
Abstract
Background
Many studies report different prevalence and incidence estimates for multiple sclerosis (MS). Epidemiological data from Southeast Europe remain scarce.
Objectives
This study aimed to estimate the prevalence, incidence, and demographic characteristics of MS in the Republic of Kosovo using data from the National MS Registry.
Methods
The Kosovo National MS Registry was established in January 2020. Patients diagnosed according to the 2017 McDonald criteria are automatically registered. Demographic and epidemiological data of all registered patients up to December 31, 2025, were analyzed. Prevalence and incidence rates were calculated using population data from the 2024 national census.
Results
A total of 776 MS patients were registered. Females accounted for 64.1% (n = 497), and males for 35.9% (n = 279), with a female-to-male ratio of 1.8:1. The mean patient age was 39.9 (±12.3) years. The national MS prevalence was estimated at 48.9 per 100,000 inhabitants. From 2020 to 2025, 373 new MS cases were diagnosed, with a mean annual incidence of 3.9 per 100,000 inhabitants. Nearly half of the patients were between 30 and 49 years old.
Conclusion
The results indicate a moderate prevalence with a steadily rising incidence, although the actual prevalence may be higher due to incomplete historical data prior to the registry's establishment.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease mainly linked to a variety of neurological symptoms. It primarily affects the central nervous system (CNS). The prevalence and incidence of MS have become key focus areas in epidemiology due to their implications for healthcare planning, research, and resource distribution, as well as for understanding the disease's underlying mechanisms. According to recent global estimates, approximately 1.89 million people were living with MS as of 2021, with a reported prevalence of 23.9 cases per 100,000 individuals, indicating a steady increase over the past three decades. 1 The epidemiological data confirmed an upward trend in MS incidence and prevalence worldwide, suggesting that factors affecting these rates are becoming more significant over time. 2 Notable variations have been documented in different areas within the same country. 3
Genetic predisposition, environmental factors, and lifestyle changes are among the elements that influence the varying prevalence and incidence of MS. Geographic factors are particularly significant; studies consistently show that MS is more common in regions at higher latitudes, where prevalence greatly exceeds that in areas closer to the equator. 4 This pattern aligns with vitamin D levels (affected by sunlight exposure), further supporting the idea that environmental factors play a role in MS development. 5 Recent demographic shifts and lifestyle changes have also been linked to increased incidence rates. Nondesired effects of urbanization, dietary changes, Epstein-Barr virus (EBV), UV exposure, smoking, and reduced physical activity have been cited as possible contributors to the observed rise in MS cases worldwide.6–10 The potential influence of social determinants of health, such as socioeconomic status and healthcare access, is increasingly recognized as important in understanding geographic and temporal variations in MS rates. 11
The only epidemiological study on MS prevalence and incidence in Kosovo was conducted from 2003 to 2012 and reported lower rates than those in regional and European data. 12 This study was limited to only hospitalized cases in the University Clinical Center, and therefore did not reflect the systematic data collection. The primary goal of this study is to analyze data from the National MS Registry of Kosovo and to determine prevalence and incidence rates of MS. After establishing the National MS Registry, which records, follows, and processes all data from Kosovo, we believe it will serve as a reliable source for understanding the epidemiological features of MS in Kosovo.
Gathering and analyzing current epidemiological data on MS is essential for several reasons. Accurate prevalence and incidence figures help shape healthcare policies, influence funding and resource allocation, and enhance patient care through informed treatment plans. 13 Additionally, understanding regional differences is vital for creating public health initiatives that address the specific demographic and environmental factors of those areas. 1 Ongoing research allows for the identification of potential risk factors and causal links, ultimately leading to better strategies for disease prevention and management.
Materials and methods
The MS National Registry of Kosovo was created in January 2020, alongside the establishment of the MS Unit within the Clinic of Neurology at the University Clinical Center of Kosovo (UCCK). This specialized unit acts as the national hub for referral, diagnosis, and comprehensive management of MS patients in Kosovo, ensuring standardized diagnostic procedures, coordinated care, and systematic data collection to support both clinical practice and epidemiological research. Since all MS patients in Kosovo are registered in the national registry and treatment decisions are made within the MS Unit, the Kosovo National Registry database was the only source of data used for epidemiological calculations in this study.
