
Abstract
Background
Telemedicine is becoming embedded within hybrid care models integrating remote and in-person services across longitudinal pathways. Implementation challenges are often driven by sociotechnical misalignment and governance fragmentation rather than by technological limitations alone. However, few studies have examined how vulnerabilities emerge and accumulate across sequential stages of telemedicine delivery.
Objective
This study aimed to not only examine process-level vulnerabilities across a hybrid telemedicine care pathway but also develop a pathway-oriented sociotechnical perspective on telemedicine implementation.
Methods
This qualitative study involved 13 participants in South Korea, including 5 physicians (individual in-depth interviews) and 8 patients (focus groups, including individuals with disabilities) with telemedicine experience. Data were analyzed using reflexive thematic analysis informed by a sociotechnical implementation perspective aligned with the Nonadoption, Abandonment, Scale-Up, Spread, and Sustainability (NASSS) framework. Sequential pathway stages—appointment, identity verification, data submission, teleconsultation, prescription, and medication access and follow-up—were mapped to identify cross-stage vulnerabilities.
Results
Vulnerabilities were categorized into four domains: responsibility ambiguity, workflow discontinuity, technological constraint, and governance fragmentation, being most pronounced at stage interfaces, where inconsistent authentication, fragmented prescribing workflows, and incomplete information transfer undermined careful continuity and safety. Accessibility challenges functioned as cross-cutting system properties rather than as individual-level limitations. Importantly, vulnerabilities accumulated across stages, reinforcing uncertainty in hybrid care coordination.
Conclusion
Telemedicine implementation should be conceptualized as a longitudinal sociotechnical pathway requiring alignment across governance, workflow, platform design, and regulatory structures. A pathway-oriented perspective could support system-level interventions to improve safety, equity, and sustainability in hybrid digital health systems.
Keywords
Introduction
Telemedicine has become an increasingly integral component of contemporary digital health systems.1,2 Rather than functioning as a standalone modality, it is now embedded within hybrid models of care that integrate both remote and in-person services across longitudinal healthcare pathways.3,4 With the expansion of telemedicine in scope and scale, scholarly attention has shifted from technical feasibility toward broader concerns regarding care quality, safety, continuity, equity, and long-term sustainability.5–7
Although telemedicine can achieve clinical outcomes comparable to in-person care in selected contexts, a recent umbrella review identified persistent implementation challenges that constrain the sustainability of digital health technologies. 8 These challenges are increasingly understood as consequences of how telemedicine is embedded within clinical workflows, organizational routines, and governance structures rather than as failures of technology alone.6,9 Implementation research highlights the interaction of sociotechnical domains—including technologies, adopters, organizational processes, and regulatory environments—as articulated in the Nonadoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework and demonstrated in subsequent digital health applications.10,11 Fragmentation across stages of care—such as scheduling, consultation, prescribing, and follow-up—has been linked to inefficiencies and discontinuities in telemedicine delivery,12,13 while broader evaluation frameworks highlight integration and coordination challenges. 5
Much of the existing literature has focused on barriers and facilitators of adoption and implementation, particularly technology acceptance and provider attitudes.8,14 However, comparatively scarce attention has been paid to how structural misalignment unfolds across interconnected stages of telehealth delivery. Viewing telemedicine as a longitudinal, pathway-oriented process—rather than as a series of isolated encounters—may provide a more comprehensive lens to identify system-level vulnerabilities.5,6
Accessibility and health equity remain central concerns in digital health. Evidence suggests that telemedicine may exacerbate disparities when system and platform designs fail to accommodate older adults, individuals with disabilities, and socioeconomically disadvantaged populations.15–17 Such barriers frequently span multiple components of telehealth delivery systems, indicating structural rather than purely individual determinants.18,19
In South Korea, telemedicine has been implemented through a government-led pilot program to assess feasibility and safety. Following temporary expansion during the COVID-19 pandemic, a nationwide pilot project was launched in June 2023, initially targeting clinic-level medical institutions and patients with prior face-to-face encounters.20,21 Telemedicine is now transitioning toward formal institutionalization, with Korean studies reporting generally acceptable safety and continuity despite persistent operational challenges.
Qualitative research is well suited to examining complex, process-oriented implementation phenomena by capturing stakeholder experiences and contextual dynamics.9,22 By eliciting perspectives from clinicians and patients, qualitative inquiry provides insights into how governance arrangements are enacted within hybrid digital care pathways. However, although prior research has addressed adoption, implementation, and equity dimensions,6,8,14,18 comparatively limited attention has been paid to governance fragmentation across platforms, providers, regulators, and patients. This study therefore examines governance fragmentation within a hybrid telemedicine care pathway and proposes a sociotechnical framework to understand implementation challenges, thereby advancing digital health implementation research through a process-oriented, system-level perspective.
Methods
Study design
This qualitative study employed reflexive thematic analysis. 23 Individual in-depth interviews (IDIs) and focus group discussions (FGDs) were conducted to examine governance fragmentation and process-level vulnerabilities within a hybrid telemedicine care pathway. The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 24 The completed checklist is provided in Supplementary Material A.
The study was informed by a sociotechnical implementation perspective conceptually aligned with the NASSS framework, 10 which was used not as a coding framework but as an interpretive lens during data analysis and the subsequent discussion. Initial coding and theme development were conducted inductively, allowing patterns of process-level vulnerabilities to emerge from the data. These themes were then interpreted in relation to NASSS domains to support a sociotechnical understanding of cross-level misalignment across sequential stages of care.
Setting and context
The study was conducted in South Korea, where telemedicine operates under a government-led pilot program and is transitioning toward formal institutionalization. The regulatory environment is characterized by evolving legal arrangements, digital platform involvement, and multi-actor governance structures, providing an ideal opportunity to examine hybrid telemedicine pathways under conditions of regulatory transition and institutional complexity.
Participants and sampling
Characteristics of study participants across stakeholder groups.
