
Abstract
Introduction
Computer-based simulation, structured around the prebriefing-simulation-debriefing model, has been increasingly integrated into health management education. This study aimed to evaluate the perceived effectiveness of computer-based simulations on the learning outcomes of final-year undergraduate health management students.
Methods
This cross-sectional study, involving 124 students, was conducted at a medical university in Eastern China from October to November 2025. Perceived effectiveness was measured using a Simulation Effectiveness Tool-Modified questionnaire. The data were analyzed using descriptive statistics and multiple regression analyses. Methodological rigor was maintained in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Results
Most participants perceived the simulation as highly effective, indicating positive learning outcomes. Learners’ perceived effectiveness was significantly enhanced by their self-efficacy (β = 0.486, p < 0.001), gains in knowledge-skills-attitudes (β = 0.188, p = 0.029), and prior simulation experience (β = -0.173, p = 0.016).
Conclusions
Grounded in the prebriefing-simulation-debriefing model, computer-based simulation demonstrates promising perceived effectiveness as an instructional method for health management education. This structured implementation ensures systematic learning, while highlighting the critical importance of fostering learner confidence and preparedness to maximize educational outcomes.
Introduction
The concept of health management was highlighted in 2016 with the release of the “Healthy China 2030″ Plan by the Central Committee of the Communist Party of China and State Council. The plan aimed to transition the healthcare system from a traditional model to one that is personalized, proactive, and patient-centered. 1 It notably introduced the concept of “active health,' emphasizing the creation of health value through preventive measures and the management of health risk factors at their source. 2 This plan aimed to enhance public health literacy, promote healthy lifestyles, and effectively control the incidence of major chronic diseases. In 2022, the Report of the 20th National Congress of the Communist Party of China reaffirmed its commitment to building a Healthy China, strengthening health management for major chronic diseases, and improving grassroots capacity for disease prevention, treatment, and health management. 3 Health management involves comprehensive monitoring, analysis, evaluation, and planned interventions for risk factors in individuals or populations. 4 These competencies constitute the core skills that health management students must acquire through health-management programs. However, in current teaching practices, these skills are often fragmented across courses. Furthermore, the long-term nature of chronic disease health management limits student opportunities to acquire the required practical competencies.
Simulation is regarded as an opportunity to integrate curricular content typically covered in separate modules 5 and foster a more robust transition from academic theory to hands-on clinical training in healthcare settings. 6 This approach provides a safe environment where mistakes can be made without adverse real-world consequences. 7 Furthermore, simulation facilitates learning by mimicking clinical situations, thereby advancing the development of technical competencies and soft skills.8,9
Simulation-based learning in nursing education involves several distinct complementary approaches that can be broadly categorized into three methodological types: role-playing, physically based, and computer-based simulations. 10 Within these categories, a range of specific tools are utilized, including anatomical or mechanical models, computer-based programs, high-fidelity human patient simulators, virtual reality systems, and simulated patients. 11 Computer-based simulations have been integrated into health management education, offering virtual environments that replicate real-world systems. 12 This “sandbox' approach—derived from computing and denoting a secure, isolated testing space—enables students to practice skills without risk to actual operations. Leveraging these advantages, this study employed a health-management scenario simulation (HMSS) system. Within the HMSS system, students assume the role of community health managers. Using visualized data and textual background information, they conduct situational health management for simulated residents. The simulation begins with the system randomly selecting a chronic disease case from the patient database. Starting from initial patient contact, the system presents sequential problem-based scenarios. As students resolve each issue, the next step in the health-management service process unfolds. Through iterative analysis and evaluation of evolving patient information, students progress until all modules of the health service process are completed. However, the effectiveness of this strategy has not yet been adequately examined. The evaluation of simulation effectiveness crucially encompasses the assessment of knowledge transfer to clinical practice and may correlate with students' self-reported learning and confidence. 13 Therefore, a computer-based simulation was introduced to support final-year undergraduate health-management students preparing for their clinical internships.
