
Abstract
Background
Patients with cancer need to make complex treatment decisions that weigh benefit, risk, and increasingly, treatment costs. Although patients desire to have information about out-of-pocket (OOP) spending to help inform such decisions, individualized OOP cost information is rarely discussed in clinical practice and often difficult for patients to access. FinCare, an online tool for generating patient-specific OOP cost estimates, was developed to address this gap. This pilot study evaluated the feasibility and acceptability of FinCare among patients receiving cancer therapy.
Methods
Patients (n=10) beginning a new cancer therapy regimen were recruited to provide feedback and input. Participants’ treatment and insurance information were entered into FinCare to generate individualized OOP cost estimates. After reviewing the report, participants rated its usefulness and their satisfaction with this online tool. Secondary outcomes of financial toxicity and anxiety were also assessed.
Results
FinCare successfully generated individualized monthly OOP estimates for all participants (range: $0–$2172.34/month). Acceptability was high, with 80%–90% endorsing its ease of use and high satisfaction with the information received. Qualitative comments indicated that participants found the information to be clear and helpful for planning. Receipt of individualized cost information did not result in significant changes in financial toxicity or anxiety.
Conclusions
FinCare was feasible to implement and acceptable to patients starting a new cancer regimen. Receipt of individualized OOP cost estimates was reported to be useful and did not increase participant anxiety. Study findings, however, are limited by the small sample of patients from a single insurer and a single academic institution. Future studies comprised of larger, more diverse patient populations from multiple insurer groups and centers are warranted to demonstrate the broader feasibility and utility of this tool.
Introduction
Patients with cancer are expected to make complex treatment decisions that weigh benefit, risk, and increasingly, treatment costs. The cost of cancer care, including chemotherapy, targeted therapies, and immunotherapies, can be substantial and are projected to increase 35% by 2030. 1 The development of novel and advanced treatments, while promising improved outcomes, often comes with steep price tags that strain patients’ financial resources. Indeed, a survey of patients seeking assistance from a national co-payment foundation found that 42% reported “significant or catastrophic” financial burden. 2 As a result, the concept of “financial toxicity” has emerged as a critically important issue in cancer care, reflecting the adverse financial burden that patients with cancer and their families often experience.3,4
Importantly, financial concerns occur in patients across all socioeconomic strata. 5 The consequences of financial toxicity can be profound and are not only associated with heightened levels of distress, anxiety, and depression,6,7 but also can lead to treatment delays or even premature discontinuation of treatment, negatively impacting treatment efficacy and clinical outcomes.8–10 The long-term consequences of financial toxicity include persistent financial struggles, debt accumulation, and bankruptcy, and may even result in a lower likelihood of seeking timely medical care in the future. 10
Experts have called for “financial interventions” to provide education, increase patient self-efficacy for managing cancer costs, and facilitate linkages to assistance programs and available resources.3,11 However, it is difficult for patients to identify in advance what their treatment costs will be. Further, understanding
To address this gap, an online tool was developed to estimate patient-specific OOP costs based on their health insurance coverage and their specific cancer treatment plan. We conducted a pilot study to evaluate the feasibility and acceptability of this online tool in a sample of patients with cancer who were starting a new regimen of systemic cancer therapy.
Methods
Study participants
We recruited patients receiving treatment from a comprehensive cancer center. Participants in this pilot study were patients who were scheduled to begin active treatment for their cancer. Eligible patients were those who: (1) were receiving a new regimen of intravenous anti-cancer therapy (chemotherapy, immunotherapy); (2) had primary health insurance through selected preferred provider organizations (PPOs); and (3) were able to read or communicate in English. In this small demonstration project, given the costs and challenges in obtaining payment rates across different insurers, the online tool was developed for use only with Independence Blue Cross PPO which is the largest PPO where the study was conducted.
Patients were excluded if they were: (1) receiving neo-adjuvant therapy; (2) receiving cancer care at an external institution (other than where the pilot study was being conducted); (3) participating in a clinical trial since some costs are covered by trial sponsors; (4) covered under more than one health insurance plan; (5) unable to provide informed consent; (6) unable to read English, as the online tool was initially developed in an English language version; and (7) receiving
This study was approved by the Institutional Review Board and all participants provided written informed consent. Participation was voluntary and participants were informed that they could choose to stop participating at any time.
FinCare: An online tool for estimating OOP costs
FinCare was created by an oncology-focused software development firm Digidence (https://digidence.co). The FinCare tool provides estimates of patient-specific out-of-pocket (OOP) costs incurred as part of intravenous anti-cancer therapy (chemotherapy, immunotherapy, biologic therapy) and oral targeted anti-cancer therapies. The software can calculate this information by interfacing with the patient’s insurer to obtain data on negotiated reimbursement rates, copays, year-to-date expenditures, and out-of-pocket caps. Initial testing of the tool prior to study deployment ensured that the software was accurately and comprehensively capturing information from Independence Blue Cross.
