
Abstract
Objectives
Fatigue and cognitive impairment are common in people with multiple sclerosis (pwMS). This study evaluated the feasibility of a digital symptom management program integrated into the Finnish MS Registry targeting fatigue and cognitive symptoms.
Materials and Methods
Forty pwMS with subjective fatigue and cognitive concerns enrolled in an eight-session eHealth program including symptom self-assessments, a mobile fatigue diary, individualized goal setting, and feedback from a neuropsychologist. Feasibility outcomes were completion rate, perceived usefulness, and technical functionality. Patient-reported outcome measures (PROMs) included the Goal Attainment Scale (GAS), Global Rating of Change (GRC), Fatigue Scale for Motor and Cognitive Functions, Multiple Sclerosis Neuropsychological Questionnaire, patient-reported Expanded Disability Status Scale, Visual Analogue Scales for neurological symptoms, and EQ-5D-5L.
Results
Twenty-three participants (58%) completed the program with follow-up. The program was rated useful by 65% and technically appropriate by 70%. The mean GAS T-score was 50 both postintervention and at follow-up. Mean GRC scores indicated slightly positive change in managing fatigue (+1.4), cognitive symptoms (+1.3), and overall effects (+1.8). Other PROM changes were minimal.
Conclusions
The registry-integrated eHealth program showed potential to support the management of fatigue and cognitive symptoms in pwMS. Further development and evaluation of digital symptom management tools are warranted.
Introduction
Multiple sclerosis (MS) is the most common disabling neurological disease among young and middle-aged adults, with substantial economic impact. 1 Invisible symptoms, such as fatigue and cognitive impairment, have been shown to negatively affect work capacity.2,3
Fatigue is reported as the most common symptom of multiple sclerosis (MS), affecting approximately 80% of patients.4,5 Cognitive deficits are also prevalent, occurring in an estimated 50–60% of individuals with MS. 6 Cognitive impairment may progress over time and involves multiple cognitive domains. 7 The functional consequences of MS-related fatigue and cognitive impairment can be substantial.6,7 Even mild cognitive deficits and fatigue can compromise productivity by reducing work capacity.2,3 These deficits may also negatively impact physical independence, quality of life, social and recreational activities, driving ability, rehabilitation outcomes, and may contribute to caregiver burden.6,7 As fatigue and cognitive problems can be present early in disease course and are poorly managed by medical treatment, early interventions to support coping and symptom management are warranted.6,8 There is growing evidence that rehabilitation can mitigate the negative effects of cognitive impairment in MS.8–11 However, access to neuropsychological services is limited, highlighting the need for new approaches and tools to address the impact of these invisible symptoms. 12
Telerehabilitation and artificial intelligence-based interventions have been proposed as cost-effective and accessible strategies for managing fatigue and cognitive symptoms in MS.13–17 To support pwMS in addressing these concerns, a digital rehabilitation module was developed within MyMS, the patient interface of the widely used Finnish MS Registry.18–21
The aim of the present study was to evaluate the feasibility and potential of the digital program for the management of fatigue and cognitive symptoms in MS.
Materials and methods
The Finnish MS Registry is utilized in 18 out of 21 wellbeing services counties in Finland and covers data for over 90% of Finnish pwMS. 18 The registry serves as the primary user interface for neurologists during patient visits and is integrated with hospital electronic patient record (EPR) systems. The registry also includes a patient interface, MyMS, which allows for the completion of patient-reported outcome measures (PROMs) to assess disease severity, relapses, quality of life (QoL), and symptoms. 19 Particular emphasis has been placed on the evaluation of invisible symptoms, such as fatigue and cognitive concerns.20,21 To provide pwMS with tools to manage fatigue and cognitive concerns from the early stages of the disease, a digital rehabilitation module accessible regardless of time and location was developed within the patient interface of the Finnish MS Registry.
Subjects
The study was conducted at four sites: the University Hospitals of Turku, Tampere, and Oulu, as well as Hospital Nova of Central Finland. All 40 participants provided written informed consent prior to participation.