Study framework
In simulation-based learning, Kolb’s experiential learning theory provides a coherent framework for instructional design. Kolb’s theory conceptualizes learning as a cyclical process that progresses sequentially through four stages: concrete experience, reflective observation, abstract conceptualization, and active experimentation. 14 These stages operate in an iterative cycle wherein each phase informs and advances the next, thereby fostering continuous knowledge development and skill integration. Specifically, simulation-based learning is an iterative process that begins with a concrete experience of performing a scenario and proceeds to a reflective observation phase conducted through debriefing. Insights from this reflection feed into an abstract conceptualization phase, where students derive general principles, theoretical understanding, and alternative strategies from their experiences. Finally, an active experimentation phase is realized as students apply this refined understanding to subsequent simulations and transfer it to future real-world practice.
Guided by this framework, we developed a health management simulation program for final-year undergraduate health management students in our simulation laboratories. Perceived effectiveness constitutes an essential component of comprehensive simulation evaluation. Grounded in Kirkpatrick’s framework, learner reaction serves as the foundation for subsequent learning and behavioral outcomes while independently capturing the self-efficacy and motivation critical for skill transfer. 15 This study aimed to evaluate the perceived effectiveness of computer-based simulations on the learning outcomes of undergraduate health management students.
Methods
Study design
We conducted a descriptive cross-sectional study in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (supplement 1). 16 This design provided a snapshot to explore undergraduate health management students’ perceptions of computer-based simulation, with the aim of describing patterns at that time rather than establishing causal relationships.
Setting and participants
A purposive sampling approach was employed. This study was conducted at a medical university in Eastern China. Data were collected between October 2025 and November 2025 in the simulation laboratories. All fourth-year undergraduate health management students (N=124) were eligible for the study because they had completed all health management curricula and possessed basic knowledge about health management. The inclusion criteria comprised those: (1) who were fourth-year undergraduate students in health management; (2) who had completed most of their practical courses, indicating sufficient competence to engage in computer-based simulations; and (3) who had no visual or hearing impairments. The exclusion criteria comprised those: (1) diagnosed with a psychiatric condition (e.g., anxiety disorder), as mental disorders may impair cognitive functioning and attentional focus required for simulation tasks; (2) with self-reported excessive stress, as high stress levels can compromise working memory and decision-making abilities; (3) with impaired hand-eye coordination, directly affecting simulation operation accuracy and introduce extraneous variables; and (4) who had transferred from another major, as they may possess different knowledge backgrounds that could create between-group differences. A simple random sampling approach was adopted for the sample size calculation. With a 95% confidence level (α = 0.05), a 7% margin of error, and an estimated 7% non-response rate, the required sample size was determined to be 115 participants. A total of 124 eligible students were enrolled and completed the study, yielding a 100% response rate. The research protocol was reviewed and approved by the Institutional Ethics Review Board of the Shanghai University of Medicine & Health Sciences (2024-zxkt-01-310225198301136663).
Procedure
After being briefed on the study’s objectives, procedures, potential risks, and benefits, all participants voluntarily provided written informed consent. Subsequently, the simulation environment was introduced. The computer simulation for the health management students followed a structured prebriefing-simulation-debriefing format.17,18 During the prebriefing, the instructor outlined the learning objectives, presented the scenario background, and explained the platform functions. In the simulation phase, the participants worked in groups of three to complete an integrated health management case comprising seven sequential modules: health information collection, assessment, goal setting, intervention, follow-up, evaluation, and emergency response. The instructor provided technical support without any intervention in the decision-making process. The debriefing session allowed the participants to review their decisions and outcomes, as guided by the instructor, and to reflect on theory–practice gaps, data-based decision quality, ethical considerations, and teamwork, while linking the experience to core competencies and future learning goals. Finally, participants were invited to complete an anonymous questionnaire via the Sojump platform (https://www.wjx.cn/). The IP address of each participant’s computer was recorded and monitored to prevent duplicate submissions. A 24-hour restriction period was implemented during which only one survey entry per unique IP address was permitted.