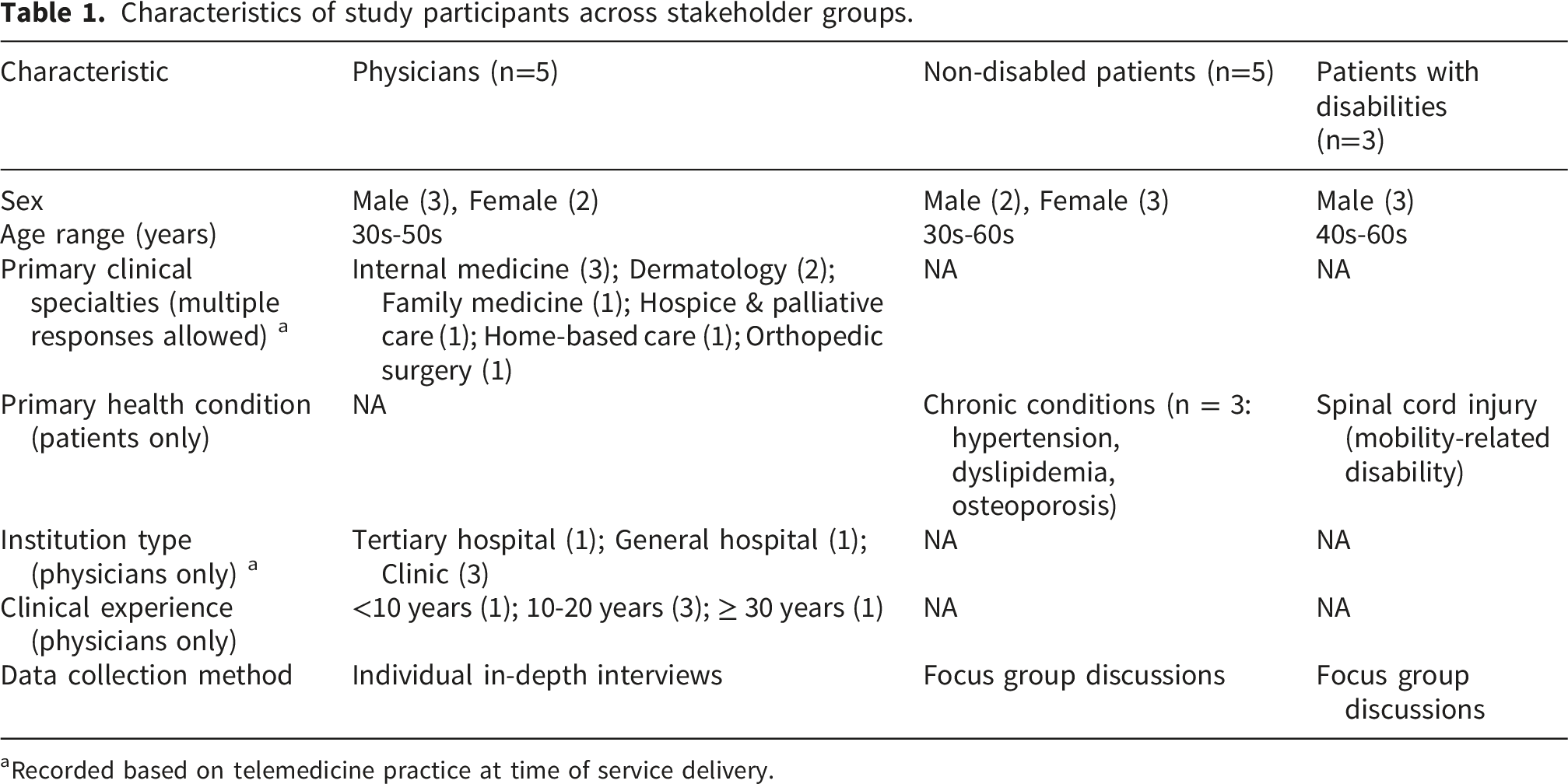
aRecorded based on telemedicine practice at time of service delivery.
Eligibility criteria were defined a priori. Physicians were required to have direct experience providing telemedicine services during the national pilot program. Patients were eligible if they had at least one prior telemedicine consultation within the pilot program, while individuals without telemedicine experience were excluded. For focus group participation, eligibility was further limited to individuals able to engage in face-to-face group discussion.
Five physicians who had provided telemedicine services during a national pilot program participated in IDIs. They were recruited using purposive and snowball sampling to ensure variation in institutional settings and clinical specialties. Initial participants were identified through academic societies and professional networks engaged in telemedicine research and guideline development and were approached via professional networks and email contact. Additional participants were recruited through peer referral.
Two FGDs were conducted with telemedicine users, one each with non-disabled patients (n=5) and one group of patients with disabilities (n=3). Non-disabled participants were recruited through a professional research agency using a structured screening questionnaire to verify telemedicine experience, and were invited via telephone.
Participants with disabilities were recruited in collaboration with a national disability organization. Initial contact and recruitment were conducted by telephone. Given the FGD format and communication requirements, only individuals able to participate in face-to-face group discussion were included. The final group comprised three participants with spinal cord injuries. None of the participants withdrew after enrollment.
Data collection
IDIs and FGDs were conducted face-to-face by members of the research team (Oh IH, Sul AR, Ju J, and Seo S), comprising two female and two male researchers trained in qualitative research and health policy. Each session was facilitated by one researcher, with a second researcher present as co-facilitator. The remaining two researchers observed from a separate room and recorded field notes during and immediately after each session to document contextual observations and non-verbal dynamics. No non-participants were present in the IDI or FGD room. All sessions were conducted in private meeting rooms at a research facility.
Participants were informed in advance of the study purpose and the institutional affiliations of the research team. No prior personal relationships existed between researchers and participants before recruitment.
Physician IDIs were conducted between September 2 and 4, 2025, and patient FGDs were held on September 3 and 9, 2025. Sessions lasted approximately 90–120 minutes and were audio-recorded with participants’ consent.
Semi-structured guides for IDIs and FGDs were developed by the research team, informed by the sociotechnical perspective. Although formal validity testing is not typically applied in qualitative data collection research, these guides were reviewed and refined through team discussion and expert review prior to data collection. The initial data collection phase functioned as an iterative refinement process, allowing minor adjustments to the guides to improve the clarity, flow, and relevance of questions as data collection progressed. The full guides are provided in Supplementary Material B. Repeat interviews were not conducted.