The Health Information System (HIS) of the Republic of Kosovo is an electronic database that registers patients’ health records. Although it includes International Classification of Diseases (ICD) categories for medical diagnoses, its failure to generate an electronic list of patients by ICD codes prevents data extraction for this query. As mentioned earlier, the request to refer all patients with MS to the MS Unit for discussion of disease-modifying treatment makes it unlikely that many patients will fall outside the scope of this calculation.
Data on the total population, sex, and municipality distribution were obtained from the latest 2024 Census of population, family economy, and housing, conducted in Kosovo between April 5 and May 17, 2024. These data were used to calculate prevalence and incidence, with separate analyses performed for the overall population and gender-specific groups.
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki. The collection and use of personal information for general, research, and scientific publication purposes are sanctioned by Law Nr. 04/L-125 for Health and Law Nr. 06/L-082 on the Protection of Personal Data, so neither ethics approval nor patient consent is required for registry studies.
Statistical analysis
Descriptive statistics of continuous data are presented as means with standard deviations (SD). Categorical variables are shown in frequencies and percentages. An independent-samples t-test was performed to compare the groups. A p-value of less than 0.05 was considered statistically significant. Statistical analyses were conducted using SPSS version 26.
Results
As of December 31, 2025, there were 776 registered MS patients diagnosed according to the McDonald criteria. Demographic data, including gender distribution, mean age, and prevalence and incidence estimates, were collected for these patients. Three patients were living outside the country at the time of diagnosis, and one was serving a prison sentence; therefore, they were excluded from regional or provincial prevalence calculations. Approximately two-thirds of the patients were female (497 or 64.1%), while the remaining were male (279 or 35.9%).
