
Abstract
Introduction
Alcohol use disorder (AUD) is a severe medical problem that affects ethnic minority young adults. An internet-based self-help program integrating acceptance and commitment therapy (ACT) and behavioral activation (BA) was found promising. However, such integration has never been applied to people with AUD. Therefore, developing and testing this integration was warranted.
Objectives
This study aimed to develop and test an internet-based self-help program integrating ACT and BA among ethnic minority young adults with AUD.
Method
Four distinct phases were employed, including preparing self-help intervention content, expert panel review, developing an online intervention using Qualtrics, and usability testing. A total of 10 ethnic minority young adults with AUD were recruited for the usability test. Descriptive statistics and a one-sample t-test were employed to determine usability.
Result
A total of 10 participants were invited to participate in the study, with a completion rate of 90%. The overall usability score was 74.72 (SD = 4.75). About 88.9% of participants found the intervention helpful, easy to navigate, and clear content and instructions. Participants spent about 10–30 minutes per module. Almost all participants received one reminder per module for completion. However, three participants experienced device incompatibility, internet interruptions, and login failures.
Conclusion
A new internet-based self-help ACT-BA intervention was developed and tested. The findings showed an excellent usability score. Future interventions will consider simple plain language over technical terms and incorporate withdrawal symptom management. Besides, conducting a brief session during recruitment to guide participants and sending a reminder, especially on holidays and weekends, is warranted.
Keywords
Introduction
AUD is a significant global health concern, which is particularly prevalent in developed countries due to the affordability, accessibility, and aggressive marketing of alcohol. 1 Although the prevalence of AUD varies across different demographics, including age, race, gender, and culture, all populations are at risk of developing the disorder.2–4 A US epidemiological study highlights a rapid rise in AUD prevalence from 8.5% to 17.7% in the total population between 2001-2002 and 2012-2013. During this period, a significant increase was observed among ethnic minorities (rose by 92.8% in Black individuals, 51.9% in Hispanic individuals, 83.7% in women, and 200% for poor people). 5 Similarly, a study in Hong Kong showed the overall prevalence of AUD among ethnic minorities was 19.8%, with 7.9%, 5.4%, and 6.4% for mild, moderate, and severe AUD, respectively. 6 Recent studies also indicate that young ethnic minority populations are especially vulnerable to substance use, including alcohol, due to various reasons, such as relaxation, socialization, mood enhancement, stress relief, and coping with negative emotions.2,7,8 Likewise, these populations often experience discrimination, stigma, and marginalization in areas such as employment, education, and social activities, leading to acculturation stress, depression, isolation, and life dissatisfaction,9–11 which places them at risk of AUD. 12 Importantly, a recent study found that only 4% of ethnic minority college students received treatment for AUD, potentially due to a lack of culturally tailored treatments, isolation, work burden, and language barriers. 13
In this regard, our research team has done a number of studies to address AUD in ethnic minority young adults in Hong Kong.14,15 Our cross-sectional study identified male gender and the age range of 18 -35 as contributing to AUD in this population group. Likewise, despite acculturation leading to challenges to ethnic minorities, it is a golden opportunity for alcohol abstinence, given that the ethnic minorities are geographically away from the parental influence, which was confirmed to be one of the significant factors contributing to AUD.16,17 Besides, the experience of discrimination and avoidance coping behaviours were shown to be significant factors contributing to AUD. 18 These highlight that the future of interventions for AUD should address these two components, thus assisting ethnic minorities with AUD to achieve alcohol abstinence.
A comprehensive review of the literature indicated that acceptance and commitment therapy (ACT) may be a viable treatment option for ethnic minority young adults with AUD. ACT, as a third wave of cognitive behavioral therapies, aims to assist individuals to achieve a meaningful life that aligns with their life goals through accepting inevitable pain and suffering.19–21 This intervention directly addresses the inevitable nature of discrimination and the use of avoidance coping behaviours in ethnic minorities with AUD. In fact, a systematic review and meta-analysis have already confirmed the effectiveness of ACT for addictive behaviours, despite only two included studies focusing on alcohol use. 14 Another comprehensive literature review regarding the effectiveness of ACT on AUD also suggested that it was a viable treatment option.22–27 Although ACT is a viable treatment option for AUD, a comprehensive literature review highlighted a substantial problem with participants’ engagement and adherence to the intervention.26,28,29 In this review, many participants exhibited low engagement and adherence to the value-based activities that guide them to commit actions toward a meaningful life.26,28 The low engagement and adherence may arise from a failure to identify enjoyable, rewarding, and positively reinforcing activities. Apart from the engagement issue, ACT primarily focuses on internal experiences such as negative emotions, thoughts, sensations, and memories, with insufficient attention to overt behaviors. Therefore, individuals may not have sufficient skills to manage the high-risk situations for drinking, notwithstanding that they understand that they should not use drinking as a coping method, resulting in high likelihoods of relapse and limited behavioural change. Besides, ACT lacks mechanisms to guide individuals in self-monitoring their daily activities and scheduling alternatives to replace drinking in their lives. However, these are critical challenges for ethnic minorities with AUD, as our previous qualitative study revealed that a substantial number of ethnic minorities with AUD attempted various coping strategies in quitting, but their engagement in alcohol-free activities remained a significant problem because they had no structured daily planning and monitoring skills, and experienced difficulties in identifying and engaging with enjoyable alcohol-free activities. As a result, participants’ efforts to quit were unsuccessful, although some managed to quit briefly; they eventually relapsed. Given the above, new strategies are needed to be incorporated into ACT to address these limitations, with an aim to enhance participants’ engagement and adherence to the intervention.
