
Abstract
Objectives
This study examined whether baseline insomnia severity modifies within-person associations of diary-based sleep-continuity and sleep-initiation metrics with next-day daytime heart rate variability (HRV) in a wearable-based dataset.
Methods
We conducted a secondary analysis of a publicly available dataset combining daily sleep diaries with wearable-derived HRV over 4 weeks. The analytic dataset was constructed from the publicly released raw files. Daytime heart rate variability (HRV) was aggregated from eligible 5-minute windows recorded between 09:00 and 23:00, and the primary outcome was daytime RMSSD on the natural log scale. Sleep efficiency was operationalized using a Consensus Sleep Diary (CSD)–style definition that explicitly incorporated wake after sleep onset (WASO). Within-person associations were estimated using participant fixed-effects linear models with standard errors clustered at the participant level. Effect modification was tested using sleep metric × baseline Insomnia Severity Index (ISI), mean-centered, interaction terms. All analyses were restricted to observations meeting prespecified coverage thresholds and day-level complete-case criteria.
Results
The analytic dataset comprised 1,372 diary-days from 49 participants. The primary sleep-efficiency model included 451 person-days from 39 participants. Baseline insomnia symptoms were largely non-severe, and no participant met criteria for severe baseline insomnia. The CSD-style sleep efficiency × baseline ISI interaction was positive (β=0.0060; 95% CI, 0.0023 to 0.0097; P=0.002), and the sleep latency × baseline ISI interaction was negative (β=−0.0034; 95% CI, −0.0051 to −0.0018; P<0.001). Interactions involving WASO and CSD-style sleep duration were not statistically significant.
Conclusions
Baseline insomnia symptom burden modified the associations of diary-based sleep efficiency and sleep latency with daytime RMSSD. The findings support symptom-dependent sleep–HRV coupling in a predominantly healthy cohort, but higher-ISI estimates were based on few participants in the moderate-ISI range and on person-days meeting daytime HRV coverage criteria. These findings should not be extrapolated to populations with severe or clinically diagnosed insomnia.
Keywords
Introduction
Sleep health is increasingly defined as a multidimensional construct of population relevance that includes sleep duration, continuity, timing/regularity, and satisfaction and is associated with cardiometabolic and mental health, and public health outcomes.1–4 Clinical guidelines for chronic insomnia and trials of digital cognitive behavioral therapy for insomnia provide context for management and digital interventions, but the present study is observational rather than interventional.5,6 In digital health research, the interpretability of wearable monitoring depends not only on quantifying sleep and physiology as separate streams, but also on establishing when changes in self-reported sleep correspond to interpretable shifts in autonomic physiology in daily life. Wearable sleep technology is increasingly deployed in clinical and research settings; accordingly, device outputs require validation and interpretation with respect to measurement conditions and behavioral context. 7 Standardized prospective sleep diary frameworks, including the Consensus Sleep Diary (CSD), support consistent recording of key sleep parameters such as sleep onset, wake time, sleep efficiency, and wake after sleep onset (WASO). 8
Heart rate variability (HRV), particularly time-domain indices such as the root mean square of successive differences (RMSSD), is often used in ambulatory settings as a proxy for vagally mediated cardiac autonomic regulation.9,10 Lower HRV has been associated with adverse outcomes across population and clinical studies, and wearable-derived HRV is increasingly incorporated into digital health research. 11 In free-living monitoring, HRV data are susceptible to missingness, variable signal quality, behavioral confounding, and device-specific preprocessing; this makes it necessary to prespecify eligible windows, aggregation rules, and coverage thresholds to support transparent inference. 12 The public dataset analyzed in this study was designed to pair wearable-based HRV summaries with daily sleep diaries, providing a setting in which diary–HRV coupling can be examined under real-world monitoring constraints. 13 The present study was not intended to validate the device-level accuracy of wearable HRV measurement. Instead, it used the released feature-level HRV summaries to examine whether diary-reported sleep–HRV coupling varied according to baseline insomnia symptom burden.
Insomnia symptoms provide a clinically relevant stratification variable for sleep-HRV analyses.14,15 In the present study, sleep continuity is operationalized using diary-derived indices of sleep maintenance and consolidation after sleep is attempted (including sleep efficiency and WASO), whereas sleep latency is treated as a sleep-initiation metric rather than a continuity metric. The hyperarousal model characterizes insomnia as persistent cognitive and physiological activation that may influence autonomic regulation both at night and during the day.14,16,17 Because RMSSD is commonly interpreted as an index of vagally mediated cardiac regulation, the present analysis is framed in terms of cardiac vagal physiology rather than sympathetic activation per se. Within this framework, no unidirectional causal assumption is required; altered cardiac vagal modulation may precede, follow, or co-occur with sleep disruption.