Inclusion criteria for participation were: a definitive diagnosis of relapsing-remitting MS; age between 18 and 65 years; absence of other neurological or psychiatric disorders; no history of head trauma or learning disabilities; Finnish as native language; at least part-time employment or enrollment in education; subjective cognitive fatigue and/or other cognitive problems affecting work or study performance; willingness to evaluate fatigue and cognitive concerns using self-report questionnaires; willingness to set goals for improved symptom management; ability to participate in web-based rehabilitation sessions (0.5–1 h per session) approximately once per week; willingness to complete a 7-day mobile fatigue diary approximately 2 weeks after the start of the rehabilitation program; access to both a laptop and a mobile phone; and ability and willingness to provide written informed consent.
Designated healthcare professionals at each study site introduced the study to potential participants, verified eligibility, and obtained written informed consent from those who agreed to participate. Participants also received an information letter detailing the MyMS platform, the symptom management program, and study procedures.
Intervention: eHealth program for the management of fatigue and cognitive problems
The program was based on the content reported in a previous study by our group, 20 with additional elements such as a mobile fatigue diary, guided diary evaluation, guided setting of individually meaningful goals and strategies for symptom management, and personalized feedback, informed by prior research and clinical experience.6,8,15,16 The program content is detailed in Table 1. A steering committee, consisting of three neuropsychologists, an MS specialist nurse, and a neurologist, supervised both the planning and execution of the study.
A detailed description of the content of the symptom management program.
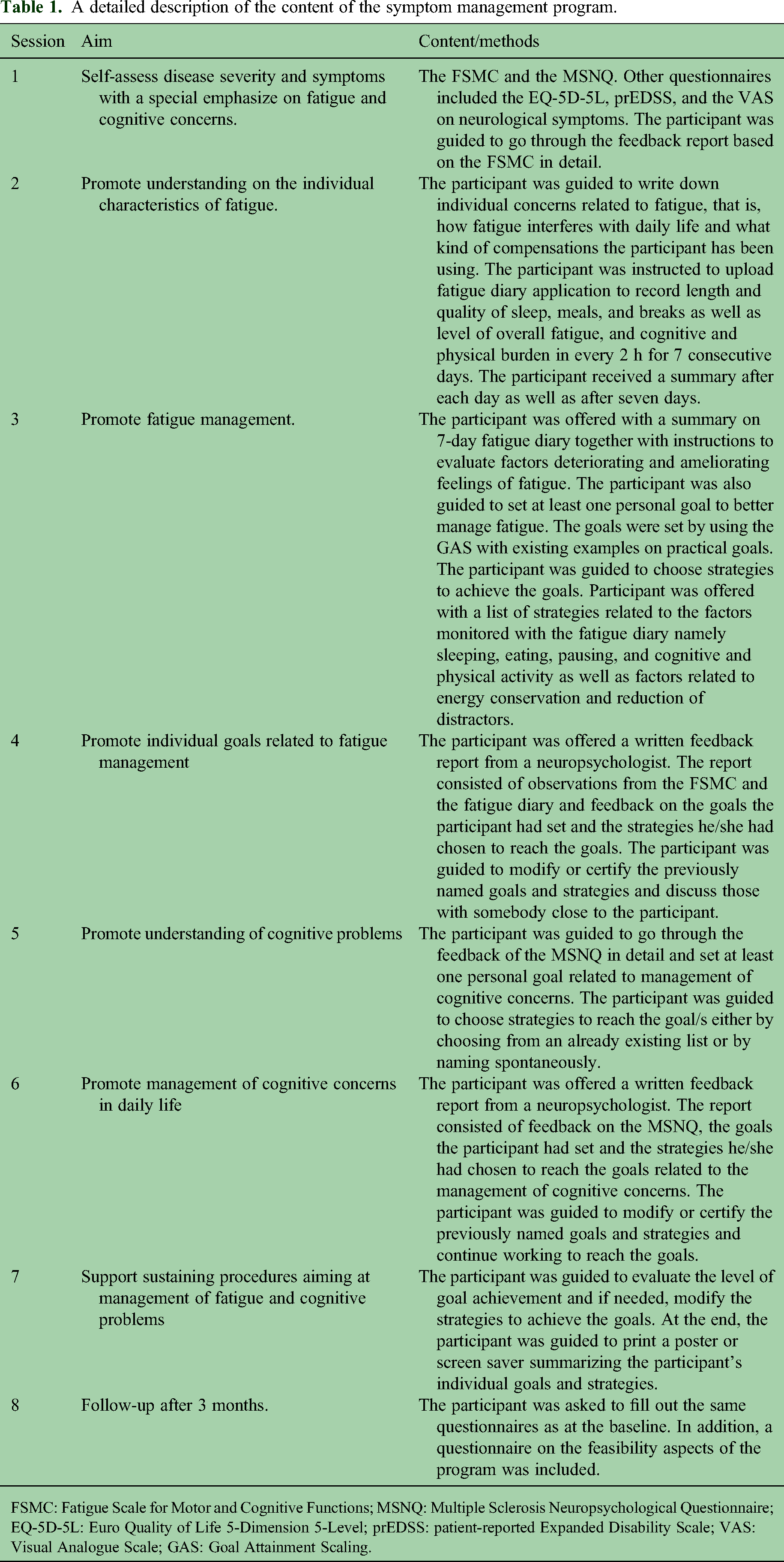
FSMC: Fatigue Scale for Motor and Cognitive Functions; MSNQ: Multiple Sclerosis Neuropsychological Questionnaire; EQ-5D-5L: Euro Quality of Life 5-Dimension 5-Level; prEDSS: patient-reported Expanded Disability Scale; VAS: Visual Analogue Scale; GAS: Goal Attainment Scaling.
