
Abstract
Background
Autologous haematopoietic stem cell transplantation (AHSCT) is a potential therapeutic strategy for patients with relapsing multiple sclerosis (pwRMS) unresponsive to disease-modifying therapies (DMTs), though its optimal position in the treatment algorithm remains undefined.
Objective
To describe treatment outcomes of 30 AHSCT performed in 29 pwRMS.
Methods
Retrospective single-centre real-world study. Patients underwent AHSCT between 2001 and 2025. Median age at disease onset, diagnosis, and AHSCT was 21, 23, and 32 years, respectively. Mean EDSS at AHSCT was 3.1 (range 1.0–9.0). Median follow-up was 8 years (range 0.5–20.6). Carmustine, etoposide, cytarabine, melphalan (BEAM) + anti-thymocyte globulin (ATG) was the most used high-dose chemotherapy regimen. Brain magnetic resonance imaging was performed at 6 months, 12 months, and then annually after AHSCT.
Results
In patients with at least 6 months of follow-up, no evidence of disease activity-3 (NEDA-3) status was present in 16 out of 27 (59.2%); evidence of disease activity appeared after a median time of 33 months (range 5–74). NEDA-3 was maintained in 75% of the BEAM + ATG subgroup at the last follow-up. In the whole cohort, the mortality rate was 0%.
Conclusions
AHSCT is a highly efficacious option for patients with hyperaggressive onset or highly active disease despite the high efficacy of DMTs.
Keywords
Introduction
Autologous haematopoietic stem cell transplantation (AHSCT) has been applied in the management of multiple sclerosis (MS) for nearly three decades. 1 Recently, the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) and the European Society for Blood and Marrow Transplantation Autoimmune Diseases Working Party (EBMT-ADWP) have issued a consensus statement outlining its indications, optimal timing within the therapeutic algorithm, criteria for patient selection, transplant procedures, and post-transplant management.
The consensus considers the most suitable candidates to be patients under 45 years of age, with a disease duration below 10 years, minimal disability, and active MS. It further recommends considering AHSCT after the failure of high-efficacy disease-modifying therapies (HE-DMTs), but before irreversible disability develops. 2
However, the optimal positioning of AHSCT is still debated; randomized clinical trials (RCTs), in which AHSCT is being compared with HE-DMTs, are ongoing.
In this study, we share our experience with AHSCT performed in 29 patients since 2001.
Patients and methods
This is a retrospective single-centre real-world study conducted at Piedmont Regional Referral Multiple Sclerosis Center (University Hospital San Luigi Gonzaga), adhering to the Declaration of Helsinki and local regulations. All patients were aged ≥18 years, had failed at least two DMTs or one HE-DMT, or had no prior treatment in a hyperaggressive onset.
The study received approval from the local ethics committee, and written informed consent was obtained from all participants.
Twenty-nine patients with relapsing MS (pwRMS) were transplanted between 2001 and April 2025.
Statistical analysis
Clinical outcomes analysed were: annualized relapse rate (ARR), disease progression (defined as ≥ 1.0 point increase in EDSS for patients with a baseline EDSS ≥1, or 0.5 point increase for patients with EDSS >6.0 confirmed over 6 months; disability improvement (defined as a ≥1 point EDSS decrease in patients with a baseline score ≥2.0, confirmed over 6 months), and no evidence of disease activity-3 (NEDA-3) defined as the absence of relapses, confirmed 6-month disability progression, and both Gd-enhancing or new/enlarging T2 lesions. NEDA-3 was evaluated cumulatively and according to the immunosuppressive regimen used.
The follow-up rate was calculated for patients with a documented end-of-follow-up date. All analyses were performed on available data, with cases containing missing values excluded.
Kaplan–Meier analyses for time to NEDA-3 stratified by the main immunosuppressive regimens (carmustine, etoposide, cytarabine, melphalan (BEAM) + anti-thymocyte globulin (ATG) vs. Other) were performed to illustrate long-term outcomes and the time-dependent effect of the regimen. Multivariate Cox regression was conducted to evaluate the hazard ratio (HR) of the BEAM + ATG regimen versus other key covariates (age, sex, disease duration, and EDSS).
NEDA-3 analyses were stratified into two eras: AHSCT performed before 2010 (pre-HE-DMTs) and from 2010 onwards (post-HE-DMTs era), and sensitivity analyses were conducted in order to evaluate the durability of the treatment effect across time.
Statistical analyses were performed using Jamovi Version 2.4.8.0.
Safety was evaluated by reviewing clinical records.
Patients’ characteristics
At the time of diagnosis, all the patients had a relapsing phenotype.
At the time of AHSCT, one out of 29 patients had a relapsing progressive course, one had a progressive course without activity, whereas the other 27 showed a relapsing remitting (RR) disease.
Two out of 29 had a highly active phenotype with an aggressive onset.
There is no universally accepted definition of aggressive MS, but it is considered a rapidly progressing form of disease marked by frequent relapses with incomplete recovery, early and significant disability (often EDSS ≥4 within 5 years), and high magnetic resonance imaging (MRI) activity despite treatment. It includes patients who respond poorly to high-efficacy therapies or have a hyperacute disease onset. 3
Median age at disease onset, at diagnosis, and at AHSCT was 21 (range 14–39 years), 23 (range 15–44), and 32 years (range 18–46), respectively. Median follow-up after AHSCT was 8 years (range 0.5–20.6). One patient received transplantation twice.
Clinical and demographic characteristics are described in Table 1.
Patients’ characteristics.