For the FGD, specific moderation strategies were employed to mitigate potential group dynamics. Given the heterogeneous composition of the group, the moderator actively facilitated balanced participation by encouraging turn-taking and explicitly inviting input from quieter participants. Probing questions were directed to individuals to elicit diverse and potentially divergent perspectives. Efforts were made to not only maintain moderator neutrality but also avoid reinforcing dominant viewpoints. During analysis, data from the FGD were coded at the level of individual contributions, and divergent or minority views were retained as meaningful data rather than being subsumed under dominant themes. Audio recordings were transcribed verbatim and anonymized prior to analysis. Transcripts were not returned to participants for comments or corrections.
Data analysis
Data were analyzed using reflexive thematic analysis following the approach of Braun and Clarke. 23 Coding was conducted manually and inductively to allow themes to emerge from the data, using standard office software (e.g., Microsoft Word and Excel); no specialized qualitative data analysis software (e.g., NVivo or Atlas. ti) was used. This approach aligns with reflexive thematic analysis, which emphasizes interpretive engagement with the data rather than reliance on software-assisted coding. Initial line-by-line coding was independently undertaken by multiple researchers to generate codes reflecting process-level vulnerabilities and sociotechnical interactions.
The codes were then compared and grouped into candidate themes, forming an analytic framework that captured misalignment across technological, organizational, workflow, and governance domains. The derived themes were refined through iterative team discussions emphasizing conceptual coherence rather than statistical agreement.
Despite the involvement of multiple researchers in coding, the analytic process did not aim to achieve inter-coder reliability or coding consensus. Instead, coding was treated as an interpretive and iterative process, with coding differences used to deepen analytic insight through reflexive discussion.
Process-level vulnerabilities across stages of the hybrid telemedicine pathway.
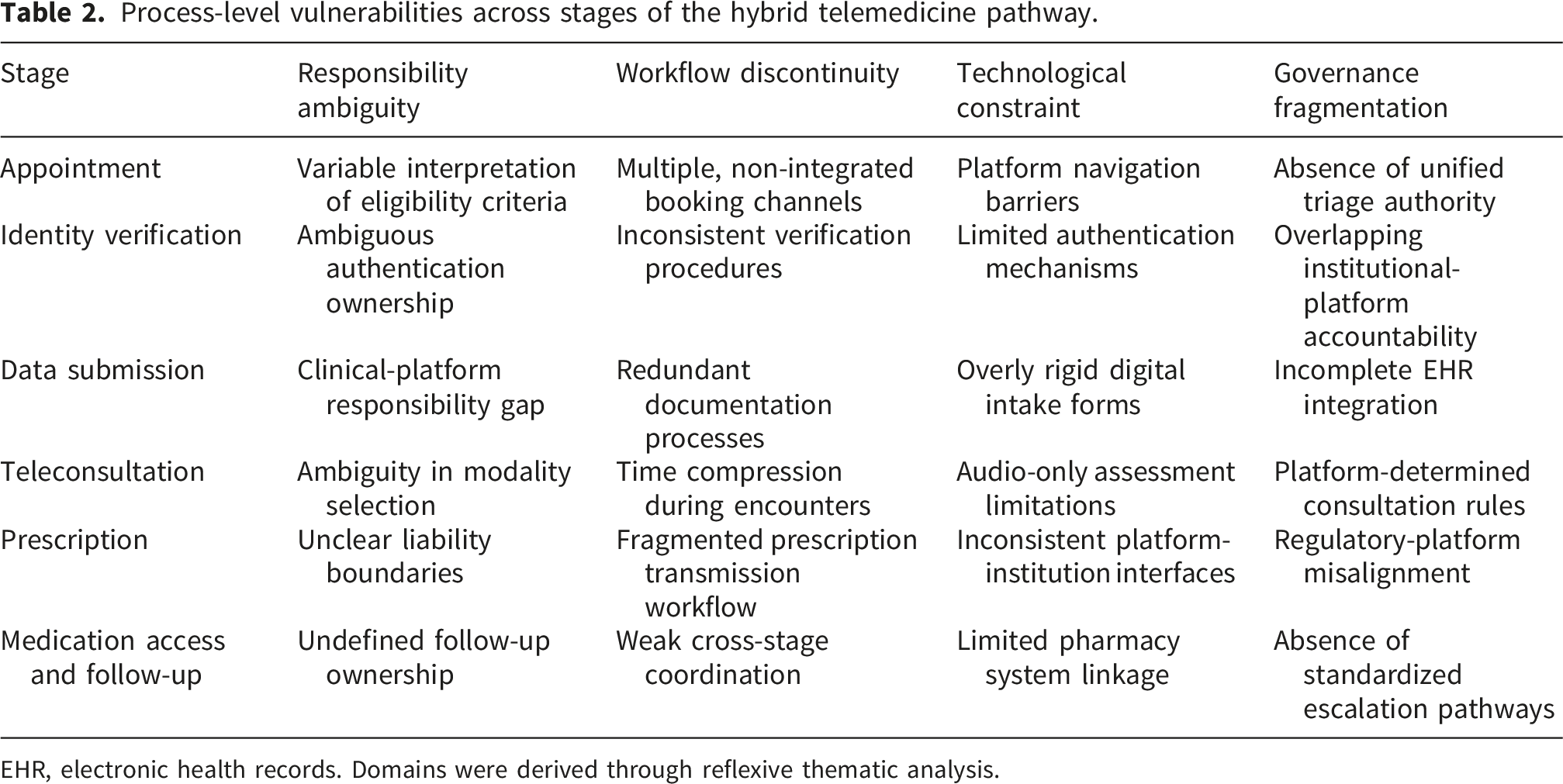
EHR, electronic health records. Domains were derived through reflexive thematic analysis.
System-level responses to cross-stage vulnerabilities in hybrid telemedicine.
