
Abstract
Background
Digital inclusion has become increasingly important for healthy aging, yet evidence on its association with depression among older adults remains limited, particularly with respect to potential cognitive heterogeneity.
Objective
This study examined the association between digital inclusion and depressive symptoms among Chinese older adults and explored whether cognitive function moderates this association, as well as potential mediating pathways.
Methods
Data were drawn from the 2020 wave of the China Health and Retirement Longitudinal Study, including 9,111 individuals aged 60 years and older. A multidimensional digital inclusion index was constructed based on access, use, and skills related to digital technologies, standardized to a 0–10 scale. Depressive symptoms were assessed using the 10-item Center for Epidemiological Studies Depression Scale (CES-D-10; each item scored 0–3, total range 0–30, treated as a continuous score). Multi-variable regression models were used to examine associations, with interaction terms and Johnson–Neyman analysis applied to assess moderation by cognitive function, with effect size estimated using Cohen’s f2. Structural equation modeling was conducted to explore potential mediating mechanisms.
Results
Cognitive function significantly moderated the association between digital inclusion and depressive symptoms (β = −0.002, P < 0.05). Among participants in the highest quartile of cognitive function, each unit increase in digital inclusion was associated with a 0.517-point decrease in depression scores, whereas no statistically significant association was observed among those in the lowest quartile (β = −0.137, P = 0.327). Pathway analyses suggested that the association operated through multiple pathways, with the direct pathway accounting for 66.7% of the total association—likely reflecting immediate psychological mechanisms including enhanced self-efficacy, expanded access to health information, and a sense of digital mastery—while cognitive-related and social participation pathways explained 8.3% and 8.0%, respectively; a sequential cognitive–social pathway accounted for a further 2.8%, and the remaining 14.2% was attributable to other model-estimated pathways, with all pathways together accounting for 100% of the total association. Executive function and immediate memory emerged as the cognitive domains most strongly associated with moderation patterns.
Conclusions
These findings suggest that greater digital inclusion is associated with lower depressive symptoms among older adults and that cognitive function shapes heterogeneity in this association. Enhancing digital inclusion while accounting for cognitive differences may help inform digital health strategies aimed at promoting mental well-being in aging populations.
Keywords
Introduction
The rapid digitization of healthcare and social services has created unprecedented opportunities for promoting healthy aging, while simultaneously risking the exclusion of digitally disadvantaged older adults. Digital inclusion—defined as meaningful access to and use of digital technologies—has emerged as a critical social determinant of health in aging populations. 1 Current conceptualizations recognize digital inclusion’s multidimensionality, encompassing access, skills, motivation, and effective usage in daily health management activities. Critically, formal access to digital devices does not guarantee substantive participation: older adults may gain nominal connectivity while remaining functionally excluded due to skill deficits, motivational barriers, or cognitive limitations—a condition described as “apparent inclusion,” wherein individuals possess the material means of digital access but cannot translate access into meaningful use or psychological benefit.2,3 Among older adults, digital inclusion presents unique challenges and opportunities, with substantial heterogeneity in adoption patterns and usage behaviors that may be associated with health outcomes differently across subgroups.2,4
Research examining digital inclusion’s mental health associations among older adults has yielded mixed findings. Recent studies using Chinese data have shown that digital technologies can effectively inhibit depression among middle-aged and older adults, 5 while digital engagement shows positive associations with mental health outcomes. 6 However, other research highlights potential negative associations, including age-related digital marginalization and technology-related stress,2,7 suggesting a more complex relationship than initially conceptualized.
Despite growing interest, existing evidence remains fragmented. Prior studies have primarily focused on general associations between digital technology use and depressive symptoms, often assuming relatively uniform benefits across older populations. Yet older adults are highly heterogeneous, particularly with respect to cognitive function, which may shape their ability to access, use, and benefit from digital technologies.8,9 Older adults with diminished cognitive capacity may face heightened techno-stress—characterized by frustration, anxiety, and helplessness when confronted with complex digital systems—which may not only diminish potential mental health benefits but actively exacerbate psychological vulnerability.2,3,7 Moreover, the cognitive reserve hypothesis suggests that engaging in cognitively stimulating digital activities may contribute to reserve against age-related cognitive decline, 10 pointing to potential bidirectional associations between cognitive function and digital engagement. In addition, the mechanisms through which digital inclusion may be linked to depression—such as cognitive engagement and social participation—have rarely been examined simultaneously within an integrated analytical framework.
From a digital health perspective, this study addresses critical gaps by providing the first systematic examination of cognitive function’s moderating role in the association between digital inclusion and depressive symptoms among older adults, using large-scale nationally representative data.11,12 Despite the theoretical importance of cognitive factors in technology interaction, no previous study has systematically tested whether digital inclusion benefits are contingent on cognitive capacity levels. We systematically investigate the multiple pathways through which digital inclusion is associated with mental health outcomes, building on recent evidence of associations between functional disability and depressive symptoms, 13 and between depressive status and cognitive impairment 14 in this population. Recent evidence on digital exclusion among older adults further underscores the urgency of understanding who fails to benefit from digital health initiatives.15,16
To address these gaps, this study examines the association between digital inclusion and depressive symptoms in a large, nationally representative sample of older adults. It further investigates whether cognitive function moderates this association and explores the concept of a cognitive threshold pattern to capture heterogeneity in how older adults may experience digital inclusion. In addition, the study applies path analysis within an integrated conceptual framework informed by cognitive aging, cognitive reserve, and social integration perspectives to explore multiple pathways linking digital inclusion to mental health.
Drawing on these perspectives, we propose three hypotheses: (1) cognitive function significantly moderates the association between digital inclusion and depressive symptoms, with stronger protective associations among older adults with higher cognitive function; (2) digital inclusion shows associations with depressive symptoms through multiple pathways, including direct associations, cognitive enhancement, and social participation; and (3) cognitive function and social participation operate sequentially, with cognitive function being associated with social participation, which in turn is associated with depressive symptoms.
Methods
Study design and data source
This cross-sectional analysis utilized data from the 2020 wave of the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative survey of adults aged 45 and above in China. CHARLS employs a multi-stage stratified probability-proportional-to-size sampling method, covering 28 provinces and 150 counties/districts with excellent representativeness for digital health research. The survey includes comprehensive modules on demographic characteristics, socioeconomic status, health conditions, cognitive assessments, and digital device usage, providing an ideal data foundation for digital health research.