Behavioural activation (BA) may be a possible method to overcome the aforementioned limitations. BA is a concept from behaviourism that states behaviour can directly affect emotions, for better or worse.30,31 Particularly, BA is guided by operant conditioning, which states that participants’ behavior and mood are mainly maintained through their environment.
32
When they experience barriers like stress, craving, stigma, and discrimination, they often withdraw from the environment, leading to loss of reinforcement.
33
Regarding AUD, alcohol often becomes the primary negative reinforcer.
33
In this regard, BA breaks the cycle of avoidance through enhancing alternative alcohol free, reinforcing, and rewarding activities that provide positive reinforcement. Hence, individuals can put themselves in a situation that is likely to foster positive emotions. For example, a positive event such as listening to uplifting music can lead to happiness, and vice versa. BA is a widely recognized and theoretically sound approach that has been applied to treat depression.34,35 Its application has been extended to substance use disorders (SUD) via providing rewarding experiences in daily life different from substance use, thus achieving abstinence and preventing relapse.36–38 Evidence suggests that BA is a promising intervention for SUD as a standalone treatment or being integrated with other therapeutic modalities. The emphasis on rewarding experiences in BA exactly addresses the low engagement and adherence of ACT due to the failure of identifying enjoyable, rewarding, and positively reinforcing activities in the intervention process. In addition, BA involves two major techniques, which are self-monitoring daily activities and scheduling, allowing individuals to monitor their usual daily activities and alcohol use, and develop a plan to schedule their identified alcohol-free rewarding activities to replace drinking in their lives. Because of the distinctive benefits of BA, it appears to be a treatment component complementary to the shortcomings of ACT, thus enhancing the intervention effectiveness if they both are integrated into the treatment protocol. Also, behavioural activation is a brief intervention (i.e., simple, cost-effective, and short-term) that can be delivered within 4 weeks, with a total duration of less than 90 minutes,
39
which will not significantly prolong the duration of each intervention session, ensuring the participants’ adherence and engagement. In sum, ACT simply encourages an individual to ACT, which includes
Concerning the mode of delivery of the intervention, an online mode may be a more favourable option for ethnic minorities with AUD than face-to-face formats due to its improved accessibility and availability, reduced stigma, and non-interference with daily activities and work.41–43 This idea is further supported by the widespread international development of websites and online technology for screening and initial counselling for alcohol use issues in the past decade, especially after the COVID-19 pandemic.44,45 A review of 41 articles involving more than 50000 participants has shown that web-based interventions were more effective in reducing alcohol consumption as compared to non-web-based interventions or no intervention in adults, notwithstanding that none of the included articles were from Eastern countries, including China. 46
Although BA has been integrated into ACT to manage different conditions, mainly delivered in a face-to-face format, 37 which is an important omission in the literature, given the benefits of web-based interventions to addictive behaviours, no such integration was applied among ethnic minority young adults with AUD. To address this gap in existing literature, our research team aimed to develop an internet-based self-help program integrating ACT and BA intervention for young adult ethnic minorities with AUD in Hong Kong. Before a large-scale RCT, evaluating this new intervention protocol with the end users is crucial to improve and revise the intervention. In this regard, usability testing is a key component of the intervention development. Usability testing can improve participant engagement by tailoring navigation and content to the needs and preferences of participants. Therefore, this study was a proof of concept which aimed to design an internet-based self-help ACT-BA intervention and test its usability among Hong Kong ethnic minority young adults with AUD.
Methods
This study was reported in accordance with the GUIDE reporting checklist. The completed checklist is provided as a Supplementary file 1.
Procedures for intervention development
The development of the intervention for ethnic minority young adults with AUD involved four distinct phases before the actual implementation of the protocol. These phases were: (1) preparation of self-help intervention content; (2) expert panel review; (3) development of the online intervention using the Qualtrics platform; and (4) usability testing. The usability test was conducted cross-sectionally, using direct observation of application navigation tasks and a quantitative self-administered questionnaire to identify areas of improvement.
Phases of intervention development
Phase 1: Preparation of self-help iACT-BA intervention content
Modules and content of interventions
Two authors (GMB and KYH) have developed the self-help iACT-BA intervention protocol. The intervention content was adapted from the ACT manual,47,48 self-help protocols, 28 and behavioral activation treatment for substance use and depression.37,38
The intervention components were drawn from the ACT manual, which includes six core ACT components47,48: (1) Acceptance; (2) Cognitive delusion; (3) Being present; (4) Self as context; (5) Values; and (6) Committed action. Additionally, Behavioral Activation (BA) components such as daily activity monitoring, activity scheduling, daily plans, and post-treatment plans were incorporated. The content was validated, and the maximum number of sessions was determined based on available literature. Participants or end users of the session were ethnic minority young adults with AUD. Each participant engaged in six sessions, with one module per week over six weeks. The integrated intervention (Self-help iACT-BA) was delivered in the following sequence: (1) introduction, confronting agenda, and daily monitoring; (2) values and activity scheduling; (3) acceptance and diffusion; (4) being present and observing self; (5) daily plans and committed action; (6) relapse prevention and plan. The participant accessed modules every week and completed assignments within the designated time.
Session 1: Introduction, confronting the agenda, and daily monitoring
In this session, participants were introduced to the objectives of the intervention, treatment rationale, and concept of experiential avoidance behaviors, which included unpleasant emotions, negative feelings, thoughts, stress, cravings, and urges. 49 Using texts, pictures, videos, and metaphors, participants would learn about the negative impact of avoidance behaviors related to alcohol consumption on various life domains, such as family, health, work, social life, and community. For instance, participants practiced the “dropping the struggle” metaphor and engaged in the “pushing away paper” exercise to understand how being hooked with negative emotions and cravings could affect them, and unhooking led them towards their life goals.