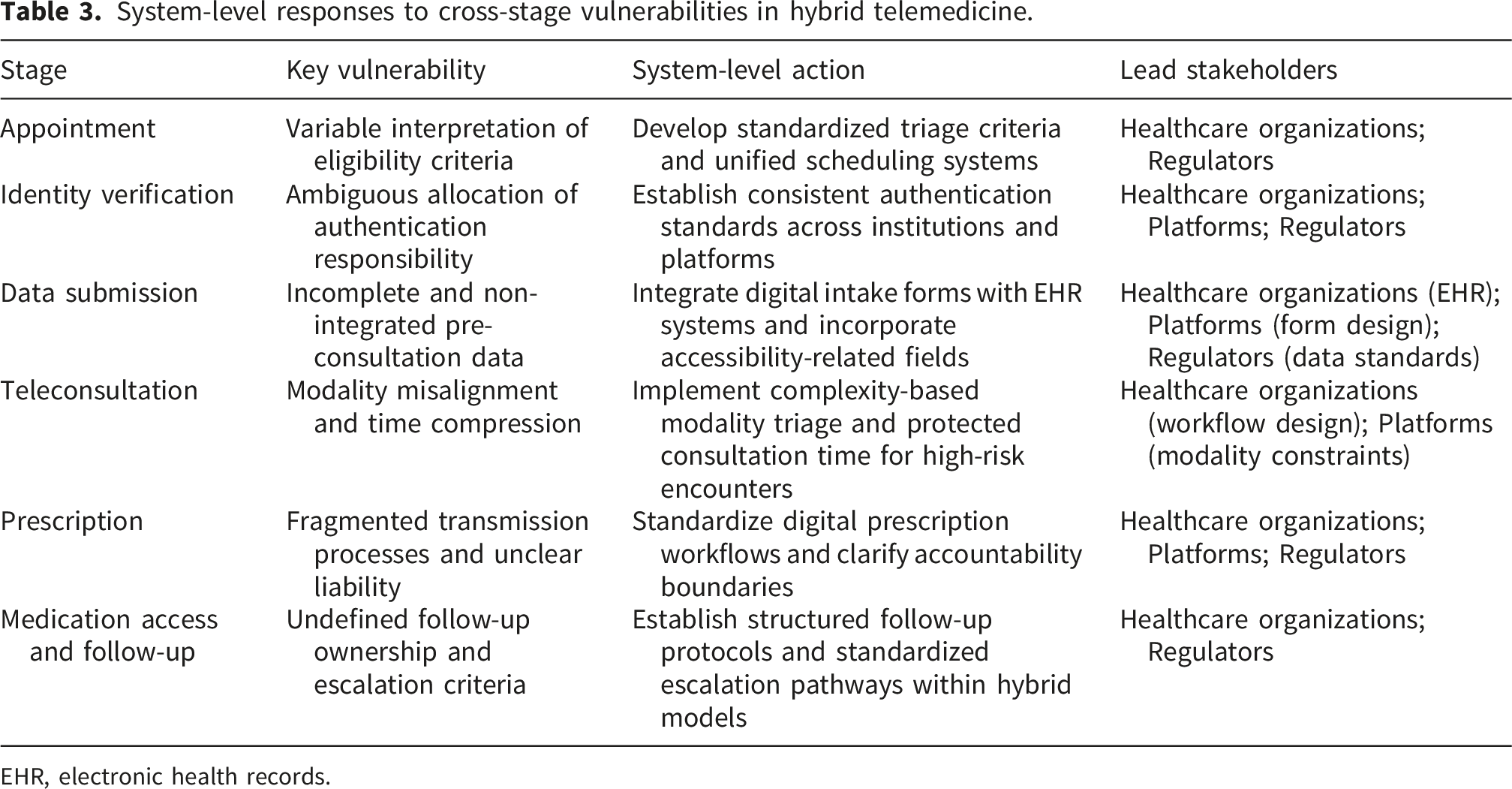
EHR, electronic health records.
Analytic rigor was supported through reflexive memoing, systematic documentation of analytic decisions, and ongoing team dialogue to enhance credibility, dependability, and confirmability in line with established trustworthiness criteria. 22
Thematic saturation was assessed iteratively. After seven IDI and FGD sessions, no substantively new conceptual categories or governance-related vulnerabilities emerged. The final session confirmed thematic redundancy and analytic depth across stakeholder groups. Saturation was conceptualized as meaning saturation and information power, focusing on conceptual depth rather than on a predefined numerical threshold,26,27 emphasizing the adequacy of analytic insight and thematic richness rather than the frequency of code emergence. Participant checking of findings was not conducted.
The final themes represent analytically derived patterns of sociotechnical vulnerability across stages of care and are organized into four domains: responsibility ambiguity, workflow discontinuity, technological constraint, and governance fragmentation.
Reflexivity
The research team comprised faculty members and health policy researchers affiliated with academic and public research institutions at the time of the study. All researchers involved in data collection had doctoral-level training in health policy, digital health, and qualitative research. Several researchers had prior professional involvement in telemedicine policy research, providing contextual familiarity and the potential to shape analytic interpretation.
Reflexive discussions were conducted throughout data collection and analysis to critically examine how prior assumptions regarding governance fragmentation, implementation challenges, and digital equity might influence coding and theme development. This process informed analytic decisions and was used to enhance transparency, credibility, and confirmability. 22
Ethical considerations
Ethical approval was obtained from the Institutional Review Board of the National Evidence-based Healthcare Collaborating Agency (NECAIRB 25-019). All participants provided written informed consent prior to participation, including consent for audio-recording. Identifying information was removed from transcripts prior to analysis, and data were stored securely in password-protected systems accessible only to the research team. To further protect participant confidentiality given the small group sizes, quotations presented in the Results are attributed to participant groups (physician, non-disabled patient, or patient with disability) without individual identifiers.
Results
Participant characteristics
As summarized in Table 1, participating physicians represented diverse clinical specialties, institutional settings, and levels of telemedicine experience within the national pilot program. Patient participants varied in age, sex, and health status. Most non-disabled patients reported chronic conditions requiring ongoing management, indicating that telemedicine use was embedded within longitudinal care rather than limited to episodic consultations. Participants with disabilities had established care needs and prior telemedicine experience, enabling examination of accessibility-related vulnerabilities within hybrid care delivery.