The most recent population census in the Republic of Kosovo was conducted in spring 2024. According to the published results, the country's population was officially recorded at 1,585,566. The prevalence of MS in Kosovo was estimated at 48.9 per 100,000 people (62.9 per 100,000 among females and 34.9 per 100,000 among males). Kosovo has 38 municipalities organized into 7 administrative regions. Because of the country's small size and the fact that some municipalities have only a few thousand residents, regional epidemiological calculations were considered more practical. The highest number of MS patients was in the capital, Prishtina, with 282 cases, and the Peja region had the highest prevalence rates (55.2 and 58.8, respectively). Gjakova and Gjilan had the lowest population and MS case counts, as well as the lowest prevalence rates (40.1 and 40, respectively). Table 1 shows the population, number of cases, age distribution, and prevalence rates for each region, while Figure 1 provides a map of Kosovo divided by regions.

Distribution of MS prevalence by region in Kosovo.
Number of cases, mean age, total population, and prevalence by sex and regions.
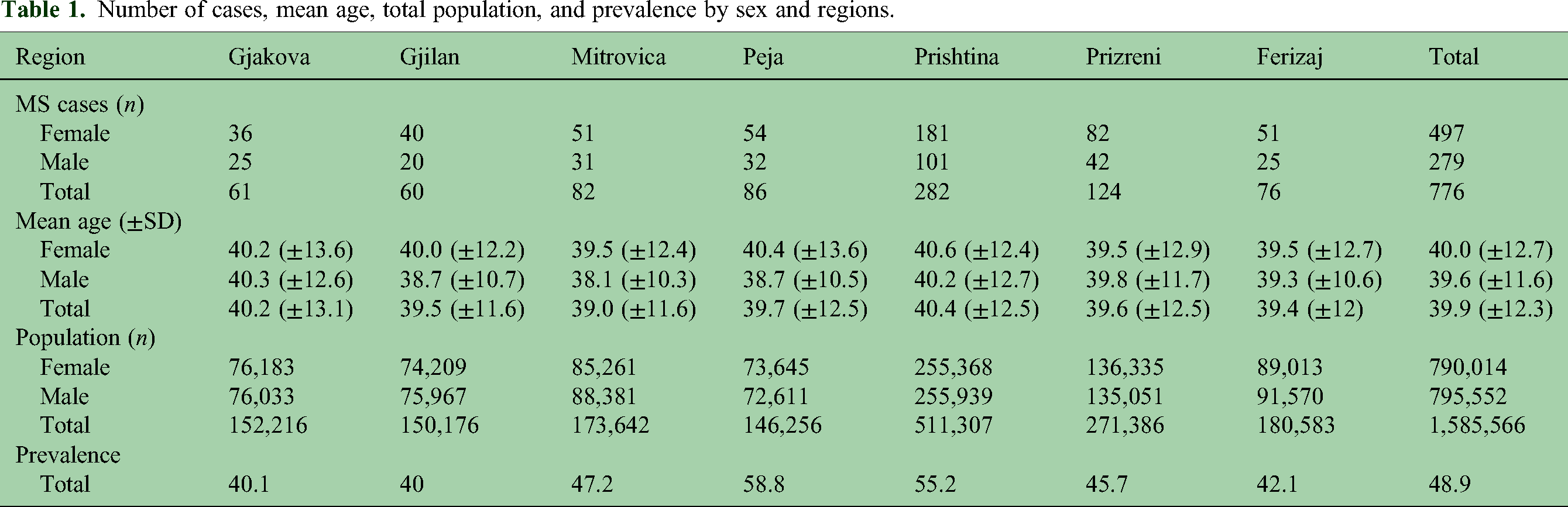
The mean age of the patients was 39.9 (±12.3) years. Female patients were slightly older, with a mean age of 40 years, while male patients had a mean age of 39.6 years (t-test p > 0.5). There was no significant difference in age distribution between the regions. Nearly half of the patients were in the 30–49 age group, and only 2.7% were under 19 years old (Table 2). About two-thirds of the patients were diagnosed between the ages of 20 and 39. The age distribution of the patients is shown in Figure 2.
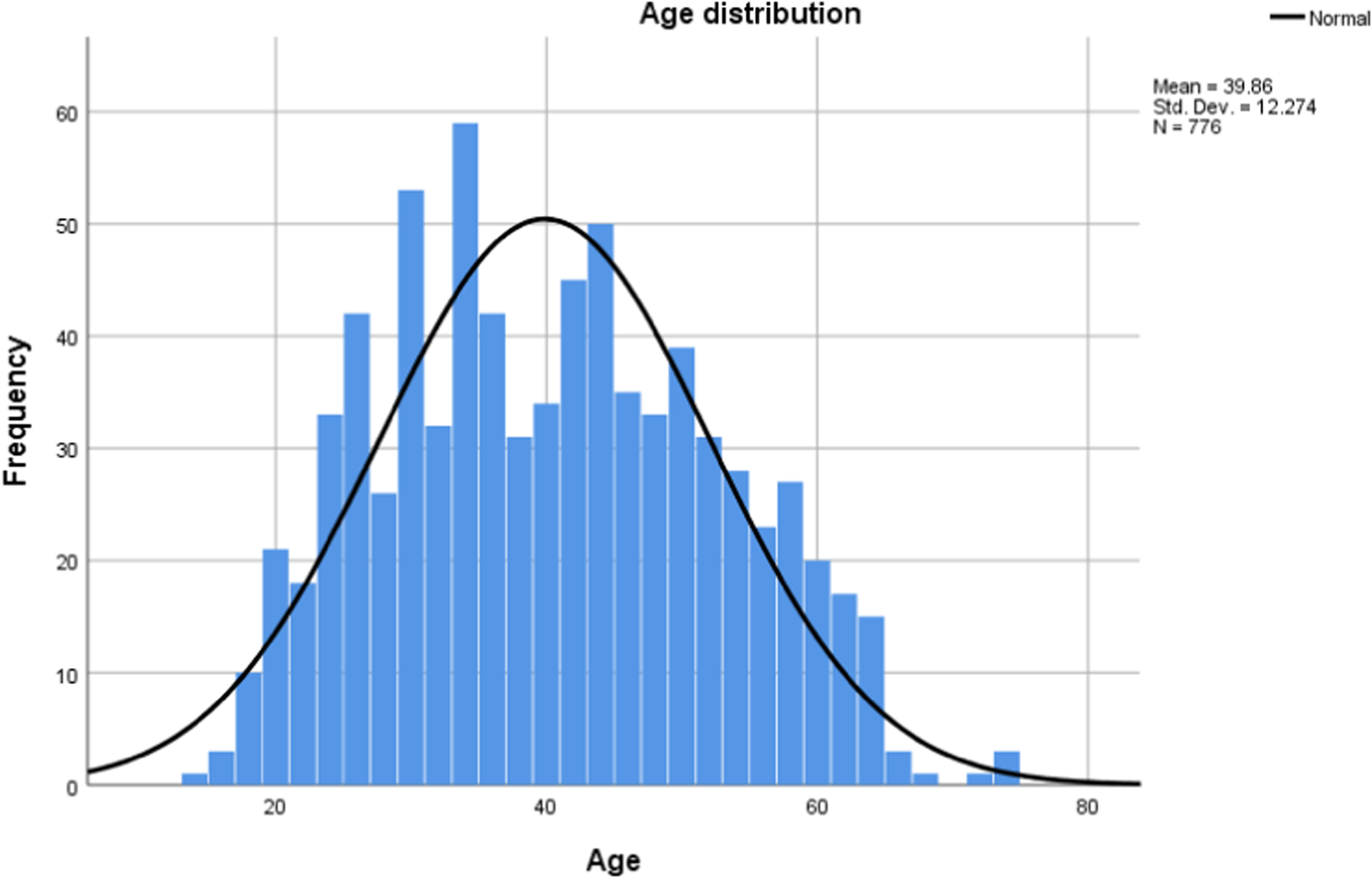
Age distribution of MS cases in Kosovo.
