
Abstract
Background
Internuclear ophthalmoparesis (INO) in multiple sclerosis (MS) reflects impaired signal transmission within the medial longitudinal fasciculus (MLF). Increased pulse size ratio (PSR) and prolonged pulse time delay (PTD) quantify interocular velocity asymmetry and transmission timing.
Objective
To characterize PSR and PTD during ocular-motor fatigue in MS-related INO and the effects of dalfampridine.
Methods
In a randomized, double-blind, placebo-controlled crossover trial, 19 participants with MS-related INO underwent eye-movement recordings during a 10-min saccadic task. PSR and PTD were analyzed at saccade, INO, and participant levels.
Results
23,904 INO and 2408 control paired saccades were analyzed. In INO, PTD was prolonged and PSR elevated, with a positive correlation. Dalfampridine did not significantly improve prespecified ocular-motor outcomes, including mean PSR, mean PTD, or early–late fatigue measures. Responses were heterogeneous. Exploratory analyses showed dynamic PSR and PTD fluctuations, with a trend toward reduced PSR variability during dalfampridine. Greater trough PTD variability was associated with larger PTD shortening during dalfampridine, but not placebo.
Conclusions
Dalfampridine did not significantly improve prespecified ocular-motor outcomes. PSR and PTD capture complementary aspects of internuclear signal transmission, with ocular-motor fatigue reflecting dynamic instability. PTD variability is associated with variation in response to dalfampridine, supporting further study as a tract-specific biomarker.
Introduction
Internuclear ophthalmoparesis (INO) is the most common ocular motor disorder in MS and reflects demyelinating injury of the medial longitudinal fasciculus (MLF), occurring in approximately one-third of patients.1–3 MLF demyelination causes slowing of eye adduction during horizontal saccades. Clinically, INO is a cornerstone diagnostic sign 4 and is associated with higher Expanded Disability Status Scale (EDSS) scores, cognitive impairment, and visual disability.1,2,5–7 No therapy specifically targets INO.
Quantitative eye tracking and video-oculography have increasingly been used to characterize MS-related ocular-motor dysfunction beyond the bedside examination. In MS cohorts, these methods have identified abnormalities of INO, saccadic timing, ocular-motor fatigability, smooth pursuit, fixation, and binocular coordination, with associations to visual function, disability, MRI measures of CNS injury, and cortical network dysfunction.8,9
The neural control of horizontal saccades is well characterized. 3 Excitatory burst neurons in the paramedian pontine reticular formation (PPRF) generate a high-frequency “pulse” of innervation to the ipsilateral abducens nucleus, which drives the lateral rectus muscle and, via the MLF, the contralateral medial rectus. In healthy individuals, this network produces rapid, conjugate saccades with closely matched peak velocities between the two eyes. In INO, demyelination within the MLF reduces the neural signal delivered to the adducting eye, resulting in decreased peak velocity. The asymmetry between the two eyes is quantified by the pulse size ratio (PSR; also termed versional disconjugacy index), defined as the abducting-to-adducting eye peak-velocity ratio.1,10–12
Pulse time delay (PTD), defined as the interocular latency between abducting and adducting saccade onset, has been proposed as a complementary measure of internuclear signal transmission. 12 Whereas PSR reflects pulse size asymmetry, PTD provides a physiologic estimate of signal transmission timing across the MLF. Based on prior healthy-control data, PTD is typically approximately 1–2 ms but is prolonged in INO. 12
Prior work, supported by a control-system model of saccadic disconjugacy, 13 showed that these measures change during repetitive saccadic activity, a phenomenon referred to as ocular-motor fatigue.12,14 Although such changes might be expected to manifest as progressive worsening over time, observations have revealed variable patterns across individuals.12,14,15 These findings indicate that ocular-motor performance during sustained activity may not be fully captured by averaged measures of PSR and PTD.
INO has been proposed as a quantitative biomarker of axonal and myelin integrity within the MLF. Diffusion tensor imaging and electrophysiologic studies have demonstrated correlations between structural injury and abnormal eye-movement metrics.16–18 However, the physiologic basis of ocular-motor fatigue in INO, its responsiveness to pharmacologic modulation, and its potential relevance to primary motor fatigue in MS remain incompletely understood.
Dalfampridine, a voltage-gated potassium channel blocker, improves action potential conduction in demyelinated axons and enhances walking speed in MS.19,20 Serra et al. demonstrated improved binocular conjugacy and reduced abducting-eye nystagmus after dalfampridine 10 mg in patients with MS-related INO. 21 In a randomized crossover study, Kanhai et al. reported short-term improvements in saccadic disconjugacy after a single 20 mg dose of fampridine. 22 However, these studies examined only pharmacological effects and did not evaluate sustained saccadic activity or conduction-timing metrics such as PTD.
In this randomized crossover study, we quantified PSR and PTD during sustained saccadic activity in MS-related INO to characterize changes in internuclear signal transmission associated with ocular-motor fatigue and to determine whether dalfampridine alters these parameters.
Methods
Trial design
This was a 10-week randomized, double-blind, placebo-controlled crossover trial of extended-release dalfampridine (10 mg twice daily) (ClinicalTrials.gov NCT02391961). Participants were randomized to dalfampridine for 4 weeks followed by a 2-week washout and 4 weeks of placebo, or the reverse sequence. All investigators and participants were masked to treatment allocation.
The trial was conducted in accordance with CONSORT guidelines for randomized crossover trials.23,24 Eye-movement recordings were obtained at four visits spanning six recording conditions: Visit 1 baseline; Visit 2 pre-dose (trough) and approximately 3-h post-dose (peak) recordings after the first 4-week treatment phase; Visit 3 washout baseline after the 2-week washout; and Visit 4 pre-dose (trough) and approximately 3-h post-dose (peak) recordings after the alternate 4-week treatment phase (Figure 1).