Assessments included in the study
At baseline and 3 months after completion of the program, participants filled out the Finnish versions of the following patient reported outcome measures (PROMs): patient-reported Expanded Disability Status scale (prEDSS),1,22 Visual Analogue Scales (VAS) for neurological symptoms, 20 Euro Quality of Life 5-Dimension 5-Level (EQ-5D-5L),1,23 Fatigue Scale for Motor and Cognitive Functions (FSMC),24,25 and Multiple Sclerosis Neuropsychological Questionnaire (MSNQ).25,26 Achievement of individual goals was assessed using the Goal Attainment Scale (GAS) T-score, 27 both at the end of the program and at 3-month follow-up. Three months after the completion of the program, participants completed a follow-up questionnaire assessing the perceived effects of the intervention using the 11-point Global Rating of Change (GRC) scale ranging from −5 (much worse) to +5 (much better) on the management of fatigue and cognitive symptoms, on the ability to work or study, and overall impact of the program. 28 Additionally, participants were asked to evaluate whether the program was useful and whether the technical implementation was appropriate, using response options of “yes,” “no,” or “unable to evaluate.”
Demographic and clinical variables were obtained from the Finnish MS Registry and included gender, year of birth, disease duration, and disease severity as assessed by the Expanded Disability Status Scale (EDSS). 29
Ethical approval and statistical analyses
The study was approved by the Ethics Committee of the Wellbeing Services County of South-West Finland (Number 49/1801/2022). The collected data were analyzed to evaluate feasibility outcomes, including (a) program attrition and adherence; (b) achievement of individual rehabilitation goals, as measured by GAS T-scores; (c) perceived benefit of the program for managing fatigue and cognitive symptoms, as assessed by GRC scores; and (d) changes in self-perceived fatigue and cognitive concerns, based on FSMC and MSNQ scores. In addition, exploratory analyses were conducted to assess potential changes in other PROMs.
Participants served as their own controls, and pre–post changes were analyzed using paired t-tests or Wilcoxon signed-rank tests, depending on the data distribution assessed by the Shapiro–Wilk test. Between-group comparisons (completers vs. noncompleters) were conducted using independent t-tests, Wilcoxon rank-sum tests, or Fisher's exact test for categorical variables.
Statistical analyses were performed using R (Version 4.4.2), with a significance threshold set at p < 0.05. Partial dates were imputed using the midpoint of the corresponding month or year. Continuous variables were summarized as means with standard deviations or medians with interquartile ranges, depending on their distribution. Categorical variables were reported as frequencies and percentages based on nonmissing data.
Results
Of the 40 recruited pwMS, 35 (88%) opened the program, 33 (83%) initiated, and 23 (58%) completed the program, including the 3-month follow-up assessment. The mean duration from baseline to the seventh session was 200 days (range 46–474 days). Adherence to the program and reasons for discontinuation are illustrated in the flowchart (Figure 1). Reported reasons for discontinuation included technical issues (n = 6), health problems (n = 4), difficulties with time management (n = 3), and lack of computer access (n = 1). For three participants, no reason for nonparticipation or discontinuation was documented.