Against this backdrop, the primary question was whether the day-to-day coupling between diary-based sleep metrics and daytime RMSSD was stronger among individuals with greater baseline insomnia symptom burden. Clarifying symptom-dependent coupling may improve the interpretation of wearable HRV by identifying conditions under which diary-reported sleep metrics more closely track cardiac vagal physiology. To address this question, we conducted a secondary analysis of a publicly available dataset pairing daily sleep diaries with wearable-derived HRV. 13 We hypothesized that sleep-continuity and sleep-initiation measures would show stronger within-person coupling with daytime RMSSD among participants with higher baseline ISI scores.
Methods
Study design and data source
We performed a secondary analysis of a publicly available, de-identified dataset that paired daily sleep diaries with wearable-derived HRV feature summaries collected over four weeks in South Korea. 13 The study’s reporting adhered to the STROBE statement for observational studies. 18 The protocol for the source study was approved by the Institutional Review Board of KAIST (KH2020-027), and all participants provided written informed consent. In the present secondary analysis, we used only de-identified records made available through Figshare (https://doi.org/10.6084/m9.figshare.28509740) no new data were collected, and participants were not recontacted. This secondary analysis of publicly available, de-identified data was reviewed by the Ethics Committee of Wuxi Huishan District People’s Hospital, which granted an exemption from full ethics review (Approval No. HYEC-Exempt-202601). In the original study, data collection was conducted in 2021 and included an in-person orientation, followed by four weeks of free-living monitoring and device return. Participants were recruited in South Korea from a university and a research institution via online postings and flyers.
Participants and original data collection
In the original study, 49 healthy adults aged 21–43 years (mean age 28.35 ± 5.87 years; 51% female), who were not undergoing hospital treatment for acute medical, surgical, or psychiatric illness, were monitored for four weeks. For the present secondary analysis, we included participants who provided at least one day of both sleep diary data and eligible daytime HRV windows, yielding an analytic sample of 49 participants. Participants attended an in-person orientation and completed four weeks of free-living monitoring, with daily reminders to facilitate diary completion. The smartwatch was worn on the non-dominant wrist during waking hours and generally removed for charging at night; hence, our analyses focused on daytime HRV.
Study size and sample-size justification
Because this study was a secondary analysis of a fixed, publicly available dataset, no recruitment-based sample-size calculation was performed. The available sample size was therefore determined by the released data, which included 49 participants and 1,372 diary-days. The primary analytic sample was subsequently defined by prespecified HRV coverage thresholds and day-level complete-case criteria. The analyses should therefore be interpreted as exploratory, with the aim of estimating within-person associations and effect modification while explicitly accounting for uncertainty, rather than producing definitive clinical estimates.
Wearable device and HRV feature generation
Physiological sensing in the source study was performed using a commercially available smartwatch and a custom research application. 13 PPG signals were segmented into consecutive 5-minute windows, and the source data descriptor reported HeartPy-based HRV feature generation after preprocessing and quality filtering.13,19 The present analysis used the released feature-level HRV summaries rather than raw photoplethysmography waveforms. Wearable-derived RMSSD was therefore interpreted with caution, and the emphasis was placed on within-person association patterns rather than on absolute clinical thresholds for HRV. 20
Sleep diary measures
Participants completed a daily sleep diary recording bedtime, sleep-onset time, wake time, nocturnal awakenings, and WASO. In this analysis, sleep continuity was operationalized using diary-derived indices of sleep maintenance and consolidation after sleep onset, specifically CSD-style sleep efficiency and WASO. Sleep latency was analyzed separately as a sleep-initiation metric.
CSD-style total sleep time was derived as time in bed minus sleep latency and WASO, and CSD-style sleep efficiency was then calculated as CSD-style total sleep time divided by time in bed. The originally released sleep efficiency variable was retained for sensitivity analyses.
The primary sleep exposures were CSD-style sleep efficiency, sleep latency, WASO, and CSD-style sleep duration. For interpretability, sleep efficiency was scaled per 10-percentage-point increase, sleep latency per 30-minute increase, WASO per 10-minute increase, and sleep duration per 1-hour increase.