Participants were also encouraged to explore their past negative events, coping strategies, and the outcomes of these strategies, whether they provided long-lasting benefits or only temporary relief. Concurrently, participants were asked to identify and monitor their daily activities. They were required to list alcohol-free activities they currently and/or previously engaged in (e.g., taking a walk, spending time with family, playing football) and to evaluate their feelings about these activities using a daily activity monitoring form. This process helped them identify the most important and enjoyable activities.
Participants rated their activities based on enjoyment and importance on a scale from one to ten. This exercise helped identify low-rated activities as opportunities to replace them with more rewarding, value-driven alternatives. By engaging in these rewarding and alcohol-free activities, participants might better manage negative emotions and urges.
Session 2: Values and activity scheduling
In the second session, participants learned about their own values and life areas and how to schedule activities that aligned with their values. They assessed whether their current activities reflected the core values that could lead them to a more meaningful life. Short-term behavioral treatment goals, linked to the participant’s values, were developed to guide future behavioral activation efforts. Participants were asked to identify new value-driven activities to incorporate into their daily schedules across various life domains. They identified at least one value in each chosen life area. Participants were introduced to “value-driven activities,” defined as behaviors that aligned with their values, and they scheduled these newly identified activities. They used the value identification inquiry sheet and the Bull’s Eye tool to identify at least one value and schedule value-congruent activities.
Session 3: Acceptance and cognitive defusion
While practicing value-congruent activities, participants might encounter difficulties due to negative thoughts, emotions, cravings, and urges. In this session, participants learned acceptance and cognitive defusion skills. The concepts of acceptance and cognitive defusion, along with various experiential exercises, paradoxes, and metaphors, were explored. Once participants identified negative emotions, urges, and thoughts that led them to drink and affect their daily activities, they practiced acceptance and defusion skills and mindfulness exercises. These skills helped them accept negative thoughts and defuse negative emotions, urges, and cravings. They learned acceptance techniques by (1) allowing feelings, urges, and thoughts to occur without acting on them, (2) recognizing their strengths while acknowledging shortcomings, and (3) facing difficulties without avoidance. They also learned defusion skills by understanding that thoughts were transient and that impulsive thoughts about drinking were not necessarily facts.
Session 4: Being present and observing self
In addition to acceptance and defusion skills, participants learned mindfulness skills to be aware of the present moment and what was happening inside and outside their bodies. They engaged in exercises and metaphors for managing negative emotions, thoughts, cravings, urges, and memories related to past or future events that contributed to alcohol addiction. Participants also learned self-observation skills, understanding that there were parts of them that could think, feel, notice, and observe their urges, cravings, thoughts, and feelings toward alcohol use. They accessed mindfulness exercises to notice private events and used the ‘Sky and Weather’ metaphor for self-observation, introduced through video, audio, and written scripts.
Session 5: Daily plans and committed action
In this session, participants learned how to plan activities and take committed actions toward their life goals. They identified new relevant values and activities and integrated them into their daily lives. They learned to develop SMART goals and created their own life goals. Through practice, participants developed planning skills to schedule specific activities aligned with their daily values. They were encouraged to plan alcohol-free activities. In their daily plans, they scheduled value-driven activities. At the end of each day, they recorded the number of planned activities completed and rated the importance and enjoyment of each activity. The main goal of this practice was to establish regular engagement with rewarding activities, helping them identify new positive experiences and maintain involvement after treatment.
Session 6: Relapse prevention and planning
The final session focused on the post-treatment plan. Participants learned about the recovery process and relapse prevention, with a particular focus on preventing relapse and post-intervention planning. Previous sessions were reviewed, and another long-term goal congruent with their values was developed. Finally, participants were asked to develop a clear post-treatment plan based on their preferences and clinical significance.
Phase 2: Expert panel review
A local expert panel including two associated professors with numerous experiences in research in child and adolescent health and delivery of different psychosocial interventions, particularly ACT, an assistant professor with experiences in research of addiction and substance abuse, and three social workers in an NGO providing services for ethnic minorities in Hong Kong reviewed the appropriateness of the intervention, in relation to six items, i.e., (1) its relevance to the study objective; (2) relevancy of content; (3) accuracy; (4) meaningfulness; (5) comprehensiveness; and (6) ease of understanding by ethnic minority young adults. Each item was rated on a 4-point Likert-type scale ranging from 1 (irrelevant/inaccurate/incomprehensive/not meaningful/difficult to understand) to 4 (relevant/accurate/comprehensive/meaningful/easy to understand).
Phase 3: Development of an online platform for intervention delivery
Our intervention was delivered using Qualtrics, a secure and versatile platform designed for web-based survey development. This platform provides a cost-effective and efficient means for self-help interventions, significantly minimizing the need for extensive technical expertise, high development costs, and the time typically associated with creating web-based programs. Although Qualtrics is primarily designed for survey administration, it offers a range of essential features that are often expensive to implement on secure and stable websites. These features include various interactive question formats, database integration for tracking user behavior, the ability to customize information and carry data forward within a session, and reliable performance across multiple browsers and devices, including mobile platforms. If this approach is acceptable to participants, it presents a feasible option for researchers to deliver interventions using an online format at minimal or no cost.
The Qualtrics interface was carefully designed to facilitate easy access to information, interventions, and questionnaires for participants. A key aspect of this design was its shallow hierarchy and use of explicit labels, which enhanced navigability.