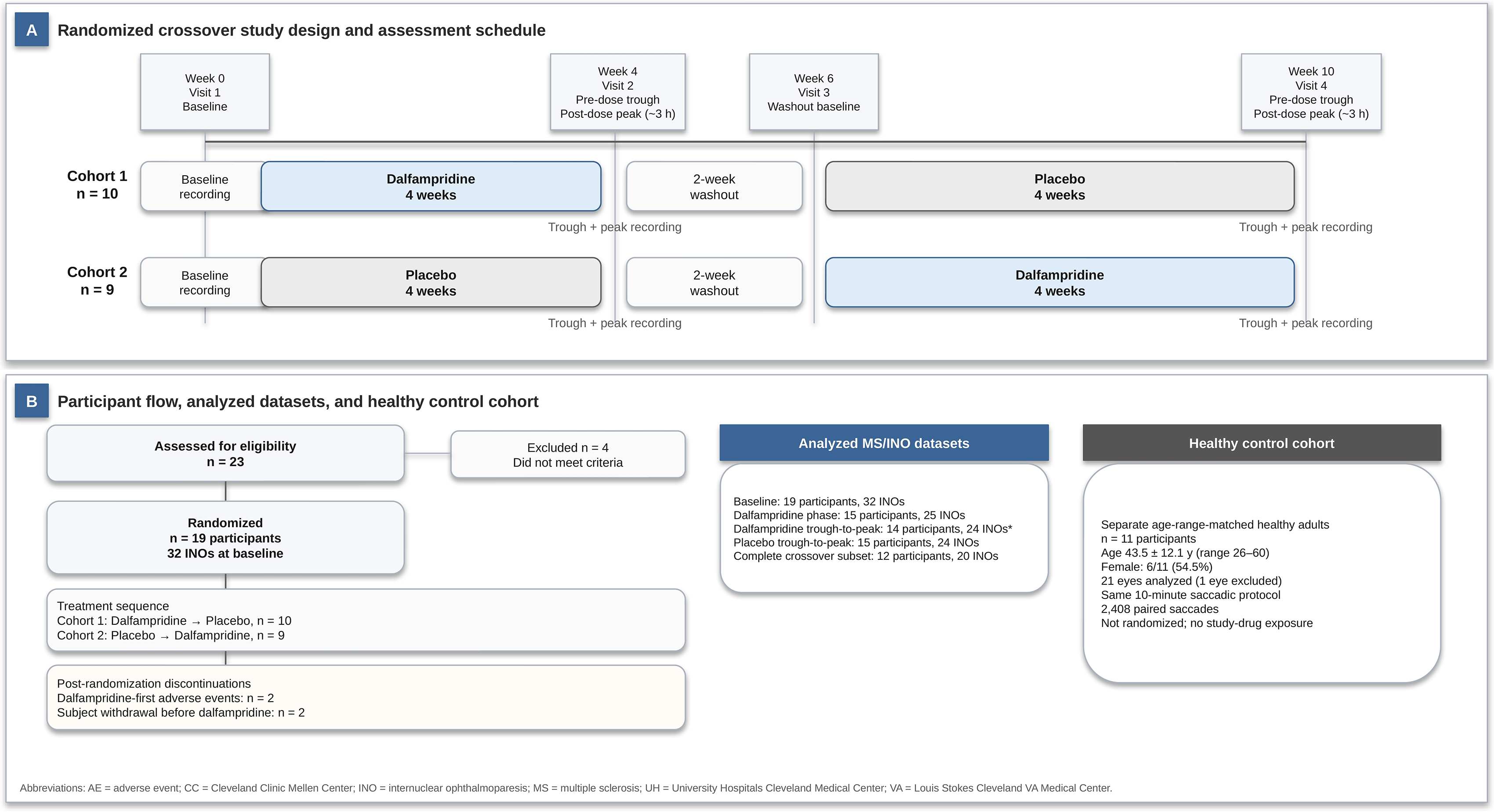
Study design, assessment schedule, participant flow, and control cohort. (A) Randomized, double-blind, placebo-controlled crossover design. Participants were assigned to dalfampridine for 4 weeks followed by a 2-week washout and 4 weeks of placebo, or to placebo followed by washout and dalfampridine. Eye-movement recordings were obtained at four visits spanning six recording conditions: Visit 1 baseline; Visit 2 pre-dose trough and post-dose peak after treatment phase 1; Visit 3 washout baseline; and Visit 4 pre-dose trough and post-dose peak after treatment phase 2. Peak recordings were obtained approximately 3 h after dosing. (B) Participant flow for the MS/INO trial cohort and separately recruited healthy control cohort. Fifteen participants contributed dalfampridine-phase data; *One INO lacked analyzable pre-dose dalfampridine data, resulting in 14 participants and 24 INOs for dalfampridine trough-to-peak analyses.
Participants
Participants were enrolled between April 2015 and January 2019 from three MS centers in Cleveland, Ohio: The Louis Stokes Cleveland VA Medical Center, University Hospitals Cleveland Medical Center, and the Cleveland Clinic Mellen Center for Multiple Sclerosis. Of 23 screened participants, 4 were identified from the Cleveland VA, 12 from University Hospitals, and 7 from Cleveland Clinic. Nineteen participants were randomized: 4 from the Cleveland VA, 11 from University Hospitals, and 4 from Cleveland Clinic. Eligible participants were adults aged 18–65 years with established MS meeting the 2010 McDonald criteria, 25 which were specified in the original IRB-approved and registered trial protocol at the time of study initiation. Potential participants were identified from MS/neuroimmunology and neuro-ophthalmology clinics, screened by chart review for MS diagnosis and dalfampridine safety criteria, and examined to confirm chronic mild-to-moderate INO. For this trial, mild-to-moderate INO was defined clinically as slowed adduction during horizontal saccades with preserved adduction range of motion and without exotropia in primary gaze. Unilateral or bilateral INO was permitted. Severe INO was defined operationally as INO with exotropia in primary gaze and/or marked limitation of adduction range of motion and was excluded. Severe INO was excluded because the study was designed to assess pharmacologic modulation of internuclear signal transmission in participants with slowed but preserved adduction. In severe INO, fixed ocular misalignment or marked adduction limitation may exaggerate PSR and PTD abnormalities and make these measures less specific for internuclear conduction alone. Such cases were therefore considered less likely to show measurable improvement with dalfampridine over the treatment interval.
Other exclusion criteria included history of seizures, moderate-to-severe renal impairment, and intolerance to dalfampridine. Prior dalfampridine use was permitted by protocol after a 2-week washout; however, no randomized participant was taking dalfampridine at enrollment or required washout for prior dalfampridine therapy.
Healthy control cohort
Healthy controls were recruited as a separate normative cohort from volunteers affiliated with the Louis Stokes Cleveland VA Medical Center and University Hospitals. Eligible controls were adults aged 18–65 years with normal visual and ocular-motor function on neurologic, neuro-ophthalmologic, and neurotologic examination by the PI. Controls were selected to approximate the age range of the MS/INO cohort, were not randomized, and underwent the same 10-min horizontal saccadic recording protocol without study-drug exposure.
Eye movement recording
Eye movements were recorded during a 10-min horizontal saccadic fatigue task (20° target jumps at 0.5 Hz) using the EyeLink II infrared eye tracker (SR Research, Ontario, Canada) sampled at 500 Hz. For best accuracy, each eye was calibrated monocularly. To avoid diplopia, recordings were performed with monocular viewing using the affected or more-affected eye in bilateral cases. Normative PSR and PTD values were derived from the healthy control cohort recorded under the same protocol. 12
Outcome measures
Primary ocular-motor outcomes
PSR (abducting-to-adducting eye peak-velocity ratio) and PTD (interocular latency difference between abducting and adducting saccade onset) were calculated for individual saccades throughout each recording. Acute pharmacodynamic response was assessed using trough-to-peak comparisons, with trough defined as the pre-dose recording and peak defined as the post-dose recording obtained approximately 3 h after dosing.
Ocular-motor fatigue
Ocular-motor fatigue was defined a priori as an increase in PSR and/or PTD during the final 100 s compared with the first 100 s of the 10-min recording.
Exploratory analyses examined dynamic changes and variability of PSR and PTD across sequential saccades throughout the recording.
Secondary outcomes
Secondary outcomes included the 25-Foot Walk Test (25FWT), MNREAD reading parameters (reading acuity, maximum reading speed, critical print size), fatigue measures including the Fatigue Severity Scale (FSS) and Modified Fatigue Impact Scale (MFIS), the National Eye Institute Visual Function Questionnaire-25 (VFQ-25), and the Neuro-Ophthalmic Supplement (NOS-10). MNREAD and 25FWT measures were assessed at pre-dose/trough and post-dose/peak time points during treatment visits. FSS, MFIS, VFQ-25, and NOS-10 were administered once per visit.
Sample size determination
Sample size was determined a priori based on feasibility and prior INO studies,14,21 with a target enrollment of 12–15 participants (approximately 20–25 INOs).