Overview of system-level vulnerabilities
The analysis identified systemic vulnerabilities across all stages of the hybrid telemedicine care pathway that did not reflect isolated technical failures but emerged from sociotechnical misalignment across governance arrangements, clinical workflows, platform design, and regulatory oversight.
Six sequential stages were examined: appointment, identity verification, pre-consultation data submission, teleconsultation, prescription, and medication access and follow-up. Across these stages, vulnerabilities clustered into four analytically derived domains, which represent the core themes of this study: (1) responsibility ambiguity, which refers to unclear allocation of decision-making authority across actors; (2) workflow discontinuity, which denotes breakdowns across sequential care processes; (3) technological constraint, which reflects structural limits imposed by platform design and interface architecture; and (4) governance fragmentation, which captures misalignment across institutional, regulatory, and platform actors.
Participants described how these vulnerabilities accumulated across stages:
“It’s not just one issue—small problems at each step build up and make the whole process feel unreliable.” (Physician)
Table 2 synthesizes these findings into a stage-by-domain diagnostic framework, illustrating how distinct forms of sociotechnical misalignment arise at specific interfaces along the telemedicine pathway. Rather than isolated issues, these vulnerabilities are embedded in routine care processes and distributed across system components.
Table 3 translates these diagnostic insights into a system-level response framework by linking key vulnerabilities to corresponding actions and responsible stakeholders. This framework outlines an operational approach to align governance structures, clinical workflows, and platform design, highlighting the role of coordinated stakeholder action in addressing cross-stage vulnerabilities in hybrid telemedicine systems.
Importantly, vulnerabilities did not operate independently but accumulated across stages, reinforcing uncertainty and reducing confidence in telemedicine as a continuous mode of care rather than as an isolated digital encounter. Together, these tables provide a pathway-oriented conceptual and practical framework that can inform both the evaluation and implementation of hybrid telemedicine systems.
To summarize these findings, we developed a conceptual diagram (Figure 1) that maps the distribution and emergence of vulnerabilities across sequential stages of the hybrid telemedicine pathway. Conceptual framework of telemedicine as a longitudinal sociotechnical pathway. Telemedicine is conceptualized as a longitudinal sociotechnical pathway rather than discrete encounters. Vulnerabilities arise across stages and domains, producing pathway-level misalignment, which system-level responses aim to address through alignment of policy, platform, and clinical workflow.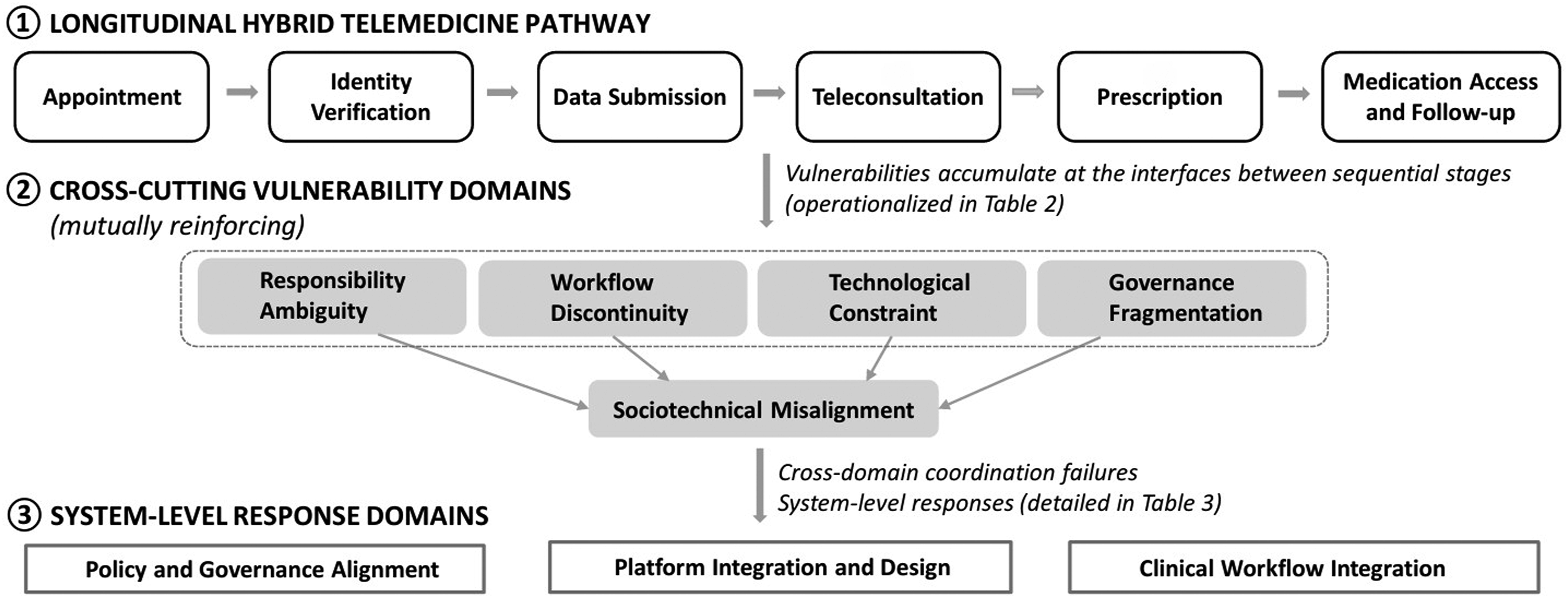
Stage 1: Appointment – Access variability and responsibility ambiguity
During the initial engagement, participants described substantial variability in how telemedicine services were accessed and coordinated. Physicians operated across multiple booking channels—including institutional systems, commercial platforms, and direct requests—without a unified scheduling framework:
“Depending on the platform or hospital, the booking system is completely different, so there’s no unified way to manage appointments.” (Physician)
Patients encountered inconsistent entry pathways, contributing to uncertainty regarding their eligibility and timing:
“I wasn’t sure if I could use telemedicine or how to start—it depends on where you hear about it.” (Non-disabled patient)
Divergent sources of telemedicine awareness shaped expectations. Physicians described structured familiarity with policy and procedural guidance, whereas patient awareness was often informed by fragmented sources such as media or platform advertisements. This divergence contributed to uneven expectations regarding the scope of care and limitations of remote consultation, particularly among first-time users. Scheduling thus functioned as an early trust-forming stage within the hybrid pathway, reflecting variability in eligibility interpretation and fragmented booking structures.
