a normal distribution (such as the C-PEMAT-P score and GQS score, presented as mean ± standard deviation [Mean ± SD]), one-way analysis of variance (ANOVA) was used for comparisons among multiple groups. 38 For variables with a non-normal distribution (such as ARI and FRES, presented as median and interquartile range [M, Q1, Q3]), the Kruskal–Wallis H test was applied to assess differences among groups. A two-sided P value < 0.05 was considered statistically significant. All data analyses were conducted using Python 3.14, and data visualizations were generated with GraphPad Prism 9.0.
Results
Readability analysis
The study uses multiple evaluation frameworks, including the Global Quality Scale (GQS), Patient-education suitability (C-PEMAT-P), and several readability indices, to systematically examine how large language models influence the quality and readability of generated texts. 33 For model type, we compared five models (DeepSeek, Doubao, GPT-5, Tongyi Qianwen, and Wenxin Yiyan) in terms of patient education suitability (C-PEMAT-P), overall quality (GQS), and readability measures (ARI, FRES, GFOG, FKGL, CL, SMOG, and LW). In terms of content, we evaluate the same indicators across five categories of health education topics (basic knowledge, etiology and risk factors, diagnosis, treatment, and prevention and rehabilitation). Based on the analysis above, the study explored the patterns of influence exerted by model type and content category on text quality and readability metrics.
Analysis results of five large models.
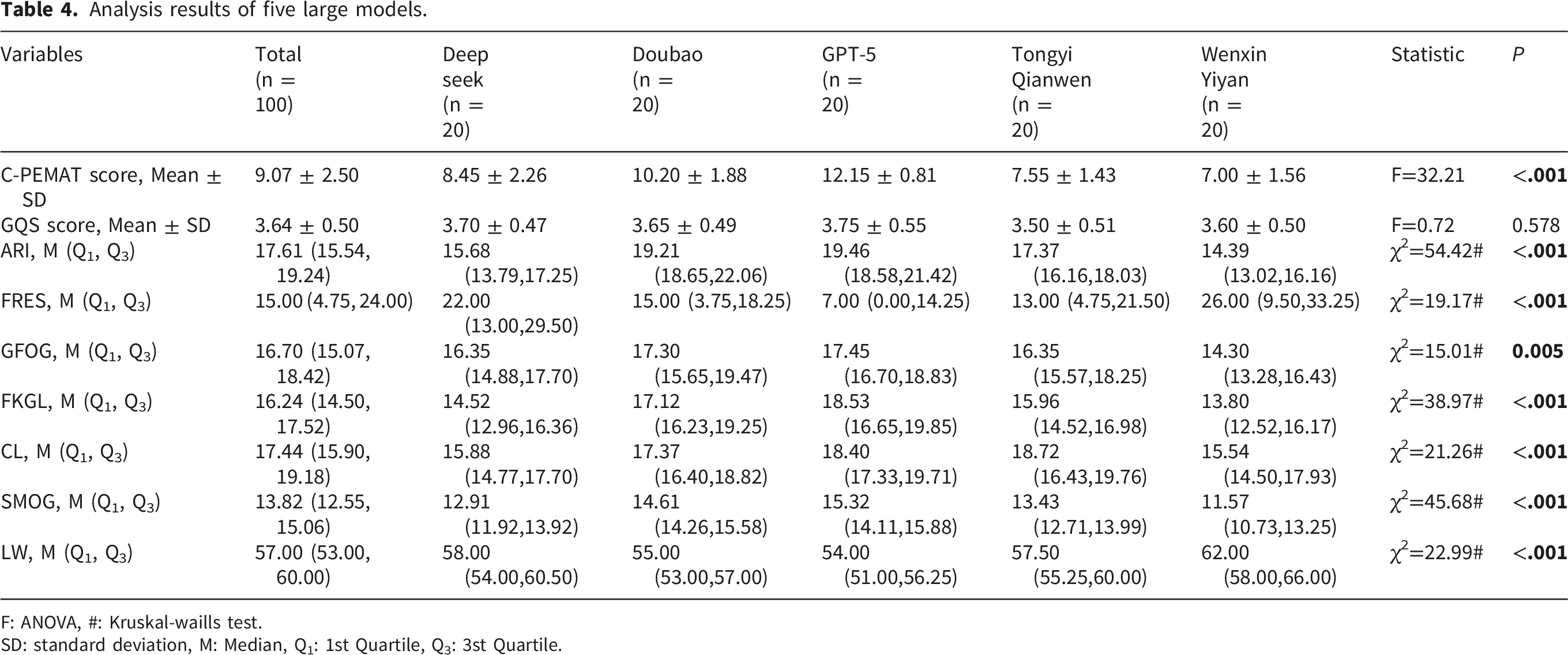
F: ANOVA, #: Kruskal-waills test.