Age at diagnosis, current age, and prevalence by age groups.
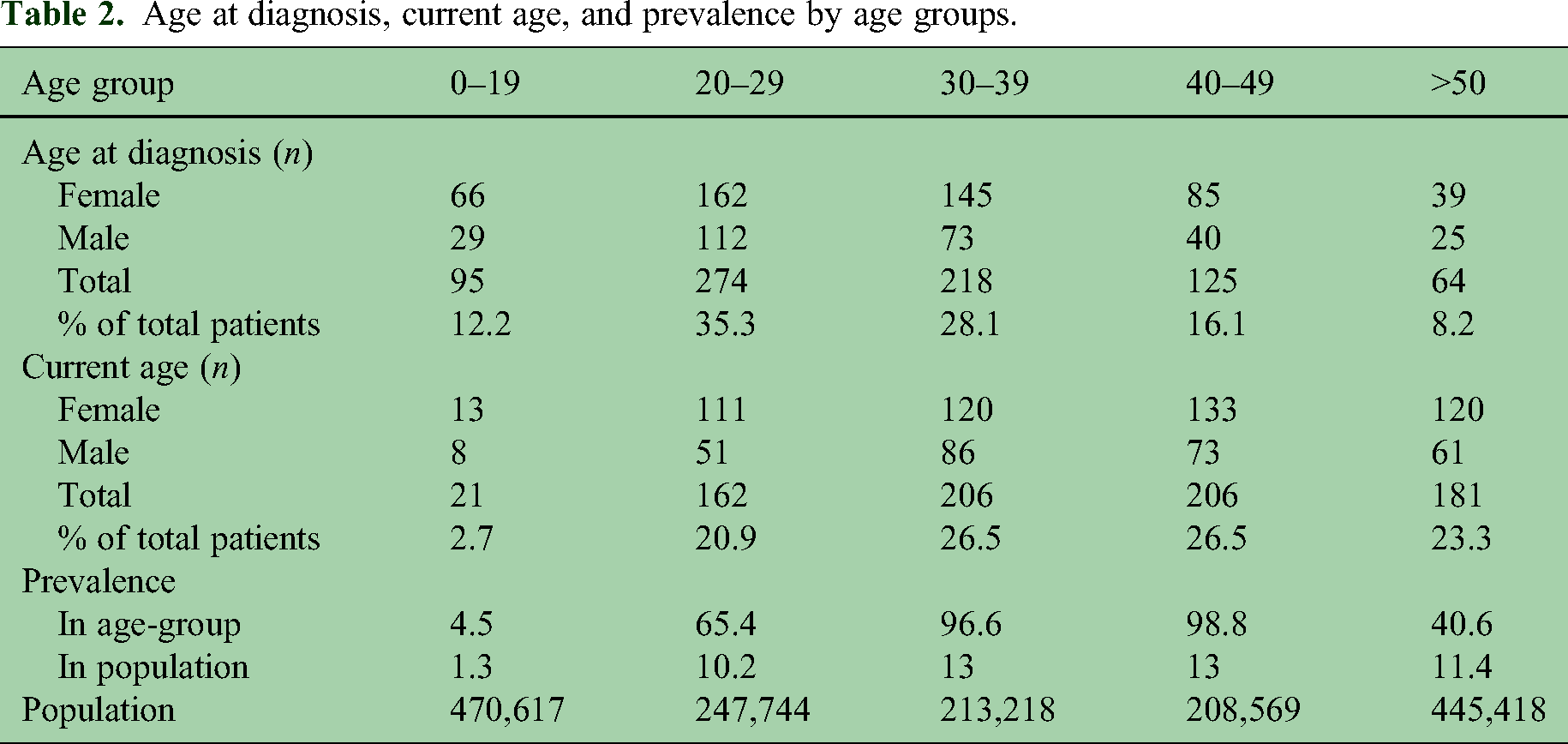
The mean age when symptoms most likely linked to MS appeared was 30.1 years, and the mean age at formal MS diagnosis was 32.2 years. Male patients were diagnosed slightly earlier, at 31.7 years, compared to females at 32.4 years (t-test, p > 0.5). The female-to-male ratio was calculated at 1.8:1. Table 2 provides a detailed breakdown by age group.