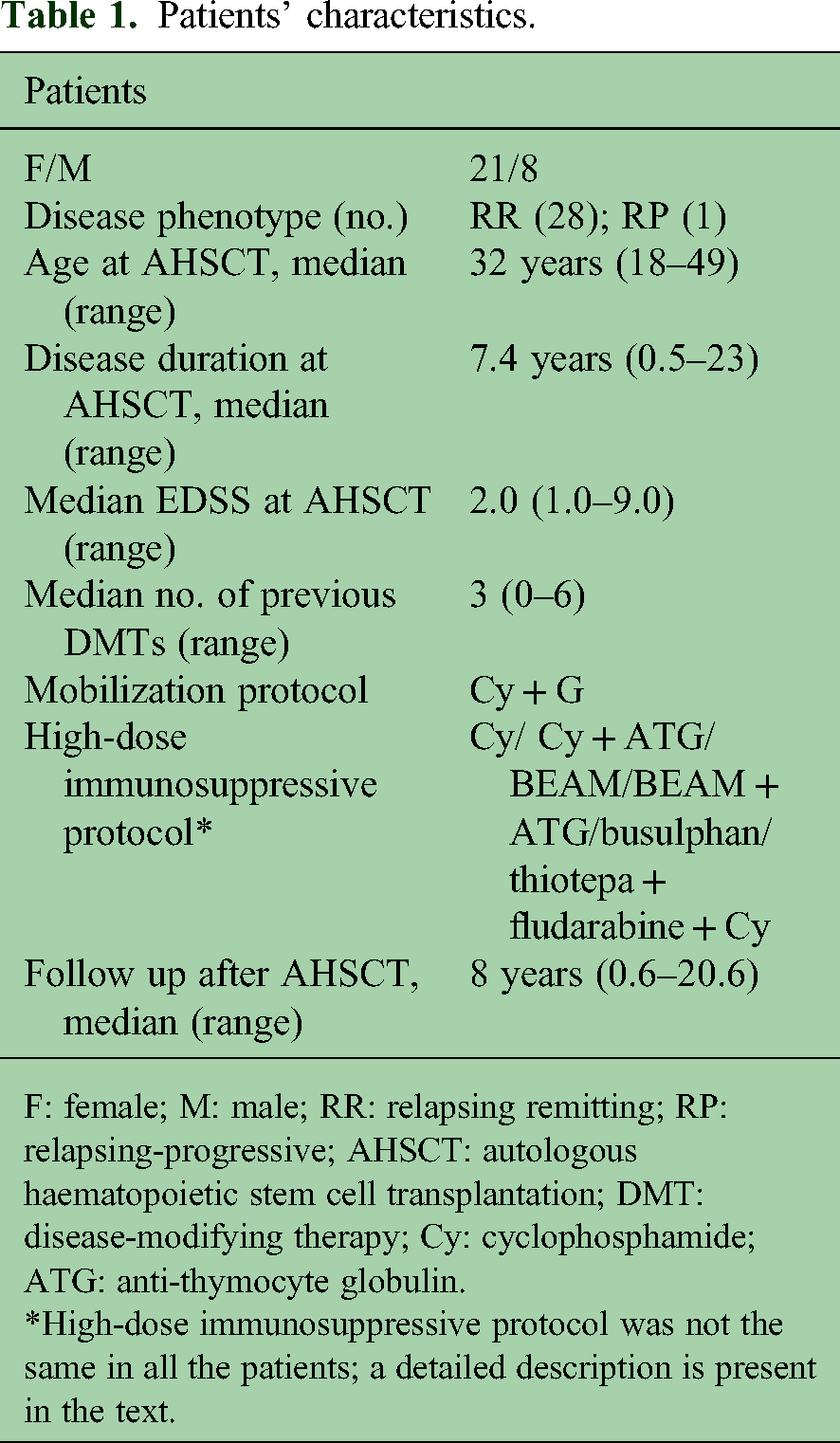
F: female; M: male; RR: relapsing remitting; RP: relapsing-progressive; AHSCT: autologous haematopoietic stem cell transplantation; DMT: disease-modifying therapy; Cy: cyclophosphamide; ATG: anti-thymocyte globulin.
*High-dose immunosuppressive protocol was not the same in all the patients; a detailed description is present in the text.
Figure 1 shows a flowchart of the study population.
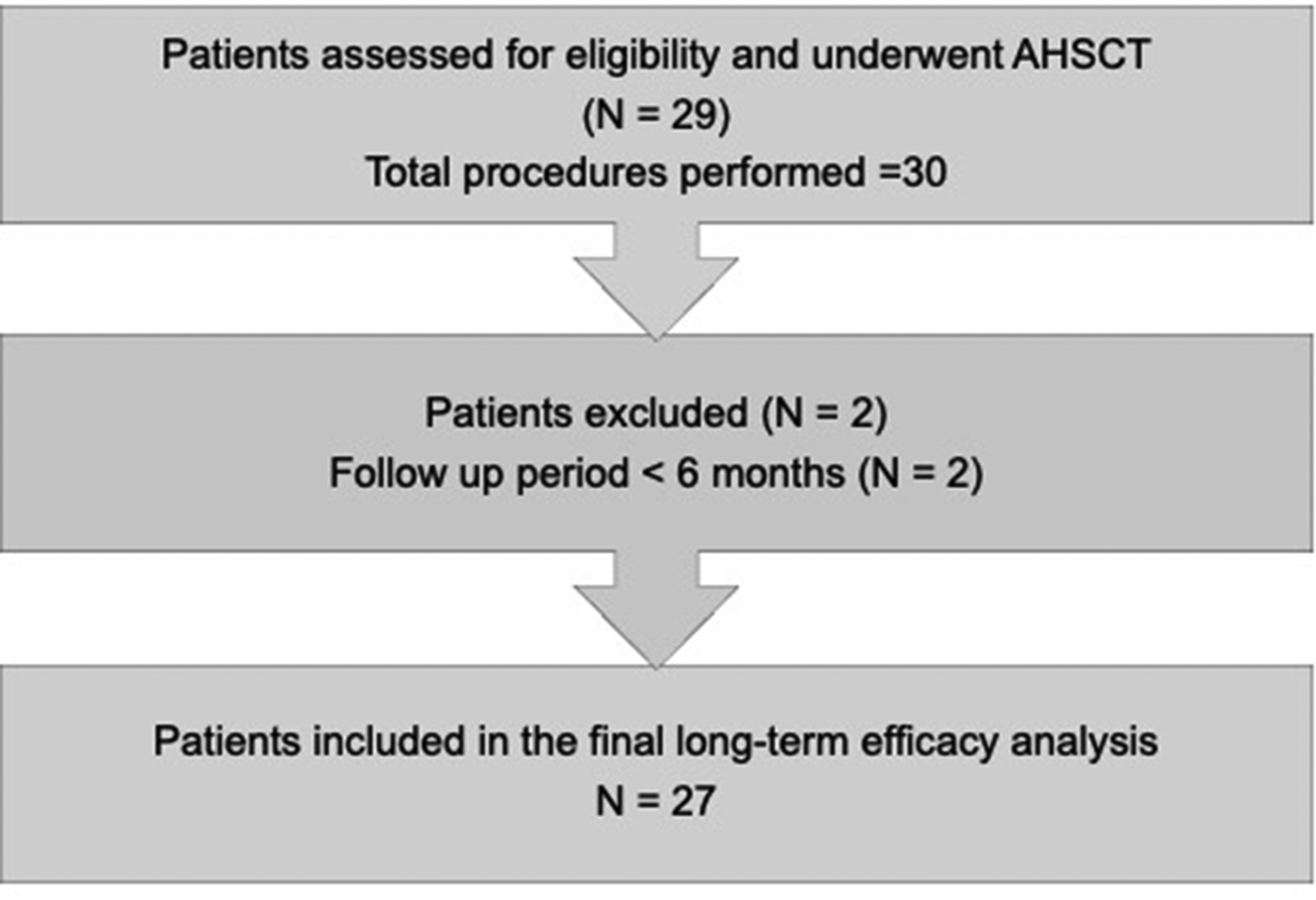
Flowchart of the study population. One patient received two transplant procedures; for this patient, follow-up was calculated from the first autologous haematopoietic stem cell transplantation (AHSCT). Two patients were excluded due to a follow-up duration of <6 months.