Data Transparency and Reproducibility: CHARLS data are publicly available through the National School of Development at Peking University (charls.pku.edu.cn).
Sample selection
We applied the following sample selection criteria: (1) adults aged 60 and above; (2) exclusion of proxy-answered questionnaires to ensure validity of cognitive assessments and self-reported data; (3) elimination of cases with missing data on core variables (digital inclusion, depression scores, cognitive function, social participation). Additional exclusions were made for participants with severe cognitive impairment (MMSE < 10) to ensure capacity for digital technology assessment. The CHARLS 2020 health module contained data from 19,367 respondents. After excluding 8,729 individuals aged below 60 years, 10,638 older adults remained. A further 1,171 respondents were excluded due to proxy-answered questionnaires, leaving 9,467 eligible participants. Missing data arose exclusively from the CES-D-10 depression scale (356 cases, 3.76%); all other core variables—the digital inclusion index, cognitive function composite score, and social participation index—were complete for all eligible respondents. Missing depression scores were handled using complete-case analysis (listwise deletion), yielding a final analytic sample of 9,111 participants (complete-case retention rate: 96.2%). The analytic sample comprised males (50.8%) and females (49.2%), with a mean age of 68.4 years (SD = 6.5 years).
Although the age range of the analytic sample extends up to 108 years, a sensitivity analysis excluding participants older than 90 years was conducted as a robustness check; the primary moderation findings were not materially altered, confirming that the inclusion of extreme-age respondents does not substantially bias the main results.
Sample selection and attrition process (N = 9,111).
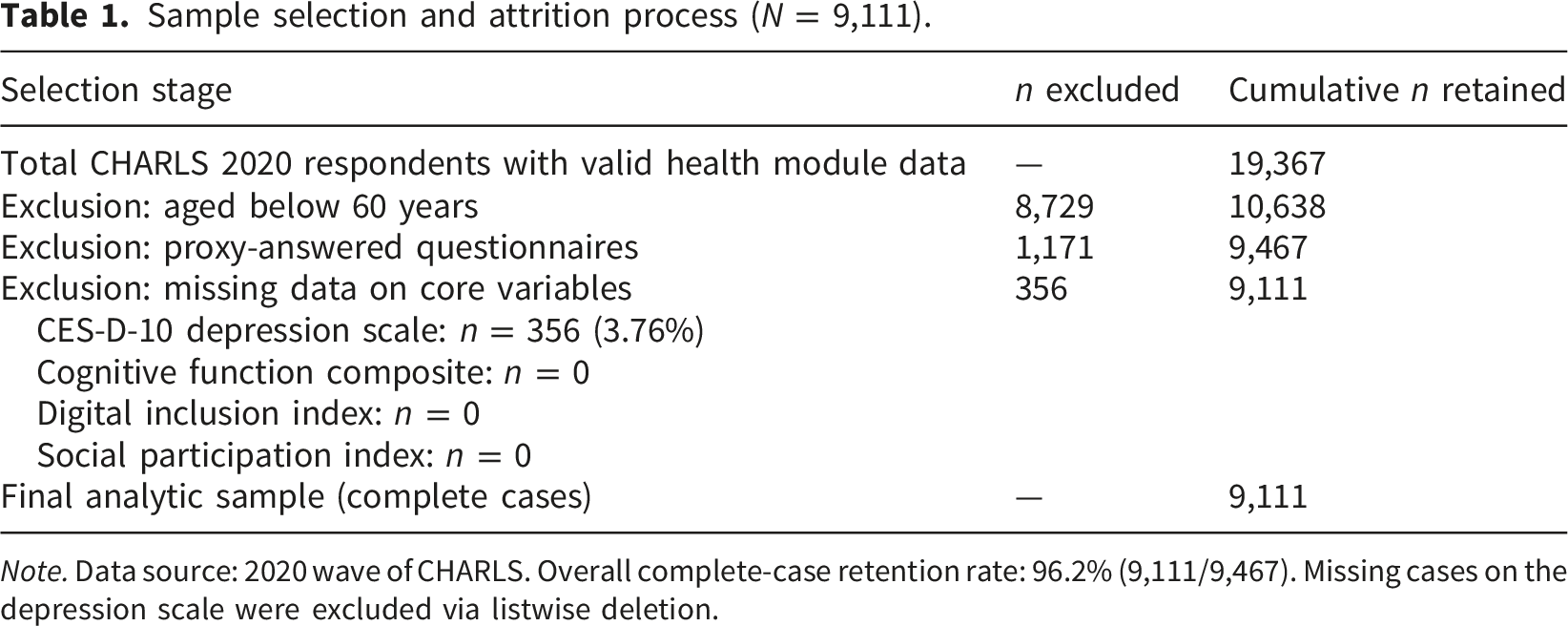
Note. Data source: 2020 wave of CHARLS. Overall complete-case retention rate: 96.2% (9,111/9,467). Missing cases on the depression scale were excluded via listwise deletion.
Measures
Digital Inclusion Index. Based on established digital health frameworks and multiple items regarding digital technology use in the CHARLS survey, we constructed a multidimensional digital inclusion index specifically relevant to health applications. The index included the following four dimensions: (1) Digital health access (0–3 points): Measuring basic digital technology access relevant to health information and services, including internet use (da040) and device usage (mobile phones/computers, da041); (2) Breadth of digital health functionality use (0–3 points): Measuring diversity of digital technology features used in health contexts, including health information searching, telemedicine use, mobile payment, social media use, information gathering, etc.; (3) Depth of digital health use (0–3 points): Measuring complexity of digital technology usage in health contexts, including frequency and proficiency of advanced functions in health management, social, financial, and entertainment domains; (4) Digital health confidence (0–1 point, normalized): Based on digital confidence ratings specifically related to health technology use, standardized to 0–1 point.
