
Abstract
With the rapid ascent of video-based social media, platforms like TikTok and YouTube have become primary sources of ophthalmic health information, shaping both patient perceptions and professional development. This narrative review synthesizes evidence from 76 empirical studies to evaluate the quality and reliability of ophthalmic video content. We identify a persistent engagement paradox, where algorithm-driven metrics such as view counts and shares often favor simplified, emotionally resonant, or visually striking narratives over medically accurate and balanced counseling. Clinician-produced content generally showed higher clinical integrity in the included studies, but it often received lower engagement than peer-led experiential narratives. Beyond patient-facing education, we explore the emerging role of video platforms as professional-facing education for residents, highlighting the risks of survivor bias in unedited or curated operative footage. Furthermore, the visual-centric nature of ophthalmology introduces unique ethical challenges, particularly regarding the anonymization of recognizable facial features and the permanence of digital consent. As Generative AI introduces new risks of sophisticated deepfake misinformation, this review emphasizes the urgent need for multi-modal assessment tools and active professional stewardship to ensure the integrity of digital eye care.
1. Introduction
Social media is now a common place where people look for health information.1,2 Many people use it before they visit a clinic. They also use it after a visit to check advice and to compare experiences. 3 Public health crises, including outbreaks of acute hepatitis of unknown origin in children, poliomyelitis during the COVID-19 pandemic, and delayed measles vaccination, have illustrated how rapidly evolving health threats and service disruptions can intensify the need for accurate, timely, and accessible health communication.4–6 In addition, inequities in specialist care for underserved populations may further increase patients’ dependence on digital information sources before or after clinical encounters. 7 This reliance underscores the critical importance of designing health communication tools that are not only evidence-based but also culturally responsive, linguistically appropriate, and accessible across varying levels of digital literacy and health numeracy.
This change is stronger in video platforms. Short video apps such as TikTok spread messages fast because the videos are easy to watch and easy to share. The platform also recommends content based on viewing history. So, a single video can reach many users in a short time. At the same time, YouTube remains a major source of longer health videos. 8 In some regions, platforms such as Bilibili also play an important role. These platforms together shape what patients learn about eye disease and eye care. 9
Eye health is a special case in online communication. 10 Many eye conditions involve symptoms that people can see and feel. People worry when vision changes, so they often search online right away. 10 Topics such as myopia prevention, dry eye, cataract surgery, refractive surgery, retinal disease, and eye injections are common in video feeds. Videos can explain these topics well because they can show signs, tests, and procedures. 11 However, the same visual strength can also increase risk. A clear and confident video may still be wrong. Some videos leave out key facts. Some mix education with marketing. Some share personal stories as if they are medical advice. These problems matter because eye diseases can be time sensitive. Delays can lead to avoidable vision loss. Inaccurate advice can also lead to unsafe self-care. It can create false hopes about surgery results. It can increase fear of needed treatment. It can also reduce trust in clinicians and in evidence-based care. 12
Many studies in this area suggest a clear gap between what users watch and what patients need for safe decisions. View counts and popularity often reflect entertainment value, strong emotions, or simple messages, not medical accuracy. 13 This creates a practical challenge for ophthalmology, where advice about symptoms, urgency, and treatment choices can directly affect outcomes. 14 The purpose of this narrative review is to describe what ophthalmic content on major video platforms looks like today and what it means for patient care. It aims to evaluate overall information quality and reliability, to summarize how engagement relates to quality, and to identify common patterns of incomplete or misleading messages. It also aims to outline practical directions for clinicians, institutions, and platform governance to improve the safety and usefulness of video-based eye health information.
2. Method
2.1. Review design
This review was designed as a structured narrative review. The objective was not to estimate pooled effects or formally grade the certainty of evidence, but to synthesize empirical literature on ophthalmology-related video-based social media content and to identify recurring themes related to information quality, engagement dynamics, misinformation risk, ethical considerations, and professional education. “Short-form video” refers specifically to ultra-brief, algorithmically-curated visual content (typically under 60–180 seconds) optimized for mobile consumption on platforms such as TikTok or YouTube Shorts, distinguished from traditional long-form educational tutorials by its emphasis on rapid engagement and fragmented messaging. We use the terms “patient-facing education” and “professional-facing education” to distinguish between content primarily intended for patients or caregivers and content intended for ophthalmologists, trainees, or other eye-care professionals.
2.2. Search strategy and study selection
We searched PubMed and Web of Science Core Collection for empirical studies evaluating ophthalmology-related content on video-based social media platforms. The search combined ophthalmology-related terms with platform- and video-related terms, together with terms related to misinformation, information quality, reliability, accuracy, and commonly used assessment instruments. The full search strategy is provided in Supplementary Material 1.
Studies were eligible if they met the following criteria: (1) empirical evaluation of ophthalmology- or eye health-related content; (2) assessment of video-based social media platforms, including YouTube, TikTok, Instagram, Bilibili, Kwai, Douyin, YouTube Shorts, or Instagram Reels; and (3) reporting of at least one structured assessment related to information quality, reliability, accuracy, educational value, misinformation, content characteristics, uploader source, or engagement metrics. Studies were excluded if they were not ophthalmology-related, did not evaluate video-based social media content, lacked an empirical assessment framework, were commentaries or purely conceptual articles, or were unavailable in full text.