Patients’ disease history
In the 2 years preceding AHSCT, 19 patients had a mean ARR of 2.0, and eight patients had no relapses but showed new and enhancing lesions during active treatment. In the two patients with hyperaggressive onset, ARR was not calculable as they reached an EDSS of 7.0 and 9.0, respectively, in 12 months due to very close relapses.
At the time of AHSCT, 22 patients had an EDSS <6.0; five patients had an EDSS between 6.0 and 6.5; two patients had an EDSS >6.5. Overall median EDSS at AHSCT was 2.0 (range 1.0–9.0).
No patient presented with comorbidities.
DMTs prior to transplantation
All patients except one underwent AHSCT after failure of at least one DMT; one patient received transplantation as the first treatment. More in detail, in five patients, AHSCT was performed before 2006, when no HE-DMT was available in Italy, with the exception of mitoxantrone; of these five patients, three patients underwent AHSCT after interferon beta treatment failure, and two patients following the failure of both interferon beta and mitoxantrone.
Twenty-four patients had AHSCT after 2007; 18 patients received at least one HE-DMT before AHSCT; in this subset, reasons to perform AHSCT were treatment failure or high progressive multifocal leukoencephalopathy (PML) risk in John Cunningham virus+ patients with prolonged natalizumab exposure (two patients).
In one patient, transplantation was proposed after failure of two platform therapies, as all available HE-DMTs were contraindicated. Of the two patients with hyperaggressive onset, one patient received AHSCT after failure of 6 monthly intravenous cyclophosphamide and the other as first treatment (Table 2).
DMTs prior to transplantation.
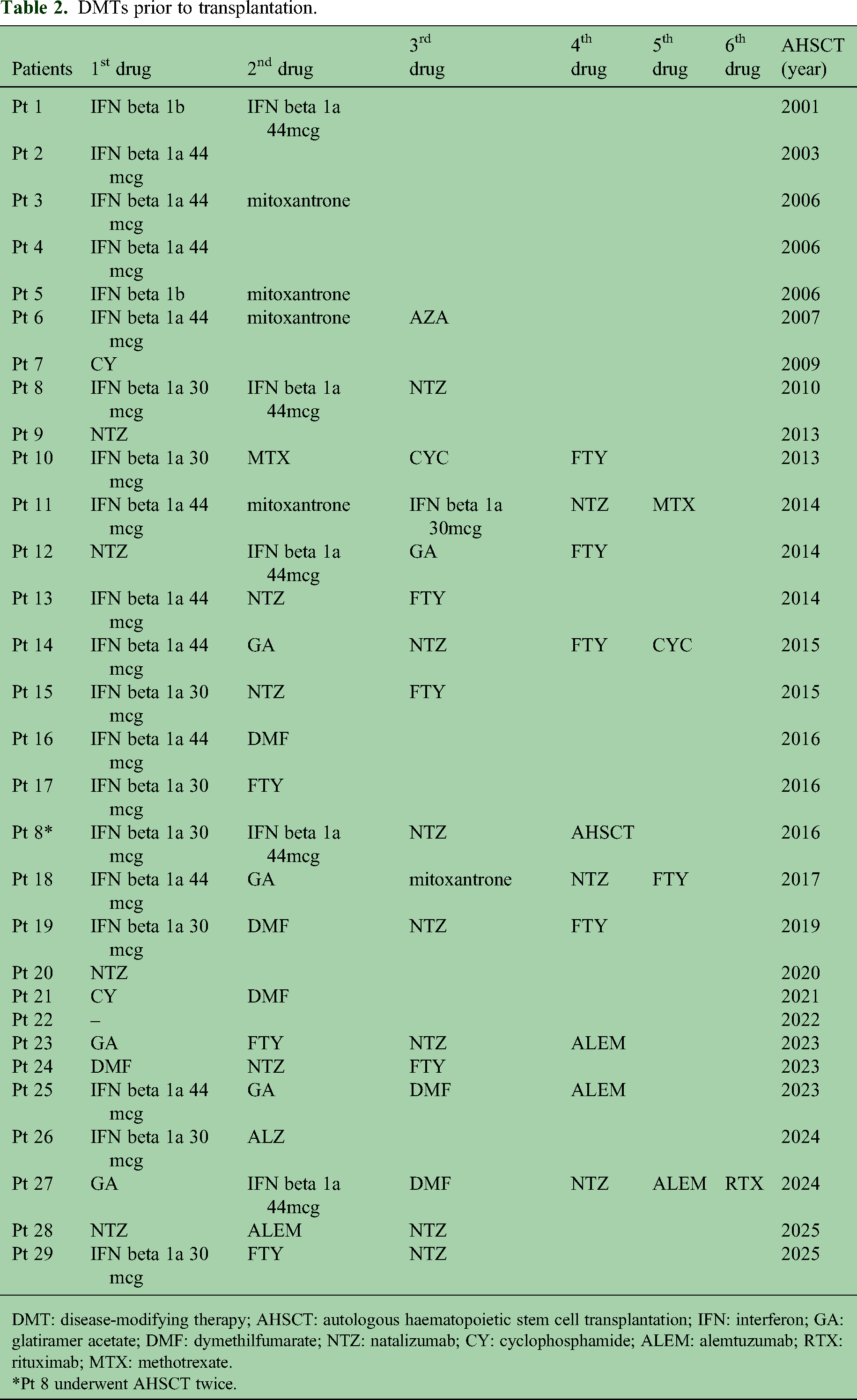
DMT: disease-modifying therapy; AHSCT: autologous haematopoietic stem cell transplantation; IFN: interferon; GA: glatiramer acetate; DMF: dymethilfumarate; NTZ: natalizumab; CY: cyclophosphamide; ALEM: alemtuzumab; RTX: rituximab; MTX: methotrexate.