Study procedures
This was a single-arm, single-center, nonrandomized feasibility study using a pre–post design. Eligible patients were referred to a study coordinator by collaborating clinicians. The study coordinator met with the potential participant to describe the study and obtain written informed consent. Participants were recruited in clinic or at another time that was convenient for the patient. Following the informed consent process, participants completed the baseline survey (see Measures below) and scheduled a follow-up appointment to meet with the study coordinator approximately 1-2 weeks later to review the FinCare OOP estimates (see Figure 1). Study flow and timeline.
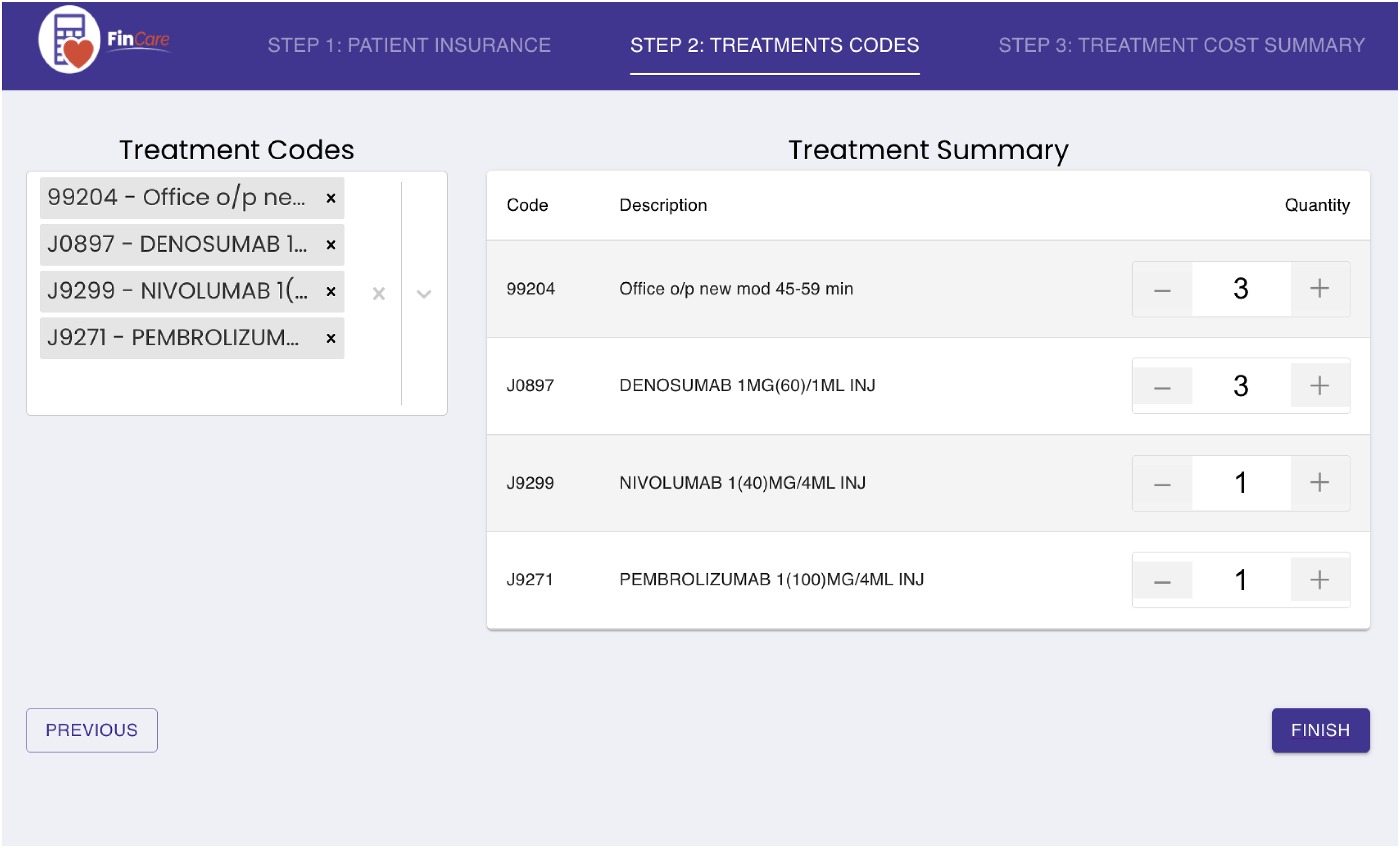