Phase 4: Usability test
The System Usability Test (SUT) was conducted before implementing the intervention with the target audience. The SUT is a method used to evaluate how effectively and efficiently users can interact with the internet-based interventions. It focuses on understanding user experiences, identifying usability issues, and collecting feedback to improve the overall design and functionality of the system. The objective of this usability testing was to assess the system’s ease of use, identify any usability problems that might affect user interaction, and evaluate user satisfaction.
Eligibility criteria
Participants for this usability testing were Hong Kong ethnic minority young adults aged 18 to 35 who can read, write, and speak English. Ethnic minorities in this age range were chosen as it aligns with the US Census Bureau classification for young adults [84], and this age group is highly vulnerable to substance use disorders [85]. According to the Hong Kong Department of Census and Statistics, ethnic minorities refer to persons who reported themselves as being of non-Chinese ethnicities in the population census. 50 They had to voluntarily participate, have internet-accessible devices, and meet the DSM-5 criteria for AUD. 51 According to the DSM-5, participants exhibiting at least two of the following symptoms were considered to have AUD. 52 The symptoms included: (1) Using alcohol in larger amounts or over a longer period than you intended; (2) Wanting to cut back on alcohol or making unsuccessful attempts; (3) Spending a great deal of time finding, using, or recovering; (4) Strong urges or cravings to use alcohol; (5) Use of alcohol that resulted in your inability to meet your obligations at work, home, or school; (6) Cut back on or abandon social, professional, or recreational activities due to your use of alcohol; (7) Repeatedly using alcohol when it was hazardous to do so; (8) Social or relationship problems due to your use of alcohol and kept using anyway; (9) Kept using alcohol knowing that it has caused physical or mental health issues; (10) Experienced uncomfortable physical or mental health symptoms (withdrawal); and (11) Diminished effects when you used alcohol compared to the past.
Sample size determination
Based on previous literature, at least five participants can provide adequate data to test the system usability. 53 Therefore, we recruited ten ethnic minority young adults with AUD for the system usability test.
Study setting, recruitment, and data collection
Using a convenience sampling technique, the study participants were recruited from bars in Chung King Mansion and Tsim Sha Tsui. These locations were chosen because it was easy to find target groups, as many ethnic minority young adults often gather there. Participants were provided with comprehensive information about the study. Their contact details, such as email, WhatsApp, or telephone numbers, were collected to receive an electronic invitation, which included a questionnaire to collect sociodemographic information, and the SUT with open-ended questions. Participants received a link to access a website with their usernames and passwords. If there was no response within one week after the invitation, reminders would be sent via email or SMS. Upon accessing the website, participants would be able to engage with the information, intervention modules, and questionnaires. They will be instructed to go through the intervention modules sequentially. Then, participants were asked to complete the SUT and provide comments for the open-ended questions. Recruitment and data collection were done from October 18 to December 31, 2024.
Measurement
A self-administered questionnaire was delivered to all participants to evaluate each module in terms of navigation, content clarity, instructions, ease of use, and module presentation. Participants responded to questions and could provide suggestions for the modules (Supplementary file 2).
System usability scale
The System Usability Scale (SUS) is a widely utilized 10-item measure designed to evaluate website usability, including aspects such as ease of navigation and user satisfaction.
54
This scale has a proven psychometric measurement, including validity and reliability.
55
The internal consistency of items in the previous study showed a Cronbach’s alpha of 0.86 55. Participants responded using a 5-point Likert scale, ranging from “strongly disagree” to “strongly agree.” The SUS score was calculated using the formula below (EQ 1),
56
where Un refers to the rating of the nth question (Supplementary file 2). The SUS scores ranged from 0 to 100, with higher values suggesting higher user satisfaction. This score was compared with a cut-off of 70, a previously established metric.
56
The scores were then rated as follows: scores <25 = worst imaginable; 25 to 39.17 = poor; 39 to 52.5 =median; 53 to 73.5 =good; 74 to 85.5 =excellent, and 86 to 100 = best imaginable/possible.
56

Data analysis
The authors checked, cleaned, and verified the data. Then, they imported the data into SPSS version 26 for analysis. Descriptive statistics were used to report the demographic characteristics of the participants, with mean and standard deviation for continuous variables and frequency and proportion for categorical variables, and median and interquartile range for non-normally distributed data. A one-sample t-test was conducted to determine whether the mean SUS score differed from the established metrics.
Ethical consideration
Ethical approval was obtained from the Human Subjects Ethics Sub-Committee of Hong Kong Polytechnic University (reference number: HSEARS20240712003). The protocol was registered on ClinicalTrials.gov under the National Clinical Trial number NCT06779006. Informed written consent was taken from each participant. They were informed about their right to decline or leave the study at any time. All data obtained from each participant was kept confidential in a non-identifying way.