SD: standard deviation, M: Median, Q1: 1st Quartile, Q3: 3st Quartile.
In contrast, no significant differences were observed in GQS scores among the five models (F=0.72, P=0.578), with median values clustering between 3.50 and 3.75. It means that the overall perceived quality of the texts was similar across models. Readability analysis showed significant differences among models across several indices, including ARI, FRES, GFOG, FKGL, CL, SMOG, and LW (all P < 0.05). GPT-5 and Doubao had higher scores on several linguistic complexity measures (such as ARI, FKGL, SMOG), indicating relatively higher linguistic complexity, with richer information content and more flexible expression. But, Wenxin Yiyan had the highest LW score (median 62.00), suggesting that the texts it generated contained longer average word length, which may reduce clarity and ease of reading and thus affect patients’ reading experience.
Analysis results by content category.
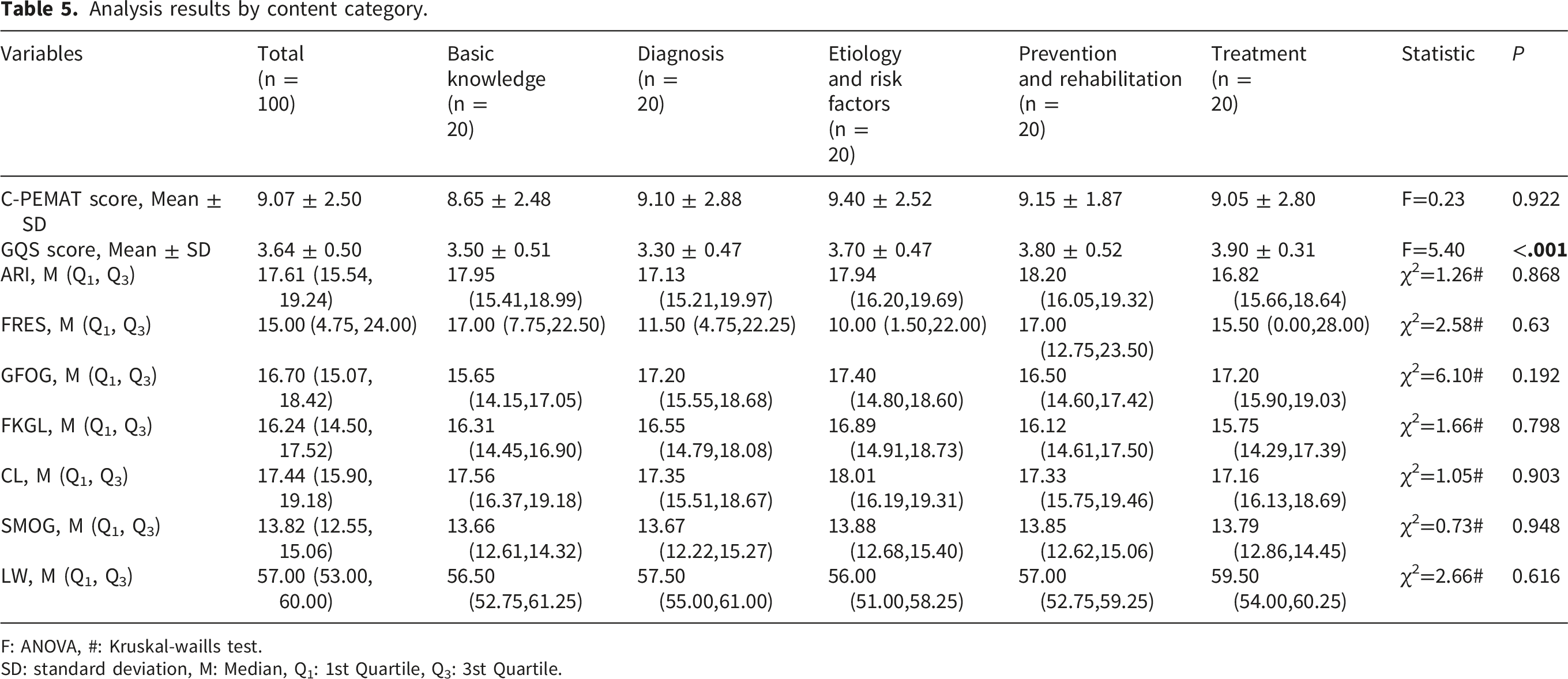
F: ANOVA, #: Kruskal-waills test.