Statistical analysis
Analyses were performed using GraphPad Prism 10 (GraphPad Software, San Diego, CA) and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided p values <.05 were considered significant. Primary analyses used within-INO paired comparisons in a crossover framework. For bilateral INO, eyes were analyzed individually and aggregated at the participant level for secondary analyses. PSR and PTD were calculated for each analyzable paired saccade and summarized as recording-level means for each INO eye and condition. Baseline INO severity was summarized using quantitative ocular-motor measures, including baseline PSR and PTD, rather than retrospective clinical severity categories. Treatment effects were assessed using trough-to-peak changes, with crossover contrasts comparing dalfampridine versus placebo. Primary treatment analyses used continuous within-INO changes in mean PSR and PTD.
For descriptive responder analyses, predefined operational thresholds for meaningful change were defined as a decrease in mean PSR ≥0.02 or a decrease in mean PTD ≥1 ms. These thresholds were selected based on expected measurement variability and the scale of physiologically meaningful change observed in prior INO and healthy-control recordings; they were not intended as validated minimal clinically important differences.
Control comparisons used per-eye mean PSR and PTD, with pooled paired saccades used only for single-saccade correlation analyses. Categorical outcomes were summarized using odds ratios with 95% confidence intervals, and correlations were assessed using Pearson or Spearman coefficients. For exploratory responder analyses, a 25FWT responder was defined as a participant with any decrease in 25FWT time from pre-dose/trough to post-dose/peak within a treatment period. Additional signal processing and mixed-effects modeling are described in the Supplementary Methods.
Standard protocol approvals, registration, and patient consents
The trial was performed in accordance with the Declaration of Helsinki and its subsequent amendments, Good Clinical Practice, and applicable regulatory requirements. The protocol was approved by the institutional review board, and all participants gave written informed consent.
Data availability
Data not provided in the article because of space limitations may be shared (anonymized) at the request of any qualified investigator for purposes of replicating procedures and results.
Results
Participants and dataset
Nineteen participants (32 INOs, 13 bilateral) were randomized. Of the four randomized participants who did not contribute dalfampridine-phase data, two withdrew during the dalfampridine-first treatment phase because of moderate adverse events, and two withdrew by subject decision after Visit 2 or Visit 3 before receiving dalfampridine. Fifteen participants contributed dalfampridine-phase data (25 INOs); one eye lacked analyzable pre-dalfampridine data, resulting in 14 participants (24 INOs) included in trough-to-peak comparisons. Fifteen participants (24 INOs) completed the placebo phase, and twelve participants (20 INOs) completed both treatment periods (Figure 1). A total of 23,904 paired INO saccades were analyzed, including 4229 at baseline.
Eleven healthy controls (mean age = 43.5 ± 12.1 years, range 26–60; 6/11 female [54.5%]) underwent the same recording protocol. One control eye was excluded because of recording-quality limitations, resulting in 21 control eyes and 2408 paired control saccades for analysis. Baseline demographic and clinical characteristics, including INO laterality and baseline quantitative ocular-motor severity measures, are summarized in Table 1.
Demographic, clinical, and ocular-motor characteristics of MS/INO participants and healthy controls.
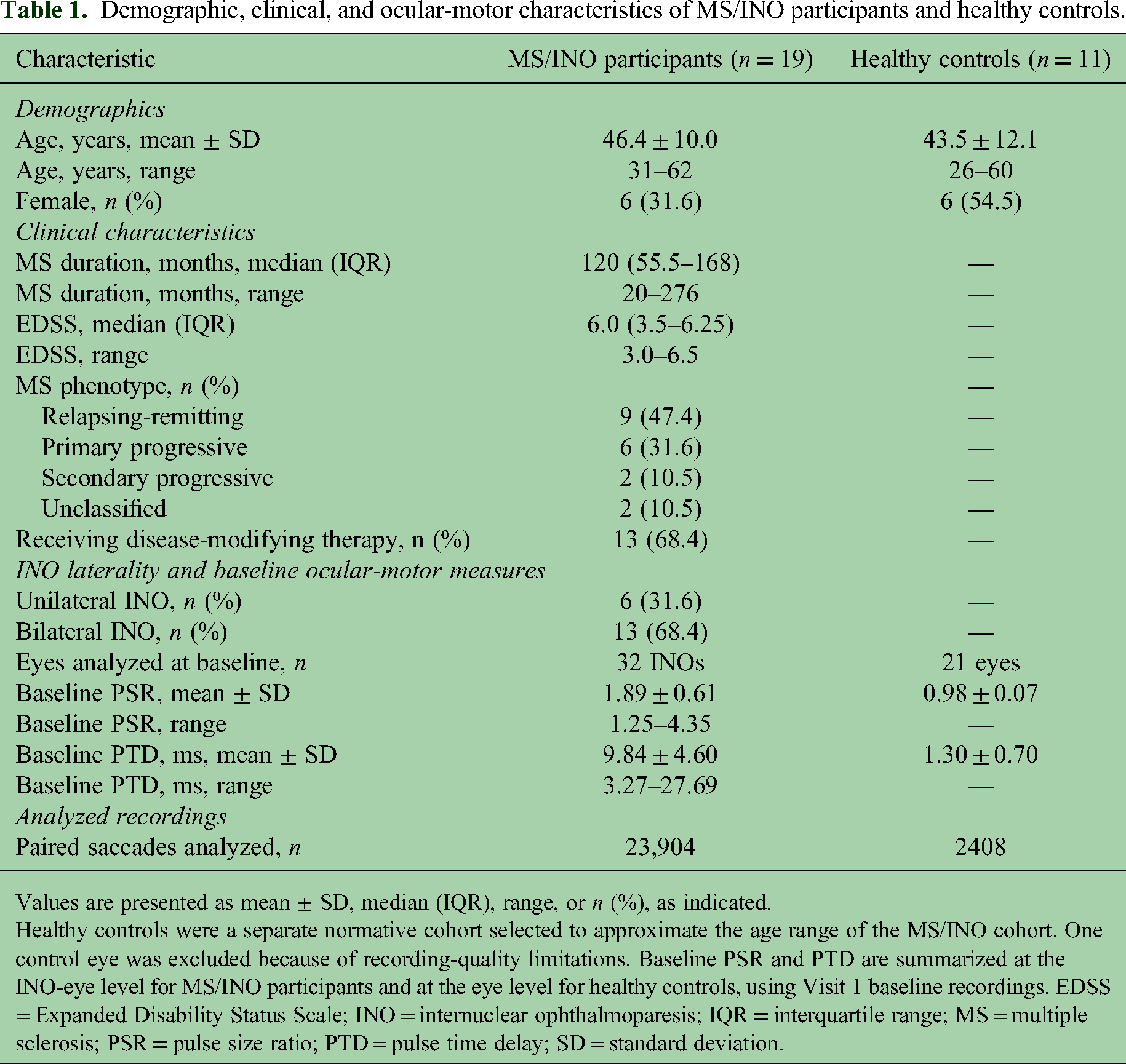
Values are presented as mean ± SD, median (IQR), range, or n (%), as indicated.
Healthy controls were a separate normative cohort selected to approximate the age range of the MS/INO cohort. One control eye was excluded because of recording-quality limitations. Baseline PSR and PTD are summarized at the INO-eye level for MS/INO participants and at the eye level for healthy controls, using Visit 1 baseline recordings. EDSS = Expanded Disability Status Scale; INO = internuclear ophthalmoparesis; IQR = interquartile range; MS = multiple sclerosis; PSR = pulse size ratio; PTD = pulse time delay; SD = standard deviation.