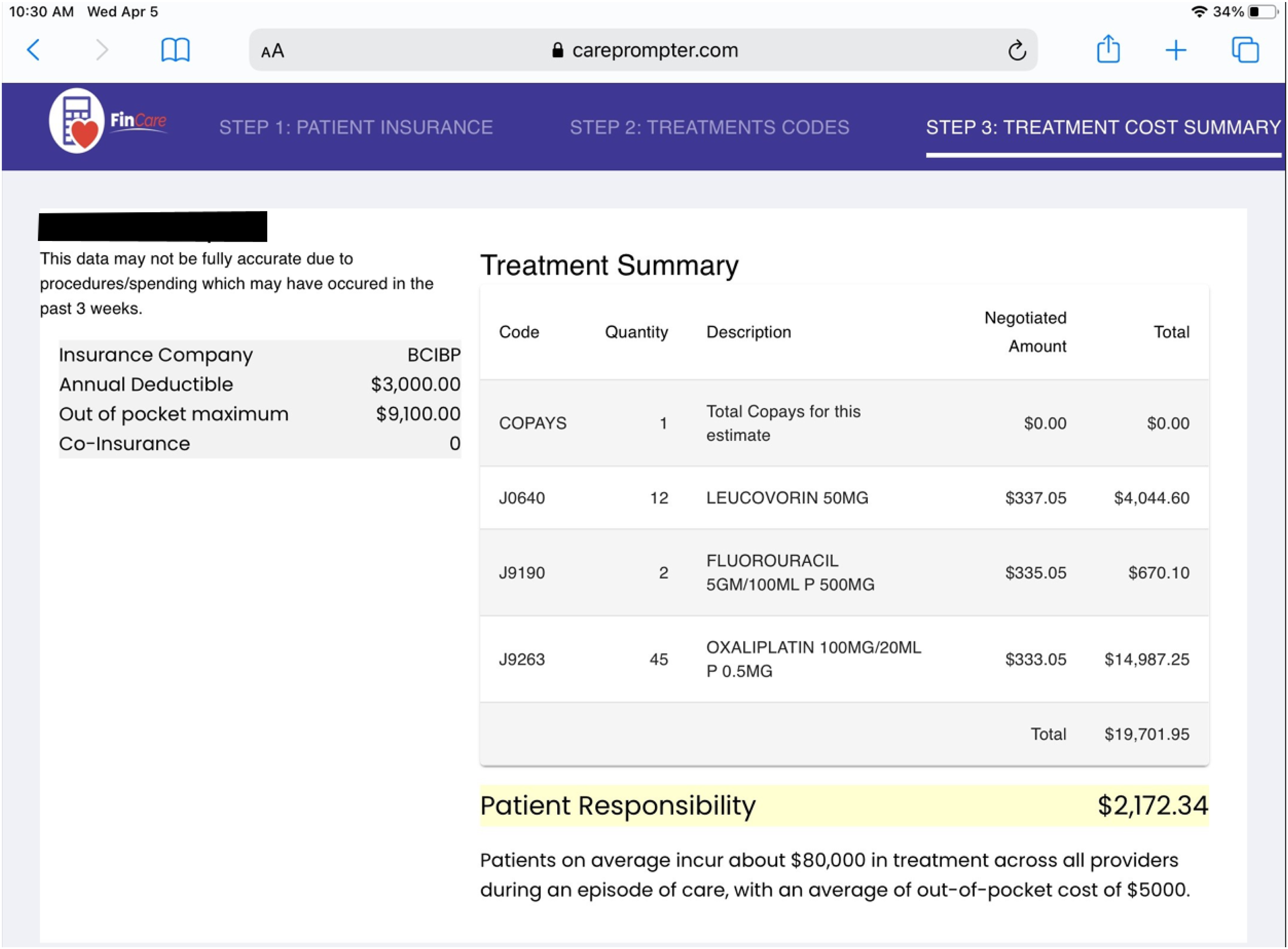
The study coordinator was responsible for locating the patient’s insurance plan and entering the treatment information into FinCare, which is a secure online system (see Figures 2 and 3). Using the patient’s specific insurance information and proposed treatment plan, FinCare then provided an estimate of the patient’s anticipated monthly out-of-pocket costs based on the health expenditures already incurred and the treatment plan entered (Figure 4).(Supplementary Figure 1) FinCare step 1: Locating patient record and insurance information. FinCare step 2: Entering treatment codes. Example FinCare report.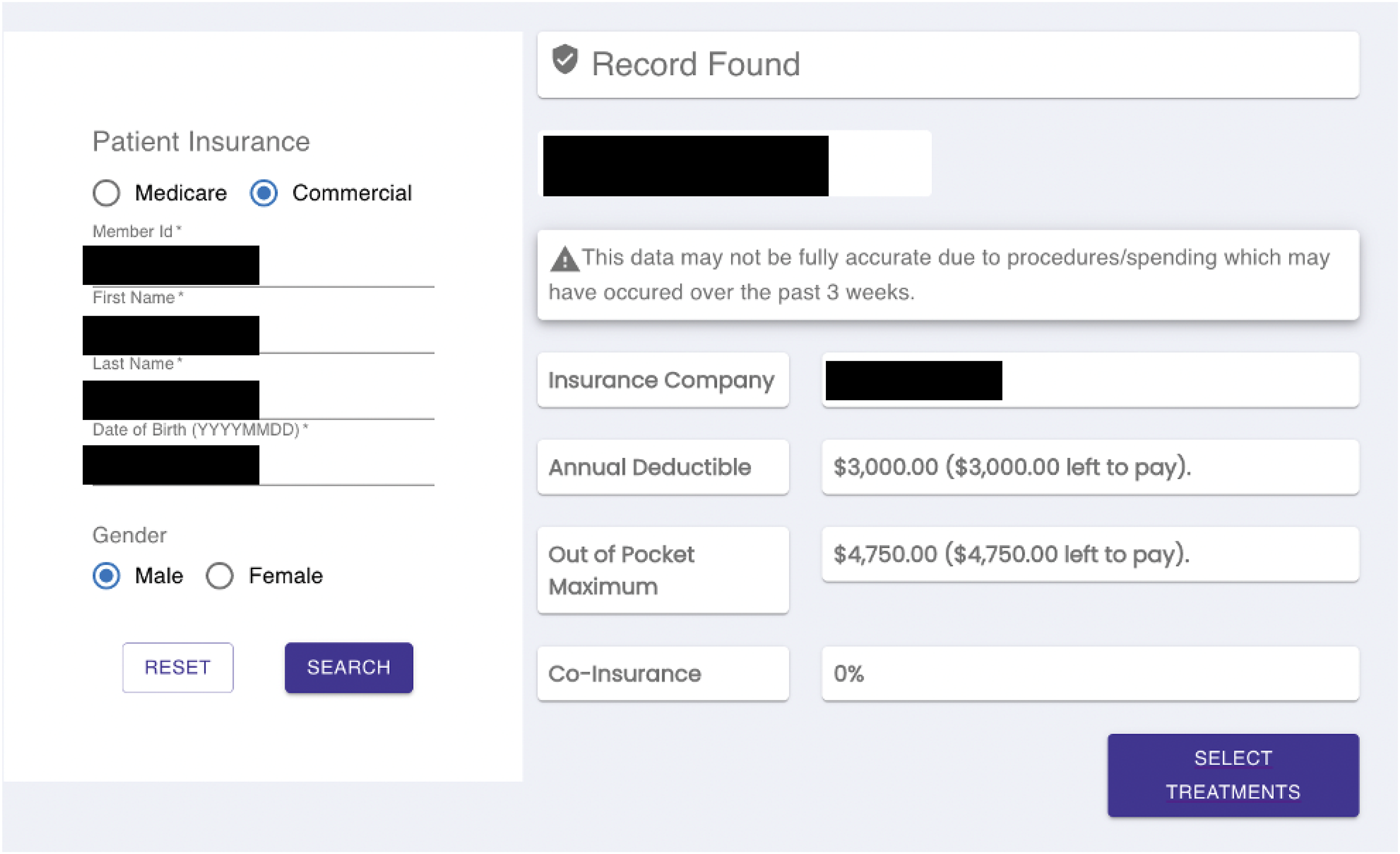
Approximately 1-2 weeks after the baseline assessment, participants reviewed the FinCare estimates with the study coordinator who described the program and how it calculated the out-of-pocket costs. After reviewing the printout, participants completed a brief acceptability measure, rating the usefulness of the information provided and their satisfaction with this information. Participants were also asked to share any comments and feedback regarding FinCare.
The final assessment was obtained four weeks later. Participants were contacted by the study coordinator to complete a final follow-up survey to assess levels of financial toxicity, anxiety, and distress. In total, the study duration was about six weeks in length.