SD: standard deviation, M: Median, Q1: 1st Quartile, Q3: 3st Quartile.
Similarly, readability indices such as ARI, FRES, GFOG, FKGL, CL, SMOG, and LW did not show significant variation across content categories (all P>0.05), showing that topic selection had a relatively limited impact on text readability. So, these findings indicate that although the texts generated by different models exhibit marked differences in linguistic features, the reading difficulty remains relatively consistent across different health education topics for all models.
Quality analysis
For the GQS score (Figure 2), no significant differences were observed among Doubao, DeepSeek, Wenxin Yiyan, Tongyi Qianwen, and GPT-5 (ns). The median scores of all platforms lay within a similar range, and the violin plots showed comparable distributional patterns. Examination of the boxplots and density contours indicated that the data for each model were relatively tightly clustered. All of these suggest that the overall performance of the five models is broadly similar, with relatively stable and consistent outputs across platforms in terms of GQS-assessed text quality. GQS score distributions across five large language models. Violin plots display the distribution of Global Quality Scale (GQS) scores for responses generated by Doubao, DeepSeek, Wenxin Yiyan, Tongyi Qianwen, and GPT-5 in pulmonary tuberculosis question-and-answer scenarios. GPT-5 shows relatively concentrated higher scores, suggesting stronger overall response quality, whereas the other models exhibit moderate variability. Statistical significance was evaluated using one-way ANOVA followed by post hoc testing (ns, not significant; p < 0.05; p < 0.01; p < 0.001; p < 0.0001).
At the C-PEMAT-P score dimension (Figure 3), GPT-5 showed excellent performance, with median scores exceeding 12 points. Statistical testing indicated highly significant differences (****) between GPT-5 and each of Doubao, DeepSeek, Wenxin Yiyan, and Tongyi Qianwen. The distribution pattern for GPT-5 was tightly clustered