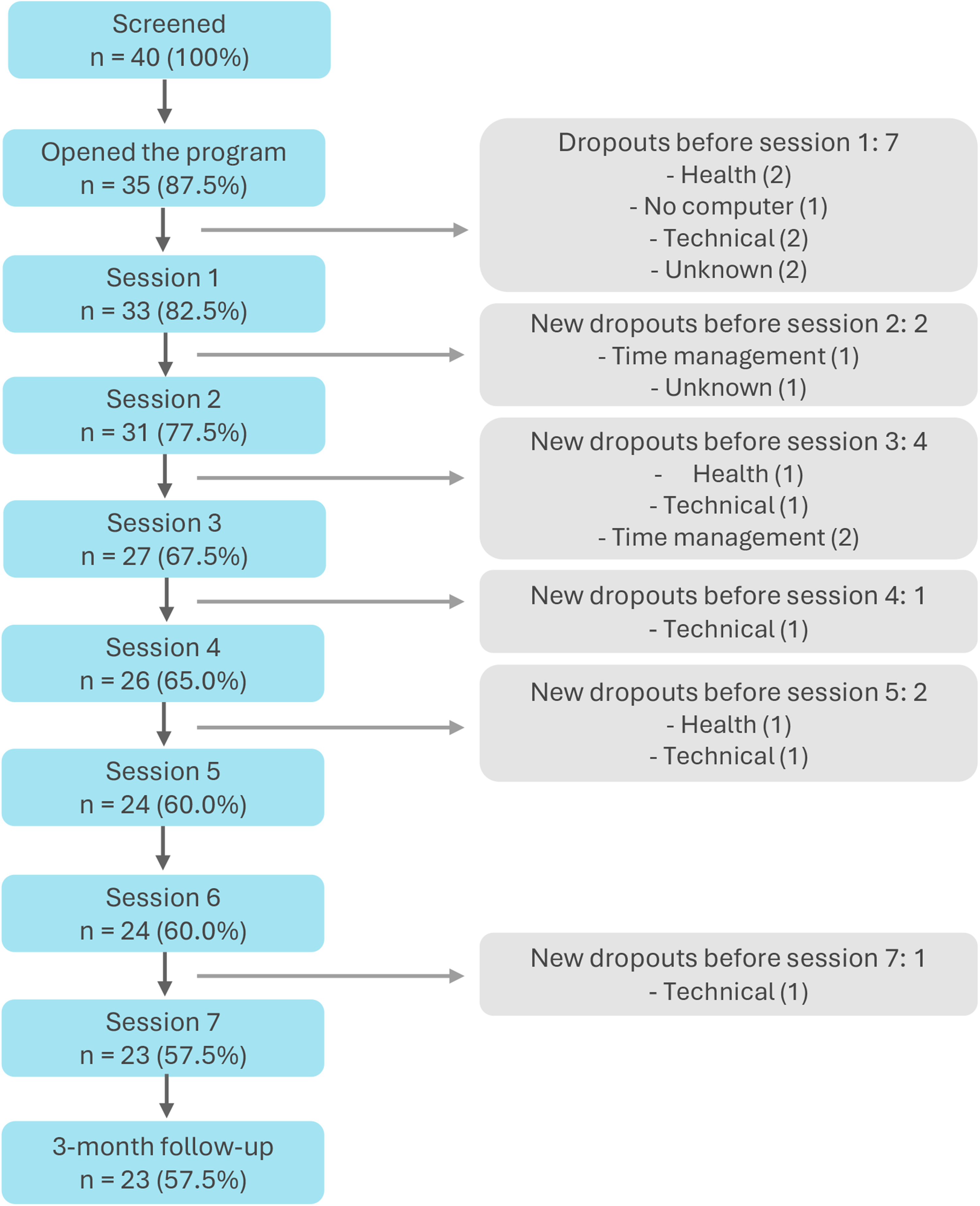
Flowchart describing the adherence to rehabilitation and reasons for discontinuation.
There were no statistically significant differences in terms of sex, age at program start, disease duration, or baseline EDSS between the group of participants who completed the program (n = 23) and the group who started but discontinued the rehabilitation (n = 10) (Table 2).
Demographics and disease-related variables of pwMS who completed the full program (n = 23) and those who discontinued the program (n = 10).
