
Abstract
Background
Glial fibrillary acidic protein (GFAP) is an astrocyte marker increasingly recognized as a biomarker of disease progression in multiple sclerosis (MS). While highly sensitive assays are available, cross-platform harmonization remains insufficient, limiting routine clinical implementation.
Objective
To compare three fully automated GFAP assays, assess their analytical agreement and clinical performance across MS subtypes and healthy controls, and evaluate cross-platform conversion approaches.
Methods
Serum samples from 435 individuals (298 healthy controls, 51 relapsing–remitting MS (RRMS), 41 primary/secondary progressive MS (PPMS/SPMS)) were analyzed using three automated platforms: Simoa HD-X (Quanterix), Elecsys (Roche), and Lumipulse G600 (Fujirebio). Correlation analyses, Passing–Bablok regression, and Lin's concordance coefficients were applied. Published regression formulas were compared with study-derived equations.
Results
Strong correlations were observed across all platforms (r > 0.90 with outliers; r > 0.95 without; p < 0.001), though minor systematic biases were detected. Progressive MS patients showed significantly higher GFAP concentrations than RRMS and controls. Conversion to a single-platform scale improved agreement, but regression formulas differed substantially from previously published equations.
Conclusion
Serum GFAP measurements demonstrate high clinical comparability across automated platforms despite systematic differences in absolute values. Robust harmonization strategies and externally validated conversion models are required before broad implementation in routine MS diagnostics.
Introduction
Glial fibrillary acidic protein (GFAP) is an intermediate filament protein expressed by astrocytes 1 and is upregulated in response to injury, inflammation and demyelination. 2 In multiple sclerosis (MS), GFAP has emerged as a promising biomarker of disease progression.3–5 Despite the availability of highly sensitive immunoassays for GFAP quantification, no universally accepted gold standard has been established. Rigorous harmonization and standardization are therefore required before GFAP measurement can be reliably implemented in routine clinical practice. Most data derive from research-based single-molecule array (Simoa; Quanterix) platforms, 6 while widely available automated immunoassays—such as the Elecsys GFAP assay (Roche Diagnostics) 7 and the Lumipulse blood GFAP assay (Fujirebio) 8 —now provide sufficient sensitivity to quantify brain-specific proteins in blood. This study aimed to compare three serum GFAP assays, assess their correlation and clinical performance across MS stages versus healthy controls, and contextualize the findings within emerging cross-platform literature.
Materials and methods
A total of 435 serum samples (298 healthy controls (HC), 51 patients with relapsing remitting MS (RRMS): 45 paired samples in relapse and remission + 6 relapse-only samples; 41 patients with primary and secondary progressive MS (PPMS/SPMS), (Supplemental Table 1) were analyzed in singlicate on three fully automated platforms using commercially available reagents: GFAP Advantage Plus on the HD-X (Quanterix, Billerica, USA), Elecsys GFAP on the cobas pro e801 (Roche Diagnostics, Rotkreuz, Switzerland), and GFAP-G Lumipulse Blood on the Lumipulse G600II (Fujirebio, Tokyo, Japan). Sample handling and statistical analyses are described in the Supplemental Material.
Results
Twelve samples (2.8%, 10 healthy controls and two RRMS patients) were identified as outliers (Supplemental Table 2). Outliers showed no systematic association with any platform or direction of deviation. Strong correlations were observed across all three platforms with (r > 0.90, p < 0.001) and without outliers (r > 0.95, p < 0.001), with a minor systematic bias indicated by Passing–Bablok regression (Figure 1A to C; Supplemental Table 3). Outliers showed no systematic association with any platform or direction of deviation and were excluded from further analyses. Elecsys GFAP and GFAP-G Lumipulse Blood values were converted to the GFAP Advantage Plus scale using Passing Bablok regression, which improved agreement across assays as reflected by higher Lin's concordance correlation coefficients (Supplemental Table 3).