in the high-score region, suggesting stable and consistently strong performance on this evaluation dimension. and there was a significant difference (*) between Doubao and DeepSeek, Doubao has a median score of approximately 10 points, while Deep Seek’s median is slightly poor, with both showing a wide distribution. In contrast, there is no significant difference between Wenxin Yiyan and Tongyi Qianwen. And their violin plots were relatively concentrated with lower medians. This pattern suggests that these two platforms may be less adequate in terms of patient education suitability, for example, in the clarity of information delivery and the practicality of behavioural or operational guidance. C-PEMAT score distributions across five large language models. Violin plots illustrate the distribution of C-PEMAT scores across all five models. GPT-5 demonstrates the highest and most concentrated scores, indicating superior educational suitability and understandability. Doubao and DeepSeek represent intermediate performance with moderate variability, whereas Wenxin Yiyan and Tongyi Qianwen generally show lower scores. Statistical significance was evaluated using one-way ANOVA followed by post hoc testing (ns, not significant; p < 0.05; p < 0.01; p < 0.001; p < 0.0001).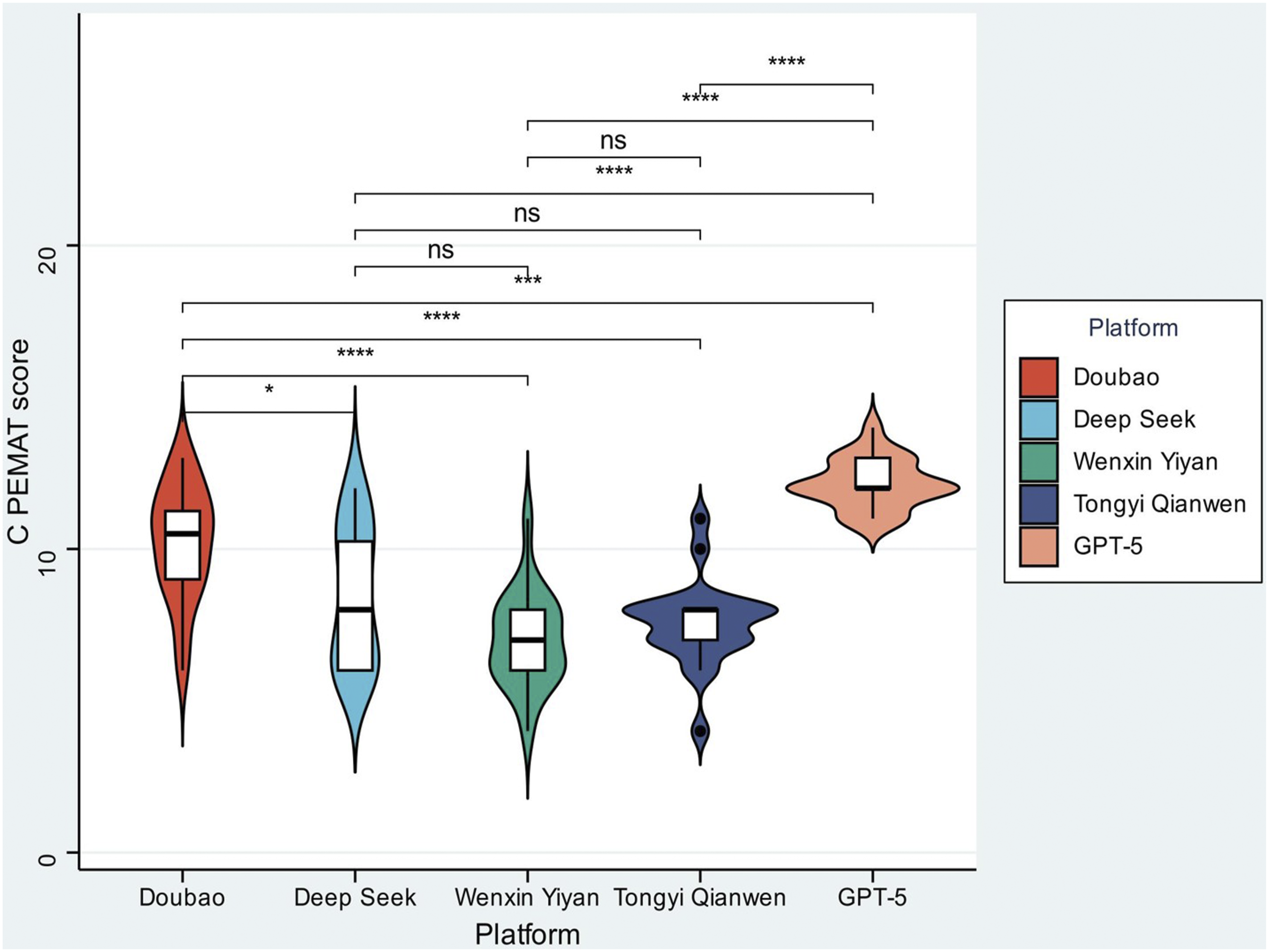
Correlation analysis
The correlation distribution in the heatmap (Figure 4) shows that we can clearly observe the relationships between GQS, C-PEMAT-P, and the different readability metrics, as well as the associations within each group of metrics. Overall, the direct linear associations between GQS or C-PEMAT-P and the readability metrics remain weak, with most correlation coefficients falling within |r| < 0.4, indicating only weak to moderate correlations. However, several patterns are still noteworthy. GQS is mildly positively correlated with ARI, FRES, CL, and LW (correlation coefficients roughly between 0.2 and 0.4), suggesting that texts are slightly more difficult to read or of moderate length tend to receive somewhat