
Abstract
Background
Primary care physicians and family medicine resident physicians report continued gaps in knowledge when diagnosing and managing pediatric patients with concussion.
Methods
A cross-sectional electronic survey of 130 primary care physicians and family medicine resident physicians in the Northeastern Ontario Local Health Integration Network (LHIN). Descriptive statistics, chi-squared Fisher exact tests, were used to compare physicians versus resident physicians with two-tailed p < 0.05 (with 95% confidence intervals).
Results
With a 48% response rate, when treating concussions 44% of providers either did not use any specific clinical practice guideline, standardized assessment tool, could not recall the source of a specific tool/guideline or omitted answering the question. However, 61% of all respondents would refer some or all concussion patients to a specialist for treatment. At least 41% of providers indicated they lacked access to a ‘Provider Decision Support Tool’ specific to concussion, and 88% of the 25 providers were without access to discharge instructions.
Conclusion
Similar to other jurisdictions, Northeastern Ontario primary care physicians and family medicine resident physicians report gaps in knowledge for both diagnosis and management of pediatric concussion. Consequently, they did not use current guidelines or best practices to guide management.
Introduction
Pediatric concussion is a major public health concern for the primary care physician. It is a common injury with immediate, as well as potential long term health related complications, that occurs in children and adolescents participating in recreational activities and sports.1,2 In 2011, the Center for Disease Control and Prevention estimated over 175,000 children and adolescents are treated annually in American emergency departments, where concussions account for 9 to 12% of all injuries in high school athletes. 3 More recently, in the US, from a population of 8.8 million private-payer insured parties, 43,884 (0.5%) were diagnosed with concussions. Of these, 55% were male and 32% were adolescents. 4 This same group saw a 60% increase in concussion diagnoses between 2007 and 2014. 4 Similarly, Gaw and Zonfrillo 5 report the annual injury rate per 10,000 population increased from 55.2 in 2007 to 85.4 in 2011. The largest increases were in children under 11 years and adults over 65 years. Recent data from Ontario, Canada found a mean incidence of 1153 per 100 000 residents in a given year (1.2% of the population) with children representing both the highest incidence 6 and highest rates of persistent symptoms.7,8 Some estimate 95% of family physicians see and treat concussions, despite a wide variance in base knowledge and management strategies. 2 Itriyeva et al., 9 in their attitudes and practices survey, report 98.7% of primary care respondents had seen at least one case in the past year, despite the fact 48.6% reported having inadequate neurocognitive assessment training. Primary care practice in Canada and particularly in the rural context of Northern Ontario, does differ in coverage and access to care compared to other areas in the country and internationally. Medical care in Canada is publicly funded however access to rehabilitative treatment providers (in Ontario) is largely not publically funded. Given the lower socioeconomic demographic across Northern Ontario, accessibility is impacted. In addition, within the publicly funded care, wait times are often lengthy and interprofessional referral centres for concussion specifically are very limited and/or geographically distant. Further, as concussion knowledge, diagnosis and management are continually evolving, front line primary care physicians in Canada and the US continue to report gaps in knowledge and training,2,9 inadequate application of existing evidence based, graded return to learn and play guidelines, as well as discomfort in diagnosing and managing concussion in the pediatric population.2,9–11
In Zonfrillo et al., 11 self-reported attitudes and practices were measured in a subgroup of US physicians and primary care providers regarding pediatric concussion diagnosis and management. Primary care providers felt they lacked adequate training and infrastructure to diagnose, educate patients and comfortably manage this demographic. 11 Others have since found similar results.9,12,13 Given these continuing deficits, the goal of the current study was to examine self-reported pediatric concussion practices, knowledge, referral patterns and attitudes of primary care practitioners and resident family physicians in a rural setting: Northeastern Ontario, Canada. With increased attention to concussion injuries and sequelae in traditional and social media, we posit current medical trainees have a greater awareness surrounding undiagnosed concussions and potential sequelae. However, as demonstrated by Mann et al. 12 in an urban environment at the University of Toronto, a deficit in knowledge base, practice patterns and limited familiarity with concussion clinical practice guidelines may persist. 14 Similar findings were reported by Herceg et al. 15 who found deficiencies in knowledge of concussion diagnosis, treatment, recovery and prognosis among family physicians in Croatia.