*Pt 8 underwent AHSCT twice.
AHSCT procedure
According to the published protocol, 4 a transplant proposal was initiated after multidisciplinary evaluation by the neurology team. A subsequent meeting with the haematologist followed, during which the AHSCT regimen was illustrated. Screening tests, including haematological and comprehensive laboratory assessment, cardiac evaluation (electrocardiogram and echocardiography), abdominal ultrasound, and infectious disease screening, were then performed to identify any contraindications to AHSCT.
Given the potential gonadotoxicity associated with the high-dose chemotherapy regimens, fertility preservation counselling and procedures were offered to all patients of reproductive age prior to AHSCT.
Mobilization and high-dose immunosuppressive regimen
Mobilization
Cyclophosphamide (Cy) and granulocyte colony-stimulating factor were used to mobilize the stem cells. Patients who underwent AHSCT up to 2021 received Cy 4 g/m2; the dosage of Cy was lowered to 2 g/m2 from 2022 onwards to reduce haematological toxicity, aligning with evolving international guidelines.
Hyperhydration and uromitexan (MESNA) were administered to prevent haemorrhagic cystitis.
Stem cell harvest was performed via peripheral blood apheresis to achieve a minimum yield of 2.0 × 106 CD34+ cells/kg. The collected stem cells were subsequently cryopreserved. Retrospective analysis on the CD34+ cell yield found no difference in the quantity of collected cells between the two protocols.
High-dose immunosuppressive regimen
Given that patients underwent AHSCT over an extended time span, the high-dose immunosuppressive regimen evolved over the years in alignment with updated haematological guidelines.
More in detail, 22 patients received the seven-day BEAM/ATG protocol, which included BCNU (Carmustine): 300 mg/m2 administered intravenously on day 6; Etoposide: 200 mg/m2 administered intravenously from day 5 to day 2; Cytarabine (Ara-C): 200 mg/m2 intravenously from day 5 to day 2; Melphalan: 140 mg/m2 intravenously on day 1; rabbit ATG was administered intravenously from day 4 to day 2, for a total cumulative dose of 10 mg/kg.
Three patients received BEAM without ATG. In addition to BEAM, patients received cyclosporine (1 mg/kg day 7 to day 2). The use of cyclosporine (1 mg/kg day 7 to day 2) in the BEAM regimen was a standard operating procedure at our Transplant Center for prophylaxis against acute Graft-versus-Host Disease (GvHD), although GvHD risk is minimal in autologous settings.
One patient had the 5-day Cy/ATG protocol, which included cyclophosphamide and thymoglobulin; two patients had the same protocol without ATG.
One patient received busulphan because she had developed acute myeloid leukaemia secondary to mitoxantrone treatment, for which busulphan was part of the standard high-dose immunosuppressive protocol. One patient had thiotepa 250 mg daily on day 6 and day 5, fludarabine 45 mg daily from day 4 to day 1, and cyclophosphamide 1500 mg daily from day 4 to day 1.
Antimicrobial prophylaxis was performed with fluconazole, acyclovir, and sulphamethoxazole-trimethoprim according to the protocol of the Transplant Unit.
During the retrospective period covered by this study, a centralized internal protocol for revaccination was not formally established, and patients were managed according to general clinical practice. However, a standardized revaccination program is currently being implemented at our Center, following the international consensus recommendations for AHSCT in MS as outlined by Muraro et al. 2 Notably, no severe vaccine-preventable infections were recorded during the follow-up period for the current cohort.
MRI monitoring
Contrast-enhanced brain MRI was performed at 6 months, 12 months, and then every year after AHSCT, in order to exclude new/enlarging T2 lesions and/or gadolinium-enhancing lesions.
Centralized blinded reading of all the images and the use of identical MRI acquisition protocols throughout the entire study period were not technically feasible due to the evolution of MRI technology and the retrospective data collection. However, all MRI scans were acquired on 1.5 Tesla scanners, performed according to established local protocols applicable at the time of acquisition, and all images were consistently evaluated for activity by experienced neuroradiologists.
Results
Effectiveness
Clinical and radiological outcomes have been evaluated in patients with at least 6 months of follow-up (27 patients). EDSS scores were assigned by experienced neurologists at the MS Center.
NEDA-3 after AHSCT
Sixteen out of 27 patients (59.2%) were in NEDA-3 status at the last visit; evidence of disease activity (EDA) appeared after a median time of 33 months (range 5–74 months).
EDA was due to both clinical and radiological activity in seven patients, only radiological activity in one patient, only clinical activity in one patient, and to confirmed disability progression in two patients.
In patients who received BEAM + ATG, NEDA-3 status was present in 15 out of 20 patients (75%), see Table 3.
Patients in NEDA-3 status after AHSCT.