The search retrieved 141 records from PubMed and 280 records from Web of Science. After cross-database deduplication by article title, 377 unique records remained. Title and abstract screening was performed independently by two reviewers according to the predefined eligibility criteria. Records considered potentially eligible by either reviewer were retained for full-text assessment. Full-text assessment was also performed by two reviewers, and disagreements were resolved through discussion; unresolved discrepancies were adjudicated by a third senior reviewer. Title and abstract screening retained 84 studies for full-text assessment. During full-text retrieval, eight otherwise eligible studies were unavailable and were excluded. The final synthesis included 76 studies (Figure 1). PRISMA-style flow diagram of study identification and selection.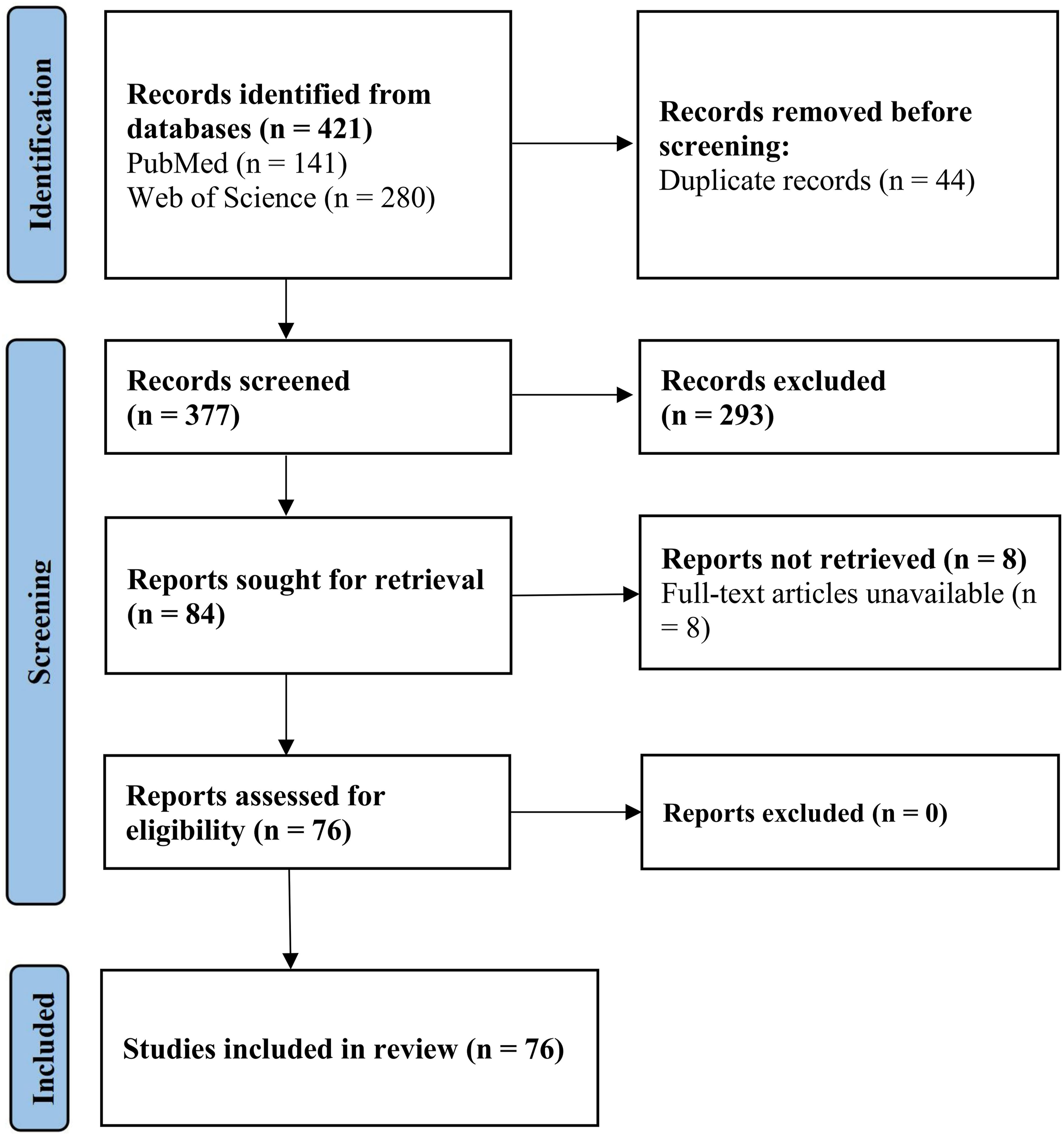
For each included study, data extraction was performed using a predefined extraction form. We extracted publication year, first author, platform, ophthalmic subspecialty or topic area, number of videos assessed, uploader or source categories when available, evaluation instruments, quality or reliability outcomes, engagement metrics, and main findings relevant to health communication or education. One reviewer performed the initial extraction, and a second reviewer checked the extracted data for accuracy and completeness. Discrepancies or uncertain items were resolved through discussion. Extracted information was summarized in evidence-mapping tables, including the characteristics of included studies, the distribution of studies across platforms and ophthalmic topic groups, and the frequency of evaluation instruments.