Measures
Demographic and clinical characteristics
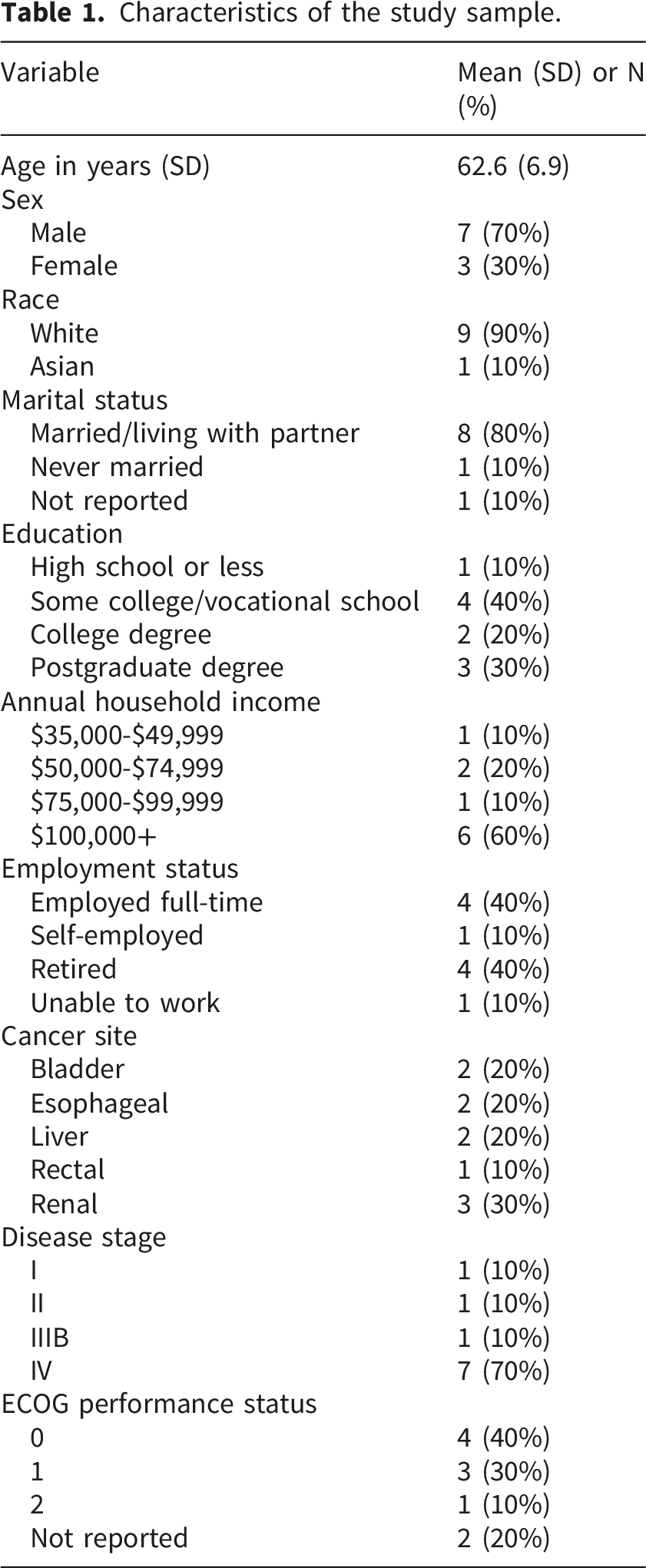
Demographic data pertaining to participant age, sex, race and ethnicity, education level, and marital status was obtained via self-report at study entry. Clinical characteristics --including site of primary disease, disease stage, and performance status -- were extracted from the electronic health record (EHR) by study staff.
Primary outcomes: Feasibility and acceptability
To assess
Several open-ended items were administered in a semi-structured interview format to probe for aspects that could be improved. Example items included “What did you like (or dislike) about this program?” and “What other types of information would you like to have?”.
Secondary outcomes
Secondary outcomes included measures of financial toxicity, general anxiety, and cost-specific distress and were administered at baseline (T1) and the final follow-up assessment (T2). Financial toxicity was assessed using the 12-item Comprehensive Score for Financial Toxicity (COST-FACIT, ver. 2) measure. 20 Each item is scored on a five-point Likert-type scale ranging from 0 (not at all) to 4 (very much). The responses are summed across all items to create a total score ranging from 0 to 48, with lower scores indicating greater financial stress within the past seven days. The scale has demonstrated high internal consistency and reliability in measuring financial toxicity and high utility as a clinically-relevant patient-centered outcome.
General anxiety was measured using the PROMIS-Anxiety short-form (PROMIS-A-SF), a 7-item measure that captures the frequency of selected anxiety symptoms over the past seven days using a five-point response scale (ranging from 1 to 5). Item scores are summed to obtain a total raw score, which is then converted to a T-score (mean 50, SD = 10). The PROMIS-A-SF has demonstrated strong validity in oncology patients.21,22
To capture levels of distress related to their cancer costs, participants completed the 6-item Impact of Events Scale-6 (IES-6). 23 This measure has demonstrated high internal consistency and reliability. 24 The scale was adapted to assess distress associated with cancer care costs and asked participants to report the frequency with which they were bothered by thoughts concerning their cancer costs. Response options ranged from “1=Not at all” to “5=Extremely.”