Stage 2: Identity verification – Procedural inconsistency and safety concerns
Identity verification practices varied across institutions and platforms. Some settings relied on minimal authentication procedures, raising concerns regarding impersonation risk and misidentification:
“Sometimes identity verification is very basic, and it makes me uneasy about whether the patient is correctly identified.” (Physician)
Responsibility for verification was perceived as ambiguously distributed between providers and platforms:
“It’s unclear whether the hospital or the platform should take responsibility for verifying the patient’s identity.” (Physician)
Participants also noted inconsistencies in verification procedures:
“Sometimes the identity check feels minimal while, at other times, it’s more thorough—it’s not consistent.” (Non-disabled patient)
Participants linked inconsistent authentication standards to broader concerns regarding procedural reliability and patient safety, especially in contexts involving prescriptions or sensitive health information. Such inconsistencies reflect underlying ambiguity in the allocation of responsibilities and the variability in verification processes across platforms.
Stage 3: Pre-consultation data submission – Fragmented information flow
Pre-consultation data submission processes were described as insufficiently integrated with electronic health records. Physicians noted that digital questionnaires were frequently overly simplified and lacked clinically meaningful detail. This led to redundant information verification during consultations, undermining intended workflow efficiencies:
“The questionnaire is too basic; so I still have to ask everything again during the consultation.” (Physician)
Patients reported difficulty navigating structured digital forms, particularly when medical terminology was used:
“The questions are too limited, and it’s hard to explain my condition properly.” (Non-disabled patient)
Patients with disabilities emphasized that functional status, mobility constraints, and contextual care needs were rarely captured adequately:
“There’s no place to explain disability-related issues, which are important for my care.” (Patient with disability)
These documentation gaps were linked to concerns about clinical safety, decision-making reliability, and alignment between submitted information and actual care needs, corresponding to workflow discontinuity, technological constraints, and incomplete system integration.
Stage 4: Teleconsultation – Interactional and diagnostic constraints
Although teleconsultation improved convenience and reduced travel burden, physicians reported reduced diagnostic confidence, particularly in audio-only encounters or when contextual cues were limited:
“Without seeing the patient directly, it’s harder to make accurate judgments, especially in complex cases.” (Physician)
Consultation modality was often predetermined by platform configuration rather than by clinical complexity:
“Whether it’s video or phone isn’t always based on the patient’s condition.” (Physician)
Both physicians and patients characterized teleconsultations as compressed and standardized, shaped by system constraints rather than by individualized care needs:
“It feels shorter and more rushed than in-person visits.” (Non-disabled patient)
While efficiency was acknowledged, participants described tension between convenience and relational depth, especially when managing complex or evolving clinical conditions. These findings reflect modality ambiguity, time compression, and platform-driven constraints.
Stage 5: Prescription – Regulatory and platform misalignment
Prescription transmission revealed tensions between digital efficiency and regulatory safeguards. Physicians reported fragmented workflows linking telemedicine platforms, healthcare institutions, and pharmacies:
“Different systems don’t communicate well with each other.” (Physician)
Ambiguity in liability distribution between clinical decision making and platform-mediated prescription processes was frequently noted:
“If something goes wrong, it’s not clear whether the responsibility lies with the doctor, the platform, or the pharmacy.” (Physician)
Participants reported uncertainty regarding medication processes:
“Sometimes the prescription doesn’t reach the pharmacy smoothly.” (Non-disabled patient)
Breakdowns at this stage were described as undermining confidence in telemedicine as a reliable modality of care, reflecting fragmented workflows, interface limitations, and regulatory–platform misalignment.
Stage 6: Medication access and follow-up – Continuity gaps
Medication access and follow-up processes lacked standardized coordination mechanisms, with patients reporting uncertainty regarding dispensing locations and monitoring responsibilities:
“After the consultation, I wasn’t sure who to contact if something changed.” (Non-disabled patient)
These vulnerabilities were amplified among individuals with mobility limitations or reduced pharmacy access:
“Getting the medication itself can be difficult, especially when mobility is limited.” (Patient with disability)
During transition to in-person care, escalation criteria were often unclear. Physicians and patients described ambiguity regarding responsibility for monitoring and referral decisions:
“There’s no clear guideline on when to switch to face-to-face care.” (Physician)
This stage proved pivotal in determining whether telemedicine functioned as an integrated component of a hybrid care continuum or as an isolated, episodic interaction, reflecting gaps in follow-up ownership, coordination, and escalation pathways.
Cross-stage finding: Governance fragmentation
Across all stages, vulnerabilities were amplified by fragmented governance structures, with platforms, clinicians, regulators, and patients operating within partially overlapping yet insufficiently aligned responsibility frameworks:
“There are multiple actors involved, but no clear coordination between them.” (Physician)
Rather than discrete operational failures, the findings highlight the systemic uncertainty generated by misaligned institutional arrangements. Governance fragmentation functioned as a cross-cutting condition shaping responsibility allocation, workflow coordination, technological design constraints, and continuity of care throughout the hybrid telemedicine pathway.
Discussion
Building on the stage-by-domain analysis presented in Tables 2 and 3, the conceptual diagram (Figure 1) illustrates how vulnerabilities arise at stage interfaces and accumulate along the care pathway. It further demonstrates how cross-cutting vulnerability domains interact to produce sociotechnical misalignments, highlighting the systemic and process-oriented nature of fragmentation in hybrid telemedicine systems.
Telemedicine as a longitudinal sociotechnical pathway
This study identifies telemedicine as a longitudinal, multi-stage sociotechnical pathway rather than as a series of isolated digital encounters. Implementation challenges arose less from resistance to digital technologies than from how care processes were structured, coordinated, and governed across sequential stages. Breakdowns were consistently observed at interfaces between scheduling, pre-visit preparation, consultation, prescribing, and follow-up, highlighting the embedded fragmentation within routine care processes rather than that arising from discrete technical failures. Similar patterns of responsibility ambiguity and workflow fragmentation have been observed in chronic care and telemonitoring contexts, 28 further supporting this pathway-oriented conceptualization and suggesting that integration unfolds across interconnected organizational processes rather than through discrete clinical events.