Final themes were generated through an iterative narrative synthesis process. After data extraction, the included studies were grouped by platform type, ophthalmic topic, target audience, and assessment focus. Recurring findings were then compared across studies to identify cross-cutting concepts, including information quality, source effects, engagement–quality mismatch, commercialization, misinformation risk, privacy and consent, professional education, and methodological limitations of existing assessment tools. These concepts were discussed among the review team and consolidated into the final narrative themes. Themes were retained when they were supported by multiple included studies or when they represented clinically important emerging issues in ophthalmic digital communication.
2.3. Structured descriptive appraisal of the evidence base
Given the narrative-review design and the methodological heterogeneity of the included studies, we did not apply a formal risk-of-bias tool or certainty-of-evidence framework. Most included studies were cross-sectional content analyses of publicly available videos and differed in platform, search strategy, sampling approach, scoring instrument, and engagement metrics, which limited the applicability of a single standardized appraisal tool.
Distribution of included studies across platforms and ophthalmic topic groups.
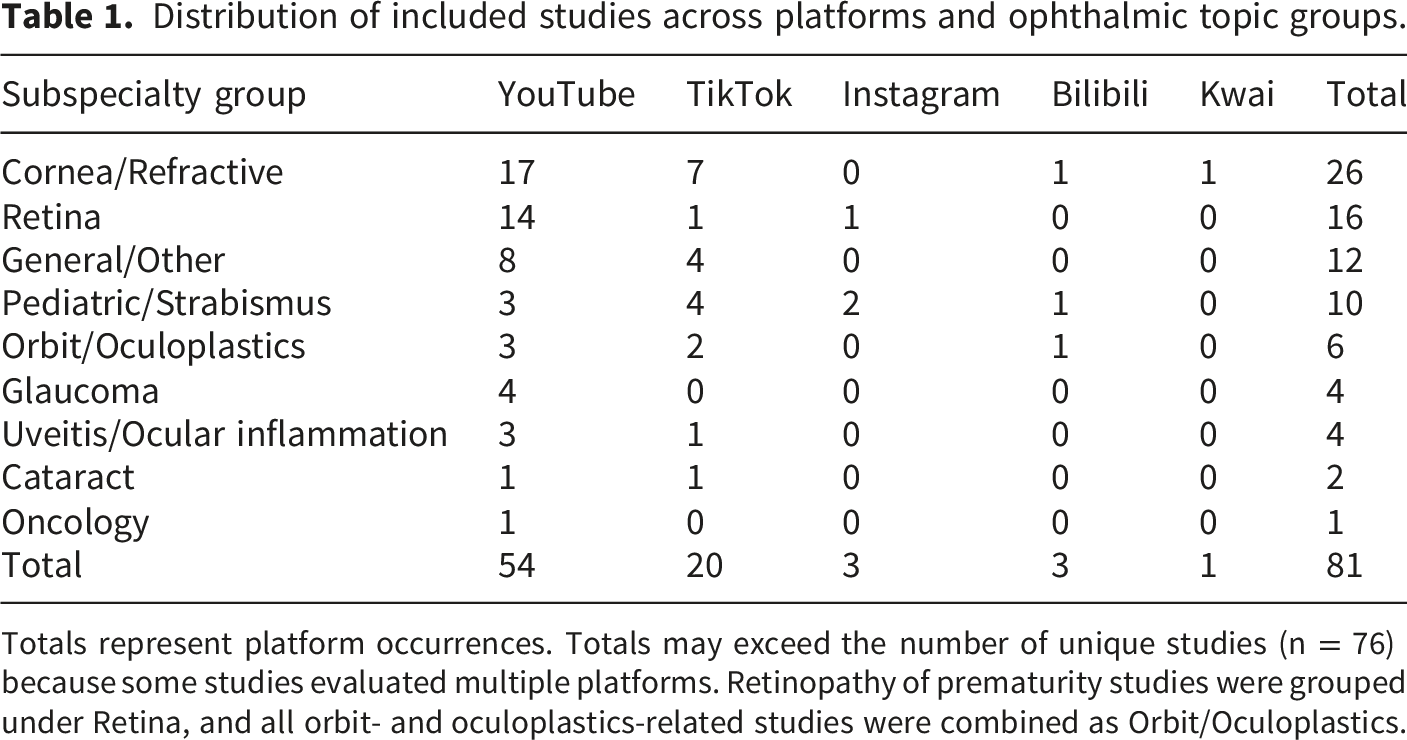
Totals represent platform occurrences. Totals may exceed the number of unique studies (n = 76) because some studies evaluated multiple platforms. Retinopathy of prematurity studies were grouped under Retina, and all orbit- and oculoplastics-related studies were combined as Orbit/Oculoplastics.
Frequency of evaluation instruments used across included studies.