Statistical analyses
Demographic and clinical characteristics of the study participants were summarized using standard statistical measures (e.g. frequencies, proportions, means, standard deviations). Descriptive statistics were used to characterize participant ratings of financial distress, anxiety and levels of satisfaction with FinCare. The primary outcome was feasibility, which was defined by whether the patient’s out-of-pocket cost estimate was retrievable by the online tool. A future study would be determined to be feasible if >6 (i.e. 7 or more out of 10) patients have retrievable out-of-pocket costs. Acceptability was assessed as a secondary outcome (e.g., was the information provided satisfactory, understandable, and helpful). Secondary endpoints were summarized using means, standard deviations, proportions, and 95% confidence intervals as appropriate.
Sample size justification: We chose the sample size to have sufficient power and Type I error to conclude that a future trial would be feasible. We will declare a future study feasible if 1) >6 (i.e. 7 or more out of 10) patients have retrievable out-of-pocket costs. We have 88% power to declare feasibility under a promising feasibility hypothesis of 80% and a 5.5% Type I error rate (1-sided) under a discouraging feasibility hypothesis of 40%. In other words, an encouraging population level rate of 80% implies that 80% of patients on average have retrievable out-of-pocket costs.
A sample size of 10 will also allow us to estimate a standard deviation of secondary endpoints with sufficient precision. The standard deviation of these endpoints is of particular interest as it will be a key statistic that allows us to power a larger trial. With 10 participants, we will be able to estimate the 95% confidence interval of a standard deviation with a width of approximately 1.14 standard deviation units. This estimate is based on the actual width when the observed standard deviation is standardized to 1.0. We estimated the width using PASS 11 software.
Results
Participant characteristics
Characteristics of the study sample.
Feasibility, acceptability and participant feedback
The primary outcomes were feasibility (i.e., did at least 70% of participants receive the program?) and acceptability (i.e., did at least 70% of participants who received the program find it to be satisfactory, understandable, and helpful?). In addition, we also collected preliminary data on secondary outcomes (i.e., financial toxicity, anxiety, and cost-specific distress).
Participant ratings of acceptability.
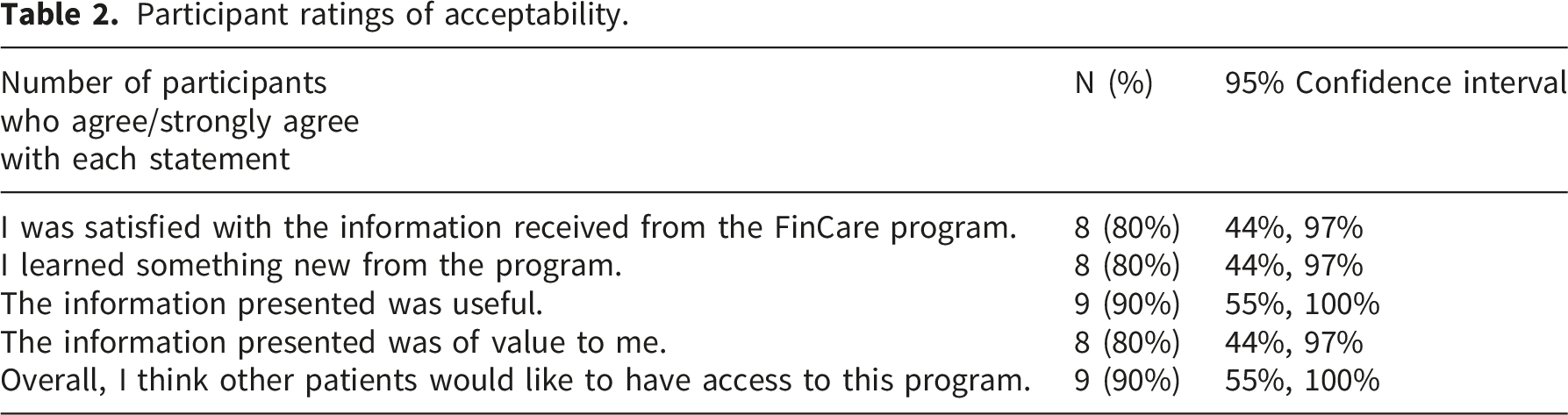
We used open-ended items to obtain participants’ input and feedback about the FinCare tool. Responses were descriptively summarized. In brief, participants generally found FinCare to be useful –all participants responded positively when queried about the program. Examples of participant feedback are presented below: “Very helpful with what to expect.” (ID# 101) “The information is clear, laid out well, and [is] a useful planning tool.” (ID# 105) “Very good information. Makes my uncertainty very clear now.” (ID# 106) “The estimate is easy to understand, and I like the information provided.” (ID# 108) “It was informative, would use if needed.” (ID# 110)
Participants did not have many comments pertaining to aspects that they disliked, but the few that were mentioned included: “Slow to respond at times. Could be the wi-fi.” (ID# 107) “Information could be missing from the past 3 weeks.” (ID# 109).