Baseline ocular-motor physiology and PSR–PTD relationship
Control recordings showed near-synchronous saccades (PTD 1.30 ± 0.70 ms; PSR 0.98 ± 0.07). In INO, PTD was prolonged (9.84 ± 4.60 ms) and PSR elevated (1.89 ± 0.61), consistent with impaired signal transmission across the demyelinated MLF (Figure 2).
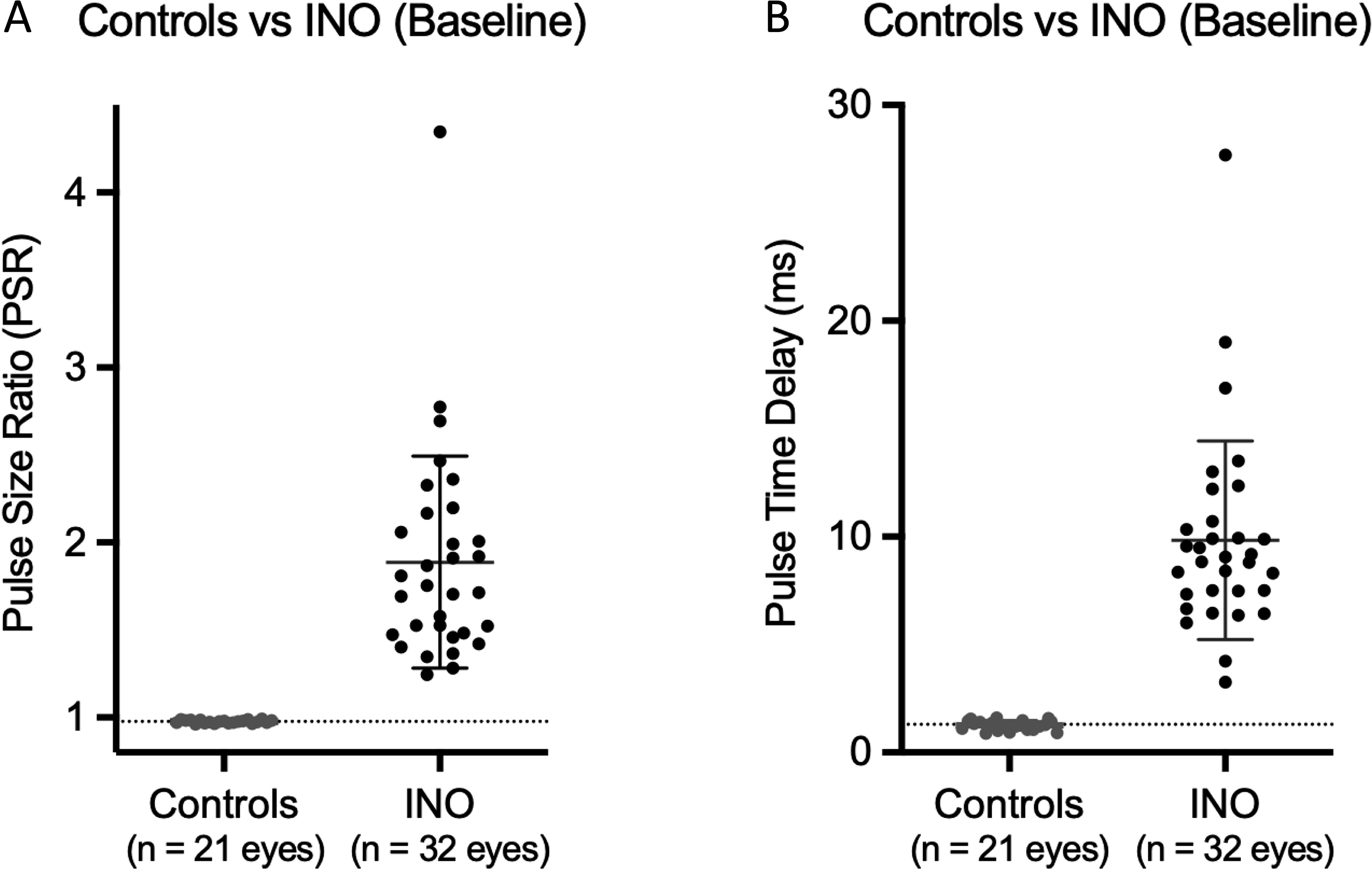
Distribution of pulse size ratio (PSR) and pulse time delay (PTD) in controls and INO at baseline: (A) Pulse size ratio (PSR) and (B) pulse time delay (PTD) in controls and in INO at baseline (Visit 1). Each point represents one eye. Horizontal lines indicate mean ± SD. Controls (n = 11 participants, 21 eyes) demonstrated tightly clustered PSR and PTD values, whereas INO eyes (n = 32) showed increased PSR and prolonged PTD. Dashed horizontal lines indicate mean control values (PSR ≈ 0.98; PTD ≈ 1.3 ms). Statistical comparisons were performed using the Mann–Whitney test.
Across pooled saccades, PTD ranged from near zero to approximately 60 ms, with PSR spanning approximately 1.0 to >5.0. PTD and PSR were positively correlated in INO (r = 0.38, R2 = 0.14, p < .0001), such that increasing interocular delay was associated with greater saccadic disconjugacy. In contrast, control data showed a narrow distribution (PTD <5 ms; PSR ∼0.8–1.2) and a weak inverse association (r = −0.24, R2 = 0.058, p < .0001). Together, PTD and PSR defined a physiologic separation between normal conjugate saccades and INO (Figure 3).