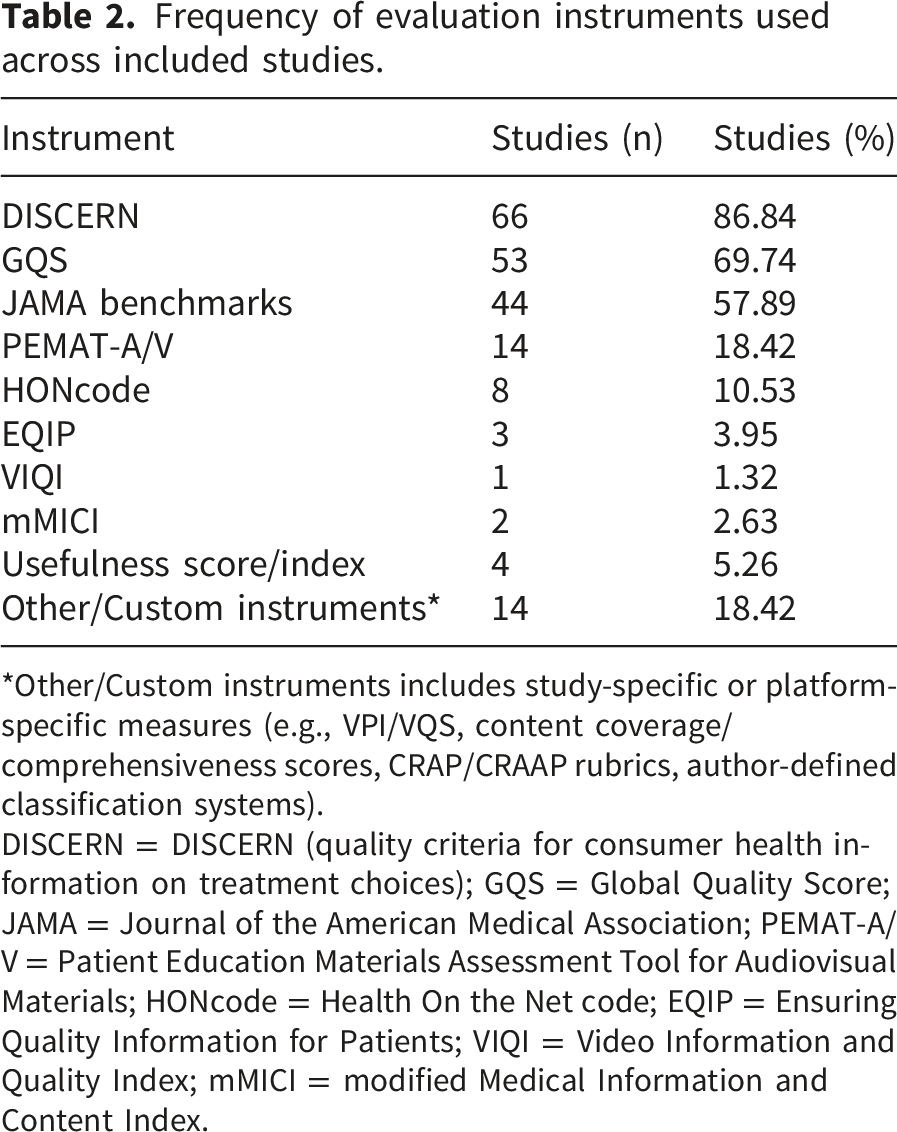
*Other/Custom instruments includes study-specific or platform-specific measures (e.g., VPI/VQS, content coverage/comprehensiveness scores, CRAP/CRAAP rubrics, author-defined classification systems).
DISCERN = DISCERN (quality criteria for consumer health information on treatment choices); GQS = Global Quality Score; JAMA = Journal of the American Medical Association; PEMAT-A/V = Patient Education Materials Assessment Tool for Audiovisual Materials; HONcode = Health On the Net code; EQIP = Ensuring Quality Information for Patients; VIQI = Video Information and Quality Index; mMICI = modified Medical Information and Content Index.
