
Abstract
We report a case demonstrating the evolution of diffusion lacunae (DL) into thrombus, supported by serial MRI and MR–pathologic correlation. A 36-year-old woman with a pregnancy achieved via frozen–thawed embryo transfer presented with complete placenta previa and vaginal bleeding. MRI at 27 weeks of gestation revealed an irregular intraplacental hypointense area on diffusion-weighted imaging corresponding to DL. Follow-up MRI at 32 weeks showed that the DL had become less discernible and appeared hyperintense, similar to the surrounding placenta. On the following day, the patient developed hemorrhagic shock and underwent emergency cesarean delivery, without evidence of placental adherence and decidual deficiency, indicating that the DL represented a placental lake rather than placental lacunae. Histopathologic examination demonstrated a paucity of chorionic villi and thrombus formation with lines of Zahn in the DL area. These findings provide direct evidence that DL may undergo thrombus formation over time, reflecting dynamic changes related to blood flow stasis within the placenta.
Keywords
Introduction
Placenta accreta spectrum (PAS) is an abnormal placental attachment due to defective decidua basalis, with rising incidence linked to increasing cesarean deliveries. 1 Prenatal diagnosis is essential, with ultrasound as first-line and MRI providing complementary information. 2
Diffusion lacunae (DL) are a recently described diffusion-weighted imaging (DWI) finding in PAS, appearing as intraplacental hypointense areas on DWI with corresponding hyperintensity on ADC maps. 3 DL are presumed to correspond to placental lacunae showing low-echoic area on ultrasound, which is suggestive of PAS. 3 Our recent MR–pathologic correlation suggests that DL represent villous-devoid placental lacunae. 4 Meanwhile, placental lakes are commonly observed as sonolucent findings in normal placentas, which represent subchorionic avillous areas surrounded by normally villous tissue.5,6 Therefore, it may be difficult to distinguish them even using MRI. 3
Meanwhile, our recent MR–pathologic correlation also suggests that T2 dark bands correspond to thrombus formation with Lines of Zahn, indicating progressive thrombosis under blood stasis in the DL. 4 In the article, we proposed that DL and thrombus formation might reflect sequential stages of a shared pathological process in PAS. 4 Herein, we report a case in which temporal changes in DL were observed on serial MRI, supporting this pathological process.
Case history
A 36-year-old woman, gravida 3, para 0 (2 spontaneous abortions), conceived via frozen–thawed embryo transfer (FET) at a local clinic. Placenta previa was suspected at 26 weeks of gestation. At 27 weeks, she experienced massive vaginal bleeding and was referred to our institution for perinatal management. Ultrasound demonstrated adenomyosis in the posterior uterine wall. The placenta was attached to the posterior wall, and complete placenta previa was identified. MRI was performed on the second day of hospitalization. MRI