Insomnia severity and other questionnaires
Insomnia symptoms were assessed using the Insomnia Severity Index (ISI), administered three times at approximately 2-week intervals. 15 Baseline ISI was specified as the primary effect modifier because exact questionnaire administration dates were not available in the released dataset; therefore, baseline status provided a stable stratification variable for within-person diary–HRV analyses. ISI categories were defined as 0–7, no clinically significant insomnia; 8–14, subthreshold insomnia; 15–21, moderate insomnia; and 22–28, severe insomnia. 15
The dataset also included the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7), which were incorporated into sensitivity analyses to assess whether the findings were robust to adjustment for depressive and anxiety symptoms. 13 The present secondary analysis did not administer questionnaires. No questionnaire items or forms were reproduced; only de-identified scores released in the public dataset were analyzed.
Outcome, exposures, and diary–HRV alignment
Daytime HRV was aggregated from eligible 5-minute wearable HRV windows recorded between 09:00 and 23:00 local time. The primary outcome was log-transformed daytime RMSSD. The primary analysis required at least 24 eligible daytime HRV windows per diary day, a threshold selected to ensure a minimum level of daytime HRV coverage while retaining sufficient repeated observations for within-person modeling.
Sleep diary variables were aligned with daytime HRV summaries from the corresponding diary day, so that the HRV summaries represented daytime autonomic function after the reported sleep episode.
Covariates and missing data
Participant-level characteristics of all participants and the primary analytic sample.
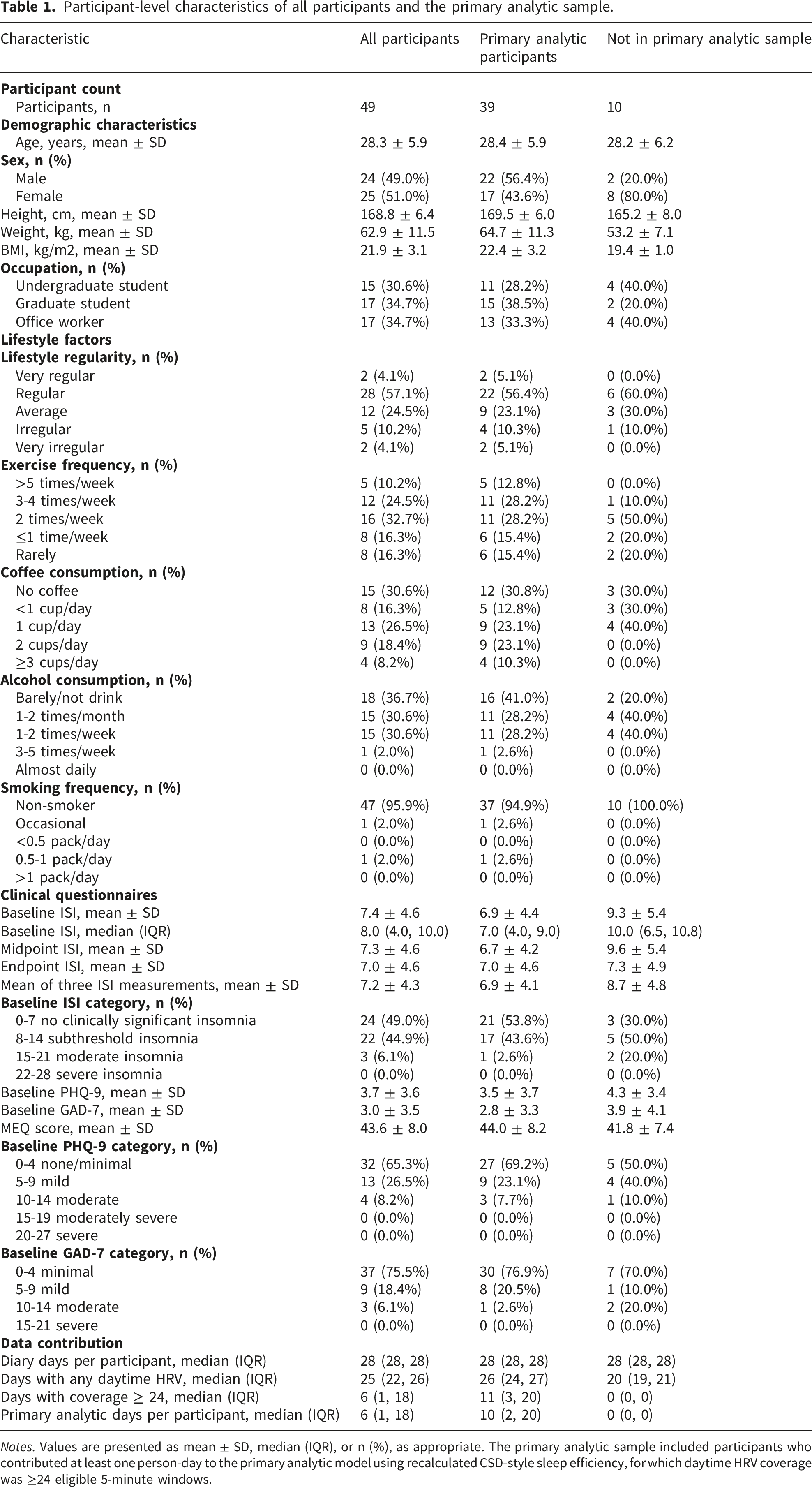
Notes. Values are presented as mean ± SD, median (IQR), or n (%), as appropriate. The primary analytic sample included participants who contributed at least one person-day to the primary analytic model using recalculated CSD-style sleep efficiency, for which daytime HRV coverage was ≥24 eligible 5-minute windows.