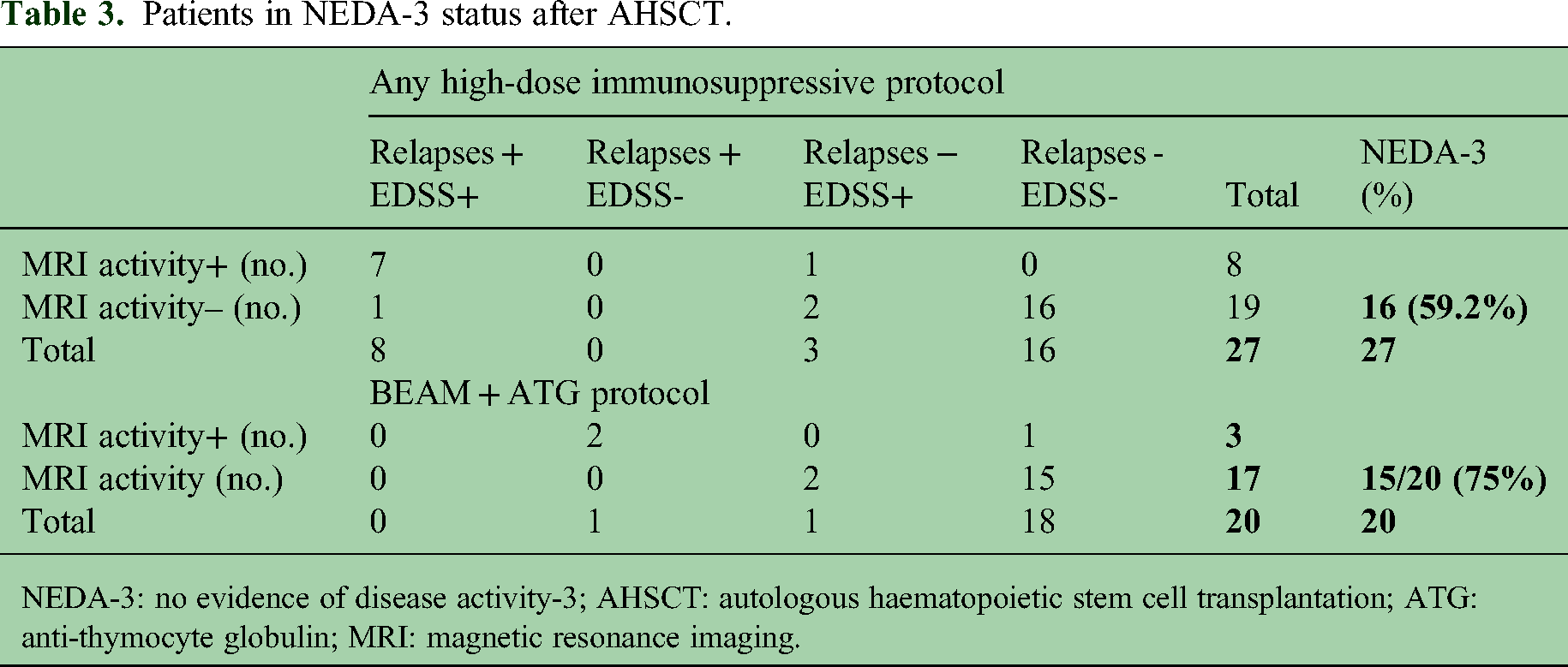
NEDA-3: no evidence of disease activity-3; AHSCT: autologous haematopoietic stem cell transplantation; ATG: anti-thymocyte globulin; MRI: magnetic resonance imaging.
Time-to-NEDA-3 failure (defined as the event) was analysed using Kaplan–Meier curves, stratified by high-dose chemotherapy protocol (‘BEAM + ATG’ vs. ‘Other’). A statistically significant difference was observed between the groups (p = 0.038, log-rank test), with the BEAM + ATG protocol demonstrating superior time to failure (Figure 2).
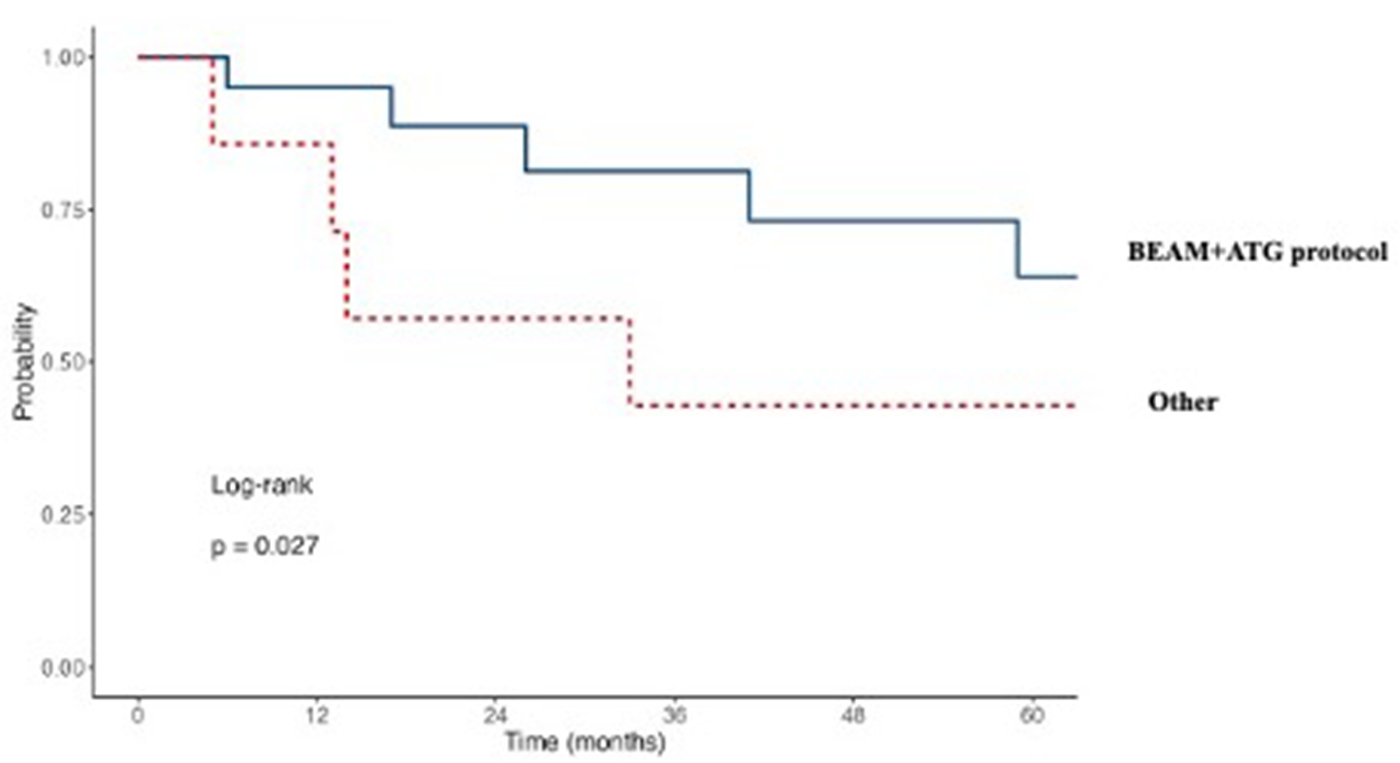
Time to NEDA-3 failure stratified by immunosuppressive regimen (‘BEAM + ATG’ vs. ‘Other’).