Result
Phase 1: Preparation of self-help iACT-BA intervention content
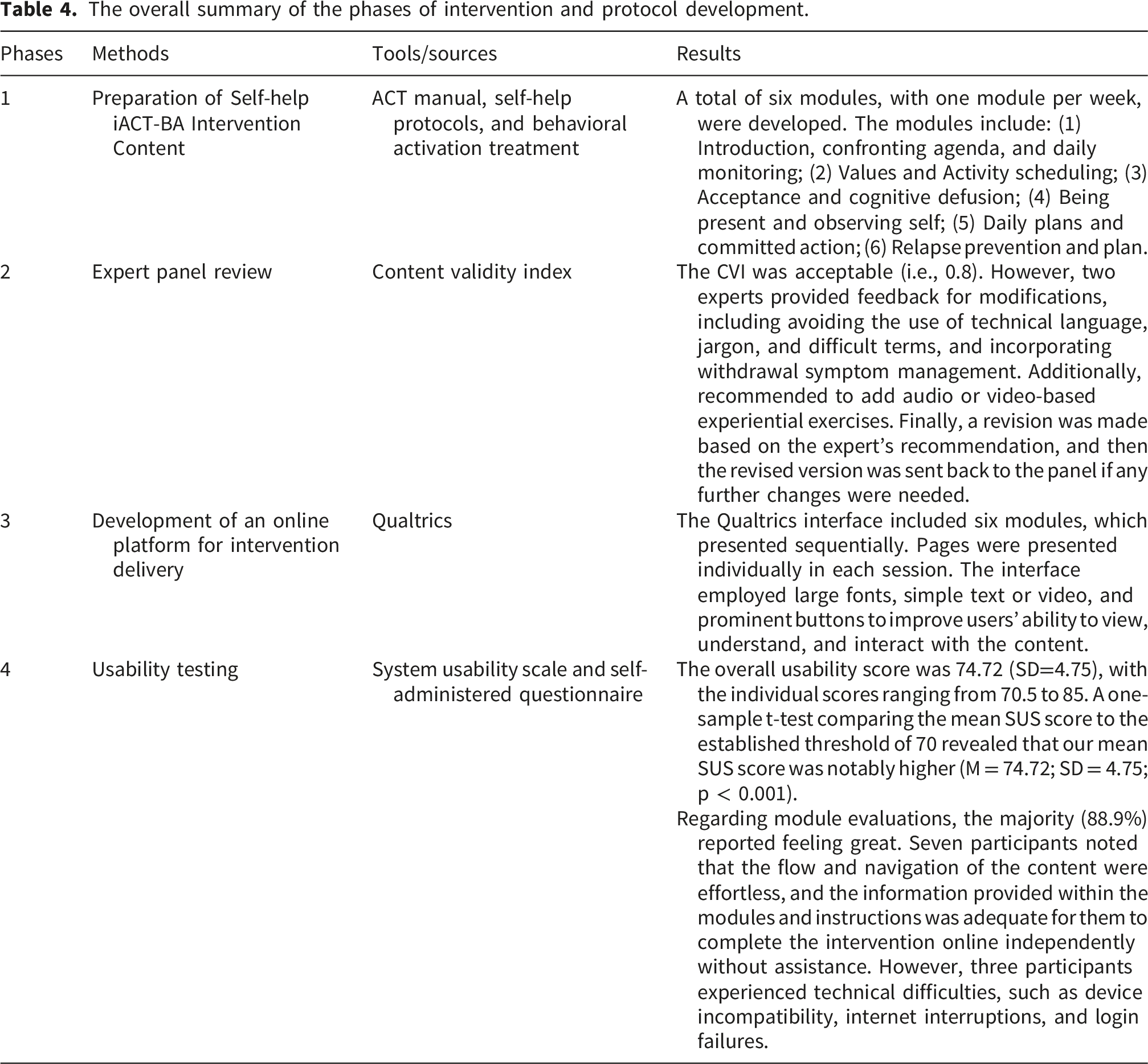
A total of six sessions, with one module per week, were delivered to ethnic minority young adults with AUD. The modules included: (1) introduction, confronting agenda, and daily monitoring; (2) values and activity scheduling; (3) acceptance and diffusion; (4) being present and observing self; (5) daily plans and committed action; (6) relapse prevention and plan.
Phase 2: Expert panel review
The overall CVI was above the acceptable threshold (i.e., 0.8). However, two experts provided feedback for modifications, including avoiding the use of technical language, jargon, and difficult terms throughout the protocol, and incorporating withdrawal symptom management in the first session. Additionally, they recommended that audio or video-based experiential exercises should be used to make the content easier for participants to understand. Finally, a revision was made based on the expert’s recommendation, and then, the revised version was sent back to the panel if any further changes were needed.
Phase 3: Development of an online platform for intervention delivery
The Qualtrics interface included six modules, which presented sequentially. This sequential approach ensured that users fully comprehended one segment of information before advancing to the next. Pages were presented individually in each session. Moreover, the interface employed large fonts, simple text or video, and prominent buttons to improve users’ ability to view, understand, and interact with the content. To minimize distractions, the design intentionally excluded advertisements and moving content.
Phase 4: Usability testing
Sociodemographic characteristics
Sociodemographic characteristics of Ethnic minority young adults with AUD (n=9).