Statistical analysis
Within-person associations were estimated using participant-fixed effects linear models with participant-level, cluster-robust standard errors.21,22 Effect modification by baseline ISI was assessed by including sleep metric × baseline ISI interaction terms. Because baseline ISI was time-invariant, its main effect was absorbed by participant fixed effects and was not estimated separately. The main effect of each sleep metric, therefore, reflects the within-person association at the sample mean of baseline ISI. For interpretability, coefficients from log-RMSSD models were expressed as percent changes, calculated as 100 × [exp(β) − 1]. Marginal effects for CSD-style sleep efficiency and sleep latency were estimated across the observed baseline ISI range and summarized in both graphical and tabular form. Statistical significance was assessed using a two-sided threshold of P < 0.05. Because this was a secondary analysis of a fixed dataset, no a priori sample-size calculation was performed; all eligible observations available in the publicly accessible dataset were analyzed.
Sensitivity analyses were conducted to evaluate whether the findings depended on modeling choices, data completeness, or variable definitions. These analyses examined alternative HRV coverage thresholds, alternative covariate sets, released versus recalculated sleep-efficiency definitions, exclusion of extreme sleep-diary values, exclusion of participants contributing only one analytic day, approximate repeated questionnaire-based measures, heart-rate outcomes, reverse-direction models, and between-person associations between baseline ISI and HRV. Participants with at least one complete analytic day were retained in the primary analysis to avoid discarding released observations at the outset; because single-day contributors provide limited within-person information, their exclusion was evaluated as a sensitivity analysis.
Analyses were conducted in Python using pandas and NumPy for data handling, statsmodels for regression modeling, and matplotlib for visualization.
Results
After the analytic criteria were applied, the final data set comprised 1372 sleep diary-days from 49 participants. The primary model for CSD-style sleep efficiency included 451 person-days from 39 participants, and the corresponding sleep-latency model included 454 person-days from 39 participants. Baseline insomnia symptoms were largely within the absent-to-subthreshold range: 24 participants (49.0%) had baseline ISI scores of 0–7, 22 (44.9%) had scores of 8–14, and 3 (6.1%) had scores of 15–21. No participant met the ISI criterion for severe insomnia (22–28) (Table 1). Compared with the full cohort, inclusion in the primary analytic sample was determined mainly by daytime HRV coverage and complete-case requirements. The implications of this reduction in analyzable observations are addressed in the Discussion and summarized in Supplementary Tables S1–S2.
Participant fixed-effects models for baseline ISI modification of sleep diary–daytime RMSSD associations.