higher overall quality scores. In contrast, the correlations between GQS and FKGL, GFOG, and SMOG are close to zero or slightly negative, indicating that the complexity of vocabulary and sentence structure has only a limited direct effect on overall quality. High-quality texts are therefore not simply those that are “harder to read” or “easier to read,” but rather those whose strengths depend more on the content itself. Correlation matrix of readability and quality metrics. Heatmap visualizing Pearson correlations between readability indices (ARI, FRES, GFOG, FKGL, CL, SMOG, and LW) and quality measures (C-PEMAT score and GQS score). Readability metrics cluster closely, reflecting shared assessment of linguistic complexity. In contrast, C-PEMAT and GQS show relatively weak correlations with most readability indices, suggesting that readability and content quality capture partially independent dimensions of generated responses. Because the correlation matrix is symmetric, each pairwise correlation appears twice in the matrix (upper and lower trianglesa), and therefore both halves of the matrix are shown in the heatmap.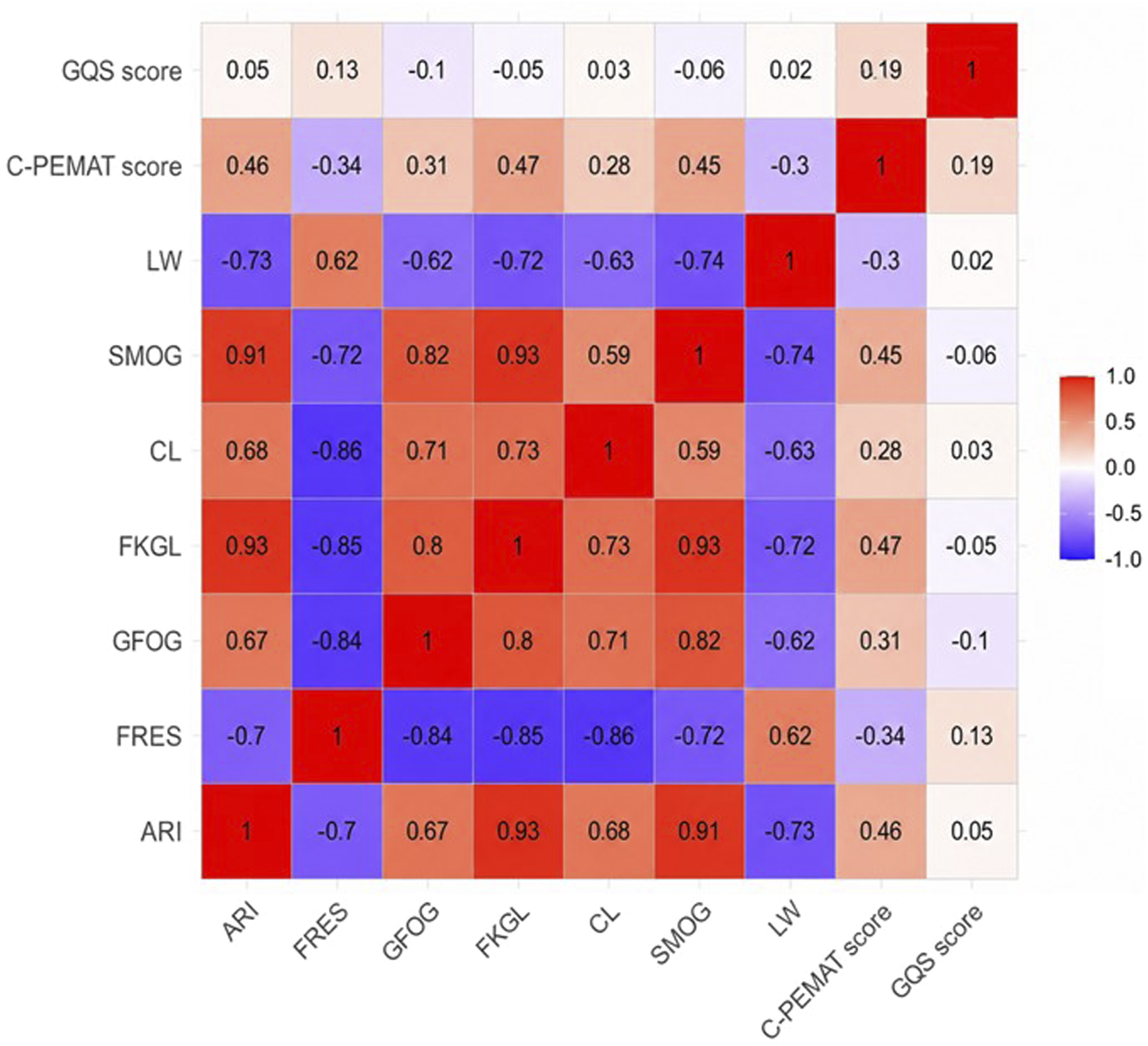
For the C-PEMAT-P scores, correlations with readability metrics were also generally weak overall. It showed moderate positive correlations with traditional readability indices, such as ARI (r = 0.46), FKGL (r = 0.47), and SMOG (r = 0.45), and moderate negative correlations with FRES (r = -0.34) and LW (r = -0.30). These patterns suggest that a moderate level of professional expression and a certain degree of structural complexity may improve the suitability of materials for patient education from a professional perspective. However, when texts become too long or when their “ease-of-reading” scores are too high (the content is overly simple and the information density is low), their practical value for patient education may be reduced. This is consistent with clinical practice, which stresses that texts should not be oversimplified as long as accuracy is maintained.