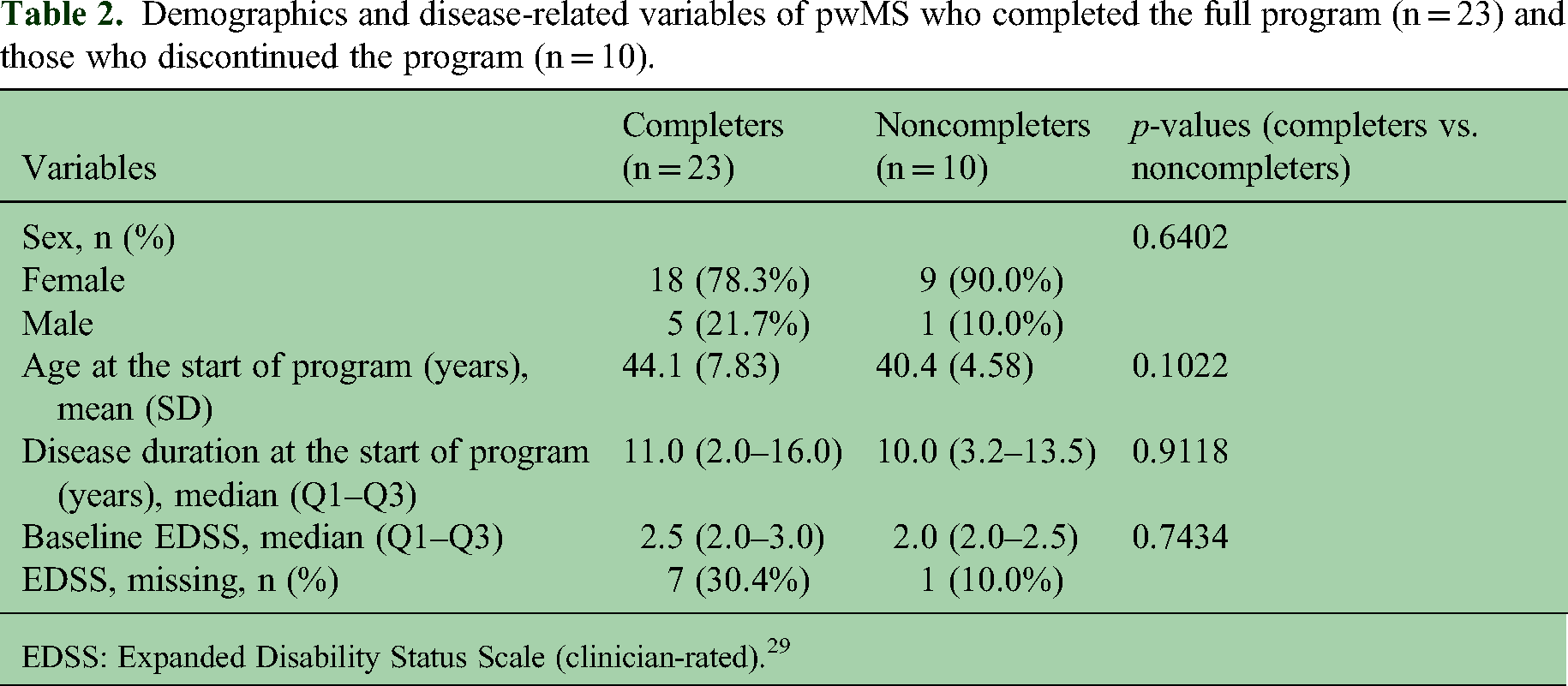
EDSS: Expanded Disability Status Scale (clinician-rated). 29
PROMs for the 23 completers and 10 noncompleters are presented in Table 3. Minimal differences were observed between completers and noncompleters at baseline. The mean MSNQ score was slightly lower among completers compared to noncompleters. The difference was, however, not statistically significant. Changes from baseline to postprogram were minimal overall.
Baseline values for pwMS who performed the baseline assessments (completers and noncompleters) and follow-up values for pwMS who conducted the full program (completers).