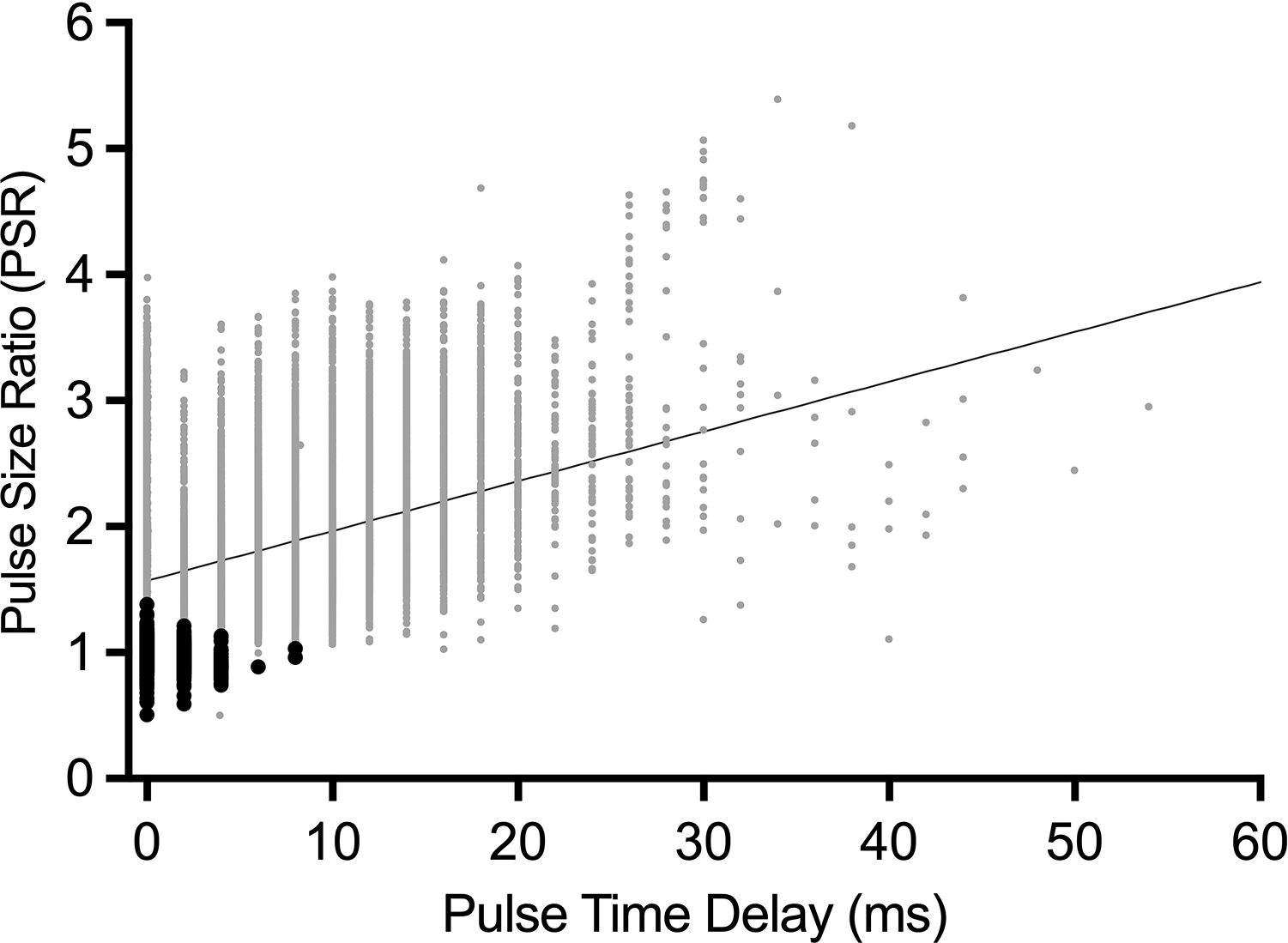
Relationship between pulse time delay (PTD) and pulse size ratio (PSR) across all saccades. Scatter plot of pooled paired saccades from INO (gray) and control (black) recordings. Each point represents a single saccade. In INO, PTD spans a wide range and was positively associated with increasing PSR (r = 0.38; solid line). Control saccades were tightly clustered at low PTD with PSR values near unity, showing a weak inverse association (r = −0.24). Together, PSR and PTD distinguish INO from normal conjugate saccades.
Effects of dalfampridine on prespecified ocular-motor outcomes
At the group level, dalfampridine did not significantly improve prespecified ocular-motor outcomes compared with placebo. Mean PSR and PTD did not show consistent treatment-related improvement, although eye-level responses were heterogeneous, with both improvement and worsening observed across INOs.
Using operational thresholds for descriptive responder analyses, defined as a decrease in recording-level mean PSR ≥0.02 or mean PTD ≥1 ms, PSR decreased in 14/24 INOs during both dalfampridine and placebo, while PTD shortened in 6/24 versus 4/24 INOs, respectively; proportions did not differ between treatment conditions.
In the crossover-complete subset (12 participants, 20 INOs), dalfampridine did not significantly improve trough-to-peak PSR or PTD compared with placebo: PSR changed by −0.028 ± 0.082 during dalfampridine versus −0.012 ± 0.074 during placebo (p = .28), and PTD changed by −0.92 ± 2.84 ms versus −0.41 ± 2.67 ms, respectively (p = .31). Effect sizes were small and imprecise, with point estimates directionally favoring dalfampridine: PSR d = −0.23 (95% CI: −0.68 to 0.22) and PTD d = −0.24 (95% CI: −0.69 to 0.21). Similar magnitudes were observed for baseline-to-peak comparisons (Supplementary Table 1). Individual INO responses are shown in Figure 4.
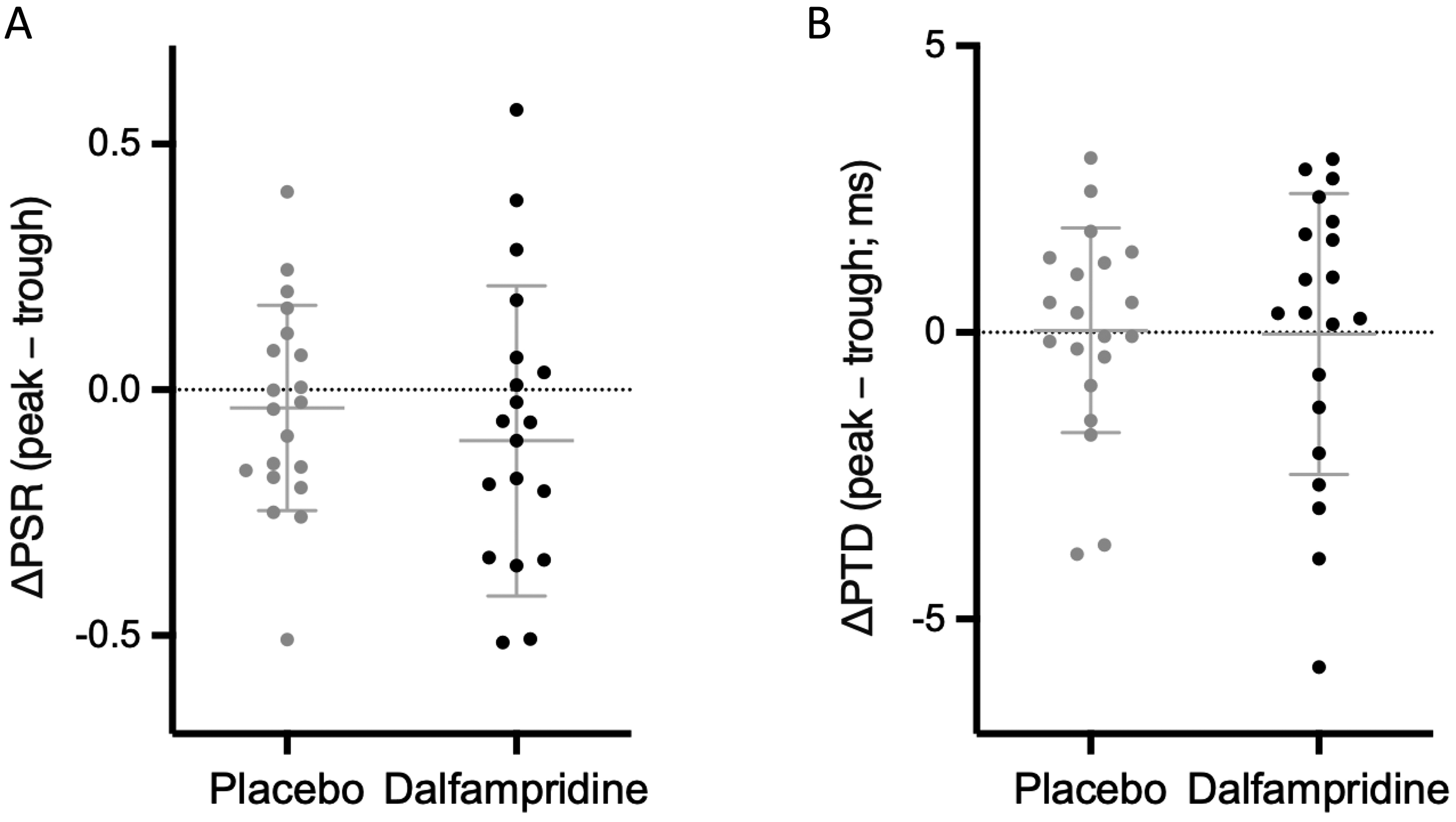
Individual INO responses to dalfampridine and placebo. (A–B) Changes in ocular-motor outcomes for individual internuclear ophthalmoparesis (INO) eyes are shown under placebo and dalfampridine conditions. (A) Pulse size ratio (ΔPSR) and (B) pulse time delay (ΔPTD) demonstrate heterogeneous responses across INOs, with both improvement and worsening observed in each condition. Distributions overlap substantially between placebo and dalfampridine, with mean changes near zero.