included T2WI in three orthogonal planes; axial and sagittal balanced steady-state free precession sequence (SSFP); axial fat-saturated T1-weighted imaging; and sagittal DWI. On DWI (b = 800 s/mm2), an irregularly shaped hypointense area was identified at the maternal surface of the placenta, corresponding to DL (Figure 1(a)). Flow void within the DL and increased vascularity of the placental bed in the surrounding region were also observed on T2WI (Figure 1(b)). Additionally, a relatively hypointense lesion suggestive of adenomyosis was observed in the posterior uterine wall. (a, b) MRI obtained at 27 weeks of gestation (initial MRI), (c, d) MRI obtained at 32 weeks of gestation (follow-up MRI). (a) Reconstructed axial diffusion-weighted imaging (DWI); (b) T2-weighted imaging (T2WI); (c) axial DWI; (d) T2WI; (e), (f) hematoxylin and eosin (H & E) staining at low magnification. On DWI, an irregularly shaped hypointense area is identified at the maternal surface of the placenta, corresponding to diffusion lacunae (DL) (a, arrow). Flow void within the DL (b, arrow) and increased vascularity of the placental bed in the surrounding region (b, arrowheads) are also observed on T2WI. Additionally, a relatively hypointense lesion suggestive of adenomyosis is observed in the posterior uterine wall (b and d, curved arrows). At the follow-up MRI, the DL that was clearly identified on the previous MRI is no longer discernible and appears to have become hyperintense, similar to the surrounding placenta (c, arrow). The area shows iso-intensity on T1WI (not shown) and hyperintensity on T2WI (d, arrow) and SSFP (not shown), which are similar to the surrounding placenta. Histopathologic examination demonstrates that the area corresponding to the DL on the initial MRI is characterized by a paucity of chorionic villi (arrowheads, (e) and (f)), thrombi with lines of Zahn (arrows, (e) and (f)), and partial villous infarction (white arrowheads, f). The thrombus exhibits a cast-like configuration that closely matched the DL on initial DWI (a, e, and f).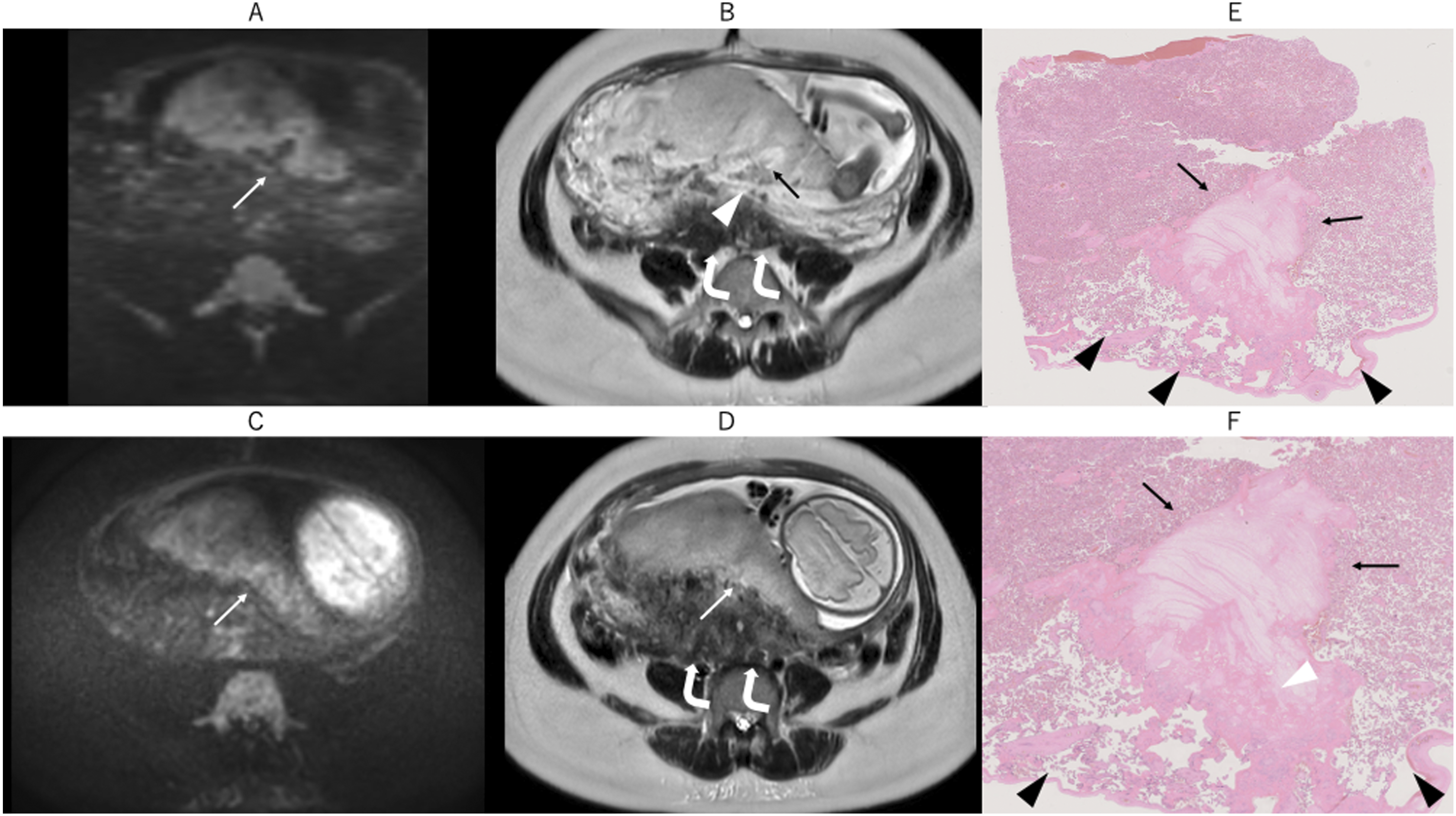
The patient was followed thereafter; however, evaluation of the relationship between the posterior myometrium and the placenta remained challenging due to adenomyosis. MRI was therefore repeated at 32 weeks of gestation; however, the DL that had been clearly identified on the previous MRI was no longer discernible and appeared to have become hyperintense, similar to the surrounding placenta (Fig. 1(c)). The area showed iso-intensity on T1WI (not shown) and hyperintensity on T2WI (Fig. 1(d)) and SSFP (not shown), which were all similar to the surrounding placenta.
The day after MRI, the patient developed vaginal bleeding due to complete placenta previa, which persisted and progressed to hemorrhagic shock, necessitating emergency cesarean delivery. The placenta was delivered without evidence of adherence. The entire placenta was formalin-fixed and sectioned through close collaboration between pathologists and radiologists to match the axial MRI slice plane.