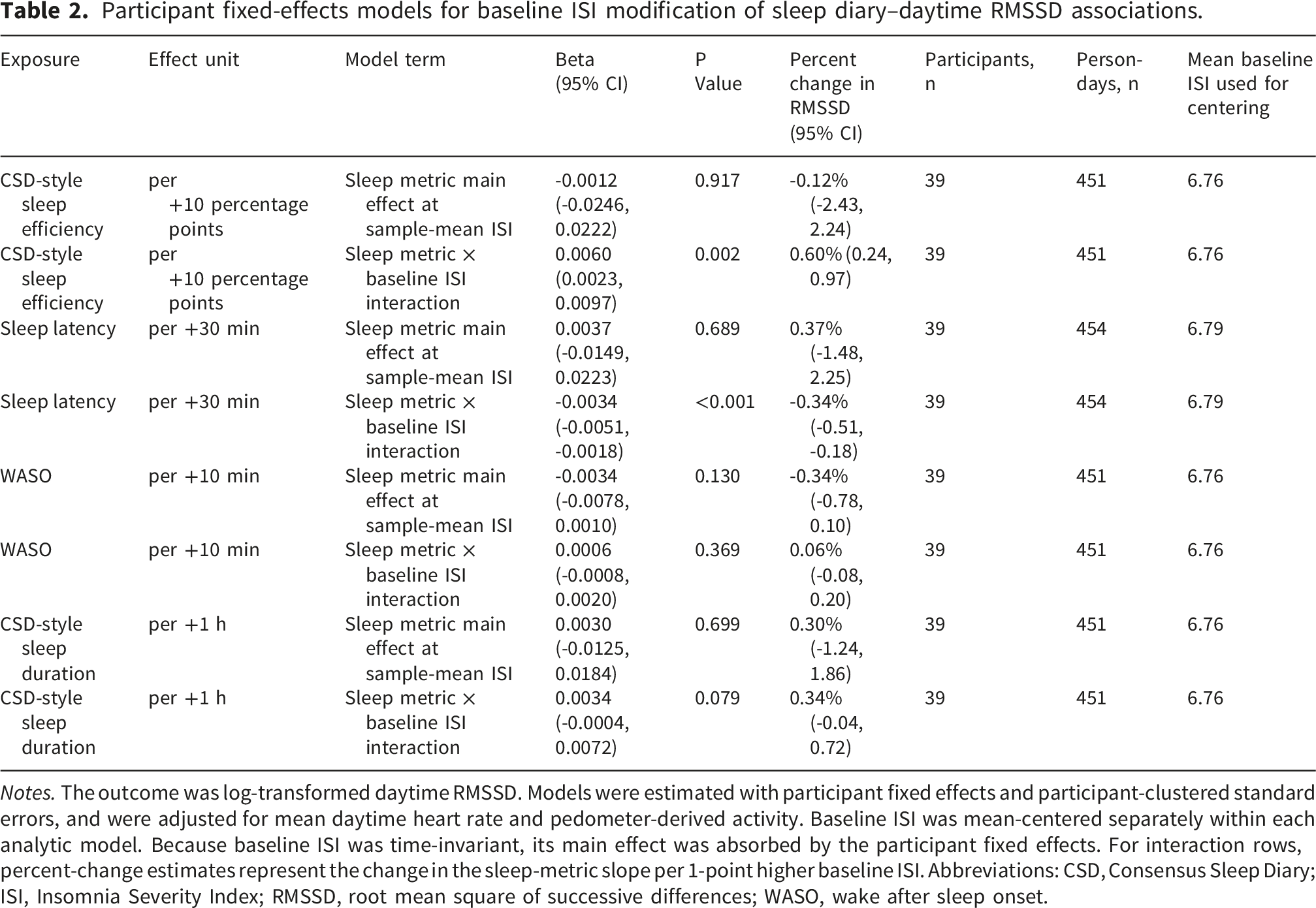
Notes. The outcome was log-transformed daytime RMSSD. Models were estimated with participant fixed effects and participant-clustered standard errors, and were adjusted for mean daytime heart rate and pedometer-derived activity. Baseline ISI was mean-centered separately within each analytic model. Because baseline ISI was time-invariant, its main effect was absorbed by the participant fixed effects. For interaction rows, percent-change estimates represent the change in the sleep-metric slope per 1-point higher baseline ISI. Abbreviations: CSD, Consensus Sleep Diary; ISI, Insomnia Severity Index; RMSSD, root mean square of successive differences; WASO, wake after sleep onset.
No comparable interaction with baseline ISI was observed for WASO. The WASO × baseline ISI interaction was small and not statistically significant (β, 0.0006; 95% CI, -0.0008 to 0.0020; P=0.369). The CSD-style sleep duration × baseline ISI interaction was positive, although the confidence interval crossed zero and the association did not reach the conventional threshold for statistical significance (β, 0.0034; 95% CI, -0.0004 to 0.0072; P=0.079) (Table 2). The four primary sleep metric × baseline ISI interaction estimates are also summarized graphically in Supplementary Figure S1.
