
Abstract
There is an urgent need to grow the behavioral health workforce so that Kindergarten (K)-12 students from all backgrounds can access affordable, interdisciplinary, and personalized treatments. This project addressed the state of Georgia’s behavioral health professional shortages in K-12 schools by offering integrated behavioral health training to students in a master’s-level school counseling program. The project provided didactic and experiential training over two semesters (30 weeks) to 62 school counseling students to prepare them to provide behavioral health services to K-12 students in rural and underserved areas of Georgia. Trainees completed online surveys pre- and post-training that assessed general counseling self-efficacy, behavioral health counseling self-efficacy, inter-professional collaboration competencies, and multicultural knowledge, awareness, and terminology. In completer-only analyses, as well as analyses involving multiple imputation methods to address missing data, trainees reported significant increases in general and behavioral health counseling self-efficacy, inter-professional collaboration competencies, and multicultural knowledge and terminology. Programs of this genus can increase the number of school counselors and other behavioral health providers prepared to work in educational settings across the globe.
Keywords
The state of Georgia is located in the southeastern region of the United States. Of the 50 U.S. states, Georgia is the 24th-largest by area and 8th most populous (NCHS Stats, 2025). In 2023, 39% of Georgia’s population was considered “rural.” Access to mental health services are significant challenges for many Georgians, particularly those in rural areas. There are 84 areas in Georgia classified as Mental Healthcare Professional Shortage Areas and 5.02 million persons live in these areas (Health Resources and Services Administration, 2025). The lack of mental health providers in the state is troubling. Based on the 2024 Annual Report of the United Health Foundation, Georgia ranks near the bottom nationally on several health metrics. Georgia ranked 47th worst in avoiding health care due to costs, 48th worst in low birthweight, 48th worst in being uninsured, 37th worst in childhood immunizations, 48th worst in access to mental health care, 46th worst in rates of chlamydia, and 44th worst in the nation in percent of residents who engage in high HIV-risk behaviors (America’s Health Rankings, 2025).
Many Kindergarten (K)-12 schools (students 5-17 years of age) in rural Georgia have only a small number of mental health practitioners available to support their students. In many schools, guidance counselors are responsible for providing both academic and mental health supports to students. Many K-12 schools lack adequate budgets to employ credentialed mental health professionals and student-to-guidance counselor ratios of 400:1 or more are common (American School Counselor Association, 2025), leaving many counselors struggling or unable to meet the mental health needs of their students.
For many reasons, it is important to train adequate numbers of mental health practitioners to meet the behavioral and mental health needs of students. First, large numbers of behavioral health professionals can ensure that behavioral and mental health workforces resemble the populations they serve in regards to gender, race/ethnicity, geography, sexual self-identity, and other characteristics. Second, highly stressful unanticipated events, such as the COVID-19 pandemic, may lead to elevated levels of burnout and attrition in mental and behavioral health practitioners. Finally, graduates of behavioral health programs may not pursue employment in rural and undeserved areas, instead, many will seek employment in large metropolitan centers (Health Workforce Technical Assistance Center, 2023).
This project addressed Georgia’s behavioral health professional shortage by offering integrated behavioral health fellowships and training to students in a university-based master’s-level school counseling program. The project’s goals were to: (i) train and place school counseling students in K-12 schools in 13 federally underserved areas of Georgia; (ii) provide contemporary curricula and experiential training opportunities that expand school counseling services to include mental health, behavioral, and substance use prevention and intervention; and (iii) strengthen the provision of integrated behavioral health services across community mental health centers, primary care clinics, and K-12 schools in federally designated underserved areas. The term “fellowship” refers to rigorous training that included existing coursework, one additional elective course, and additional professional development trainings conducted primarily in integrated healthcare settings.
The training program sought to increase student-trainees’ self-efficacy to provide behavioral health services and enhance their abilities to function as part of interdisciplinary healthcare teams across diverse school and healthcare settings. The project also enhanced trainees’ multicultural competency, defined as the ability to work effectively and ethically with persons from diverse cultural, racial, ethnic, and social backgrounds. Three domains of multicultural competency were emphasized throughout the program, specifically, awareness of one’s own cultural values and biases; knowledge of clients’ cultural contexts and worldviews; and skills to deliver culturally-responsive interventions (Sue et al., 1982). Greater multicultural competency enables behavioral health practitioners to (i) provide comprehensive, integrated, and culturally-contextualized behavioral health assessments and treatments, and (ii) improve student achievement and engagement, create a stronger sense of belonging among students from diverse backgrounds, and enable trainees and practitioners to implement culturally-responsive practices that can, in turn, improve student outcomes (Evans et al., 2011; Green & Keys, 2001; Owens et al., 2010).