MR–pathologic correlation was performed using representative axial MRI and corresponding histopathologic findings (Fig. 1). Histopathologic examination demonstrated that the area corresponding to the DL on the initial MRI was characterized by a paucity of chorionic villi and thrombi with lines of Zahn (Fig. 1(e), (f)). The thrombus exhibited a cast-like configuration that closely matched the DL (Fig. 1(e), (f)). Histopathologic examination of the delivered placenta around the DL showed no evidence of decidual deficiency. Consequently, the DL were considered to correspond to placental lakes. MR–pathologic correlation suggested that thrombus formation occurred within the placental lakes corresponding to DL over the course of gestation.
Discussion
Recently, we reported that pathological findings about DL and T2 dark bands by whole-uterus sectioning enabled precise MR–pathologic correlation. 4 In the article, T2 dark bands primarily represent thrombus formation with lines of Zahn, which commonly occur in thrombi formed in the presence of blood flow. Therefore, we speculated that such thrombi gradually develop under conditions of blood stasis with residual blood flow. Namely, these findings may suggest a possible pathological continuum between DL and T2 dark bands, reflecting sequential stages from villous destruction to thrombus formation. However, the underlying mechanism remained speculative, as cross-sectional imaging could not directly capture the temporal evolution of these findings.
In this present case, serial MRI demonstrated that the DL identified on the initial examination evolved into hyperintense areas resembling the surrounding placenta. Histopathologic evaluation revealed thrombus formation with lines of Zahn, supporting the pathophysiological interpretation proposed in our previous case report. The present case provides the first direct evidence of this sequential process through serial MRI. Although the definitions and diagnostic criteria for placental lakes vary among studies, 7 the DL in the present case were considered to represent placental lakes based on the clinical and histopathologic findings. Placental lakes are observed sonographic findings in normal pregnancy, 5 but their temporal evolution remains incompletely understood. A pathological textbook described that “intervillous thrombi and what may also actually correspond to clinically diagnosed placental lakes, in contrast, are either fresh red hemorrhage (‘clots’) and shiny, or they are laminated and light tan-gray and generally basal. They are not generally associated with villous infarction but appear to represent regions of sluggish flow or stasis in the perivillous space.” 8 Additionally, Jauniaux et al. also described cases in their review article in which placental lakes detected on ultrasound were identified as intervillous thrombi at delivery. 5 These findings support the concept that placental lakes are regions of sluggish flow or stasis, which may provide a plausible hemodynamic basis for thrombus formation in the present case. Taken together, these findings suggest that thrombus formation may not be a phenomenon specific to PAS, but rather a broader placental response to blood flow stasis, as previously implied in the pathological literature.
In this case, adenomyosis was present in the posterior uterine wall, which is known to be a potential risk factor for PAS. 9 However, histopathologic examination of the delivered placenta showed no evidence of decidual deficiency, making PAS unlikely in this case. It should be noted, however, that definitive exclusion of PAS would require hysterectomy specimens, and the absence of placental adherence at delivery does not entirely rule out focal or superficial forms of PAS.
As described above, our MR–pathologic correlation revealed that T2 dark bands primarily represent thrombus formation. 4 However, this thrombus showed hyperintensity on T2-weighted imaging, and no T2 dark bands was identified. Meanwhile, it demonstrated hyperintensity on DWI resembling the surrounding placenta. These findings may be explained by stage-dependent changes in signal intensity of the thrombus. 10 It might have been identified as T2 dark bands if obtained at a different stage.
Although the initial MRI in this case was performed earlier than the 28–32 weeks recommended in the SAR–ESUR joint consensus statement, previous studies suggest that placental MRI is generally reliable after 24 weeks’ gestation. 11 Therefore, the MRI findings obtained at 27 weeks in the present case are likely to be reliable. Furthermore, even at 32 weeks of gestation, the thrombus was not depicted as T2 dark bands. These findings suggest that, rather than gestational age itself, understanding the underlying pathophysiology and recognizing the potential for signal intensity changes are essential.
The limitation of the present case is the lack of corresponding ultrasound findings. However, MRI has recently been increasingly applied to placental research using various advanced techniques. 12 The identification of DL represents one such example. Radiologists should further utilize MRI to explore the placenta, which may be regarded as one of the last frontiers in imaging research, in order to gain new insights into placental pathophysiology.
Conclusion
Signal changes on DWI were observed within DL presumed to represent placental lakes, which were pathologically confirmed to represent thrombi. The present findings suggest that villous-devoid regions within the placenta may undergo thrombus formation due to blood flow stasis. This temporal evolution is considered important not only for the interpretation of placental MRI but also for understanding the underlying placental pathophysiology.
Footnotes
Ethical considerations
This case report was approved by the Institutional Review Board (2026, No. 26J002).
Consent to participate
The requirement for written informed consent was waived.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Japan Society for the Promotion of Science (25K10912).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.