Methods
A cross-sectional study targeted primary care physicians in family medicine, emergency departments and walk-in clinic settings, as well as family medicine residents completing their training in Northeastern Ontario, Canada. The survey sought self-reported information surrounding practices, attitudes, barriers and knowledge of concussion in the pediatric population. 11 An electronic survey was distributed to 130 eligible physicians and family medicine residents in the Northeastern Ontario LHIN (Local Health Integration Network) across rural, remote and urban settings reflecting the territory of the East Campus of the Northern Ontario School of Medicine (NOSM). The recruitment period extended across three months, ending in February 2016. Potential primary care physician survey participants were identified from physician recruitment and retention officers for the jurisdictions of interest. Residents were contacted via a shared email list maintained by the medical school. Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at Laurentian University. 16 Two reminders were sent, approximately 1 every 3 weeks, to eligible participants who had not responded. No incentive was provided for participation.
The survey included 87 items, including multiple-choice, Likert-scale, free-text questions and scenarios designed to capture demographic information, measure physician comfort and competency in treating pediatric concussion patients and assess barriers to concussion care. This survey was based largely on the tool developed by Zonfrillo et al. 11 Three scenarios were used which are from a previously validated survey Zonfrillo et al. 11 Each hypothetical scenario (Appendix) represents a case with decreasing ambiguity. The intent was to determine practitioner confidence in dealing with this ambiguity when forming a diagnosis.
Statistical analysis
Data from the REDCAP database was downloaded into SPSS software for statistical analyses (SPSS version 22, SPSS Inc., Chicago, Illinois). Demographic and descriptive statistics were calculated in addition to Chi-squared and Fischer’s exact tests, which were used to examine the difference in responses between the resident and attending physician groups. A two-tailed analysis was performed, with p < 0.05 and 95% confidence intervals. Missing data was excluded from analysis.
Ethics approval
Research Ethics approval for this study was obtained from the university’s institutional research ethics board. A cover letter was provided electronically with the survey distribution noting that by completing the survey, participants had provided implied consent and participation was voluntary.
Results
A total of 62 respondents (from a possible 130) completed the survey; a 48% response rate. Table 1 shows demographic data including the number of years since medical school, geographic location and primary practice setting. Table 1 also reports the number of concussion patients treated, as well as referral patterns.
Demographics of survey respondents.

Across all respondents, the SCAT-3 tool was the most commonly cited initial approach utilized. Forty four percent of respondents indicated they either “did not use a guideline at all”, “couldn’t recall the name of the guideline they used when treating concussion”, or chose not to answer this question.
Table 2 reports responses to a scenario-based case that measured the ability of respondents to diagnose and manage pediatric concussion cases based on most up to date guidelines. Three clinical scenarios (see Appendix), which differed in the subtlety of the concussion symptoms, were included (Case 1: most subtle to Case 3: least (direct helmet-to-helmet injury and classic concussion symptoms)). As a follow-up to this question, in Figure 1, a significant proportion of practitioners incorrectly identified the more subtle signs of concussion as non-contributory to diagnosis: tinnitus 36% (95% CI: 23%–48%), perseveration 31% (95% CI: 20%–43%), positive Romberg sign 28% (95% CI: 17%–39%), abnormal eye tracking 18% (95% CI: 8%–28%), visual problems 18% (95% CI: 8%–28%), and vomiting 18% (95% CI: 8%–28%).
Scenario-based case response for likelihood of diagnosis, treatment, and referral for concussion.