In the multivariable Cox regression model, the BEAM + ATG regimen was utilized as the reference group (HR = 1). The model showed that ‘other’ immunosuppressive regimens were associated with a significantly 3.5-fold higher risk of NEDA-3 failure compared to the BEAM + ATG protocol (HR = 3.50; 95% CI 1.07–11.62; p = 0.038). This suggests that the addition of ATG to the BEAM regimen provides a sustained, independent protective effect against disease reactivation. To identify independent predictors of NEDA-3 failure, a multivariable Cox regression model was performed, including the high-dose chemotherapy regimen, age at AHSCT, baseline EDSS, and disease duration as covariates. The analysis confirmed that the high-dose immunosuppressive regimen was the strongest independent predictor of long-term outcome. Using the BEAM + ATG protocol as the reference, patients treated with other regimens showed a significantly 3.5-fold higher risk of experiencing NEDA-3 failure (HR = 3.50; p = 0.038).
To assess the robustness of our findings in relation to changes in therapeutic access over time, we performed a sensitivity analysis by dividing the cohort into two treatment eras: pre-2010 (before the widespread use of high-efficacy DMTs) and post-2010. No statistically significant difference between the two periods was found.
Clinical activity
Nineteen out of 27 patients (70.1%) did not experience any relapse for the whole follow-up period; eight out of 27 patients (29.6%) had clinical reactivation, occurring after a median time of 22.8 months (range 6.1–75.1 months).
Of the 19 patients free from relapses, 18 patients had received the BEAM + ATG protocol.
Radiological activity
MRI activity was observed in seven patients who also presented clinical activity; in one more patient, radiological activity was present in the absence of clinical relapse.
Disease progression
Overall, median EDSS changed from 2.0 at the time of AHSCT to 1.5 at the last follow-up visit.
In more detail, it decreased or remained stable in 20 patients (13 and seven patients, respectively) and increased in seven patients. Among these seven patients, five patients also had clinical and radiological reactivation, and two patients had clinical progression independent of relapses (Table 4).
DMTs sequencing, AHSCT protocol, and NEDA-3 status after AHSCT.

DMT: disease-modifying therapy; M: mobilization; IS: immunosuppressive regimen; ΔEDSS: difference between the EDSS score at the last follow-up and the EDSS score at the time of transplantation; na: not applicable (follow-up <6 months); Cy + G: cyclophosphamide + granulocyte colony-stimulating factor; BEAM: carmustine, etoposide, cytarabine, melphalan; ATG: anti-thymocyte globulin; T + F: thiotepa and fludarabine; DMF: dymethilfumarate; GA: glatiramer acetate; MTX: methotrexate; NEDA-3: no evidence of disease activity-3; NTZ: natalizumab; RTX: rituximab; ALEM: alemtuzumab; IFN: interferon.
DMTs after AHSCT
Six out of 11 patients received DMTs after AHSCT failure: five patients started a HE-DMT, and one patient received AHSCT a second time.
Five patients did not receive further treatment: two patients experienced non-inflammatory progression, one patient had a mild relapse 6 years post-AHSCT, one patient declined additional therapy, and one patient exhibited mild radiological activity and is being closely monitored.
Safety
Mortality rate was 0%.
Notably, there was only one case of septic shock from saprophytic Staphylococcus, accompanied by respiratory failure requiring transfer to intensive care, which resolved completely. Interestingly, no hospital admissions due to COVID-19 were reported.
Neutrophil engraftment occurred between day 8 and day 14.
Table 5 reports early and late adverse events, their severity, and transfusion support. One case of secondary autoimmune disorders (mild rheumatoid factor-positive rheumatoid arthritis) occurred in one patient, manifesting 3 years after AHSCT. The patient was successfully managed with hydroxychloroquine. No secondary malignancies/neoplasms were reported.
Adverse events.

AE: adverse event; BEAM: carmustine, etoposide, cytarabine, melphalan; ATG: anti-thymocyte globulin; FUO: fever of unknown origin; RBC: red blood cell; PLT: platelets; E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; AHSCT: autologous haematopoietic stem cell transplantation; Cy: cyclophosphamide; T + F: thiotepa and fludarabine; PML: progressive multifocal leukoencephalopathy.
Patients 1 to 6 received AHSCT before 2007.
Type of AE: 0 = organ-limited infection; 1 = systemic infection; 2 = drug-related organ toxicities; 3 = autoimmune disorder; 4 = malignancies; 5= PML; 6 = death.
Severity of AE: 0 = mild AE, no treatment required; 1 = moderate AE, treatment required; 2 = severe AE, hospitalization required; 3 = life-threatening.
A safety comparison between BEAM ± ATG (n = 24) and other regimens (n = 5) is reported in Table 6.
Safety and tolerability profile according to immunosuppressive regimen. Comparison of early toxicities, haematological recovery, and healthcare utilization (length of stay) between patients treated with BEAM ± ATG and alternative immunosuppressive protocols.

BEAM: carmustine, etoposide, cytarabine, melphalan; ATG: anti-thymocyte globulin; AE: adverse event.
Fertility was not evaluated, but all patients of reproductive age underwent fertility preservation procedures prior to the immunosuppressive regimen. Notably, one patient reported a spontaneous, naturally conceived pregnancy post-AHSCT. The pregnancy resulted in a healthy live birth.
Selected clinical cases
Case 1: Second autologous transplantation with long-term NEDA-3 maintenance
A female patient with paediatric-onset MS, diagnosed in 2004 at age 14, failed platform therapies in 2008 and started natalizumab, discontinued after six infusions due to clinical/radiological activity and persistent neutralizing antibodies. One month later, mobilization with high-dose cyclophosphamide (4 g/m2) was performed. Five months later, she underwent AHSCT with BEAM (2009); EDSS was 1.5. NEDA-3 status maintained for 7 years. In 2016, disease activity resumed, and she underwent a second AHSCT using previously collected stem cells. High-dose immunosuppressive protocol: thiotepa, fludarabine, and cyclophosphamide. She remains in NEDA-3.
Case 2: AHSCT in progressive disability despite multiple high-efficacy therapies
Female patient, MS onset at 26, diagnosed at 27 (in 2002). After failure of first-line injectable and oral therapies, she started natalizumab in 2015 (EDSS 3.0), discontinued after 1 year due to high PML risk. She received two courses of alemtuzumab (2016 and 2017).
Despite treatment, clinical worsening continued without radiological activity. Rituximab was tried, but EDSS progressed to 6.0 by 2020.