Prespecified ocular-motor fatigue analysis
Ocular-motor fatigue was defined a priori as an increase in PSR and/or PTD during the final 100 s compared with the initial 100 s of the 10-min recording. Mean PSR and PTD did not differ significantly between early and late epochs. Using this prespecified early–late fatigue definition, dalfampridine did not significantly improve ocular-motor fatigue measures compared with placebo.
Exploratory sequential and variability analyses
Exploratory analyses of sequential saccades across the full 10-min recording demonstrated dynamic fluctuations of PSR and PTD in INO (Figure 5(a) and (b)), whereas control recordings remained tightly clustered near normal values in PSR–PTD space (Figure 5(c)). PTD variability, defined as the within-recording standard deviation, averaged 2.46 ms in INO versus 1.29 ms in controls, and PSR variability averaged 0.200 versus 0.048. In baseline recordings, increased PSR and PTD variability in INO was evident throughout the recording rather than emerging only during the final epoch. Variability did not show a consistent early-to-late increase across the 10-min task, indicating that the prespecified early–late fatigue comparison did not fully capture the dynamic behavior of PSR and PTD. In PSR–PTD space, INO recordings showed dispersed distributions reflecting dynamic variation in interocular signal transmission timing and saccadic disconjugacy, whereas controls remained tightly clustered near normal values (Figure 5(c) and (d)).
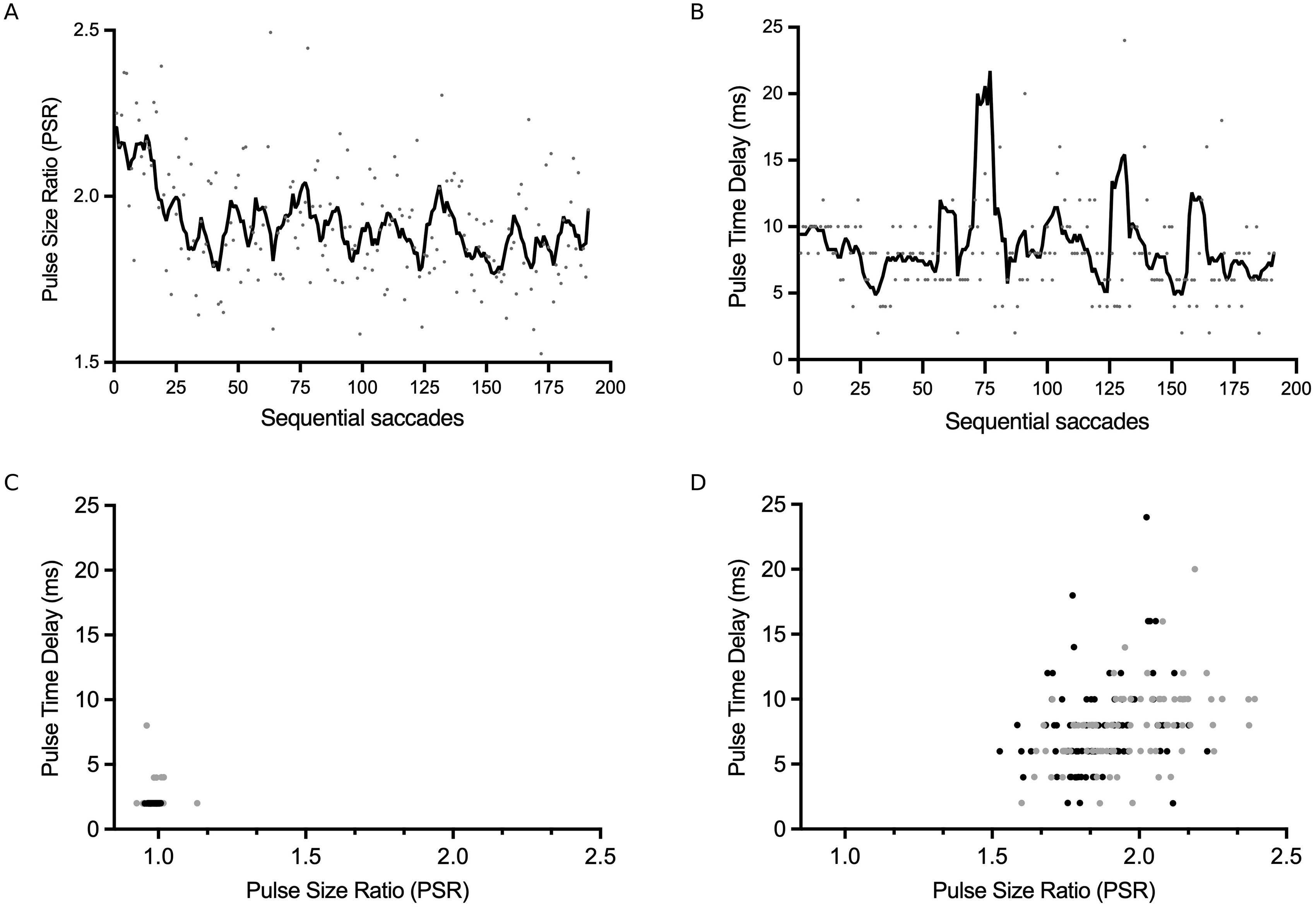
Dynamic fluctuations in pulse size ratio (PSR) and pulse time delay (PTD) during the 10 min saccadic fatigue task in internuclear ophthalmoparesis (INO). (A–B) Sequential PSR and PTD values from a representative INO eye show fluctuations across paired saccades during the 10 min saccadic fatigue task.
PSR variability, which was elevated in INO relative to controls, showed a trend toward reduction during dalfampridine (0.225 to 0.184, p = .061), with no change during placebo. PTD variability did not differ significantly in either treatment condition (Supplementary Table 2).
Mean PSR and PTD values were not associated with trough-to-peak changes during either dalfampridine or placebo. In exploratory analyses, greater trough PTD variability was moderately associated with larger trough-to-peak PTD shortening during dalfampridine (r = −0.4567, p = .043), whereas no association was observed during placebo (r = 0.06, p = .815) (Figure 6). Peak PTD variability was also associated with trough-to-peak PTD change during dalfampridine (r = 0.4574, p = .0426), while the corresponding placebo association was weaker and not statistically significant (r = 0.38, p = .095). Because PTD change was calculated as peak minus trough, higher change values indicate less PTD shortening or PTD lengthening; accordingly, the peak-variability association was interpreted descriptively as residual post-dose instability rather than as a baseline predictor of response.