3. The landscape of ophthalmic social media: Content patterns and characteristics
3.1. Common chronic conditions and lifestyle-oriented content: The tension between high traffic and commercialization
Content on myopia, dry eye disease, and thyroid eye disease frequently becomes highly visible on short-form platforms, particularly when it can be framed as daily-life advice and quick self-management tips.9,15 This visibility is not accidental. These topics are easy to package into short clips that match the attention patterns of algorithm-driven feeds. 16 As a result, users are repeatedly exposed to symptom checklists, home care routines, product recommendations, and simplified “do and do not” messages that require little background knowledge to understand. 17
Across studies that assessed ophthalmic videos using established scoring systems, a recurrent pattern is content polarization by uploader type. Health care professionals and institutional accounts more often adopt an educational approach that covers basic definitions, common symptoms, and guideline-consistent management options. In myopia-focused content, clinician-produced videos are more likely to describe risk factors and prevention strategies in a structured way. 11 In contrast, videos produced by non-professional creators or accounts with commercial incentives more often emphasize “vision training,” device-based interventions, or product-centered narratives.18,19 These videos can be compelling and highly shareable, but they often provide limited scientific justification and less balanced discussion of uncertainty and contraindications. For dry eye disease, YouTube-based analyses suggest that even when videos are frequently produced by clinicians, the content tends to emphasize symptoms and general management more than diagnostic standards, differential diagnosis, and escalation thresholds. 20
Overall, available studies generally portray information quality in these lifestyle-oriented areas as modest and inconsistent, with short-form platforms amplifying content that is easy to consume rather than content that is complete. This creates an environment in which users can receive frequent exposure to plausible recommendations, but still remain under-informed about diagnostic framing and evidence hierarchy. 14
3.2. Surgical and interventional content: Expectation management and the appeal of visual demonstration
Surgical topics such as refractive procedures, cataract surgery, retinal detachment surgery, vitrectomy-related care, and keratoconus interventions are strongly driven by the visual nature of ophthalmology. Video is uniquely well-suited to demonstrate operative steps, show anatomical concepts, and illustrate postoperative experiences. 2 Consequently, YouTube remains a primary venue for longer procedural explanations and for content that resembles a tutorial. At the same time, short-form platforms increasingly host patient experience narratives, particularly for elective procedures such as LASIK-related surgery, where the emotional arc of decision-making and early recovery fits well with short clips and personal storytelling.21,22
Despite the abundance of videos, several disease-specific analyses reported similar limitations in patient-facing surgical education. Many videos are rated as low quality or low utility when judged against tools that emphasize balanced discussion of indications, alternatives, risks, and expected outcomes. This concern appears in studies of cataract surgery videos, retinal detachment surgery videos, and other procedure-focused materials.23–25 A common weakness is incomplete expectation management. Videos may highlight “success stories,” technical visuals, or simplified claims of rapid recovery, while devoting less attention to contraindications, variability in outcomes, realistic timelines, and the trade-offs that matter most to patients.
The literature also suggests that professional perspective and patient perspective contribute different strengths and different blind spots. Clinician-produced videos tend to perform better when assessments prioritize accuracy, procedural detail, and risk disclosure. 22 However, these videos can become overly technical and may not address practical concerns that patients often prioritize, including daily functioning, fear and uncertainty, recovery milestones, and how to interpret postoperative symptoms. Patient-produced videos often fill this gap by providing lived experience and peer support, but they can unintentionally generalize from individual outcomes or normalize marketing narratives, especially when content is sponsored or closely linked to commercial branding. 26 Together, these studies indicate that surgical content is plentiful but uneven, and that the most visible videos do not consistently deliver comprehensive counseling that supports informed consent and realistic expectations.25,27
3.3. Content for vulnerable groups and caregiver audiences: Emotional resonance and heightened risk of misinformation
A distinct content ecology emerges in pediatric ophthalmology and in chronic conditions that require long-term follow-up, where the primary audience is often anxious caregivers or patients facing sustained uncertainty. Studies examining social media content on strabismus, amblyopia, retinopathy of prematurity, and childhood glaucoma commonly reported a related structural issue.28–30 High emotional stakes increase engagement, and engagement-friendly narratives may crowd out careful clinical framing. This is especially relevant when families seek quick answers about prognosis, developmental outcomes, and whether non-surgical interventions can substitute for professional care.
Within this space, misinformation risk is repeatedly observed in content that promotes unverified vision therapy or broad claims about visual training for learning or developmental problems. 31 Such claims are frequently disseminated by non-specialists and are presented with high confidence, simple success stories, and appealing before-and-after narratives. Several analyses also highlight that high-quality clinician videos can receive lower engagement than experiential content, which suggests that caregiver audiences may not be systematically guided toward the most reliable material.28,32 These observations suggest a clinically important mismatch between medically responsible communication and algorithmically rewarded content.
At the same time, the literature emphasizes that social media is not only an information source. 2 It is also a space for emotional processing and community building. In at least one TikTok analysis of strabismus-related content, patient experience posts represented more than half of the videos, which underscores the importance of peer narratives in shaping perceptions of stigma, treatment burden, and recovery.32,33 This community function can be valuable, but it also increases the need for credible guidance that helps caregivers interpret stories without mistaking them for general medical advice. For complex conditions such as retinopathy of prematurity, YouTube-based evaluations suggest that available videos are often insufficient in quality and structure to meet parental needs.30,34 This gap suggests an important role for academic institutions and professional societies to provide caregiver-oriented materials that are both emotionally sensitive and clinically rigorous, with explicit guidance on urgency, follow-up, and red-flag symptoms.
4. Uploader sources and the engagement paradox
4.1. Source effects and the displacement of trust
Across ophthalmic topics, uploader source remains one of the most consistent correlates of informational quality. Videos produced by health care professionals, academic institutions, and non-profit organizations more often present clinically structured education, including clearer definitions, more balanced discussion of management options, and stronger alignment with evidence-based recommendations. 35 However, source credibility does not invariably guarantee content exhaustiveness.36,37 Even professional videos may foreground symptoms and general advice while giving limited attention to diagnostic thresholds, uncertainty, contraindications, and when escalation to in-person assessment is warranted.28,38
We interpret the prominence of patient narratives and influencer-led content as a potential form of trust displacement, in which viewers may rely more on perceived authenticity than on traditional medical authority. 39 Patient influencers and experience-based creators can be perceived as more authentic because their stories resemble the viewer’s own concerns. This dynamic is particularly visible in ophthalmology, where stigma, appearance-related anxiety, and fear of irreversible vision loss can make narrative medicine a powerful credibility currency.32,40 Empirically, this “trust displacement” aligns with observations that patient experience posts dominate parts of pediatric ophthalmology and strabismus-related content, while non-professional advice also circulates widely in myopia prevention discussions. 28 These narratives can provide community support and reduce isolation, but they can also generalize individual outcomes into implicit guidance and amplify misinformation risk when clinical context is missing.