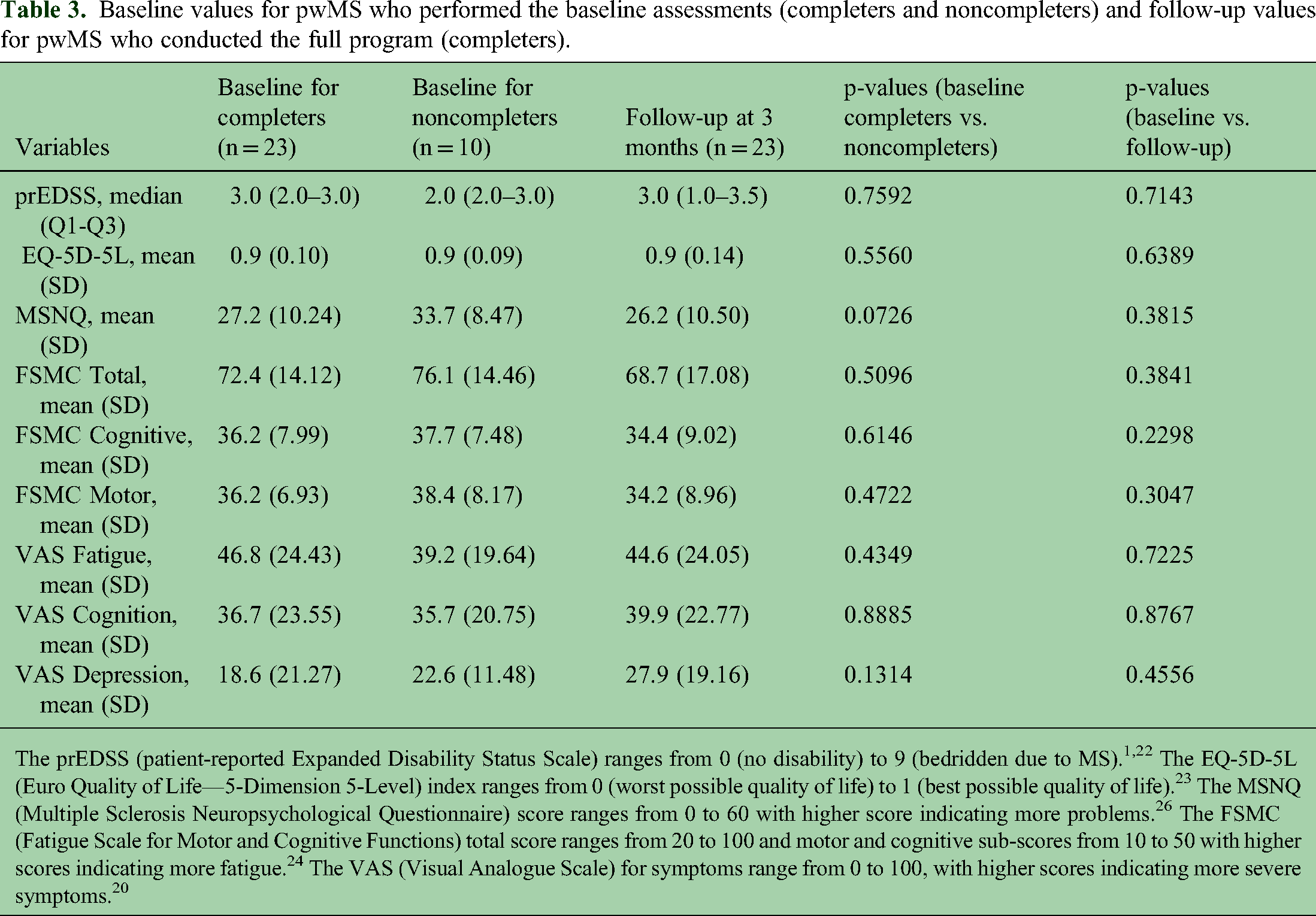
The prEDSS (patient-reported Expanded Disability Status Scale) ranges from 0 (no disability) to 9 (bedridden due to MS).1,22 The EQ-5D-5L (Euro Quality of Life—5-Dimension 5-Level) index ranges from 0 (worst possible quality of life) to 1 (best possible quality of life). 23 The MSNQ (Multiple Sclerosis Neuropsychological Questionnaire) score ranges from 0 to 60 with higher score indicating more problems. 26 The FSMC (Fatigue Scale for Motor and Cognitive Functions) total score ranges from 20 to 100 and motor and cognitive sub-scores from 10 to 50 with higher scores indicating more fatigue. 24 The VAS (Visual Analogue Scale) for symptoms range from 0 to 100, with higher scores indicating more severe symptoms. 20
Of the 23 participants who completed the program, 15 (65%) rated the program as beneficial, and 16 (70%) considered the technical implementation to be appropriate. At the end of the program, participants had achieved their individual rehabilitation goals, as indicated by a median GAS T-score of 50 (Table 4), which was maintained at 3-month follow-up. Participants also reported slight positive changes in the management of fatigue, cognitive symptoms, and ability to work or study, as reflected by slightly positive mean GRC scores (Table 4). The majority of participants evaluated the effects positively, which was defined as a GRC of +1 or higher. In the free feedback, completers acknowledged especially the usefulness of the fatigue diary and personal written feedback from the neuropsychologist.