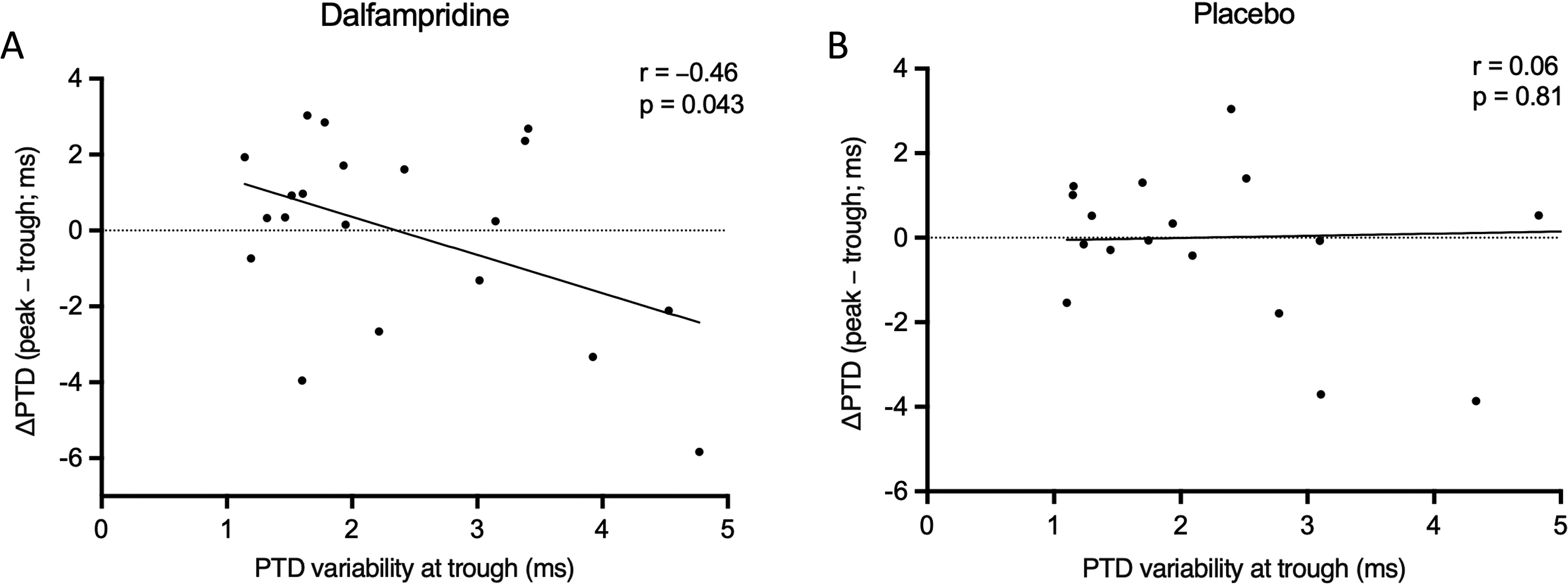
Baseline PTD variability and acute physiologic response to dalfampridine. (A) Relationship between PTD variability at trough and change in PTD (peak − trough) during dalfampridine. Greater baseline variability is associated with larger PTD shortening (r = −0.46, p = .043). (B) Corresponding analysis during placebo, showing no association (r = 0.06, p = .81).
Secondary clinical outcomes and adverse events
Among 12 participants completing both treatment periods, 25FWT time showed a numerical decrease during dalfampridine from 8.99 to 8.57 s compared with 9.11 to 9.18 s during placebo; the between-treatment comparison of change was not statistically significant. Improvement, defined as any decrease in 25FWT time from trough to peak, occurred in 10/12 participants (83%) during dalfampridine versus 7/12 participants (58%) during placebo, but this difference was also not statistically significant (OR: 3.57, 95% CI: 0.55–23.1; p = .37).
Among participants with a 25FWT response, defined as any decrease in 25FWT time from trough to peak, PSR improvement in at least one eye was observed in 10/10 responders (100%) during dalfampridine versus 4/7 responders (57%) during placebo (OR: 15.0, 95% CI: 0.64–351; p = .052). Detailed secondary clinical outcomes are reported in Supplementary Table 3. FSS scores decreased more during dalfampridine than placebo (ΔFSS −0.61 ± 0.99 vs. +0.18 ± 0.61; p = .026), whereas MFIS changes did not differ between conditions. Reading measures showed numerical changes but no significant between-treatment differences, including critical print size, reading acuity, and maximum reading speed. Patient-reported visual outcomes did not differ between conditions, including VFQ-25 and NOS-10.
Two participants in the dalfampridine-first group withdrew because of moderate adverse events: gastrointestinal upset and insomnia, respectively. Both events were non-serious and previously reported with dalfampridine. No serious adverse events occurred.
Discussion
In this randomized, double-blind, placebo-controlled crossover study of MS-related INO, dalfampridine did not significantly improve the prespecified primary ocular-motor outcomes, including mean PSR and PTD, or the prespecified early–late ocular-motor fatigue measures. Secondary clinical and visual outcomes were mixed: FSS decreased more during dalfampridine than placebo, whereas MFIS, 25FWT, reading measures, and patient-reported visual outcomes did not show significant between-treatment effects. These findings should be interpreted cautiously given the modest sample size, multiple secondary comparisons, and heterogeneous eye-level responses. Within this context, high-resolution ocular-motor recordings provided several physiologic observations. First, PSR and PTD behaved as complementary measures of pulse size asymmetry and interocular signal transmission timing, defining a continuum of internuclear dysfunction separating INO from normal conjugate saccades. Second, ocular-motor fatigue was not captured by simple early–late recording comparisons but was better reflected by dynamic fluctuations in PSR and PTD during sustained saccadic activity. Third, PSR variability during sustained activity showed a trend toward reduction with dalfampridine, consistent with possible partial stabilization, and greater trough PTD variability was associated with larger PTD shortening during dalfampridine but not placebo, suggesting that temporal fluctuations in interocular signal transmission may help identify pathways more likely to respond to pharmacologic modulation.
Across nearly 24,000 analyzable saccades pooled across recordings, PTD and PSR were positively correlated in INO, such that increasing interocular delay was associated with greater horizontal saccadic disconjugacy. In contrast, control recordings remained tightly clustered, with minimal variability and no meaningful relationship between these measures. These findings indicate that interocular delay and pulse size asymmetry co-vary across a continuum of internuclear dysfunction. In this framework, demyelination likely produces both slowing of conduction and temporal dispersion of the neural saccadic burst (“pulse”), degrading both the timing and effective magnitude of the signal delivered to the adducting eye.
The present data refine the concept of ocular-motor fatigue. Mean PSR and PTD did not differ between early and late epochs of the recording, but sequential analyses revealed fluctuations in both measures in INO, whereas controls remained stable. When examined jointly in PSR–PTD space, these fluctuations formed dispersed trajectories reflecting dynamic variation in interocular timing and saccadic disconjugacy. Rather than showing uniform progressive worsening from the beginning to the end of the task, INOs demonstrated persistently increased PSR and PTD variability during sustained saccadic activity, with heterogeneous temporal patterns across eyes. Thus, ocular-motor fatigue in demyelinated internuclear pathways may reflect dynamic instability and reduced conduction reliability, rather than a simple linear accumulation of impairment over time. Some fluctuations may also reflect intrinsic conduction instability rather than task-related fatigue alone. This behavior is consistent with impaired conduction in demyelinated axons, where reduced safety factor and temporal dispersion may lead to intermittent transmission failure during repetitive firing.26,27 Sustained saccadic activity may therefore function as a tract-specific physiologic stress test, revealing moment-to-moment instability that could contribute to transient visual disturbance rather than symptoms emerging only after prolonged visual effort.
At the group level, dalfampridine did not produce a consistent shift in mean PSR or PTD compared with placebo. Responses were heterogeneous, with both improvement and worsening across INOs, and small effect sizes that directionally favored dalfampridine. PSR variability, which was increased in INO compared with controls during sustained activity, showed a trend toward reduction during dalfampridine exposure, consistent with possible partial stabilization rather than normalization. These findings are consistent with pharmacologic modulation of a system in which pulse size and timing are tightly coupled, rather than with uniform normalization of mean PSR or PTD. In chronically demyelinated MLF pathways, interocular timing and pulse-size relationships may be partially adapted, such that enhancing conduction could alter this balance differently across INOs.