4.2. The engagement paradox and platform-driven simplification
A second recurring observation is the engagement–quality mismatch, which we refer to as the “engagement paradox.” Several platform-specific evaluations reported that views, likes, comments, and shares did not consistently correspond to educational quality, and some studies observed inverse associations in specific contexts. 27 This preferential propagation may reflect platform-level incentives rather than random variation. Recommendation systems may reward watch time and emotional response, which is consistent with the observed misalignment between popularity and educational quality.41,42
This mechanism has distinct ophthalmic specificity. Eye care is unusually “visual-first,” and short video ecosystems are primed to amplify visual symbols that suggest immediacy and certainty. Examples that repeatedly appear in platform content include refractive surgery clips that imply instant transformation after LASIK or SMILE, and highly shareable procedural visuals used in chronic symptom management. 42 These formats can create an impression of simple solutions while downplaying surgical risk trade-offs, variability in outcomes, or the long time horizon of chronic disease management.
Short-form constraints further intensify distortion. Many ophthalmic conditions rely on anatomy and pathophysiology to explain risk and to guide safe decisions, for example, glaucoma mechanisms, 43 corneal biomechanics 25 in keratoconus, 22 or long-term behavioral drivers in myopia control. 9 These concepts compete poorly in fragmented videos that prioritize a single takeaway, a single product, or a single personal story. As a result, content may default to oversimplified heuristics that are easier to watch but harder to translate into safe care-seeking behavior.
4.3. Platform architecture, ecosystem differences, and cultural context
Differences in ophthalmic video quality across platforms may partly reflect platform architecture. Short-form, feed-driven platforms such as TikTok and Kwai emphasize rapid viewing, emotional response, and algorithmic recommendation.44,45 These features can improve reach and accessibility, but they may also compress clinical reasoning into simplified messages and amplify visually striking, emotionally resonant, or product-centered claims. 46 In ophthalmology, this is particularly relevant because procedural images, visible symptoms, and before-and-after narratives can appear persuasive even when clinical context is incomplete.9,14 By contrast, YouTube functions more as a searchable long-form archive, allowing more detailed explanations, procedural demonstrations, and professional-facing surgical learning. 47 However, longer format does not ensure higher quality, because YouTube videos may still contain commercial intent, selective case presentation, outdated information, or insufficient discussion of risks and contraindications. 48
Cultural and regional differences should also be considered. Chinese platforms such as Bilibili, Douyin, and Kwai operate within media ecosystems, user communities, and public-health priorities that differ from those of Western platforms. Comparative digital health communication research has shown that visual health discourse may vary across countries, languages, and platform environments, supporting the need to interpret online health content within its cultural and media context. In China, myopia prevention and child eye health have become prominent public-health priorities, reflected in national eye health plans and multi-sectoral policies targeting childhood and adolescent myopia.49,50 This context may partly explain why myopia prevention and child vision care receive substantial attention in Chinese short-video environments. Recent studies of Chinese platforms have specifically evaluated myopia-related videos on TikTok, Bilibili, and Kwai, and reported suboptimal or variable information quality despite high public-health relevance.9,11 Because current evidence remains uneven across platforms, diseases, and cultural settings, future studies should use platform-specific and culturally contextualized evaluation frameworks rather than assuming that findings from YouTube or Western TikTok can be directly generalized to Chinese video platforms. 51
4.4. Covert commercial intent and source signaling as practical levers
Covert commercial intent is an under-addressed driver of both engagement and misinformation risk.52,53 In several high-interest ophthalmic areas, particularly elective procedures and chronic symptom markets, videos that appear educational may function as indirect marketing for clinics, devices, or service packages, while conflicts of interest are not consistently disclosed. 52 This blurs the boundary between education and promotion and can mislead viewers who interpret confident delivery and professional aesthetics as clinical endorsement.
In this environment, source signaling becomes a practical lever for harm reduction. Clear credential disclosure, transparent conflict-of-interest statements, and institution-linked provenance can help viewers interpret content more appropriately. 54 Yet source signaling alone is insufficient if high-quality videos remain less discoverable than sensational content. 55 These observations suggest a dual strategy. The first is to improve the completeness and actionability of professional content without sacrificing accessibility and narrative connection. The second is to strengthen platform and professional standards for disclosure and labeling, particularly for commercially adjacent ophthalmic content, so that users are not forced to infer credibility from popularity cues that are poorly aligned with medical quality. 52
4.5. The ethical dimension: Patient privacy and digital consent
The visual-first nature of ophthalmology introduces unique ethical challenges regarding patient privacy. 10 Unlike other specialties where cases can be easily de-identified, ocular conditions often involve recognizable facial features (e.g., strabismus, ptosis) that make complete anonymization difficult.56,57 This raises critical concerns about informed consent, particularly for vulnerable populations such as pediatric patients, whose images may be permanently archived on social platforms without their future agency in mind. 58 Furthermore, the commercial incentive to showcase dramatic “before-and-after” results can inadvertently prioritize engagement over dignity. 54 Consequently, current ethical frameworks may need to evolve to better address the permanence and limited controllability of algorithmic distribution.