In contrast, there were strong correlations within the readability metrics themselves. The correlation coefficients between ARI and FKGL reached 0.93, while that between ARI and SMOG was 0.91. The coefficients between FRES and GFOG, FKGL, and CL were -0.84, -0.85, and -0.86, respectively. In addition, GFOG showed strong positive correlations with FKGL (0.80) and SMOG (0.82). These patterns indicate that the readability metrics are highly consistent in measuring “textual reading difficulty” and can be used as complementary tools to cross-check one another. However, their direct influence on quality metrics such as GQS and C-PEMAT-P is relatively limited, further showing that “textual quality” and “readability” are relatively independent dimensions. These findings provide a multi-dimensional perspective for evaluating text.
Discussion
With the model type and medical popular science content as the main variables, GQS, C-PEMAT-P, and a panel of readability indices were employed to systematically evaluate the quality and readability of texts generated by large language models. This study shows that model type has a marked impact on structural integrity and informational accuracy, whereas topic category mainly drives differences in readability. More importantly, the “quality dimension” and the “reading difficulty dimension” emerged as relatively independent axes of evaluation. These findings provide important theoretical support and practical guidance for the precise application of large language models in the field of health education.
Determinant role of model type in text quality and mechanisms analysis
At the level of large language models, GPT-5 shows outstanding performance in terms of patient education suitability of patient education texts, followed by Doubao, whereas Tongyi Qianwen and Wenxin Yiyan perform comparatively less well. For the core quality indicator C-PEMAT-P, GPT-5 reaches a mean score of 12.15 ± 0.81, significantly higher than Doubao (10.20 ± 1.88), DeepSeek (8.45 ± 2.26), Tongyi Qianwen (7.55 ± 1.43), and Wenxin Yiyan (7.00 ± 1.56) (F=32.21, P<0.001). Doubao also scored significantly higher than DeepSeek, Tongyi Qianwen, and Wenxin Yiyan.
These differences may be closely related to how each model has been adapted to patient education scenarios during training. GPT-5 may have been exposed to a large volume of patient education materials, with targeted optimisation for information clarity and the actionability of instructions. Doubao may have benefited from long-term training on health education, gradually forming an expression style that aligns more closely with patients’ cognitive patterns.
In terms of distributional characteristics, the violin plot for GPT-5’s C-PEMAT-P scores exhibits a highly concentrated distribution in the high-score range, while Doubao shows a wider spread but a relatively high median; the interquartile ranges in the boxplots for both models are relatively narrow (Figure 2), suggesting that the patient education suitability of their generated texts is fairly stable. Conversely, Tongyi Qianwen and Wenxin Yiyan not only have markedly lower C-PEMAT-P scores (both < 8 points), but their violin plots show a slender pattern, indicating clear limitations in the translation of technical terminology into lay language. This pattern implies a higher probability of generating low-quality texts, which makes it difficult to meet the needs of patients’ health education.
In contrast, no significant differences were observed among models in terms of GQS (overall text quality) (F=0.72, P=0.578), whereas the readability indices (such as ARI, FRES, FKGL) differed significantly between models (all P<0.05). For example, the median ARI exceeded 19 in Doubao and GPT-5, but was only 14.39 in Wenxin Yiyan; the median FRES reached 26.00 in Wenxin Yiyan, while it was as low as 7.00 in GPT-5. All of these indicate that mainstream models differ in their capacity to control text complexity; such differences do not directly translate into changes in overall text quality. It further supports the view that “quality” and “readability” represent relatively independent dimensions of evaluation.
Modulating effect of content category on text readability and its clinical implications
Analysis of the content categories revealed a divergent pattern between the stability of text quality and the variability of readability in health education text; the content category did not affect patient education suitability, but it did modulate overall text quality (GQS) and several readability indices.