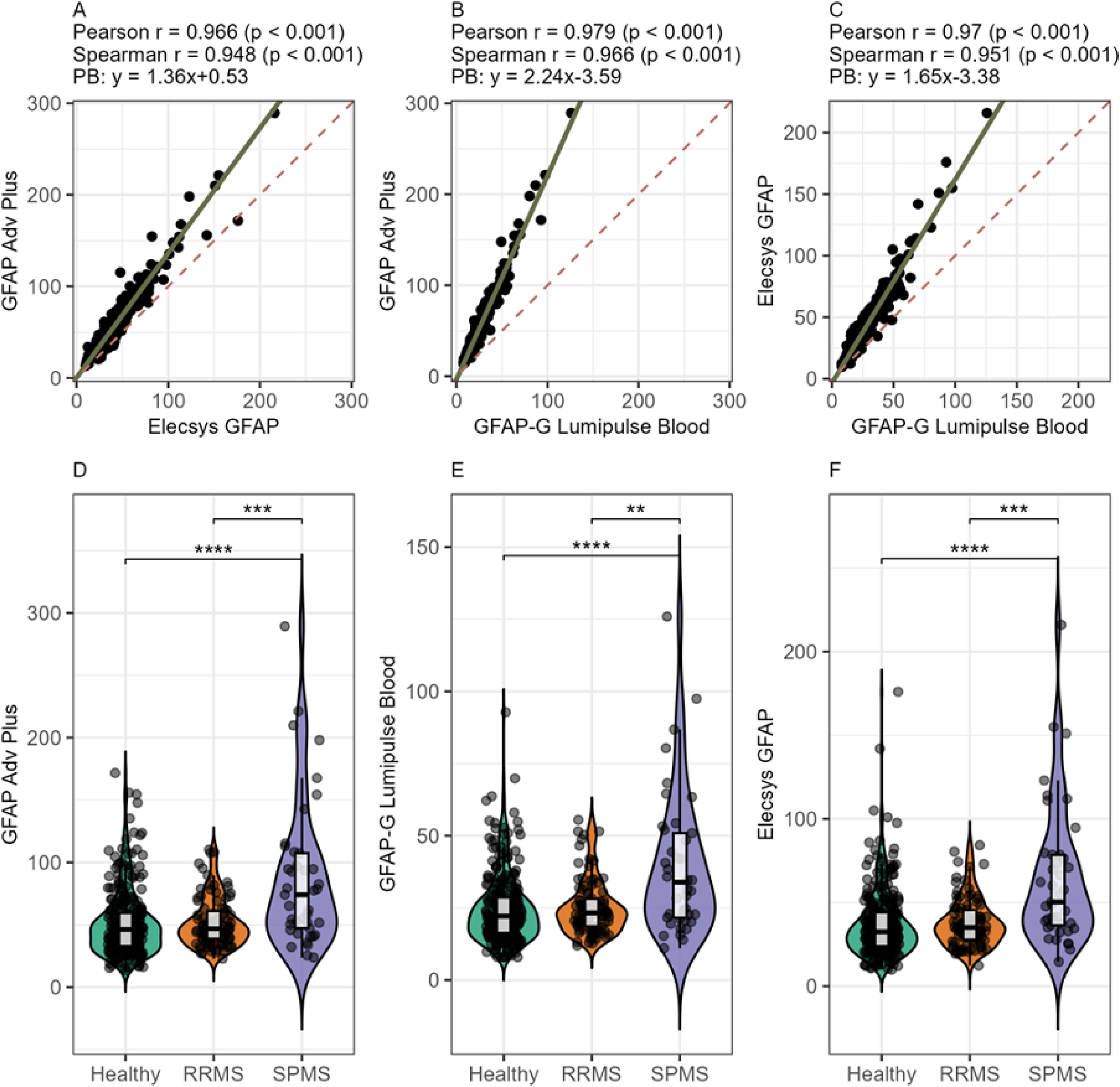
Cross-platform comparison: (A–C) correlation and Passing–Bablock (PB) regression between platforms and (D–F) comparison between groups (healthy controls (HC)), patients with relapsing-remitting multiple sclerosis (RRMS) and progressive multiple sclerosis (PMS). ** p < 0.01; *** p < 0.001; **** p < 0.0001, Adv = advantage.
A moderate positive correlation between age and GFAP concentration in HC was observed on all platforms (r > 0.4, p < 0.001, Supplemental Figure 2). Group comparisons revealed higher GFAP levels in PPMS/SPMS patients compared with HC and RRMS patients (Figure 1D to F), remaining significant after adjusting for age (Supplemental Table 4). No significant differences were detected between HC and RRMS patients or between relapse and remission in the RRMS group (Figure 1 and Supplemental Figure 3).
We extracted the reported Passing–Bablok regression formulas from previously published studies that used the same assays as ours and compared them with our results.9,10 Visual inspection of the Passing–Bablok regression lines revealed noticeable discrepancies between studies, and the 95% confidence intervals for slope and intercept showed only minimal overlap, indicating study-specific differences in proportional and constant components of the regression relationships (Figure 2).