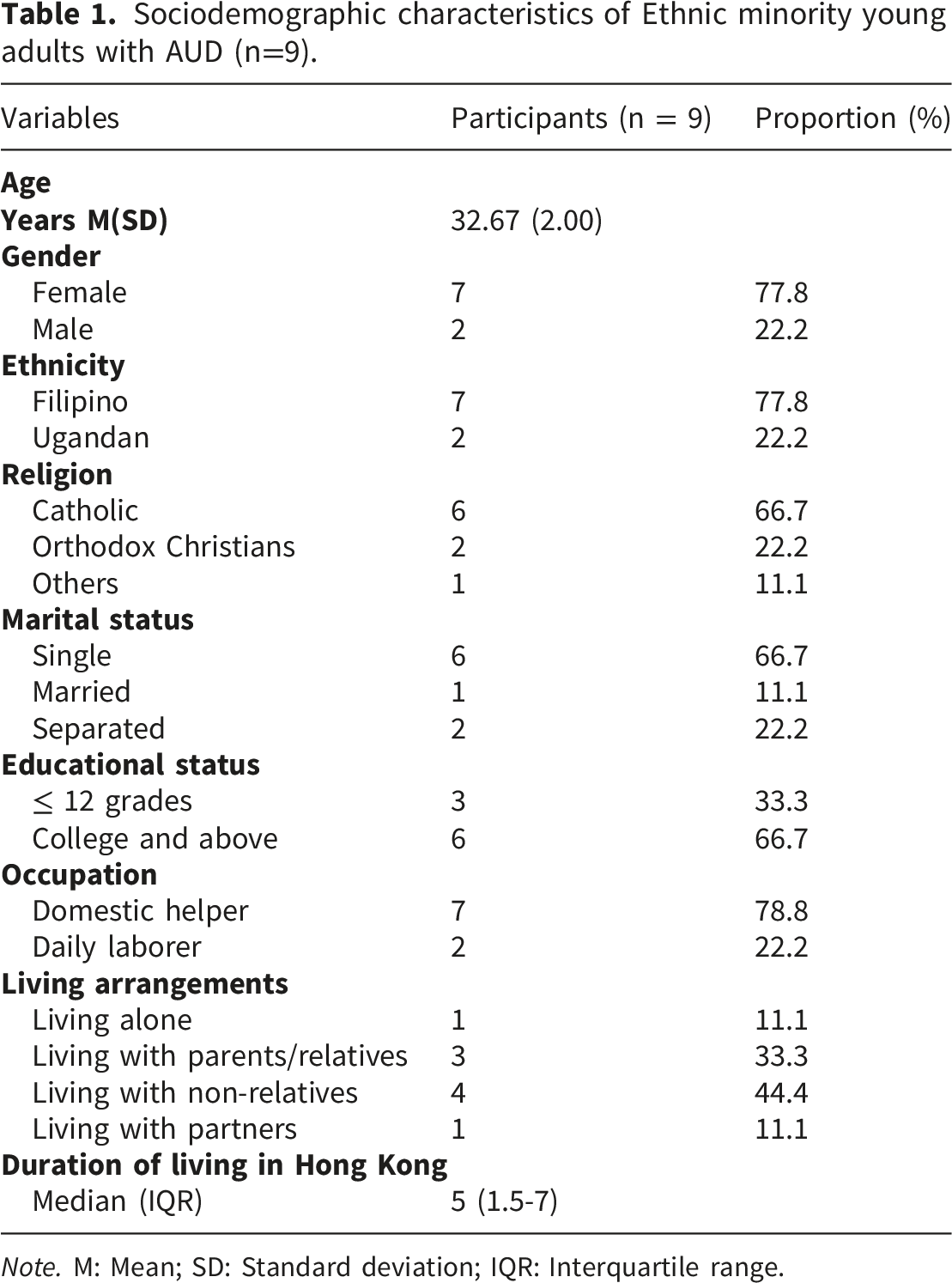
Note. M: Mean; SD: Standard deviation; IQR: Interquartile range.
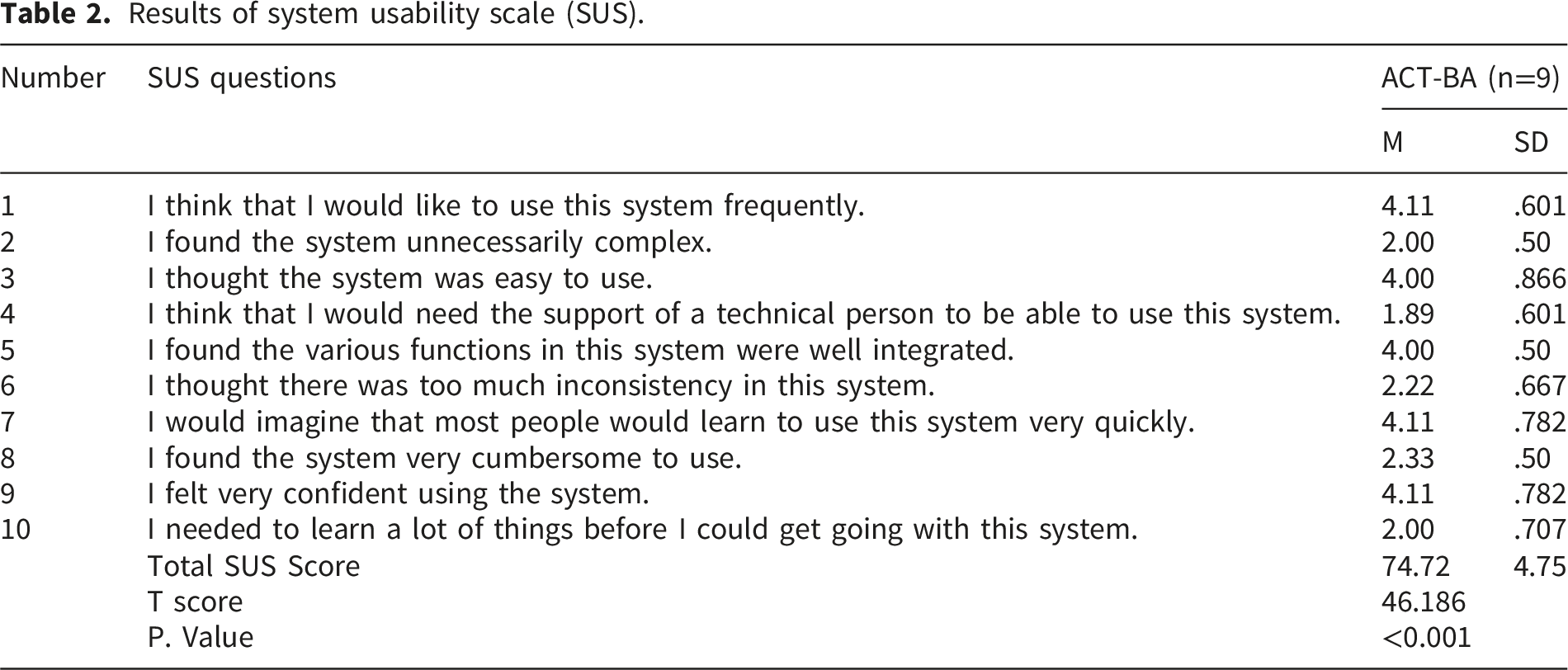
System usability scale (SUS) score
Results of system usability scale (SUS).