DIi = 0.3 × Accessi + 0.3 × Breadthi + 0.2 × Depthi + 0.2 × Confidencei
Weight allocation was based on digital health theoretical considerations and validated through sensitivity analyses using alternative weighting schemes (equal weights, expert-derived weights). Specifically, access and breadth each received a weight of 0.3, reflecting the established primacy of connectivity and functional diversity as foundational prerequisites for meaningful digital participation in health contexts2,17; depth and digital confidence, while important, serve as amplifying rather than enabling factors and were thus assigned lower weights of 0.2 each. This weighting scheme was further validated by sensitivity analyses using equal weights (0.25 per dimension) and expert-derived weights, both of which yielded substantively identical results for the primary moderation findings. As the theoretical maximum of the raw composite formula is 2.6 (i.e., 0.3×3 + 0.3×3 + 0.2×3 + 0.2×1 = 2.6), the raw score was subsequently standardized to a 0–10 scale by dividing by 2.6 and multiplying by 10, yielding a final DI index with a theoretical range of 0 to 10. Higher scores indicate higher levels of digital inclusion relevant to health applications.
Statistical analysis plan
All analyses followed a pre-specified plan to minimize researcher degrees of freedom and enhance reproducibility: (1) descriptive analysis with comprehensive missing data assessment and sensitivity analysis; (2) correlation analysis with 95% confidence intervals and significance testing; (3) hierarchical regression for moderation testing with interaction terms; (4) structural equation modeling for mediation pathways with bootstrap confidence intervals; (5) multiple sensitivity analyses using alternative model specifications and variable transformations.
Power calculations indicated adequate statistical power (>95%) to detect small-to-medium interaction effects (f2 = 0.02) with our analytic sample size (N = 9,111)
Cognitive function assessment
Cognitive function was assessed using the CHARLS harmonized cognitive assessment protocol, which has been validated for older Chinese adults and is relevant to digital health capacity evaluation.
12
The assessment includes comprehensive cognitive domains that are critical for digital technology interaction and health information processing9,14: (1) Immediate and delayed memory: Assessed through word recall tests, with 1 point for each correct recall, providing measures relevant to digital health information processing; (2) Executive function and attention: Assessed through mathematical calculations and task management, critical for digital health technology navigation; (3) Orientation and visuospatial ability: Assessed through recognition tasks and drawing tests, important for digital interface interaction.
A composite cognitive function score was computed by summing scores across all assessed domains and was treated as a continuous variable in all analyses (observed M = 562.35, SD = 235.78 in the analytic sample; higher scores reflect greater cognitive capacity). Domain-specific scores were retained for supplementary moderation analyses, reported in the Results section.
Depressive symptoms assessment
Depressive symptoms were measured using the 10-item depression symptom scale (CES-D-10) in CHARLS, validated for use in Chinese older adult populations. Each item is scored on a 0–3 scale (0 = rarely or never; 3 = most of the time; positive affect items are reverse-scored), yielding a total CES-D-10 score ranging from 0 to 30. In the present study, CES-D-10 scores were treated as a continuous variable across the full range, consistent with prior CHARLS-based analytical approaches.14,18 No clinical cutoff was applied in the primary analyses; the continuous operationalization preserves gradations in symptom severity and maximizes statistical power for examining dose–response associations. Higher scores indicate greater depressive symptom burden. The scale showed excellent internal consistency in our sample (Cronbach’s α = 0.86) and has demonstrated validity for identifying clinically relevant depressive symptoms in older adults.
Statistical analysis
Moderation Analysis. To test the moderating role of cognitive function in the association between digital inclusion and depressive symptoms, we constructed hierarchical regression models following established protocols for digital health research:
Depressioni = β0 + β1DigitalInclusioni + β2Cognitioni + β3(DigitalInclusioni × Cognitioni) + β4Controlsi + εi
We employed the Johnson–Neyman technique to identify regions of significance for the moderation
Cognitioni = α0 + α1DigitalInclusioni + α2Controlsi + ε1i SocialParticipationi = γ0 + γ1DigitalInclusioni + γ2Cognitioni + γ3Controlsi + ε2i Depressioni = δ0 + δ1DigitalInclusioni + δ2Cognitioni + δ3SocialParticipationi + δ4Controlsi + ε3i
Sensitivity and Robustness Analyses. To ensure robustness of findings for digital health applications, we conducted multiple sensitivity analyses: (1) alternative digital inclusion weighting schemes (equal weights, expert-derived weights); (2) different depression score transformations (log transformation, quantile normalization); (3) subgroup analyses by demographic characteristics relevant to digital health disparities; (4) propensity score matching to address potential selection bias in digital adoption; (5) exclusion of participants aged over 90 years to assess whether extreme-age respondents materially altered the primary findings; (6) comparison of complete-case results with multiply-imputed estimates to assess sensitivity to the missing data approach.
Results
Sample characteristics
Descriptive statistics and correlation matrix (N = 9,111).
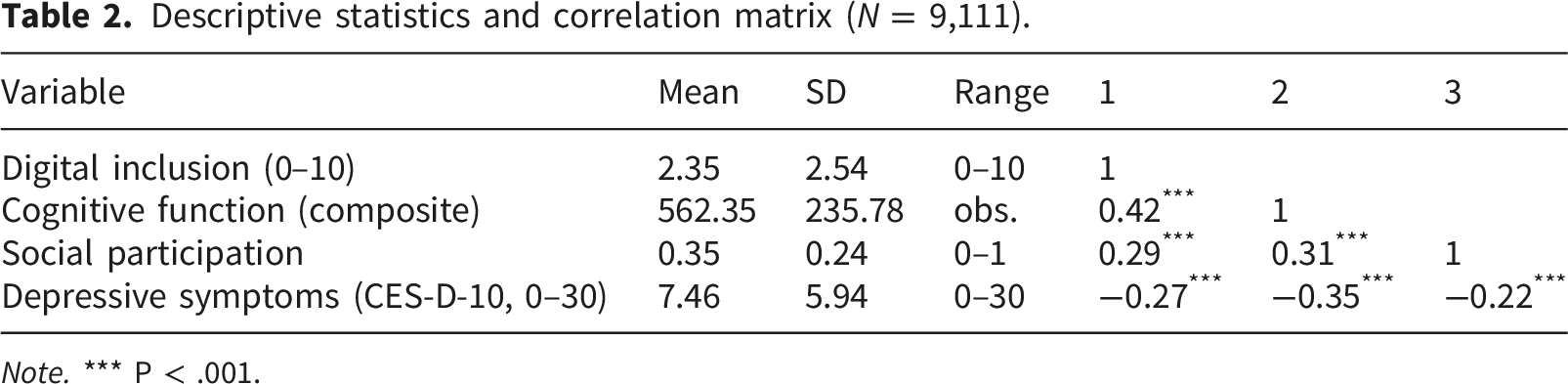
Note. *** P < .001.