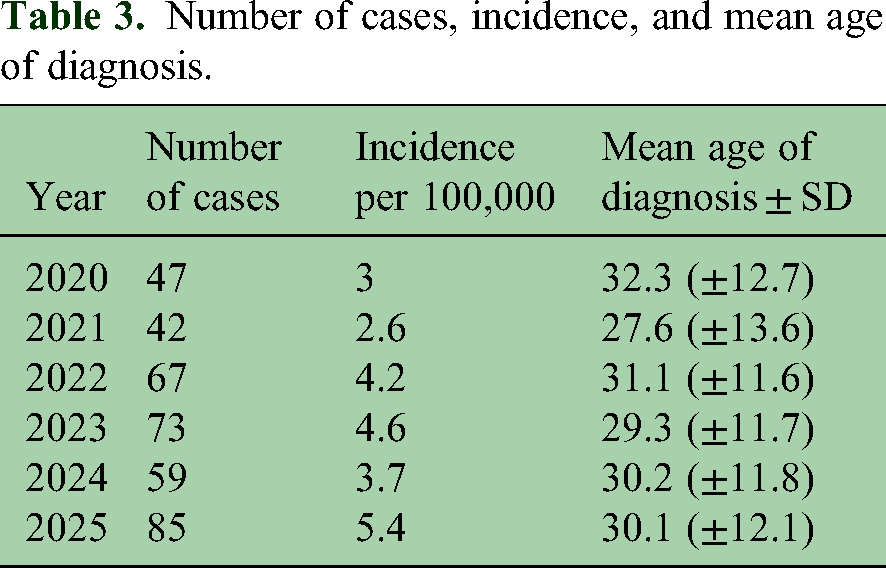
The incidence calculation was based on data from 2020 to 2025. During these 6 years, 373 new MS cases were diagnosed, representing 48% of all patients in our National MS Registry. This suggests that many patients diagnosed before 2020 are missing, indicating that the true national prevalence rate could be higher than estimated in this study. The incidence from 2020 to 2025 averaged 62.2 cases per year, or 3.9 cases per 100,000 inhabitants. Although the age at MS diagnosis has remained stable over these 6 years, the incidence appears to be gradually increasing, especially since 2022. Table 3 shows the number of cases, annual incidence rates, and mean age at diagnosis from 2020 to 2025.
Number of cases, incidence, and mean age of diagnosis.
Discussion
This study demonstrates that the prevalence of MS in Kosovo is 48.9 per 100,000 inhabitants, with an incidence of 3.9 per 100,000 inhabitants (2020–2025) and a mean age at symptom onset of 30.1 years. Nearly half of registered patients were diagnosed after 2020, reflecting the rapid expansion of case capture following the establishment of the National MS Registry. Importantly, our findings suggest that MS epidemiology in Kosovo remains actively shaped by improvements in diagnostic access, healthcare organization, and registry completeness. The main contribution of this study is establishing a baseline epidemiological framework for MS in Kosovo, which was previously unavailable.