5. Professional education and surgical learning: An emerging subtheme
Beyond patient-facing education, a smaller but clinically relevant subset of the included literature addressed the use of video platforms for professional education and surgical learning. Compared with the broader literature on patient-oriented information quality and engagement, the evidence base for professional-facing education learning was more limited and was therefore interpreted as an emerging subtheme rather than a fully established major review domain. The evidence map further clarified the scope of this subtheme. Among the 76 included studies, only two studies directly framed video platforms as resources for ophthalmic professional education or surgical training, both focusing on vitreoretinal surgery training on YouTube.59,60 In Table S1, these studies were categorized under retina and assessed YouTube videos, with sample sizes of 392 and 125 videos, respectively. By contrast, most included studies evaluated patient-facing information quality, reliability, content characteristics, or engagement. This distribution supports interpreting professional-facing education learning as an emerging subtheme rather than as a mature evidence domain equivalent to patient-facing health communication.
Platform relevance differed between these two audiences. Short-form platforms such as TikTok and related feeds were more commonly discussed in relation to patient-facing communication, rapid dissemination, and engagement dynamics. 14 By contrast, YouTube appeared more relevant to professional learning because its longer video format, higher-resolution surgical footage, and tutorial-like structure can better support procedural explanation, replay, and comparison of technique variants. 47 In practice, YouTube has evolved into an informal but expansive archive of surgical footage, operative demonstrations, and technique pearls. 61 Many residents use it to supplement formal didactics, wet labs, and supervised cases, leveraging platform advantages for procedural learning: replaying critical steps, comparing technique variants across surgeons and systems, and visualizing intraoperative decision points that are difficult to convey in text-only resources.62,63
The educational utility of surgical videos is also shaped by technical presentation. Three-dimensional recordings and other depth-enhancing formats have been reported to improve spatial reasoning and step comprehension, which may be particularly relevant for depth-dependent microsurgical tasks such as phacoemulsification and vitrectomy.64,65 By clarifying tissue planes, instrument trajectories, and hand–eye coordination, these formats can lower the cognitive barrier for novices and enhance preoperative cognitive priming before entering the operating room. 66
However, the open-library structure that enables broad access also introduces important limitations for professional-facing education training. Even when content is intended for professional audiences, quality varies widely in completeness, safety framing, and transparency regarding case selection, adverse events, and alternative maneuvers. A recurrent concern is potential selection or “survivor” bias: surgical videos may preferentially showcase uncomplicated or highly successful cases while underrepresenting intraoperative challenges, error recovery, and complication management, such as posterior capsule rupture, zonular weakness, IOL-related issues, or patient-cooperation constraints. 67 Such non-standardized surgical maneuvers, or edited narratives that truncate decision-making under uncertainty, may create an exaggerated impression of procedural simplicity and could encourage premature imitation without appropriate supervision. 68 Compounding this concern, most open video platforms lack standardized peer review, consistent reporting checklists, or accreditation signals that could help learners distinguish exemplary teaching material from idiosyncratic demonstrations. 69
Taken together, the available evidence supports a cautious and balanced interpretation. Although video platforms may meaningfully complement surgical training, they should be viewed as adjuncts rather than stand-alone curricula. Their use in professional education should ideally be integrated into institutional guidance, including curated playlists, minimum reporting standards, explicit disclosure of case selection and editing, and structured discussion of indications, pitfalls, and complication management. This framing is consistent with our interpretation of professional-facing education learning as an emerging subtheme rather than a mature evidence domain.
6. Methodological challenges: Applying static metrics to dynamic media
The rapid evolution of ophthalmic video content highlights a persistent gap in evaluative methodology. Most studies were cross-sectional content analyses using DISCERN, 70 Global Quality Score (GQS), 71 and JAMA benchmarks, 72 with occasional use of PEMAT and platform-specific engagement metrics. 73 (Table 2). These tools offer standardization and have clear value for judging reliability and clinical alignment. However, they were originally developed for static, text-based patient education. As a result, they may not fully capture how meaning is produced on modern video platforms, where visual framing, editing, and algorithmic distribution can shape interpretation as much as the spoken script. 74 This limitation is especially salient in ophthalmology because eye care is inherently visual. A video can be verbally accurate yet visually misleading through selective editing, exaggerated outcome framing, or decontextualized procedural footage. 46 Current tools are not designed to evaluate visual integrity, the informational consequences of montage and pacing, or the persuasive effects of background music and other attention cues.67,75 Short-form platforms add an additional challenge. Brief formats often optimize for a single take-home message, which can improve accessibility and engagement, but they reduce the space for diagnostic framing, uncertainty, contraindications, and escalation advice. In this context, completeness-based criteria may systematically underrepresent the educational contribution of high-quality micro-lessons. 27
A related challenge is the instability of the platform environment itself. Social media platforms are not static repositories of videos; they are dynamic ecosystems shaped by recommendation algorithms, moderation policies, interface design, video formats, monetization rules, and user behavior. 76 Changes in any of these components can alter which videos are retrieved, recommended, amplified, or suppressed over time. 77 As a result, cross-sectional studies of platform content may capture only a time-specific snapshot rather than a stable representation of ophthalmic information quality. 78 This temporal instability limits the durability and comparability of findings across studies and highlights the need for repeated sampling, transparent search procedures, and longitudinal or platform-aware evaluation designs.