Following multidisciplinary discussion, she underwent AHSCT in June 2024 (EDSS 6.5). Currently, EDSS remains 6.5, with complaints of increased fatigue and memory impairment.
Hyperaggressive disease presentation
Two patients presented with hyperaggressive MS, reaching EDSS scores of 9.0 and 7.0, respectively. The first patient, who reached an EDSS of 9.0, underwent AHSCT after failure of six monthly intravenous cyclophosphamide cycles. At 14-year follow-up, EDSS was 1.0, with no further relapses. The second patient reached an EDSS of 7.0 and received AHSCT as first-line treatment. At 3-year follow-up, EDSS improved to 2.0, with no evidence of further clinical or radiological disease activity.
Discussion
In recent years, the attitude to treat pwMS early and efficaciously has become prevalent.
Literature data agree that a better treatment response occurs when therapy starts in the early phase of the disease.5,6
Currently, several HE-DMTs are available. Choice of first DMT depends on clinical and radiological prognostic factors, drug risk/benefit profile, neurologist's experience, patient perspective, and comorbidities.
HE-DMTs as initial treatment represent an emerging alternative to the escalation approach, though they may entail chronic immunosuppression and associated long-term safety concerns. Consequently, de-risking strategies following disease stabilization, as well as immune-reconstitution therapeutic approaches, are gaining interest. About the de-risking strategy, no guidelines on optimal timing and methodology exist. Immune-reconstitution therapeutic strategy through pulsed immunosuppression, particularly in treatment-naïve patients or in those with a short disease duration, offers a promising option in active MS. Two approved DMTs employ this strategy. Long-term follow-up data confirmed the prolonged efficacy of cladribine over a median of 10.9 years, 7 with recent safety evaluations supporting findings from its clinical development program. 8 Similarly, alemtuzumab provided long-term efficacy after two treatment courses, substantially lowering relapse rates and enhancing MRI outcomes, with benefits enduring up to 13 years.9,10 However, post-marketing surveillance has reported serious adverse events, including autoimmune disorders and cerebrovascular complications.11–13
In the current therapeutic scenario, the use of AHSCT, the most powerful immune-reconstitution therapeutic approach, is becoming more frequent, as it is increasingly recognized as highly efficacious and with a safety profile improved with increasing experience.
Based on the recent consensus statement by an expert panel, 2 AHSCT is designated as the standard of care for pwRRMS in several scenarios: for patients refractory to conventional HE-DMTs, as a first-line therapy in treatment-naïve patients presenting with a hyperaggressive course, and following the failure of a single DMT within the context of clinical trials.
Until now, few RCTs of AHSCT have been completed. The ASTIMS trial included 21 patients randomly assigned to receive either AHSCT with the BEAM–ATG protocol or mitoxantrone. 14 AHSCT demonstrated superiority over mitoxantrone in reducing inflammatory disease activity as measured by MRI; disability progression showed no significant difference between the treatment arms.
It must be considered that this trial also included patients with secondary progressive MS (SPMS).
In the MIST trial, 15 a total of 110 pwRRMS were randomly allocated to either receive AHSCT with the cy-ATG protocol or one of the Food and Drug Administration-approved DMTs, with the exception of alemtuzumab.
With a median follow-up of 2 years, AHSCT was found to be superior to DMTs across several endpoints: progression-free survival (90% vs. 25%), relapse-free survival (85% vs. 15%), and in NEDA-3 at 5 years (78% vs. 3%), as determined by a post-hoc analysis.
Approximately only half of the control group received HE- DMTs; the remainder received moderate-efficacy DMTs, which represents a limitation.
Most data on AHSCT outcomes come from observational studies.
Kalincik et al. 16 compared 4915 pwRRMS from the MSBase registry, evaluating AHSCT versus fingolimod, natalizumab, and ocrelizumab. Over 5 years, AHSCT showed a much lower relapse rate than fingolimod, slightly lower than natalizumab, and higher disability recovery rates than both. At 3 years, no significant differences were observed between AHSCT and ocrelizumab, possibly due to the short follow-up period.
A more recent study 17 retrospectively compared AHSCT with alemtuzumab and ocrelizumab in a single cohort of 621 pwRRMS. The study showed the superiority of transplantation in preventing relapses compared to alemtuzumab and ocrelizumab, and in suppressing radiological activity compared to alemtuzumab; no differences were found in the risk of disability accrual, with a median follow-up of 3 years.
Recent evidence supports AHSCT as a treatment option also for active SPMS. In the work by Boffa et al., 18 data from the Italian Bone Marrow Transplantation Study Group and MS Registry compared 79 AHSCT-treated patients with 1975 patients on other DMTs.
AHSCT was found to delay confirmed disability progression, a result classified as Class III evidence by the study. However, the study's scope was limited by the absence of siponimod, cladribine, ocrelizumab, or rituximab in the comparator arm.
Leptomeningeal enhancing lesions (LME) were analysed as an exploratory endpoint in the study conducted by Marchi et al., 19 aiming to further characterize AHSCT and other treatments’ effects on pathogenetic mechanisms of the disease. The study included 55 relapsing and SPMS patients. A correlation was found between age at AHSCT and basal LME count. In one of four AHSCT-treated and longitudinally followed patients, one LME disappeared, suggesting AHSCT may affect LME development and persistence, supporting its early use.