Correlation analysis showed significant associations between all core variables relevant to digital health interventions. Digital inclusion was moderately positively correlated with cognitive function (r = 0.42, P <0.001), suggesting that cognitive capacity is an important determinant of successful digital health technology adoption. The negative correlation between digital inclusion and depressive symptoms (r = −0.27, P <0.001) provides initial support for protective associations, with effect sizes comparable to other established digital health interventions. The analytic sample size (N = 9,111) provides adequate statistical power to detect these associations and supports the robustness of our findings for precision digital health applications.
Cognitive function as a moderator
Hierarchical regression results: Cognitive function moderation of the association between digital inclusion and depressive symptoms.
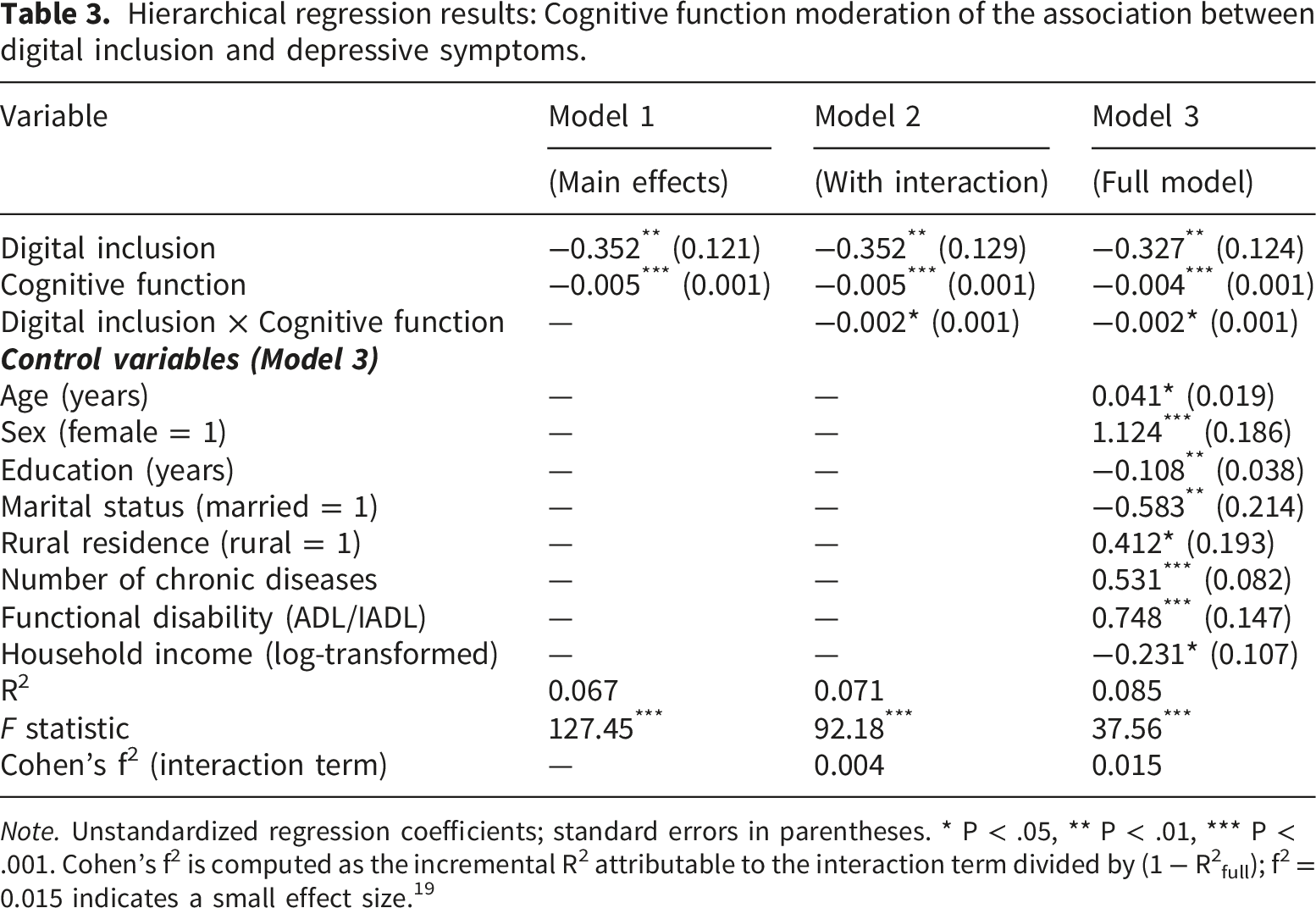
Note. Unstandardized regression coefficients; standard errors in parentheses. * P < .05, ** P < .01, *** P < .001. Cohen’s f2 is computed as the incremental R2 attributable to the interaction term divided by (1 − R2full); f2 = 0.015 indicates a small effect size. 19
The cognitive moderation association translates to meaningful clinical differences for digital health interventions: the association between digital inclusion and depressive symptoms in the highest cognitive function quartile (β = −0.517) was approximately 3.8 times the magnitude observed in the lowest quartile (β = −0.137). At high cognitive function levels (mean + 1 SD), each unit increase in digital inclusion was associated with a 0.517-point reduction in CES-D-10 scores (P < 0.001), while no significant association was observed at low cognitive function levels (mean − 1 SD, β = −0.137, P = 0.327). The Cohen’s f2 value for the interaction term (f2 = 0.015 in the full model) indicates a small effect size by conventional standards 19 ; although this suggests a modest practical magnitude, the association is statistically robust given the large sample and is theoretically meaningful for identifying cognitively stratified subgroups warranting differentiated digital health intervention.