MS affects about 2.8 million people worldwide. 14 The global burden of MS, as shown by the Global Burden of Disease (GBD) 2019 database, indicates significant differences across regions and countries. 15 Prevalence rates vary widely by region, with consistently higher rates in Europe and North America than in Asia and other regions. A 2020 study by the MS International Federation (MSIF) estimated that the number of people with MS increased from 2.3 million in 2013 to 2.8 million in 2020, with a global prevalence rate of 36 per 100,000. 13 MS prevalence and incidence estimates in South-eastern Europe, or the Balkan countries, generally show an increasing disease burden, consistent with global trends, but country-level data are inconsistent and often not directly comparable due to differences in methodology. Prevalence values are estimated at 96.4 in Turkey, 100–150 in Bulgaria, 136 in Serbia, and 143 per 100,000 in Croatia.16–19 Data are limited for other neighboring countries, including North Macedonia, Montenegro, and Albania. While the European mean prevalence rate is 133 per 100,000 people, Scandinavian countries consistently report among the highest MS prevalence rates globally, ranging from 188.9 per 100,000 in Sweden to 284 per 100,000 in Denmark.20–23 Conversely, South Korea, Japan, and China report lower MS prevalence and incidence rates than Western European and North American nations.15,24 The Middle East region is among the lowest-prevalence areas, with rates as low as 26 per 100,000 in the United Arab Emirates. 25
Prevalence values in Kosovo remain lower than those reported in Northern and Western European countries at similar latitudes. This difference is unlikely to be explained by latitude alone and instead likely reflects a combination of health system, diagnostic, and population-level factors. First, underdetection and historical underdiagnosis are highly probable. Prior to 2020, Kosovo lacked a centralized MS registry and had limited access to MRI and disease-modifying therapies. Many patients with milder or early disease may therefore have remained underdiagnosed or unrecorded. Second, registry completeness and case capture bias likely influence prevalence estimates. Although the current registry has improved coverage, cases diagnosed before its establishment may not have been systematically retrieved, particularly those managed outside specialized neurology services or those who migrated abroad. Third, healthcare access and referral patterns may have contributed: delayed neurologist referral, reliance on primary care, and variable access to neuroimaging likely contributed to missed or delayed diagnosis. Fourth, population mobility and migration may have reduced the observed burden, as some patients diagnosed earlier may have relocated to Western European countries for treatment or long-term care. Finally, genetic and environmental contributors cannot be excluded. Differences in vitamin D exposure, lifestyle factors, infectious exposures, and genetic background may also play a role.
National multiple sclerosis registries have become essential tools for large-scale epidemiological research, providing population-level data on disease incidence, prevalence, natural history, risk factors, and treatment results. These registries, which operate across multiple countries, enable researchers to conduct studies that would be impossible with traditional clinical trial designs.20,21 The expanding body of research based on national MS registries shows a notable shift toward real-world evidence in MS research. 21 The Danish MS Registry (DMSR) is considered the world's oldest operational and nationwide MS registry. The Swedish, Norwegian, Finnish, and, most recently, German MS Registries follow a similar pattern of prospectively recording and collecting all MS cases within their respective countries, integrating and cross-checking the data with their national healthcare databases.22,23,26,27
A key strength of the Kosovan system is the establishment of a centralized MS Reference Unit and National Registry, which has fundamentally changed disease detection and management. The MS Unit at the University Clinical Center of Kosovo serves as the national referral hub for the diagnosis, initiation of treatment, and long-term follow-up of all suspected and confirmed cases. The introduction of a structured referral pathway has led to mandatory central evaluation of all suspected MS cases, standardized diagnostic confirmation using contemporary criteria, systematic initiation and monitoring of disease-modifying therapies, improved continuity of care and completeness of follow-up, and the creation of a unified electronic registry with unique patient identifiers. Importantly, nearly 48% of all registry cases were diagnosed after 2020, highlighting the direct impact of system organization on case detection rather than a sudden epidemiological surge. This demonstrates that the observed increase in prevalence is likely driven by improved ascertainment rather than a true abrupt rise in disease occurrence. Thus, the MS Reference Center serves not only as the clinical infrastructure but also as an epidemiological surveillance tool, significantly enhancing the accuracy and completeness of national MS data.