In the quality indicators, C-PEMAT-P scores did not differ significantly among the five topic categories, “basic knowledge,” “etiology and risk factors,” “diagnosis,” “treatment,” and “prevention and rehabilitation” (F=0.23, P=0.922). This suggests that higher performance models (such as GPT-5 and Doubao) are able to maintain stable patient education suitability across health education topics with varying levels of technical complexity. Even for more specialised content such as “treatment” and “diagnosis,” appropriate information structuring—for example, outlining treatment procedures in bullet points or explaining diagnostic reasoning through concrete cases—can support patient understanding. At the same time, “basic knowledge” content does not appear to lose essential information as a result of simplification.
These findings have important implications for clinical practice, and healthcare professionals can select topic-specific materials, like postoperative recovery or chronic disease prevention, adapting to patients’ needs, thereby substantially improving the efficiency of AI-assisted health communication. However, GQS scores differed significantly across content categories (F=5.40, P<0.001), while the readability indices (such as ARI and FRES) showed no significant differences between categories (all P>0.05). This pattern suggests that the professional attributes of the content influence the assessment of overall text quality, but have only a limited direct impact on reading difficulty. In other words, even for highly specialised topics, models can balance quality and readability by adjusting linguistic expression rather than simplifying the content itself. It further exhibits the notion that “quality” and “readability” are relatively independent dimensions.
Features and optimization paths for text quality and readability
With the help of correlation analysis, the misconception that “readability equals quality” was clarified, and the relative independence and limited overlap of these two constructs were demonstrated. The heatmap shows several key links between quality indices and readability measures: GQS is strongly positively correlated with ARI (r=0.85), FKGL (r=0.83), and SMOG (r=0.91). It should be noted that the evaluation of overall text quality partly depends on linguistic complexity, including vocabulary, sentence structure, and length. C-PEMAT-P is moderately positively correlated with ARI (r=0.46) and FKGL (r=0.47), suggesting that patient education suitability also requires an appropriate degree of linguistic complexity to support informational accuracy and professional adequacy. For instance, the standardised use of terms such as “active pulmonary tuberculosis” and “drug-resistant pulmonary tuberculosis” can help avoid distortion of meaning that may arise from excessive simplification.
The readability indices showed highly internal correlations between ARI and FKGL (r=0.93), SMOG (r=0.91), and between FRES and GFOG (r=-0.80). hese findings suggest that these indices can be used as tools to assess “reading difficulty,” providing a more precise measure of linguistic complexity.
Meanwhile, these findings point to practical directions for model optimisation and clinical application. On the modelling side, it is possible to balance linguistic complexity and patient suitability while maintaining overall quality, for instance by adding plain-language explanations for technical terms and avoiding excessively long or complex sentences. This approach can help ensure informational accuracy while improving patients’ understanding. Clinically, when choosing AI-generated health education texts, healthcare professionals can jointly consider readability and quality indicators to identify texts that are of high quality and readily readable.
Limitations
This study systematically evaluated the quality and readability of health education texts generated by artificial intelligence; however, several limitations should be acknowledged. First, the sample size was relatively limited, including five large language models and five tuberculosis-related health education topics, which may not fully capture the generation characteristics of different systems when addressing specialized diseases or more complex medical topics. Secondly, the evaluation framework relied mainly on objective indicators, a lack of some evidence on patients’ subjective experiences, such as comprehension scores and operation implementation rates, as well as professional evaluations from clinical medical staff, making it difficult to fully evaluate the real-world effectiveness of the texts. Third, there is currently a lack of widely accepted readability evaluation metrics specifically designed for Chinese medical texts, which limits the methodological options available for assessing the readability of Chinese health education materials. Fourth, the limitation of this study is that the evaluation focused primarily on readability and general information quality, while a detailed assessment of clinical accuracy and safety was not performed. Lastly, the study does not consider patient-level heterogeneity, which may influence acceptance of the texts and limit the specificity of any recommendations regarding personalised adaptation strategies.
Future directions
Further research may focus on four areas: First, expand the sample size and further diversify the source data, including incorporating a larger number of cases, drawing on clinical practice guidelines from multiple institutions, interdisciplinary medical knowledge, and common questions of patients, with particular emphasis on specialised content related to the prevention, treatment, and follow-up of pulmonary tuberculosis. Such expansion is expected to enhance the accuracy and comprehensiveness of model-generated materials.