Importantly, this pathway-oriented perspective extends prior research that has typically examined telemedicine challenges within single domains—such as technology performance, patient experience, or policy constraints—by demonstrating how vulnerabilities accumulate across sequential stages of care. This perspective advances pathway-oriented evaluation beyond single-domain analyses, aligning with broader digital health literature emphasizing that healthcare transformation is driven by not only technological advancement but also the integration of technological, organizational, and social-ethical dimensions as interconnected domains.29,30
By mapping vulnerabilities to specific pathway interfaces, this study advances a pathway-oriented sociotechnical perspective that specifies where and how governance misalignment manifests within routine hybrid care processes.
Telemedicine challenges as sociotechnical misalignment
Consistent with implementation research, sustained telemedicine use seemingly depends more on organizational alignment, workflow compatibility, and institutional coordination than on clinician attitudes alone.6,9 While clinician perceptions were generally favorable, vulnerabilities emerged from interactions among platform design, workflow structure, and governance arrangements.
Extending NASSS-based evaluations, these findings reveal how adoption, scale-up, and sustainability challenges arise from interacting complexities across technological, organizational, and regulatory domains. 31 Telemedicine implementation therefore reflects coordination failures across domains rather than deficits in technology acceptance.
This interpretation is consistent with prior studies, which reveal that digital transformation in healthcare is contingent on organizational capability and leadership alignment, particularly in resource-constrained settings, where institutional readiness and leadership support shape implementation outcomes. 32 At the institutional level, leadership perceptions of digital capability have been shown to directly influence the quality of patient-centered care, with leadership support for digital adoption and availability of trained ICT personnel identified as the most significant contributing factors in lower-resource hospital settings. These findings suggest that sociotechnical misalignment is not solely a technological issue but also reflects gaps in cross-level governance and organizational coordination.
These patterns should be interpreted in the context of the South Korean healthcare system, which is characterized by high accessibility under a universal national health insurance scheme alongside structural concentration of patients and resources in large tertiary hospitals. 2
In particular, prior studies have documented regional differences in not only healthcare access and utilization but also the concentration of specialized care in major hospitals, which may contribute to the uneven access pathways and patient flow patterns observed in telemedicine settings. 2
Pre-visit preparation and information continuity
Insufficient pre-visit preparation emerged as a critical determinant of downstream care quality. Both physicians and patients described limitations in the completeness and usability of pre-consultation information, echoing evidence that inadequate pre-consultation information increases clarification burdens and contributes to diagnostic uncertainty during time-limited encounters.18,33
From a sociotechnical perspective, pre-visit preparation represents a structural interface between patient-generated data and clinician interpretation. Structured information exchange and communication maturity appear foundational to digital health system capability and implementation effectiveness. 30
In addition, consumer-oriented research on telehealth services has identified service quality and accessibility as primary determinants of user satisfaction and engagement, with innovation emerging as a key pathway through which service challenges are translated into improved care experiences. 34 Our findings extend this literature by demonstrating that such perceptions are not only user-level experiences but are shaped by structural misalignments in information continuity across care settings.
Accessibility as a cross-cutting system property
Accessibility-related vulnerabilities were evident across all stages, particularly among patients with disabilities. Exclusion risk extended beyond dissatisfaction to the functional inability to engage with digital systems, consistent with quantitative evidence linking frailty and socioeconomic deprivation to reduced telemedicine access. 15
Qualitative syntheses further indicated that equitable telemedicine delivery requires workflow adaptation, supportive infrastructure, and organizational redesign rather than reliance on technology alone.16,19,35,36 Our findings underscore the need to conceptualize accessibility not as an individual trait but as a system-level design property intersecting multiple stages of care.
This interpretation is consistent with research on the digital health divide, which demonstrates that disparities in telemedicine access arise from structural factors—including infrastructure, policy environments, and community capacity—rather than from individual-level limitations. 37 By situating accessibility within a pathway-oriented framework, this study highlights how exclusion is produced and reinforced across interconnected stages of care.
Post-consultation workflows, reimbursement, and sustainability
Post-consultation processes—including prescription transmission, medication access, and follow-up—represented areas of heightened vulnerability. Although meta-analyses demonstrate that telemedicine can significantly reduce outpatient waiting times, 38 they primarily assess access metrics, overlooking coordination processes beyond the initial consultation.
Weaknesses in post-consultation workflows and reimbursement alignment may constrain the sustainability of telemedicine integration. 12 Reimbursement structures and payment models shape how telemedicine is positioned within care delivery, influencing its use for follow-up versus first-contact encounters.12,39
Legal analyses further demonstrate that fragmented accountability structures and ambiguous professional qualification standards can amplify governance-related risks in telemedicine systems. 40 Emerging AI-driven capabilities—including predictive analytics, automated triage, and remote monitoring tools—serve as potential pathways to address coordination gaps and extend service reach in resource-constrained settings, although their implementation introduces additional ethical and regulatory considerations that must be managed alongside governance reform. 37 Sustainable telemedicine delivery therefore depends on managing cross-domain complexity and aligning technological, organizational, financial, and regulatory domains over time. 31
Implications for pathway-oriented evaluation frameworks
Recent evaluation frameworks emphasize multi-domain, stakeholder-informed assessment in telehealth, with some incorporating developmental staging approaches.5,41 A Delphi-based telemedicine implementation framework similarly identifies multi-level constructs spanning clinical, technological, regulatory, economic, and monitoring domains. 42
However, many frameworks lack telehealth-specific operationalization and provide limited guidance on how implementation and equity challenges unfold in routine care settings,36,43 while evaluation models often remain fragmented or narrowly scoped. 44 By contrast, this study integrates multiple domains—technological, organizational, experiential, and policy-related—within a single pathway-oriented framework, complementing prior research on consumer experience, organizational leadership, and digital health equity by demonstrating how these dimensions interact dynamically rather than in isolation across sequential stages of care. This has direct implications for policy design, platform development, and clinical workflow integration at each stage of the care pathway.32,34,37
Limitations
This study has several limitations. First, it did not include hospital administrators or other meso-level actors, which limited direct examination of organizational governance and decision-making processes. This reflects the study’s intentional focus on the interaction between micro-level clinical practice and macro-level policy contexts, aimed at identifying process-level vulnerabilities in telemedicine care pathways. Although institutional factors were indirectly captured through physician accounts, future studies should incorporate meso-level stakeholders to provide a more comprehensive understanding of governance fragmentation across system levels.