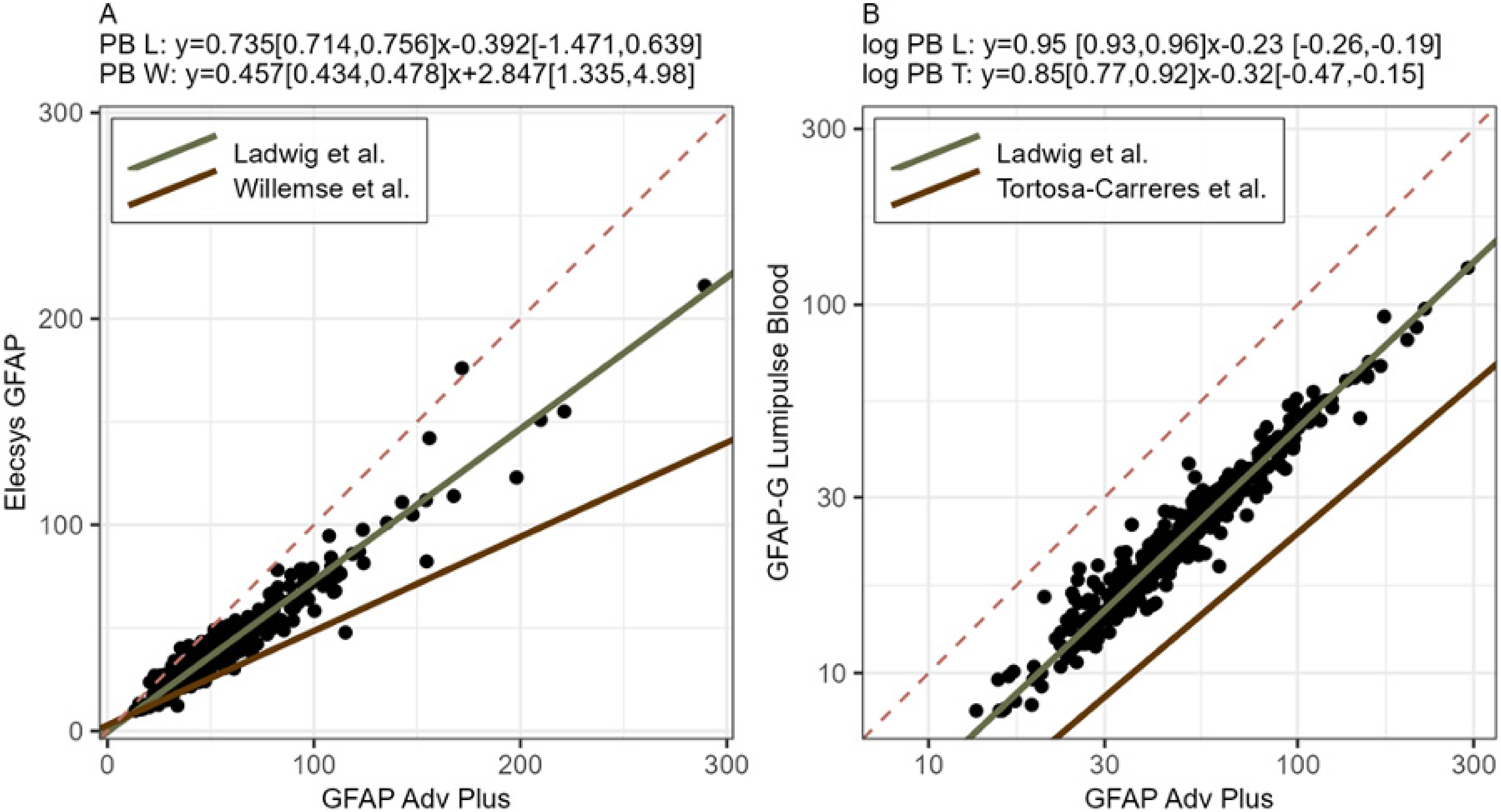
Comparison of Passing–Bablok (PB) regression from this study (Ladwig et al.) with Willemse et al. (W) in (A) and Tortosa-Carreres et al. (T) in (B). In (B), all values are converted to a logarithmic scale as in the referred publication.