Method
Student-Trainees
The study used a quasi-experimental, one-group, pre-test/post-test design. The 62 student-trainees in this project who completed pre-training measures consisted of 55 females and 7 males. Most self-identified as White (n = 37; 61%), with the remainder self-identifying as African American (n = 16; 26%), Asian American (n = 4; 7%), Latinx (n = 3; 5%), and biracial (n = 1; 1%). The average trainee was 27.5 years old (SD = 2.6, range = 24-36 years).
Assessment Instrument
Two assessments measured the program’s effectiveness. After being accepted into the fellowship program early in the student’s first year of the master’s program, student-trainees completed pre-training assessments. Post-assessments were completed at the end of Year 2, after trainees had completed their student internships. Both assessments were completed using the Qualtrics platform and no monetary compensation was provided. Trainees completed both assessments as part of their stipend-supported fellowship.
The assessment instrument included the following measures:
The Student Counselor Self-Efficacy (SCSE) Scale (Bodenhorn & Skaggs, 2005) was developed specifically for school counselors to assess their self-efficacy for counseling in school settings. The 43 SCSE items used a 5-point response scale (1 = “Not confident to 5 = “Highly confident”). Sample items included: “I can establish rapport with a student for individual counseling” and “I can model and teach conflict resolution skills. Coefficient alpha for the measure was α = .94 (present study).
The Adapted Self-Efficacy Scale (ASES; Schwarzer & Jerusalem, 1995) is a 10-item scale that assessed trainees’ confidence in their abilities to perform counseling-related tasks in behavioral-health settings and situations. Sample items included “When I am confronted with a complicated behavioral or mental health problem, I can usually find several solutions” and “If I encounter a client who is referred to me for behavioral health issues, I know I can work with them to solve the problem.” All items used a 4-point scale to indicate level of agreement (1 = “Not at all true” to 4 = “Exactly true”). Higher mean scores indicated greater behavioral health counseling self-efficacy. The scale’s internal consistency was α = .97 (current study).
The Interprofessional Education Collaborative (IPEC) Competency Survey is a 42-item self-administered survey developed specifically for this project that assessed confidence in one’s ability to work as part of an interdisciplinary team and deliver integrated behavioral health-primary care services (sample item: “I am able to engage diverse healthcare professionals with complementary professional expertise to develop strategies to meet specific patient care needs”). Each item used a five-point scale to indicate level of agreement (1 = “Strongly disagree” to 5 = “Strongly agree”). Higher scores indicated greater confidence to function as part of an interdisciplinary healthcare team. The scale’s internal consistency was α = .93 (current study).
The Multicultural Counseling Competence and Training Survey – Revised (MCCTS-R; Holcomb-McCoy & Day-Vines, 2004) is a 32-item, three-factor scale that evaluated trainees’ multicultural awareness (9 items, sample item: “I am able to discuss how my culture has influenced the way I think”), multicultural knowledge (19 items, sample item: “I can discuss family counseling from a multicultural perspective”), and multicultural terminology (4 items, sample item: “I can define racism”). Each item used a 4-point Likert scale to assess level of agreement (1 = “Not competent” to 4 = “Extremely competent”). Higher scores indicated greater amounts of each competency. Coefficient alpha for the total scale was α = .96 (current study).
Procedures
Trainees were enrolled in a two-year school counseling master’s program accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP). Students received information about the fellowship program during the department’s orientation and admissions events and in the Fall Semester of the student’s first year in the graduate program. Students were selected for fellowships early in their first year of graduate study. Four annual cohorts were assembled, trained, and assessed over the course of the program. All trainees received a stipend while enrolled in the program. The university’s Institutional Review Board (IRB) approved the program and trainees provided written informed consent prior to participation.
This study utilized a prospective cohort design to evaluate students’ counseling self-efficacy, ability to work as part of an interdisciplinary team, and multicultural competencies while providing integrated behavioral health services and interventions in K-12 schools during their internship year. Cohort 1 (n = 21) completed post-training assessments in 2016, Cohort 2 (n = 18) in 2017, and Cohort 3 (n = 13) and Cohort 4 (n = 10) in 2018.
Through a variety of training formats, trainees learned how to provide services and interventions related to integrated mental and behavioral health in schools. The program’s curriculum consisted of 10 modules: (1) an overview of integrated care and school-based health centers; (2) multi-tiered systems of support (MTSS); (3) consultation and advocacy; (4) suicide crisis management; (5) substance abuse and motivational interviewing; (6) Cognitive Behavioral Therapy (CBT)-based models and interventions; (7) youth mental health; (8) family counseling and engagement; (9) resiliency and mindfulness strategies; and (10) referral processes and wrap-around plans. The 10 modules were contextualized for school settings.