Marginal-effect estimates within the observed range of ISI values provided a more direct expression of these interaction terms. A 10-percentage-point higher CSD-style sleep efficiency was associated with a 4.33% (95% CI, 1.86% to 6.86%) higher daytime RMSSD at an ISI value of 14 and an 8.16% (95% CI, 3.84% to 12.67%) higher daytime RMSSD at the observed maximum ISI value. In contrast, each 30-minute longer sleep latency was associated with a -2.09% (95% CI, -3.32% to -0.85%) lower daytime RMSSD at an ISI value of 14 and a -4.10% (95% CI, -5.49% to -2.68%) lower daytime RMSSD at the observed maximum ISI value (Figure 1 and Supplementary Table S3). Baseline insomnia severity modifies day-to-day sleep–HRV coupling. Predicted percent changes in daytime RMSSD across baseline ISI values were estimated from participant fixed-effects models. Panel A presents the estimated RMSSD change per 10-percentage-point higher CSD-style sleep efficiency, whereas Panel B presents the estimated RMSSD change per 30-minute longer sleep latency. Models used daytime HRV values aggregated from 09:00 to 23:00 and required ≥24 eligible 5-minute daytime HRV windows per day. Estimates are restricted to the observed baseline ISI range of 0–20. Shaded bands indicate 95% confidence intervals, and dashed vertical lines mark ISI cut points at 7 and 14. CSD-style sleep efficiency reflects sleep continuity, whereas sleep latency reflects sleep initiation.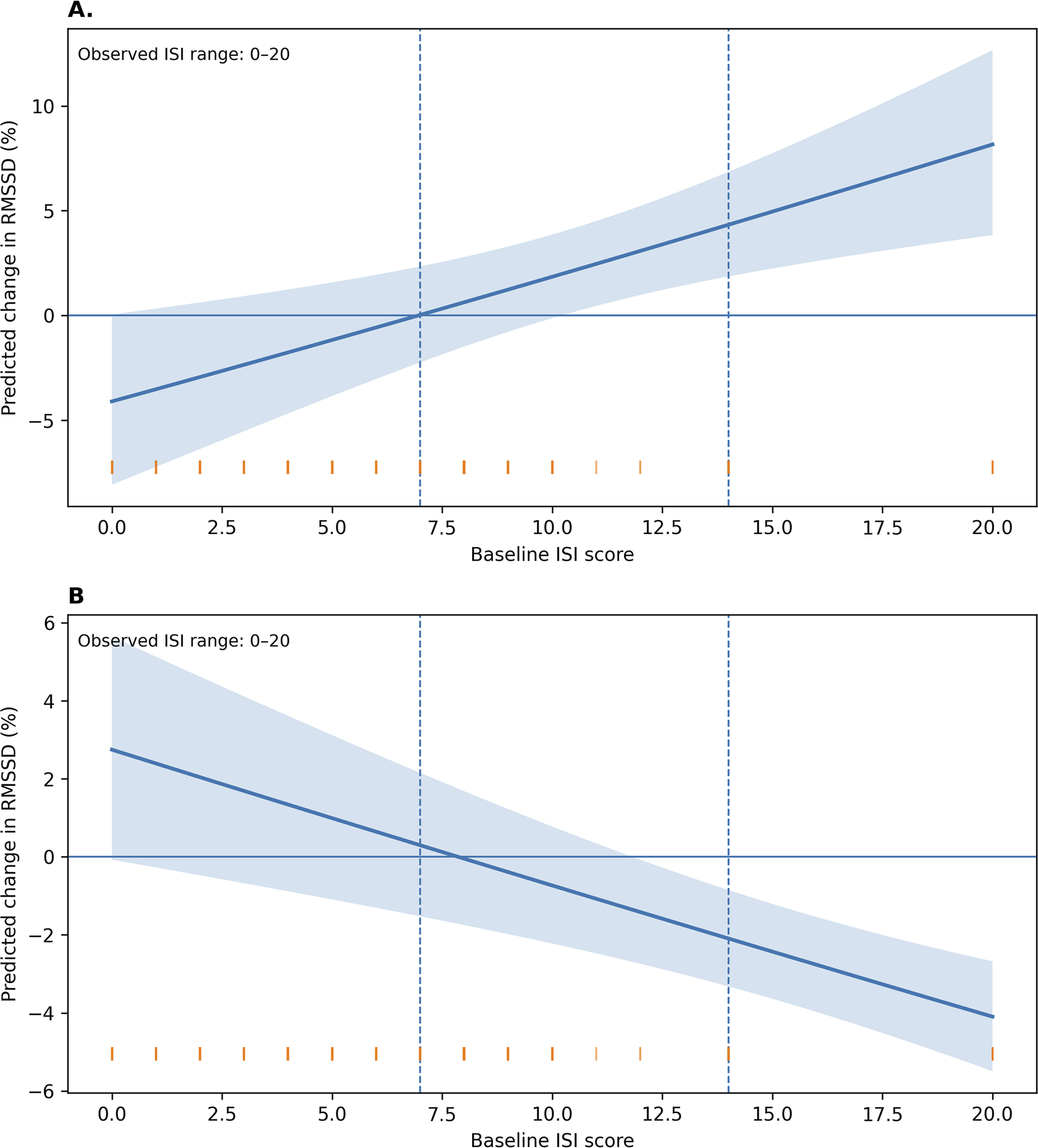
The main interaction patterns were generally retained in sensitivity analyses that used alternative HRV coverage thresholds, different covariate specifications, recalculated rather than released sleep-efficiency values, exclusion of extreme sleep-diary values, exclusion of single-day contributors, and additional adjustment for PHQ-9 and GAD-7 measures (Supplementary Tables S4–S7 and Supplementary Figures S2–S3). Models using mean heart rate as the outcome did not reproduce the same interaction pattern, suggesting that the primary findings were more closely tied to RMSSD-based HRV than to mean heart rate alone (Supplementary Table S8). In exploratory reverse-direction models, daytime log-transformed RMSSD also showed ISI-dependent associations with subsequent sleep-diary measures. The daytime log-transformed RMSSD × baseline ISI interaction was positive for next-night CSD-style sleep efficiency (β=0.1482; 95% CI, 0.0255 to 0.2710; P=0.019) and negative for next-night sleep latency (β=−0.2905; 95% CI, −0.5625 to −0.0185; P=0.037), whereas the corresponding interactions for next-night WASO and next-night CSD-style sleep duration were not statistically significant (Supplementary Table S9). These exploratory findings are consistent with stronger coupling between daytime cardiac vagal physiology and subsequent diary-reported sleep among participants with higher baseline ISI scores. Between-person models of baseline ISI and HRV were exploratory and are reported in Supplementary Tables S10.
Discussion