Suggestions for improvement included requests for more information on how to get funding or financial support if their treatment is not covered by insurance; and information on whom to contact and how to cover non-medical costs particularly during employment breaks (i.e. work stoppage). “Offering alternative ways to pay would be helpful. Ex: charities, drug companies, alternative pay methods.” (ID# 105) “Maybe instead of just one treatment, [it] could also show up to date yearly costs.” (ID# 106) “Ways to fund other aspects of life during work outages.” (ID# 101)
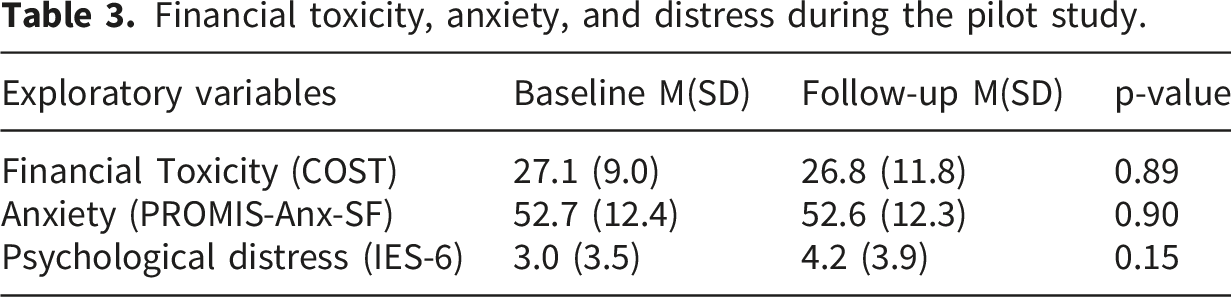
Secondary outcomes
Financial toxicity, anxiety, and distress during the pilot study.
Discussion
The findings from this pilot study indicate that FinCare is feasible and acceptable to patients with cancer. The FinCare online tool estimated monthly out-of-pocket costs for each participant, with costs ranging from $0 to $2172.34. Participants were generally satisfied with the online tool, rating FinCare as helpful and valuable. Notably, receipt of this information did not result in increased levels of anxiety or cost-related distress. Overall, participants found the information to be easy to understand and helpful.
These data suggest that FinCare may be a useful tool for mitigating uncertainty around cancer costs in patients with cancer, which could yield beneficial effects on treatment decision making and psychological well-being. Studies have shown that uncertainty and distress surrounding cancer care costs can lead to heightened anxiety, which can hinder treatment adherence and compromise overall quality of life. 7 For example, Zafar and colleagues reported that insured cancer patients experienced significant financial distress, which was strongly associated with emotional symptoms and overall distress. 2 Other studies have similarly reported that financial distress is a significant predictor of emotional distress in cancer patients. 6 The provision of clear and specific information, such as that offered through the FinCare tool, may be helpful for patients to identify key areas of short-term need that could then be managed through coordination with insurance companies, pharmaceutical resources, and patient financial services.
Despite patients’ reports that receiving estimated OOP costs was useful and helpful, we did not observe a decrease in financial toxicity, anxiety, or cost-related distress at follow-up. The absence of any change in the secondary outcomes could be attributed in part to the small sample size and the relatively short follow-up period. In addition, it is acknowledged that the provision of OOP cost estimates alone – without accompanying financial navigation resources or assistance packages -- is unlikely to impact distress outcomes. Indeed, prior studies have also reported mixed or null effects on anxiety-related outcomes, even when financial navigation programs improved knowledge and uptake of financial assistance programs.25,26 Such findings highlight how emotional distress may persist despite resolution of discrete financial barriers, requiring further support from mental health professionals for oncology patients. 25
This pilot study offers several promising avenues for future research. First, it is essential to explore how providing additional support at follow-up time points can help mitigate and reduce concerns about cancer care costs. As alluded to above, it is critical to consider integrating other resources and support services with the use of this tool. Incorporating consultations with Patient Financial Counselors and evaluations by the Department of Social Work to assist with managing non-medical financial needs and employment-related issues would be beneficial. Offering psychological support in addition to financial navigation may also be needed to address the persistent distress commonly reported during this challenging period of time, as other researchers have advocated. 27
Second, future research should focus on refining and enhancing the program based on the feedback we received. Participants provided practical suggestions for enhancing program content and delivery. These included improving the responsiveness of the program and addressing the applicability of financial situations for patients with multiple insurance plans. Towards this end, in subsequent iterations of the tool we plan to use the API (application programming interface) of a commercial health insurance integration service, such as Change Healthcare, which is able to verify insurance coverage from virtually all health insurance plans in the United States as well as contractual rates. Future plans may also involve developing a clinician-facing version of the tool to help promote greater adherence to national recommendations for clinicians to discuss potential OOP costs with their patients14,15 and increase clinician efficacy in initiating such discussions.