As part of the fellowship, formal lectures enabled students to develop competencies in evidence-based interventions shown to be efficacious for youth in school settings. Trainees participated in courses that included content on integrated behavioral health interventions. In addition to formal coursework, student-trainees participated in the following activities:
Data Analysis
Paired t-tests assessed outcomes of the fellowship training program using pre-and post-training data. Two approaches were used in outcome analyses: (i) completer-only analyses, and (ii) a sensitivity analysis with multiple imputations for missing data (n = 77). Completer-only analyses analyzed data from trainees who completed pre- and post-training measures (N = 62, although ns vary across outcome measures because of missing data). Intent-to-treat analyses with multiple imputation methods for missing data were based on 77 trainees; 62 trainees who completed training and post-training measures combined with 15 trainees who completed training but did not complete pre-training measures. Bonferroni corrections were implemented to reduce Type I error across multiple comparisons. Academic records were reviewed to determine the number of students who (1) obtained employment in schools in underserved areas, and (2) successfully passed the Counselor Preparation Comprehensive Examination (CPCE).
Results
Data was re analyzed using the Statistical Package for the Social Sciences (SPSS) Version 26 (IBM Corp., 2017). Data screening analyses found no univariate or multivariate outliers or out-of-range values. All assumptions relevant to paired t-tests were satisfied.
Analyses Comparing Training Completers to Non-completers
Training completion rates differed across racial/ethnic groups, although estimates should be interpreted with caution given small subgroup sizes. Retention was highest among Biracial (100%; 1/1), Asian (75%; 3/4), and White participants (70%; 26/37), and lower among African American (44%; 7/16) and Latinx participants (0%; 0/3). The association between race/ethnicity and completion did not meet conventional thresholds for statistical significance, χ²(4) = 8.9, p = .06. Training completer vs. non-completer status was not associated with gender, X2(1) = 0.34, p = .56.
Completers-Only Outcome Analyses
A series of paired t-tests with Bonferroni adjustments was initially conducted using complete data provided by trainees at both pre- and post-training assessments (N = 62, ns vary due to missing data). As shown in Table 1, students reported significant increases in general and behavioral health counseling self-efficacy, inter-professionalism competency, and multicultural counseling competency, awareness, knowledge, and terminology (all ps < .01).
Changes From Pre- Through Post-Training Using Completers and Multiple Imputation Approaches.
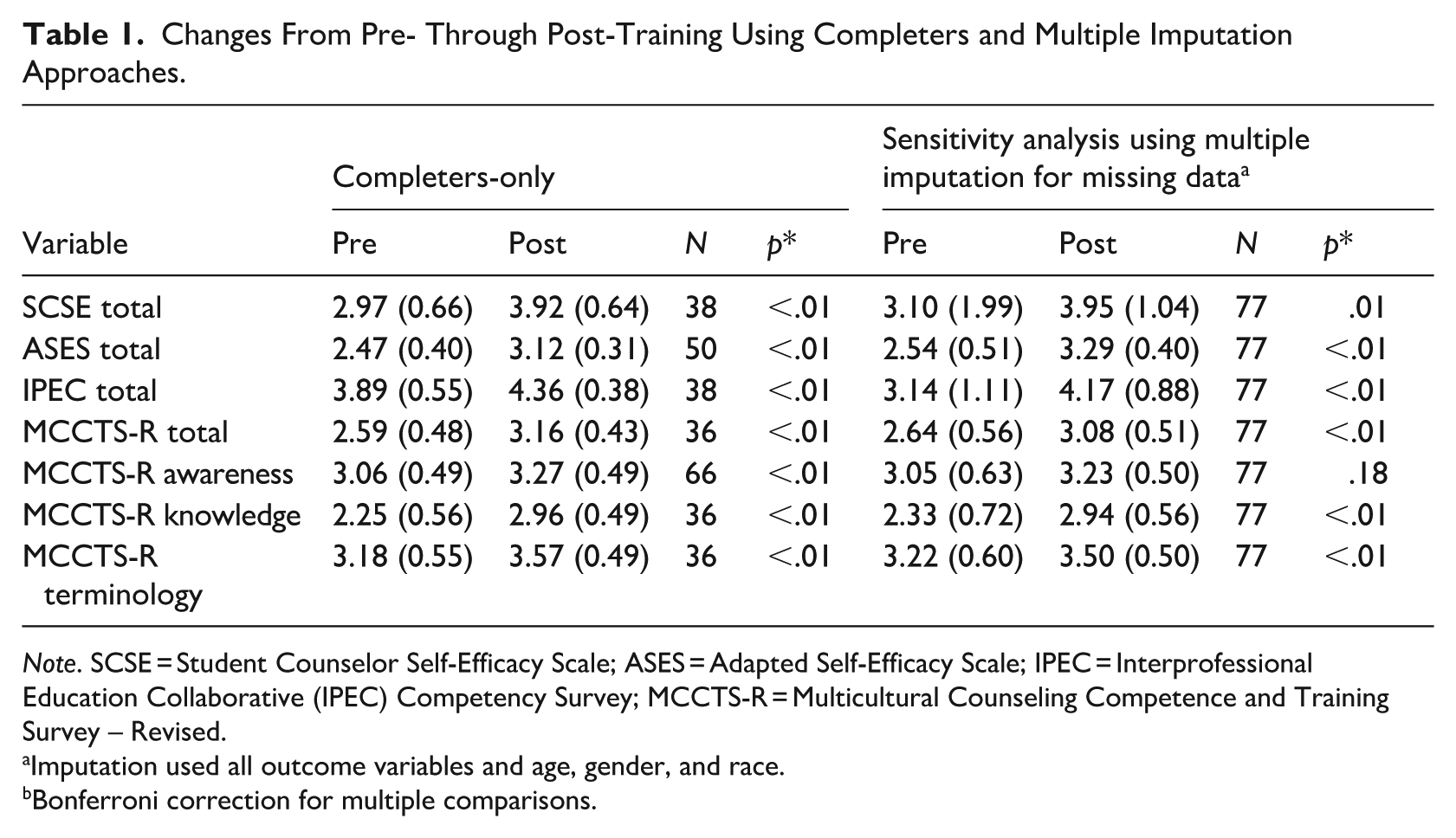
Note. SCSE = Student Counselor Self-Efficacy Scale; ASES = Adapted Self-Efficacy Scale; IPEC = Interprofessional Education Collaborative (IPEC) Competency Survey; MCCTS-R = Multicultural Counseling Competence and Training Survey – Revised.
Imputation used all outcome variables and age, gender, and race.
Bonferroni correction for multiple comparisons.
Multiple Imputation Analyses