Module evaluations
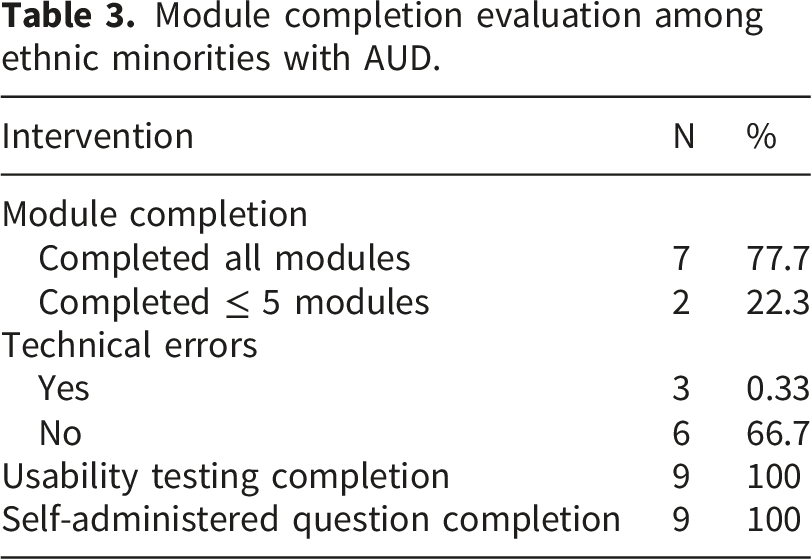
A total of nine participants completed a self-administered questionnaire that collected their feedback on the internet-based self-help intervention. The majority of them (88.9%) reported feeling great about the intervention, stating that it was useful to assist them in quitting alcohol. Additionally, seven participants noted that the flow and navigation of the content were effortless, and the information provided within the modules and instructions was adequate for them to complete the online intervention independently without assistance. However, three participants experienced technical difficulties, such as device incompatibility, internet interruptions, and login failures.
Module completion evaluation among ethnic minorities with AUD.
The overall summary of the phases of intervention and protocol development.
Discussion
A significant number of ethnic minorities are affected by AUD. A few of the major reasons were acculturation stress, avoidance behaviour, stigma, and discrimination. To address these reasons, ACT-BA was found as a viable option. Before the pilot and full-scale RCT to examine the feasibility and effectiveness, usability testing is a key component for the intervention development. Therefore, this proof-of-concept aimed to develop and test the usability of a web-based self-help ACT-BA intervention for ethnic minority young adults with AUD in Hong Kong. The findings provide us with valuable information to identify areas of improvement to finalize the intervention.
In phase 1, two authors have developed a protocol from different sources, including the ACT manual,47,48 self-help protocols, 28 and behavioral activation treatment.37,38 The content was adapted from this evidence and prepared into six self-help modules for ethnic minority young adults. The modules included introduction, confronting agenda, and daily monitoring; values and activity scheduling; acceptance and cognitive defusion; being present and observing self; daily plans and committed action; and relapse prevention and planning. The content of each module was developed according to its purpose and relations; for instance, we have prepared acceptance and cognitive defusion in one module, with acceptance content coming first, then cognitive defusion. The sequence and number of sessions were determined based on the existing literature.57,58 Consistent with previous studies,28,57 study participants were allowed one week per module, for a total of six weeks for six modules.
In phase 2, a local expert panel comprised of professionals with expertise in addiction and ACT implementation was rigorously reviewed and suggested modifications to the intervention before conducting the usability testing. Their evaluations focused on the intervention’s content, accuracy, comprehensiveness, meaningfulness, relevance to the study’s objective, and ease of understanding for ethnic minority young adults. Most of the items were considered quite or highly relevant by most experts, which made the content validity index acceptable, aligned with its intended purpose and population. Despite this positive evaluation, the experts provided insightful recommendations for refinement in future iterations. Firstly, the panel experts suggested simplifying the technical ACT language. This comment was particularly essential for ethnic minorities with lower educational levels, who may struggle with complex terms. The panel members specifically recommended that the technical terms of ACT should be translated into plain and simple language, thus enabling the ethnic minorities to self-complete the intervention modules without assistance. Additionally, experts suggested that audio and video-based metaphors and exercises should be used instead of only providing textual descriptions. This provided additional benefits, particularly for visual learners and individuals with limited proficiency in language comprehension. Another crucial recommendation was the incorporation of withdrawal symptoms management in the first session of intervention. One expert stated that participants might experience withdrawal symptoms immediately after deciding to quit alcohol. Focusing on these symptoms in the first module could enhance engagement and adherence to the subsequent sessions. Following a rigorous refinement based on the expert feedback, in phase 3, an online intervention delivery platform was developed for ethnic minority young adults. This modality offers several advantages over the traditional face-to-face format.41–43 Firstly, online intervention is highly accessible for participants living in remote areas where access to healthcare services is limited. 59 Additionally, findings from our previous qualitative and quantitative studies have indicated that most ethnic minority young adults in Hong Kong are employed and have limited free time. 18 This makes it difficult to attend in-person sessions or participate in various supporting groups or organizations. All these shortcomings of in-person modalities can be solved through online interventions. 59 Furthermore, existing evidence supports the feasibility and effectiveness of online interventions for AUD. 60 In this regard, WHO has recommended the adoption of digital health interventions to increase healthcare coverage, particularly for diverse and hard-to-reach populations. 61 This growing emphasis on digital health and artificial intelligence-assisted healthcare services provides a broader and more efficient dissemination of interventions.61,62
Apart from the panel’s suggestion, in phase 4, a usability test was conducted in a group of ethnic minority young adults. The results of our one-sample t-test showed that the mean SUS score among the participants markedly higher than the threshold, suggesting that the intervention content was appropriate to the target population. Also, the mean score of three items, including (1) I think that I would like to use this system frequently; (2) I would imagine that most people would learn to use this system very quickly; and (3) I felt very confident using the system, was higher than 4, reflecting that our intervention could be completed independently by the participants without any assistance.