Discussion
In our study, a high level of association was observed across all three platforms in both healthy controls and patients with multiple sclerosis at different disease stages, reflected by strong correlations between all tested assays, supporting the high clinical comparability of serum GFAP measurements. This is further reinforced by known consistent group differences observed across all assays, with higher GFAP concentrations in SPMS and PPMS compared with RRMS and HC,11–14 in line with the role of GFAP as a biomarker of smouldering, compartmentalized inflammation. 15 Low GFAP levels in patients with RRMS were also clinically plausible, given the short follow-up time, short disease duration, and the absence of relapse-independent disease progression in our cohort. In addition, the known positive association between GFAP and age in HC was reproduced across all tested assays. 8
However, despite strong cross-platform correlation and substantial concordance in clinical stratification, systematic differences in absolute GFAP concentrations remained between analytical platforms. Such platform-dependent bias is clinically relevant for longitudinal assessments across methods, the application of established cut-off values, and comparisons with historical cohorts. Consistent with our findings, several prior cross-platform comparison studies of GFAP measurements have also reported high correlations between the tested assays with systematic bias in absolute values.9,10,16 However, none of these publications, including our own work, evaluated all commercially available assays for GFAP quantification. Notably, our study extends beyond prior work by being the first to systematically compare Passing–Bablok regression relationships across different studies, thereby highlighting clinically relevant discrepancies between reported conversion approaches and underscoring the limited generalizability of such models across platforms and cohorts.
Although conversion of GFAP values to a single-platform scale using Passing–Bablok regression—here based on a Simoa assay—improved cross-platform agreement, the generalizability of published conversion formulas remains limited, as illustrated by differences between Passing–Bablok regression equations reported across studies. Potential explanations include the use of different assay generations for GFAP quantification, differences in antibody epitope specificity and binding characteristics, and heterogeneity in cohort composition. In particular, varying proportions of healthy and diseased individuals may have resulted in spectrum effects and unequal distribution of low and high GFAP concentrations, thereby influencing regression estimates.
A small subset of samples showed discrepant values on one platform, similar to observations in NfL analyses. 17 These outliers may reflect matrix effects, heterophilic antibody interference or interference from endogenous substances, whereas pre-analytical variability appears unlikely given the standardized sampling and processing conditions in our cohort. GFAP values should therefore be interpreted within the clinical context, and confirmation on an alternative platform may be warranted when results appear inconsistent.
This study has several limitations. We focused on analytical comparison and did not assess detailed associations with clinical parameters. Not all available GFAP platforms were included; thus, our findings provide proof of concept rather than a definitive harmonization framework. Future studies should incorporate all assays used in routine diagnostics, validate conversion formulas in independent external cohorts, and include larger, more diverse populations encompassing other neurological diseases with balanced distributions of low and high GFAP concentrations.
In conclusion, serum GFAP measurements obtained with three automated immunoassays showed strong correlation despite systematic differences in absolute values. Although Passing–Bablok-based conversion improved agreement within our dataset, the derived formulas differed from previous reports. More robust conversion equations based on larger, more heterogeneous cohorts are therefore required. Until validated harmonization approaches are available, the assay used should be explicitly reported, particularly for individual patient interpretation. External quality controls and clinical verification of unexpected results are also recommended.
Supplemental Material
sj-docx-1-mso-10.1177_20552173261460155 - Supplemental material for Cross-platform comparison of blood glial fibrillary acidic protein quantification in healthy controls and multiple sclerosis
Supplemental material, sj-docx-1-mso-10.1177_20552173261460155 for Cross-platform comparison of blood glial fibrillary acidic protein quantification in healthy controls and multiple sclerosis by Anne Ladwig, Antje Torge, Kim Kristin Falk, Antonia Dammann, Melanie Schlapkohl, Klarissa Hanja Stürner, Klaus-Peter Wandinger, Robert Markewitz, Ralf Junker, Malte Ziemann, Sven Ole Schuster, Johannes Piel, Frank Leypoldt and Justina Dargvainiene in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Data availability statement
Original data can be provided upon reasonable request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FL receives funding from the German Federal Ministry of Education and Research (CONNECT-GENERATE grant no. 01GM1908A and 01GM2208). FL is also supported by E-Rare Joint Transnational research support (ERA-Net, LE3064/2-1), European Joint Program for Neurodegenerative Diseases (EJPRD) IGNITEMIND (01ED2506B), ERA-Net MICE-AE (01EW2507B), Stiftung Pathobiochemie of the German Society for Laboratory Medicine and HORIZON MSCA 2022 Doctoral Network 101119457—IgG4-TREAT and discloses speaker honoraria from Grifols, Teva, Biogen, Bayer, Roche, Novartis, Fresenius, travel funding from Merck, Grifols and Bayer and serving on advisory boards for Roche, Biogen and Alexion. AL discloses speaker honoraria from UCB pharma. KHS has received speaker honoraria and/or travel grants from Sanofi, F. Hofmann-La Roche, Biogen, Bristol Myers Squibb, Merck, and UCB pharma.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a habilitation grant from the Faculty of Medicine at Christian-Albrechts-University of Kiel, awarded to Justina Dargvainiene. Additionally, we received funding from Damp Stiftung for recruitment of the relapse cohort, awarded to Anne Ladwig and Klarissa Hanja Stürner.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.