Multiple imputation analyses used data from 77 trainees. Largely consistent with outcome findings that used a completer-only approach, trainees reported significant increases in general and behavioral health counseling self-efficacy, interprofessional collaborative competencies, and multicultural knowledge and terminology (all ps < .01; see Table 1). The difference in multicultural counseling awareness from pre- to post-training was not statistically significant, due primarily to the conservative nature of the Bonferroni adjustment in the multiple imputation analysis.
Finally, based on trainees. academic records and alumni tracking data, 100% of trainees who completed the fellowship passed the program’s exit examination (i.e., CPCE) required for graduation and 80% obtained employment in schools in rural and high needs areas of Georgia following graduation.
Discussion
This project found that a training program consisting of formal interdisciplinary didactic and experiential training provided school counseling trainees with greater levels of general and behavioral health counseling self-efficacy, interprofessional collaborative competencies, and multicultural competencies, attributes that will prepare them to work with diverse students. School settings are ideal venues in which to identify and treat youth at elevated risk for behavioral health disorders (Carlson et al., 1995). Unfortunately, many schools—particularly those in rural and high-need areas—employ very few formally trained behavioral health practitioners to deliver and/or coordinate preventative and contextualized counseling services to youth in need of these services (Ziomek-Daigle et al., 2016). The training program evaluated in this project has the potential to grow the behavioral health workforce and reduce the shortage of mental and behavioral health providers in schools (Health Workforce Technical Assistance Center, 2023).
In completer-only and intent-to-treat outcome analyses with multiple imputation methods, trainees reported significant increases in counseling self-efficacy on two different self-efficacy measures (general counseling and behavioral health counseling). This finding is important, as school counselors who report greater counseling self-efficacy can develop better relationships with students, engage in more self-reflection (resulting in more effective counseling practices), and enjoy a greater sense of professional identity, attributes that can lead to greater job satisfaction and better outcomes for counselors and students (Camp et al. 2019).
Trainees also reported a significant increase in interprofessional collaborative skills. Interprofessional competency is an important skill for school counseling trainees to learn in educational settings and practice in real-world venues (Schmidt, 2024). Greater interprofessional competency can increase school counselor effectiveness by providing them with the ability to collaborate with other professionals and stakeholders in school systems and communities (Burgess et al., 2023). This competency also enables school counselors to better address the unique needs of students, families, and school systems. Finally, enhanced inter-professional collaborative competency also facilitates the development of effective communication skills and sharing of knowledge and resources (McClain et al., 2024).