This methodological mismatch is particularly important for the emerging professional-facing education subtheme, because the directly relevant evidence was limited and concentrated on YouTube-based surgical training. Criteria developed for patient education are poorly suited to assess technical fidelity in surgical demonstrations, where evaluation should emphasize stepwise clarity, safety-critical points, complication management, case selection transparency, and disclosure of edited segments. 79 Methodologically, exclusive reliance on manual expert review is also difficult to scale given the volume and velocity of new uploads. Future work should therefore move toward integrated, multi-modal assessment models that combine clinical validity with structured appraisal of visual integrity and transparent production practices, potentially supported by automated screening for high-risk cues. 46 Tools that are explicitly sensitive to the visual-first nature of ophthalmology will be essential to distinguish superficial popularity from substantive educational value for both patients and clinicians.
7. Future directions: Towards a validated digital ophthalmology
The rapid evolution of social media necessitates a transition from passive observation to active professional stewardship. Future efforts must prioritize the development of platform-native educational strategies that balance clinical integrity with the narrative engagement required by modern algorithms.
For academic societies and medical institutions, this involves the establishment of transparent source signaling mechanisms, 54 such as professional certification badges and institutional curation of high-quality surgical playlists. Furthermore, the ophthalmic community should advocate for the evolution of quality assessment metrics that account for visual accuracy and the unique constraints of short-form media. While AI offers promise for automated screening, it presents a dual challenge. The rise of Generative AI creates a risk of sophisticated deepfake medical advice that is harder to distinguish from professional content. 80 Therefore, future verification systems must evolve to detect AI-generated fabrications in addition to traditional misinformation.
8. Limitation
This review has several limitations. First, because it was designed as a narrative review, no formal risk-of-bias assessment or certainty-of-evidence grading was performed. Therefore, the conclusions should be interpreted as a structured synthesis of recurring findings rather than as quantitatively graded evidence. Second, most included studies were cross-sectional evaluations of platform content, and many relied on platform-specific search algorithms, time-limited sampling, and heterogeneous scoring instruments. These features limit direct comparability across studies and preclude causal inference regarding the relationship between engagement metrics and information quality. Third, the rapidly changing nature of social media platforms, including changes in recommendation algorithms, moderation policies, video formats, and user behavior, may affect the durability of the observed patterns. Accordingly, our conclusions emphasize recurring signals and conceptual implications rather than definitive estimates of content quality across all video-based platforms.
9. Conclusion
The integration of video platforms into the ophthalmic ecosystem represents a sustained and likely irreversible shift, offering both expanded educational reach and substantial risks of misinformation. This review identifies a recurring mismatch between popularity and quality across patient-facing content, with related but more limited evidence in professional-facing content. Short-form platforms are well suited to rapid dissemination and engagement but may limit clinical nuance, whereas longer-form video archives can provide procedural depth but often lack the standardized oversight required for formal training. In conclusion, the future of ophthalmology in the digital age depends on the ability of clinicians to bridge the gap between technical expertise and digital communication. Clinicians and professional organizations can contribute more effectively to trustworthy digital eye-health communication by combining evidence-based standards, transparent disclosure, and platform-appropriate communication strategies. Ultimately, the goal is to make video-based platforms more reliable and transparent for patient education, while cautiously developing their emerging role as adjunctive resources for professional learning and surgical training.
Supplemental material
Supplemental material - Ophthalmic health communication in the video-based social media era: A narrative review of information quality, engagement dynamics, and professional education
Supplemental material for Ophthalmic health communication in the video-based social media era: A narrative review of information quality, engagement dynamics, and professional education by Yizhou Yang, Yuecheng Ren, Luze Liu, Yue Li and Xuanqiao Lin in DIGITAL HEALTH.
Supplemental material
Supplemental material - Ophthalmic health communication in the video-based social media era: A narrative review of information quality, engagement dynamics, and professional education
Supplemental material for Ophthalmic health communication in the video-based social media era: A narrative review of information quality, engagement dynamics, and professional education by Yizhou Yang, Yuecheng Ren, Luze Liu, Yue Li and Xuanqiao Lin in DIGITAL HEALTH.
Footnotes
Acknowledgement statement
We sincerely thank Dr. Jin Yang for her encouragement and support throughout the study.
Author contributions
Yizhou Yang and Yuecheng Ren: Formal analysis, Investigation and Writing of the original draft. Luze Liu and Yue Li: Writing-review and editing, Resources and Validation. Xuanqiao Lin: Conceptualization, Supervision and Writing, review, and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.