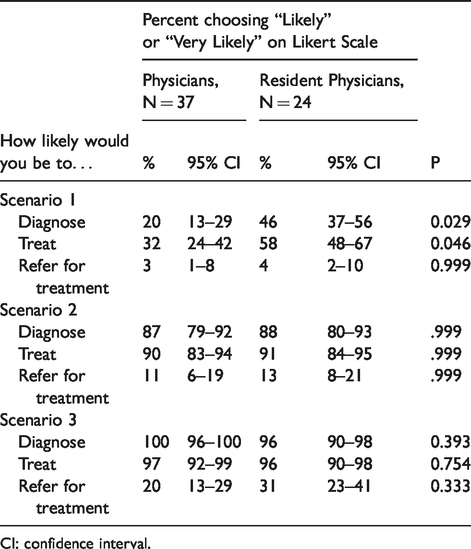
CI: confidence interval.

Relevancy of signs and symptoms for the diagnosis of a concussion.
Table 3 lists the barriers for providers to implementing initial concussion management strategies including formal neurocognitive testing, educating families about the diagnosis, recommending appropriate time to resume school, and prescribing a gradual return to play protocol for sports. A statistically significant number of attending and resident physicians identified barriers; in particular, inadequate training and inadequate time to complete neurocognitive testing were identified.
Barriers surrounding concussion management.

CI: confidence interval.
Discussion
Most practitioners captured in our study population were seeing and treating pediatric concussion patients with some regularity, yet, as in other studies,9,11,12 self-reported deficiencies in knowledge surrounding diagnosis and management. Practitioners were often unable to identify a guideline used in their pediatric concussion management, which suggests 1) a likely deficiency in education or learning and 2) inconsistency in approach to diagnosis and management among individual practices. This inconsistency was reflected in the free-text analysis which indicated a wide variety of diagnostic and management styles from one practitioner to another. These findings are in keeping with other literature, which revealed only 9.4% of US physicians used the International Consensus Statements.2,17,18 A high percentage of both practising primary care physicians and family medicine resident physicians, were unable to correctly recognize and identify subtle signs and symptoms of pediatric concussion as potentially contributing to the overall clinical picture. However, in the clinical scenarios presented, family medicine resident physicians were more likely than practicing primary care physicians to correctly diagnose, and opt to treat, a patient with more subtle signs of concussion. With respect to formal neurocognitive testing (NCT), primary care physicians and resident physicians disagreed as to their role in the use of NCT to aid diagnosis and management of pediatric patients with concussion. Interestingly, all responding resident physicians felt it was within their scope to use NCT and had fewer concerns with time pressure to complete them. Both groups, however, identified training and a lack of local resources for referral, such as neuropsychology, as barriers to comprehensive NCT and care. This finding is similar to others9,10,12 who have also shown considerable gaps in knowledge and application of best practice and reference guidelines to assist with treatment of concussion. Zemek et al. 10 also found similar barriers to care, such as lack of local expertise or concussion specialists in the geographical area and a lack of awareness that this type of specialist exists. However, in larger metropolitan areas this does not seem to be as prevalent.9,12
Our survey revealed that, while 100% of the primary care physicians felt it was their role to educate patients and family about concussion, 14% noted significant lack of training to do so. Similarly, Zonfrillo et al., 11 found while 99% of primary care providers acknowledged it was their role to educate patients and families, alarmingly only 16% felt they had adequate training and 16–30% felt they had inadequate resources to properly manage concussions or recommend return to play and learn. Given our data supports previous literature, 2 which indicated primary care physicians are regularly managing sport and recreational related concussion, we are in agreement there is a need for optimization and inclusion of enhanced formal educational concussion management strategies and training opportunities for medical learners, residents and practicing physicians. The literature further suggests our findings surrounding accurate diagnosis of concussion in patients with subtle symptoms are consistent with existing studies in the field. Zonfrillo et al., 11 identified primary pediatric practitioners in Philadelphia area pediatric hospitals were also unable to consistently identify the subtle signs of concussion (tinnitus, perseveration, and abnormal eye tracking). This is similar to both Taylor et al. 19 and Mann et al., 12 who also note challenges interpreting nonspecificity and vagueness of symptoms, as well as the lack of formal diagnostic criteria. The physicians in that study also had more difficulty correctly diagnosing concussed pediatric patients presented in a clinical scenario with more subtle signs of concussion, which is consistent with our results.11,19 Resident physicians were more likely than physicians already in practice to correctly identify these patients. This finding may reflect an increasing awareness and shift in pediatric concussion, from one of ignoring the injury to one of absolute and immediate cognitive rest with graded return to learn, play or work. However, given the lack of specific training provided to the surveyed cohort of family medicine residents regarding pediatric concussion and diagnosis, this may represent a growing cultural awareness, spurred by recent events in the national sporting arena, rather than a concerted educational effort on the part of the residency program.