Only in this decade has at least one immunomodulatory treatment option become available to all people diagnosed with MS. Notification of the entire neurological community about the establishment of the National MS Unit and Registry, along with information on treatment availability, has led to the mandatory referral of all suspected and diagnosed cases to the University Clinical Center. The functionality of the MS Unit and Referral Center, including monitoring, follow-up, and treatment of all MS patients, also serves as a feedback loop for government agencies to better plan and fund more diverse and effective treatment options for the future.
A consistent finding across multiple studies is an increase in MS prevalence over time.28,29 This rise in prevalence has been attributed to several factors, especially the longer life expectancy among individuals with MS. 29 Improved diagnostic criteria, greater clinical awareness, and advancements in neuroimaging have also contributed to increased case identification. Recent international epidemiological data estimate the global MS incidence at approximately 2.1–2.5 per 100,000 per year. 2 National MS registries have facilitated the monitoring of long-term incidence patterns. In Sweden, the nationwide mean MS incidence from 2001 to 2008 was estimated at 10.2 per 100,000 people, which was significantly higher than earlier estimates. 20 In Denmark, MS incidence remained steady at around 3.5 per 100,000 until 1975, then increased steadily by more than 2.5 times to 11.4 per 100,000 by 2000. 30 A key contribution of national MS registries has been the ability to evaluate how changing diagnostic criteria affect incidence estimates. 23
Although the prevalence rate in Kosovo remains lower than in European and neighboring countries, the incidence of 3.9 per 100,000 is closer to the figures reported in those countries. Considering that the incidence estimate is based on data from 2020 to 2025, this trend indicates that, with this incidence, the number of people diagnosed with MS will increase each year, and the prevalence rate will approach the values seen in neighboring and Central European countries. Our study found a mean age of symptom onset suggestive of MS at 30.1 years, aligning with many studies indicating a mean onset in the early to mid-30s.31,32 Some studies have observed that the interval between the first symptom and diagnosis ranges from 2.5 to 3 years. 33 In our cohort, this interval was 25 months. Most delays were caused by patients not being seen by a general practitioner or neurologist, or by mild, nonspecific symptoms that did not suggest MS, leading to a lack of referral for further investigation. The use of MRI-based diagnostic criteria has helped reduce the time between symptom onset and diagnosis. 34 Diagnosis was made earlier in familial cases compared to sporadic cases. 35
The strength of this study lies in selecting data from a single, centralized database that serves as the primary source for referring all suspected and diagnosed MS cases in Kosovo. The MS Unit at the Clinic of Neurology at the University Clinical Center of Kosovo conducts formal MS diagnoses, diagnostic and pretreatment assessments, decides on the type of disease-modifying treatment, and provides ongoing patient follow-up. All MS patients in Kosovo have a unique identification number within the National MS Registry. Healthcare professionals in the MS Unit keep physical files, while the lead author manages electronic records, coding, and updates. The electronic database is an Excel sheet tailored for each item, and coding enables quick, easy data extraction for presentation and publication. We believe that the centralized National Registry is valuable for managing disease flow among MS patients and offers the most accurate, current data on the condition in the country.
This study has several important limitations. The absence of reliable pre-2020 registry data limits the ability to reconstruct historical incidence and assess long-term temporal trends. Consequently, true changes in disease frequency over time cannot be distinguished from improved detection. Underascertainment of pre-existing cases is likely, particularly among patients diagnosed before the registry's establishment who were not retrospectively captured. Although the registry is population-based, referral bias may persist, as case inclusion depends on interaction with healthcare services and referral to the MS Unit. Also, healthcare-seeking behavior may influence case capture, as individuals with mild or nonspecific symptoms may delay or avoid medical evaluation. Despite these limitations, establishing a centralized registry represents a major methodological advance and provides the most reliable epidemiological data on MS currently available in Kosovo.
Conclusion
Multiple sclerosis in Kosovo shows a moderate prevalence with a clear female predominance and a peak diagnosis age in early adulthood. The increasing number of newly diagnosed cases in recent years may reflect improved diagnostic capacity and better case registration following the establishment of the National MS Registry in 2000. However, incomplete data from the pre-registry period likely underestimate the true national prevalence. Continued registry strength and systematic data collection will be essential for accurately monitoring MS epidemiology and planning healthcare resources in Kosovo.
Footnotes
Data availability statement
Data are available upon reasonable request from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.