The present findings should be interpreted in relation to prior studies reporting improved binocular conjugacy after dalfampridine or fampridine in MS-related INO.21,22 Those studies primarily assessed saccadic disconjugacy using VDI/PSR or related velocity- or position-based measures, whereas PTD was not measured. Direct comparison is also limited by differences in operational INO severity definitions. Because PTD specifically quantifies interocular onset timing, it provides information complementary to measures of velocity asymmetry or positional disconjugacy. Thus, improved binocular conjugacy in prior studies may have reflected reduced abducting-to-adducting velocity asymmetry, increased adducting-eye pulse magnitude, reduced abducting-eye nystagmus, or reduced trial-to-trial dispersion without requiring uniform shortening of mean PTD. In the present study, mean PTD did not significantly decrease at the group level, and PSR and PTD responses were heterogeneous across INOs, sometimes changing in different directions. This suggests that pulse size and timing may change differently across INOs rather than improving uniformly. Future studies should directly compare INO responders and nonresponders using simultaneous measures of binocular conjugacy, PSR, PTD, and within-recording variability.
Within INO, changes in PSR and PTD were frequently coordinated, supporting a dynamic interaction between pulse size asymmetry and interocular timing. This behavior aligns with control-system models of saccadic generation in which amplitude and timing are jointly regulated to maintain binocular conjugacy.12,13 Dalfampridine, by blocking voltage-gated potassium channels, improves conduction in demyelinated axons,19,20,28 and may increase the reliability of the neural pulse to the adducting eye. In this context, downstream premotor and cerebellar circuits may adjust timing to preserve binocular coordination, resulting in rebalancing of coupled size–timing behavior. Heterogeneity in response likely reflects differences in structural injury of the MLF, intrinsic conduction instability, and adaptive capacity across individuals.
A key exploratory finding was the association between trough PTD variability and treatment response. Greater variability at trough was associated with larger PTD shortening during dalfampridine, with no relationship observed during placebo. The complementary peak-variability analysis supported this interpretation descriptively: greater residual PTD variability after dalfampridine was associated with less PTD shortening or with PTD lengthening, whereas the placebo association was weaker and not significant. Together, these findings suggest that fluctuations in interocular transmission timing, as measured by PTD, reflect a dynamic property of conduction rather than measurement noise. Notably, baseline severity measures such as mean PSR or PTD did not predict response, whereas variability did, supporting its potential as a more sensitive index of demyelinated axonal function. PTD variability may help identify patients more likely to respond to conduction-enhancing or remyelinating therapies. The incorporation of ocular-motor measures in ongoing remyelination trials (e.g., RESTORE; NCT05338450) 29 further supports their role as tract-specific biomarkers.
Secondary clinical outcomes were mixed and should be interpreted cautiously. FSS decreased more during dalfampridine than placebo, whereas MFIS, 25FWT, reading measures, VFQ-25, and NOS-10 did not show significant between-treatment effects.19,20,30,31 The numerical decrease in 25FWT time and the exploratory concordance between 25FWT response and PSR improvement suggest a possible link between ocular-motor physiology and broader motor performance, but these analyses were underpowered and hypothesis-generating. Similarly, reading measures showed numerical changes, including critical print size, but did not demonstrate significant between-treatment differences. These findings are consistent with broader principles of motor fatigue in MS, in which impaired signal transmission and reduced conduction reliability contribute to task-dependent performance fluctuations. However, larger studies are needed to link tract-specific ocular-motor metrics to clinical outcomes.
Practice-related and nonspecific effects may have contributed to changes observed during placebo, particularly in repeated ocular-motor and performance measures. However, treatment-specific patterns, including the relationship between trough PTD variability and PTD shortening during dalfampridine but not placebo, suggest that pharmacologic modulation may influence aspects of internuclear conduction dynamics beyond nonspecific task effects.
This study has several limitations. The sample size was modest, and exclusion of severe INO with primary-gaze exotropia or marked adduction limitation limits generalizability to patients with more advanced ocular-motor involvement. The study was designed to evaluate conduction modulation in mild-to-moderate INO with preserved adduction range; whether severe INO responds to dalfampridine requires separate study. Although a crossover design was used, carryover and practice effects cannot be fully excluded. Eye movements were recorded binocularly under monocular viewing conditions, which may underestimate abnormalities present during natural binocular viewing. The study was not powered to detect small treatment effects or to definitively link physiologic changes with clinical outcomes; findings should be interpreted as hypothesis-generating.
In summary, PSR and PTD behave as coupled physiologic variables that reflect dysfunction of internuclear signal transmission in MS-related INO. Dalfampridine did not significantly improve mean PSR or PTD at the group level, but responses were heterogeneous across INOs, consistent with modulation of these dynamics rather than uniform normalization; changes during placebo were less consistent and may reflect practice-related or nonspecific effects.
Sustained saccadic activity reveals dynamic fluctuations in this system, with interocular timing variability (PTD) emerging as a key feature of internuclear physiology and a candidate marker of ocular-motor fatigue. Baseline PTD variability was associated with variation in treatment response across INOs, suggesting that such variability may help identify pathways more likely to respond to pharmacologic modulation. These findings support the potential of quantitative ocular-motor measures as tract-specific biomarkers and provide a physiologic framework for evaluating therapies targeting conduction and remyelination in multiple sclerosis.
Supplemental Material
sj-pdf-1-mso-10.1177_20552173261464348 - Supplemental material for Ocular-motor conduction dynamics and variability in multiple sclerosis–related internuclear ophthalmoparesis: A randomized dalfampridine trial
Supplemental material, sj-pdf-1-mso-10.1177_20552173261464348 for Ocular-motor conduction dynamics and variability in multiple sclerosis–related internuclear ophthalmoparesis: A randomized dalfampridine trial by Alessandro Serra, Clara Chisari, Jonathan B Jacobs, Margaret M Skelly, Jessica McCabe, Hesham Abboud and Mark F Walker in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-2-mso-10.1177_20552173261464348 - Supplemental material for Ocular-motor conduction dynamics and variability in multiple sclerosis–related internuclear ophthalmoparesis: A randomized dalfampridine trial
Supplemental material, sj-docx-2-mso-10.1177_20552173261464348 for Ocular-motor conduction dynamics and variability in multiple sclerosis–related internuclear ophthalmoparesis: A randomized dalfampridine trial by Alessandro Serra, Clara Chisari, Jonathan B Jacobs, Margaret M Skelly, Jessica McCabe, Hesham Abboud and Mark F Walker in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
We are grateful to Drs. John Leigh, Jeffrey Cohen and Daniel Ontaneda for critical feedback, and for referring participants to our study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alessandro Serra: Biogen, Bristol Myers Squibb (speakers’ bureau). Clara Chisari: none. Jonatan Jacobs: none. Margaret M Skelly: none. Jessica McCabe: none. Hesham Abboud: Alexion Pharmaceuticals, Biogen, Horizon Therapeutics (consulting fee). Bristol Myers Squibb, Genentech (consulting fee, contracted research). Guthy-Jackson Foundation, Novartis, Sanofi Genzyme (contracted research). Mark Walker: none.
Disclaimer
The contents of this work do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Serra was funded for this work by Career Development Award #IK2RX001180 from the United States Department of Veterans Affairs, Rehabilitation Research & Development Service.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.