Interestingly, the rate of referral for treatment of pediatric concussion was somewhat lower in our study (61%) than reported in at least one other study (76.6%), 9 but proved similar to findings by Zemek et al. 10 Patients with ongoing symptoms, despite initial appropriate management strategies, are at risk of protracted recovery and should be referred to a medical practitioner with experience in concussion management. 20 More recent research recommends referral to an experienced interprofessional management team for those with persistent symptoms or risk factors for protracted recovery.21,22 This rate of referral pattern may reflect the rurality and relative isolation of many of the practice locations surveyed and the lack of providers with expertise available to treat concussion. Moreover, referral depends on the local availability of knowledgeable rehabilitation health professionals such as chiropractors, physiotherapists, occupational therapists, psychologists and others who may not practice in these areas or have the appropriate knowledge about concussive injury and best practices. Alternately, this referral pattern may reflect the lack of economic resources of patients in these areas, who are unable to pay for uninsured health care services, or confidence in their family medicine practitioners in managing without further referral.
This study was limited by the discrepancies in community inclusion based on physician recruiter response, and by the comprehensiveness of the contact lists. Our study was also limited by a relatively short recruitment period. Some practitioners may have felt inconvenienced or hampered by the electronic response form, so further studies in the area could include provision of a paper copy of the form. However, it should be noted that the response rate (48%) for this survey was similar to Zonfrillo’s deployment of the survey (53%). 11 In addition we recognize that there may be a bias in terms of who responds where, conceivably, those who are more interested and knowledgeable in the area are more likely to respond.
Conclusion
In conclusion, both primary care physicians and family medicine resident physicians in rural areas (particularly northern Ontario) may benefit from further formal and accredited training opportunities and education in the field of pediatric concussion in medical school, residency training and via CME sessions. Further, clinicians may benefit from dissemination and widespread adoption of standardized clinical decision making tools and patient discharge instructions. Such tools have been developed by the Center for Effective Practice for the adult population since data collection occurred for the study. 23 Future study of utilization of the standardized diagnostic and education tool would speak to the utility of this approach in the pediatric population. Availability and utilization have remained dichotomies in practice in concussion diagnosis and management. A comprehensive listing of qualified regulated health professionals providing neurocognitive testing and evidence-based concussion treatment would also be helpful in making practitioners more aware of the resources available in their communities. Ideally, medically-led interprofessional concussion teams or clinics with health care providers who have expertise in concussion would be available even in rural cities with outreach available to more remote locations. Barriers to uptake would need to be considered with the availability of such tools more recently, however no known new data is available on the clinical application and use of such resources. Lastly, research into concussion prevalence in subgroups across the northern context, which evolves over time, could assist with targeting appropriate evidence based protocols.
Footnotes
Acknowledgements
The authors wish to thank Dr. Mark Zonfrillo, M.D. for sharing the survey used in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Northern Ontario Academic Medicine Association’s Clinical Innovation Opportunities Fund.