Goal achievement values (GAS) at end of the program and after 3 months and global rating of change (GRC) values after 3 months.

In the GAS (Goal Attainment Scaling), the expected level of goal achievement is scored as 0; somewhat better achievement as +1; much better as +2; somewhat worse as −1; and much worse as −2. These ratings are converted to T-scores ranging from 30 (corresponding to −2) to 70 (corresponding to +2), with 50 representing the expected level of achievement. 27 Goals were not weighted. In the GRC (Global Rating of Change), the 11-point scale ranging from −5 (much worse) to +5 (much better) was used. 28
Discussion
The aim of the present study was to evaluate the feasibility and initial experiences of a digital symptom management program implemented within the Finnish MS Registry. The goal was to assess whether a registry-embedded digital intervention could serve as a practical and cost-effective tool to address early concerns related to fatigue and cognitive symptoms in pwMS. Early interventions should particularly target symptoms that impact employment, such as fatigue and cognitive impairment.2,3
In this study, 58% of the recruited pwMS completed the full program, including the 3-month follow-up. No statistically significant differences were observed between participants who completed the program (completers, n = 23) and those who started but discontinued (noncompleters, n = 10) in terms of demographic variables or PROMs. Among completers, 65% rated the program as useful, and 70% considered the technical implementation appropriate. GAS T-scores indicated that participants achieved their personal rehabilitation goals, and GRC evaluations suggested slight improvements in the management of fatigue, cognitive difficulties, and ability to work or study. However, no significant effects were observed on perceived cognitive problems or fatigue when measured by the MSNQ, the FSMC, or the VAS.
Earlier studies have demonstrated that neuropsychological and cognitive interventions can have positive effects on the management of cognitive symptoms.10,30 There is a particular need for cost-effective and individualized interventions that involve at least some input from healthcare professionals (HCPs). 6 The current Finnish initiative focused on developing an easily accessible program to help patients understand, evaluate, and manage cognitive problems and fatigue. It was integrated into the widely used Finnish MS Registry to enhance accessibility. 18 Motivation for self-management was supported through the use of GAS, which has been shown to capture individual patient needs and to serve as an appropriate outcome measure in traditional face-to-face neuropsychological rehabilitation. 31 GAS also showed potential in this web-based program, as indicated by the low number of missing evaluations and the overall positive goal attainment. These modest but encouraging results are in line with findings from other digital interventions and add to the growing evidence supporting the further development of eHealth approaches in MS care.14,32,33
A key strength of this study is that the program was accessible regardless of time and place, supporting flexible use by pwMS and potentially reducing burden on traditional face-to-face services. Further, the required HCP input was minimal (approximately 1–1.5 h per participant), supporting cost-effectiveness. The intervention targeted early fatigue and cognitive symptoms, which often remain under-addressed despite their substantial impact on work capacity and quality of life.2,3,6 The program was designed to support symptom awareness, understanding, and self-management. Many participants reported that the fatigue diary enhanced their understanding of the nature and variability of their symptoms and helped them identify appropriate management strategies. These characteristics suggest potential for broader clinical implementation as a scalable digital tool for early symptom management in MS.