Third, in this pilot demonstration, the FinCare tool was limited to estimating OOP costs associated with receipt of oral and intravenous anti-cancer therapy due to the additional complexity of incorporating surgery or radiation therapy. However, advances in radiation oncology–specific Fast Healthcare Interoperability Resources (FHIR) profiles that are being developed through collaborations among professional societies, electronic health record (EHR) vendors, and standards bodies provide a foundation for the future deployment of the FinCare tool in the setting of radiation therapy. 28 Thus, these opportunities to address current interoperability challenges represent the next stage of development.
This pilot study is the first evaluation of the feasibility and acceptability of using FinCare to estimate monthly out-of-pocket costs based on the patient’s specific treatment plan and insurance carrier. This approach provides patients with valuable – and targeted – information about upcoming costs. Additionally, the high feasibility and acceptability ratings of the program suggest that patients desire this information. However, we acknowledge several limitations of the present study. A key limitation is that the study did not validate the accuracy of the generated OOP cost estimates. Future studies should include a formal comparison between the estimated OOP costs and patients’ actual OOP costs. A validation analysis using actual billed amounts or patients’ explanation of benefits (EOBs) can be included in the next phase to enable a prospective comparison of FinCare estimates with actual patient expenditures.
Another limitation is the small sample size, which constrains generalizability and our ability to draw conclusions about the potential impact of the FinCare tool in a broader, more diverse patient population. This pilot study only enrolled patients with primary health insurance through selected preferred provider organizations (PPOs), which may not be representative of all cancer patients and insurance plans. Indeed, the sample in this demonstration project was comprised of predominantly non-Hispanic White patients with relatively high income. The exclusion of patients with dual insurance omitted the larger population of older patients with Medicare as well as those with Medicaid who may be more likely to have medically complex care (due to age or other co-morbidities) or experience socioeconomic vulnerability and/or structural barriers to care. In addition, the FinCare tool is presently available only in English and therefore, study findings may not be generalizable to non-English speaking patients. Factors such as language proficiency and socioeconomic status can contribute to how digital health tools are perceived and experienced by patients. As a result, the present findings may underestimate challenges related to usability, perceived usefulness and value in more diverse patient samples. To promote digital health equity, it is imperative to ensure that the developed tools can be accessed and utilized across the broader population. Thus, additional studies are required to validate these findings and assess the impact and utility of this novel tool with patient samples that are inclusive of diverse sociodemographic characteristics and insurance coverage.
Conclusions
This study contributes to the field of digital health by evaluating the real-world feasibility and acceptability of a patient-facing cost estimation tool within an oncology care setting. The findings from our pilot study suggest that the FinCare online tool is feasible and acceptable to patients with cancer. Patients valued the information they received and found it easy to understand. Recommendations for enhancing program content will help refine the program for patients seeking information on other sources of financial support for treatment. In addition, opportunities to strengthen linkages with existing resources, such as financial counselors and social workers, will also support patients with managing a variety of both financial and psychosocial needs.
Supplemental material
Supplemental material - Feasibility and acceptability of FinCare: A personalized online tool for estimating out-of-pocket costs for cancer treatment
Supplemental material for Feasibility and acceptability of FinCare: A personalized online tool for estimating out-of-pocket costs for cancer treatment by Carolyn Y. Fang, Amani Boudriga, Amine Raounak, Howard Isenstein, Brian L. Egleston, Erin Tagai, Melissa McShane, Efrat Dotan, Daniel M. Geynisman in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the patient participants for their helpful feedback and input. We thank the FCCC Biostatistics and Bioinformatics Facility and the Population Studies Facility for their services.
Ethical considerations
This study was approved by the Fox Chase Cancer Center Institutional Review Board (IRB no. 22-8011) on September 19, 2022.
Consent to participate
All participants provided written informed consent prior to participating.
Author contributions
CYF: conceptualization, data curation, funding acquisition, investigation, project administration, writing-original draft and writing-review & editing. AB: methodology, resources, software, validation, and writing-review & editing. AR: methodology, resources, software, validation, and writing-review & editing. HI: conceptualization, methodology, resources, software, validation, and writing-review & editing. BLE: funding acquisition, data curation, formal analysis, visualization, and writing-review & editing. ET: resources, writing-review & editing. MM: investigation, resources, writing-review & editing. ED: investigation, resources, writing-review & editing. DMG: conceptualization, funding acquisition, investigation, project administration, writing-review & editing. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a pilot grant from Fox Chase Cancer Center and National Institutes of Health grants P30 CA06927 and U54 CA221705.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
De-identified data reported in this study are available upon reasonable request from the corresponding author.
Guarantor
CYF.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.