In this secondary analysis of a free-living wearable dataset, baseline insomnia symptom burden modified the within-person associations of diary-based sleep-continuity and sleep-initiation measures with daytime RMSSD. Higher recalculated sleep efficiency was associated with higher daytime RMSSD, and this association was stronger among participants with higher baseline ISI scores. A similar but opposite pattern was observed for sleep latency: longer sleep latency, a diary-based marker of difficulty initiating sleep, was more strongly associated with lower daytime RMSSD within the same observed ISI range.
The findings are consistent with a sleep health framework in which sleep maintenance and sleep initiation are treated as clinically relevant dimensions rather than interchangeable summary measures. 1 This interpretation is further supported by literature linking insomnia symptoms to hyperarousal, altered cardiac autonomic and vagal regulation, and ecological or wearable approaches to insomnia assessment.23–26 The present results therefore do not indicate a uniform association between diary-based sleep metrics and HRV across all participants. Instead, they suggest that the physiological relevance of sleep continuity measures may vary according to baseline insomnia symptom burden.
Several non-mutually exclusive mechanisms may explain the observed effect modification, although the temporal sequence cannot be determined from this analysis. Because RMSSD is commonly interpreted as an index of vagally mediated cardiac regulation, these findings should be interpreted as relating primarily to cardiac vagal modulation rather than as direct evidence of sympathetic activation. Higher ISI scores may reflect a symptom profile characterized by greater cognitive or physiological arousal,14,16,17 in whom sleep initiation, sleep maintenance, and cardiac vagal regulation may be more closely linked. Under this interpretation, poorer sleep continuity could be accompanied by lower next-day vagally mediated HRV. The exploratory reverse-direction models are consistent with this interpretation because daytime RMSSD showed stronger associations with subsequent sleep-efficiency and sleep-latency measures among participants with higher baseline ISI scores. Nevertheless, altered cardiac vagal modulation may precede poorer sleep, follow sleep disruption, or co-occur with sleep disturbance as part of a shared arousal-related process. For these reasons, the findings should be interpreted as evidence of symptom-dependent sleep–HRV coupling, not as evidence that sleep disruption causes next-day autonomic change.
A strength of this analysis is the use of a publicly available wearable dataset that combined repeated sleep diaries with standardized HRV feature extraction. The participant fixed-effects design reduced confounding by time-invariant participant characteristics, and segment-level quality filtering and prespecified HRV coverage thresholds made the availability of usable physiological data explicit.13,21,22 This issue is particularly relevant in free-living wearable studies, where missingness and signal-quality filtering are integral to the measurement process rather than secondary technical issues.