This study has several limitations. One of the main limitations is the absence of predefined criteria for feasibility. The study design could have benefited from closer alignment with current recommendations for pilot studies, particularly with regard to sample size justification and the assessment of feasibility outcomes. For example, the hypothesis-testing framework for feasibility outcomes proposed by Lewis et al. 34 may have supported a more rigorous and transparent evaluation of progression criteria. Further, the sample size was small and limited to participants who were working or studying, potentially affecting generalizability. The program relies on participant motivation and cognitive capacity and may therefore be less suitable for individuals with more severe or widespread cognitive impairment. A total of 23 out of 40 (58%) pwMS completed the program. This was lower than typically reported for face-to-face interventions and lower than that observed in a web-based neuropsychological program for Finnish stroke patients (68%) 35 but fell within the range reported for exercise-based telerehabilitation (mean 67%, range 36–100%). 36 A more detailed survey, interviews, and qualitative analysis would have helped to identify factors underlying differential responses to the intervention, as well as the program components perceived as beneficial, with 65% of participants reporting benefit and 35% not perceiving benefit. The proportion of participants who initiated but did not complete the program (83%) was similar to the discontinuation rate in the Finnish stroke study (86%). 35 The main reasons for noncompletion were technical difficulties, health-related issues, and time management challenges. Participants with more pronounced cognitive impairment and fatigue may be at higher risk of discontinuation due to the increased burden these symptoms impose on everyday functioning. Further, the program lacked automated notifications for scheduling the next session, which may have contributed to lower adherence and prolonged completion times. The participants were, however, reminded about the ongoing process by e-mail if the interval from the previous session exceeded several weeks. Moreover, the browser-based interface was not optimal for younger users, some of whom would have preferred a mobile application. Automated notifications and a mobile application may be necessary improvements before the program can be further evaluated and considered for implementation. The results of the present study should be regarded as preliminary also due to the uncontrolled study design and due to the fact that we did not collect data on how many of the potential participants were unwilling to participate.
In conclusion, this study demonstrated that a web-based symptom management program integrated within an existing digital platform, the Finnish MS Registry, is a potentially useful tool for supporting the management of fatigue and cognitive symptoms in pwMS. Future development could include delivery through a mobile application, automated notifications, and more personalized feedback based on individual PROM responses. The fatigue diary, in particular, was highly valued and could also be used as a standalone tool. Additional enhancements such as artificial intelligence based virtual assistant functionalities or integration of individualized cognitive training modules could further strengthen the program. A more controlled study design is, however, needed to allow more robust evaluation of the program's effects.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contribution of the StellarQ IT team for building and continuously developing the Finnish MS Registry IT platform. Members of the study steering committee (Aija Kallio, Eeva-Liisa Kallio, Elina Lämsä, Taru Nikkilä, Eija Rosti-Otajärvi, Mervi Ryytty, Karoliina Tuominen) as well as participants of the present study are gratefully acknowledged. We also thank the study nurses for their efforts in participant recruitment. Building up the Finnish MS registry and the patient interface have received funding from Biogen Idec, Janssen, Merck, Novartis, Roche, Sanofi Genzyme, Teva, and Business Finland. The project received funding from Novartis Finland and Sanofi. The preparation of the manuscript was in part funded by the Strategic Research Council (SRC) established within the Academy of Finland (Funding Number 358415). ChatGPT was used solely for language editing. All scientific content, analysis, and interpretations were produced by the authors.
Data availability
The data is owned by the Finnish wellbeing services counties. StellarQ Ltd is the data processor for all the extracted data.
Declaration of conflict of interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PH is an employee of the Finnish Neuro Society and StellarQ. HK has served as an adviser or speaker or participated in a clinical trial for Merck, Biogen, Celgene, Novartis, Cytel, and Sanofi and received support for congress participation from Merck, Alexion and Novartis; Novartis, Roche, Sanofi. HN: none. SA: none. M S-H has served as an adviser or speaker or participated in a clinical trial for Biogen, Celgene (BMS), Novartis, Roche, Sanofi, and Teva; has received institutional research grants for clinical research from Bayer, Biogen, Merck, Novartis and Roche; and support for congress participation from Biogen, Celgene (BMS), Novartis, Roche, Sanofi, and Teva. MR has received honoraria for lectures, advisory boards, or congress visit from Abbvie, Biogen, Merck. JR None.
Ethical disclosure and patient consent
The study was approved by the Ethics Committee of the Wellbeing Services County of South-West Finland (Number 49/1801/2022). In the present study, patients consented the use of the data for the purposes of the study with their voluntary written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Building up the Finnish MS registry and the patient interface have received funding from Biogen Idec, Merck, Novartis, Roche, Sanofi Genzyme, Teva, and Business Finland. The project received funding from Novartis Finland and Sanofi. The preparation of the manuscript was in part funded by the Strategic Research Council (SRC) established within the Academy of Finland (Funding No. 358415).