The participants were asked to fill in demographic data in relation to age, gender, and prior health management simulation experience. Perceived effectiveness was assessed by administering the Simulation Effectiveness Tool-Modified (SET-M) questionnaire. The SET-M was used to evaluate the students’ perceptions of the effectiveness of learning in the simulation environment. The SET was first developed in 2005 and subsequently modified to become the SET-M, conforming with international standards of best practices for healthcare simulation. 19 The SET-M has been psychometrically tested and is recognized as a reliable and valid measure of simulation learning effectiveness. 20 The SET-M questionnaire comprises four subscales with a total of 19 items: prebriefing (two items), learning (six items), confidence (six items), and debriefing (five items). Two bilingual experts independently translated the items into the Chinese language. These versions were synthesized and back-translated into English by independent translators. Subsequently, both language versions were reviewed by an expert panel selected based on their expertise to verify their comprehension and cultural appropriateness. Responses are measured on a three-point Likert scale (1= disagree, 2=somewhat agree, and 3=strongly agree). The reliability analysis yielded an overall Cronbach’s α of 0.936 for the 19-item scale. The subscales exhibited high internal consistency, with Cronbach’s α values between 0.792 and 0.913.20,21 The constructs of knowledge, skills, and attitudes (KSAs) 22 were measured using nine items. These items were adapted from previously validated instruments and were reviewed by an expert panel. All items are rated on a six-point Likert scale ranging from 1 (strongly agree) to 6 (strongly disagree). Self-efficacy was measured using a validated Chinese version of the General Self-Efficacy Scale (GSES). 