The distinction between within-person coupling and between-person HRV differences should also be emphasized. In between-person sensitivity analyses, baseline ISI was not statistically significantly associated with participant-mean daytime HRV. The main finding therefore does not appear to reflect a simple pattern in which participants with higher ISI had uniformly lower HRV. Rather, it concerns how day-to-day deviations in sleep continuity were associated with daytime RMSSD within the same participant, conditional on baseline insomnia symptom burden.
Several limitations should be considered. The cohort consisted of healthy adults and did not include participants with severe baseline insomnia; therefore, these results should not be extrapolated to patients with severe insomnia or clinically diagnosed sleep disorders. Monitoring was also conducted during the COVID-19 era, when sleep, activity, stress, and cardiac vagal physiology may have been affected by broader contextual factors. Because the released dataset did not include individual-level variables that captured these contextual influences, they could not be modeled directly. The reduction from the full diary dataset to the primary analytic sample was substantial and reflected real-world HRV coverage and complete-case requirements. Selection bias may have occurred if participants or days with sufficient daytime HRV coverage differed systematically from those excluded. Possible contributors include non-wear, device removal during daytime activities, motion artifacts, physiological or proprietary signal-quality filtering, and other behavioral factors.
Additional limitations relate to daytime wearable HRV measurement and unmeasured time-varying behaviors. This analysis relied on publicly available feature-level HRV summaries and could not independently validate device-specific accuracy of daytime RMSSD. Daytime HRV is sensitive to physical activity, posture, psychological stress, caffeine intake, alcohol use, and related behaviors. Although the models adjusted for mean daytime heart rate and pedometer-derived activity, and for baseline alcohol, coffee, smoking, and exercise patterns, daily alcohol and caffeine intake were not available. Residual behavioral confounding, therefore, remains possible. Sensitivity analyses generally supported the main interaction patterns across alternative HRV coverage thresholds, covariate specifications, recalculated versus released sleep-efficiency values, exclusion of extreme sleep-diary values, and adjustment for PHQ-9 and GAD-7 measures. Because exact questionnaire administration dates were unavailable, analyses incorporating approximate time-varying questionnaire variables should be regarded as exploratory. Reverse-direction models were also exploratory and should not be interpreted as causal evidence.
Clinical reviews of insomnia, guidelines, and reviews of behavioral and digital cognitive behavioral therapy provide a clinical context.27–29 The present secondary analysis did not evaluate insomnia interventions. Accordingly, the findings should not be used to infer treatment effects or to guide intervention selection.
Conclusion
In this free-living wearable dataset, baseline insomnia symptom burden modified the within-person associations of diary-reported sleep efficiency and sleep latency with next-day daytime RMSSD. Higher sleep efficiency showed stronger positive coupling with RMSSD, whereas longer sleep latency showed stronger negative coupling with RMSSD among participants with higher observed baseline ISI scores. These findings provide exploratory evidence of symptom-dependent sleep–HRV coupling in a predominantly healthy cohort spanning the range from absent to non-severe insomnia. Further validation is needed in larger cohorts enriched for clinically diagnosed insomnia and a broader range of sleep-disorder severity, particularly because the higher-ISI estimates in this dataset were based on a small number of participants with moderate insomnia symptoms and on a daytime HRV analytic sample defined by coverage criteria.
Supplemental material
Supplemental material - Insomnia severity modifies diary-based sleep-continuity and sleep-initiation associations with next-day daytime HRV in a real-world wearable dataset
Supplemental material for Insomnia severity modifies diary-based sleep-continuity and sleep-initiation associations with next-day daytime HRV in a real-world wearable dataset by Xiangming Meng, and Mingjing Cai in DIGITAL HEALTH.
Footnotes
Acknowledgments
We thank the original dataset authors for making the de-identified data publicly available.
Ethical considerations
This secondary analysis of a publicly available, de-identified dataset was approved by the Ethics Committee of Wuxi Huishan District People’s Hospital with exemption from full ethics review (Approval No. HYEC-Exempt-202601). No new data were collected, no participants were contacted, and no questionnaires or proprietary tools were administered by the present investigators. The original study protocol received Institutional Review Board approval from KAIST (KH2020-027).
Consent to participate
Participants provided informed consent during the original data collection.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset analyzed in this study is publicly available and de-identified. It can be accessed via Figshare (![]() )
30
. The dataset and associated data descriptor were released under a Creative Commons Attribution 4.0 International License, permitting reuse with appropriate attribution.
)
30
. The dataset and associated data descriptor were released under a Creative Commons Attribution 4.0 International License, permitting reuse with appropriate attribution.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.