Conducting this proof of concept was instrumental in revealing areas that needed further improvement. The process evaluations showed both strengths and challenges with this platform. Most participants felt happy with the intervention and were actively engaged in the intervention. Participants completed most modules, including weekly assignments and exercises. Most participants stated that the module was clear, coherent, understandable, and helpful, despite a few technical errors and some difficulties in understanding a few words, which needed self-searching. Future interventions could optimize the content by further simplifying the language. Additionally, a few participants experienced difficulties in navigating the content and reported technical challenges, including device incompatibility, internet interruptions, login failures, and other technical errors. These problems need to be solved for future interventions, for instance, by considering a brief session (∼10 minutes) to go through the intervention together with the participants using their mobile phones or electronic devices during subject recruitment and ensuring the intervention to be functional on multiple electronic devices and in different operating systems, e.g., Android and iOS. Besides the technical challenges, most participants needed frequent reminders for module completion. Notably, almost all participants needed at least one reminder per module. However, the timing of reminders is incredibly important for ethnic minority young adults. Many participants reported being quite busy during weekdays and unable to use mobile devices for personal activities, often due to work restrictions by their employers. They indicated that they were mostly available on Sundays, holidays, or late at night, and sending reminders during these periods could substantially enhance engagement and module completion for future intervention in this segment of the population.
Limitations
Despite its novelty, this study has some limitations. First, since the authors used online self-administered questionnaires, they did not employ a think-aloud technique to capture their thoughts. Second, the self-reported outcome measurement may have led to underestimating or overestimating the outcome variable. Third, the sample was small, which limited the statistical power of SUS scores and the generalizability of findings to the broader population.
Future interventions
Intervention protocol development and usability testing are key preliminary steps before actual implementation. The results of usability testing indicated that the internet-based self-help ACT-BA intervention was appropriate for ethnic minority young adults. However, a few modifications would be made based on the suggestions provided by experts and end-users. Future research will conduct a brief session to guide the participants to access the intervention using their smart devices during subject recruitment, ensure that the intervention content can be accessed using different smart devices and operating systems, and frequently send reminders to participants, especially during holidays and weekends, to improve their engagement. Interventions could also be prepared in plain and simple language and can incorporate withdrawal symptom management in the first session.
Conclusion
A new internet-based self-help ACT-BA intervention was developed and evaluated for its usability among Hong Kong ethnic minority young adults with AUD. The findings of this usability testing showed an excellent usability score. However, minor technical errors and layout issues were identified. Future studies should consider minimal modifications. The efficacy and feasibility of our proposed intervention shall be further examined in the future randomized controlled trial.
Supplemental material
Supplemental material - Development and usability testing of an internet-based self-help program integrating acceptance and commitment therapy and behavioral activation intervention for ethnic minority young adults with alcohol use disorder: Usability study
Supplemental material for Development and usability testing of an internet-based self-help program integrating acceptance and commitment therapy and behavioral activation intervention for ethnic minority young adults with alcohol use disorder: Usability study by Getaneh Mulualem Belay, Katherine Ka Wai Lam, Qi Liu, Ting Mao, Qian Sun, Yim Wah Mak, Ka Yan Ho in DIGITAL HEALTH.
Supplemental material
Supplemental material - Development and usability testing of an internet-based self-help program integrating acceptance and commitment therapy and behavioral activation intervention for ethnic minority young adults with alcohol use disorder: Usability study
Supplemental material for Development and usability testing of an internet-based self-help program integrating acceptance and commitment therapy and behavioral activation intervention for ethnic minority young adults with alcohol use disorder: Usability study by Getaneh Mulualem Belay, Katherine Ka Wai Lam, Qi Liu, Ting Mao, Qian Sun, Yim Wah Mak, Ka Yan Ho in DIGITAL HEALTH.
Footnotes
Acknowledgement
Firstly, we would like to express our gratitude to the Hong Kong Polytechnic University for granting the Qualtrics platform to design this internet-based self-help intervention. Secondly, we want to express our sincere acknowledgment to all study participants who took part in this study. Finally, the authors would like to thank the expert review panel for their expertise in evaluating the intervention protocol.
Ethical considerations
This study received ethical approval from the Human Subjects Ethics Sub-Committee of the Hong Kong Polytechnic University (reference number: HSEARS20240712003). The protocol was registered on ClinicalTrials.gov with a National Clinical Trial number of NCT06779006. Informed written consent was taken from each participant.
Author Contributions
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare no conflict of interest.
Data Availability Statement
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
Guarantor
KYH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.