Second, the sample size was modest and participants were recruited through professional networks and a research agency using prior telemedicine experience as a screening criterion. This approach may have introduced selection bias toward individuals with greater familiarity or engagement with telemedicine, potentially underrepresenting the perspectives of those with limited access or lower utilization. In addition, the inclusion of only a small number of patients with disabilities limits subgroup-specific insights, although these participants were included as information-rich cases to identify accessibility-related vulnerabilities. Future research should employ purposive sampling strategies that deliberately recruit underrepresented populations—such as individuals with limited digital access and those across a broader range of disability types—and adopt larger, multi-site designs to strengthen the transferability of findings.
Third, patient data were collected through two FGDs with heterogeneous participant composition, which may have introduced group dynamic effects such as the dominance of certain participants or convergence of views. Although moderation strategies were applied and individual-level analysis was conducted, some influence of group interaction is inevitable. Future research could incorporate complementary individual interviews or stratified focus groups with more homogeneous participant characteristics to reduce group dynamic effects and enrich the depth and diversity of perspectives. In addition, participant checking (member checking) was not conducted, which may limit the extent to which the interpretations were validated by participants.
Fourth, variability across telemedicine platforms and institutional workflows was not examined as an independent analytic dimension. Given that participants reported heterogeneous experiences across platforms, differences in platform design, interface functionality, and system integration may have contributed to the observed workflow fragmentation and access variability. Future studies should systematically compare platform-level characteristics and their impact on care processes.
Finally, as is common in qualitative research, the findings are not intended for statistical generalization and reflect a specific institutional and regulatory context. In particular, the governance challenges identified in this study are closely tied to South Korea’s evolving telemedicine policy environment and hybrid implementation model. Caution is therefore warranted when transferring these findings to other national contexts with different regulatory environments, healthcare infrastructure, and platform governance models. Nevertheless, the pathway-oriented sociotechnical framework may offer analytic relevance to telemedicine settings with similar hybrid care structures, consistent with prior studies.6,18,36,45
Conclusion
Telemedicine implementation in hybrid care settings should be understood not simply as technology adoption but as sociotechnical alignment across interconnected stages of care. This study demonstrates that responsibility ambiguity, workflow discontinuity, technological constraint, and governance fragmentation accumulate across appointment, consultation, prescribing, and follow-up processes, resulting in system-level uncertainty rather than isolated operational failures. By conceptualizing telemedicine as a longitudinal hybrid pathway, the findings clarify where and how cross-domain misalignment emerges in routine care. Strengthening telemedicine integration therefore requires coordinated attention to workflow design, information continuity, equitable access, and reimbursement alignment within broader institutional structures.
These findings contribute to digital health research by shifting analytic attention from individual-technologies toward system-level integration and process-based governance. They suggest that digital health interventions may be more effective when explicitly aligned with existing care pathways and institutional arrangements, and that cross-stage coordination—encompassing data interoperability, accountability frameworks, and access equity—represents an important consideration for context-sensitive implementation.
Supplemental material
Supplemental material - Governance fragmentation and sociotechnical misalignment in hybrid telemedicine care pathways: A qualitative study
Supplemental material for Governance fragmentation and sociotechnical misalignment in hybrid telemedicine care pathways: A qualitative study by Ah-Ram Sul, Eu Sun Lee, Jieun Ju, Seongwoo Seo, Min-Woo Jo, In-Hwan Oh in DIGITAL HEALTH.
Supplemental material
Supplemental material - Governance fragmentation and sociotechnical misalignment in hybrid telemedicine care pathways: A qualitative study
Supplemental material for Governance fragmentation and sociotechnical misalignment in hybrid telemedicine care pathways: A qualitative study by Ah-Ram Sul, Eu Sun Lee, Jieun Ju, Seongwoo Seo, Min-Woo Jo, In-Hwan Oh in DIGITAL HEALTH.
Footnotes
Acknowledgments
The authors sincerely thank all participants for sharing their experiences and insights during the interviews and focus group discussions.
Ethical considerations
This study was approved by the Institutional Review Board of the National Evidence-based Healthcare Collaborating Agency (NECAIRB 25-019), Seoul, Republic of Korea.
Consent to participate
All participants were informed about the purpose and procedures of the study. Written informed consent was obtained from all participants prior to data collection.
Author contributions
Conceptualization: In-Hwan Oh. Methodology: In-Hwan Oh, Ah-Ram Sul. Investigation: In-Hwan Oh, Ah-Ram Sul, Jieun Ju, Seongwoo Seo. Data curation: Ah-Ram Sul, Jieun Ju, Seongwoo Seo. Formal analysis: Ah-Ram Sul, Jieun Ju, Seongwoo Seo. Interpretation: In-Hwan Oh, Eu Sun Lee, Min-Woo Jo. Writing – original draft: Ah-Ram Sul. Writing – review & editing: All authors. Project administration: Ah-Ram Sul, Jieun Ju. Supervision: In-Hwan Oh
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Evidence-based Healthcare Collaborating Agency, Republic of Korea (Grant No. NECA-A-2025-017).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality considerations but are available from the corresponding author on reasonable request.
Disclaimer
Portions of this manuscript were prepared with the assistance of AI language tools, including ChatGPT (OpenAI, GPT-5.2), Claude (Anthropic, Claude Sonnet 4.6), and Gemini (Google, Gemini 3 Flash) for language editing and structural refinement. All analyses, interpretations, and conclusions were developed and verified by the authors, who take full responsibility for the content of this manuscript.
Supplemental material
Supplemental material for this article is available online.