Second, a three-dimensional evaluation framework should be established that integrates medical accuracy assessment, patient-centred readability validation, and clinical utility testing. In practice, this would involve inviting clinical specialists from relevant departments to review the professional quality of the content, collecting patients’ feedback on comprehension and ease of use, and conducting follow-up surveys to examine the impact of popular science texts on outcomes such as adherence to follow-up visits and relief of disease-related anxiety.
Third, although the responses were reviewed using established evaluation tools and assessed by pharmacists with professional medical training, the study did not include a systematic comparison with clinical guidelines or a formal analysis of potential hallucinations or factual errors generated by large language models. Given the importance of medical accuracy in tuberculosis education, future studies should incorporate guideline-based verification and hallucination rate analysis to further strengthen the clinical reliability of AI-generated health information.
Finally, it is important to develop a personalized pulmonary tuberculosis education generation system. This system could generate health education content tailored to different users and educational needs. Adapting language complexity and presentation style may improve the accessibility and effectiveness of tuberculosis health education. Leveraging large language models, such a system could dynamically consider patients’ age, educational level, clinical status, and specific informational needs (such as support for treatment decision-making, psychological counselling), and automatically adjust the frequency of technical terms, the emotional tone, and the hierarchical structure of the text. In this way, the system would deliver tailored educational materials and promote the deep integration and practical implementation of artificial intelligence in the early prevention, screening, and long-term health management of pulmonary tuberculosis. So, these results indicate that although the texts generated by different models exhibit marked differences in linguistic features, the reading difficulty remains relatively consistent across different health education topics for all models.
Conclusion
This study systematically evaluated the quality and readability of generated texts by focusing on two core variables, large language model type and health education content category, and used patient education suitability (C-PEMAT-P) and overall text quality (GQS). The main findings indicate that model type is a key determinant of text quality. High-performing models can stably produce high-quality texts across different topics and show superior performance in both patient education suitability and overall quality.
By contrast, content category mainly affects readability. More specialised topics (such as aetiological mechanisms and treatment regimens) tend to increase reading difficulty but do not significantly compromise text quality, as high-performance models can adjust their wording to balance professional depth and readability. Further analyses indicate that text quality and readability are relatively independent dimensions: appropriate length and standardised use of technical terms help maintain quality, whereas excessive accumulation of jargon can reduce patient comprehension, offering an important reference point for text optimisation.
In light of these findings, health communication practice should prioritise the use of high-performance models to ensure accuracy and suitability at the source. At the same time, it is necessary to tailor texts to topic complexity and the target audience’s health literacy level by simplifying sentence structure, providing explanations for technical terms, and otherwise improving readability to enhance communicative precision. In the Future, studies should broaden the range of models and topics examined, incorporate patients’ subjective experiences and clinical outcome data, and thereby strengthen the evidence base for the regulated and evidence-informed use of large language models in health education.
Supplemental material
Supplemental material - Performance evaluation of five major large language models in tuberculosis Q&A systems: A multidimensional assessment of readability, quality, and reliability
Supplemental material for Performance evaluation of five major large language models in tuberculosis Q&A systems: A multidimensional assessment of readability, quality, and reliability by Rong Liu, Ying Chen, Wenzhuo Zhao, Yihuan Cai in DIGITAL HEALTH
Supplemental material
Supplemental material - Performance evaluation of five major large language models in tuberculosis Q&A systems: A multidimensional assessment of readability, quality, and reliability
Supplemental material for Performance evaluation of five major large language models in tuberculosis Q&A systems: A multidimensional assessment of readability, quality, and reliability by Rong Liu, Ying Chen, Wenzhuo Zhao, Yihuan Cai in DIGITAL HEALTH
Footnotes
Acknowledgements
The manuscript was edited and polished for language using Grammarly. We appreciate the help of all evaluators and contributors for their efforts in data collection and validation. The author takes full responsibility for any errors or oversights.
Author contributions
Rong Liu retrieved the relevant literature and drafted the manuscript. Yihuan Cai originated the work, led the discussions, provided helpful comments, and revised the manuscript. and Ying Chen assisted in designing a structured set of 20 representative questions to capture the practical information needs related to pulmonary tuberculosis, helpful responsible for data collection and curation. Wenzhuo Zhao contributed to data analysis, project administration, supervision, and interpretation. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.