23 The scale comprises ten items, each rated on a 4-point scale. Higher total scores indicate greater levels of self-efficacy.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows version 23.0 software. Survey completion was high and missing data were excluded from the analysis. Demographic and outcome data were analyzed using means and standard deviations for normally distributed variables, medians and interquartile ranges for skewed continuous variables, and frequencies and percentages for categorical variables. The Shapiro–Wilk test indicated that the aggregated SET-M scores were not normally distributed (p < 0.05). A non-parametric test was used to compare various demographic variables and the perceived effectiveness of computer-based simulation learning. Multiple regression analysis was conducted to examine the relationships among demographic information, KSAs and self-efficacy, and perceived effectiveness. Multicollinearity was assessed using tolerance values and variance inflation factors (VIFs), with VIF values exceeding 10 indicating potential multicollinearity concerns. Statistical significance was set at p < 0.05.
Results
A total of 124 undergraduate health-management students participated in this study. The mean age of the students was 20.24±1.14 years and most were female (n = 90, 72.58%). Most participants had no prior health management simulation experience (54.03%, n = 67).
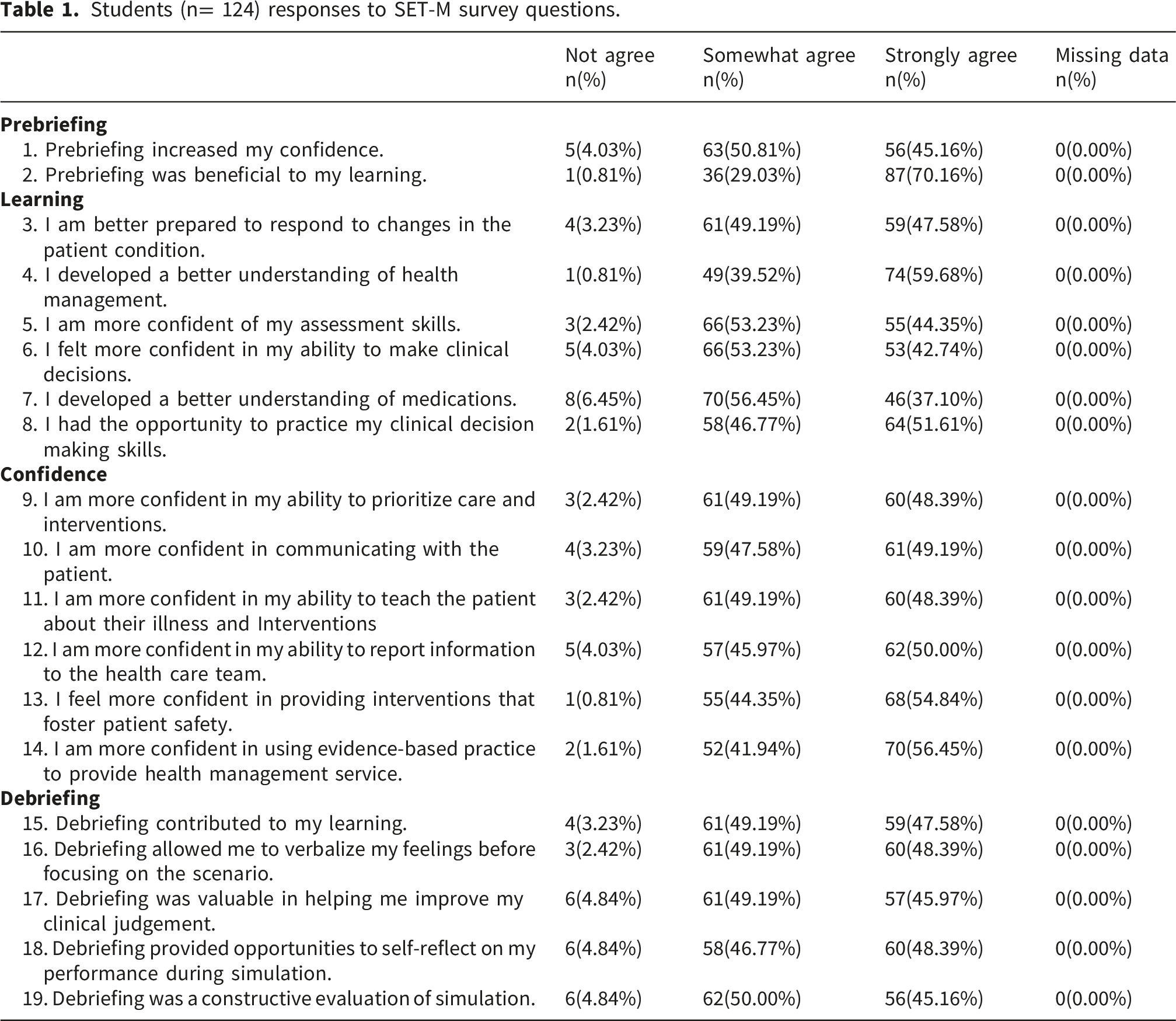
Students (n= 124) responses to SET-M survey questions.
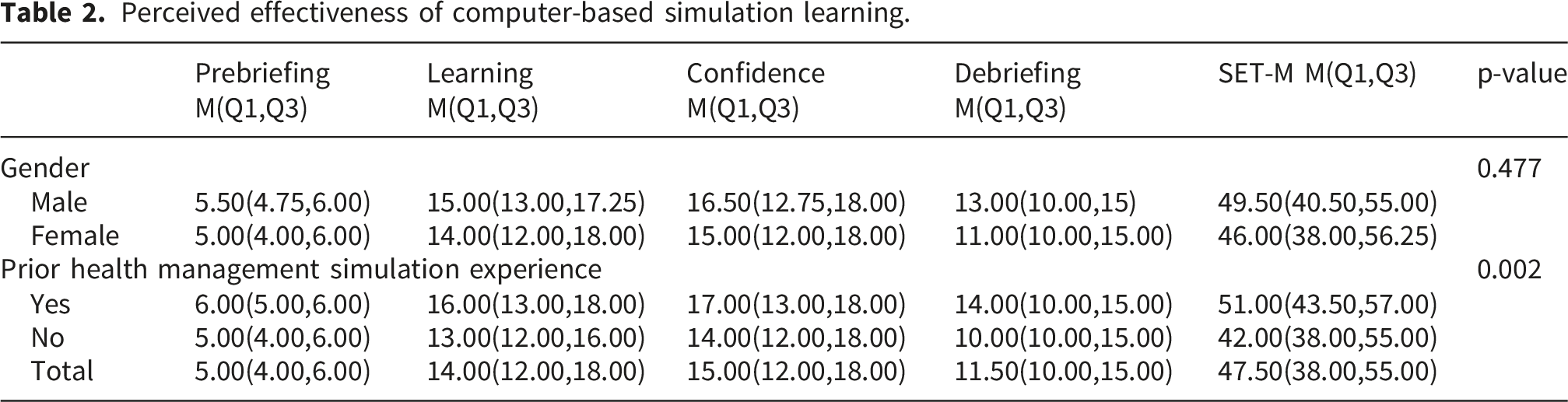
Perceived effectiveness of computer-based simulation learning.
Multiple regression analysis results of factors associated with perceived effectiveness of computer-based simulation learning.