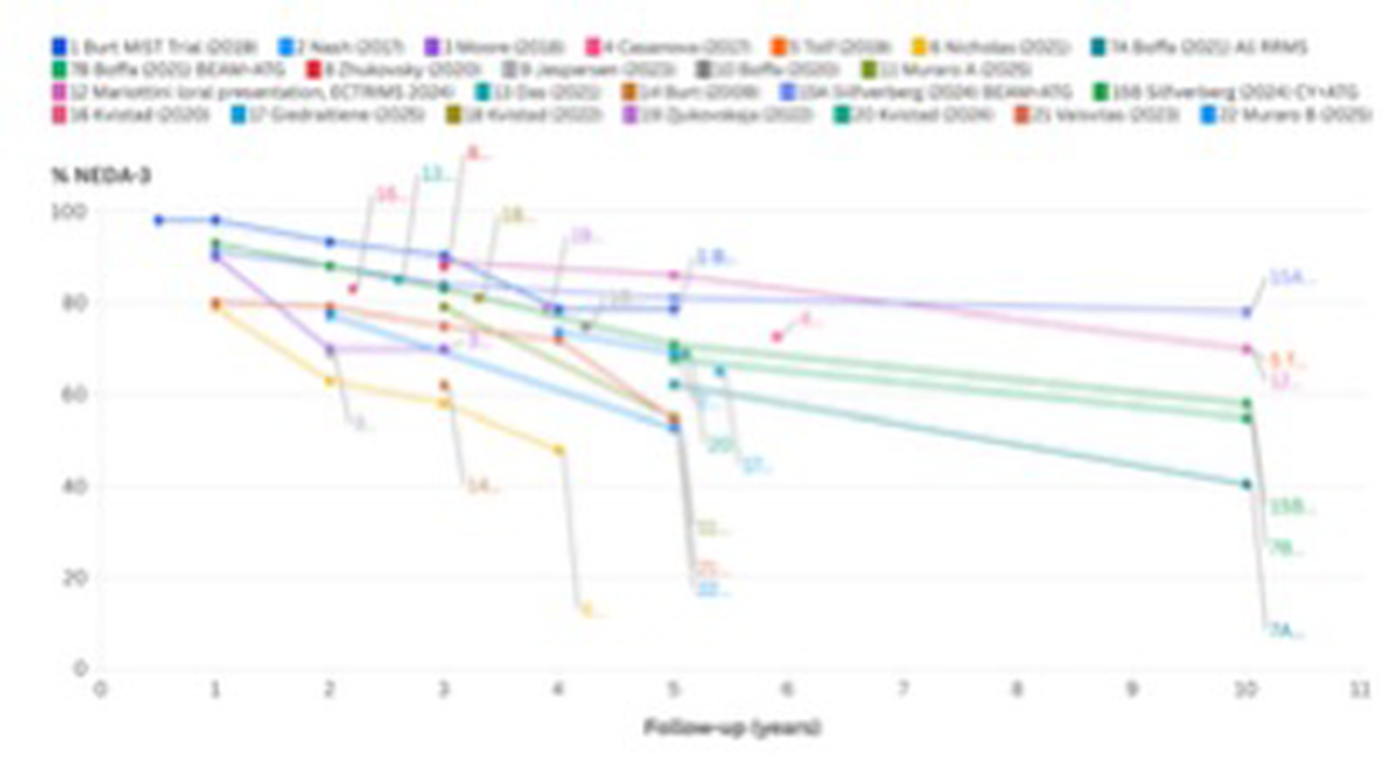
Globally, PubMed and Google Scholar searches of studies on pwRMS who underwent AHSCT show that 40% to 78% of patients maintain NEDA-3 at 10 years (Figure 3).20–42
Despite the extensive literature, several questions remain unresolved.
One of these concerns the intensity of the high-dose immunosuppressive regimen, providing the optimal ratio between efficacy and safety. A Swedish retrospective analysis 39 of 231 patients treated with BEAM + ATG (33 patients) or Cy + ATG (141 patients) showed a higher percentage of NEDA at 5 years in the BEAM group (81%) compared to Cy group (71%), not significantly different (p = 0.29), but a greater number of severe adverse events in the BEAM group (3.1 vs. 1.4 per patient, respectively) with an average hospitalization 3 days longer than in the Cy + ATG group.
A further relevant factor to consider is the economic aspect.
The cost-effectiveness of AHSCT and HE-DMTs was the subject of a recent Italian study, 42 which concluded that AHSCT was the less expensive option when assessed over the five-year term, despite similar costs over a two-year period.
Based on the MIST Study data, 19 a major cost-utility analysis conducted by the UK National Health Service 43 determined that AHSCT was the dominant strategy, meaning it was both more effective and less costly, compared to the DMTs for treating people with highly active disease.
Further aspects need to be addressed about AHSCT in clinical practice, such as the benefit on the risk of progression independent of inflammation, the occurrence of cognitive deficits, and the appropriate placement in the therapeutic algorithm.
In order to address this issue, an Italian-controlled randomized phase 3 study of AHSCT versus the best available therapy in aggressive MS, the NET-MS study (EudraCT No. 2022-002654-95) 44 is ongoing; the trial includes patients who have failed one DMT regardless of the type of treatment (high or low–moderate efficacy). A subsequent amendment was approved to include naïve patients with aggressive onset.
In this paper, we shared our experience about the use of AHSCT in 29 patients, treated between 2001 and 2025. In our cohort, after a median follow-up of 8 years, 59% of patients were in NEDA-3; this percentage increases to 75% in patients who received ATG in addition to BEAM. Even if the number of treated patients is small, ATG appears to significantly enhance BEAM's effectiveness. Among the 29 treated patients, two have sustained NEDA-3 for more than 15 years. Although the concept of a definitive cure for MS remains elusive, prolonged disease remission of this extent suggests that AHSCT could act as a potentially curative approach.
In summary, in our cohort, AHSCT outcomes were consistent with the literature, confirming the procedure's safety and efficacy. We suggest AHSCT as first-line therapy for aggressive cases and early in the treatment sequence for active disease. If AHSCT can prevent LME, early intervention may reduce inflammation, disability, and socioeconomic impact in MS. The benefit for moderate disease remains unclear and requires long-term data from large randomized trials.
Footnotes
Acknowledgment
We sincerely thank the Oncohematology and Bone Marrow Transplant Center for the transplantation procedures and the support in patient management.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM received compensation for speaking and consulting by Novartis, Sanofi, Roche, Merck, Biogen, and travel reimbursement for attending conferences by Roche, Novartis, and Amgen. MM received honoraria for a scientific talk by Alexion and Merck and travel reimbursement by Roche and Alexion. AB served on the scientific advisory board of Almirall, Bayer, Biogen, and Genzyme; received speaker honoraria from Biogen, Novartis, and Sanofi, grant support from Almiral, Biogen, Associazione San Luigi Gonzaga ONLUS, Fondazione per la Ricerca Biomedica ONLUS, Mylan, Novartis, and the Italian Multiple Sclerosis Society. ADS received personal compensation for speaking and consulting by Biogen, Novartis, Roche, Sanofi, Merck, Bristol Meyer Squibb, Janssen, Alexion, Alnylam, and Amgen, and has been reimbursed by Merck, Novartis, and Roche for attending several conferences. MDG, SU, and CA have nothing to disclose.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the local ethics committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The clinical data supporting this study are available in the patients’ medical records and can be accessed upon request, subject to institutional and ethical approvals.