Figure 1 illustrates the Cognitive threshold pattern: the association between digital inclusion and depressive symptoms across levels of cognitive function.The three-dimensional interaction plot illustrates the “cognitive threshold pattern.” Colors from dark to light represent CES-D-10 scores from low to high. As cognitive function increases (right side), the protective association between digital inclusion and depressive symptom burden becomes progressively more pronounced, indicating that the mental health benefits of digital inclusion strengthen with increasing cognitive capacity rather than switching abruptly at a fixed threshold. Cognitive threshold effect in digital health applications. The three-dimensional interaction plot demonstrates the “cognitive threshold effect” relevant to digital health intervention design. Colors from dark to light represent depression scores from low to high. As cognitive function increases (right side), the association between digital inclusion and reduced depression risk becomes more pronounced, suggesting optimal cognitive function levels for digital health intervention targeting.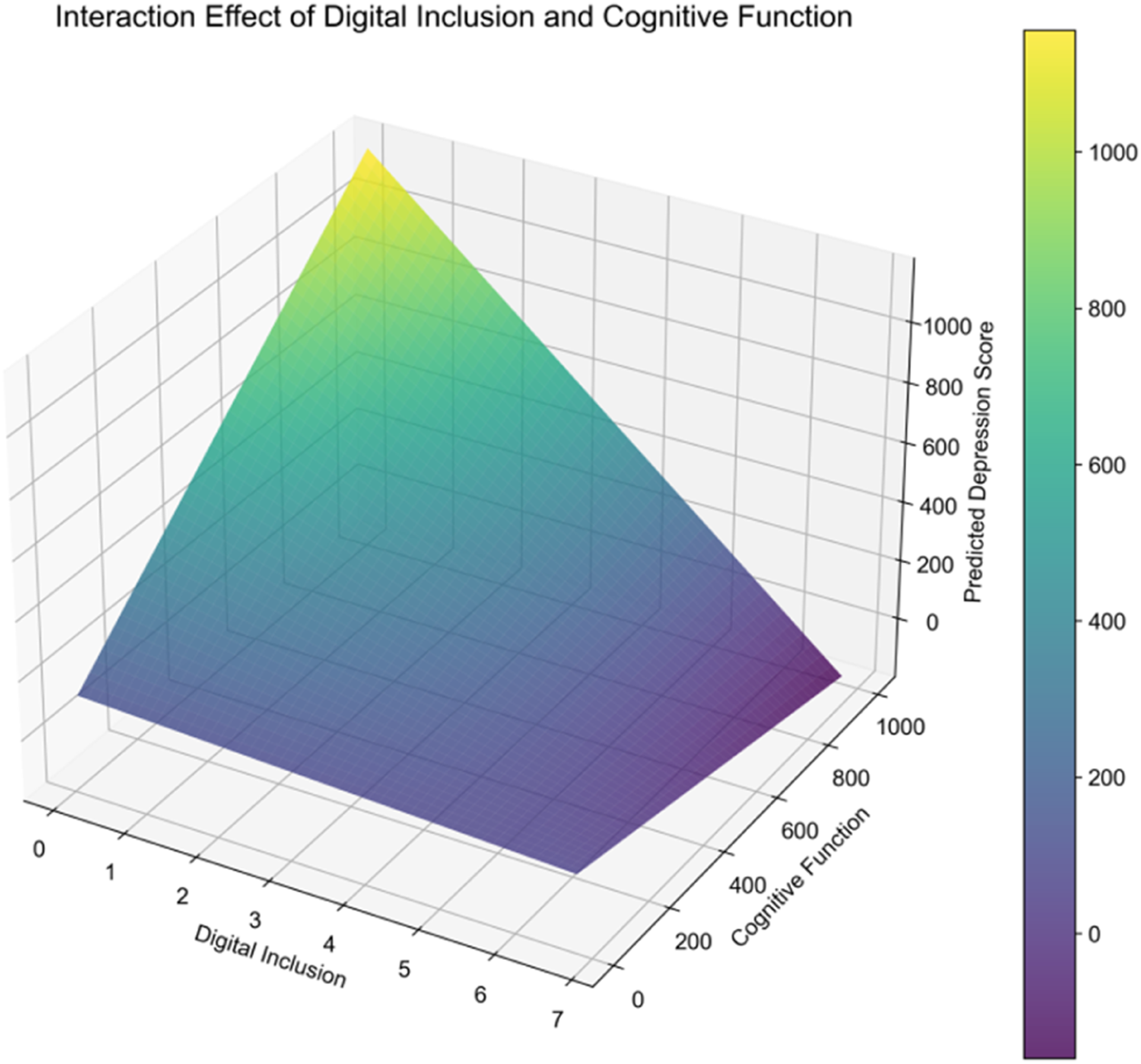
Multiple pathway analysis
Path analysis: Multiple pathways linking digital inclusion to depressive symptoms.
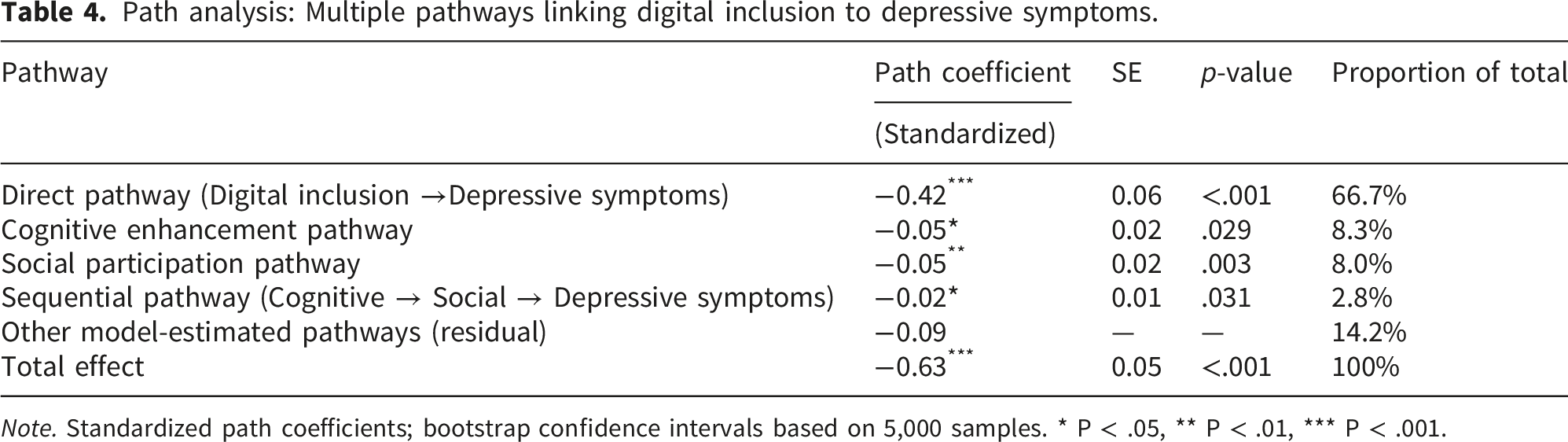
Note. Standardized path coefficients; bootstrap confidence intervals based on 5,000 samples. * P < .05, ** P < .01, *** P < .001.