In completer-only analyses, trainees reported significant increases in multicultural awareness, knowledge, and terminology although, with the more conservative alpha level used in Bonferroni adjustments, the pre- to post-training increase in multicultural awareness was lost. School counselors play an integral role in helping students, particularly those from diverse backgrounds, realize their educational and personal goals (Mulhern, 2020). In today’s increasingly diverse society, school counselors should possess high levels of multicultural competence to more effectively support the needs of their students. This ability, however, depends largely on their multicultural competency. Trainees who enter the behavioral health workforce who are culturally competent can create more affirming environments for students of all backgrounds (Holcomb-McCoy, 2005). They can also better understand the histories and needs of individual students, enabling them to develop personalized solutions for the student and their family (Lefurgey et al., 2025). Importantly, greater multicultural competency also reduces the likelihood of bias, prejudice, and discrimination in the school environment (Holcomb-McCoy & Day-Vines, 2004).
When applying more conservative statistical tests using Bonferroni adjustments, study findings were similar to those of Holcomb-McCoy (2005), who found that completing a formal multicultural counseling course increased school counselors’ multicultural terminology but did not yield increases in multicultural awareness. As Owens et al. (2010) posit, perhaps certain areas of multicultural competence (e.g., terminology and knowledge) can be improved in educational settings but more complex forms of multicultural awareness must be developed over time in real-world settings that include diverse groups and opportunities to address challenges that members of diverse communities confront.
Limitations and Future Directions
This study had several limitations. All participating schools were located in a single state; the extent to which study findings generalize to schools in other states is unknown. The study’s design lacked a control group, leaving outcome findings susceptible to history effects, demand characteristics, and other threats to internal validity. While student-trainees provided data before and after the program, no objective data assessing the academic performance or behavioral conduct of K-12 students were collected. The study’s findings included only one follow-up assessment. Longer-term follow-ups would be informative to determine if the program’s beneficial effects were sustained over time. Finally, with the exception of job placement and examination performance data, all study data were self-report.
Conclusions
In spite of these limitations, this fellowship program is highly scalable. The additional didactic and experiential training opportunities included in this project can be easily integrated into existing school counseling programs’ curricula through seminars, case presentations and discussions, internships and externships, supervision activities, and elective courses that best meet the students’ needs. Institutions interested in offering this (or a related) fellowship program can leverage existing resources and faculty expertise, thereby avoiding costs associated with hiring new personnel. All didactic seminar materials (e.g., PowerPoint presentations), recorded webinars, training manuals, supervision manuals, and assessment instruments used in the current project are available upon request (
As the number of youth with behavioral health disorders continues to grow (Sappenfield et al., 2024) it will be increasingly important for counseling programs to produce greater numbers of school counselors who can be placed in under-served and rural educational settings. Fellowships of this genre offer avenues to place highly-qualified counselors in school settings where they can provide services and interventions to K-12 students and their families and collaborate with local agencies. Employing additional school counselors in high-need and underserved schools can improve the lives of students in numerous ways (Hurwitz & Howell, 2013). Specifically, with additional access to counseling and support services, many K-12 students will better understand their feelings and emotions and act on them adaptively and develop more positive coping skills when they are stressed or overwhelmed (Durlak et al., 2011). School counseling students trained in programs such as this one will possess the interdisciplinary skills sets needed to identify mental health issues early on and refer students to appropriate resources for timely assistance. Ultimately, increasing the number of school counselors in underserved schools has the potential to lead to positive psychological and behavioral changes in students and more general improvements in the overall well-being and success of school systems.
Footnotes
Ethical Considerations
This study was approved by the University of Georgia’s Institutional Review Board (IRB) in August 2020. All student-trainees provided written informed consent prior to participating in the training program. This research was conducted in a highly ethical manner and in accordance with the ethical guidelines of the American Psychological Association.
Consent to Participate
All student-trainees reviewed and signed a written informed consent form prior to training in which they provided the study team with permission to publish their de-identified data and review their academic records at the end of the training period.
Consent for Publication
Informed consent forms indicated that study data could be used for publication purposes but that all data would be groups and de-identified for any analyses and publications that result from the study.
Human Subjects
This study was approved by the University of Georgia’s Institutional Review Board (IRB).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration (HRSA), Grant Number G02HP27977.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study’s de-identified dataset is available upon request.