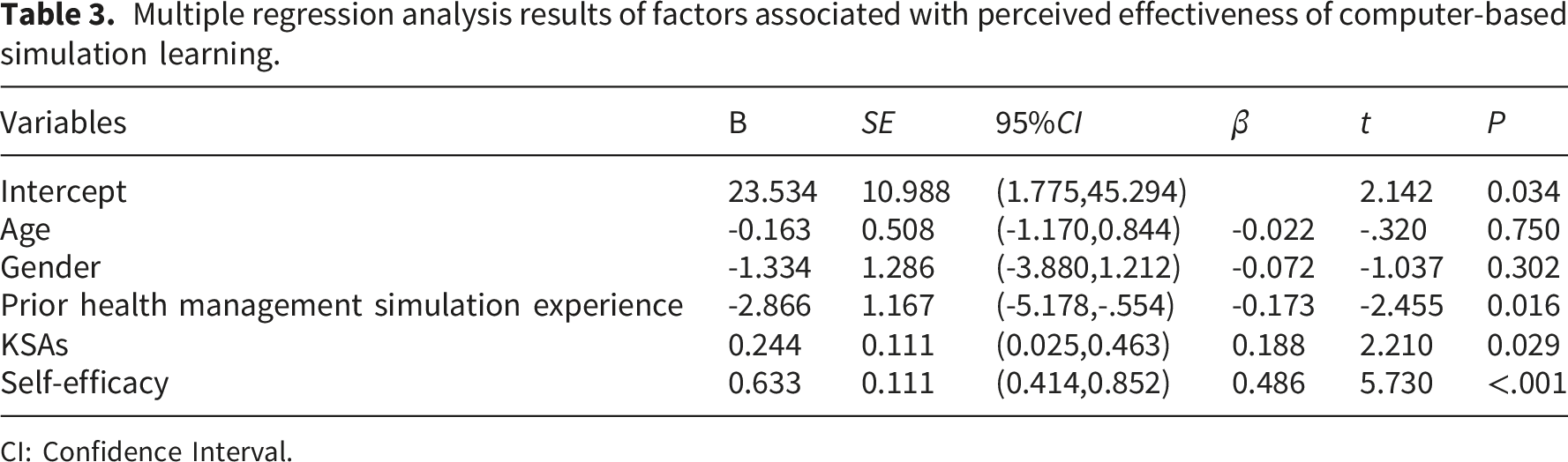
CI: Confidence Interval.
Discussion
Health management majors, intended to equip students to deliver integrated health services to individuals and populations, encompass continuous monitoring, systematic analysis, evidence-based evaluation, preventive planning, and targeted interventions for health risk factors. Computer-based simulation learning for health management is designed to bridge theoretical knowledge with real-world practice and to cultivate students' problem-solving abilities. In this study, the Chinese version of the SET-M was considered suitable for use in general undergraduate health management education. This tool can be applied to improve the design of simulation-related educational practices, enabling simulation instructors to gain insight into what works or does not. 20 It also provides students with opportunities to reflect on their own performance during simulation learning. 21 Simulation instructors may use it to conduct summative evaluations of scenario-based simulation effectiveness while also offering students a structured opportunity for self-reflection on their simulation performance, thereby promoting the comprehensive implementation of simulation-based teaching.
The consistent concentration of responses toward the “strongly agree” and “somewhat agree” categories suggests that students perceived the computer-based simulation positively. However, the negatively skewed distribution of SET-M scores raises the possibility that the scale’s item wording may have framed participants toward favorable responses, or that the measure exhibited ceiling effects in the context of our study. 25 Although our analytical approach addressed distributional concerns, future research should consider complementary measures to triangulate self-reported efficacy gains. The prebriefing-simulation-debriefing model aligns with the principles of Kolb’s experiential learning theory and serves as a valid and reliable pedagogical strategy for structuring simulation-based education. 26 It operationalizes the theory by systematically guiding learners through an experiential cycle of concrete experience, reflective observation, abstract conceptualization, and active experimentation.
This study examined the factors that influence the perceived effectiveness of computer-based simulation learning. The findings indicated that self-efficacy and KSAs significantly contributed to enhanced perceived effectiveness. Self-efficacy is defined as the perceived competence in effectively managing a designated task. 27 Consistent with previous research, a positive correlation was observed between participation in clinical simulations and increased self-efficacy.28,29 Consequently, students with higher levels of self-efficacy were more likely to report greater perceived effectiveness of their learning experience. A potential concern regarding the regression analysis is the conceptual proximity between self-efficacy and the confidence dimension of perceived effectiveness. Therefore, we emphasize two considerations. Theoretically, self-efficacy centers on competence judgment, one’s capability to perform specific actions, 27 whereas perceived confidence reflects outcome valuation, the perceived value of simulation experiences. 19 Furthermore, the Fornell-Larcker criterion was applied to assess discriminant validity. The square roots of average variance extracted for self-efficacy (0.835) and perceived confidence (0.839) both exceeded their inter-construct correlation (0.592), satisfying the criterion for discriminant validity. 30 These findings suggest that the significant association between self-efficacy and perceived effectiveness is not merely an artifact of construct overlap.