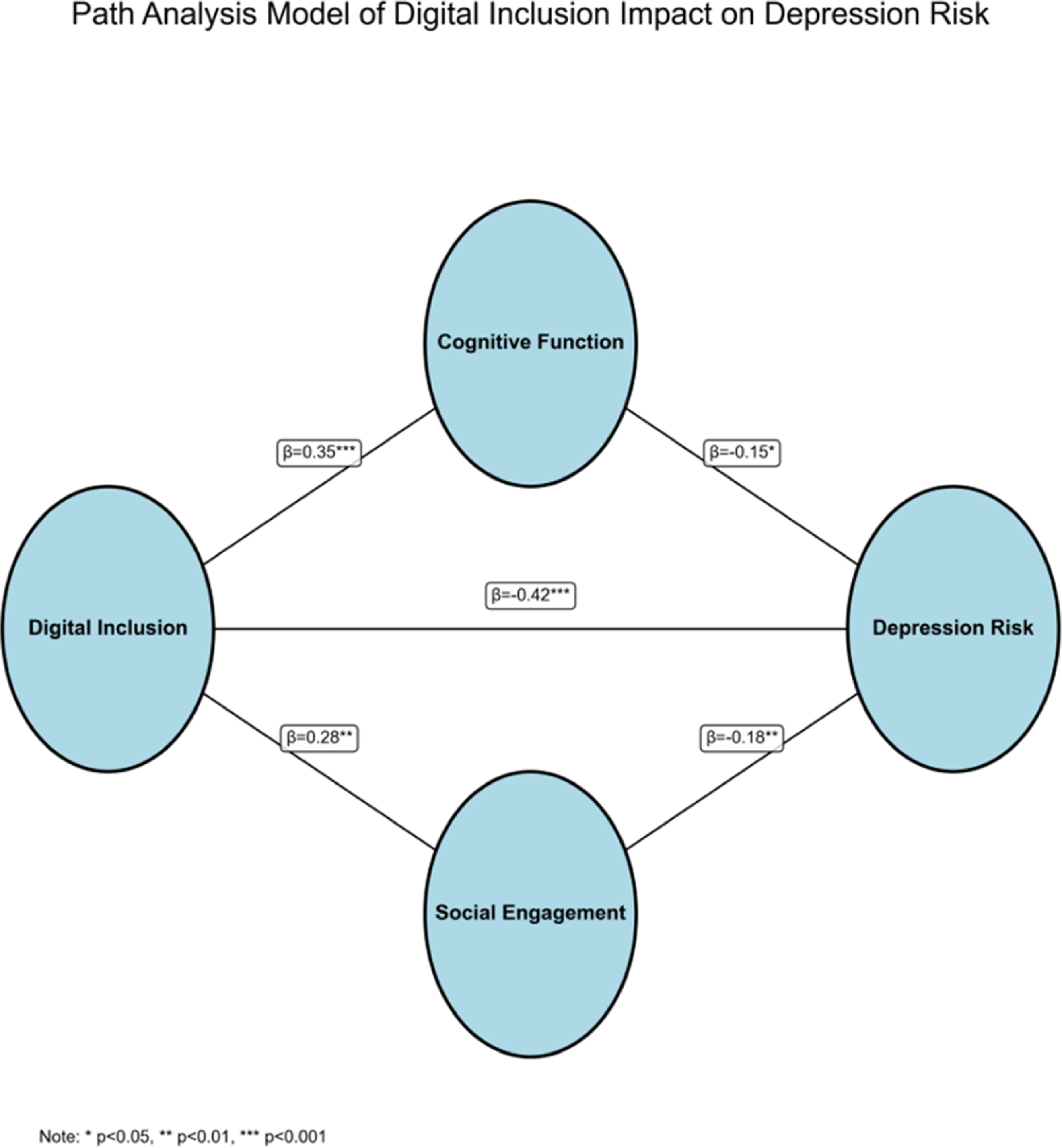
Digital health intervention pathway model. Path analysis model showing digital inclusion’s associations with depression risk through multiple mechanisms relevant to digital health interventions. The model demonstrates direct effects and mediation through cognitive enhancement and social participation pathways. Path coefficients represent standardized effects. Line thickness is proportional to effect size, providing visual guidance for intervention prioritization.
Figure 2 illustrates the Pathway model linking digital inclusion to depressive symptoms through cognitive enhancement and social participation. Path analysis model showing digital inclusion’s associations with depressive symptoms through multiple mechanisms relevant to digital health interventions. The model demonstrates direct associations and indirect associations through cognitive enhancement and social participation pathways. Path coefficients represent standardized effects. Line thickness is proportional to effect size, with the direct pathway predominating.
From a digital health intervention perspective, the direct pathway’s predominance (66.7% of total association) suggests that immediate psychological benefits of digital engagement—including enhanced self-efficacy, access to health information, and digital mastery experiences—constitute the primary mechanism. The cognitive enhancement pathway (8.3%) provides evidence for digital activities’ role in maintaining cognitive function, while the social participation pathway (8.0%) confirms digital technologies’ importance in facilitating social connection for mental health. A sequential pathway operating through both cognitive enhancement and social participation accounted for a further 2.8% of the total association; together with the other model-estimated pathways (14.2%), all identified pathways account for the full 100% of the total association, as shown in Table 4.
Domain-specific cognitive moderation associations
Domain-specific cognitive moderation associations with the digital inclusion–depressive symptoms relationship.
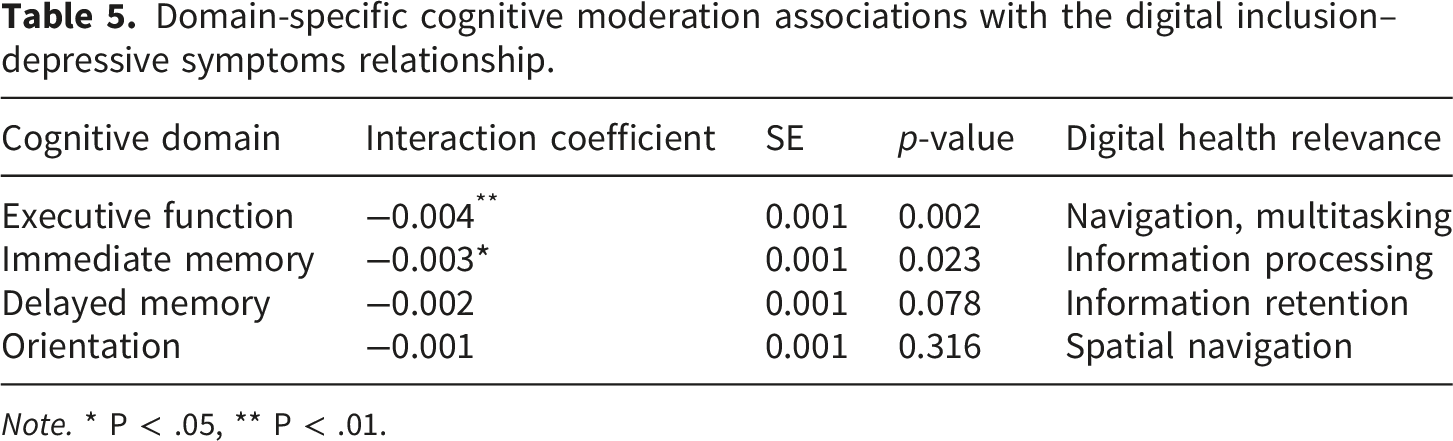
Note. * P < .05, ** P < .01.
Discussion
Summary of main findings
This study provides novel evidence for a cognitive threshold pattern in the association between digital inclusion and depressive symptoms, suggesting heterogeneity in how older adults may benefit from digital technologies. Using a nationally representative sample (N = 9,111), we find that the protective associations of digital inclusion with depressive symptoms are contingent on cognitive capacity levels, with significant associations emerging only above certain cognitive function thresholds. These findings highlight the potential value of moving beyond uniform digital health approaches by considering individual differences in cognitive capacity.
The cognitive moderation pattern has important implications for digital health intervention design and implementation, building on recent evidence that digital engagement can be associated with mental health outcomes 6 but revealing that individual cognitive capacity may moderate the association between digital inclusion and mental health outcomes. 8 Our findings show that among participants with higher cognitive function, digital inclusion showed strong protective associations with depressive symptoms (β = −0.517, p < .001), while those with lower cognitive function showed no significant associations (β = −0.137, p = 0.327). This difference in association strength suggests that cognitive stratification may be important to consider when developing digital health interventions.
Comparison with prior literature
The present findings align with, and extend, previous research demonstrating that digital technology use is associated with reduced depressive symptoms among middle-aged and older adults in China.5,6 However, whereas prior studies have largely treated digital inclusion as conferring relatively uniform benefits across older populations, the current results reveal important heterogeneity. The absence of a significant association in the lowest cognitive function quartile is a novel finding that challenges the assumption of universal benefit. Earlier work has documented associations between cognitive function and digital technology adoption, 8 but has not systematically examined whether cognitive capacity conditions the mental health associations of digital inclusion itself.
Our identification of multiple pathways adds to the existing literature by offering insights into potential mechanisms linking digital inclusion and depressive symptoms. The direct pathway’s predominance (66.7% of total association) suggests that digital health interventions may prioritize immediate psychological benefits including enhanced self-efficacy, health information access, and digital mastery experiences, aligning with evidence from digital inclusion initiatives for mental health services. 20 However, this study suggests that these direct associations may be contingent on cognitive capacity, highlighting an individual difference factor that has received limited attention in prior digital health research.
The cognitive enhancement pathway (8.3% of total association) supports the integration of cognitive training components within digital health platforms, building on recent evidence of associations between social integration and cognitive function trajectories. 10 This pathway is consistent with evidence of bidirectional associations between cognitive status and depressive symptoms,14,21 and highlights the potential for digital engagement to serve as a mechanism of cognitive maintenance.
The social participation pathway (8.0% of total association) emphasizes the importance of social features in digital health platforms, consistent with recent findings on the protective role of social integration against depression among older adults.22,23 This pathway was statistically significant (p = 0.003) but accounted for a relatively modest proportion of the total association. Several explanations may account for this: the CHARLS measure of social participation may not fully capture online social engagement; data collection during the COVID-19 pandemic may have suppressed offline social participation; and the primary mechanism linking digital inclusion to mental health may operate through informational and efficacy-related channels rather than increased social activity per se. These findings are also consistent with longitudinal evidence on the bidirectional association between functional disability and depressive symptoms in this population. 24
Theoretical implications
The identification of a cognitive threshold pattern carries important theoretical implications. From the perspective of Cognitive Load Theory, 25 older adults with limited executive function and working memory capacity may experience digital interfaces as imposing excessive extraneous cognitive load, particularly when interfaces are designed for users with typical cognitive abilities. Under conditions of high cognitive load, available mental resources are consumed by the demands of navigation and information processing, leaving insufficient capacity for higher-order cognitive engagement—such as meaning-making, social interaction, and health information appraisal—that may underlie the mental health benefits of digital participation. This account is consistent with the finding that executive function and immediate memory, most directly implicated in managing complex digital interactions, showed the strongest moderation associations.
A related theoretical lens concerns the concept of apparent inclusion. The present findings suggest that gains in formal digital access among cognitively impaired older adults do not translate into mental health benefits, indicating a form of functional digital exclusion that is invisible to access-based metrics. Older adults with lower cognitive function may possess smartphones or internet connections yet remain unable to engage with digital content in ways that confer psychological benefit. This apparent inclusion not only fails to reduce the mental health burden associated with social isolation and information poverty, but may compound existing stress through repeated frustrating encounters with digital systems. Future theoretical and empirical work should move beyond binary inclusion/exclusion distinctions to grapple with the quality and meaningfulness of digital participation across the cognitive spectrum.