Our study found that students with prior experience in health management simulations reported higher levels of perceived effectiveness. This result is consistent with the findings of a recent comprehensive study highlighting that nursing students viewed previous simulation encounters as instrumental in boosting their confidence, skills, knowledge, and overall competence in engaging in acute and critical care simulations. 31 Such prior exposure has been shown to be particularly beneficial in familiarizing learners with the operation of relevant medical equipment and instruments, thereby reducing procedural anxiety and enhancing technical readiness. 32 Together, these parallel findings underscore the foundational value of simulated practices in building learner preparedness and perceived efficacy across different healthcare disciplines, suggesting that structured prior exposure can serve as a key facilitator of simulation-based educational outcomes.
This study has some limitations. First, the generalizability of the results is constrained by the modest sample size and use of a single sampling site, which may limit representation in relation to broader populations. Second, reliance on self-reported data introduced the potential for response bias, such as social desirability and recall bias. Third, the study design did not allow causal inferences owing to its observational nature. Fourth, this study employed the SET-M, which uses positively worded items and a 3-point Likert scale. This design may limit the expression of neutral or negative views and could contribute to ceiling effects. Finally, although the study examined the perceived effectiveness of computer-based simulation learning, it did not directly assess objective learning outcomes or performance improvements. As Bergamasco and Cruz 21 demonstrated, SET-M scores may not correlate with objective performance assessments or simulation design quality. Although learners' subjective experiences are educationally meaningful in their own right, future research should incorporate objective outcome measures. Future studies should incorporate multi-site sampling, longitudinal designs, and objective performance indicators, including pre- and post-simulation knowledge tests, assessor-rated performance, and decision-making accuracy metrics. Comparative designs contrasting simulation-based learning with traditional teaching or alternative simulation formats would further strengthen the evidence base. Qualitative approaches (e.g., open-ended questions probing ineffective or unhelpful aspects) would capture perspectives that structured scales may miss. Moreover, future research should employ scales with balanced item wording and expanded response options to reduce response framing and better assess actual learning processes.
Conclusions
Computer-based simulation learning allows health management students to experience a full spectrum of health management processes in a controlled environment. The findings suggest that students perceived the computer-based simulation positively, particularly in relation to confidence, preparedness, and self-reported learning. The prebriefing-simulation-debriefing model, implemented through an HMSS system, demonstrates promise as a pedagogical framework for structuring simulation-based education, with perceived effectiveness significantly associated with self-efficacy, knowledge-skills-attitudes gains, and prior simulation experience. These results highlight the importance of fostering learner confidence and preparedness to maximize educational outcomes.
Supplemental material
Supplemental material - Perceived effectiveness of computer-based simulation learning in health management students: A cross-sectional study
Supplemental material for Perceived effectiveness of computer-based simulation learning in health management students: A cross-sectional study by Ren-Ping Gu, Jie Xia, Fang Zhao, Xiang-Dong Peng, Ai-Yong Zhu in DIGITAL HEALTH
Footnotes
Ethical considerations
The studies involving humans were approved by the Institutional Ethics Review Board of Shanghai University of Medicine & Health Sciences. The studies were conducted in accordance with the local legislation and institutional requirements.
Consent to participate
Written informed consent was obtained from all study participants and their proxy respondents.
Author contributions
Conceptualization, AYZ; Data curation, XDP; Funding acquisition, RPG, AYZ; Methodology, RPG, FZ; Writing–original draft, RPG, JX; Writing–review & editing, RPG, AYZ.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University-Industry Collaborative Education Program (grant number 241005095300316) and Education and Scientific Research Project of Shanghai (grant number C2025240). The sponsor had no role in study design; collection, analysis and interpretation of data; writing of the report; or the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used in this study are available from the authors upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.