Regarding the absence of a significant association in the lowest cognitive function group, this finding has important implications for digital health equity. If digital inclusion interventions are deployed universally without accounting for cognitive accessibility, they risk being systematically ineffective for the most cognitively vulnerable older adults—precisely those who may carry the greatest burden of depressive symptoms.9,14 This raises concerns about potential exacerbation of existing cognitive-health inequalities: policy efforts to promote digital inclusion may inadvertently widen the mental health gap between cognitively intact and cognitively impaired older populations if cognitive barriers are not concurrently addressed.
Policy and practical implications
These findings have implications for digital health intervention design. Rather than uniform digital health programs, our results suggest that cognitive-stratified approaches may be worth exploring: individuals with higher cognitive function may benefit from comprehensive digital platforms, those with moderate cognitive function may require simplified interfaces and structured support, while those with lower cognitive function may benefit most from human-mediated or hybrid approaches. Policymakers should exercise caution in mandating digital-only service delivery for older adults without accounting for cognitive accessibility, and analog or human-mediated alternatives should be maintained as genuine options. These recommendations are exploratory given the cross-sectional study design and require prospective validation before adoption.
At the level of technology design, our pathway findings point to the potential value of adaptive interfaces that adjust complexity based on user cognitive capacity, alongside integrated social networking and health information features that activate the multiple pathways identified in the analysis. These design principles are exploratory directions informed by the present cross-sectional findings, and their effectiveness requires prospective evaluation.
Study limitations and future research directions
This study has several limitations relevant to digital health research, though the nationally representative design strengthens the external validity of key findings. First, the cross-sectional design prevents definitive causal inference; all associations reported should be interpreted as statistical associations rather than causal relationships. Accordingly, we have employed associational terminology (e.g., “is associated with”) throughout the manuscript. Future longitudinal studies may examine bidirectional associations between digital inclusion and cognitive function over time, building on recent longitudinal CHARLS research on disability prediction 11 and cognitive function trajectories. 10
Second, the data were collected during the 2020 wave of CHARLS, which coincided with the peak of the COVID-19 pandemic in China. This period was characterized by unprecedented forced digitization—as lock downs and social distancing compelled older adults and healthcare systems to rapidly adopt digital communication tools—and by heightened baseline psychological distress across the population. Consequently, the observed associations between digital inclusion and depressive symptoms may partly reflect pandemic-specific dynamics, including accelerated digital adoption among those with sufficient cognitive resources and amplified distress among those unable to adapt to rapid digital transition. Readers should exercise caution in generalizing the magnitude of these associations to non-crisis contexts, and future research should replicate these analyses using data collected under more typical social conditions.
Third, the digital inclusion measurement, while comprehensive, may not fully capture emerging digital health technologies such as artificial intelligence-powered health assistants, virtual reality therapeutics, or advanced wearable devices. Future research may expand measurement frameworks to include these evolving technologies, particularly given rapid advances in digital health interventions for older adults with depression. 26
Fourth, although the analytic sample includes respondents up to 108 years of age, sensitivity analyses excluding participants older than 90 years confirmed that the primary moderation findings were not materially altered. Future studies focusing specifically on the oldest-old (aged 80+) are warranted given their distinct patterns of cognitive decline and digital engagement.
Fifth, missing data on the CES-D-10 depression scale (n = 356, 3.76%) were handled using complete-case analysis (list-wise deletion). While the high retention rate (96.2%) limits the potential for systematic bias, multiple imputation methods were not employed; future work should verify that results are not materially sensitive to the choice of missing data strategy.
Sixth, the present analyses did not account for sleep duration, which has been independently associated with depressive symptoms in Chinese older adult populations. 27 Future studies should include sleep quality as a co-variate to address potential residual confounding.
Several promising directions for future digital health research include: (1) randomized controlled trials testing cognitive-stratified digital health interventions; (2) longitudinal studies examining digital health technology adoption trajectories across cognitive decline; (3) development and validation of brief cognitive assessments specifically designed for digital health contexts; (4) investigation of cultural moderators affecting digital health intervention effectiveness across diverse populations, building on recent research on digital inclusion policies 17 and cultural factors in digital engagement. 28
Conclusions
In conclusion, this study found that higher levels of digital inclusion were associated with lower depressive symptoms among Chinese older adults, and that this association varied by cognitive function. The findings underscore the relevance of considering cognitive heterogeneity when examining the mental health implications of digital inclusion. While causal inferences cannot be drawn due to the cross-sectional design, these results may help inform future research and policy discussions on promoting mental well-being in aging populations within increasingly digital environments.
Footnotes
Acknowledgements
The author gratefully acknowledges the China Health and Retirement Longitudinal Study (CHARLS) research team for providing access to the 2020 dataset, and appreciates their contribution to advancing gerontological and public health research in China. We thank the CHARLS research team and all study participants.
Ethical considerations
This study utilized publicly available data from the 2020 wave of the China Health and Retirement Longitudinal Study (CHARLS), which does not involve direct interaction with participants and ensures anonymity. As the data were anonymized and publicly available, no informed consent or ethics committee approval was required for this study. The authors declare that all procedures followed were in accordance with relevant ethical guidelines, and the study was exempted from requiring ethics approval by the affiliated institution’s ethical review board.
Consent to participate
Not applicable.
Author contributions
Author initials: G.X. = Gang Xiao, Q.Y. = Qian Yang, F.B. = Fuyun Bai, Y.J. = Yanlong Jia, T.N. = Tingting Nie. G.X. and T.N. conceived and designed the study. G.X., Q.Y., and Y.J. developed the methodology. G.X. developed the analysis software and, together with Y.J., performed the formal analysis. Q.Y. and F.B. conducted the investigation, and F.B. and T.N. provided study resources. G.X. and Q.Y. curated the data, drafted the original manuscript, and prepared the figures. Y.J. and T.N. validated the results, critically reviewed and edited the manuscript, and supervised the project. T.N. handled project administration, and Y.J. acquired the funding. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hubei Provincial Natural Science Foundation of China (Grant No.2025AFD099), Health Science and Technology Project of Hubei Province (Grant No.WJ2025Q067), Xiangyang Central Hospital Personnel-Training Project (2025RCGD-016), Institutional-Level Scientific Research Project of Xiangyang Central Hospital (2025YA01A).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.